")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Barriers and Facilitators for Female Healthcare Professionals to Be Leaders in Pakistan: A Qualitative Exploratory Study
Authors Iftikhar S, Yasmeen R, Khan RA, Arooj M
Received 28 November 2022
Accepted for publication 15 April 2023
Published 31 May 2023 Volume 2023:15 Pages 71—82
DOI https://doi.org/10.2147/JHL.S399430
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Sundus Iftikhar,1 Rahila Yasmeen,2 Rehan Ahmed Khan,2 Mahwish Arooj1
1University College of Medicine and Dentistry, University of Lahore, Lahore, PB, Pakistan; 2Islamic International Medical College, Riphah International University, Rawalpindi, PB, Pakistan
Correspondence: Sundus Iftikhar, 26-C extension DHA Phase 8 ex-Parkview, Lahore, Pakistan, Tel +923457363111, Email [email protected]
Purpose: Despite being in high numbers in medical colleges, only a small proportion of women join the workforce and even fewer reach leadership positions in Pakistan. Organizations like United Nations and Women Global Health are working towards closing the gender gap. The study aims to explore the enablers and barriers for women in healthcare leadership and to explore the strategies to promote women in leadership positions in Pakistan’s specific societal culture.
Methods: In this qualitative exploratory study, semi-structured interviews of 16 women holding leadership positions in the health-care profession, ie, medical and dental (basic or clinical sciences) were included. The data were collected until saturation was achieved. The data were analyzed in MS Excel. Deductive and Inductive thematic analysis was done.
Results: Thirty-eight codes were generated that were combined in the form of categories. The major themes that emerged from the data were: elevating factors, the shackles holding them back, let us bring them up and implicit bias. Elevating factors were intrinsic motivation and exceptional qualifications, while the shackles were related to gender bias, male insecurities, and lack of political background. It was noteworthy that differences in gender roles were highly defined by culture and religion.
Conclusion: There is a need to change the perception of South Asian society and redefine gender roles through media and individual attempts. Women must take charge of their choices and believe in themselves. The institutional policies to help promote gender equality would be mentorship programs for new faculty, gender-responsive training for everyone, equal opportunities for all, and maintaining gender diversity on all committees.
Keywords: gender disparity, leadership in the health profession, gender roles in Pakistani society
Introduction
The number of female doctors around the world has increased in the last 50 years. For example, the percentage of women in medical schools in America has risen from 11.1% in 1970 to 47.8% by 2001 and from 25% in 1970 to a little over 50% by 2015 in Australia.1,2 Nowadays, girls are higher achievers than boys academically, and girls also make up 56% of students in A level taking biological sciences.3 This trend is not different in developing countries like India and Pakistan where it has been noted that nearly 70% of students in medical colleges comprise females.4
Despite being in high numbers in medical colleges, only a small proportion of these women join the workforce, particularly in South Asian countries.5 Several studies have been conducted to determine the reasons behind this fallout.4,6,7 One of the major causes of this fallout is the fixed gender roles in the society which expects the women to take care of the household while the men are expected to be the breadwinner for the family.4 This disparity in gender representation has been observed in several instances in the West, especially in leadership positions in medicine. In the US, it has been reported that women in high-level leadership positions (Medical school dean, department chair) remain scarce.8
In Pakistan, according to the list of private medical colleges issued by PMC (Pakistan Medical Commission), out of the 97 medical colleges, only 10 medical and dental colleges had a female deans/principal which makes only 10% of all colleges. Similarly, 22 (refer Figure 1) medical and dental colleges that were surveyed at the beginning of this study showed a huge disparity in the ratio of males and females at leadership positions.
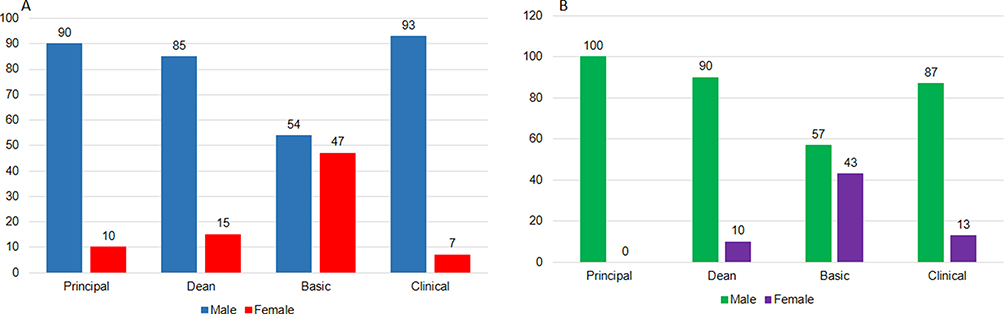 |
Figure 1 Percentage of females and males at senior leadership posts in (A) MBBS and (B) BDS colleges in Pakistan (n = 22). |
A good leader in healthcare should be approachable by welcoming the team members to voice their opinions while at the same time he or she should be able to balance autonomy and accountability. All of this should be carried out by prioritizing patient care and safety.9 Apart from identifying the qualities required to be an effective leader, the role of gender differences in leadership has also been debated for a long time. Research has shown that there are differences in the performance of men and women as leaders, especially with respect to their leadership styles. Men are mostly perceived as task-oriented leaders who follow a more transactional leadership approach. Therefore, in order to be goal-oriented, they display certain characteristics that may come across as dictatorial to some.10 In contrast, women leaders are seen as relationship-oriented and follow a more transformational leadership approach. This means that they focus a lot on developing interpersonal relationships at work by showing concern for the well-being of the employees and including them in decision-making affairs.11 Literature has conflicting views on which type of leadership style predominantly improves the quality of healthcare. Some authors have suggested a transactional while others advocate a transformational style; however, there is a consensus that there should be a mixture of both styles in order to achieve the goals set up to improve the healthcare system including health-care education and patient care.12
Globally, it has been observed that there is an under-representation of women in leadership roles in specific specialties for example in plastic surgery and cardiology.13,14 Different approaches have been identified in the literature to address the under-representation of women. It was observed that although the opportunities existed, individuals required guidance and support in identifying those pathways. Different approaches have been identified in the literature to address the under-representation of women like creating a team of multidisciplinary mentors who would work together to assist women to strive for leadership positions.15 However, the factors identified from the literature may not hold true for Pakistan entirely due to cultural, social, and religious differences. It is evident from another study carried out in Pakistan in the education sector whereby, the stereotypes in the society induce prejudice against women in leadership positions.16
Hence, the aim of the study was to explore the factors, ie, enablers and barriers for health-care professions women leadership in Pakistan’s specific societal culture.
Methods
Study Design
This was a qualitative exploratory study designed to obtain in-depth knowledge about the experiences of women in leadership positions in the health-care profession. After getting ethical approval from the University of Lahore (ERC/81/21/12). The literature was reviewed thoroughly to develop the questions. The questionnaire included questions regarding the demographics of the participants, years of leadership experience, their career paths, the enabling, and hindering factors, the role of Pakistan’s societal culture in their professional progress, gender stereotypes, and the strategies that can be undertaken at the personal and institutional level to encourage women in leadership positions.
Setting and Participants
Purposive sampling was done to conduct semi-structured interviews of participants from all over Pakistan. A total of twenty women are contacted and sixteen responded and consented to be a part of the study. The women who did not respond were given a gentle reminder once only after which they were not contacted further. The target population in this study were women holding leadership positions in the health-care profession, ie, medical and dental, basic and clinical sciences. Leadership position refers to the principal of the institute, dean of the institute and Head of departments. These positions were chosen because in Pakistani medical colleges Dean, Principal or Head of Departments have the autonomy to make decisions. Therefore, the women currently working in these positions or had been working in these positions would be better able to give their perspective on what enabled them to reach this position or what hurdles did they face during their journey. They would be able to suggest how women can overcome these hurdles in Pakistani cultural context.
Ethical Approval
Ethical approval from Ethical Review Board of University of Lahore was obtained on 20/1/2022. Reference number: ERC/81/21/12. The study complies with the declaration of Helsinki. Written consent was obtained from the participants to participate in the study. The consent also contained permission to publish the results anonymously.
Tools
The interview was based primarily on the questions developed through literature review. However, follow-up questions or probing questions were also asked. The questions were shared with Medical Educationists who had worked in the field for at least three years. Six Medical Educationists gave their feedback on the questions. The feedback was incorporated and in the end the semi-structured interview broadly contained questions mentioned in Figure 2. (Detailed interview guide available as Supplemental File 1).
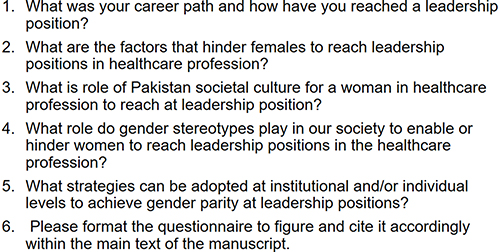 |
Figure 2 The questions used to conduct semi-structured interview. |
Data Collection Procedure
Initially, an e-mail or WhatsApp message was sent to the participant introducing the researcher and describing the study objectives briefly. The participants were informed that the study was a part of Master thesis. An explanation was also given as to why the participant was chosen for the study. After receiving an affirmative response, the participant was thanked and was asked for their availability for the interview. The participants were given a choice between online and face-to-face interview; ten participants opted for online interviews via Zoom. Similarly, participants’ preference of language was also taken into consideration and the interviews were conducted in both Urdu and/or English depending on their preference. E-signatures were taken on consent form by participants who had consented. Informed consent was taken by participants to participate in the study and to publish the results anonymously. The interviews were conducted by a female researcher (SI), as this was a part of the author’s thesis for Master in Medical Education. The researcher has prior experience in qualitative interviews and/or formal/informal training in communication skills. No other researcher was present during the interviews and none of them had a personal relationship with any of the participants. On average, the interview lasted from 25min to 40min. In order to obtain sufficient data, it was made sure that the interview was not less than 25min and similarly the interview was not stretched beyond 45min. The interview was not extended beyond 45min because the participants had busy schedules and a time-consuming interview could result in lesser participants consenting to give an interview. The main interview started after establishing an initial rapport with the participant. The interviewer took field notes during the interview to note down any change in expression or tone that seemed relevant. The interviews were recorded on a laptop using Camtasia software (TechSmith) for transcription afterward. A formal verbal consent with a clearly defined study purpose and permission to audio record was recorded before each interview. The information rendered by the participants was kept strictly confidential and the audio recording was shared only among the investigators of this study. The names of the participants were given codes to keep anonymity. No repeat interviews were carried out.
Data Collection and Analysis
The data was collected from February 2022 to March 2022. The data consisted of demographics (Table 1) and open-ended questions. In this study, women from three provinces of Pakistan were interviewed (Punjab, Sindh, and Khyber Pakhtunkhwa) and women from Punjab and Sindh mostly belonged to Lahore and Karachi, respectively.
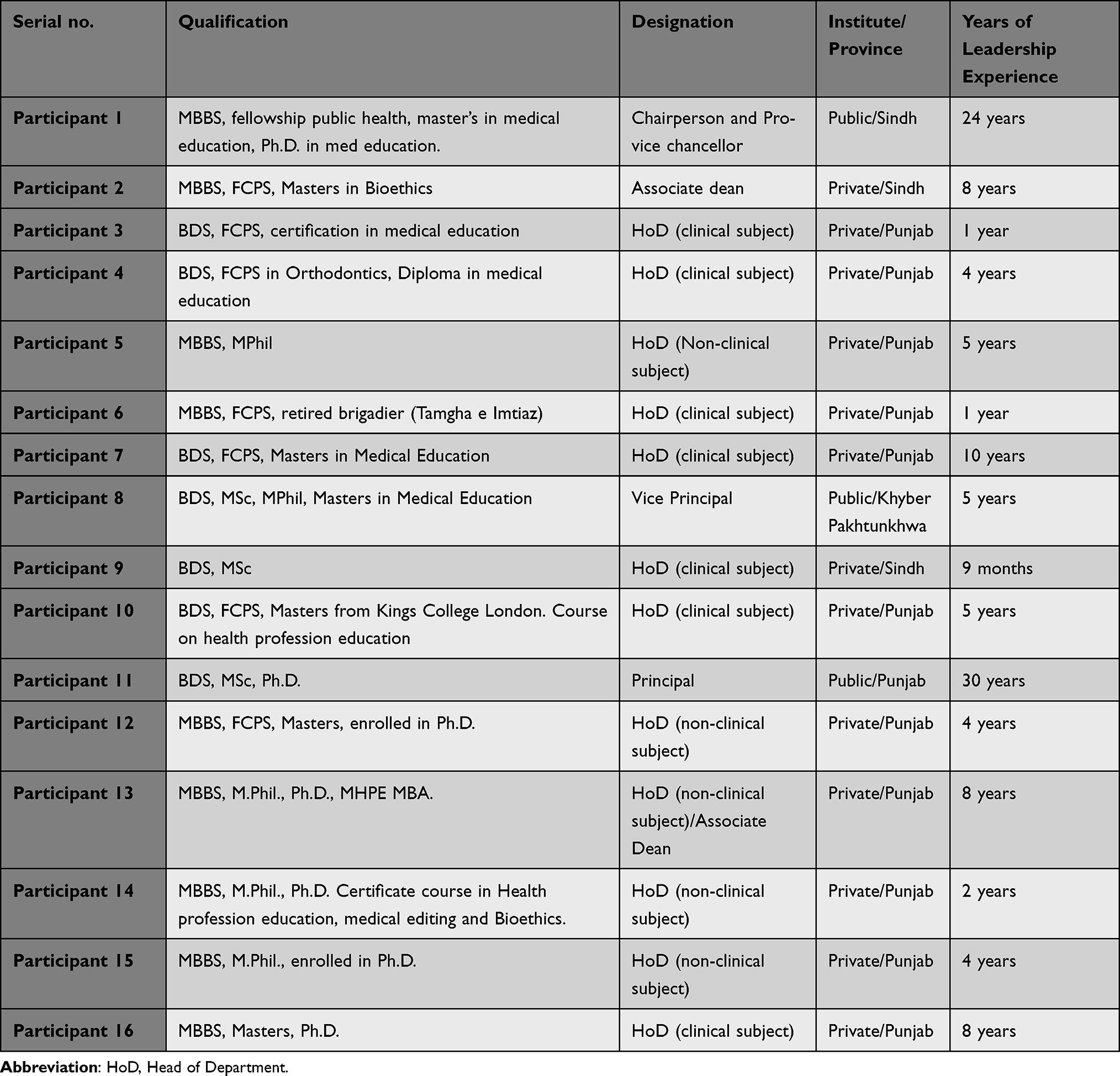 |
Table 1 Demographics of Participants |
The data collection and analysis were done side by side and data was collected until saturation was achieved, that is, no new information was rendered by the participants. Literature suggests that a sample size of 10 is adequate if a homogenous group of people are interviewed. Nevertheless, a sample size of 15–30 is considered appropriate for qualitative study except grounded theory.17 In this study, after interviewing 16 women, the authors felt that saturation has been achieved. The interviews were transcribed and then translated in English language. All the authors read the transcripts and discussed them among themselves. It was mutually decided to manually analyze the data. Since the interviews were done in both English and Urdu so the authors (SI, RY, RAK, MA) felt that the software might misinterpret some of the Urdu words and correct context will be lost. Some of the Urdu phrases were kept in Urdu to keep the context intact and to personalize the data. The transcripts were shared with the participants for member checking before conducting the analysis. Only one participant sent a few comments to add in the transcript. The suggestion was incorporated before initializing the analysis.
Tables were developed to handle a large amount of the gathered information (Supplement File 2). A backup of the entire data collected was made in Google drive to ensure the safety of the data. Deductive and inductive thematic analysis was done. All the authors went through the transcripts together and developed codes that were aggregated to form categories and similar categories were gathered to generate a theme. The results were based on the thematic areas identified during the initial phase of analysis. The role congruity theory was used as a theoretical framework.
Results
The following themes were developed through coding of the data:
- Theme 1: Elevating factors.
- Theme 2: The shackles holding them back.
- Theme 3: Let us bring them up.
- Theme 4: Implicit bias.
The researcher aimed to select participants from all over Pakistan. Table 1 provides the details of the participants.
Elevating Factors
The factors that propelled the women in health-care profession towards leadership positions were divided into their personal qualities, some of which were inherent, and others obtained over time with experience and qualification (Figure 3). The women believe that when their perseverance, enthusiasm and good communication skills combined with relevant opportunity it became a recipe for success. Women were also motivated by witnessing their colleagues and friends succeed in their professions. Participant 5 said:
When I saw my husband is in a very good position and when I assessed myself I wasn’t at that position as my colleagues were…At that stage when all these things came to me I was very depressed and thought I should do something.
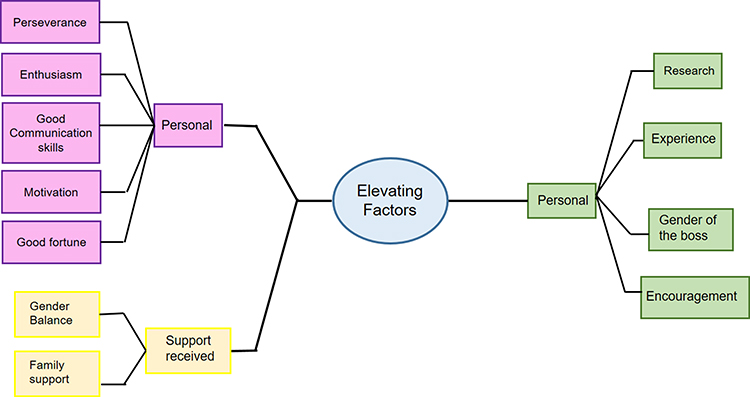 |
Figure 3 The factors that enabled women and elevated them to leadership positions in healthcare. |
Women also believed that to compete with men, they had to be ten steps ahead professionally. Most of the women credit their foreign experience and grants for their success as this made them stand apart and above their counterparts. Participant 11, with an overall experience of three decades (including principal and other administrative posts) in the health-care profession said:
Foreign experience (improved) my confidence, my skills, competency, and my research abilities. It also groomed me well.
It was seen that having a female boss was considered an impetus for many as Participant 2 claims:
My female boss allowed me to come half day a week. Male boss would not have understood that. Eight years I did that. During that time, I did masters in bioethics, developed training programs for anesthesia
It is noteworthy that participant 2 was aware that her institute believed in promoting gender parity hence this institutional value helped her to progress based on her credentials and regardless of gender.
University especially from the last three years has been promoting gender balance very vigorously. When I was applying for this post I had to give a lot of interviews and in those interview panels as well there were more female leaders than males. Participant 2
The Shackles Holding Them Back
It did not come as quite a shock when the women shared that the shackles that held women back from achieving were mostly related to their gender (Figure 4). Participant 1 shared her personal experience in the following statement:
I and all the men that were fighting for the position of vice chancellor, I beat them all they were not even close. The numbering was not fair if they had numbered everyone fairly my numbers would have been way higher than men at second and third positions…In medicine we are lucky that we have a fixed criteria for promotion but if a man and a woman is equally qualified then the position goes to the man.
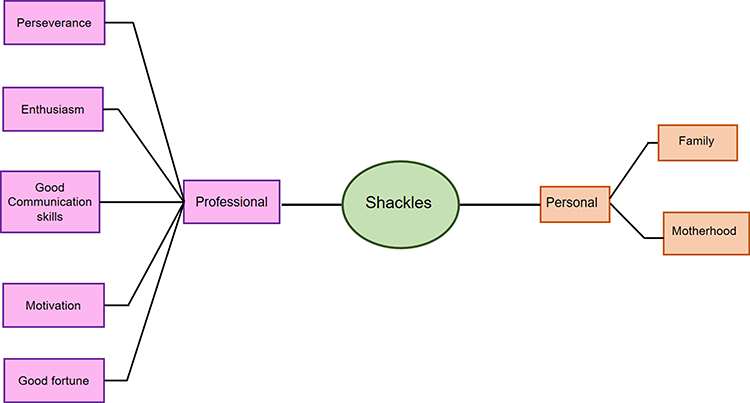 |
Figure 4 The factors that hindered women from reaching leadership positions in the healthcare system of Pakistan. |
Nobody would directly confess that they are biased towards one gender over the other; however, it is covertly a part of our workplace as explained by Participant 10:
…If the same thing the same point is said by a male faculty member even if he is the junior-most member of the department then that point is given more weightage than that of a woman even if she is the head of the department…
The women feel that men are insecure when they see a more qualified woman excelling in her career, so they tend to pull them down through different ways. A few women claim that they were not taken seriously during meetings and were not involved in decision-making process despite being in higher positions. If they dared to give their opinion, they were judged rather than acknowledged. Married women face more prejudice as people including supervisors question their commitment towards their profession. It is true that when unsupportive workplace is accentuated with the immense pressure of family commitments and motherhood, a lot of women give up and only a few get across. Participant 9 who commenced her post-graduation in middle age observed:
All those people whom I see in higher positions, have no family life. All my female classmates who became professors, all have broken marriages.
Even if the women reach the position of Head of Department, only a handful of them would strive for higher administrative positions. Women feel that in order to pursue these positions, one must have a strong political background and a lack thereof meant that women never even attempted to seek these positions. Some women believed that they themselves did not take the initiative to strive for these positions. Interestingly, Participant 12 had an explanation for this:
I’ve heard from my male colleagues saying that females don’t want to come to leadership positions because of their own personal preferences. I disagree with that because in our society females don’t make fully autonomous decisions. Whereas males are privileged. Even females at top positions don’t make voluntary decisions because they have to consider so many things. So, for a female, it’s not a fully autonomous or voluntary decision.
Let Us Bring Them Up
Several women shared what strategies they adopted to survive in the cut-throat system in which their gender was at a disadvantage. They also shared their recommendations for institutes to promote gender balance at leadership positions (Figure 5). In leadership positions, some women had to be more assertive while staying facilitative and accommodating simultaneously so that everyone takes them seriously. The women at leadership positions choose their battles wisely, by raising their voice in situations where it mattered the most and stayed quiet in situations where they thought it was futile. All of this made them more vigilant.
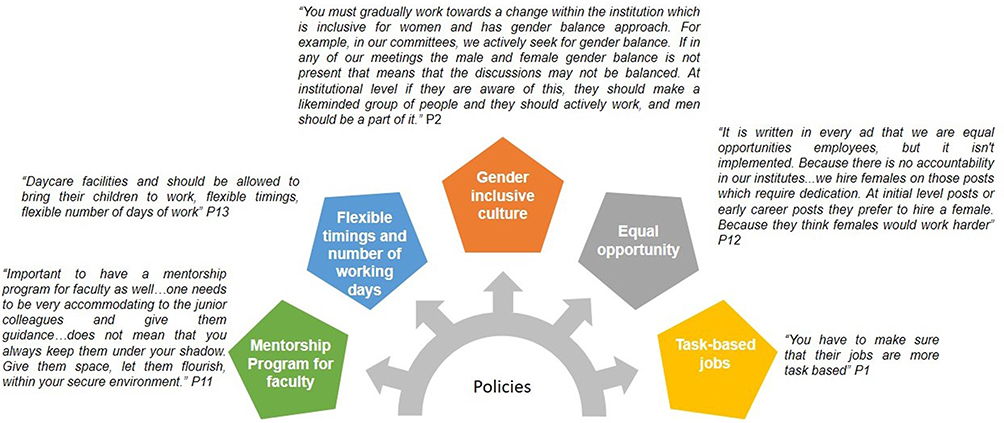 |
Figure 5 Recommendations by participants to promote gender parity at leadership positions on an institutional level. The text in italics shows the quotes by participants. |
It is suggested that
Women should make way for other women. (Participant 2)
Nearly all the women in the study explained how they support their juniors in research, and facilitate them by accommodating them during personal commitments, especially women. Junior colleagues are intentionally tasked with leadership roles in the departments ranging from obtaining their opinion in decision-making and designing assessments. The participants realized that it was necessary to train aspiring women for leadership tasks early in their career so that they are ready to deal with any situation in future. The participants also believed that women at workplace should be highly motivated, hard-working and should have a strong voice to counter workplace gender bias.
So, to counter these things every time I have put up a fight I have gone with evidence. This is what the literature is saying so if you are saying otherwise, prove it. That’s why they are mostly scared of me. Participant 1
Participant 10 had a piece of advice
One very important thing if someone tries to insult you publicly your first Instinct should be to remain silent…I know it is very difficult to maintain composure at that time but do maintain that composure because if you are successful in maintaining that composure then you have a chance at the second shot.
Implicit Bias
Culturally, the Pakistani society has rigid beliefs on gender roles, some of which are influenced by local interpretation of religion. Women in this study believe that culture has a lot of influence on religion in Pakistan that has resulted in these preconceived notions about the ability of men and women. Participant 8 explained:
They (men) feel that a woman is inferior. They twist Quranic verses in which Allah has made men the care provider, but they used it in such a way that a woman is impure and inferior. So, if someone they consider inferior comes at a leadership position or says something that they disagree with then they take it very personally. Workplaces will not improve as long as this mentality is prevalent. P8
Surprisingly, Participant 9, who herself was a Head of the Department, had widely contrasting views compared to the rest of the participants. She said:
I always believe that woman’s money is not a blessing. If the same chunk of money was brought by the woman and the same chunk of money brought by the man, then the man would run the whole house with it. This is one of my religious beliefs. P9
The gender roles depicting that women belong at home and men should be breadwinners and leaders are prevalent in all parts of the society. The women felt that the rigid stereotypical beliefs about gender roles affect workplace politics as well. The women are judged on their appearance, and they face character assassination.
Even if a girl goes to the front position, the people behind her start talking negatively about her so the other girls get scared too. They say she is a corrupt person. She has gone up through the wrong means. P9
The media plays a major role in mitigating or aggravating cultural beliefs. Nearly all the participants narrated different advertisements that they had seen which promoted gender equality. Participant 11 reiterated how in recent times, the media is taking responsibility and propagating gender equity than gender equality which is the need of the hour. This would mean that women are given fair ground to compete with their male counterparts.
The leadership styles have been perceived differently for men and women. Participants of the study believe that men are stricter and have better decision-making skills while women are more considerate towards their so their leadership style depends on their interpersonal relationships.
Discussion
Women working in the health-care profession have diverse personalities and individual journey. It is important to note what characteristics and opportunities enabled them to excel in their field to become leaders and how did they surpass the hurdles that they faced being a woman in personal and professional fronts.
At a personal level, the participants noted that their internal motivation played a great role in helping them achieve their goals. It was a triad of internal motivation, qualities that set them apart from their contemporaries like exceptional communication skills and opportunities that came with good fortune were very crucial in uplifting the women to leadership positions. Ellinas et al18 deduced that lack of women’s intrinsic motivation plays a major role in obstructing their pathway towards leadership positions.9 Our findings also reveal that women who have achieved leadership positions give credit to their intrinsic motivation and personal qualities. The motivation came from seeing their male peers excel in their fields.
On the professional front, several interviewees recognized that a vast array of experience and national and international research, as well as grants won by these women set them apart from others. Few of the women who had female supervisors or mentors stated that having female mentors made their journey easier. The other participants were of the opinion that having a mentor was important but not the gender of the mentor. Literature recognizes the importance of having a mentor and a supportive role model for aspiring females regardless of gender.19,20 The author believes that having a female mentor in our study was highlighted due to the cultural context. This is because in Pakistani society, women feel more comfortable sharing their issues and problems with women only and there is a communication barrier with the opposite gender. It is also observed through research that an increased number of women in leadership positions has resulted in increased awareness and encouragement of gender equity.19
One participant stated that her institute is consciously trying to promote gender equality, which is why she got the support needed to advance in her career. It is for this reason that international organizations like Women in Global Health and HeforShe movement of the United Nations, Global health 50/50, and the like are striving continually to encourage an inclusive environment within institutes which would close the gender gap at leadership positions.21
It is noteworthy that most of the challenges faced by the participants of this study on a professional level were related to their gender. The first type of response obtained from the participants was related to the implicit bias faced by women in the workplace. The women reasoned that Pakistani culture and religion have certain defined gender roles due to which people do not accept women in leadership roles. This is why men feel insecure when a more qualified and experienced woman is leading. Participants also highlighted that they are discouraged to give opinions in decision-making matters, and it is conveyed to them through indirect gestures and comments that it is due to their gender. Evidence shows that regardless of the post, whether nurse or physician, women are not taken seriously during decision-making. It affects their self-confidence and ultimately self-efficacy.22 A study conducted by Durand et al, explicitly shows that gender bias exists for leadership positions as women were seen as an ideal fit for the role of a follower so people do not see them as leaders. This is often ingrained in the minds of women as well and despite their qualifications and credentials, they see themselves in supporting roles.22 This was endorsed in this study by Participant # 2 who stated that in a medical college with only one female professor, the professor is given the role of announcer instead of being a part of the academic panel and the female professor obliges to this treatment stoically.
Gender bias is also noted when selecting a vice chancellor medical college principal. Lately, with fast-paced changes occurring in healthcare, it has become more commercialized hence there is a lot of political influence involved.23 Therefore, men are preferred and women who fulfill the criteria do not even apply for the position because they fear having no political background would adversely affect their performance and survival in the leadership position.
Women’s leadership ensures stricter monitoring and fewer embezzlements. Furthermore, gender diversity in decision-making positions invites heterogeneity of ideas.24 This evidence should be enough to advocate for gender parity in health-care fields as well; however, the healthcare research community should also present evidence-based benefits in order to encourage organizations to actively seek gender parity.
It is also noteworthy that when we talk about equal opportunities for all it does not mean the same opportunities. It means equal opportunity to excel by keeping in mind the liabilities that come with gender. Females are often preferred at mid-level positions because they are considered hard-working and good at following the leaders.25 This was further reiterated by participants # 4 and 7 who claimed that they have witnessed women being more hard-working and multi-tasking. Consequently, it is suggested that everyone in leadership positions must undergo gender-responsive training in order to create an inclusive environment where aspiring leaders would thrive regardless of gender.26
The gender roles defined by society are mostly influenced by religion and culture; this is why they are manifested in different ways across communities. A couple of women had worked in Karachi and Lahore as well. Through their individual experiences, it was observed that Karachi was slightly more accommodating to women in the workplace as gender stereotyping was not too obvious. The reason cited by one of the participants was that since Karachi has multi-ethnicities, the people are more accommodating towards differences in lifestyles, beliefs, and cultures. No direct link between gender discrimination was found in multi-ethnic cities in the literature. However, a study conducted in the Russian context found that ethnic discrimination was considerably less in multi-ethnic societies.27 A relationship between gender and multi-ethnicity is yet to be determined. One of the gender stereotypes most commonly noticed in Pakistani culture is that professional women are expected to dress up and act in a certain way. They are expected to stay submissive, not interact much with the opposite gender, not apply much make-up and dress up in neutral colors. This becomes a challenge for women who do not conform to these stereotypes as they are then targeted specifically, and their moral values and character is questioned in the workplace. This falls under the category of workplace bullying, a vicious cycle that affects the mental, emotional, and physical health of the victim and adversely affects their productivity at work.28 Research conducted in the Pakistani context unsurprisingly concluded that women were bullied more in workplace than men. More importantly, it was seen that women were bullied over their clothing, demeanor, and moral values, while men were bullied over their performance and efficiency at workplace.29
Limitations of the Study
The limitation of this study is that sixteen women were interviewed. A larger number of women could have been included in the study and women belonging to smaller cities should have been approached as well. In this study, women working in big cities like Lahore, Islamabad, Abbottabad, and Karachi were included. A representation from Balochistan could also have benefitted the study. This study only explored the perception of women regarding gender roles in Pakistan. The perception of men was not explored since it was beyond the scope of this study. Perception of men should also be explored to completely understand thinking of the society.
Future Directions
It is recommended that a conscious effort should be made by the accrediting bodies to address the gender disparity in leadership positions. It may be done by encouraging institutes to have a formal mentorship program for the faculty so that potential health-care leaders are identified early on in their career. To deal with gender bias at workplace, it is crucial that an inclusive institutional culture is developed where gender bias is not be tolerated. One way of doing it is by conducting seminars and workshops where faculty is trained to tackle their inherent biases. Unconscious bias trainings should be made mandatory for the faculty. The medical institutes should provide the option of flexible working hours and part-time job for the faculty. The institutes should ensure gender balance is not completely off in academic activities. Women should have representation in discussion panels, as keynote speakers in conferences and as members of decision-making committees.
Conclusion
If Pakistan needs gender diversity at leadership positions in healthcare, certain strategies must be adopted by individuals and institutes. At the institutional level, like-minded people, especially men in leadership positions should be involved to ensure that women deserving women are visible in leadership positions. A structured mentorship program can be developed for aspiring women. Tasks especially designed to train young faculty for leadership roles should be given to men and women equally. One way to ensure diversity in leadership positions is to start at the lowest level and ensure gender diversity in all committees so that there is diversity in point of view.
Acknowledgments
The authors would like to thank Dr. Abdul Samad Khan and Dr Sarosh Saleem for their help and guidance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chambers C, Ihnow S, Monroe E, Ls- JBJS. Women in orthopaedic surgery: population trends in trainees and practicing surgeons. J Bone Joint Surg. 2018;17:e116.
2. Bismark M, Morris J, Thomas L, Loh E, Phelps G, Dickinson H. Reasons and remedies for under-representation of women in medical leadership roles: a qualitative study from Australia. BMJ Open. 2015;5(11):11. doi:10.1136/bmjopen-2015-009384
3. Thompson J. Male and female participation and progression in higher education: further analysis Part 1: employment outcomes; 2010. Available from: https://www.hepi.ac.uk/wp-content/uploads/2014/02/48-Gender-further-analysis-full.pdf.
4. Moazam F, Shekhani S. Why women go to medical college but fail to practise medicine: perspectives from the Islamic Republic of Pakistan. Med Educ. 2018;52(7):705–715. doi:10.1111/medu.13545
5. Nagarajan R. More women study medicine, but few practice. The times of India - google search. Times of India; 2016. Available from: https://www.google.com/search?q=More+women+study+medicine%2C+but+few+practice.+The+Times+of+India&rlz=1C1CHBF_enPK915PK915&oq=More+women+study+medicine%2C+but+few+practice.+The+Times+of+India&aqs=chrome.69i57.554j0j4&sourceid=chrome¡UTF-8.
6. Masood A. Influence of marriage on women’s participation in medicine: the case of doctor brides of Pakistan. Sex Roles. 2019;80(1–2):105–122. doi:10.1007/S11199-018-0909-5
7. Mohsin M, Syed J. The missing doctors—an analysis of educated women and female domesticity in Pakistan. Gend Work Organ. 2020;27(6):1077–1102. doi:10.1111/gwao.12444
8. Lautenberger D, Raezer C, Bunton S. The underrepresentation of women in leadership positions at U.S. medical schools | AAMC. AAMC Anal Br. 2015;15(2):1–2.
9. van Diggele C, Burgess A, Roberts C, Mellis C. Leadership in healthcare education. BMC Med Educ. 2020;20(Suppl 2):1–6. doi:10.1186/s12909-020-02288-x
10. Eagly AH, Johannesen-Schmidt MC, Van Engen ML. Transformational, transactional, and laissez-faire leadership styles: a meta-analysis comparing women and men. Psychol Bull. 2003;129(4):569–591. doi:10.1037/0033-2909.129.4.569
11. Merchant K. How men and women differ: gender differences in communication styles, influence tactics, and leadership styles. C Sr Theses. 2012;2012:1.
12. Sfantou DF, Laliotis A, Patelarou AE, Sifaki-Pistolla D, Matalliotakis M, Patelarou E. Importance of leadership style towards quality of care measures in healthcare settings: a systematic review. Healthc. 2017;5(4):1–17. doi:10.3390/healthcare5040073
13. Carnes M, Noel Bairey Merz C. Women are less likely than men to be full professors in cardiology: why does this happen and how can we fix it? Circulation. 2017;135(6):518–520. doi:10.1161/CIRCULATIONAHA.116.026671
14. Chen W, Baron M, Bourne DA, Kim JS, Washington KM, De La Cruz C. A report on the representation of women in academic plastic surgery leadership. Plast Reconstr Surg. 2020;145(3):844–852. doi:10.1097/PRS.0000000000006562
15. Coe C, Piggott C, Davis A, et al. Leadership pathways in academic family medicine: focus on underrepresented minorities and women. Fam Med. 2020;52(2):104–111. doi:10.22454/FamMed.2020.545847
16. Samo AH, Qazi SW, Buriro WM. Labelling them is negating them: a phenomenological study of stereotypes and followers’ experiences about women leadership in Pakistan. Manag Res Rev. 2019;42(3):391–411. doi:10.1108/MRR-04-2018-0170
17. Boddy CR. Sample size for qualitative research. Qual Mark Res. 2016;19(4):426–432. doi:10.1108/QMR-06-2016-0053
18. Ellinas EH, Fouad N, Byars-Winston A. Women and the decision to leave, linger, or lean in: predictors of intent to leave and aspirations to leadership and advancement in academic medicine. J Womens Health. 2018;27(3):324–333. doi:10.1089/jwh.2017.6457
19. Mousa M, Boyle J, Skouteris H, et al. Advancing women in healthcare leadership: a systematic review and meta-synthesis of multi-sector evidence on organisational interventions. EClinicalMedicine. 2021;39:101084. doi:10.1016/J.ECLINM.2021.101084
20. Boylan J, Dacre J, Gordon H. Addressing women’s under-representation in medical leadership. Lancet. 2019;393(10171):e14. doi:10.1016/S0140-6736(18)32110-X
21. Jovanovic A, Wallace JE. Lean on me: an exploratory study of the spousal support received by physicians. Psychol Health Med. 2013;18(5):543–551. doi:10.1080/13548506.2013.765018
22. Durand F, Bourgeault IL, Hebert RL, et al. The role of gender, profession and informational role self-efficacy in physician – nurse knowledge sharing and decision-making knowledge sharing and decision-making. J Interprof Care. 2022;36(1):34–43. doi:10.1080/13561820.2021.1890006
23. Dle Zulueta PC. Developing compassionate leadership in health care: an integrative review. J Healthc Leadersh. 2016;8(1). doi:10.2147/JHL.S93724
24. Chisholm-Burns MA, Spivey CA, Hagemann T, Josephson MA. Women in leadership and the bewildering glass ceiling. Am J Health Pharm. 2017;74(5):312–324. doi:10.2146/ajhp160930
25. Braun S, Stegmann S, Hernandez Bark AS, Junker NM, van Dick R. Think manager—think male, think follower—think female: gender bias in implicit followership theories. J Appl Soc Psychol. 2017;47(7):377–388. doi:10.1111/jasp.12445
26. Dhatt R, Thompson K, Lichtenstein D, Ronsin K, Wilkins K. The time is now - a call to action for gender equality in global health leadership. Glob Health Epidemiol Genom. 2017;2:1–4. doi:10.1017/gheg.2017.1
27. Bessudnov A, Shcherbak A. Ethnic discrimination in multi-ethnic societies: evidence from Russia. Eur Sociol Rev. 2020;36(1):104–120. doi:10.1093/ESR/JCZ045
28. MacIntosh J, Wuest J, Gray MM, Aldous S. Effects of workplace bullying on how women work. West J Nurs Res. 2010;32(7):910–931. doi:10.1177/0193945910362226
29. Tariq Q. Role of popularity in being bullied at the workplace. Pak Bus Rev. 2012;13(4):367–378. doi:10.35826/ijoecc.125
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.