")
Back to Journals » Open Access Journal of Sports Medicine » Volume 14
Calisthenics: Epidemiology of Injury Patterns and Their Risk Factors
Authors McDonald-Wedding L, Goodwin L , Preston A , McKay G, Williams C
Received 1 November 2022
Accepted for publication 4 April 2023
Published 24 May 2023 Volume 2023:14 Pages 47—57
DOI https://doi.org/10.2147/OAJSM.S394044
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff
Laura McDonald-Wedding,1 Lauren Goodwin,2 Annabel Preston,3 Gaylene McKay,4 Cylie Williams3
1Austin Health, Heidelberg, VIC, 3078, Australia; 2Department of Health Sciences, School of Public Health and Preventive Medicine, Monash University, Alfred Medical Research and Education Precinct (AMREP), Melbourne, VIC, 3004, Australia; 3Department of Physiotherapy, School of Primary and Allied Health Care, Monash University, Frankston, VIC, 3199, Australia; 4Alphington Sports Medicine Exercise and Rehabilitation, Alphington, VIC, 3078, Australia
Correspondence: Laura McDonald-Wedding, Austin Health, 145 Studley Road, Heidelberg, Victoria, Australia, Tel +61 403 313 972, Email [email protected]
Objective: To quantify the prevalence and nature of injuries and their risk factors in calisthenics to, therefore, inform the practitioner what to expect from these athletes.
Methods: This study was an online cross-sectional survey of calisthenics athletes. Data were collected online and the survey was distributed via social media over six months in 2020. The purpose-built survey consisted of demographic, training and loading questions. Participants were provided with an injury definition and reported their total number of injuries sustained during calisthenics including detailed information on three most significant injuries, along with mechanism of injury and risk factors. Multivariate regression analyses were used to determine objective factors associated with the number of injuries.
Results: There were 543 participants describing 1104 injuries. Mean (standard deviation (SD)) injury prevalence was 4.5 (3.3) per person. Of these injuries, 820 (74.3%) required training modification or treatment. Participants missed a mean (SD) 3.4 (5.1) weeks of training and engaged in a mean (SD) 10.9 (9.1) health professional consultations. The most common injuries were upper leg (24.5%), ankle/foot (22.8%) and lumbar spine (19.3%), with the majority being sprains/strains in nature (56.3%). Mechanism of injury included elevated work (27.6%), overuse (38.0%) and specific calisthenics skills (38.9%) – such as lumbar (40.6%) and lower limb (40.3%) extension-based movements. Subjective risk factors included load (66.8%), preparation (55.9%) and environmental factors (21.0%). Objective risk factors associated with higher numbers of injuries included increased years of participation, left leg dominance, increased training hours (regardless of training type) and state team participation (p< 0.05).
Conclusion: Practitioners need to be aware that calisthenics athletes demonstrate a high proportion of strain/sprain injuries involving the lower limb and lumbar spine with causative movements being extension-based. Addressing risk factors such as loading, preparation, asymmetry, and the environment related to these movements are important for the treating practitioner.
Keywords: sport injury, injury epidemiology, calisthenics, dancing, gymnastics, ballet, risk factors, injury prevention
Introduction
The sport of calisthenics, originating in Australia, offers athletes the opportunity to perform in groups and individually. Its unique design consists of several disciplines practiced to music, and usually performed on stage in competition, with origins developed from American and European Physical Culture.1,2 Calisthenics adopts elements from gymnastics, ballet, musical theater and dance, and also involves handheld apparatus (rods and clubs).1,2 The disciplines consist of a core group of routines including figure march, free exercises (similar to artistic gymnastics floor), club swinging (similar to rhythmic gymnastics clubs), rod exercises and aesthetics (similar to contemporary style dance and ballet).1,2 While these disciplines involve a wide range of skills and movement patterns, strength, flexibility, and coordination play significant roles in determining athletes’ ability, along with non-physical factors such as musical interpretation and rhythm. Calisthenics is taught during childhood development from the age of three, with pupils progressing through Tinies (under 7s), Sub Juniors (7–10), Juniors (10–13), Intermediates (13–17), Seniors (18+) and Masters (26+) with no upper age limit set on participation.3 It is predominantly a team-based sport where athletes compete with a local club and can, in addition, compete at a national level, or once completing national examinations (called Levels) can perform as a solo and/or duo competitor. Local clubs compete at varying levels of competition from elite championship level as the highest, followed by division one through to division ten.3 Calisthenics is taught competitively and recreationally across Australia and New Zealand with growing numbers each year.3,4
Despite its growing popularity, there are few sports and exercise (SEM) clinicians familiar with this sport and less research to inform practitioners of the injury patterns involved. Only one study to date has focused on collecting data from calisthenics athletes. Research conducted in 1996 found a participant injury rate of 27.8% across one year in elite level athletes, with most injuries sustained at the lower-back, hip, thigh and groin.5
Due to the lack of data available for calisthenics athletes, clinicians must rely on research from other related sports. For instance, gymnastics has one of the highest injury incidences among female sport with 0.3–3.6 injuries per artistic gymnast,6,7 while professional ballet dancers demonstrate an incidence of 1.24 injuries per 1000 dance hours.8 In both cases lower limb and lower back injuries demonstrate a high occurrence. In ballet, foot/toe and ankle injuries demonstrate the highest prevalence with 25% and 21% respectively.8 The prevalence of lower back injury, on the other hand, is 13–15% in gymnastics and 17% in ballet.8–10 These regions, therefore, should be of interest to the treating practitioner.
While evidence in similar sporting genres may exist, it can be a guide only for the clinician until further calisthenics injury research is performed. The reasons for this are, firstly, calisthenics is unique; by contrast to ballet, calisthenics athletes typically train and perform barefoot, and contrary to ballet and gymnastics, calisthenics athletes train on hard flooring rather than sprung flooring or foam mats. Movement patterns are likewise unique, for instance, rod manipulation has no analogous sport known to the authors. As such, evidence surrounding ballet and gymnastics injuries cannot be directly transferred to calisthenics. Secondly, calisthenics is a rapidly growing recreational and competitive sport in both numbers and locations. Peak bodies tracking athlete numbers have seen registrations grow with 13,265 registered athletes in 2019 in Australia.3 Additionally, calisthenics is being practiced internationally with New Zealand hosting clubs and competitions since 2014.4 Thirdly, the sport of calisthenics has significantly changed since the previous research into calisthenics athletes was conducted.5 With athlete growth comes more competition and, therefore, in order to win there is a natural evolution of routines with new movement patterns and skills being introduced (often with increased difficulty/complexity). As a result, the sport appears very different when observing routines performed in 1996 compared with currently. Lastly, the previous calisthenics injury study surveyed athletes in the two highest levels of competition (state team and championship division), therefore no data to date exist for athletes competing in lower divisions.5 These factors cumulatively necessitate updated research on calisthenics injuries to inform SEM practitioners on current injury patterns and how they can help address them.
This study aimed to quantify the prevalence and nature of calisthenics injuries and their risk factors. Understanding these components will help inform the SEM practitioner on diagnosis, injury prevention and management in the calisthenics athlete. The implications of this research will also benefit athletes, as it will provide necessary information to clubs and governing associations to help improve safety within the sport and therefore injury prevention and athlete longevity.
Materials and Methods
This study was an online cross-sectional survey which received ethics approval (Approval Number: 23859).
Eligible participants were current or retired calisthenics athletes in Australia or New Zealand. The survey was distributed via social media (Facebook, LinkedIn, Twitter and Instagram) and calisthenics state organizations using survey-linked Uniform Resource Locators (URLs) and Quick Response (QR) codes, providing a convenience sample via snowballing technique. All participants provided online informed consent via a check box, or where the participant was under 18, parents provided online informed consent and supported survey completion. Participants were able to withdraw at any time by closing the browser.
Survey questions were initially pilot tested with three current or retired calisthenics athletes. Set one of the questions asked demographic information (eg, gender, age, state, years of calisthenics participation, types of participation and level). The second set of questions consisted of athletes’ training regimes and loading based questions (eg, hours class training, hours home training, hours other sports training). The final set of questions asked information pertaining to the number of injuries sustained and details of athletes’ three most significant injuries. Injury significance was a self-determined measure by the participants. These injury aspects included body region, diagnosis, laterality, acuity, severity, mechanism of injury and risk factors. Severity was divided into mild or moderate/severe, with moderate/severe being defined by an injury requiring either modification to training/choreography, health professional attendance or at least one class absence. Mild injuries were defined as not requiring these interventions.
To standardize injury responses, participants were provided with an injury definition11 and asked to report the number of different injuries they had sustained during calisthenics. This was to ensure a definitive number was given for each participant and they were describing a different injury rather than one chronic injury with multiple exacerbations. The upper limit of injuries was set at 20 injuries to minimize recall bias. Survey logic was used to minimize participants’ attrition rate, therefore depending on a participant’s answers only relevant questions were presented.
As this was the first survey of its kind, survey face validity was provided through researchers’ experience in injury management, research team’s participation in calisthenics as coaches and competitors, evidence in similar sporting genres and through pilot survey development. For instance, where a question asked for body region of injury, the upper and lower back were split into two separate answers for body part injured due to the high incidence of lower back injuries recorded in similar sporting genres such as gymnastics and ballet.8,9 Where applicable, participants were invited to provide free text responses.
The online survey was open with three separate advertisement drives on the different social media platforms and through club notices between 29/04/2020 and 17/09/2020. All data were collected through Qualtrics (Qualtrics Research Suite, 2013: Appendix A – Calisthenics Survey). Any non-completion was treated as missing data for the remaining non-completed variables. The CHERRIES (Checklist for Reporting Results of Internet E-Surveys) guided the reporting of collected data12 (Appendix B). Data were cleaned and responses removed if they were consent-only or demographic-only responses with no further data.
Free text responses were reviewed by two researchers independently and agreed upon coding the participant’s response to existing categories or creating new categories. New categories were created if multiple participants gave the same response (Appendix C – Coding rules). Categories were subsequently grouped together based on common themes decided by two researchers independently – these are listed in brackets, where relevant, in Table 1 and Table 2 and the breakdown can be found in Supplementary Data Table 1. Text responses where a specific calisthenics skill was named were reviewed and each component used as a search term to look for other responses containing the same answer. This provided a total number of participants who stated a specific skill as the mechanism of injury.
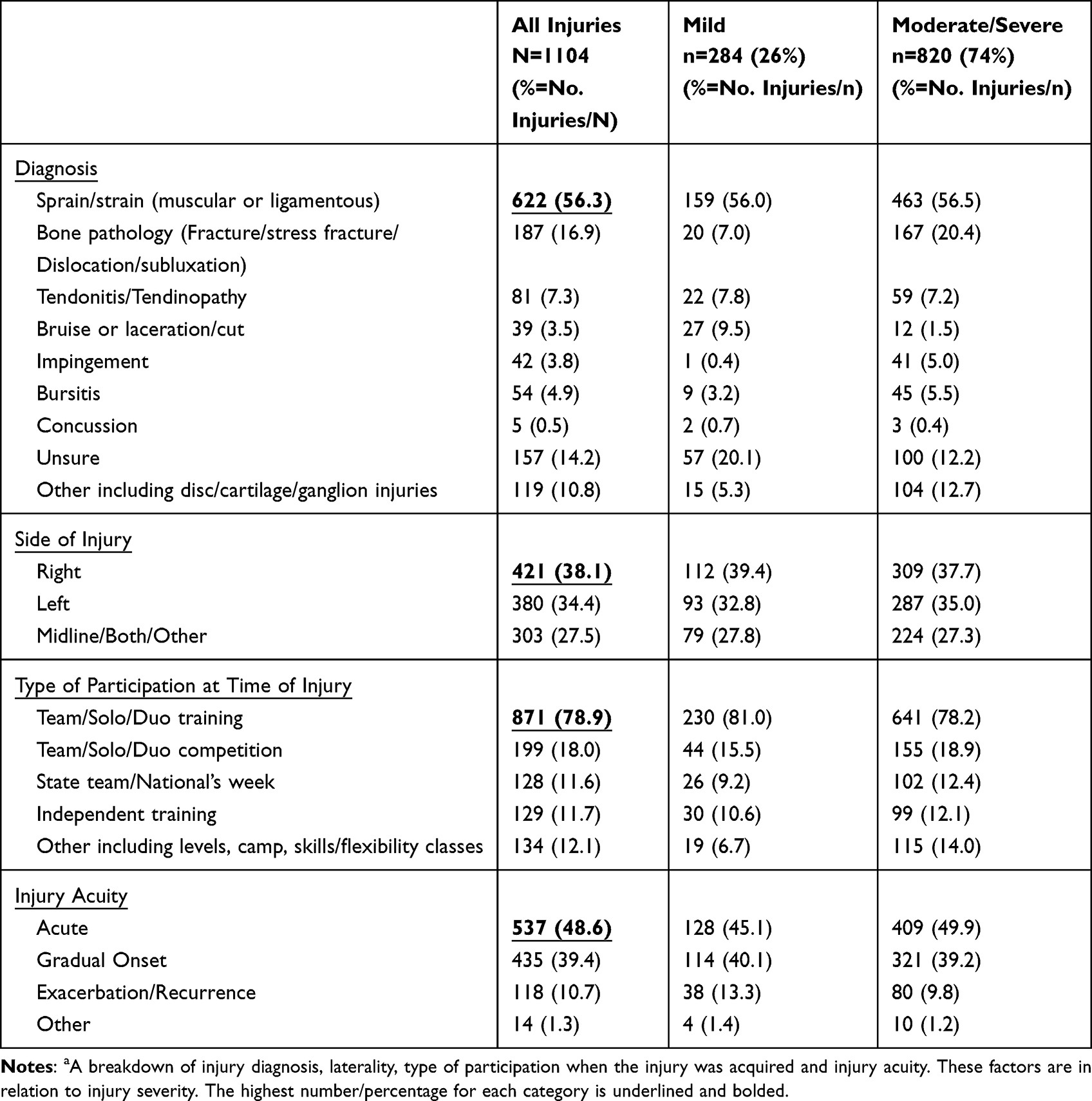 |
Table 1 Injury Featuresa |
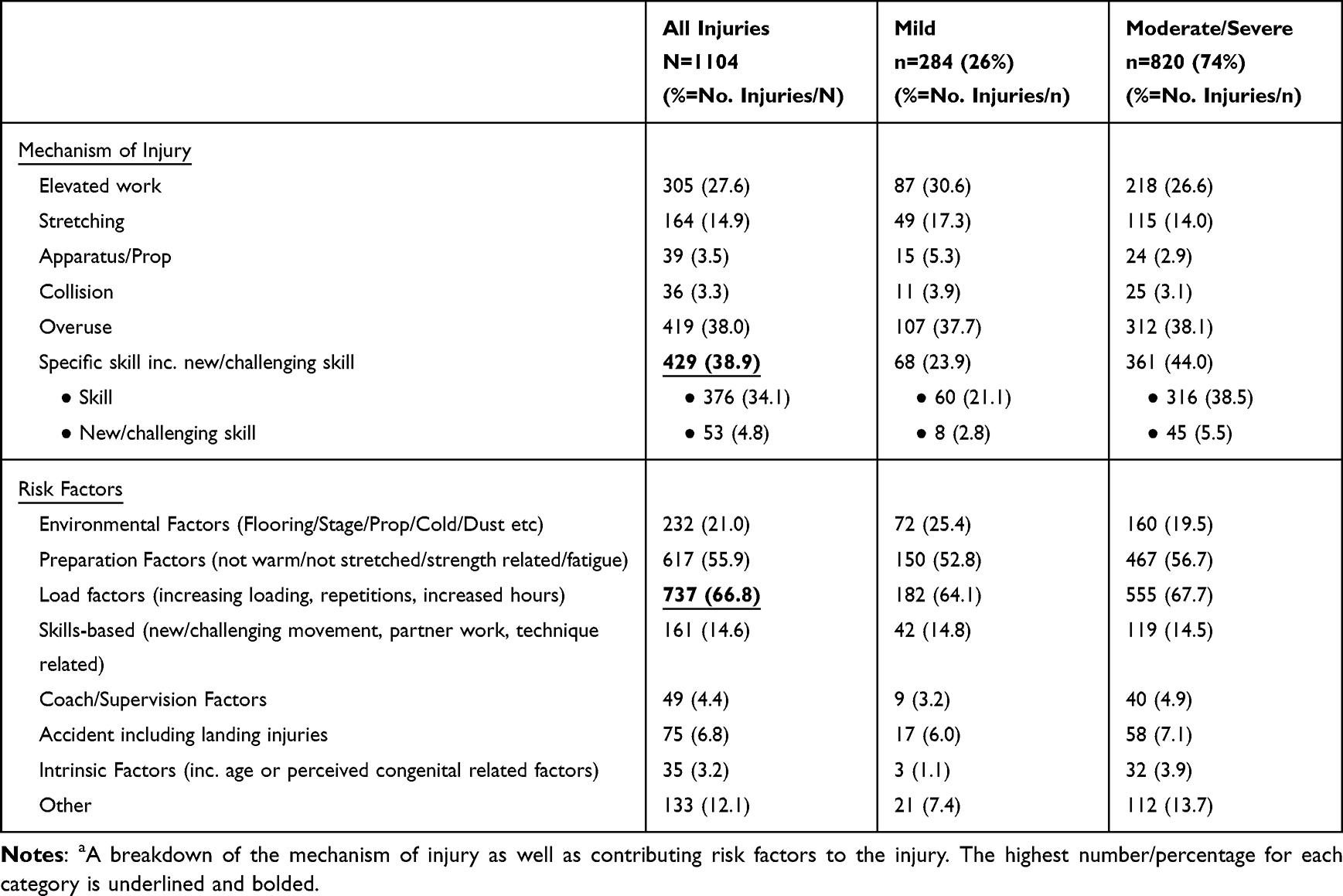 |
Table 2 Risk Factors of Injurya |
Data were analyzed in Stata 15 (StataCorp, College Station, TX, USA). Descriptive statistics were used to report on each variable of interest. Chi-square statistics were used to determine if hand or leg dominance was associated with side of injury, and significance set at p<0.05.
Multivariate regression analyses were used to determine objective risk factors independently associated with the number of injuries. Intrinsic factors were age, years of training, arm or leg dominance. Data transformations were investigated to improve model fit. Log transformations were applied where residuals from regression analysis were visually inspected and not normally distributed, as this was identified as the most appropriate transformation to improve model fit. Extrinsic factors were the number of hours of different training forms (formal training, home training or other sport) and participation types (eg, levels, solos, nationals). The regression model was built through a purposeful selection process. This included investigating the univariate analysis of each variable. Where p<0.2, this variable was included in the model to ensure we could identify if that variable was an important covariate or confounder to another variable.13 A backwards step multivariate regression analysis was then conducted for intrinsic and extrinsic variables. The preliminary multivariable model was reduced by removing variables one at a time, based on the highest p-value variable. This backward step removal continued until all remaining model variables had a p-value <0.05.13 Standardized beta coefficients were also calculated to give a measure of the contribution of each variable to the model.
Results
There were 680 survey responses. Following data cleaning there were 543 participant responses included within the analysis.
The majority of participants were Victorian (59.7%), current athletes (75.0%), in the Seniors age-group (18yrs and over; 58.4%). All but one participant identified as female and was removed for privacy purposes. There was an even divide of both elite (championship/championship reserve, 47.3%) and non-elite (division 1–10/recreational, 45.9%) athletes. In addition to mandatory team training, most participants took part in further solo training/competition (73.5%) or Levels training/examinations (69.1%). Right-sided dominance of both upper and lower limbs was also reported in large numbers (79.9%, 56.9%, respectively). Demographic data are tabulated in Supplementary Table 2.
Participants described 1104 injuries, with a mean (standard deviation (SD)) of 4.5 (3.3) injuries per participant. The mean (SD) recency since their injury was 7.3 (6.9) years. From the total injuries, 820 (74.3%) were deemed moderate/severe. Of the moderate/severe injuries, participants missed a mean (SD) 3.4 (5.1) weeks of training, had a mean (SD) 6.7 (6.2) weeks of modified choreography and engaged in a mean (SD) 10.9 (9.1) health professional consultations. Table 1 provides a breakdown of injury diagnosis, laterality, acuity, type of participation at time of injury acquisition. Figure 1 describes the body regions affected by injury while Figure 2 demonstrates the timing of injury relative to the calisthenics season.
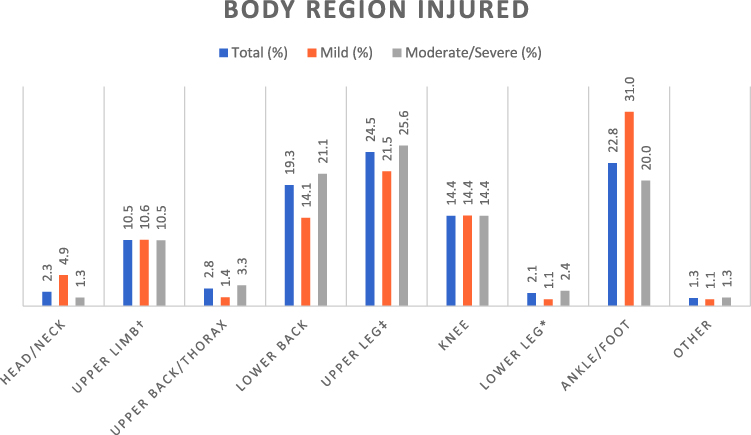 |
Figure 1 Body region injured: the percentage of injuries in each body region comparing severity and total. Notes: †Upper limb comprised of shoulder, elbow, wrist, hand. ‡Upper leg comprised of hip, thigh, quadricep, groin, adductor, buttock/gluteal region, hamstring. *Lower leg comprised of calf, tibia/shin, achilles. |
 |
Figure 2 Timing of injury: the number of injuries acquired relative to the training season during the year with a trendline present. Notes: †Early team training represents the first 6 weeks of training. ‡Pre-competition season is 7th week of training until commencement of competitions. |
Subjective factors identified by participants as the mechanism of injury as well as risk factors contributing to their injury are detailed in Table 2. Perceived calisthenics skills listed by participants ≥10 times are listed in Table 3 and divided by the body region the participant injured. Remaining responses can be found in Supplementary Data Table 3.
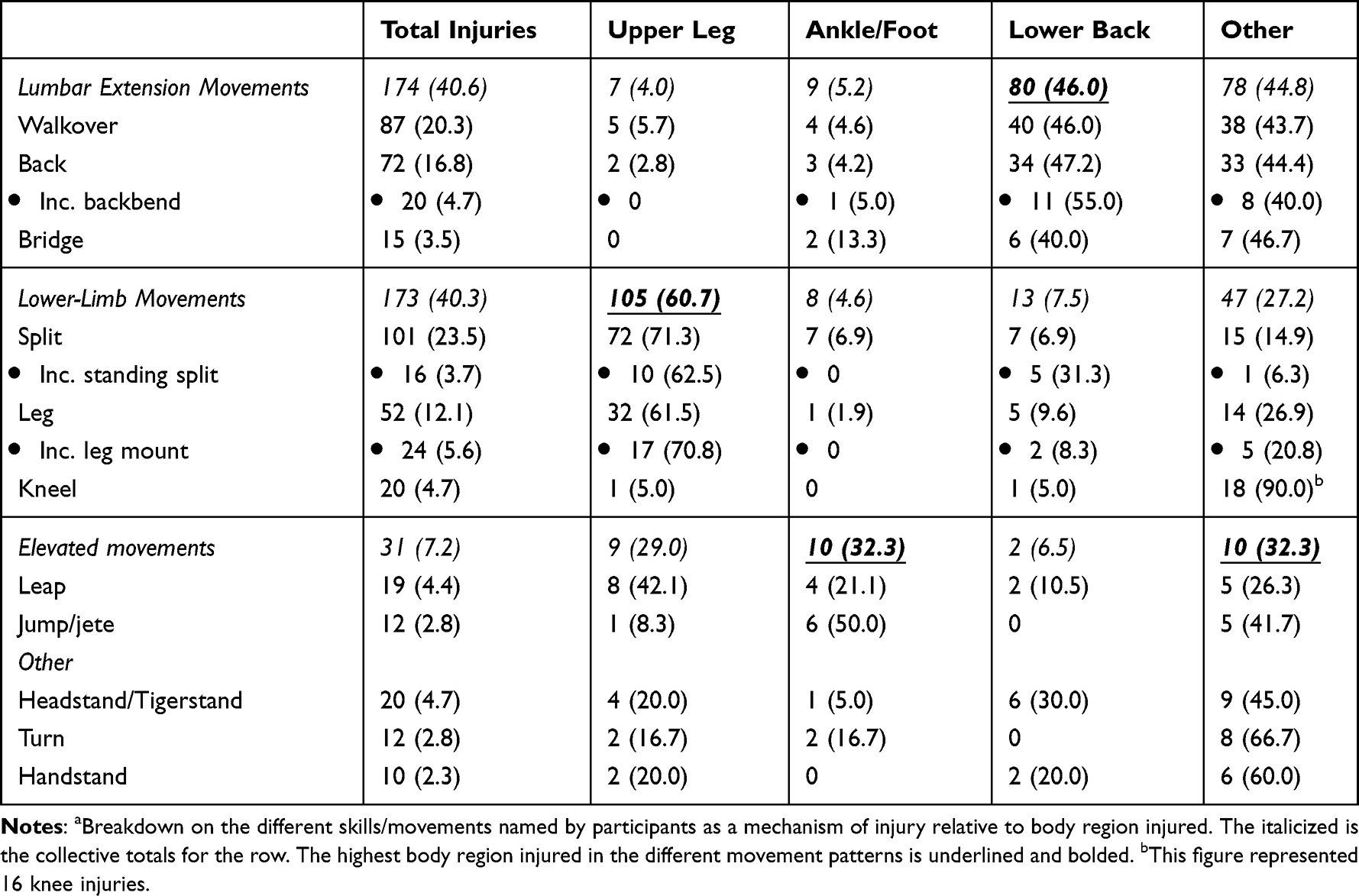 |
Table 3 Skills and Region of Injurya |
Objective risk factors examined for significant associations with number of injuries were divided into extrinsic and intrinsic variables. Intrinsic factors associated with a higher number of injuries included longer participation years (Coef=0.13, 95% CI=0.07 to 0.20, p<0.001) or if the athlete had a definite leg side dominance (Right Coef=0.015, 95% CI 0.01, 0.28, p=0.034, Left Coef=0.04, 95% CI=0.01, 0.28, p=0.034). Extrinsic factors associated with a higher number of injuries included higher hours of calisthenics training during the week (Coef=0.12, 95% CI=0.02 to 0.21, p=0.014), higher home training hours (Coef=0.17, 95% CI=0.07 to 0.28, p=0.001), higher training hours in other sports (Coef=0.08, 95% CI=0.03 to 0.14, p=0.005) and participation at national level/state team (Coef=0.19, 95% CI=0.06 to 0.32, p=0.004). Laterality had no association with side of injury for either arm or leg (p>0.05).
Discussion
This insight into injuries relating to participation in calisthenics is essential for health care professionals who work with calisthenics athletes. Our research is the second only examination of injuries relating to this unique sport and the first to include all competition levels. The even divide of elite and non-elite athletes means the SEM clinician can apply this research to all calisthenics athletes.
Calisthenics is a competitive and evolving sport, that, like many similar aesthetic-based sports, introduces new movements. As such, there is potential for such “new” or “challenging” movements to be contributing to injury development. However, this was not supported by the results with few participants selecting this option. Whereas movements considered core to calisthenics (walkovers, backbends, standing splits, bridges and tigerstands/headstands, as demonstrated in Figure 3) were considerably perceived to cause injuries in this and the only other calisthenics study.5 This demonstrates despite 20 years between the historic and present, calisthenic studies, together with an increased focus of strength and conditioning,14,15 these movements remain common skills perceived as causing injury within the sport.
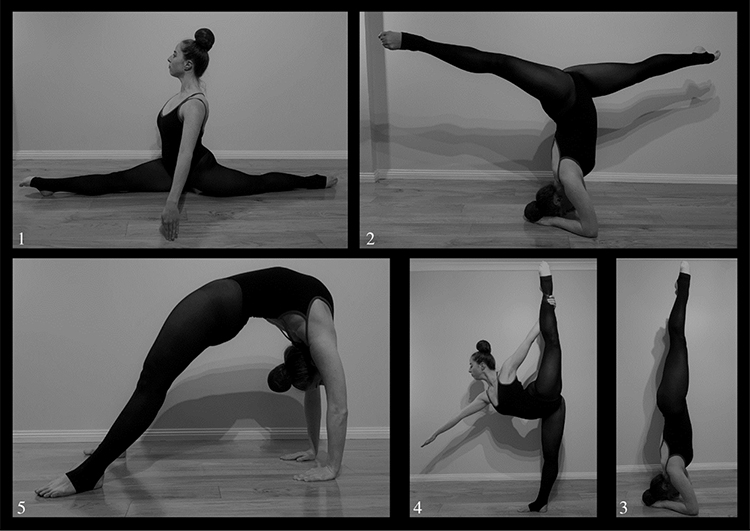 |
Figure 3 Common calisthenics skills: from top left going clockwise; 1. Split, 2. Tigerstand Split or Headstand Split, 3. Tigerstand or Headstand, 4. Standing Split or Held Arabesque, 5. Bridge. |
Our study identified a similar prevalence of ankle/foot injuries compared to a previous systematic review of injuries in ballet dancers.8 Calisthenics has balletic foundations and maintains similarities in terminology and steps,1,2 however, in relation to ankle/footwork it diverges with training without footwear and training on different floor types to those most commonly used in ballet (which is further explored in the next paragraphs). Therefore demonstrating, despite these footwear and environmental differences, calisthenics athletes’ prevalence of ankle/foot injuries remains similar to ballet dancers.
Other lower-limb injuries with high prevalence included upper leg and knee. These regions are involved in leg split-based movements, which was the most common lower limb skill reported as causing participants’ injuries. A finding which was confirmed in a recent prospective cohort study looking at injuries in the aesthetic-based sport of pole dancing.16 This movement pictured in Figure 1 is common within calisthenics in multiple forms and involves great flexibility of the hamstring and hip flexor muscle groups. It is possible, that overuse and preparation (identified as contributing factors for injury), in the form of excessive repetitions and poor warm-up respectively, of this highly predominant movement could be contributing to injury rate and severity, of the upper leg and knee regions.
Increase in elevated footwork, landing or take-off, is another possible mechanism of injury contributing to the high rates of lower limb injuries within calisthenics athletes. While elevated skills (eg, leaps/jumps) was a perceived mechanism of injury identified by participants in this study, the first calisthenics injury study did not state elevation throughout its questionnaire or in its open-ended text responses.5 This suggests in 1996, either there was less elevation content or elevation was less likely to cause injury. The former is more likely given injury-provoking movements identified by participants have, otherwise, remained the same. Therefore, evolving calisthenics choreography with increased elevation may be contributing to lower limb injuries seen in this study.
Unlike the comparable prevalence of ankle/foot injuries, lower back injuries were found to have a higher prevalence reported by participants compared with those in ballet and gymnastics.8–10 The lumbar extension-based movements which were represented in the data as the highest direct cause of participants’ injuries are also commonly performed in gymnastics – a sport known for its extreme lumbar hyperflexion, hyperextension and high axial load forces.17 Therefore, the training strategies which gymnastics adopt in relation to these movements may be of interest to the SEM clinician and coaches as a means of injury prevention.
The pathology of injuries occurring in calisthenics athletes is useful information for health practitioners. Being a self-reported measure, these data may be limited in that regard, however, are beneficial in highlighting the understanding of an injury by the calisthenics athlete, which in turn demonstrates, the education an SEM clinician may need to provide. This study identified a significant proportion of athletes who were uncertain about their diagnosis. Factors that may be contributing to this and warrant further investigation include injury education of athletes, health literacy and destinations athletes refer to for injury diagnosis. Additionally, without athletes having a clear injury diagnosis they cannot subsequently undertake best practice management, possibly affecting not only the athlete’s ability to participate in calisthenics, but also their overall participation in daily living. This demonstrates the necessity for a future study using health practitioner reporting for this measure as well as exploring factors contributing to diagnostic uncertainty in this athletic population.
Overuse and increased loading as a factor for injury was a theme identified throughout the study (eg, mechanism of injury, risk factor, increased training hours regardless of training type). This would confirm similar previous findings related to load and injury in other sports (including analogous sports such as gymnastics and dance)7,18–20 while also confirming overuse as a risk factor regardless of injury acuity21 given the relatively even divide between acute and gradual onset injuries identified. Additionally, there was a documented increase in injuries as the calisthenics year progressed, alongside an increase in injury number for those participating in state team/national level. These injury rates can likely be explained by the increased loading required for training and performance. For instance, as the calisthenics year progresses, more repetitions of the same routine/movements are needed to improve execution and uniformity within a team (both key scoring criteria),22 while clubs may also schedule additional classes in the lead-up to competitions. Furthermore, state team participation requires competitors to train simultaneously for both their local club and state (effectively doubling their loading). Other factors potentially contributing to an increased risk of injury at a state team level are the higher pressure environment and the increased difficulty in movement – the latter is less likely given few participants attributed their injury to a new or challenging skill. These elements highlight overuse as a significant factor contributing to injury development within calisthenics. Therefore, SEM clinicians should consider a careful loading history and addressing of this factor as vital to their treatment of the calisthenics athlete. Additionally, given the majority of injuries occurred at training, this also provides a convenient location where overuse can be effectively targeted, with the SEM clinician providing clear load management to both their patient as well as coaches.
Preparation factors such as strength and conditioning were, prior to this study, anecdotally thought to be contributing to injuries among the calisthenics community.14,15 This was addressed when the Australian peak body introduced a new module in coaching accreditation in 2014 solely focused on strength and conditioning education.14,15 Our study confirms athletes view preparation-related factors (eg, inadequate warm-up/stretching/strength) as major risk factors to their injuries. It is unknown if the peak body’s intervention has been effective in addressing these factors, as the mean recency of injury was prior to this module being introduced. In either instance, the high prevalence of responses stating lack of preparation as a risk factor warrants the SEM clinician focusing on warm-up, activation and strengthening in both their clinical history as well as their management advice.
Following individual preparation-related factors, environmental elements (eg, flooring, dust, cold) were key variables identified by participants as injury contributors. Unfortunately, while this demonstrates an important area of questioning for the SEM practitioner, these factors are likely to be the most difficult to modify. Flooring should be a key consideration to minimize injury given the increase in elevation work since the previous calisthenics study.5 While comparable sports (eg, gymnastics and ballet) train on foam mats or sprung flooring, calisthenics is a community-based sport occurring largely in local school/community halls where sprung flooring is less common. The lack of sprung flooring in training settings (where the majority of injuries are occurring) leads to higher stress impact through the lower limb on landing23,24 and may be contributing to the high lower limb injury rates. Numerous barriers may exist to changing calisthenics training facilities, including sprung flooring expense or lack of input/control over the space due to third-party ownership. This research should highlight to governing bodies as well as SEM clinicians the impact of training environments and the importance of advocating for change where able.
With regards to objective risk factors identified in the multivariate regression analyses not previously discussed, the finding that higher participation years are associated with higher injuries is logical given causal links between time, load and injury are well established.7,18–20 Therefore, reducing the number of injuries occurring in the sport may prolong participation which has benefits for long-term health and wellbeing.25
In contrast, finding left leg dominance and its association with injury should be further explored, particularly as these participants (in the minority) were at an increased risk of injury regardless of which side of the body they injured. Movement uniformity is a key component of adjudication.22 This study identified a majority of participants are right-dominant and, therefore, the need for uniformity likely leads to a bias of choreography toward the right side. This bias may contribute to injury either by the aforementioned factors of preparation (ie, increased preparation on the right at the expense of the left, leading to left-sided injury) or overuse (ie, increased repetition on the right, leading to right-sided injury). In either instance, symmetrical preparation and use of the whole body (also a scoring criterion for adjudicators)22 should be a focus for the SEM practitioner in prescribing rehabilitation for the injured athlete, to both reduce injury rates as well as improve performance.
Limitations of this study include its retrospective nature and reliance on self-reported data. This introduces potential recall bias. Furthermore, recall may be influenced due to the unknown health literacy of participants. We aimed to reduce recall bias through providing a clear injury definition, setting a maximum injury rate and asking for detailed information on only three most significant injuries. An additional limitation of the retrospective study is that the data cannot be transferred to a rate-based measure of injury incidence. As this is only the second study to date investigating calisthenics injuries it can provide a baseline for future development of a prospective study. Peak bodies may also consider injury database preparation to gather real-time data to inform the effect of training modules, judging criteria changes or introduction of skills on injury rates. Future research should also consider using triangulating data between the athlete, health professionals and coach for injury reporting data to minimize recall bias, improve diagnostic accuracy and improve data collection on activities which may have contributed to the injury.
Conclusion
Calisthenics demonstrates a high proportion of strain/sprain injuries involving the lower limb and lumbar spine with causative movements described being extension-based movements and elevation work. Addressing overuse, preparation and environmental factors related to these movements is important for the consulting SEM practitioner and may reduce overall injury prevalence, classes missed, and health professional sessions. Organizational bodies should provide coaches and participants with training and resources to enable the implementation of evidence-based injury prevention strategies into practice across the season.
Abbreviations
ACF, Australian Calisthenics Federation; CHERRIES, Checklist for Reporting Results of Internet E-Surveys; URL, Uniform Resource Locator; QR, Quick Response; SEM, Sports and Exercise Medicine.
Ethics Approval and Informed Consent
Ethics approval was given via Monash University Human Research Ethics Committee, Victoria, Australia (Approval Number: 23859). All participants provided online informed consent via a check box, or where the participant was under 18, parents provided online informed consent and supported survey completion. This study was performed in accordance to the World Medical Association Declaration of Helsinki.
Consent for Publication
Authors confirm this manuscript and Supplementary Material has been reviewed and provide consent to publication of its contents. The authors confirm the person featured in Figure 3 provided informed consent for publication and reproduction of their image.
Acknowledgments
The authors wish to acknowledge support with data collection from The Australian Calisthenics Federation, Calisthenics Victoria Incorporated, Calisthenics Association of South Australia, Calisthenics Association of Western Australia, Northern Territory Calisthenics Association, Calisthenics Association of Queensland Incorporated, Calisthenics New South Wales and Calisthenics Australian Capital Territory.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Otzen R. Recovering the past for the present: the history of Victorian calisthenics. Lilith. 1988;5:96–112.
2. Otzen R. Grace & Strength: Calisthenics in Australia. Sydney: Walla Walla Press; 2012.
3. Australian Calisthenics Federation. Annual Report. South Australia: Australian Sports Commission, Australian Government; 2019.
4. Roar Calisthenics Academy, Dance with Pride. Est 2014 [Internet]. Auckland: New Zealand Calisthenics; 2022. Available from: roarcalisthenics.com.
5. Leaf JR, Keating JL, Kolt GS. Injury in the Australian sport of calisthenics: a prospective study. Australian J Physiother. 2003;49(2):123–130. doi:10.1016/S0004-9514(14)60128-8
6. Campbell RA, Bradshaw EJ, Ball NB, et al. Injury epidemiology and risk factors in competitive artistic gymnasts: a systematic review. Br J Sports Med. 2019;53(17):1056–1069. doi:10.1136/bjsports-2018-099547
7. Caine DJ, Nassar L. Gymnastics injuries. Med Sport Sci. 2005;48:18–58. doi:10.1159/000084282
8. Smith PJ, Gerrie BJ, Varner KE, et al. Incidence and Prevalence of Musculoskeletal Injury in Ballet: a Systematic Review. Orthopaedic J Sports Med. 2015;3(7):2325967115592621. doi:10.1177/2325967115592621
9. Kolt GS, Kirkby RJ. Epidemiology of injury in Australian female gymnasts. Sports Med Training Rehabilitation. 1995;6(3):223–231. doi:10.1080/15438629509512053
10. Thomas RE, Thomas BC. A systematic review of injuries in gymnastics. Phys Sportsmed. 2019;47(1):96–121. doi:10.1080/00913847.2018.1527646
11. Garrick JG, Requa RK. Role of external support in the prevention of ankle sprains. Med Sci Sports. 1973;5(3):200–203.
12. Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. 2004;6(3):e34. doi:10.2196/jmir.6.3.e34
13. Hosmer D, Lemeshow S, Sturdivant RX. Applied Logistic Regression.
14. Australian Calisthenics Federation.Annual Report. South Australia: Australian Sports Commission, Australian Government; 2014.
15. Australian Calisthenics Federation Coaching Committee. Level One Program; 2014.
16. Nicholas J, Weir G, Alderson JA, et al. Incidence, Mechanisms, and Characteristics of Injuries in Pole Dancers: a Prospective Cohort Study. Med Probl Perform Art. 2022;37(3):151–164. doi:10.21091/mppa.2022.302217
17. Kruse D, Lemmen B. Spine Injuries in the Sport of Gymnastics. Curr Sports Med Rep. 2009;8(1):20–28. doi:10.1249/JSR.0b013e3181967ca6
18. Drew MK, Finch CF. The Relationship Between Training Load and Injury, Illness and Soreness: a Systematic and Literature Review. Sports Med. 2016;46(6):861–883. doi:10.1007/s40279-015-0459-8.
19. Lindner KJ, Caine DJ. Injury patterns of female competitive club gymnasts. Can J Sport Sci. 1990;15(4):254–261.
20. Chéron C, Le Scanff C, Leboeuf-Yde C. Association between sports type and overuse injuries of extremities in children and adolescents: a systematic review. Chiropr Man Therap. 2016;24:41. doi:10.1186/s12998-016-0122-y
21. Warden M. Sports injuries: acute. In: Brukner P, Khan K, editors. Clinical Sports Medicine.
22. Australian Society of Calisthenics Adjudicators. Critiques and Adjudication. Victoria: Calisthenics Victoria Inc; 2019.
23. Hackney J, Brummel S, Becker D, et al. Effect of sprung (suspended) floor on lower extremity stiffness during a force-returning ballet jump. Med Probl Perform Art. 2011;26(4):195–199. doi:10.21091/mppa.2011.4031
24. Hackney J, Brummel S, Jungblut K, et al. The effect of sprung (suspended) floors on leg stiffness during grand jeté landings in ballet. J Dance Med Sci. 2011;15(3):128–133.
25. Eime RM, Young JA, Harvey JT, Charity MJ, Payne WR. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: informing development of a conceptual model of health through sport. Int J Behav Nutr Phys Activity. 2013;10(1):98. doi:10.1186/1479-5868-10-98
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.