")
Back to Journals » Hepatic Medicine: Evidence and Research » Volume 15
Clinical and Histopathological Discoveries in Patients with Hepatic Injury and Cholangiopathy Who Have Died of COVID-19: Insights and Opportunities for Intervention
Received 15 June 2023
Accepted for publication 28 September 2023
Published 4 October 2023 Volume 2023:15 Pages 151—164
DOI https://doi.org/10.2147/HMER.S385133
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gerry Lake-Bakaar
Joseph K Lim, Basile Njei
Yale Liver Center and Section of Digestive Diseases, Yale University School of Medicine, New Haven, CT, USA
Correspondence: Joseph K Lim, Yale Liver Center and Section of Digestive Diseases, Yale University School of Medicine, 333 Cedar Street, LMP 1080, New Haven, CT, 06520, USA, Email [email protected]
Abstract: The COVID-19 pandemic has had a profound impact on global health, necessitating a comprehensive understanding of its diverse manifestations. Cholangiopathy, a condition characterized by biliary dysfunction, has emerged as a significant complication in COVID-19 patients. In this review, we report the epidemiology of COVID-19, describe the hepatotropism of SARS-CoV-2, and present the histopathology of acute liver injury (ALI) in COVID-19. Additionally, we explore the relationship between pre-existing chronic liver disease and COVID-19, shedding light on the increased susceptibility of these individuals to develop cholangiopathy. Through an in-depth analysis of cholangiopathy in COVID-19 patients, we elucidate its clinical manifestations, diagnostic criteria, and underlying pathogenesis involving inflammation, immune dysregulation, and vascular changes. Furthermore, we provide a summary of studies investigating post-COVID-19 cholangiopathy, highlighting the long-term effects and potential management strategies for this condition, and discussing opportunities for intervention, including therapeutic targets, diagnostic advancements, supportive care, and future research needs.
Keywords: cholangiopathy, COVID-19, long-COVID-19, histopathology, interventions
Introduction
The COVID-19 pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has resulted in a global health crisis since its emergence in December 2019. It has affected millions of individuals worldwide, and its impact extends beyond respiratory manifestations, involving various organ systems, including the liver.1–3 The incidence and implications of COVID-19-associated liver dysfunction, particularly cholangiopathy, have gained significant attention in emerging research. While the respiratory aspects of COVID-19 have been the primary focus of research and clinical management, mounting evidence suggests that the disease can also lead to liver dysfunction and cholangiopathy.4–6 The liver, being vital to the body’s immune response and susceptible to viral infections, including SARS-CoV-2, plays a crucial role in understanding the disease’s pathophysiology and potential interventions. Exploring the relationship between COVID-19 and cholangiopathy holds promise for uncovering new intervention strategies and improving clinical outcomes for patients with COVID-19-associated liver dysfunction.
This comprehensive review aims to address several key aspects. Firstly, understanding the epidemiology, hepatotropism, and histopathology of COVID-19-related liver dysfunction is crucial. By examining the prevalence, incidence, and associated risk factors, we can gain insights into the epidemiological aspects of COVID-19 liver dysfunction. Exploring the hepatotropism of SARS-CoV-2 provides a deeper understanding of the involvement of the liver in COVID-19. Furthermore, investigating the histopathology of acute liver injury (ALI) helps elucidate specific changes in liver tissue. Additionally, it is important to recognize the interaction between pre-existing chronic liver disease and COVID-19, as it impacts disease severity and outcomes. By summarizing the emerging literature on COVID-19 cholangiopathy and discussing opportunities for managing cholangiopathy in subjects who have died of COVID-19, this review aims to contribute to existing knowledge and facilitate the development of targeted strategies to improve patient care and outcomes.
Epidemiology of COVID-19
In December 2019, the first occurrence of SARS-CoV-2, an RNA virus, was documented in humans in Wuhan, China.7 This viral infection, known as COVID-19, continues to pose a significant global public health crisis. The World Health Organization (WHO) reports that COVID-19 has impacted over 750 million individuals worldwide and has resulted in more than 6 million deaths.8 Within the United States, the number of diagnosed COVID-19 cases has exceeded 100 million, with over 1 million cumulative deaths attributed to complications from the disease.9 When discussing the epidemiology of COVID-19, it is important to note that certain individuals may be at a higher risk of experiencing severe illness or complications from COVID-19.10 This includes older adults, particularly those over the age of 65, as well as individuals with underlying health conditions such as heart disease, lung disease, diabetes, obesity, and weakened immune systems.10,11 Other factors that may increase the risk include living in congregate settings such as nursing homes or crowded households, working in high-risk settings with close contact to others, and belonging to certain racial or ethnic groups that have been disproportionately affected by the virus.12 Initially regarded as primarily affecting the respiratory system, COVID-19 is now acknowledged to impact various organs, including the lungs, heart, brain, endothelium, kidneys, and liver.2,3
Hepatotropism of SARS-CoV-2
Emerging evidence suggests that SARS-CoV-2 enters host cells through the ACE2 receptor,13 with TMPRSS2 playing a crucial role in viral entry.14,15 The spike protein (S) of SARS-CoV-2 interacts with ACE2 and TMPRSS2 receptors,16 and there is increasing recognition of the involvement of additional accessory receptors, such as SR-B1, in viral attachment.13 Notably, SR-B1 expression facilitates SARS-CoV-2 entry into ACE2-expressing cells, including cholangiocytes in the liver.17
In the liver, SARS-CoV-2 can induce local inflammation by activating liver-resident immune cells or directly infecting cholangiocytes and hepatocytes that express ACE2 receptors.18–20 The virus promotes intracellular cytotoxic actions in hepatocytes, resulting in cell membrane destruction and cellular structure edema.21,22 While cholangiocytes predominantly experience biliary injury due to higher ACE2 expression, hepatocyte injury can be more predominant in cases of re-infection or liver damage, where ACE2 expression increases during hepatocyte regeneration.19,20,23 Additionally, SARS-CoV-2 infection affects mitochondrial activity and induces oxidative stress,24–26 leading to potential complications such as steatohepatitis and exacerbation of comorbidities like non-alcoholic fatty liver disease (NAFLD).27 Furthermore, severe infection can trigger a cytokine storm, involving the release of proinflammatory cytokines and chemokines, which can damage multiple organs, including the liver.28–43
Histopathology of COVID-19 in the Liver
Histological examination of liver tissue from COVID-19 patients reveals various vascular abnormalities, steatosis (accumulation of fat in liver cells), and mitochondrial abnormalities, suggesting a multifactorial pathogenesis of liver injury. These changes can be attributed to multiple factors, including direct viral damage to hepatocytes/cholangiocytes, immune-mediated liver damage, systemic inflammation, hypoxia, and drug-induced liver injury.19,27,31,35,40,44–58 Proteomic studies have further revealed dysregulation of liver proteins associated with hepatic steatosis, sinusoidal congestion, necrosis, vascular thrombosis, hepatic fibrosis, Kupffer cell proliferation, and portal inflammation.59
Liver histopathological changes observed in COVID-19 patients range from moderate micro-vesicular steatosis with mild lobular and portal inflammation to focal necrosis.25,60–62 One of the earliest pieces of evidence came from liver biopsy of a 50-year-old man who was diagnosed with COVID-19. Histopathology of his liver tissue showed moderate microvesicular steatosis and mild lobular activity.42 Furthermore, macrovesicular hepatic steatosis, characterized by the accumulation of larger fat droplets, is commonly observed in COVID-19 patients.25,49,60,63–65 Additionally, mild lobular and portal inflammation, as well as infrequent vascular pathology like sinusoidal microthrombi, have been reported.62 Studies involving proteomic analysis have detected SARS-CoV-2 RNA in liver tissue and identified the presence of the virus within hepatocytes using electron microscopy.38,54
Pre-Existing Chronic Liver Disease and COVID-19
Pre-existing chronic liver disease (CLD), particularly cirrhosis, is associated with impaired immune function and increased vulnerability to infections, including COVID-19.21,33,52,66 Cirrhosis-associated immune dysfunction (CAID) leads to alterations in innate and adaptive immunity, dysfunctional macrophage activation, impaired neutrophil and lymphocyte function, Toll-like receptor dysfunction, and increased gut permeability with changes in the gut microbiome.67,68 COVID-19 patients with pre-existing chronic liver disease, especially cirrhosis, have higher rates of hospitalization, mortality, thromboembolism, and severe disease course compared to those without liver disease.69,70 Alcohol-associated liver disease (AALD) and decompensated cirrhosis, in particular, pose the highest risk for all-cause mortality from COVID-19.33,69–71
Patients with chronic hepatitis B or hepatitis C infection without advanced fibrosis or cirrhosis do not appear to have a greater risk of acquiring or experiencing worse outcomes with COVID-19.72–74 While HCV-infected individuals may have a higher likelihood of hospitalization, no independent association with death has been observed for HBV or HCV.70,72,75 Direct-acting antiviral therapy for HCV may be delayed in patients with COVID-19, although there is some evidence suggesting potential benefits of these antivirals in treating COVID-19.40,76–78 NAFLD, the most common chronic liver disease, may impact the course of COVID-19, with higher mortality and need for mechanical ventilation observed in NAFLD patients.25,50,64,65,79,80 The impact of COVID-19 on individuals with autoimmune hepatitis (AIH) is comparable to that of non-immunosuppressed persons, contrary to initial speculations that AIH patients may be protected due to immunosuppression.22,81,82 Finally, the impact of COVID-19 on liver transplant recipients is controversial, with some studies reporting increased risk of COVID-19-related death and others suggesting increased risk of hospitalization but not higher mortality, thrombosis, or ICU requirement compared to non-transplanted COVID-19 patients. Medications used by liver transplant recipients may influence outcomes, with tacrolimus potentially associated with better outcomes and mycophenolate mofetil identified as an independent predictor of severe COVID-19.40,83
Cholangiopathy in COVID-19
Cholangiopathy, a term encompassing diseases affecting the bile ducts, has emerged as a noteworthy aspect of COVID-19 pathology. Cholangiopathy is a rare but severe complication of COVID-19 infection. The pathophysiology of COVID-19 cholangiopathy is not yet fully understood, but it is believed to be related to the virus’s direct or indirect effects on the liver and bile ducts. COVID-19 cholangiopathy can present as liver infarction, severe cholangiopathy, biliary cast syndrome, and progressive cholangiopathy. The intricate pathophysiology underpinning COVID-19 cholangiopathy remains a subject of ongoing investigation. Current understanding suggests a complex interplay of the virus’s direct or indirect impact on both the liver and bile ducts. Sequential synergies between Systemic Inflammatory Response (SIR) triggered by the viral infection, Non-Alcoholic Steatohepatitis (NASH), and hypoxemia may initiate a cascade of events. This cascade culminates in oxidative stress, which could subsequently prompt mitochondrial biogenesis while diminishing oxidative capacity. The resultant imbalance may ultimately foster the development of ischemic cholangiopathy. This proposed model offers a glimpse into the intricate connections underlying hepatic health in the context of COVID-19, although further research to establish this is necessary.
Furthermore, several studies have investigated the risk factors associated with the development of cholangiopathy in COVID-19 patients. Risk factors identified include signs of systemic reduced blood oxygen supply, multi-organ failure, high fibrinogen levels, and intravenous ketamine use.84 Additionally, disease severity and the need for ICU admission have been linked to an increased risk of cholangiopathy.85 These findings suggest that certain demographic and clinical factors contribute to the development of cholangiopathy in individuals affected by COVID-19.
While a universally agreed-upon diagnostic criteria for post COVID-19 cholangiopathy is yet to be established, several studies have provided insights into its clinical manifestations and diagnostic approaches. Typically, severe COVID-19 cholangiopathy is characterized by elevated levels of alkaline phosphatase (ALP) greater than 1.5 times the upper limit of normal (ULN), serum bilirubin greater than 2 times the ULN, or gamma-glutamyl transferase (GGT) greater than 3.0 times the ULN.86–89 Notably, these patients often lack active sepsis or underlying chronic liver disease, which suggests a direct association between COVID-19 and cholestasis or liver injury. Imaging studies such as magnetic resonance cholangiopancreatography (MRCP) have revealed various bile duct abnormalities, including biliary strictures, beaded appearance of intrahepatic bile ducts,86,90 biliary dilation,5,91 and irregularities of the common bile duct. Additionally, endoscopic retrograde cholangiopancreatography (ERCP) may be employed to assess the bile ducts more extensively, manage biliary strictures, or address choledocholithiasis, which can contribute to cholestasis.89
Summary of Studies on Post-COVID-19 Cholangiopathy
Emerging research in the literature has investigated cholangiopathy in post-COVID-19 patients. Post-COVID-19 cholangiopathy is a novel entity that has been increasingly reported in the literature.85–94 upon those basis, we conducted a scoping review of the literature, and Table 1 presents the findings as a summary of study characteristics for reports on cholangiopathy in COVID-19, with additional summaries for histopathological findings (Table 2) and MRCP/ERCP findings (Table 3). These investigations have documented various manifestations of biliary system involvement, including persistent liver dysfunction, cholestasis, and biliary abnormalities. For instance, Zhang et al identified biliary dilatation and sludge formation in the gallbladder as common findings in post-COVID-19 patients.43 Similarly, among COVID-19 pneumonia patients in an ICU in Zurich, four cases with persistent elevated cholestatic markers and abnormal imaging were reported. MRCP showed irregular bile ducts with stricturing. Diagnosis of cholangiopathy ranged from two weeks to over nine months. Mechanical ventilation and hydroxychloroquine treatment were required. Two patients died, one underwent liver transplant evaluation, and one had persistent disease after one year.95
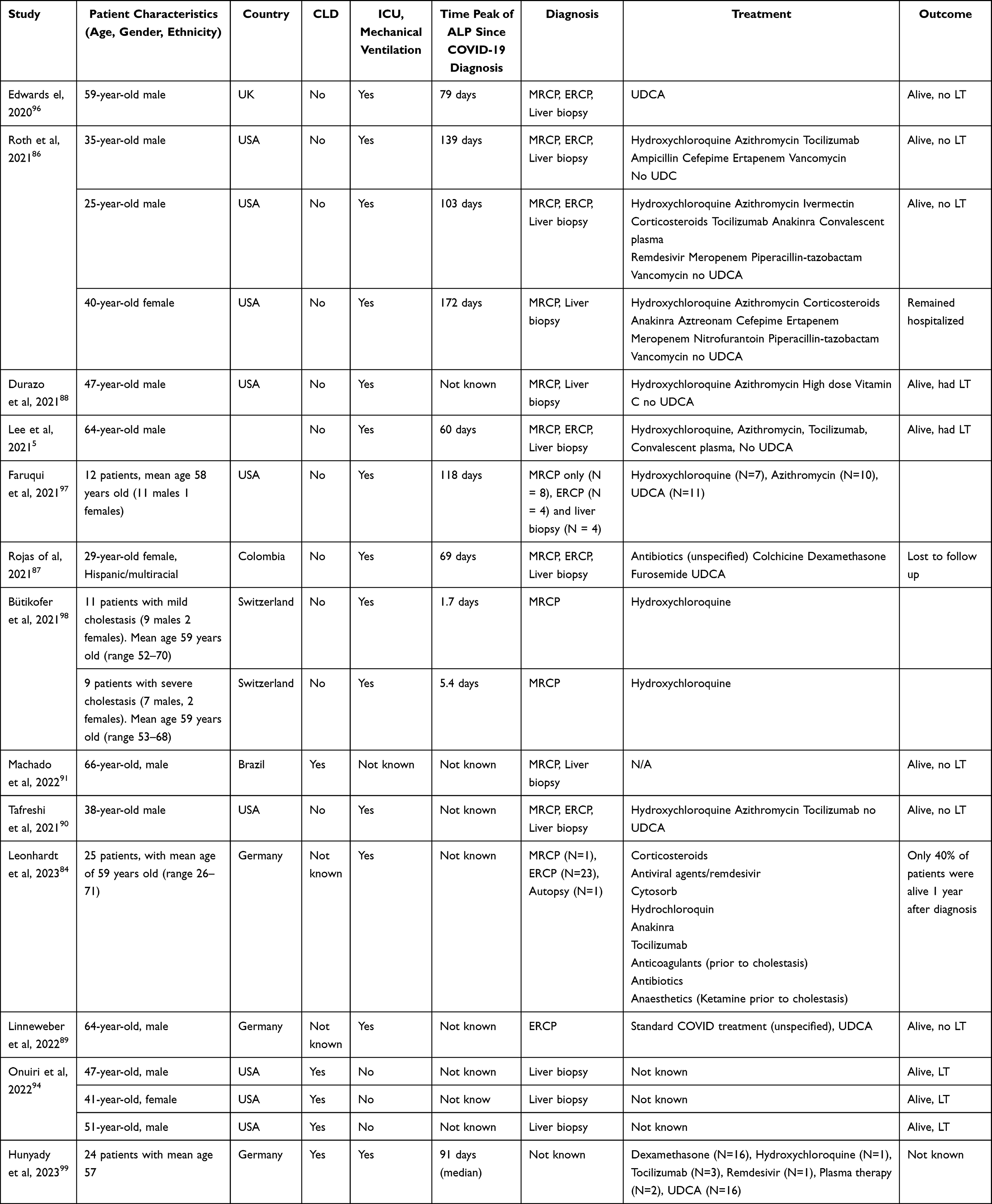 |
Table 1 Summary of Study Characteristics for Case Reports and Case-Control Studies on Cholangiopathy in COVID-19 |
 |
Table 2 Summary of Histopathological Findings |
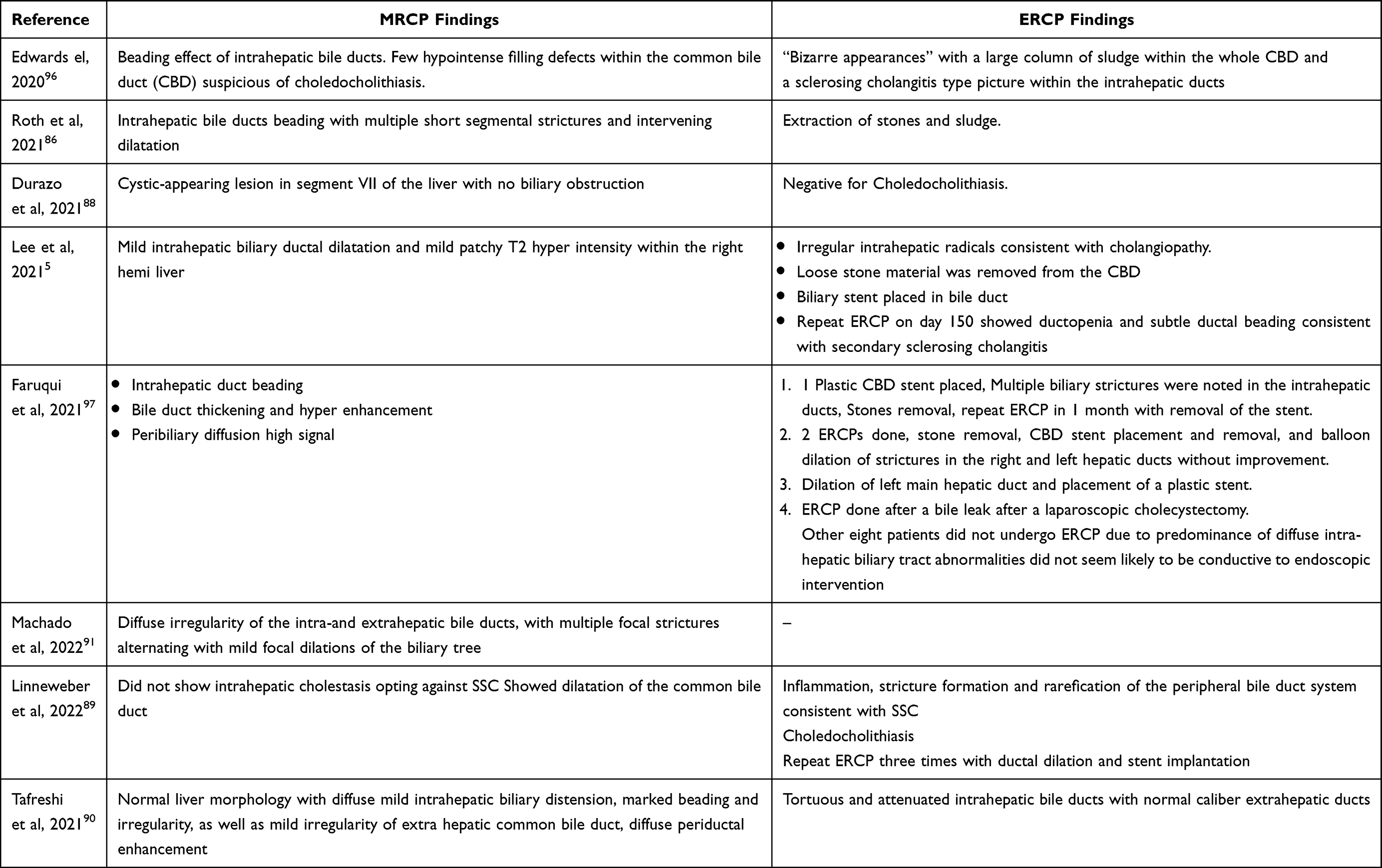 |
Table 3 Summary of MRCP and ERCP Findings |
Numerous studies have also reported secondary sclerosing cholangitis (SSC) in post-covid-19 patients. Leonhardt et al, conducted an observational study to investigate the occurrence and outcomes of SSC as a long-term complication of COVID-19.84 Their findings revealed that SSC occurred exclusively in critically ill patients who required invasive ventilation, with a clustering effect observed among them. The occurrence rate of SSC in invasively ventilated COVID-19 patients was approximately 1 in 43. Risk factors associated with SSC development included signs of reduced blood oxygen supply, multi-organ failure, high fibrinogen levels, and intravenous ketamine use. The study highlighted severe tissue hypoxia and fibrinogen-associated circulatory disturbances as potential mechanisms underlying SSC in COVID-19 patients. The 1-year transplant-free survival rate for COVID-19-associated SSC was reported to be 40%, and an increase in SSC cases is anticipated in the post-COVID era. Moreover, Linneweber et al documented two cases in Germany where biliary injury emerged during the recuperation phase from COVID-19.89 Both patients experienced the development of biliary strictures, necessitating ERCP and stent insertion. MRCP results exhibited a general conformity with SSC. While one patient remained stable but needed multiple ERCP procedures, the other patient exhibited progressive intrahepatic bile duct destruction and succumbed to the condition eight months after the initial diagnosis. Similar studies reporting SSC after COVID-19 infections are becoming increasingly prevalent in the literature, including cases in the United Kingdom,96 Switzerland,98 United States,5 and Colombia.87 It is important to note that all reported cases of cholangiopathy in COVID-19, identified since May 2021, have been in individuals who had experienced severe COVID-19. Severe cases are characterized by factors such as ICU admission, the need for intubation or ECMO due to respiratory or circulatory failure or requiring vasopressor support. However, Onuiri et al, reported three cases of post-COVID-19 cholangiopathy arising in patients who recovered from severe COVID-19.94 In a retrospective review, six cases of COVID-19-related cholangiopathy were identified, including three cases in patients who did not develop critical COVID-19. Histological analysis of these cases revealed features consistent with secondary sclerosing cholangitis.94
Finally, Hunyady et al presented a pioneering retrospective cohort study that marks a significant step forward in the investigation of COVID-related SSC within ICU settings, distinct from the isolated case reports dominating prior research.99 Encompassing 127 patients across 9 German tertiary care centers, the study comprehensively contrasts COVID-SSC with SSC-CIP, shedding light on transplant-free survival determinants. Notably, COVID-SSC’s median onset occurred 91 days post-COVID-19 diagnosis, following extensive ICU care, including a median 48-day ventilation period.
Of particular interest, the comparison between COVID-SSC and SSC-CIP highlights striking similarities in clinical aspects and disease progression. Furthermore, valuable therapeutic insights emerge, with Ursodeoxycholic acid (UDCA) use and heightened serum albumin levels correlating independently with improved transplant-free survival. This is in line with other preliminary findings reported by Brevini et al, which demonstrated a correlation between UDCA treatment and positive clinical outcomes after SARS-CoV-2 infection using retrospective registry data and confirm these findings in an independent validation cohort of recipients of liver transplants.100 Additionally, they have shown that UDCA reduces farnesoid X receptor (FXR) signaling and downregulate ACE2 in human lung, cholangiocyte and intestinal organoids and in the corresponding tissues in mice and hamsters. In turn, UDCA-mediated downregulation of ACE2 reduces susceptibility to SARS-CoV-2 infection in vitro, in vivo and in human lungs and livers perfused ex situ.100
Opportunities for Intervention
Despite the growing knowledge about cholangiopathy in COVID-19, there remains an urgent need for effective interventions to address this complex condition. With the epidemiology, hepatotropism, and histopathology of COVID-19-associated cholangiopathy established, it is crucial to explore potential opportunities for intervention that could improve patient outcomes. In this section, we discuss the current gaps in our understanding and present potential strategies for intervention in cholangiopathy associated with COVID-19, aiming to pave the way for targeted approaches that can optimize patient care and improve overall outcomes.
Therapeutic Targets
COVID-19-related cholangiopathy poses a significant clinical challenge, necessitating the exploration of therapeutic targets to mitigate liver injury and promote regeneration. One potential avenue for intervention lies in targeting key pathways involved in cholangiocyte injury and inflammation. Consequently, establishing the pathway(s) in which cholangiopathy occurs within the context of COVID-19 is detrimental. We reviewed the article by Hartl et al regarding progressive cholestasis and sclerosing cholangitis in COVID-19 patients with chronic liver disease and found their findings to be highly relevant.101 It has been observed that patients with pre-existing chronic liver diseases, such NAFLD, have an increased susceptibility to cholestatic liver failure following COVID-19. The underlying mechanism for this remains unclear but may involve the toxic effects of the virus on cholangiocytes and sepsis-induced cholestasis. Studies have indicated that SARS-CoV-2 can induce mitochondrial dysfunction, oxidative stress, and interfere with hepatic lipogenesis, potentially exacerbating comorbidities like NAFLD. In liver pathology studies of fatal COVID-19 cases, increased expression of inositol 1,4,5‐trisphosphate receptors (ITPR3) was observed alongside inflammation and hepatic steatosis, suggesting a potential role of ITPR3 in COVID-19 cholangiopathy.100 These findings highlight the potential for therapeutic intervention in COVID-19 cholangiopathy by targeting the identified mechanisms, such as mitochondrial dysfunction, oxidative stress, and altered calcium signaling through ITPR3 receptors. A deeper understanding of these mechanisms can pave the way for the development of targeted interventions to mitigate cholangiopathy progression and improve patient outcomes.
Patients with AALD and NAFLD are particularly vulnerable to hepatic dysfunction and decompensation following COVID-19 infection. The mechanisms underlying this association are not fully elucidated, but previous research has shown increased expression of inositol 1,4,5-trisphosphate receptors (ITPR3) and hepatic steatosis in lethal COVID-19 cases.102 Chronic alcohol consumption influences calcium (Ca2+) signaling, leading to sustained elevation in Ca2+ levels, and enhanced phospholipase C (PLC) activity, resulting in inositol 1,4,5-trisphosphate (IP3) production.103 Perturbations in Ca2+ signaling can affect mitochondrial function and contribute to mitochondrial reactive oxygen species formation and opening of the permeability transition pore (PTP).104 The combination of AALD and the pathological stress induced by COVID-19 infection may exacerbate hepatic dysfunction and worsen clinical outcomes, as demonstrated in our study. Targeting these mechanisms associated with chronic liver diseases, such as modulating Ca2+ signaling pathways and mitochondrial function, holds potential for therapeutic interventions to mitigate the impact of COVID-19-related cholangiopathy in susceptible populations. Further research is needed to explore the precise mechanisms and develop targeted interventions for this high-risk population.
Diagnostic Advancements
In the quest for improved diagnostic methods for COVID-19-related cholangiopathy, there is a pressing need for standardized diagnostic criteria. The utilization of advanced imaging techniques holds promise in enhancing diagnostic accuracy and facilitating the characterization of biliary abnormalities. Advanced magnetic resonance imaging (MRI) sequences, including MRCP, can provide detailed visualization of the biliary system, enabling the identification of strictures, dilation, and other pathological changes. Additionally, elastography techniques can assess liver stiffness and provide valuable insights into the presence of fibrosis and cholestasis. Finally, cholangioscopy has been shown to be a promising in establishing early diagnosis.105
In parallel, identifying specific biomarkers associated with cholangiopathy could revolutionize the diagnostic process. Biomarkers, such as liver enzymes, cytokines, and molecular markers, may serve as early indicators of biliary dysfunction and help differentiate COVID-19-related cholangiopathy from other liver diseases. Early detection through biomarker analysis can enable timely intervention and risk stratification, allowing for targeted therapeutic approaches. By harnessing the potential of advanced imaging techniques and identifying reliable biomarkers, clinicians can improve the accuracy and efficiency of diagnosing COVID-19-related cholangiopathy. These diagnostic advancements will not only aid in the early detection and risk assessment but also contribute to a better understanding of the pathogenesis and natural history of the disease, ultimately guiding the development of effective interventions and improving patient outcomes.
Supportive and Tailored Care
Supportive care plays a vital role in the management of patients with COVID-19-related cholangiopathy, focusing on optimizing patient outcomes and alleviating associated complications. Continuous monitoring of liver function tests, including ALP, bilirubin, and GGT is essential for the early detection of cholestasis, allowing for timely intervention and treatment adjustment. Serial measurements of these biomarkers can aid in risk stratification, tracking disease progression, and assessing the response to therapeutic interventions.
In the presence of complications such as choledocholithiasis or biliary strictures, endoscopic interventions can offer significant benefits. ERCP enables both diagnostic and therapeutic interventions, allowing for the identification and removal of biliary stones, as well as the placement of stents to relieve biliary obstruction. By addressing these underlying factors, ERCP not only improves biliary flow but also mitigates the risk of complications such as ascending cholangitis and liver abscesses. Regular monitoring and intervention in cases of biliary obstruction can contribute to improved outcomes and enhance the overall management of COVID-19-related cholangiopathy. In addition to specific interventions, supportive care strategies should encompass general measures aimed at optimizing the patient’s overall well-being. This includes close monitoring of fluid and electrolyte balance, nutritional support, and appropriate pain management. Multidisciplinary collaboration among hepatologists, gastroenterologists, infectious disease specialists, and intensivists is crucial to tailor the supportive care approach to the individual patient’s needs, ensuring comprehensive management and improved clinical outcomes.
Future Research
Future research in the field of COVID-19-related cholangiopathy should aim to investigate the long-term effects of the disease and expand our understanding of its implications, considering the significant impact of COVID-19 on the population at large. Further studies employing chart review methodologies are needed to identify and validate risk factors associated with COVID-19-induced liver injury. This will facilitate risk stratification of COVID-19 patients, leading to improved long-term outcomes. Additionally, there is a need to delve into the pathobiology of patients exhibiting a mixed pattern of ALI, and longitudinal data on COVID-19 patients are crucial in determining whether hepato-cholangiopathy resolves or persists as a chronic condition. To gain further insights, future research can explore the role of ACE2, ITPR3 receptors, mitochondrial Ca2+ signals, as well as the influence of AALD and NAFLD in enhancing COVID-19 hepato-cholangiopathy. Complementary investigations using cell cultures, animal models, or liver biopsy specimens can shed light on whether SARS-CoV-2 directly affects cholangiocytes, resulting in liver injury with cytopathic effects. These research avenues hold promise in uncovering underlying mechanisms and guiding potential interventions for COVID-19-related cholangiopathy. Finally, future research endeavors should also delve into the intricate dynamics between COVID-19 infection and the increased prevalence of autoimmune disorders observed during the pandemic, such as Type 1 Diabetes (T1D), Sjogren’s syndrome, Systemic Lupus Erythematosus (SLE), Rheumatoid Arthritis, and autoimmune thyroid disease. Understanding the multifaceted interactions and potential implications for disease severity, distinct from the clear association observed in secondary sclerosing cholangitis (SSC), could illuminate novel avenues for intervention and contribute to a more comprehensive understanding of the evolving landscape of COVID-19-related hepatic complications.
Ethics Approval and Informed Consent
This manuscript is a review article and does not involve any primary research or data collection from human subjects. As such, it does not require ethics approval. Additionally, this review does not involve the collection of personal data or the inclusion of individual patient information. Therefore, informed consent from human subjects is not applicable.
Funding
The authors declare that there was no specific funding received for the research, authorship, or publication of this manuscript.
Disclosure
Dr Joseph K Lim reports grants from Intercept, Viking, Novo Nordisk, Gilead, Pfizer, and Inventiva, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Alenazy AES, Alabdulwahab K, Alabdulwahab F, Alanazi SIS. Cutaneous manifestations and types of skin affection associated with COVID-19 infection: a simple review. Arch Pharm Pract. 2022;13(2):95.
2. Lala A, Johnson KW, Januzzi JL, et al. Prevalence and impact of myocardial injury in patients hospitalized with COVID-19 infection. J Am Coll Cardiol. 2020;76(5):533–546. doi:10.1016/j.jacc.2020.06.007
3. Elrobaa IH, New KJ. COVID-19: pulmonary and extra pulmonary manifestations. Front Public Health. 2021;9:711616. doi:10.3389/fpubh.2021.711616
4. Hanif FM, Majid Z, Ahmed S, Luck NH, Mubarak M. Hepatic manifestations of coronavirus disease 2019 infection: clinical and laboratory perspective. World J Virol. 2022;11(6):453. doi:10.5501/wjv.v11.i6.453
5. Lee A, Wein AN, Doyle MBM, Chapman WC. Liver transplantation for post-COVID-19 sclerosing cholangitis. BMJ Case Rep CP. 2021;14(8):e244168. doi:10.1136/bcr-2021-244168
6. Feng Y, Liu Y, Zhao Q, et al. Liver injury in patients with COVID-19: a Retrospective Study. Int J Med Sci. 2023;20(3):385. doi:10.7150/ijms.81214
7. Lu H, Stratton CW, Tang YW. Outbreak of pneumonia of unknown etiology in Wuhan, China: the mystery and the miracle. J Med Virol. 2020;92(4):401–402. doi:10.1002/jmv.25678
8. World Health Organization. WHO Coronavirus (COVID-19) Dashboard; 2022. Available from: https://covid19.who.int/.
9. Centers for Disease Control and Prevention. COVID Data Tracker. Atlanta, GA: US Department of Health and Human Services, CDC; 2022. Available from: https://covid.cdc.gov/covid-data-tracker.
10. Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. 2020;369. doi:10.1136/bmj.m1966
11. Ganatra S, Hammond SP, Nohria A. The Novel Coronavirus Disease (COVID-19) Threat for Patients with Cardiovascular Disease and Cancer. Vol. 2. Washington DC: American College of Cardiology Foundation; 2020:350–355.
12. Barnett ML, Grabowski DC. Nursing homes are ground zero for COVID-19 pandemic.
13. Hoffmann M, Kleine-Weber H, Schroeder S, et al. SARS-CoV-2 Cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181(2):271–280.e278. doi:10.1016/j.cell.2020.02.052
14. Menachery VD, Dinnon KH, Yount BL, et al. Trypsin treatment unlocks barrier for zoonotic bat coronavirus infection. J Virol. 2020;94(5). doi:10.1128/JVI.01774-19
15. Simmons G, Gosalia DN, Rennekamp AJ, Reeves JD, Diamond SL, Bates P Inhibitors of cathepsin L prevent severe acute respiratory syndrome coronavirus entry. Proc Natl Acad Sci U S A. 2005;102(33):11876–11881.
16. Jackson CB, Farzan M, Chen B, Choe H. Mechanisms of SARS-CoV-2 entry into cells. Nat Rev Mol Cell Biol. 2022;23(1):3–20. doi:10.1038/s41580-021-00418-x
17. Wei C, Wan L, Yan Q, et al. HDL-scavenger receptor B type 1 facilitates SARS-CoV-2 entry. Nat Metabol. 2020;2(12):1391–1400. doi:10.1038/s42255-020-00324-0
18. Chidambaram V, Shanmugavel Geetha H, Kumar A, et al. Association of lipid levels with COVID-19 infection, disease severity and mortality: a systematic review and meta-analysis. Front Cardiovasc Med. 2022;9:862999. doi:10.3389/fcvm.2022.862999
19. Li D, Ding X, Xie M, Tian D, Xia L. COVID-19-associated liver injury: from bedside to bench. J Gastroenterol. 2021;56(3):218–230. doi:10.1007/s00535-021-01760-9
20. Li Y, Xiao S-Y. Hepatic involvement in COVID-19 patients: pathology, pathogenesis, and clinical implications. J Med Virol. 2020;92(9):1491–1494. doi:10.1002/jmv.25973
21. Ge J, Pletcher MJ, Lai JC, Harper JR, Chute CG, Haendel MA. Outcomes of SARS-CoV-2 infection in patients with chronic liver disease and cirrhosis: a National COVID Cohort Collaborative Study. Gastroenterology. 2021;161(5):1487–1501.e1485. doi:10.1053/j.gastro.2021.07.010
22. Gerussi A, Rigamonti C, Elia C, et al. Coronavirus disease 2019 in autoimmune hepatitis: a lesson from immunosuppressed patients. Hepatol Commun. 2020;4(9):1257–1262. doi:10.1002/hep4.1557
23. Li D, Long Y, Huang P, et al. Clinical characteristics of 80 patients with COVID-19 in Zhuzhou City. J Chin J Infect Control. 2020;19(03):227–233.
24. Chu H, Chan JF, Yuen TT, et al. Comparative tropism, replication kinetics, and cell damage profiling of SARS-CoV-2 and SARS-CoV with implications for clinical manifestations, transmissibility, and laboratory studies of COVID-19: an observational study. Lancet Microbe. 2020;1(1):e14–e23. doi:10.1016/S2666-5247(20)30004-5
25. Ji D, Qin E, Xu J, et al. Non-alcoholic fatty liver diseases in patients with COVID-19: a retrospective study. J Hepatol. 2020;73(2):451–453. doi:10.1016/j.jhep.2020.03.044
26. Koliaki C, Szendroedi J, Kaul K, et al. Adaptation of hepatic mitochondrial function in humans with non-alcoholic fatty liver is lost in steatohepatitis. Cell Metab. 2015;21(5):739–746. doi:10.1016/j.cmet.2015.04.004
27. Nardo AD, Schneeweiss-Gleixner M, Bakail M, Dixon ED, Lax SF, Trauner M. Pathophysiological mechanisms of liver injury in COVID-19. Liver Int. 2021;41(1):20–32. doi:10.1111/liv.14730
28. Bangash MN, Patel JM, Parekh D, et al. SARS-CoV-2: is the liver merely a bystander to severe disease? J Hepatol. 2020;73(4):995–996. doi:10.1016/j.jhep.2020.05.035
29. Bryce C, Grimes Z, Pujadas E, et al. Pathophysiology of SARS-CoV-2: the Mount Sinai COVID-19 autopsy experience. Mod Pathol. 2021;34(8):1456–1467. doi:10.1038/s41379-021-00793-y
30. Chen C, Zhou Y, Wang DW. SARS-CoV-2: a potential novel etiology of fulminant myocarditis. Herz. 2020;45(3):230–232. doi:10.1007/s00059-020-04909-z
31. Chen LY, Chu HK, Bai T, et al. Liver damage at admission is an independent prognostic factor for COVID-19. J Dig Dis. 2020;21(9):512–518. doi:10.1111/1751-2980.12925
32. Khateri S, Mohammadi H, Khateri R, Moradi Y. The prevalence of underlying diseases and comorbidities in COVID-19 patients; an updated systematic review and meta-analysis. Arch Acad Emerg Med. 2020;8(1):e72–e72.
33. Bajaj JS, Garcia-Tsao G, Biggins SW, et al. Comparison of mortality risk in patients with cirrhosis and COVID-19 compared with patients with cirrhosis alone and COVID-19 alone: multicentre matched cohort. Gut. 2021;70(3):531. doi:10.1136/gutjnl-2020-322118
34. Kulkarni AV, Kumar P, Tevethia HV, et al. Systematic review with meta-analysis: liver manifestations and outcomes in COVID-19. Aliment Pharmacol Ther. 2020;52(4):584–599. doi:10.1111/apt.15916
35. Kumar MP, Mishra S, Jha DK, et al. Coronavirus disease (COVID-19) and the liver: a comprehensive systematic review and meta-analysis. Hepatol Int. 2020;14(5):711–722. doi:10.1007/s12072-020-10071-9
36. Kumar P, Sharma M, Kulkarni A, Rao PN. Pathogenesis of liver injury in Coronavirus Disease 2019. J Clin Exp Hepatol. 2020;10(6):641–642. doi:10.1016/j.jceh.2020.05.006
37. Moreira JLS, Barbosa SMB, Gonçalves Júnior J. Pathophysiology and molecular mechanisms of liver injury in severe forms of COVID-19: an integrative review. Clin Res Hepatol Gastroenterol. 2021;45(6):101752. doi:10.1016/j.clinre.2021.101752
38. Phipps MM, Barraza LH, LaSota ED, et al. Acute liver injury in COVID-19: prevalence and association with clinical outcomes in a large US cohort. Hepatology. 2020;72(3):807–817. doi:10.1002/hep.31404
39. Shokri Afra H, Amiri-Dashatan N, Ghorbani F, Maleki I, Rezaei-Tavirani M. Positive association between severity of COVID-19 infection and liver damage: a systematic review and meta-analysis. Gastroenterol Hepatol Bed Bench. 2020;13(4):292–304.
40. Spearman CW, Aghemo A, Valenti L, Sonderup MW. COVID-19 and the liver: a 2021 update. Liver Int. 2021;41(9):1988–1998. doi:10.1111/liv.14984
41. Wu Y, Li H, Guo X, et al. Incidence, risk factors, and prognosis of abnormal liver biochemical tests in COVID-19 patients: a systematic review and meta-analysis. Hepatol Int. 2020;14(5):621–637. doi:10.1007/s12072-020-10074-6
42. Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8(4):420–422. doi:10.1016/S2213-2600(20)30076-X
43. Zhang Y, Zheng L, Liu L, Zhao M, Xiao J, Zhao Q. Liver impairment in COVID-19 patients: a retrospective analysis of 115 cases from a single centre in Wuhan city, China. Liver Int. 2020;40(9):2095–2103. doi:10.1111/liv.14455
44. Bloom PP, Meyerowitz EA, Reinus Z, et al. Liver Biochemistries in Hospitalized Patients With COVID-19. Hepatology. 2021;73(3):890–900. doi:10.1002/hep.31326
45. Du M, Yang S, Liu M, Liu J. COVID-19 and liver dysfunction: epidemiology, association and potential mechanisms. Clin Res Hepatol Gastroenterol. 2022;46(2):101793. doi:10.1016/j.clinre.2021.101793
46. Feng G, Zheng KI, Yan QQ, et al. COVID-19 and liver dysfunction: current insights and emergent therapeutic strategies. J Clin Transl Hepatol. 2020;8(1):18–24. doi:10.14218/JCTH.2020.00018
47. Gabrielli M, Franza L, Esperide A, et al. Liver injury in patients hospitalized for COVID-19: possible role of therapy. Vaccines. 2022;10(2):192. doi:10.3390/vaccines10020192
48. Hundt MA, Deng Y, Ciarleglio MM, Nathanson MH, Lim JK. Abnormal liver tests in COVID-19: a retrospective observational cohort study of 1827 patients in a major US hospital network. Hepatology. 2020;72(4):1169–1176. doi:10.1002/hep.31487
49. Jothimani D, Venugopal R, Abedin MF, Kaliamoorthy I, Rela M. COVID-19 and the liver. J Hepatol. 2020;73(5):1231–1240. doi:10.1016/j.jhep.2020.06.006
50. Marjot T, Webb GJ, Barritt AS, et al. COVID-19 and liver disease: mechanistic and clinical perspectives. Nat Rev Gastroenterol Hepatol. 2021;18(5):348–364. doi:10.1038/s41575-021-00426-4
51. Moon AM, Barritt A. Elevated liver enzymes in patients with COVID-19: look, but not too hard. Dig Dis Sci. 2021;66(6):1767–1769. doi:10.1007/s10620-020-06585-9
52. Sarin SK, Choudhury A, Lau GK, et al. Pre-existing liver disease is associated with poor outcome in patients with SARS CoV2 infection; the APCOLIS Study (APASL COVID-19 Liver Injury Spectrum Study). Hepatol Int. 2020;14(5):690–700. doi:10.1007/s12072-020-10072-8
53. Schaefer EAK, Arvind A, Bloom PP, Chung RT. Interrelationship between coronavirus infection and liver disease. Clin Liver Dis. 2020;15(5):175–180. doi:10.1002/cld.967
54. Singh S, Khan A. Clinical characteristics and outcomes of coronavirus disease 2019 among patients with preexisting liver disease in the United States: a Multicenter Research Network Study. Gastroenterology. 2020;159(2):768–771.e763. doi:10.1053/j.gastro.2020.04.064
55. Tang H, Zhou L, Li X, et al. Drug-induced liver injury associated with lopinavir-ritonavir in patients with COVID-19: a disproportionality analysis of U.S. food and drug administration adverse event reporting system (FAERS) data. Int J Clin Pharm. 2021;43(4):1116–1122. doi:10.1007/s11096-021-01311-5
56. Wan J, Wang X, Su S, et al. Digestive symptoms and liver injury in patients with coronavirus disease 2019 (COVID-19): a systematic review with meta-analysis. JGH Open. 2020;4(6):1047–1058. doi:10.1002/jgh3.12428
57. Z-h W, Yang D. A meta-analysis of the impact of COVID-19 on liver dysfunction. Eur J Med Res. 2020;25(1):54. doi:10.1186/s40001-020-00454-x
58. Yadav DK, Singh A, Zhang Q, et al. Involvement of liver in COVID-19: systematic review and meta-analysis. Gut. 2021;70(4):807–809. doi:10.1136/gutjnl-2020-322072
59. Nie X, Qian L, Sun R, et al. Multi-organ proteomic landscape of COVID-19 autopsies. Cell. 2021;184(3):775–791.e714. doi:10.1016/j.cell.2021.01.004
60. Chornenkyy Y, Mejia-Bautista M, Brucal M, et al. Liver pathology and SARS-CoV-2 detection in formalin-fixed tissue of patients with COVID-19. Am J Clin Pathol. 2021;155(6):802–814. doi:10.1093/ajcp/aqab009
61. Kushner T, Cafardi J. Chronic liver disease and COVID-19: alcohol use disorder/alcohol-associated liver disease, nonalcoholic fatty liver disease/nonalcoholic steatohepatitis, autoimmune liver disease, and compensated cirrhosis. Clin Liver Dis. 2020;15(5):195–199. doi:10.1002/cld.974
62. Lagana SM, Kudose S, Iuga AC, et al. Hepatic pathology in patients dying of COVID-19: a series of 40 cases including clinical, histologic, and virologic data. Mod Pathol. 2020;33(11):2147–2155. doi:10.1038/s41379-020-00649-x
63. Díaz LA, Idalsoaga F, Cannistra M, et al. High prevalence of hepatic steatosis and vascular thrombosis in COVID-19: a systematic review and meta-analysis of autopsy data. World J Gastroenterol. 2020;26(48):7693–7706. doi:10.3748/wjg.v26.i48.7693
64. Sachdeva S, Khandait H, Kopel J, Aloysius MM, Desai R, Goyal H. NAFLD and COVID-19: a pooled analysis. SN Comprehen Clin Med. 2020;2(12):2726–2729. doi:10.1007/s42399-020-00631-3
65. Zhou YJ, Zheng KI, Wang XB, et al. Metabolic-associated fatty liver disease is associated with severity of COVID-19. Liver Int. 2020;40(9):2160–2163. doi:10.1111/liv.14575
66. Leo M, Galante A, Pagnamenta A, et al. Hepatocellular liver injury in hospitalized patients affected by COVID-19: presence of different risk factors at different time points. Dig Liver Dis. 2022;54(5):565–571. doi:10.1016/j.dld.2021.12.014
67. Bajaj JS. Altered microbiota in cirrhosis and its relationship to the development of infection. Clin Liver Dis. 2019;14(3):107–111. doi:10.1002/cld.827
68. Yeoh YK, Zuo T, Lui GC-Y, et al. Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. Gut. 2021;70(4):698. doi:10.1136/gutjnl-2020-323020
69. Kovalic AJ, Satapathy SK, Thuluvath PJ. Prevalence of chronic liver disease in patients with COVID-19 and their clinical outcomes: a systematic review and meta-analysis. Hepatol Int. 2020;14(5):612–620. doi:10.1007/s12072-020-10078-2
70. Marjot T, Moon AM, Cook JA, et al. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: an international registry study. J Hepatol. 2021;74(3):567–577. doi:10.1016/j.jhep.2020.09.024
71. Williamson EJ, Walker AJ, Bhaskaran K, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. 2020;584(7821):430–436. doi:10.1038/s41586-020-2521-4
72. Butt AA, Yan P. Rates and characteristics of SARS-CoV-2 infection in persons with hepatitis C virus infection. Liver Int. 2021;41(1):76–80. doi:10.1111/liv.14681
73. Guan W-J, Z-Y N, Hu Y, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi:10.1056/NEJMoa2002032
74. He Q, Zhang G, Gu Y, et al. Clinical characteristics of COVID-19 patients with pre-existing hepatitis b virus infection: a multicenter report. Am J Gastroenterol. 2021;116(2):420–421. doi:10.14309/ajg.0000000000000924
75. Kim D, Adeniji N, Latt N, et al. Predictors of outcomes of COVID-19 in patients with chronic liver disease: US Multi-center Study. Clin Gastroenterol Hepatol. 2021;19(7):1469–1479.e1419. doi:10.1016/j.cgh.2020.09.027
76. Fix OK, Blumberg EA, Chang KM, et al. American Association for the Study of liver diseases expert panel consensus statement: vaccines to prevent Coronavirus Disease 2019 infection in patients with liver disease. Hepatology. 2021;74(2):1049–1064. doi:10.1002/hep.31751
77. Fix OK, Hameed B, Fontana RJ, et al. Clinical best practice advice for hepatology and liver transplant providers during the COVID-19 pandemic: AASLD Expert Panel Consensus Statement. Hepatology. 2020;72(1):287–304. doi:10.1002/hep.31281
78. Simmons B, Wentzel H, Mobarak S, et al. Sofosbuvir/daclatasvir regimens for the treatment of COVID-19: an individual patient data meta-analysis. J Antimicrob Chemother. 2021;76(2):286–291. doi:10.1093/jac/dkaa418
79. Hashemi N, Viveiros K, Redd WD, et al. Impact of chronic liver disease on outcomes of hospitalized patients with COVID-19: a multicentre United States experience. Liver Int. 2020;40(10):2515–2521. doi:10.1111/liv.14583
80. Shelton JF, Shastri AJ, Ye C, et al. Trans-ancestry analysis reveals genetic and nongenetic associations with COVID-19 susceptibility and severity. Nat Genet. 2021;53(6):801–808. doi:10.1038/s41588-021-00854-7
81. D’Antiga L. Coronaviruses and immunosuppressed patients: the facts during the third epidemic. Liver Transplant. 2020;26(6):832–834. doi:10.1002/lt.25756
82. Marjot T, Buescher G, Sebode M, et al. SARS-CoV-2 infection in patients with autoimmune hepatitis. J Hepatol. 2021;74(6):1335–1343. doi:10.1016/j.jhep.2021.01.021
83. Belli LS, Fondevila C, Cortesi PA, et al. Protective role of tacrolimus, deleterious role of age and comorbidities in liver transplant recipients with Covid-19: results from the ELITA/ELTR Multi-center European Study. Gastroenterology. 2021;160(4):1151–1163.e1153. doi:10.1053/j.gastro.2020.11.045
84. Leonhardt S, Jürgensen C, Frohme J, et al. Hepatobiliary long-term consequences of COVID-19: dramatically increased rate of secondary sclerosing cholangitis in critically ill COVID-19 patients. Hepatol Int;2023. 1–16. doi:10.1007/s12072-023-10521-0
85. Yadlapati S, Jarrett SA, Baik D, Chaaya A. COVID-19 related biliary injury: a review of recent literature. World J Gastroenterol. 2023;29(14):2127. doi:10.3748/wjg.v29.i14.2127
86. Roth NC, Kim A, Vitkovski T, et al. Post-COVID-19 Cholangiopathy: a Novel Entity. Am J Gastroenterol. 2021;116(5):1077–1082. doi:10.14309/ajg.0000000000001154
87. Rojas M, Rodríguez Y, Zapata E, Hernández JC, Anaya J-M. Cholangiopathy as part of post-COVID syndrome. J Transl Autoimmun. 2021;4:100116. doi:10.1016/j.jtauto.2021.100116
88. Durazo FA, Nicholas AA, Mahaffey JJ, et al. Post–Covid-19 cholangiopathy—a new indication for liver transplantation: a case report.
89. Linneweber L, Mann AB, Denk G, Kraft E, Weber S. Cholangiopathy in early rehabilitation after intensive care treatment of patients with COVID-19. Off J Am College Gastroenterol. 2022;117(1):197–198. doi:10.14309/ajg.0000000000001511
90. Tafreshi S, Whiteside I, Levine I, D’Agostino C. A case of secondary sclerosing cholangitis due to COVID-19. Clin Imaging. 2021;80:239–242. doi:10.1016/j.clinimag.2021.07.017
91. Machado MCC, Kalil Filho R, El Bacha IAH, et al. Post-COVID-19 secondary sclerosing cholangitis: a rare but severe condition with no treatment besides liver transplantation. Am J Case Rep. 2022;23:e936250–e936251. doi:10.12659/AJCR.936250
92. Wongtanasarasin W. Cholestatic liver injury: a rare but fatal complication during and after COVID-19 infection. World J Virol. 2022;11(6):435. doi:10.5501/wjv.v11.i6.435
93. Bauer U, Pavlova D, Abbassi R, et al. Secondary sclerosing cholangitis after COVID-19 pneumonia: a report of two cases and review of the literature. Clin J Gastroenterol. 2022;15(6):1–6.
94. Onuiri J, Fiel M. COVID cholangiopathy can occur despite mild COVID. Am J Clin Pathol. 2022;158(Supplement_1):S128–S129. doi:10.1093/ajcp/aqac126.272
95. Mallet V, Bock K, Mandengue PD, et al. Intravenous ketamine and progressive cholangiopathy in COVID-19 patients. J Hepatol. 2021;74(5):1243–1244. doi:10.1016/j.jhep.2021.02.007
96. Edwards K, Allison M, Ghuman S. Secondary sclerosing cholangitis in critically ill patients: a rare disease precipitated by severe SARS-CoV-2 infection. BMJ Case Rep CP. 2020;13(11):e237984. doi:10.1136/bcr-2020-237984
97. Faruqui S, Okoli FC, Olsen SK, et al. Cholangiopathy after severe COVID-19: clinical features and prognostic implications. Am J Gastroenterol. 2021;116(7):1414–1425. doi:10.14309/ajg.0000000000001264
98. Bütikofer S, Lenggenhager D, Wendel Garcia PD, et al. Secondary sclerosing cholangitis as cause of persistent jaundice in patients with severe COVID‐19. Liver Int. 2021;41(10):2404–2417. doi:10.1111/liv.14971
99. Hunyady P, Streller L, Rüther DF, et al. Secondary sclerosing cholangitis following Coronavirus Disease 2019 (COVID-19): a Multicenter Retrospective Study. Clin Infect Dis. 2023;76(3):e179–e187. doi:10.1093/cid/ciac565
100. Brevini T, Maes M, Webb GJ, et al. FXR inhibition may protect from SARS-CoV-2 infection by reducing ACE2. Nature. 2023;615(7950):134–142. doi:10.1038/s41586-022-05594-0
101. Hartl L, Haslinger K, Angerer M, et al. Progressive cholestasis and associated sclerosing cholangitis are frequent complications of COVID‐19 in patients with chronic liver disease. Hepatology. 2022;76(6):1563–1575. doi:10.1002/hep.32582
102. Santana MF, Guerra MT, Hundt MA, et al. Correlation between clinical and pathological findings of liver injury in 27 patients with lethal COVID‐19 infections in Brazil. Hepatol Commun. 2022;6(2):270–280. doi:10.1002/hep4.1820
103. Bartlett PJ, Antony AN, Agarwal A, et al. Chronic alcohol feeding potentiates hormone‐induced calcium signalling in hepatocytes. J Physiol. 2017;595(10):3143–3164. doi:10.1113/JP273891
104. Iwakiri Y, Nathanson MH. Alcohol and calcium make a potent cocktail. J Physiol. 2017;595(10):3109. doi:10.1113/JP274133
105. Kroepfl V, Treml B, Freund MC, Profanter C. Early detection of COVID-19 cholangiopathy using cholangioscopy—a case report of two critically ill patients. Eur Surg. 2022;54(6):326–330. doi:10.1007/s10353-022-00776-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.