")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 17
Burden of Tuberculosis in End Stage Renal Disease Patients Undergoing Maintenance Hemodialysis: A Multicenter Study and Experience from Ethiopian Dialysis Setting
Authors Beyene E, Demissie Z , Jote WT, Getachew S, Ejigu AM , Degu WA
Received 5 December 2023
Accepted for publication 14 February 2024
Published 15 February 2024 Volume 2024:17 Pages 59—69
DOI https://doi.org/10.2147/IJNRD.S450565
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Eyob Beyene,1 Zekewos Demissie,2 Wubshet Tolossa Jote,3 Seyfemichael Getachew,3 Addisu Melkie Ejigu,4 Wondwossen Amogne Degu1
1Department of Internal Medicine, Division of Infectious Disease, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Internal Medicine, Lancet General Hospital, Addis Ababa, Ethiopia; 3Department of Internal Medicine, Division of Nephrology, St. Paul Millennium Medical College, Addis Ababa, Ethiopia; 4Department of Internal Medicine, Division of Nephrology, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Eyob Beyene, Email [email protected]
Background: Patients with end stage renal disease (ESRD) are at a higher risk of developing tuberculosis (TB) due to the immunosuppressed state along with concomitant comorbidities and socioeconomic and demographic factors. Data on the prevalence of tuberculosis in ESRD are scarce despite the high burden of the disease in developing nations.
Methods: A multicenter, cross-sectional study was conducted at eight dialysis centers in Addis Ababa on the prevalence of TB among CKD patients on maintenance hemodialysis from August 2022 to October 2022 G.C. The study enrolled 263 participants selected by systematic random sampling. Data were collected by reviewing the patient’s electronic medical records. The Collected data were analyzed using SPSS version 26.0.
Results: Our study found a 27% prevalence of TB in patients with ESRD receiving maintenance hemodialysis (MHD). Pulmonary tuberculosis was the most prevalent form, and lymphadenitis was the most common extra-pulmonary tuberculosis (EPTB). Only 5.6% of the study participants had microbiologic evidence of TB. Chemistry and cytological studies from pleural fluid and imaging evidences were commonly used diagnostic modalities. The presence of HIV infection, longer duration of dialysis (> 1 year), and contact history with a known TB patient were all significantly associated with higher prevalence of TB among the study participants.
Conclusion: Although there is a strong association between TB and CKD, there are no local data from Ethiopia. Our study identified a higher prevalence of TB among CKD patients on MHD. Thus, maintaining a high index of suspicion and early diagnosis and treatment of TB among ESRD patients on MHD and use of TB preventive therapy (TPT) is important in decreasing morbidity and mortality.
Keywords: dialysis, end stage renal disease, tuberculosis, extrapulmonary TB
Introduction
Up until the corona virus (COVID 19) pandemic, tuberculosis (TB), a communicable disease, was the leading cause of death from a single infectious agent. Mycobacterium tuberculosis is the bacillus that causes TB. Droplets that are expelled by TB patients disseminate these bacteria. TB is a curable and preventable disease. About 85% of people who develop TB disease can be successfully treated with six months drug regimen.1,2
Anyone anywhere is susceptible to falling infected with TB. It is estimated that M. tuberculosis infects about 25% of the world’s population. In the course of their lifetime, a comparatively small percentage (5–10%) may develop TB illness. However, those with HIV and those who are vulnerable to risk factors such as malnutrition, diabetes, smoking, alcoholism, and poverty are considerably more likely to develop TB illness. In addition, other factors that are immunosuppressive and linked to TB reactivation include age, malignancies, chronic and end-stage renal disease, corticosteroid use, and TNF-alpha inhibitor use.1,3,4
The overall incidence of TB worldwide reached an all-time high about 2003 and is now steadily declining. WHO estimates that 9.9 million people contracted TB in 2020, and 1.5 million died from it. The sub-Saharan Africa, India, islands of Southeast Asia, and Micronesia have the highest rates of TB incidence. Nearly 95% of TB cases happen in nations with minimal resources. Additionally, it has been demonstrated that immunosuppressive conditions are linked to the emergence of active TB and its reactivation. Chronic kidney disease is one of these immunosuppressive diseases.1,2,4
Chronic Kidney disease (CKD) is a worldwide public health problem. The number of patients enrolled in the end-stage renal disease (ESRD) care is increasing every year. Globally, the estimated overall prevalence of CKD is 8% to 16%. In sub-Saharan Africa, people between the ages of 20 and 50 are more likely to have CKD, and people of African origin experience the onset of ESRD 20 years earlier than people from other ethnic groups. Globally the leading causes of CKD and ESRD are diabetes (30–50%) followed by hypertension.5,6
Early CKD and ESRD are both linked to significant morbidity and mortality. For ESRD patients, infections are one of the main causes of hospital admissions and the third most frequent cause of death, following cardiovascular diseases and treatment discontinuation. One of the serious bacterial diseases in CKD is tuberculosis.5–8
Although the relationship between TB and CKD has been known for more than 40 years, little is known about how these two conditions interact with one another. Once infected with Mycobacterium tuberculosis, those with CKD, especially those with ESRD receiving hemodialysis, are at a higher risk of developing active disease. According to reports, uremic immunodeficiency causes a 6.9 to 52.5-fold increase in the frequency of tuberculosis in dialysis patients compared to the general population. In addition, these specific immunocompromised patients may be at greater risk of developing infectious problems due to a higher likelihood of primary infection brought on by frequent visits to dialysis facilities, advanced age, and immunosuppressive medications.7–9
Both TB and CKD continue to be significant global public health issues in spite of the WHO’s and other regional and national health organizations’ commitments. TB is linked to higher rates of morbidity and death in CKD patients. The issue at hand is made worse by atypical TB presentations and poor performance of screening and diagnostic methods in patients with chronic kidney disease. One of the most promising TB-preventative interventions for dialysis patients is tuberculosis prevention therapy (TPT). We believe the information this study will give us on the prevalence of tuberculosis among ESRD patients in Ethiopia undergoing dialysis will serve as a foundation for future recommendations for prevention, diagnosis, and treatment.
Study Methodology: Design and Setting
We conducted a multi-center; cross-sectional study on the prevalence of TB among CKD patients on maintenance hemodialysis and associated factors from August 2022 to October 2022 G.C. The current study tried to assess the current prevalence of Tuberculosis in ESRD patients receiving hemodialysis, to identify risk factors associated with TB infection in ESRD patients receiving hemodialysis and to characterize the type of Tuberculosis infection in ESRD patients receiving hemodialysis in Addis Ababa, Ethiopia. The study took place at eight governmental and non-governmental dialysis centers in Addis Ababa. These include St. Paul Millennium Medical College, Menelik General Hospital, Zewditu Memorial Hospital, Lancet General Hospital, Flow dialysis center, Tom dialysis center, MCM general hospital, and Bethzatha General Hospital. These centers provide maintenance hemodialysis for more than 800 CKD patients.
Study Participants
Inclusion Criteria
- Age >/=18 years.
- CKD on maintenance hemodialysis and who can provide consent.
Exclusion Criteria
- Diagnosis of tuberculosis before the diagnosis of CKD
- Patients with incomplete medical records and those who are unable to provide the appropriate information
- Patients with mental health problems
- Critically ill patients
- Those who cannot provide consent
The sample size of 273 was calculated by using single population proportion formula based on the results of a study conducted at inner-city biomedical research laboratory in Berlin with a biosafety level 3 facilities showed a 20% general prevalence of tuberculosis among CKD patients.10 A systematic random sampling method was used to recruit participants during their dialysis unit visit. Written consent was obtained from all the study participants. From the total 273 patients identified during the study period, 10 were excluded for diagnosis of TB before CKD (5), age below 18 (3), and incomplete medical record (2). A total of 263 CKD patients on maintenance hemodialysis were included in the final analysis.
Data Collection Procedure
Patients were recruited in to the study during their routine dialysis center visit using systematic random sampling. After explaining the purpose of the study, written informed consent was obtained from all study participants and a structured questionnaire was used to evaluate study participants. Data were collected through both patient interviews and a review of patient’s medical records.
Operational Definitions
History of contact with TB patient: Patients who had shared airspace with a person with infectious TB disease ie with family members, friends, coworkers, classmates, and others.2
Diagnosis of pulmonary TB: A diagnosis of pulmonary TB was established by treating physician or nephrologist based on sputum microscopic examination for AFB, sputum for Gene-Xpert test or on the basis of clinical presentation and chest imaging.2
Diagnosis of extra-pulmonary TB: Diagnosis of extra-pulmonary TB was established by treating physician or nephrologist based on microbiologic confirmation using AFB or Gene-Xpert test, Biopsy, cytology, or culture from appropriate specimen or imaging evidence.2
Diagnosis of disseminated TB: Disseminated TB was diagnosed if TB involved two or more noncontiguous sites.2
Diagnosis of miliary TB: Miliary TB was diagnosed by presence of diffuse miliary infiltrate on chest radiograph or high-resolution CT scan, or evidence of miliary tubercles in multiple organs at laparoscopy or open surgery.2
Data Analysis
The acquired data was verified, cleaned up, and then given a final analysis. The statistical data were entered using Microsoft Excel, and IBM SPSS Statistics software package version 26.0 was used for analysis. Frequency data was used to generate descriptive statistics. The terms used to express continuous variables were means, standard deviations, and range. The multicollinearity was evaluated using the variance inflation factor (VIF), and none was collinear. To evaluate the relationship between each independent variable and the treatment outcome, univariable logistic regression and multivariable binary logistic regression models were used. P-values under 0.05 were taken into consideration when assessing statistical significance.
Ethics Approval and Informed Consent
The ethical clearance of the present study was obtained from the institutional review board of Addis Ababa University, College of Health Sciences. We fully explained the purpose and protocol of the study to all participants included in the study and written informed consent was obtained from each participant. The data collected was recorded and anonymously examined. All acquired information was kept in strict confidence and exclusively applied to the desired goal. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Results
Sociodemographic Profile
The mean [± SD] age of the participants was 43.8 ± [15.96] with minimum and maximum ages of 18 and 88, respectively. Two-thirds participants were male. The majority (87%) of the participants resided in Addis Ababa. About two-third of the participants were married, and more than half were Orthodox Christian.
The Sociodemographic data are shown in Table 1.
 |
Table 1 Sociodemographic Characteristics of Study Participants at Hemodialysis Centers, Addis Ababa, Ethiopia, August 2022 – October 2022 (N = 263) |
Clinical Characteristics of the Study Participants
The mean [± SD] duration of follow-up for ESRD of the participants was 3.77 ± [3.03] with minimum and maximum duration of 01 month and 17 years, respectively. More than two-third (69%) of the participants were on follow-up for more than a year. About third of patients did not have identified documented cause of ESRD. Diabetes was responsible for one-third of ESRD cases and the other third was due to hypertension. About two-third of the participants were on dialysis for more than a year and more than half of the participants undergo dialysis three times a week.
About 78% of participants had comorbidities and one-quarter of the participants had two or more comorbidities. Hypertension was the commonest comorbidity identified in 166 (63.1%) patients followed by diabetes in 86 (32.7%). Fifty-three (20.2%) patients had both diabetes and hypertension. HIV and CLD were found in 18 and 3 participants, respectively.
The mean [± SD] follow-up for treatment of HIV among HIV positive patients was 8.83 ± [4.7] with minimum and maximum duration of 2 and 17 years, respectively. The mean [± SD] CD4 count among HIV-positive patients was 209 ± [135] with minimum and maximum CD4 count of 86 and 500, respectively. ABC + 3-TC + EFV were the most commonly used regimen. Among HIV patients 50% had history of Tuberculosis prophylaxis use.
Twenty-three participants had history of smoking and four were on immunosuppressive therapy. One-third of the participants were underweighted.
The Clinical and Treatment-Related Characteristics are shown in Table 2.
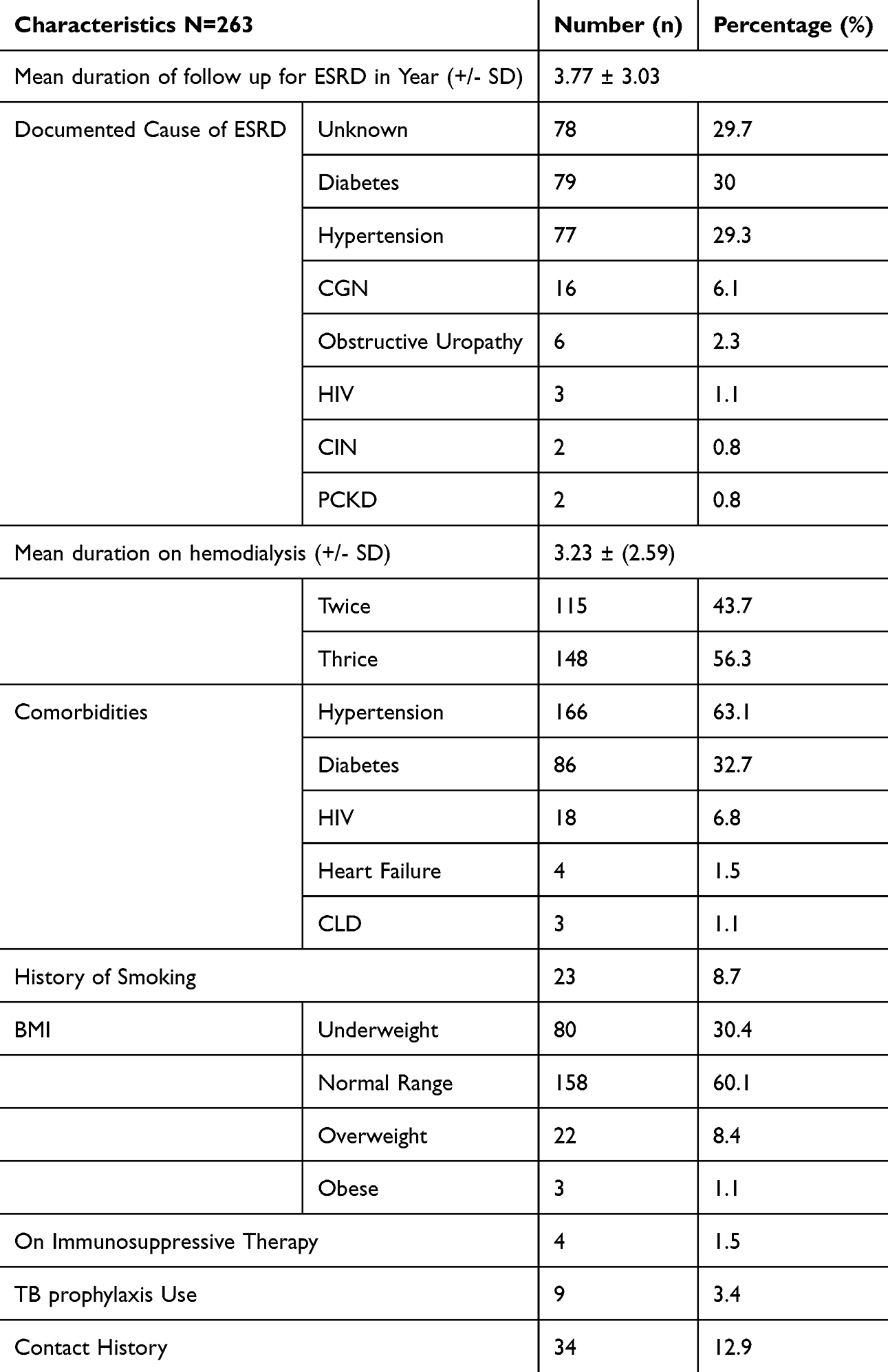 |
Table 2 The Clinical and Treatment-Related Characteristics of Study Participants at Hemodialysis Centers, Addis Ababa, Ethiopia, August 2022 – October 2022 (N = 263) |
Tuberculosis Diagnosis and Treatment-Related Characteristics of Study Participants
Among 263 participants 71 (27%) had diagnosis of tuberculosis. Sixty-four (24.3%) had previous history of tuberculosis. Pulmonary tuberculosis was diagnosed in two-third of cases and about third had EPTB, TB lymphadenitis was the most common type followed by pleural TB. Imaging evidence was used to make a diagnosis of TB in one-third patients followed by FNAC (26.6%) and Pleural fluid analysis (26.6%). Clinical diagnosis of TB was made only in two patients. More than half (54.7%) of TB diagnosis was made after initiation of haemodialysis. All participants with diagnosis of TB were received first-line anti-TB and only one had treatment failure.
Active TB was found in 12 patients and among them 5 had previous history of TB. Pulmonary TB accounted for 66% of participants. Again, imaging evidence was the commonest modality to make a diagnosis of TB followed by sputum and cytology evidences. All patients with active TB were receiving first-line anti-TB.
TB diagnosis and treatment-related characteristics are shown in Table 3 and Table 4.
 |
Table 3 Previous TB Diagnosis, Type, and Treatment-Related Characteristics of Study Participants at Hemodialysis Centers, Addis Ababa, Ethiopia, August 2022 – October 2022 (n=64) |
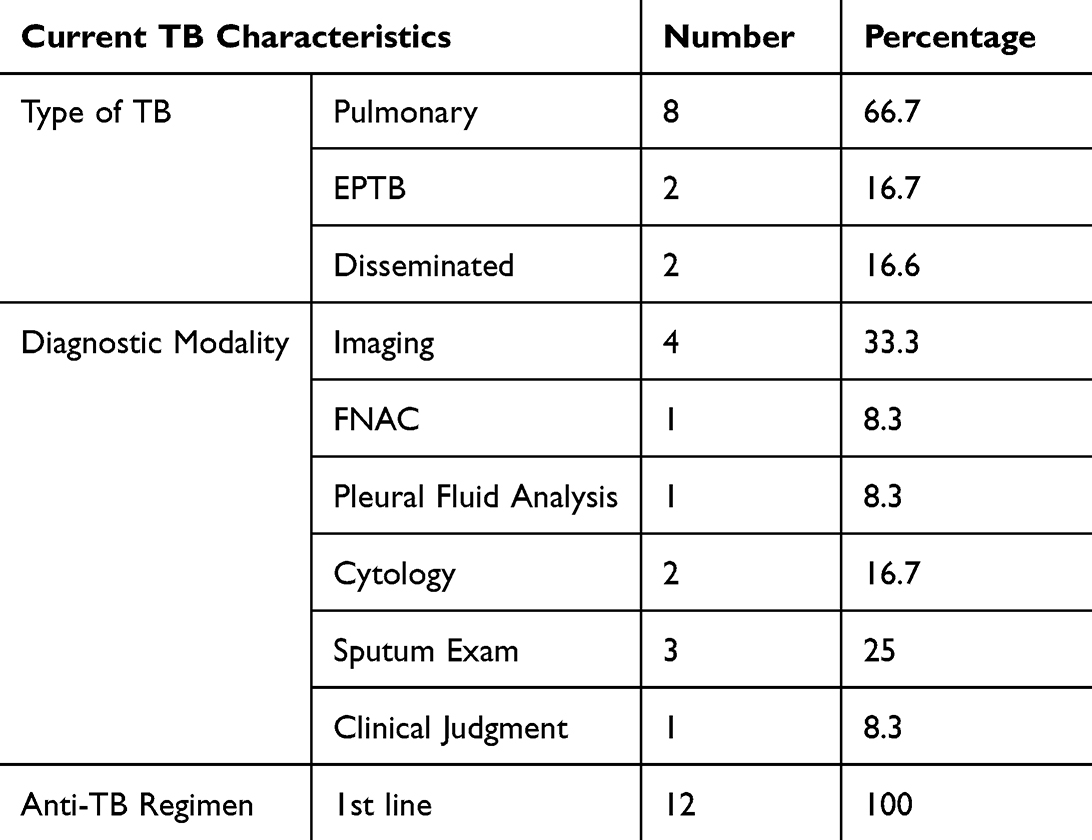 |
Table 4 Current TB Diagnosis, Type, and Treatment-Related Characteristics of Study Participants at Hemodialysis Centers, Addis Ababa, Ethiopia, August 2022 – October 2022 (n=12) |
Multivariate Logistic Regression Analysis of Factors Associated with TB in ESRD Patients
Table 5 shows the logistic regression analysis of factors associated with increased tuberculosis diagnosis, and odds ratio and a 95% confidence interval were used to measure the degree of association between the independent variables and increased tuberculosis diagnosis. Multicollinearity was assessed among independent variables using the variance inflation factor (VIF) and none was collinear. Initially, bivariate binary logistic regression was performed on selected sociodemographic, clinical, and treatment-related characteristics to identify variables candidate for multivariate binary logistic regression and a total of 5 variables were found to be candidates at a P-value of ≤0.2.
 |
Table 5 Factors Associated with TB Occurrence Among the Study Participants at Hemodialysis Centers, Addis Ababa, Ethiopia, August 2022 – October 2022 (n=263) |
These include contact history with a known TB patient (Crude odds ratio (COR) 3.241, 95% confidence interval (CI) 1.549–6.781), presence of HIV infection (COR 8.383, 95% CI: 2.868–24.504), presence of comorbidities (COR 1.670, 95% CI: 0.809–3.448), duration on dialysis for more than 1 year (COR 2.341, 95% CI: 1.235–4.439), and dialysis sessions 3 times per week (COR 1.920, 95% CI: 1.084–3.402). However, in the final multivariate regression model, only 3 variables were found to have a statistically significant association with increased tuberculosis diagnosis at a P-value of ≤0.05. These included having a contact history with a known TB patient, presence of HIV infection, and duration on dialysis for more than 1 year.
The diagnosis of tuberculosis among participants who had a contact history with a known TB patient was 2.5 times as compared to patients who had not a contact history Adjusted odds ratio (AOR 2.581, 95% CI: 1.152–5.781, p=0.021). The study also found a significant association between the presence of HIV infection and diagnosis of tuberculosis, which was 15 times as compared to HIV negative patients (AOR 15.047, 95% CI: 2.841–79.697, p=0.001). Participants who were on dialysis for more than 01 year had 2.5 times increased TB diagnosis as compared to participants on dialysis for 01 and less year (AOR 2.510, 95% CI: 1.219–5.171, P=0.013).
Multivariate logistic regression analysis of factors associated with increased tuberculosis diagnosis shown in Table 5.
Discussion
Even though TB affects anyone anywhere, dialysis and renal transplant patients are at higher risk of TB. The increased risk of TB among these patients is related to the presence of multiple comorbidities, nosocomial transmission, and immunosuppressed state from the ESRD and use of immunosuppressive treatments, and Sociodemographic factors. Increased prevalence of latent TB infection (LTBI) in CKD patients also contribute for the higher burden of TB in CKD patients.5–8
The study found the diagnosis of TB in 27% (71) of study participants. This a figure that is higher as compared to previous studies done at different Asian countries. A retrospective study from Saudi Arabia showed a 7% prevalence of TB over 10-year period of time. Another study from Nepal, a university hospital-based study showed prevalence of 13.7% among dialysis patients. Studies from other countries showed 10.5% (India), 15.1% (Belgium) and 20% (berlin).10–12 The variation in the prevalence of TB in patients who undergo hemodialysis among the various studies done could be due to the differences in sample characteristics, use of TB prophylaxis and dialysis setting. The higher rate of TB diagnosis in our study could be due to the higher prevalence of tuberculosis in the country and overcrowding of the dialysis centers (the center has small capacity and they are few in number) and lack of adequate use of prophylaxis for anti-TB.
In this study, PTB accounted for 66% (47), EPTB in 28% (20) and disseminated TB was found in 5.6% (4) of study participants, respectively. This is a different figure from other similar studies. Study from Nepal showed a higher prevalence of EPTB in 69.1% of TB cases and another study done in Saudi Arabia showed 77.8% prevalence of EPTB among the diagnosed TB cases.11,12 The higher prevalence of EPTB in other studies could be due to availability of diagnostic modalities. From EPTB, TB lymphadenitis was commonest which accounted for 90% of all EPTB the higher prevalence of PTB in our study could be due to acquisition of the infection in dialysis center and overcrowding might contribute.
In this study, the burden of TB higher among patients on dialysis and TB was diagnosed in 67.6% (48) after initiation of hemodialysis which is comparable with Nepal study which showed 63%. The diagnosis of TB in CKD patients is changing. In our study only 4 patients (5.6%) of patients found to have positive Gene-Xpert as the only microbiologically confirmed cases. This figure is lower than the Nepal study in which 12.3% of the cases were confirmed microbiologically. Most cases of TB were diagnosed by pleural fluid chemistry and cytology studies on (35.2%) followed by imaging evidences in 32.4% patients which is a comparable figure with other studies. Unlike the other studies, our study found a higher figure of TB after the 1st year of dialysis.11,12
In this study, three variables were found to be independent predictors of TB burden among dialysis patients. The presence of contact history with diagnosed with a known TB patient, presence of HIV infection and duration of dialysis for more than 01 year was significantly associated with TB burden among dialysis patients.
The prevalence of TB was 2.5 times higher among ESRD patients on MHD who had a contact history with known TB patient. In our study only 13% of patients had contact history which is lower than a study done by Chagas et al which showed an 80% contact history.13
A 15-times higher prevalence of TB was found among patients who had both HIV and ESRD on MHD. The possible explanation could be augmented immunosuppressive effect by the two disease states, psychosocial impact, and possible poor drug and dialysis adherence by these patients.
Duration of dialysis of more than 01 year was significantly associated with increased TB burden among patients on MHD. The possible justification could be the longer duration of the dialysis is associated with increased risk of contact history with TB patients in overcrowded dialysis centers.
None of the sociodemographic characteristics, causes of ESRD, and comorbidities were found to be significant predictors of TB burden among ESRD patients on MHD. As it is suggested by studies, the mortality of TB among HD patients is very high.14,15 Atypical presentation and diagnostic challenges leading into late diagnosis and treatment play an important role. Our study did not assess characteristics and mortality among TB patients.
Conclusion
Our study identifies a high prevalence of TB (27%) in patients with ESRD on MHD. PTB is the most common type, and TB lymphadenitis was the most common form of EPTB. Microbiologic evidence was found only in 5.6% of study participants. Pleural fluid chemistry and cytologic studies and imaging evidences were the most common diagnostic modalities. Contact history with a known TB patient, presence of HIV infection, and longer duration of dialysis (>1year) were significantly associated with higher prevalence of TB among the study participants. A significant association was not found for sociodemographic characteristics, underlying etiology, and comorbidities. Maintaining a high index of suspicion and early diagnosis and treatment of TB among ESRD patients on MHD is important in decreasing morbidity and mortality.
Strengths and Limitations of the Study
To the best of our knowledge, this is the first study of its kind from Ethiopia on the prevalence of TB in CKD patients on MHD. It included reasonable sample size and involved multiple-dialysis centers including the largest dialysis centers at tertiary hospitals in Addis Ababa. We believe this study will provide baseline information regarding the current status of burden of TB among these patients and provide a motivation for further investigation to identify the reason for this high burden and remedy the gap. Since it is a cross-sectional study, incidence of TB among CKD patients on MHD could not be calculated. We did not follow patients on Anti-TB to assess their treatment outcome. The other limitation of this study is, it did not assess the dialysis centers’ setup and Anti-TB drug adherence among the patients. Therefore, further study is required.
Recommendations
A large-scale prospective study with a longer duration of follow-up is needed for further assessment of burden of TB among ESRD patients on MHD and for determination of factors associated with high burden of TB in these patients. Pattern of clinical presentations, TB type, Treatment adherence and outcome, clinical knowledge and inertial in suspecting and diagnosing TB among ESRD patients on MHD, and standardization of dialysis centers should be determined in the future studies.
Abbreviations
AAU, Addis Ababa University; AOR, Adjusted Odds Ratio; BP, Blood Pressure; CHS, College of Health Sciences; CKD, Chronic Kidney Disease; COR, Crude Odds Ratio; CVD, Cardiovascular Disease; DM, Diabetes Mellitus; EPTB, Extra pulmonary Tuberculosis; ESRD, End-Stage Renal Disease; HD, Hemodialysis; MHD, Maintenance Hemodialysis; HF, Heart Failure; MDRD, Modification of Diet in Renal Diseases; NCD, Non-Communicable Diseases; NGOs, Non-Governmental Organizations; PTB, Pulmonary Tuberculosis; RCTs, Randomized controlled Trials; SoM, School of Medicine; TASH, Tikur Anbessa Specialized Hospital; TB, Tuberculosis; TPT, Tuberculosis prevention therapy; WHO, World Health Organization.
Acknowledgment
We would like to express our heartfelt gratitude to our advisors, Dr. Wondwossen Amogne and Dr. Addisu Melke, for their thorough counsel and invaluable insight. We also want to thank staff members at dialysis centers.
Disclosure
All authors declare that they have no competing interests in this work.
References
1. World Health Organization. Global Tuberculosis Report 2021. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO.
2. WHO consolidated guidelines on Tuberculosis. Module 1: Prevention – Tuberculosis Preventive Treatment. Geneva: World Health Organization; 2020. Licence: CC BY-NC-SA 3.0 IGO.
3. Centers for Disease Control and Prevention. Tuberculosis: Basic TB Facts. Available from: https://www.cdc.gov/tb/topic/basics/risk.htm.
4. Horsburgh CR, Rubin EJ. Clinical practice. Latent tuberculosis infection in the United States. N Engl J Med. 2011;364(15):1441. doi:10.1056/NEJMcp1005750
5. Carney EF. The impact of chronic kidney disease on global health. Nat Rev Nephrol. 2020;16(5):251. doi:10.1038/s41581-020-0268-7
6. Lv JC, Zhang LX. Prevalence and disease burden of chronic kidney disease. Adv Exp Med Biol. 2019;1165:3–15. doi:10.1007/978-981-13-8871-2_1
7. Romanowski K, Clark E, Levin A, et al. Tuberculosis and chronic kidney disease: an emerging global syndemic. Kidney Int. 2016;90(1):34–40. doi:10.1016/j.kint.2016.01.034
8. Segall L, Covic A. Diagnosis of tuberculosis in dialysis patients: current strategy. Clin J Am Soc Nephrol. 2010;5(6):1114–1122. doi:10.2215/CJN.09231209
9. Chia S, Karim M, Elwood RK, et al. Risk of tuberculosis in dialysis patients: a population-based study. Int J Tuberc Lung Dis. 1998;2(12):989–991.
10. Pilsczek FH, Kaufmann SHE, Kaufmann SHE. Prevalence and predictors of positive tuberculin skin test results in a research laboratory. Revista da Sociedade Brasileira de Medicina Tropical. 2008;41(4):416–418. doi:10.1590/S0037-86822008000400019
11. Abdelrahman M, Sinha A, Karkar A. Tuberculosis in end-stage renal disease patients on hemodialysis. Hemodialysis Int. 2006;10(4):360–364. doi:10.1111/j.1542-4758.2006.00130.x
12. Pradhan R, Sigdel M. Prevalence, clinical presentation, and outcome of tuberculosis in patients with chronic kidney disease at a Tertiary Care Hospital in Nepal. Hindawi Intl J Nephrol. 2020;7401541. doi:10.1155/2020/7401541
13. Chagas ACF, Hans Filho G, Oliveira SMDVLD, Ivo ML, Corrêa Filho RAC, Donatti MI. Prevalence of latent tuberculosis and treatment adherence among patients with chronic kidney disease in Campo Grande, State of Mato Grosso do Sul. Revista da Sociedade Brasileira de Medicina Tropical. 2014;47(2):204–211. doi:10.1590/0037-8682-0035-2014
14. Lundin AP, Adler AJ, Berlyne GM, Friedman EA. Tuberculosis in patients undergoing maintenance hemodialysis. Am J Med. 1979;67(4):597–602. doi:10.1016/0002-9343(79)90240-7
15. Pradhan RP, Katz LA, Nidus BD, Matalon R, Eisinger RP. Tuberculosis in dialyzed patients. JAMA. 1974;229(7):798–800. doi:10.1001/jama.1974.03230450032020
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.