")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Bridging the “Know-Do” Gaps in Five Non-Communicable Diseases Using a Common Framework Driven by Implementation Science
Authors Donohue JF , Elborn JS, Lansberg P , Javed A, Tesfaye S, Rugo H, Duddi SRD , Jithoo N, Huang PH, Subramaniam K , Ramanjinappa N, Koltun A, Melamed S, Chan JCN
Received 19 October 2022
Accepted for publication 12 April 2023
Published 3 July 2023 Volume 2023:15 Pages 103—119
DOI https://doi.org/10.2147/JHL.S394088
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
James F Donohue,1 J Stuart Elborn,2 Peter Lansberg,3 Afzal Javed,4 Solomon Tesfaye,5 Hope Rugo,6 Sita Ratna Devi Duddi,7,8 Niraksha Jithoo,9 Pai-Hui Huang,10 Kannan Subramaniam,11 Nagendra Ramanjinappa,12 Arkady Koltun,13 Shari Melamed,13 Juliana CN Chan14
1UNC School of Medicine, Chapel Hill, NC, USA; 2Queen’s University, Belfast, UK; 3University Medical Center, Groningen, the Netherlands; 4Warwick Medical School, University of Warwick, Warwick, UK & Pakistan Psychiatric Research Centre, Coventry, UK; 5Sheffield Teaching Hospitals and the University of Sheffield, Sheffield, UK; 6University of California San Francisco Comprehensive Cancer Center, San Francisco, CA, USA; 7International Alliance of Patients’ Organisations, London, United Kingdom; 8DakshamA Health and Education, Delhi, India; 9Viatris Ltd, Johannesburg, South Africa; 10Viatris Pharmaceutical Co., Ltd, Taipei, Taiwan; 11Viatris Ltd, Auckland, New Zealand; 12Viatris Ltd, Bangalore, India; 13Viatris Ltd, Canonsburg, PA, USA; 14Department of Medicine and Therapeutics, Hong Kong Institute of Diabetes and Obesity, Li Ka Shing Institute of Health Sciences, The Chinese University of Hong Kong, Prince of Wales Hospital, Hong Kong, Special Administrative Regions of the People’s Republic of China
Correspondence: Juliana CN Chan, Department of Medicine and Therapeutics, Hong Kong Institute of Diabetes and Obesity, Li Ka Shing Institute of Health Sciences, The Chinese University of Hong Kong, Prince of Wales Hospital, Hong Kong, Special Administrative Regions of the People’s Republic of China, Tel +852 3505 3138, Email [email protected]
Abstract: According to the United Nations High-Level Meeting 2018, five non-communicable diseases (NCDs) including cardiovascular diseases, chronic respiratory diseases, diabetes mellitus, cancer, and mental health conditions accounted for two-thirds of global deaths. These five NCDs share five common risk factors including tobacco use, unhealthy diets, physical inactivity, alcohol use, and air pollution. Low- and middle-income countries (LMICs) face larger burden of NCDs than high-income countries (HICs), due to differences in ecological, technological, socioeconomic and health system development. Based on high-level evidence albeit mainly from HICs, the burden caused by NCDs can be reduced by affordable medicines and best practices. However, “know-do” gaps, ie, gaps between what we know in science and what we do in practice, has limited the impact of these strategies, especially in LMICs. Implementation science advocates the use of robust methodologies to evaluate sustainable solutions in health, education and social care aimed at informing practice and policies. In this article, physician researchers with expertise in NCDs reviewed the common challenges shared by these five NCDs with different clinical courses. They explained the principles of implementation science and advocated the use of an evidence-based framework to implement solutions focusing on early detection, prevention and empowerment, supplemented by best practices in HICs and LMICs. These successful stories can be used to motivate policymakers, payors, providers, patients and public to co-design frameworks and implement context-relevant, multi-component, evidence-based practices. In pursuit of this goal, we propose partnership, leadership, and access to continuing care as the three pillars in developing roadmaps for addressing the multiple needs during the journey of a person with or at risk of these five NCDs. By transforming the ecosystem, raising awareness and aligning context-relevant practices and policies with ongoing evaluation, it is possible to make healthcare accessible, affordable and sustainable to reduce the burden of these five NCDs.
Keywords: non-communicable diseases, know-do gaps, implementation science, evidence-based practices, healthcare policies
Introduction
The healthcare burden of five non-communicable diseases (NCDs) including atherosclerotic-cardiovascular diseases (ASCVD; eg ischemic heart disease [IHD], stroke, peripheral vascular disease), chronic respiratory diseases (CRDs; eg, chronic obstructive pulmonary disease [COPD] and asthma), diabetes mellitus, cancer, and mental health conditions is rising exponentially, especially in low- and middle-income countries (LMICs).1,2 In 2018, the United Nations prioritized these 5 NCDs to reduce the global burden of morbidity and mortality.3 In 2019, NCDs accounted for 73.6% of all global deaths, with CVD being responsible for 44% of all NCD-related deaths.2,4 Nearly half of these fatalities occurred before the age of 70, among which 85% of premature deaths occurred in LMICs.5,6 In addition, mental health conditions, notably depression, contribute to significant disability burden.2
Rapid changes in the ecosystem and acculturation, driven by globalization and urbanization, as well as increased life expectancy due to demographic transition have led to differences in changing patterns of prevalence of NCDs between LMICs and high-income countries (HICs).7 Despite differences in risk factors, awareness, care and practices between LMICs and HICs, there are commonalities across most NCDs in terms of environmental and lifestyle variables, such as unhealthy diet, lack of physical activity and use of tobacco in LMICs and HICs.8 However, due to insufficient evaluation to guide healthcare policies, there are major know-do gaps related to NCDs, especially in LMICs.9,10 Although several review articles have summarized the implementation gaps for individual NCD, there has not been a discussion on how to leverage lessons learnt from different NCDs for adaptation to develop solutions in different settings.11–13 Given the paucity of data in LMICs, evidence-based best practices (EBPs) focusing on early detection, prevention and empowerment in HICs can be used to guide reform in LMICs. Closing these implementation gaps in LMICs is particularly important to reduce the negative impacts of these five NCDs on the already overburdened health systems which would impede socioeconomic development.
The “Know-Do” Gap
The theory-practice gap, research-practice or knowledge-action gap, also known as the know-do or implementation gap, occurs when healthcare practitioners (HCPs) struggle to integrate the knowledge gained through an academic or a research environment with real-world clinical practice.14 A major contributing factor to this know-do gap is the gap between research and policy.14 With rapid gain in academic knowledge which forms the basis of EBP, the implementation gap is likely to widen unless changes are executed in a timely fashion.14
“Know-do” gaps to manage NCDs exist worldwide with similarities and differences between HICs and LMICs. While HICs generally have more resources for health research, the rest of the world struggles to gain scientific knowledge for informing context-relevant practice and policies. In LMICs, apart from limited funding, there are also insufficient capacity and infrastructure to conduct applied health research on NCDs.15 There is now robust evidence supporting the cost-effectiveness of many preventive treatments and care models for NCDs in HICs.10 In Turkey, researchers conducted a macro-simulation analysis using demographic and epidemiological data in 2017 and concluded that population-level reductions in salt intake and physical inactivity presented the greatest opportunity to reduce deaths due to NCDs.16 In a review by experts from ASEAN (Association of Southeast Asian Nations), it was concluded that Southeast Asian nations were not contributing enough to NCD surveillance efforts.17 The recent Coronavirus infectious disease in 2019 (COVID-19) pandemic has further compromised the ongoing efforts in the prevention of NCDs. According to the World Health Organization (WHO), 94% of countries stated that all or some of the staff employed by health ministries working on NCDs had been reallocated to control and treatment program for COVID-19. This sudden change in priorities had posed additional challenges to individual nation in addressing the needs of people with NCDs, who were also most vulnerable during acute emergencies.18
Apart from public health measures, research data from HICs suggested that many of the risk factors of NCDs were manageable, and if implemented effectively, many NCDs could be prevented and controlled.7,18,19 However, even in HICs with well-developed healthcare system, there is a considerable know-do gap in harnessing the research knowledge to develop action plans within the RE-AIM (reach, effectiveness, adoption, implementation and maintenance) framework for reducing the burden of NCDs.20,21 The paucity of similar efficacy data in LMICs has led to low levels of adoption of EBP, where local or regional data are required to formulate context-relevant policies and practices to close the know-do gap.22,23
Implementation Science
Implementation science, as defined by Global Alliance for Chronic Diseases (GACD), is the study of methods and strategies to promote the uptake of interventions that have been proven effective into routine practice, with the aim of improving people’s health.24,25 In order to close these know-do gaps and optimize NCD management, a multi-component strategy including enabling policies, people-centric healthcare practices and professional capacity is required.26 In the field of NCDs, there are examples where strategies aimed at improving settings and capacity to implement practices and policies have been rigorously evaluated.11,26 These strategies target patients, providers and systems (eg, care pathways) by improving practice environment, adapting team structures, empowering patients, relaying information to improve communications between patients and HCPs, providing feedback and incentives through audit, bridging inequality in health, promoting self-management and mobilizing community to raise awareness and promote better health and disease prevention.13,27,28
Objectives and Methods of Synthesis of Evidence
Compared to the enormous research efforts and investments which have created epidemiological and trial evidence regarding the preventable and treatable nature of many NCDs, attempts to bridge the know-do gap between research, policies and clinical practice have only been partially effective. Traditionally, the hierarchy of evidence starts with observational studies followed by randomized clinical trials (RCTs) and meta-analysis to inform practice guidelines.29 However, in order to create societal impacts, multiple stakeholders are required to bring these practice guidelines to fruition. Leaderships and partnerships are needed to co-design innovative or bold initiatives in policies (eg, legislation on seat belts, taxation on sugar sweetened beverages, tobacco control) or practices (eg, technologically-enhanced, team-based care models including peers) supported by evidence to create paradigm shifts in the current clinical practice.7
The size of population with NCDs as well as their complexity and chronicity call for concerted actions from many stakeholders in the diagnosis and management of NCDs. In this article, a group of experts familiar with the policies, practice and research relevant to these five NCDs reviewed and summarized the similarities and differences in the know-do gaps and proposed to use implementation science as a methodology to evaluate policies and practices aimed at bridging this know-do gap. Although there are review articles on similar subject mainly for individual NCD,30–33 this paper explicitly explained the principles of implementation science to develop an evidence-based framework to implement solutions, supported by best practices in these five NCDs in both HICs and LMICs. Despite differences in the clinical courses of these five NCDs, these successful stories in different settings share commonality where multi-stakeholder collaborations involving policymakers, payors, providers, patients and public participated in concert to co-design frameworks and implement evidence-based, multi-component, person-centered strategies. The multi-phase holistic care model aims at increasing health literacy, empowering patients and improving practice environment to enable early detection, prevention and treatment using a team-approach. These solutions are important in LMICs in order to make prevention and control of NCD accessible, affordable and sustainable.
Current Evidence
A literature search was conducted using PubMed, Google Scholar and Cochrane library databases to identify available evidence on the “know-do” gaps and implementation science and research in the five major NCDs: cardiovascular diseases, chronic respiratory diseases, diabetes mellitus, cancer, and mental health conditions, in LMICs and HICs. There was no date restriction in the literature search. This paper was synthesized from the results of this literature search and based on the authors’ clinical experience and perspectives related to the know-do gaps in key NCDs.
Cardiovascular Disease
In 2019, CVD was the leading cause of death contributing to 17.9 million lives lost. It explained 32% of deaths in women and 27% of deaths in men.34–36 Cardiovascular diseases include IHD, cerebrovascular disease (stroke), rheumatic heart disease, and other vascular conditions. In 2019, stroke and IHD accounted for four of five CVD fatalities, with one-third of these deaths occurring before the age of 70.36 Moreover, the number of years lived with disability (YLDs) due to CVDs has increased from 17.7 million in 1990 to 34.4 million in 2019.37 The global control rate for hypertension in 2019 was 23% for women and 18% for men with substantial variability within any level of economic development.38 In recent years, with the availability of treatments with proven efficacy and safety, characteristics such as geographic location; professional, lay and patient education; availability, access and affordability to care; as well as national and personal affluence have become important determinants for CVD mortality. Disparities in access to primary care and risk-reduction therapies, social determinants (eg, level of education and income), health literacy, suboptimal lifestyles (eg, diet, physical activity, smoking, sleep quality) can contribute to the variations in outcomes amongst countries, jurisdictions and populations.37 Despite the availability of highly affordable medications, detection, treatment and control rates remained low in the world’s poorest nations.38
Targeted education to increase disease awareness at all levels including lay persons, patients, providers and payors is emerging as a frontrunner to bridge these know-do gaps. In a survey of South Asians living in the United States, more than half of the population believed that CVD could not be prevented with many of them having poor knowledge about common modifiable risk factors. For effective outcomes, values, beliefs and behaviors need to be aligned and congruent. In some ethnic groups, apart from low health literacy, lack of data on cultural values and beliefs might lead to inappropriate use of language to address the needs and wants of individuals with widening know-do gap.39 Besides, many research and implementation efforts in CVD focused on intervention of established diseases with less focus on prevention or risk-reducing strategies by physicians or patients.40 Worldwide, not all clinicians adhered to practice guidelines or did so with low fidelity or suboptimal standard of care. Despite widespread knowledge about efficacy of many interventions, many patients remained undiagnosed, untreated or uncontrolled. Therapeutic inertia, insufficient awareness, suboptimal self-management and lack of access to continuing care and support system further widened this care gap.41
That said, there are also successful stories. In the Valsartan Amlodipine and Rosuvastatin for global cardiovascular risk decrease in daily practice (VARO) study conducted in the Czech Republic, participating physicians (N = 263) regularly screened and assessed treatment goals of CV risk in patients during visits for unrelated problems. In this study, each physician recorded clinically relevant information of 20 consecutive eligible patients giving a total of 3015 patients of whom, 2932 completed 6 months of follow-up. The WHO-SCORE system was used to assess CV risk, and treatment goals were attained in accordance with the national guidelines.42 The preferential therapy was rosuvastatin for hyperlipidemia and amlodipine and valsartan for hypertension, but additional medications could be prescribed according to the physicians’ preferences. Patients were examined at baseline, 3 months, and 6 months. Overall, the mean 10-year risk score of fatal CVDs was decreased by 35%. Systolic and diastolic blood pressure as well as total cholesterol were reduced by 12.5% (from 152 ± 8 to 133 ± 1 mmHg, p < 0.001); 11.4% (from 88 ± 1 to 78 ± 7 mmHg, p < 0.001) and 21% (from 6.3 ± 1.2 to 5.0 ± 0.9 mmol/L, p < 0.001), respectively. Lipid profiles also improved with LDL-C reduced by 28% (from 3.9 ± 1.1 to 2.8 ± 0.8 mmol/L, p < 0.001); HDL-C increased by 7% (from 1.43 ± 0.58 to 1.53 ± 0.56 mmol/L, p < 0.001) and triglycerides decreased by 25% (from 2.4 ± 0.3 to 1.8 ± 0.9 mmol/L, p < 0.001). Treatment goals for LDL-C and blood pressure were achieved by 34% and 68% of patients, respectively. The VARO study demonstrates that by using a simple but systematic approach in daily practice to assess individual and global CV risk factors, followed by treatment using modern pharmacotherapy, the risk of CVD can be reduced substantially.43
To close these know-do gaps, public awareness programs on early recognition of risk factors and promoting healthy lifestyle, timely diagnosis and risk stratification, patient education and support focusing on empowerment and engagement, optimal use of first-line and advanced treatments with reinforcement of adherence to therapy together with use of supportive services are important CVD management strategies44 (Figure 1).
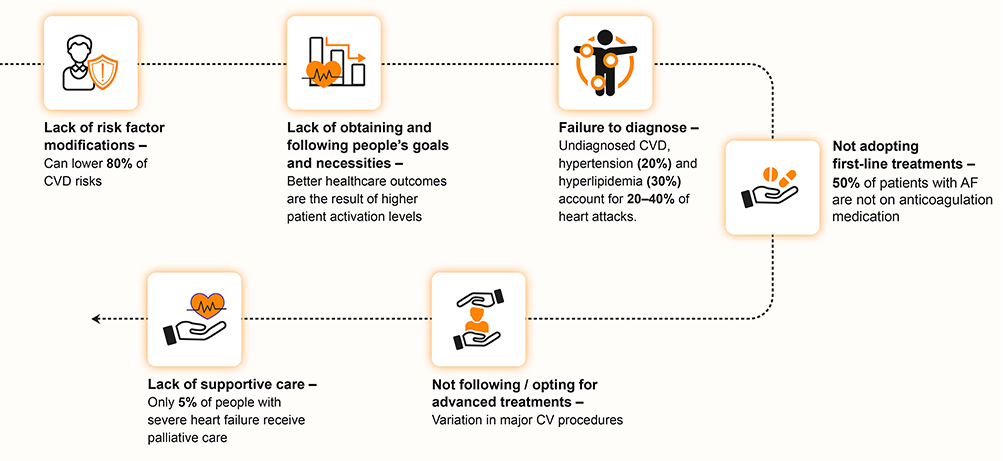 |
Figure 1 Potential impacts in reducing “know-do” gaps in patients with or at risk of CVD. Abbreviations: AF, atrial fibrillation; CV, cardiovascular; CVD, cardiovascular disease. |
Chronic Respiratory Disease
Chronic respiratory diseases (CRDs) are common consequences in modern and industrialized countries/areas. The most frequent CRDs include COPD, asthma, occupational lung disorders, bronchiectasis, and pulmonary hypertension.8 Globally, COPD is the third leading cause of death and accounted for 3.23 million deaths in 2019, predominantly in LMICs.45 In 2019, more than 300 million people worldwide suffered from asthma. The latter is the most common chronic condition in children. In LMICs, amongst those affected, disproportionately more people suffer from more severe disease.46
In 2017, an estimated 545 million people (7.4% of the global population) were diagnosed with CRDs, which had increased by 39.8% since 1990. Chronic respiratory diseases are most common in HICs and less common in South Asia and sub-Saharan Africa. While smoking is a major risk factor for CRDs in men, passive smoking, domestic air pollution from solid fuels, ambient particulate matters, and other environmental factors are the leading risk factors for women with CRDs in the Asian and African regions.47
The key know-do gap lies in the misdiagnosis of CRDs in a large proportion of those affected by the condition, even in HICs.48,49 Reducing exposure to tobacco smoke and domestic smoke are critical know-do gaps. In HIC, taxation of tobacco and banning of smoking in public places have reduced tobacco use and improved outcomes of tobacco-related diseases. In LMICs, public health measures including use of legislation are critically important to prevent these long-term conditions associated with tobacco and indoor smoke exposure.50,51
Environmental pollution from carbon fuel combustion is a preventable cause of CRDs, cardiovascular conditions and cancers. Reducing these exposures in LMICs is a high priority.52 Appropriate access and use of diagnostic tools such as spirometry and chest imaging are essential procedures for timely diagnosis of CRDs.48,49 Risk stratification and access to additional diagnostic blood tests are important know-do gaps in COPD which is a curable trait. However, even if barrier to access is removed, there are knowledge gaps regarding disease progression and residual risk. For example, the course of lung inflammation after quitting smoking as well as strategies to halt or delay disease progression remains unknown. Exploration of inter-ethnic differences in pathophysiology is constrained by lack of availability of advanced diagnostic methods/technologies or knowledge about the natural course of disease in LMICs.53 Defining the relationship between phenotype and endotype (ie, endoscopic findings), as well as understanding the cellular and molecular pathways that modulate disease pathogenesis, are prerequisites to improve the precision of diagnosis and treatment of COPD.53
In respiratory medicine, large gaps between evidence-based recommendations and clinical practice persist, posing a challenge to achieve better outcomes. For example, in Canada, asthma is inadequately assessed despite its high prevalence. Asthma action plans (AAPs), a critical component of asthma management, were offered by only 22% of physicians to affected patients.54 Similarly, sleep history was obtained in only 10% of patients with obstructive sleep apnea. The long waiting times for polysomnography to assess sleep quality delayed diagnosis and treatment resulting in avoidable deaths and economic burden. In Canada, most primary care centers have limited diagnostic facilities and/or expertise resulting in misdiagnosis or underdiagnosis of COPD. Despite the cost-effectiveness of pulmonary rehabilitation, only 10% of eligible patients benefited from this program due to lack of resources such as spirometry testing results.54 In Denmark, patients with COPD and their households only answered correctly for two-thirds of questions on COPD, reflecting major gap in health literacy.55 These examples illustrate how lack of education (professional or lay) and assessment tools delay intervention with poor outcomes. Apart from developing innovative medicine, there should be more funding to build capability of primary care centers for detecting CRDs early and ensuring access to treatment.49 Moreover, complementary medicine (eg, yoga) and pulmonary rehabilitation improved pulmonary function, quality of life and exercise tolerance in patients with COPD and can be used as an adjunct to pharmacotherapy.56,57
In LMICs, tobacco smoke is second to biomass fuels and other irritants as the cause of COPD. Biomass fuels such as charcoal, animal dung, other woods and coals are often burned in a single cook stove in the main room. This may be the only room in dwellings with poor ventilation where the exhaust may accumulate. Women who spent long hours in room with such condition either preparing meals or sleeping were disproportionately affected. Phenotypes of COPD due to exposure to environmental irritants are similar to that due to tobacco, albeit with some differences.58 By providing an exhaust pipe of the stove to outdoor, the oxygen concentration in the room can be improved with reduced deposition of particles and irritants in the lung. However, the effects of these measures on outcomes need to be evaluated systematically using implementation science methodologies in order to turn this into a practice, supported by policy.
Cancer
Globally, cancer is the second leading cause of death and accounted for 9.6 million (or one in six) deaths in 2018. The most common types of cancer in men include lung, prostate, colorectal, stomach, and liver cancer. In women, breast, colorectal, lung, cervical, and thyroid cancer are most common.59 The number of patients with cancer may rise from 19.3 million in 2020 to 28.4 million in 2040, in part driven by risk factors associated with globalization and economic growth, such as obesity.60 The rising burden of cancer imposes enormous physical, emotional, and financial strain on individuals, families, communities, and health systems. The situation is especially stark in LMICs with poorly funded and unprepared healthcare system where many patients do not have timely access to high-quality diagnosis and treatment, despite the advances made in recent years.59
The major know-do gaps identified in oncology are insufficient communication and sharing of knowledge amongst researchers, policymakers, guideline developers, and healthcare providers. There are minimal formalization or implementation of EBPs due to insufficient leveraging of current knowledge on molecular pathways and system biology underlying various types of cancer. From a broader perspective, obesity is a major risk factor for all-site cancer with some evidence supporting a multimodal weight-reducing strategy through changing lifestyles (eg, healthy diet and physical activity), avoiding harmful substances (eg, tobacco and alcohol), performing targeted screening (eg, fecal occult blood and colonoscopy for colorectal cancer) and providing personalized chemo-radiotherapy to treat cancer or prevent its recurrence.61,62
For example, in breast cancer, critical know-do gaps include defining the effects of genetic, cellular, and molecular effects on cell signaling for cancer initiation; understanding the regulators and markers of early progression, tumor development, angiogenesis, and metastasis; determining treatment targets and therapy; designing new biomarkers and treatments (eg, estrogen-receptor negative tumors); implementing sustainable lifestyle changes as well as maintaining mental well-being of patients with cancer.61,63
Regardless of cancer types, there are key challenges such as ensuring health equity and access to high-quality healthcare, using big data to detect health disparities and improve outcomes, mitigating risk factors such as smoking, providing robust post-treatment survivorship care plans, and managing comorbidities in older patients and those with NCDs with complex clinical course. To maximize the return of investment for cancer research, there is an urgent need to create national frameworks to formulate recommendations for implementation supported by other public health initiatives in order to improve health equity among cancer survivors.64
Diabetes Mellitus
Type 2 diabetes mellitus (T2DM) is the most common type of diabetes and accounts for approximately 90% of people with diabetes globally.65 In 2019, 463 million adults (aged 20–79 years) were estimated to have diabetes with 80% of them living in LMICs and 80% of the latter were undiagnosed.66 In 2021, T2DM was responsible for 6.7 million deaths.67 By 2030, the prevalence of diabetes is expected to rise to 10.2% (578.4 million people) and to 10.9% by 2045 (700.2 million people).66
Diabetes affects all age groups, especially those aged between 60 and 69 years. Whilst the rising prevalence is in part due to aging and obesity, changing ecosystem and lifestyles may also contribute to the increasing prevalence of diabetes in young people who are at high risk of premature death due to long disease duration. This double burden of aging and young onset diabetes and NCD will have a heavy toll on the healthcare system with reduced societal productivity. Apart from having two- to four-times higher risk of ASCVD and heart failure than those without diabetes, people with diabetes have high risk of comorbidities including visual loss, limb amputation, kidney disease, cancer, acute infections, liver disease and mental illness. The 2–3-fold increased risk of severe COVID-19 amongst people with diabetes highlights the vulnerability of this silent population for both acute emergencies and chronic complications making diabetes one of the biggest healthcare challenges in modern times.7,68,69
The key know-do gaps in T2DM include the whole spectrum from raising awareness, targeted screening, risk stratification, diagnostic classification and precision/personalized treatment strategies. The silent, progressive and chronic nature of diabetes calls for regular measurement and monitoring of health indexes (eg, blood glucose, blood pressure, blood cholesterol, body weight, kidney function), access to medications and support for self-management through empowerment and engagement (eg, diet, physical activity, use of alcohol and tobacco, sleep habits and stress management, treatment adherence, regular clinic visits, self-monitoring of health indexes). The lack of knowledge and awareness about diabetes and its complications has a detrimental impact on patients’ connect with healthcare services and treatment adherence.70,71 Public awareness and screening facilities followed by access to education, continuing care and medications are needed to maximize impacts.72 However, the shortage of endocrinologists and trained HCPs (notably nurses and primary care practitioners) to deliver integrated care, limited access to optimal laboratory facilities, uninterrupted supply of medications (notably insulin and organ-protective drugs including statins and renin angiotensin system inhibitors), and medical supplies (eg, test strips for blood glucose testing especially for insulin-treated patients) are major barriers in translating evidence to practice. The situation is especially stark in LMICs as well as resource-restrained settings and socially disadvantaged communities in HICs. This fragmentation of care often leads to delayed diagnosis and intervention resulting in multi-organ failure which is expensive to treat and yet highly preventable in the first place. In the United States, 33%–49% of patients with diabetes did not achieve blood glucose, blood pressure, or blood cholesterol control targets, and only 14% accomplished all three targets and did not smoke.72,73 Based on high-level evidence, the American Diabetes Association (ADA) established a framework to help primary care practitioners implement the recommendations and bridge the care gaps72 (Figure 2).
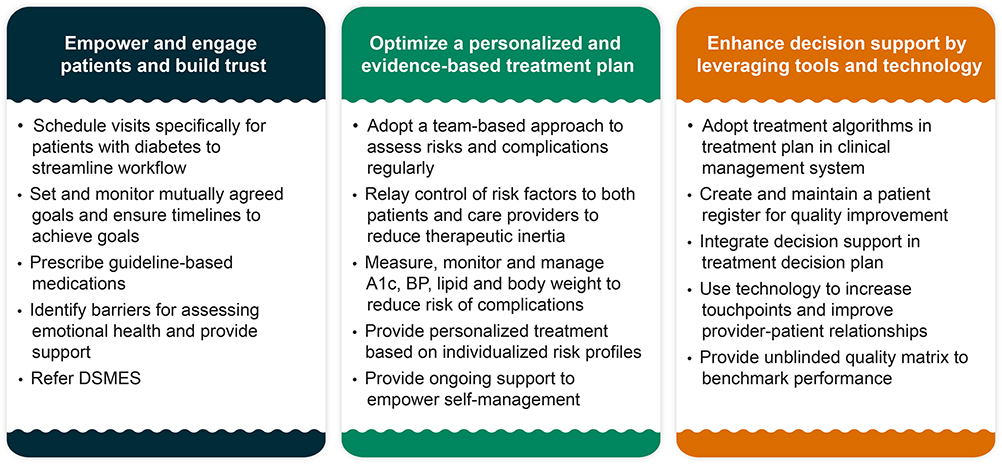 |
Figure 2 Leveraging the best practices framework in patients with diabetes. Abbreviations: A1C, glycated hemoglobin; DSMES, diabetes self-management education and support. |
In 2016, 44 thought leaders including public health workers, epidemiologists, care providers, clinical trialists and health economists were commissioned by The Lancet to review and synthesize evidence on the causes and consequences of action versus no-action in the prevention and control of diabetes. In this Lancet Commission Report published in 2020, the authors highlighted the gaps in data, care, prevention and professional knowledge, all of which were needed to translate evidence to action. To close these gaps, they recommended changing clinical settings and using a team approach to collect data systematically during routine practice for quality assurance and use the personalized data to stratify risk, empower self-management and promote shared decision-making. With increasing data digitalization, these real-world registers can be periodically linked to electronic medical record system to benchmark performance, identify unmet needs and detect disease trends for surveillance, policy planning and practice guidelines (Figure 3).7
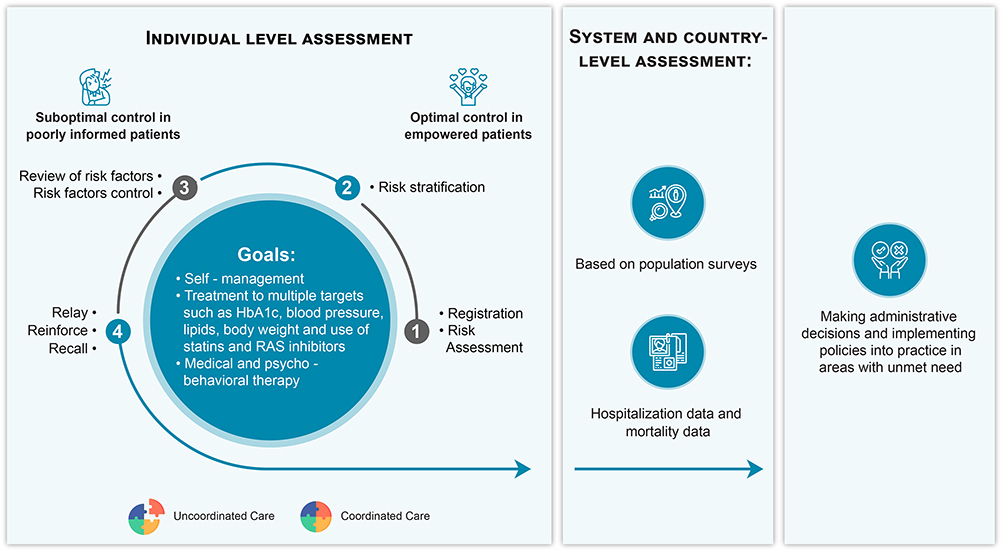 |
Figure 3 Transforming fragmented diabetes care into integrated and data-driven diabetes care using a team approach. Abbreviations: HbA1C, glycated hemoglobin; RAS inhibitors, Renin-angiotensin system inhibitors. Note: Reprinted from The Lancet, 396, Chan JCN, Lim LL, Wareham NJ, et al. The Lancet Commission on diabetes: using data to transform diabetes care and patient lives, 2019–2082, Copyright 2020, with permission from Elsevier.7 |
One example which adopts the principle of implementation science is the establishment of the Hong Kong Diabetes Register as a university-initiated quality improvement program in 1995 within a framework of universal care coverage through the Hong Kong Hospital Authority. The latter operates all publicly-funded hospitals and clinics that provide healthcare to 7 million people in Hong Kong, a cosmopolitan city in Southern China. This academic-led initiative has provided the template for the territory-wide reform of the diabetes service. Since the year 2000, diabetes centers away from busy clinics and hospital wards were set up and career paths for diabetes nurses were developed to close the gaps in assessment, education and data. These data-driven, integrated care programs had created local and regional impacts through establishment of the territory-wide Risk Assessment and Management Program in Hong Kong and the web-based Joint Asia Diabetes Evaluation Program in Asia, both of which were proven to reduce multiple risk factors, improve self-management and prevent major events and premature death. In a recent analysis of 21 million deaths during 0.5 billion patient-years among people with diagnosed diabetes from 16 HICs or jurisdictions with territory-wide data, Hong Kong had the largest decrement with 70% decline in death rates between 2000 and 2016 followed by other Asian countries including Singapore, Korea and Taiwan.74 In the UK, the One-Stop Screening Service for nine annual health checks/care processes for people with diabetes had >85% uptake. This nurse-led service was associated with early detection of diabetes complications and reduced inequality in health and received the UK National Health Service Innovation Award in 2021.75,76 This service is now being piloted in large primary care practices with high patient acceptability and can be adapted to improve quality of care in LMICs.76
Mental Health Conditions
Mental health conditions are responsible for nearly a quarter of all YLDs and are a leading cause of socio-economic burden.77 Major depressive disorder (MDD), anxiety, schizophrenia, bipolar disorder, and dementia are the most common mental health conditions.78 In 2017, MDD affected 300 million people and is one of the key causes of disability.79 In the same year, 200 million people suffered from anxiety disorders. The current pandemic of COVID-19 had led to an additional 76.2 million and 53.2 million people affected by anxiety and MDD, respectively. Suicide is the second leading cause of death among people aged 15–29 years.80 Mental health conditions have a negative impact on every aspect of life, including productivity at school or work, relationships with family and friends, and community participation which contribute towards the 20% of all YLDs.78
Many people with NCDs suffer from anxiety, stress and depression which share similar biological pathways. Co-existence of MDD with other NCDs worsen the clinical course of each other through suboptimal self-management and treatment adherence.81 Either as a standalone NCD or coexisting with other NCDs, the treatment rates for mental disorders are relatively low compared with other highly prevalent NCDs.82,83 According to the WHO, in emerging nations, more than three-quarters of people with mental, neurological, or substance abuse disorders receive no effective treatment.78 For major mental health conditions, the prevalence of care gaps is estimated to be 35–50% in HICs and 76–90% in LMICs.83,84 Adding to this challenge is social stigma, where many individuals who would benefit from mental health treatment or services choose not to seek or continue with care or do not fully engage despite treatment initiation to avoid the label of mental illness. In this light, stigma causes two types of harm, one that reduces participation in treatment by lowering people’s self-esteem and one that prevents people from social opportunities.85
Implementation Science for NCDs
These five NCDs account for the majority of global deaths and disabilities associated with poor quality of life. To increase the adoption and sustained practice of effective healthcare measures in real-world settings,27 implementation science that embraces the following tenets may close the know-do gaps in these top NCDs:
- Effective use of RCTs or quasi-experimental research designs to evaluate impact of implementation strategies to close know-do gaps.86
- Refinement of clinical practice guidelines based on RCTs taking into consideration emerging data from real-world clinical practice.
- Promotion of healthy living and creating public awareness about the risk factors for NCDs (eg, graphic warnings on cigarette packs).87
- Prescription of a series of steps summarizing how implementation should ideally be planned and executed (eg, the Consolidated Framework for Implementation Research, which classifies influential moderators or mediators of implementation outcomes).27
- Use of social and digital media to engage patients and practitioners for increasing awareness with data collection to understand where the gap is in education and how it can be improved.
Traditional clinical research studies focus on proving the efficacy of EBP on health outcomes in controlled settings. In contrast, implementation studies evaluate the impact of EBP with emphasis on the rate and quality of the utilization of EBP. There are different approaches in implementation science when generating hypotheses and creating evaluation designs.27 For example, when studying the effects of a program related to cognitive-behavioral-therapy (CBT), the subject of EBP research would be the impact of CBT on health status, whereas implementation science research may measure the proportion of clinicians providing effective CBT or the proportion of patients who attend the minimum desired number of CBT sessions.88 Between 2016 and 2018, in the Republic of Moldova, adapting existing educational training resources for NCD (eg, WHO package of essential noncommunicable [PEN] disease)89 and conducting focused clinical training in 20 sites was accompanied by sustained improvement in NCD risk factors in primary health care.90 In Nepal, similar professional educational program had been implemented and the results on quality of care are awaited.91
In the field of medicine, knowledge translation (KT) is defined as the synthesis, exchange, and application of knowledge by relevant stakeholders to accelerate the benefits of global and local innovation in strengthening health systems and improving people’s health.92,93 It is a critical strategy and opportunity for bridging know-do gaps and improving global and personal health. Strategies of KT, particularly those aimed at bridging the know-do gap in nations with emerging economies, need to align with modern medicine and practice. These KT initiatives and programs should have monitoring and evaluation built-in right from the outset to help relevant stakeholders, eg, payors, policymakers, patients, public and patients, make informed decision. The overarching goal of KT is to use “learning by doing” as a core strategy of learning organizations to implement projects93 and create societal impact through change of practice, dogma and value.
Methodological Views/Frameworks Used in Implementation Science
The current implementation science toolkit proposed by the WHO aims to assist people in learning and adapting a standard process in order to produce positive results. This toolkit comprises three modules to support multi-stakeholders including HCPs, researchers, decision makers, finance and administration officers, professionals, and journalists in implementation science.94 The first part of the toolkit introduces validated implementation science methodologies and frameworks as well as information on how to collaborate with communities, officials, and program implementers to identify locally relevant research questions that address local health concerns.95 The second part of the toolkit explains the advancement of inclusive and participatory techniques used by relevant parties in LMICs in the management of neurological or brain illnesses. It describes different participatory approaches and specific strategies to foster community relationships in implementing healthcare research results in practice.96 The third part of the toolkit proposes EBP solutions by deepening relationships with policymakers. An annotated bibliography offers a glimpse into the literature on EBP as well as successful examples of dissemination of evidence based on implementation science.97
A taxonomy of implementation science has been proposed that differentiates the theories, models, and frameworks into five categories (Figure 4) to facilitate appropriate selection and implementation of relevant approaches, and to facilitate cross-disciplinary discussions among implementation researchers.98
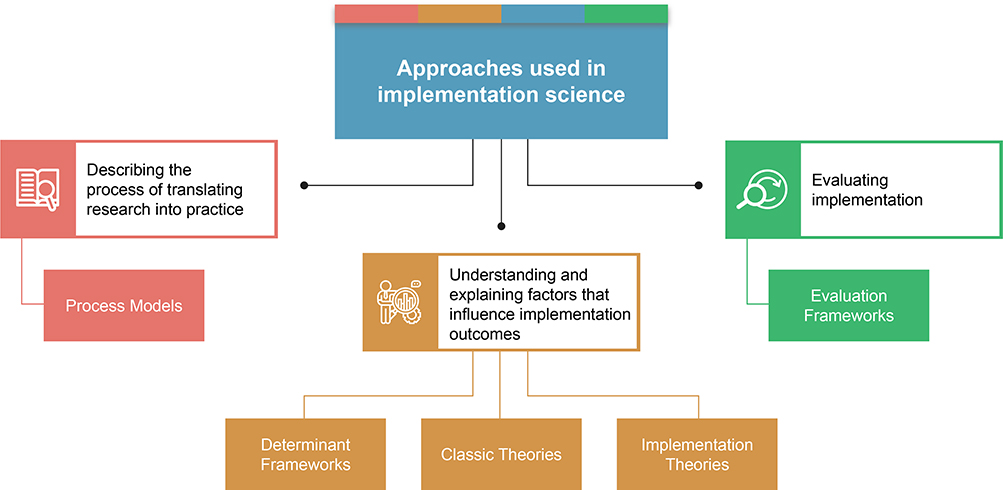 |
Figure 4 Implementation science – categories of theories, models, and frameworks. |
Bridging the Know-Do Gap Using Implementation Science
Implementation science forms a pivotal part of the roadmap for designing solutions to prevent and control NCDs. The contributions from implementation science could have a greater impact through integration with other disciplines or sectors, such as economics and public policy.9,99 Addressing the know-do gap through KT using implementation science can engage more stakeholders, notably practitioners and decision makers, to co-design best practices in clinics and increase the number of interventions that can improve health outcomes. Investment in promoting health and reducing the burden of NCDs aligns fully with the Sustainable Development Goals (SDGs) defined by the United Nations which highlight the interlinking nature of environment, health, education and the importance of reducing social disparity and health illiteracy in creating personal, community and societal wellness.12,100 To achieve these desired outcomes, the country needs to adopt a comprehensive approach in designing frameworks, formulating national policies and implementing interventions with governance, surveillance and evaluation. This will require a combination of societal, community and individual strategies acting in concert to expedite our pursuit of eradicating NCDs.26
In this review article, we propose three pillars, namely, partnership, leadership, and access to continuing care and treatment in the development of this roadmap. Partnerships, based on the concept of shared value centered on the cusp of societal and economic advancement, have the potential to imbue innovation and deliver greater societal benefits. Localization of partnerships strengthens the impact of collaboration by involving regional partners to embrace shared values and co-ownership. Implementation science adds value by facilitating champions and leaders to prove the effectiveness of adapting a localized approach supported by real-world evidence with estimation of return on investment.2,101 Promoting leadership in adopting patient-centered decision-making will result in better results, increased satisfaction, and lower healthcare costs for patients with NCDs. While payors should invest in value-added solutions for long-term sustainability, the pharmaceutical sector plays a critical role in raising awareness, developing healthcare capabilities, and improving access to affordable quality medicines and technologies for diagnosing and treating NCDs in resource-limited settings.2
Discussion
Implementation science can bridge the know-do gaps between research-proven effective treatments as well as their translation into practice and application in communities, especially in LMICs. Although the concept of EBP for NCDs has been accepted internationally, its implementation and incorporation into practice is neither uniform nor optimal. Here, global policies and international practice guidelines need to be contextualized through inter-sectoral collaborations with multi-stakeholder support during implementation. Given the regional differences in cultures, perspectives and development, setting regional goals can synergize these collaborations to improve outcomes and maximize impacts.
The five NCDs share commonality, especially in their risk factors. Over the past ten years, the United Nations High-Level Meetings (HLMs) have developed a 5 × 5 method to incorporate 5 risk factors (tobacco use, unhealthy diets, physical inactivity, alcohol use, and air pollution) that need to be changed in order to prevent these five NCDs (diabetes, chronic respiratory disease, cardiovascular disease, cancer and mental illnesses).9,19 In terms of treatments and interventions for these NCDs, the HICs have developed different strategies with the majority of patients having access to treatments compared to the poor access in many LMICs. Hence, to overcome these differences in treating NCDs, LMICs can adapt strategies from HICs to develop their own systems that prioritize primary care and treatment, use of community health workers and the use of technology.9
With increasing population growth, the prevalence of CVD is expected to rise significantly, particularly in Africa, Asia, Latin America, and the Caribbean. This will be accelerated by the growing aging population, which is expected to double between 2019 and 2050.102 Promoting optimal cardiovascular health through healthy ageing across patients’ lifespan is therefore critical. During the last four decades, many epidemiological studies and RCTs have confirmed the life-saving nature of reduction of risk factors through lifestyle modification, timely use of medications and continuing quality care. The time has come to implement healthcare and economic policies to close the know-do gaps in CVDs and evaluate their societal impacts.
For COPD, the availability and adequate use of screening and diagnostic assessments using spirometry and chest imaging is the critical first step to close the know-do gap.49 Patients with COPD often have comorbidities calling for comprehensive assessment and holistic management. These comorbidities, such as obesity and cardiometabolic risk factors, can aggravate exacerbations and adversely affect prognosis with increased hospitalization and mortality rates.103 Concerted global, regional and local efforts are needed to improve air quality, create tobacco-free environment and promote universal health care through multi-lateral collaborations including governments, non-governmental organizations, industry, academia, health administrators, medical societies, civil communities, and health care providers in order to close the know-do gaps in COPD.104
In the oncology field, the discovery of molecular targets has led to the implementation of precision medicine including the use of targeted therapy with companion diagnostics to maximize benefits, minimize harm and increase cost-effectiveness. With this head start, implementation science by combining basic science and clinical practice can be instrumental in developing novel and sustainable approaches to prevent cancer, optimize patient-centered cancer care, and improve the quality of life for cancer survivors.61,105 To this end, the impact of cancer on mental health is an area that requires more research in order to improve the holistic nature of cancer care.
Early diagnosis and intervention of T2DM is key to preventing disability and premature death.66 Apart from ensuring continuing access to care, a surveillance system will identify best practices regarding the effects of medications, lifestyle and care models using real-world evidence. The multi-system nature of diabetes which is often a cause to many NCDs makes diabetes a top priority for preventing premature death, improving quality of life and reducing personal and financial burdens.106,107 Several large-scale studies have demonstrated the life-saving and cost-effective nature of a data-driven, patient-centered care package delivered by a multidisciplinary team focusing on regular assessment of risk factors, empowerment of self-management, and access to medications with ongoing support.108,109 In Europe, based on a wealth of evidence, there is now a movement to adopt the combined use of registers, digital tools and integrated care to improve diabetes care through advocacy and setting up dialogues with key stakeholders including the European Union.110 In LMICs, the lack of infrastructures, capacity and resources are major barriers in implementing EBP29 calling for multisectoral partnerships and government leadership to strengthen the system and contextualize the evidence to transform delivery of diabetes care.7
The treatment gap remains wide for mental health conditions. To minimize the mental health treatment gap, there is an urgency to implement equity-enabling mental health system structures and procedures.99 The key recommendations include improved access to primary care as well as availability and affordability of psychotropic drugs with continuing care and support. In addition, launching information campaigns to raise awareness, increasing public investment in mental healthcare, developing integrated people-centered health systems, implementing national guidelines and policies to promote early diagnosis, and providing holistic care will increase value and bridge the treatment gap in mental healthcare.82,83
To increase local adoption, there is a need to tailor the WHO-recommended interventions and targets for NCD to local needs of the population. The diversity of stakeholders, health systems, and political structures, as well as differences in target population’s culture, language, demographic and socioeconomic background across regions, countries, and localities which change over time further emphasize the importance of using implementation science to ensure solutions are timely and relevant. In this context, social validity through alignment amongst policymakers, implementers and relevant stakeholders is the key to success. Effective NCD prevention strategies are often results of collaborative efforts where media, government and private finance institutions, multiple healthcare disciplines, regulatory agencies, and civil organizations share a common vision with willingness to overcome contextual barriers for common good.100,111 Given the overlapping nature of NCD with shared and unique causes, trajectories and consequences, the NCD agenda must shift away from focusing on a particular disease but move toward bolstering countries’ capacity to implement multi-faceted interventions to maximize the use of finite resources to achieve positive outcomes. At each stage of the implementation process, both leaderships and partnerships at different levels are needed to identify barriers and enablers in order to improve access. Here, private–public partnerships can bolster implementation efforts and expedite progress through increased funding of pilot projects with evaluation using methodologies and instruments of implementation science to inform practice and policies.100,112 Against this background, adopting good practices such as monitoring of NCDs, developing quality improvement systems focusing on primary health care, promoting active lifestyle and healthy diet are priority strategies for prevention and control of NCD in both HICs and LMICs.19
Conclusion
In this perspective article led by experts involved in implementation of EBP in NCD, we introduced the concept of implementation science with respect to five major NCDs, ie, CVDs, CRDs, cancer, diabetes, and mental health conditions. These NCDs affecting a large global population share common know-do gaps with insufficient infrastructures, capacity, equipment, protocols, policies and incentives needed to develop an integrated system from screening, diagnosis, treatment to surveillance in both LMICs and HICs. In this article, we have explained the principles of implementation science illustrated by successful stories where policies and EBP have been used to tackle some of these NCDs. These stories share commonality in adopting a multi-pronged solution to deliver multi-sectoral, multi-component and multi-disciplinary strategies focusing on early detection, prevention and empowerment to mitigate the burden of NCDs. By placing implementation science in the frontier, we aim to motivate funders, payors and policymakers to support interventions aimed at closing this know-do gap by translating evidence into clinical practice to achieve positive health outcomes. Practice aside, implementation science should also be embedded in the selection, adaptation, and evaluation of policies. To maximize the impact, knowledge generated through implementation science must be disseminated among all stakeholders including media, policymakers, payors, organizations, practitioners, researchers, patients and public through global platforms to promote multi-level collaborations to make prevention and control of NCD accessible, affordable and sustainable.
Acknowledgment
Medical writing assistance was provided by Uma Dasam and Gaurav Anand (both Tata Consultancy Services, India). The assistance was funded by Viatris.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Juliana C N Chan has received research grants and/or honoraria for consultancy and/or giving lectures from Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Celltrion, Eli-Lilly, Hua Medicine, Lee Powder, Merck Serono, Merck Sharp & Dohme, Pfizer, Servier, Sanofi and Viatris, holds patents for using biomarkers to predict risks of diabetes and its complications, and is the Chief Executive Officer (probono) of Asia Diabetes Foundation and a co-founder of GemVCare, a biotechnology company partially supported by the Hong Kong Government startup fund to use biogenetic markers, digital solutions and partnerships to implement prevention and precision care in diabetes and NCDs. Solomon Tesfaye has received honoraria from Worwag Pharma, Pfizer, Novo Nordisk, Merck, Eva Pharma, Hikma, Abbott, AstraZeneca, Nevro, P&G Health, Astellas Pharma, Viatris, Berlin-Chemie; and is on the advisory boards of Bayer, NeuroPN, Worwag Pharma, Angelini, Grunenthal, Trigocare International, Nevro, Mitsubishi Tanabe Pharma and Confo Therapeutics. Stuart Elborn has received funding as research grants or honoraria for consultancy from Novartis, Spexis, Viatris and Vertex. Peter Lansberg has received research grants and/or honoraria for consultancy and/or giving lectures from AstraZeneca, Merck Sharp & Dohme, Pfizer, Sanofi, Amgen, Kaneka and Viatris. Ratna Devi has received educational grants from Viatris, Becton Dickenson, Pfizer, Johnson and Johnson, Boehringer Ingelheim and Merck Sharp & Dohme as Chair of International Alliance of Patients’ Organizations, received educational grants as CEO DakshamA Health from Sanofi, Medtronic, Boehringer Ingelheim and Merck Sharp & Dohme. Professor Hope Rugo reports grants from Pfizer, Novartis,Eli Lilly,Genentech/Roche,OBI,Merck,Gilead Sciences,Daiichi sankyo,Seattle Genetics,Sermonix,AstraZeneca,Astellas,Veru,GSK,Taiho,AMBRXand Pionyr, personal fees from Puma,NAPO,and Blueprint, non-financial support from Merck, AstraZeneca and Gilead, outside the submitted work. Dr Kannan Subramaniam and Dr Nagendra Ramanjinappa report being employees of Viatris, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Jailobaeva K, Falconer J, Loffreda G, Arakelyan S, Witter S, Ager A. An analysis of policy and funding priorities of global actors regarding noncommunicable disease in low- and middle-income countries. Global Health. 2021;17:68. doi:10.1186/s12992-021-00713-4
2. Creating an integrated approach to noncommunicable diseases: through focus on patient-centered, sustainable, scalable local solutions. Whitepaper. Available from: https://protect-us.mimecast.com/s/EdQfCM8E9pHxgZMOMI9SERc?domain=newsroom.viatris.com.
3. United Nations. General Assembly. Political declaration of the third high-level meeting of the General Assembly on the prevention and control of non-communicable diseases Time to deliver: accelerating our response to address non-communicable diseases for the health and well-being of present and future generations. Available from: https://digitallibrary.un.org/record/710899.
4. World Health Organization. 2021 World Health Statistics. Available from: https://apps.who.int/iris/bitstream/handle/10665/342703/9789240027053-eng.pdf.
5. Bharatan T, Devi R, Huang P-H, et al. A methodology for mapping the patient journey for noncommunicable diseases in low- and middle-income countries. J Healthc Leadersh. 2021;13:35–46. doi:10.2147/JHL.S288966
6. World Health Organization. SDG target 3.4 Non-communicable diseases and mental health. Available from: https://www.who.int/data/gho/data/themes/topics/sdg-target-3_4-noncommunicable-diseases-and-mental-health.
7. Chan JCN, Lim LL, Wareham NJ, et al. The Lancet Commission on diabetes: using data to transform diabetes care and patient lives. Lancet. 2020;396:2019–2082.
8. World health organization. Chronic respiratory diseases. Key facts. Available from: https://www.who.int/health-topics/chronic-respiratory-diseases#tab=tab_1.
9. Checkley W, Ghannem H, Irazola V, et al. Management of NCD in low- and middle-income countries. Glob Heart. 2014;9:431–443. doi:10.1016/j.gheart.2014.11.003
10. Hategeka C, Adu P, Desloge A, et al. Implementation research on noncommunicable disease prevention and control interventions in low- and middle-income countries: a systematic review. PLoS Med. 2022;19(7):e1004055. doi:10.1371/journal.pmed.1004055
11. Collins T, Akselrod S, Berlina D, et al. Unleashing implementation research to accelerate national noncommunicable disease responses. Global Health. 2022;18:6. doi:10.1186/s12992-021-00790-5
12. Jackson-Morris AM, Mutungi G, Maree E, Waqanivalu T, Marten R, Nugent R. ‘Implementability’ matters: using implementation research steps to guide and support non-communicable disease national planning in low-income and middle-income countries. BMJ Glob Health. 2022;7(4):e008275. doi:10.1136/bmjgh-2021-008275
13. Peters DH, Tran NT, Adam T. Implementation research in health: a practical guide. Available from: https://apps.who.int/iris/bitstream/handle/10665/91758/9789241506212_eng.pdf.
14. Ausmed. Closing the Theory-practice gap: is it possible? Available from: https://www.ausmed.com/cpd/articles/close-theory-practice-gap.
15. Charani E, Abimbola S, Pai M, et al. Funders: the missing link in equitable global health research? PLOS Glob Public Health. 2022;2(6):e0000583. doi:10.1371/journal.pgph.0000583
16. Breda J, Allen LN, Tibet B, et al. Estimating the impact of achieving Turkey’s non-communicable disease policy targets: a macro-simulation modelling study. Lancet Reg Health Eur. 2021;1:100018. doi:10.1016/j.lanepe.2020.100018
17. Castillo-Carandang NT, Buenaventura RD, Chia Y-C, et al. Moving towards optimized noncommunicable disease management in the ASEAN Region: recommendations from a review and multidisciplinary expert panel. Risk Manag Healthc Policy. 2020;15(13):803–819. doi:10.2147/RMHP.S256165
18. GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;393(10184):1958–1972. doi:10.1016/S0140-6736(19)30041-8
19. Budreviciute A, Damiati S, Sabir DK, et al. Management and prevention strategies for non-communicable diseases (NCDs) and their risk factors. Front Public Health. 2020;8. doi:10.3389/fpubh.2020.574111
20. Miranda JJ, Kinra S, Casas JP, Davey Smith G, Ebrahim S. Non-communicable diseases in low- and middle-income countries: context, determinants and health policy. Trop Med Int Health. 2008;13:1225–1234. doi:10.1111/j.1365-3156.2008.02116.x
21. Glasgow RE, Battaglia C, McCreight M, Ayele RA, Rabin BA. Making implementation science more rapid: use of the RE-AIM framework for mid-course adaptations across five health services research projects in the veterans health administration. Front Public Health. 2020;27(8):194. doi:10.3389/fpubh.2020.00194
22. World health organization. Noncommunicable diseases. Key facts. Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases.
23. Pakenham-Walsh N. Learning from one another to bridge the “know-do gap”. Br Med J. 2004;329:1189. doi:10.1136/bmj.329.7475.1189
24. Global Alliance for Chronic Diseases. Dissemination & implementation. Available from: https://www.div12.org/implementation/overview/.
25. Eccles MP, Mittman BS. Welcome to Implementation Science. Implementation Sci. 2006;1(1). doi:10.1186/1748-5908-1-1
26. University of Washington. What is implementation science? Available from: https://impsciuw.org/implementation-science/learn/implementation-science-overview/.
27. Bauer MS, Damschroder L, Hagedorn H, Smith J, Kilbourne AM. An introduction to implementation science for the non-specialist. BMC Psychol. 2015;3:32. doi:10.1186/s40359-015-0089-9
28. Lim LL, Lau ESH, Kong APS, et al. Aspects of multicomponent integrated care promote sustained improvement in surrogate clinical outcomes: a systematic review and meta-analysis. Diabetes Care. 2018;41:1312–1320. doi:10.2337/dc17-2010
29. Owolabi MO, Yaria JO, Daivadanam M, et al. Gaps in guidelines for the management of diabetes in low- and middle-income versus high-income countries-a systematic review. Diabetes Care. 2018;41:1097–1105. doi:10.2337/dc17-1795
30. Mitchell SA, Chambers DA. Leveraging implementation science to improve cancer care delivery and patient outcomes. J Oncol Pract. 2017;8:523–529. doi:10.1200/JOP.2017.024729
31. Dineen TE, Bean C, Jung ME. Implementation of a diabetes prevention program within two community sites: a qualitative assessment. Implement Sci Commun. 2022;3:11. doi:10.1186/s43058-022-00258-6
32. Gotham HJ, Cummings JR, Dolce JN, et al. Applying implementation science in mental health services: technical assistance cases from the Mental Health Technology Transfer Center (MHTTC) network. Gen Hosp Psychiatry. 2022;75:1–9. doi:10.1016/j.genhosppsych.2022.01.004
33. Musinguzi G, Wanyenze RK, Ndejjo R, et al. An implementation science study to enhance cardiovascular disease prevention in Mukono and Buikwe districts in Uganda: a stepped-wedge design. BMC Health Serv Res. 2019;19:253. doi:10.1186/s12913-019-4095-0
34. King A. The heart of a woman: addressing the gender gap in cardiovascular disease. Nat Rev Cardiol. 2011;8:239–240. doi:10.1038/nrcardio.2011.49
35. Aifah A, Iwelunmor J, Akwanalo C, et al. The Kathmandu declaration on global CVD/hypertension research and implementation science: a framework to advance implementation research for cardiovascular and other noncommunicable diseases in low- and middle-income countries. Glob Heart. 2019;14:103–107. doi:10.1016/j.gheart.2019.05.006
36. World health organization. Cardiovascular diseases. Key facts. Available from: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1.
37. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
38. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957–980. doi:10.1016/S0140-6736(21)01330-1
39. Kandula NR, Tirodkar MA, Lauderdale DS, Khurana NR, Makoul G, Baker DW. Knowledge gaps and misconceptions about coronary heart disease among U.S. South Asians. Am J Prev Med. 2010;38:439–442. doi:10.1016/j.amepre.2009.12.034
40. Chow CK, Rodgers A. Lost in translation: the gap between what we know and what we do about cardiovascular disease. Med J Aust. 2016;204:291–292. doi:10.5694/mja16.00190
41. Pearson TA, Peters TD. The treatment gap in coronary artery disease and heart failure: community standards and the post-discharge patient. Am J Cardiol. 1997;80:45H–52H. doi:10.1016/S0002-9149(97)00820-5
42. World health organization. SCORE for health data package. Available from: https://www.who.int/data/data-collection-tools/score.
43. Štulc T, Lánská V, Šnejdrlová M, Vrablík M, Prusíková M, Češka R. A comprehensive guidelines-based approach reduces cardiovascular risk in everyday practice: the VARO study. Arch Med Sci. 2017;13:705–710. doi:10.5114/aoms.2016.64865
44. McClellan M, Brown N, Califf RM, Warner JJ. Call to action: urgent challenges in cardiovascular disease: a presidential advisory from the American Heart Association. Circulation. 2019;139:e44–e54. doi:10.1161/CIR.0000000000000652
45. World health organization. Chronic obstructive pulmonary disease. Key facts. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
46. The global asthma report 2018. Auckland, New Zealand: Global Asthma Network; 2018. Available from: http://globalasthmareport.org/2018/index.html.
47. GBD Chronic Respiratory. Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8:585–596. doi:10.1016/S2213-2600(20)30105-3
48. Labaki WW, Han MK. Chronic respiratory diseases: a global view. Lancet Respir Med. 2020;8:531–533. doi:10.1016/S2213-2600(20)30157-0
49. Labaki WW, Han MK. Improving detection of early chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2018;15:S243–S248. doi:10.1513/AnnalsATS.201808-529MG
50. Laniado-Laborín R. Smoking and chronic obstructive pulmonary disease (COPD). Parallel epidemics of the 21 century. Int J Environ Res Public Health. 2009;6:209–224. doi:10.3390/ijerph6010209
51. Balmes JR, Eisen EA. Household air pollution and chronic obstructive pulmonary disease. “a riddle, wrapped in a mystery, inside an Enigma”. Am J Respir Crit Care Med. 2018;197:547–549. doi:10.1164/rccm.201801-0033ED
52. Perera F. Pollution from fossil-fuel combustion is the leading environmental threat to global pediatric health and equity: solutions exist. Int J Environ Res Public Health. 2017;15:16. doi:10.3390/ijerph15010016
53. Sidhaye VK, Nishida K, Martinez FJ. Precision medicine in COPD: where are we and where do we need to go? Eur Respir Rev. 2018;27:180022. doi:10.1183/16000617.0022-2018
54. Boulet LP, Bourbeau J, Skomro R, Gupta S. Major care gaps in asthma, sleep and chronic obstructive pulmonary disease: a road map for knowledge translation. Can Respir J. 2013;20:265–269. doi:10.1155/2013/496923
55. Nakken N, Janssen DJA, van den Bogaart EHA, et al. Knowledge gaps in patients with COPD and their proxies. BMC Pulm Med. 2017;17:136. doi:10.1186/s12890-017-0481-8
56. Jin L, An W, Li Z, Jiang L, Chen C. Pulmonary rehabilitation training for improving pulmonary function and exercise tolerance in patients with stable chronic obstructive pulmonary disease. Am J Transl Res. 2021;13:8330–8336.
57. Sahasrabudhe SD, Orme MW, Jones AV, Tillu G, Salvi SS, Singh SJ. Potential for integrating yoga within pulmonary rehabilitation and recommendations of reporting framework. BMJ Open Respir Res. 2021;8:e000966. doi:10.1136/bmjresp-2021-000966
58. Pratiti R, Vadala D, Kalynych Z, Sud P. Health effects of household air pollution related to biomass cook stoves in resource limited countries and its mitigation by improved cookstoves. Environ Res. 2020;186:109574. doi:10.1016/j.envres.2020.109574
59. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. doi:10.3322/caac.21660
60. World health organization. Cancer. Available from: https://www.who.int/health-topics/cancer#tab=tab_1.
61. Elmore LW, Greer SF, Daniels EC, et al. Blueprint for cancer research: critical gaps and opportunities. CA Cancer J Clin. 2021;71:107–139. doi:10.3322/caac.21652
62. Eccles SA, Aboagye EO, Ali S, et al. Critical research gaps and translational priorities for the successful prevention and treatment of breast cancer. Breast Cancer Res. 2013;15:R92. doi:10.1186/bcr3493
63. Thompson A, Brennan K, Cox A, et al. Evaluation of the current knowledge limitations in breast cancer research: a gap analysis. Breast Cancer Res. 2008;10:R26. doi:10.1186/bcr1983
64. Lee Smith J, Hall IJ. Advancing health equity in cancer survivorship: opportunities for public health. Am J Prev Med. 2015;49:S477–S482. doi:10.1016/j.amepre.2015.08.008
65. International Diabetes Federation. Type 2 diabetes. Available from: https://idf.org/aboutdiabetes/type-2-diabetes.html.
66. International Diabetes Federation. IDF diabetes atlas. Brussels, Belgium: International Diabetes Federation; 2019. Available from: https://diabetesatlas.org/upload/resources/material/20200302_133351_IDFATLAS9e-final-web.pdf.
67. International Diabetes Federation Diabetes Atlas. Diabetes around the world in 2021. Available from: https://diabetesatlas.org/.
68. Dunlay SM, Givertz MM, Aguilar D, et al. Type 2 diabetes mellitus and heart failure: a scientific statement from the American Heart Association and the Heart Failure Society of America: this statement does not represent an update of the 2017 ACC/AHA/HFSA heart failure guideline update. Circulation. 2019;140:e294–e324. doi:10.1161/CIR.0000000000000691
69. Steenblock C, Schwarz PEH, Ludwig B, et al. COVID-19 and metabolic disease: mechanisms and clinical management. Lancet Diabetes Endocrinol. 2021;9:786–798. doi:10.1016/S2213-8587(21)00244-8
70. Karachaliou F, Simatos G, Simatou A. The challenges in the development of diabetes prevention and care models in low-income settings. Front Endocrinol. 2020;11:518. doi:10.3389/fendo.2020.00518
71. Shivashankar R, Kirk K, Kim WC, et al. Quality of diabetes care in low- and middle-income Asian and Middle Eastern countries (1993–2012): 20-year systematic review. Diabetes Res Clin Pract. 2015;107:203–223. doi:10.1016/j.diabres.2014.11.004
72. Davies MJ, D’Alessio DA, Fradkin J, et al. Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2018;61:2461–2498. doi:10.1007/s00125-018-4729-5
73. American Diabetes Association. Standards of medical care in diabetes-2015 abridged for primary care providers. Clin Diabetes. 2015;33:97–111. doi:10.2337/diaclin.33.2.97
74. Magliano DJ, Chen L, Carstensen B, et al. Trends in all-cause mortality among people with diagnosed diabetes in high-income settings: a multicountry analysis of aggregate data. Lancet Diabetes Endocrinol. 2022;10:112–119. doi:10.1016/S2213-8587(21)00327-2
75. Ross JAD, Barron E, McGough B, et al. Uptake and impact of the English National Health Service digital diabetes prevention programme: observational study. BMJ Open Diabetes Res Care. 2022;10:e002736. doi:10.1136/bmjdrc-2021-002736
76. Binns-Hall O, Selvarajah D, Sanger D, Walker J, Scott A, Tesfaye S. One-stop microvascular screening service: an effective model for the early detection of diabetic peripheral neuropathy and the high-risk foot. Diabet Med. 2018;35:887–894. doi:10.1111/dme.13630
77. Hyman SE. The unconscionable gap between what we know and what we do. Sci Transl Med. 2014;6:253cm9. doi:10.1126/scitranslmed.3010312
78. World Health Organization. World Health Report 2001. Mental health: new understanding, new hope. Geneva, Switzerland: World Health Organization; 2001. Available from: https://apps.who.int/iris/handle/10665/42390.
79. James SL, Abate D, Abate KH. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858.
80. IHME. New Global Burden of Disease analyses show depression and anxiety among the top causes of health loss worldwide, and a significant increase due to the COVID-19 pandemic. Available from: http://www.healthdata.org/acting-data/new-ihme-analyses-show-depression-and-anxiety-among-top-causes-health-burden-worldwide.
81. Fisher EB, Chan JC, Nan H, Sartorius N, Oldenburg B. Co-occurrence of diabetes and depression: conceptual considerations for an emerging global health challenge. J Affect Disord. 2012;142:S56–S66. doi:10.1016/S0165-0327(12)70009-5
82. Qin X, Hsieh CR. Understanding and addressing the treatment gap in mental healthcare: economic perspectives and evidence from China. Inquiry. 2020;57. doi:10.1177/0046958020950566
83. Kohn R, Saxena S, Levav I, Saraceno B. The treatment gap in mental health care. Bull World Health Organ. 2004;82:858–866.
84. Van Ginneken N, Tharyan P, Lewin S, et al. Non-specialist health worker interventions for the care of mental, neurological and substance-abuse disorders in low- and middle-income countries. Cochrane Database Syst Rev. 2013;11. doi:10.1002/14651858.CD009149.pub2
85. Corrigan P. How stigma interferes with mental health care. Am Psychol. 2004;59:614–625. doi:10.1037/0003-066X.59.7.614
86. Miller CJ, Smith SN, Pugatch M. Experimental and quasi-experimental designs in implementation research. Psychiatry Res. 2020;283:112452.
87. Allen NL, Nicholson DB, Yeung TB, Goiana-da-Silva F. Implementation of non-communicable disease policies: a geopolitical analysis of 151 countries. Lancet Glob Health. 2020;8:e50–e58. doi:10.1016/S2214-109X(19)30446-2
88. Lopez MA, Basco MA. Effectiveness of cognitive behavioral therapy in public mental health: comparison to treatment as usual for treatment-resistant depression. Adm Policy Ment Health. 2015;42:87–98. doi:10.1007/s10488-014-0546-4
89. World Health Organization. WHO package of essential noncommunicable (PEN) disease interventions for primary health care; 2022.
90. Collins D, Inglin L, Laatikainen T, et al. Implementing a package of noncommunicable disease interventions in the Republic of Moldova: two-year follow-up data. Prim Health Care Res Dev. 2020;21. doi:10.1017/S1463423620000420
91. Schwarz D, Dhungana S, Kumar A, et al. An integrated intervention for chronic care management in rural Nepal: protocol of a type 2 hybrid effectiveness-implementation study. Trials. 2020;21:119. doi:10.1186/s13063-020-4063-3
92. Pablos-Mendez A, Shademani R. Knowledge translation in global health. J Contin Educ Health Prof. 2006;26:81–86. doi:10.1002/chp.54
93. World health organization. Bridging the “Know–Do” gap meeting on knowledge translation in global health. Available from: https://www.measureevaluation.org/resources/training/capacity-building-resources/high-impact-research-training-curricula/bridging-The-know-do-gap.pdf.
94. World health organization. A guide to implementation research in the prevention and control of noncommunicable diseases. Available from: https://apps.who.int/iris/bitstream/handle/10665/252626/9789241511803-eng.pdf.
95. NIH. Fogarty international center. Toolkit Part 1: implementation science methodologies and frameworks. Available from: https://www.fic.nih.gov/About/center-global-health-studies/neuroscience-implementation-toolkit/Pages/methodologies-frameworks.aspx.
96. NIH. Fogarty international center. Toolkit part 2: participatory research models and building stakeholder relationships. Available from: https://www.fic.nih.gov/About/center-global-health-studies/neuroscience-implementation-toolkit/Pages/methodologies-frameworks.aspx.
97. NIH. Fogarty international center. Toolkit part 3: dissemination strategies in evidence-based policy and practice. Available from: https://www.fic.nih.gov/About/center-global-health-studies/neuroscience-implementation-toolkit/Pages/methodologies-frameworks.aspx.
98. Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015;10:53. doi:10.1186/s13012-015-0242-0
99. McGinty EE, Eisenberg MD. Mental health treatment gap-the implementation problem as a research problem. JAMA Psychiatry. 2022;79(8):746. doi:10.1001/jamapsychiatry.2022.1468
100. Breda J, Wickramasinghe K, Peters DH, et al. One size does not fit all: implementation of interventions for non-communicable diseases. BMJ. 2019;367. doi:10.1136/bmj.l6434
101. Votova K, Laberge A-M, Grimshaw JM, Wilson B. Implementation science as a leadership capability to improve patient outcomes and value in healthcare. Healthc Manage Forum. 2019;32:307–312. doi:10.1177/0840470419867427
102. United Nations. World population ageing 2019. highlights. Available from: https://www.un.org/en/development/desa/population/publications/pdf/ageing/.WorldPopulationAgeing2019-Highlights.pdf.
103. Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95–109. doi:10.2147/COPD.S54473
104. Ministry of Health and Family Welfare. National multisectoral action plan for prevention and control of common NCDS. Available from: https://main.mohfw.gov.in/sites/default/files/National%20Multisectoral%20Action%20Plan%20%28NMAP%29%20for%20Prevention%20and%20Control%20of%20Common%20NCDs%20%282017-22%29_1.pdf.
105. Thamlikitkul V. Bridging the gap between knowledge and action for health: case studies. Bull World Health Organ. 2006;84:603–607. doi:10.2471/BLT.05.023622
106. Low Wang CC, Hess CN, Hiatt WR, Goldfine AB. Clinical update: cardiovascular disease in diabetes mellitus: atherosclerotic cardiovascular disease and heart failure in type 2 diabetes mellitus - mechanisms, management, and clinical considerations. Circulation. 2016;133:2459–2502. doi:10.1161/CIRCULATIONAHA.116.022194
107. Seshasai SR, Kaptoge S, Thompson A, et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N Engl J Med. 2011;364:829–841.
108. Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008;358:580–591. doi:10.1056/NEJMoa0706245
109. Jiao FF, Fung CSC, Wan EYF, et al. Five-year cost-effectiveness of the multidisciplinary risk assessment and management programme-diabetes mellitus (RAMP-DM). Diabetes Care. 2018;41:250–257. doi:10.2337/dc17-1149
110. European Diabetes Forum. EUDF policy recommendations. European Diabetes Forum (eudf.org); 2022.
111. World Health Organization. A guide to implementation research in the prevention and control of noncommunicable diseases. Geneva: World Health Organization; 2016. Available from: https://apps.who.int/iris/bitstream/handle/10665/252626/9789241511803-eng.pdf.
112. Goyet S, Touch S, Ir P, et al. Gaps between research and public health priorities in low income countries: evidence from a systematic literature review focused on Cambodia. Implement Sc. 2015;10:1–2.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.