")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Blueberry (Vaccinium myrtillus) Induced Anaphylaxis in a Chinese Child with Lipid Transfer Protein Sensitization
Authors Jiang N, Xiang L, Guan H, Zhang X
Received 14 September 2023
Accepted for publication 10 November 2023
Published 18 November 2023 Volume 2023:16 Pages 1253—1258
DOI https://doi.org/10.2147/JAA.S436561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Luis Garcia-Marcos
Nannan Jiang,1– 3 Li Xiang,1– 3 Hui Guan,1– 3 Xudong Zhang1– 3
1Department of Allergy, Beijing Children′s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, People’s Republic of China; 2Key Laboratory of Major Diseases in Children, Ministry of Education, Beijing, People’s Republic of China; 3China National Clinical Research Center for Respiratory Diseases, Beijing, People’s Republic of China
Correspondence: Li Xiang, Department of Allergy, Beijing Children′s Hospital, Capital Medical University, National Center for Children′s Health, No. 56 Nanlishi Road, Xicheng District, Beijing, 100045, People’s Republic of China, Tel/Fax +861059616934, Email [email protected]
Purpose: Fruits have been identified as the primary triggers of anaphylaxis in older children in the Chinese population, especially among individuals with pollen sensitization. To date, no allergies have been reported after blueberry ingestion in the Chinese population.
Case Report: A 12-year-old girl experienced one episode of anaphylaxis within 30 minutes of having breakfast (including milk, egg, wheat bread, and blueberry) while walking to school. She menstruated during this episode. Prompt treatment with epinephrine and fluid therapy led to full recovery within 24 h. Specific IgE was conducted using ImmunoCAP, and the patient exhibited sensitization to several pollens, mainly Japanese hop (74.3 kUa/L) and mugwort (26.5 kUa/L). Regarding specific IgE to allergen components, the patient showed sensitization primarily to lipid transfer protein (LTP) components from mugwort Art v 3 (79.7 kUa/L), wheat Tri a 14 (12.4 kUa/L) and peach Pru p 3 (2.15 kUa/L), but tested negative for omega-5 gliadin. The prick test results were positive for blueberries (wheal size 9.5 mm), cherries (wheal size 6.5 mm), kiwifruits (wheal size 6 mm), and pears (wheal size 4.5 mm). Our patient was provided with an epi-pen and was advised to avoid consuming relevant fruits. After four months of follow-up, the patient had not experienced any episodes of anaphylaxis since these recommendations were implemented.
Conclusion: We report for the first time a Chinese child with severe IgE-mediated immediate-type anaphylactic reaction to blueberries, in whom we identified LTP as the suspected allergen component.
Keywords: anaphylaxis, lipid transfer protein, food allergy
Introduction
Fruits, particularly in individuals with pollen sensitization, have been identified as the primary triggers of anaphylaxis in preschool and school-age children in the Chinese population.1 Blueberry, a member of the Ericaceae family and genus Vaccinium, is consumed worldwide in various forms such as fresh fruits, jams, and juices, and is recognized as a rich source of natural antioxidants. Blueberry-induced anaphylaxis is extremely rare. In a community-based study conducted in Turkey, where blueberry production and consumption were highest, the prevalence of blueberry allergy in children, as confirmed by a double-blind placebo-controlled food challenge (DBPCFC), was found to be 0.0000634% (1/20,288).2 Gebhardt et al reported a case of a 21-year-old woman who experienced anaphylaxis after consuming a blueberry pancake. Further investigation through IgE immunoblotting and inhibition tests confirmed that the causative allergen was lipid transfer protein (LTP)3 and, to date, no allergies have been reported after blueberry ingestion in the Chinese population. Here, we report for the first time a Chinese child with severe IgE-mediated immediate anaphylactic reaction to blueberries, in whom we identified LTP as the suspected allergen component.
Case Presentation
A 12-year-old girl was referred to our clinic in April 2023 after experiencing flushing, hives, vomiting, fainting, and syncope within 30 minutes of having breakfast (including milk, egg, wheat bread, and blueberry) while walking to school. Upon admission to the emergency department (ED), the patient presented with hypotension (BP, 89/52 mmHg). Prompt treatment with epinephrine and fluid therapy led to full recovery within 24 h. She menstruated during this episode. Additionally, six months before this episode (October 2022), she had experienced similar symptoms during fast walking outdoors, but she did not remember the specific foods she had eaten before the episode. The patient had a history of rhinoconjunctivitis due to pollen sensitization since the age of 5 years, and was being treated with oral antihistamines on demand. The patient’s father and mother had a history of recurrent urticaria, and her father experienced anaphylaxis, although the cause was uncertain. Specific IgE were measured using ImmunoCAP (Thermo Fisher Scientific, Sweden), The patient exhibited sensitization to several pollens, mainly Japanese hop (74.3 kUa/L), mugwort (26.5 kUa/L), mountain juniper (2.23 kUa/L) and Dermatophagoides pteronyssinus (2.89 kUa/L), Dermatophagoides farina (13.2kUa/L), but that for common foods (including soybean, egg, milk, wheat, peanut, crab, shrimp) was negative (Table 1). Regarding specific IgE to allergen components, the patient showed sensitization primarily to LTP components from mugwort Art v 3 (79.7 kUa/L), wheat Tri a 14 (12.4 kUa/L) and peach Pru p 3 (2.15 kUa/L), but tested negative for omega-5 gliadin. Prick-to-prick testing (PPT) was performed on 22 fruit and wheat allergens (salt-soluble proteins and gliadins). Histamine and normal saline were used as the positive and negative controls, respectively (Beijing Macro-Union Pharmaceutical Co. Ltd., Beijing, China). The prick test results were positive for blueberries (wheal size 9.5 mm), cherries (wheal size 6.5 mm), kiwifruits (wheal size 6 mm), and pears (wheal size 4.5 mm) (Table 1 and Figure 1). Challenges were not performed due to ethical and safety concerns, considering the high clinical suspicion of blueberry hypersensitivity based on the patient’s clinical history and confirmed blueberry sensitization on skin testing. Our patient was provided with an epi-pen and advised to avoid consuming relevant fruits. After four months of follow-up, the patient had not experienced any episodes of anaphylaxis since these recommendations were implemented.
 |
Table 1 In vitro Allergy Diagnostics: Specific IgE-Antibody Detection Results (Immuno CAP) |
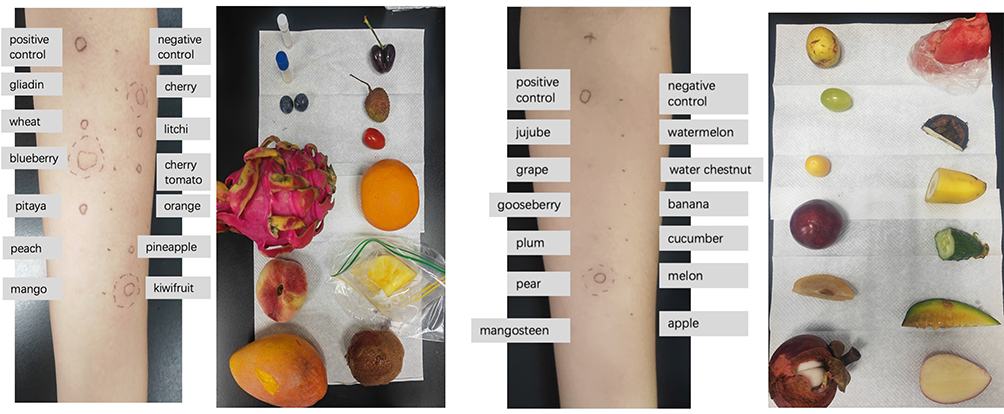 |
Figure 1 Legends: Prick-to-prick testing for 22 fruits and wheat allergens (water/dilute soluble allergens and gliadins soluble in 75% alcohol) shows strong positive results for blueberry (wheal size 9.5mm), cherry (wheal size 6.5mm), kiwifruit (wheal size 6mm), and pear (wheal size 4.5mm). A positive score was considered negative if it was less than 1/3 of the wheal diameter or if it was not different from saline. |
Discussion
The sensitization profile of the patient revealed regional pollen and multiple plant food sensitization. We then performed component-resolved diagnosis and found evidence of LTP sensitization in this patient. Allergic reactions to LTP tend to be more severe, and are the main cause of primary food allergies in Mediterranean countries by far. They are also responsible for the largest number of food-induced anaphylactic reactions, as well as food-dependent NSAID-induced hypersensitivity (FDNIH).4 Although LTP sensitization is more common in children living in Mediterranean areas, it is rare but has been increasingly reported in the Chinese population.5 One study recently published study demonstrated that Art v 3 (LTP) might be a major biomarker for plant food allergies in Chinese individuals with autumn pollinosis, and LTPs (Pru p 3, Ara h 9, and Cor a 8) have been suggested as major food allergens for mugwort pollen-related food allergies in China and may contribute to systemic reactions.5
Cofactors reportedly play a role in 14–18.3% of cases in children, and exercise and concomitant infections are well-documented cofactors of anaphylaxis in children.6 The patient suffered two anaphylactic episodes during fast walking rather than high intensity exercise. A study by Wong et al showed that even mild levels of physical activity can also provoke systemic symptoms in patients with wheat-dependent exercise-induced anaphylaxis (WDEIA).7 Additionally, the patient experienced anaphylaxis during her monthly menses, which is consistent with a case reported by Fischer et al,8 in which a WDEIA patient’s anaphylactic reactions occurred exclusively during her menses, thus indicating the potential contribution of female sex hormones in allergic reactions. The contribution of gender or female sex hormones in allergic reactions has been discussed for a long time; however, mechanisms underlying hormone-triggered allergic reactions are still poorly understood.9 Sex steroids, mainly estradiol and progesterone, have been demonstrated to elicit mast cell activation. Mast cell degranulation is modulated by sex hormones in a gender-selective fashion, with mast cells from females being more susceptible to the effects of sex steroids than mast cells from males.10 Female patients presenting with anaphylaxis before and during the menstrual period are given a diagnosis of catamenial anaphylaxis.11 Furthermore, the patient experienced two anaphylactic episodes during the pollen season (April and October, spring, and autumn, respectively). Our previous study, which enrolled 108 children with pollen sensitization and anaphylaxis, found that approximately 64% of exercise-induced anaphylaxis cases occurred during pollen season, particularly in autumn.1 On the other hand, Gabrielli et al12 revealed that severe anaphylactic reactions to fruits were more likely to occur in spring among the Canadian population; the authors concluded that the increased risk in spring may be related to higher pollen counts that sensitize the immune system and reduce the reaction threshold. Given these data and the recognized cofactors of anaphylaxis, it would be worthwhile to advise patients with pollen allergies who have a known fruit/vegetable allergy to avoid cofactors associated with food consumption.
Due to the limitations of the purified allergen component, we were unable to conduct immunoblotting and inhibition tests, and the reagents for other pan-allergens or cross-allergens such as PR-10 and profilin are not available in our hospital. It is worth noting that PR-10 and profilin typically induce oral allergy symptoms. Based on the patient’s history of anaphylaxis and previous published data, we suspect that LTPs are responsible for inducing anaphylaxis in this patient.
Conclusion
In summary, we report for the first time a Chinese patient with an IgE-mediated allergy to blueberries, which was most likely attributable to sensitization to LTP.
Ethical Approval
The study was approved by the Research and Ethics Board of Beijing Children’s Hospital (approval number: 2022-E-023-R).
Declaration of Patient Consent
The authors obtained informed consent for publication from the patient and her parents. The patient and her parents understand that her personal information will not be published. The case required institutional approval to publish the case details and was reviewed and approved by the Ethical Committee of Beijing Children’s Hospital.
Acknowledgment
We appreciated the patient and investigators who participated in this case report.
Funding
This study was supported by the Respiratory Research Project of the National Clinical Research Center for Respiratory Diseases (HXZX-20210203, HXZX-20210204, HXZX-202107) and The Project for Development of Beijing Municipal Research Ward (BCRW202101).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Jiang N, Xu W, Huang H, et al. Anaphylaxis in Chinese Children with Pollen Sensitization: triggers, Clinical Presentation, and Acute Management. J Asthma Allergy. 2022;15:633–643. doi:10.2147/jaa.S363113
2. Dereci S, Orhan F, Koca T, et al. Prevalence of blueberry allergy in a Turkish population. Ann Allergy Asthma Immunol. 2015;114(3):259–260. doi:10.1016/j.anai.2014.12.016
3. Gebhardt C, Vieths S, Gubesch M, et al. 10 kDa lipid transfer protein: the main allergenic structure in a German patient with anaphylaxis to blueberry. Allergy. 2009;64(3):498–499. doi:10.1111/j.1398-9995.2008.01923.x
4. Sánchez-López J, Araujo G, Cardona V, et al. Food-dependent NSAID-induced hypersensitivity (FDNIH) reactions: unraveling the clinical features and risk factors. Allergy. 2021;76(5):1480–1492. doi:10.1111/all.14689
5. Deng S, Yin J. Mugwort Pollen-Related Food Allergy: lipid Transfer Protein Sensitization and Correlation With the Severity of Allergic Reactions in a Chinese Population. Allergy Asthma Immunol Res. 2019;11(1):116–128. doi:10.4168/aair.2019.11.1.116
6. Shin M. Food allergies and food-induced anaphylaxis: role of cofactors. Clin Exp Pediatr. 2021;64(8):393–399. doi:10.3345/cep.2020.01088
7. Wong GK, Huissoon AP, Goddard S, et al. Wheat dependent exercise induced anaphylaxis: is this an appropriate terminology? J Clin Pathol. 2010;63(9):814–817. doi:10.1136/jcp.2010.078808
8. Fischer J, Schuck E, Biedermann T. Wheat-dependent exercise-induced anaphylaxis exclusively during menstruation. Allergy. 2010;65(10):1347–1348. doi:10.1111/j.1398-9995.2010.02356.x
9. Jensen-Jarolim E, Untersmayr E. Gender-medicine aspects in allergology. Allergy. 2008;63(5):610–615. doi:10.1111/j.1398-9995.2008.01645.x
10. Muñoz-Cruz S, Mendoza-Rodríguez Y, Nava-Castro KE, et al. Gender-related effects of sex steroids on histamine release and FcεRI expression in rat peritoneal mast cells. J Immunol Res. 2015;2015:351829. doi:10.1155/2015/351829
11. Lavery WJ, Bernstein JA. Cyclical hypersensitivity, anaphylaxis, and related hormonal reaction. Ann Allergy Asthma Immunol. 2019;122(2):140–147. doi:10.1016/j.anai.2018.11.016
12. Gabrielli S, Clarke AE, Morris J, et al. Fruit-Induced Anaphylaxis: clinical Presentation and Management. J Allergy Clin Immunol Pract. 2021;9(7):2825–2830.e2822. doi:10.1016/j.jaip.2021.02.055
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.