")
Back to Journals » International Journal of General Medicine » Volume 17
Awareness, Attitude, and Fertility Desire in Elective Oocyte Cryopreservation of Adults in Four Areas of China
Authors Xie Y , Liao C, Zhai X
Received 29 November 2023
Accepted for publication 27 March 2024
Published 2 April 2024 Volume 2024:17 Pages 1281—1292
DOI https://doi.org/10.2147/IJGM.S449573
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sandul Yasobant
Yijing Xie,1 Chenge Liao,2,* Xiaomei Zhai1,*
1School of Population Medicine and Public Health, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 2School of Rehabilitation Medicine, Binzhou Medical University, Yantai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chenge Liao, School of Rehabilitation Medicine, Binzhou Medical University, 346 Guanhai Road, Laishan District, Yantai, People’s Republic of China, Email [email protected] Xiaomei Zhai, School of Population Medicine and Public Health, Chinese Academy of Medical Sciences & Peking Union Medical College, No. 31, 3 Tiao, Bei-Ji-Ge Street, Dongcheng District, Beijing, People’s Republic of China, Email [email protected]
Purpose: Controversy exists on whether or not elective oocyte cryopreservation (eOC) can be conducted in public hospitals in China. Policymakers should take into account the benefits and risks in the Chinese population. This study explored basic data concerning the awareness, attitudes of eOC, and fertility desire of eOC in China to offer evidence for policy making.
Methods: A total of 442 people in four areas of China responded to a survey. The questionnaire was divided into three parts: awareness, attitude, and fertility desire of eOC. Descriptive analysis and multivariable regression analysis were used in the study.
Results: Generally, the respondents had a positive or neutral attitude towards eOC. However, about 90% of respondents did not know the cost of eOC. In general, a more positive attitude was found towards eOC among participants who had heard of the procedure compared with those who had not. Most women did not desire to reproduce by eOC. After adjusting for access to information, we found that female, older age groups, and singles were more likely to have increased awareness than their counterparts. The awareness of participants who accessed information from any source had a higher relative probability of having good awareness levels compared to participants who had not accessed the information. Undergraduates exhibited significantly higher levels of cognitive understanding, as indicated by their increased familiarity and comprehension, compared to high school students (relative risk ratio = 1.44, confidence interval = 0.48,4.29).
Conclusion: Continued discussion is needed regarding the ethical, legal, and social aspects of performing eOC in public hospitals. Furthermore, policies are needed to regulate eOC to protect the reproductive freedom of healthy women.
Keywords: elective oocyte cryopreservation, awareness, attitude, fertility desire
Introduction
Oocyte cryopreservation (OC) was first reported in 1986 by vitrification, which is a freezing process. Oocyte resuscitation is conducted before fertilization. Fertilization is accomplished by intracytoplasmic sperm injection that develops into an embryo. The embryo is then transferred into the uterus after a certain stage.1–3 Initially, OC was used for medical reasons. Medical OC is indicated for patients receiving gonadotoxic therapies for cancer or genetic conditions or failure to obtain sperm for in-vitro fertilization (IVF) or for someone unable to cryopreserve embryos.4 Medical OC is suitable for fertility preservation in women who suffer from chemotherapy or radiotherapy. Medical OC is also good for infertility with IVF or women who suffer ovarian dysfunction.5,6 Later, target populations for OC were extended to healthy women, which is called social egg freezing or elective OC (eOC).7 Healthy women in many countries, such as Israel, the United Kingdom, the United States, and Japan, are allowed to freeze their eggs for eOC.8–10 However, ethical debates surround eOC regarding safety, effectiveness, and reproductive rights.11–13 Philosophers and ethicists have differing opinions about autonomy. According to Beauchamp’s opinion, if people do not understand the action, the action is not autonomous.14 The current study aimed to explore whether or not the public understands eOC. In China, the practice of eOC is still very controversial. Some researchers believe that eOC should be allowed in China in the near future because it would benefit the fertility rate and it preserves female autonomy from an ethical perspective.15 Some think related policies and legislation should be established to help women conduct eOC in the future.16 Prof. Xiaomei Zhai, who is the eminent ethics expert of China, has shown concern over some of the ethical issues of conducting eOC in public hospitals. We need more evidence to know whether or not the public in China has knowledge of eOC well before they use it. These controversies stem from a famous eOC case in China.
In December 2018, a single 30-year-old woman sought oocyte cryopreservation services at a hospital in Beijing. The results of various health examinations showed she was in good health and met the needs of egg freezing. However, the hospital refused to provide egg freezing services because she was unmarried and the procedure was not for medical purposes. She then sued the hospital.17 She claimed the hospital’s behavior was a kind of stigma for women, and it was a violation of her general personal rights. According to the third article of the Administrative Measures for Human Assisted Reproductive Technology (ART),18 which is promulgated by the Ministry of Health, the application of human ART should be carried out in medical institutions for medical purposes and in accordance with the national family planning policy, ethical principles, and relevant legal provisions. The hospital argued in court that the hospital cannot conduct eOC for her. In July 2022, the court dismissed all of her claims. The woman appealed the court’s decision. To date, the court has not issued a ruling. This case has sparked a broad discussion concerning bioethics among the legal and medical experts in China.
Actually, this was not the first event to arouse discussion on eOC in China among the scholars. In 2018, Trip.com Group, a travel service conglomerate formerly known as Ctrip.com International Ltd., offered eOC to female employees to be performed abroad as an employee benefit, which triggered a heated discussion in China. The head of the travel company thought eOC was a good business strategy to encourage fertility. Nevertheless, the fee for eOC was around 200,000 CNY (approximately USD27,800) by users; therefore, only middle and higher class female employees could take advantage of this offer. This employee benefit was similar to the policies of Facebook and Google.19,20 In any case, it was criticized by bioethics experts in China. Whether women are the real beneficiaries of eOC is questionable. This type of incentive creates a hidden motive to keep employees working. This technology may encourage women to put their career ahead of their family, which may unduly influence the reproductive choices of women, especially professional women.
In March 2023, the relevant departments of the National Health Commission called for opinions of the experts to obtain more evidence on allowing single women to participate in the eOC procedure. Data was needed on the likely consequences of eOC for developing sound policies. Such questions are as follows: Does the public have sufficient knowledge about eOC before agreeing to use it? And what is the public attitude towards this technology? To answer these questions, it is crucial to explore the existing knowledge, attitude towards eOC technology as well as their needs and desirability of using it. The answers are important for policy-makers in developing a strategy and future policy direction for this technique. Therefore, this paper aims to explore the awareness, attitude, and fertility desire of eOC in China.
Materials and Methods
Study Design and Study Setting
This was a cross-sectional study conducted from June to August 2022. The aim of this study was to obtain some very basic data about the attitudes of people towards eOC in China. Through purposive sampling, we selected populations from the northwest, northern, eastern, and southern parts that covered five provinces of China. The provinces of Inner Mongolia, Shandong, Beijing, Hunan, and Fujian were included in our research. Inner Mongolia is an autonomous region in the northwest of China that is populated by an ethnic minority of China. Beijing is in the northern part of China and is the capital of China. Shandong Province belongs to the eastern part of China that is a relatively well-developed province. Hunan and Fujian provinces are in the southern part of China. The geographic variable was categorized into two groups: the high economic group of the North and Northwest regions and the low economic group of the East and South regions.
Study Population
The study recruited people who were ≥18 years old who could access the internet and were able to read the questionnaire.
Sample Size Calculation
The sample size was calculated based on the 71.8% proportion of participants desired to undergo OC, using infinite population proportion formula.21 At least 341 respondents were required considering the 20% non-response rate.
Questionnaire Development
We designed the questionnaire according to issues raised in the literature on eOC.22,23 It was reviewed by two obstetrics and gynecology (OBGYN) specialists to find out whether the items covered or missed certain components of the objectives. One expert co-specialized in epidemiology and OBGYN research for many years, and the other expert specialized in ART and was experienced in fertility consultation. In the first part of the questionnaire, we provided information about the survey and asked potential participants to join the survey. If they completed the questionnaire, we regarded that as their consent to participate in the survey. We did not ask for any identifying information; therefore, the collection was anonymous.
There were three domains in the questionnaire: (1) awareness among the respondents regarding eOC; (2) attitudes of respondents towards eOC; and (3) the desire among female respondents towards using eOC for reproductive purposes (Figure 1). Three items were under the awareness domain: (1) hearing of eOC; (2) how they heard about eOC; and (3) knowing the cost of eOC. Seven items were under the attitude domain: (1) whether eOC is bad for women’s health; (2) whether eOC is bad for the fetus’s health; (3) whether they agreed that women without cancer or infertility should be allowed to use eOC in China; (4) whether they agree that unmarried women should be allowed to use eOC; (5) whether they agree that the government needs to make a policy for using eOC in China; (6) whether they agree that women’s rights are violated when eOC is not allowed in China; and (7) the attitude of men towards his partner using eOC. Five items were under fertility desire: (1) fertility desire by eOC; (2) for the reason of having no partner; (3) because of unstable relationships; (4) for job reasons; and (5) for the reason of unstable financial status.
 |
Figure 1 The questionnaire development. Abbreviation: eOC, elective oocyte cryopreservation. |
Data collection procedure
Snowball sampling was used for this survey. Due to the zero-case COVID-19 policy in China at the time of this survey, the questionnaire was prepared in the Wen Juan Xing application and shared with potential participants using a WeChat account. We recruited the first group of participants and requested them to invite other potential participants among their friends and continued the procedure until we got the desired sample size of 442 participants.
Statistical Analysis
The provinces included in our research were Inner Mongolia, Shandong, Beijing, Hunan, and Fujian. Given that Inner Mongolia is a developing region of China, while the other provinces are developed areas, we stratified these five provinces into two categories: one category comprised the participants from Inner Mongolia as a developing area, and the others included Beijing, Shandong, Hunan, and Fujian Provinces as representatives of developed areas.
In the domain of attitudes, we employed standard 5-level Likert scales. The first two questions asked the participants to rate their agreement on a scale from 1 to 5, where 1 represented “strongly agree”, 2 denoted “agree”, 3 indicated “neutral”, 4 signified “disagree”, and 5 corresponded to “strongly disagree”. A response of strong disagreement for these initial questions implied a positive attitude towards the eOC concept. Conversely, for the remaining four questions, the scores ranged from 5 to 1 where higher values indicated stronger agreement and lower values represented disagreement or opposition. We analyzed the question regarding the attitude of men towards using eOC independently due to missing female data that could not be included in the dataset. The total scores derived from these six items were then categorized into high, medium, and low grades based on quartiles.
The statistical analysis was performed using R version 4.2.1. All hypothesis tests were conducted with a two-sided significance level of α = 0.05. A one-way analysis of variance (ANOVA) was employed to compare multiple groups, and a post hoc least significant difference test was conducted for pairwise comparisons if significant differences were found in the ANOVA results. Non-normally distributed measurement data were represented by median (interquartile range), and group comparisons were analyzed using the H-test for independent samples. The Chi-square test was used to analyze categorical data. Independent variables significantly associated with awareness, attitude, and fertility desire on eOC (p-value < 0.05) were further adjusted in the multivariable regression models. Additionally, the effect of different age groups, marital status, and economic disparity by region were controlled in the final regression regardless of their association in the Chi-square test analysis.
Multinomial regression was employed to identify the factors associated with awareness and attitude levels as indicated by adjusted relative risk ratios. Binary logistic regression was utilized to determine the factors associated with female fertility desire reported as odds ratios. A likelihood ratio test with a p-value < 0.05 was considered significant for binary logistic regression, while the Wald test was used to ascertain significance in the multinomial regression model.
Reliability and validity testing of all domains showed Cronbach’s α = 0.72, KMO = 0.68, and Bartlett’s ball test p < 0.001. The reliability and validity test results of the awareness domain showed Cronbach’s α = 0.6, KMO = 0.55, and Bartlett’s ball test p < 0.001. Reliability and validity testing of the attitude domain showed Cronbach’s α = 0.71, KMO = 0.69, and Bartlett spherical test p < 0.001. Reliability and validity testing of the desire domain showed Cronbach’s α = 0.62, KMO = 0.64, and Bartlett’s ball test p < 0.001.
Results
A total of 442 respondents participated in this survey with 183 (41.4%) males and 259 (58.6%) females. Among them, 207 (46.8%) were from the northwest region of China, 105 (23.8%) from the northern part, 91 (21.3%) from the northeast, and 36 (8.1%) from the southern region. The average age of all participants was 39.3 years old. Approximately half of the participants were 18–34 years old, which accounted for 45.5% of the total sample size. One hundred and four participants were 35–45 years old, while 137 participants were >45 years old. More than half of the respondents had completed high school education or higher. Furthermore, 67.6% of participants reported being married or living with partners (Table 1).
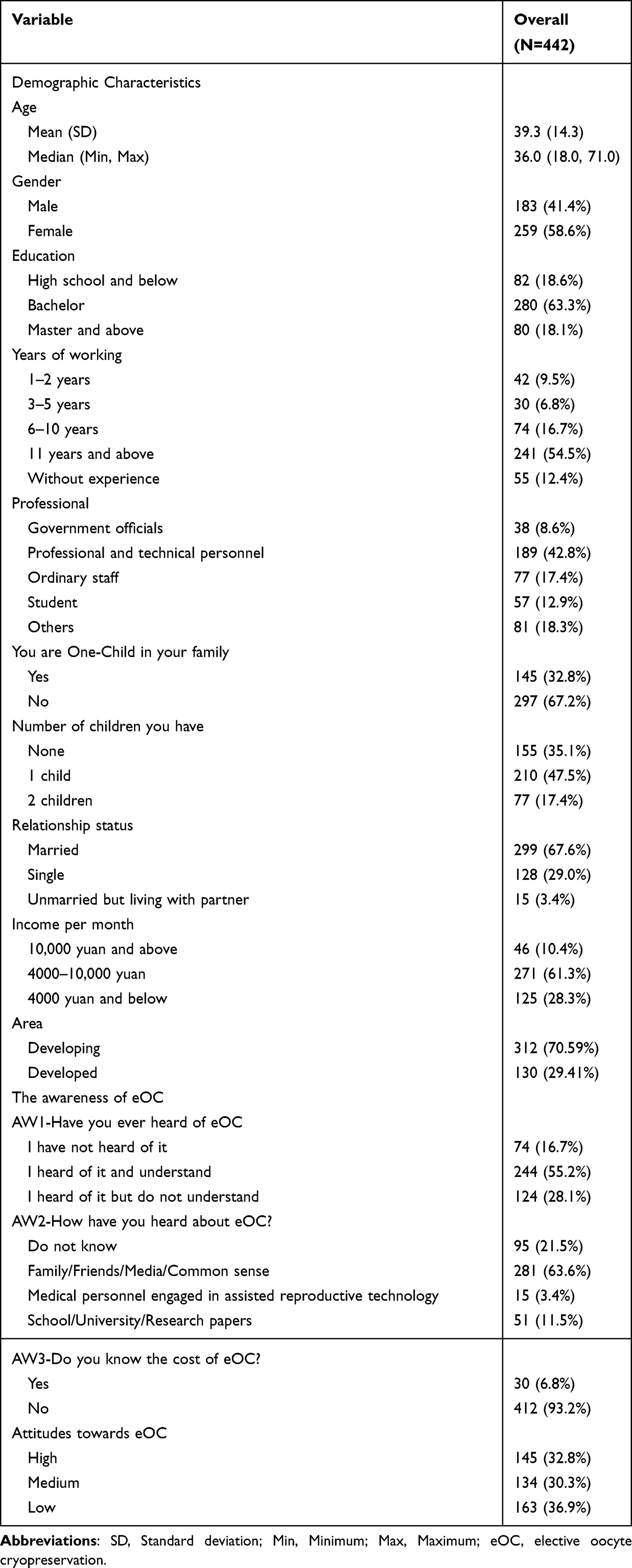 |
Table 1 General Information of the Study |
Out of all respondents, 244 (55.2%) were familiar with and comprehended the concept of eOC (Table 2). A significant number of respondents (281 [63.57%]) acquired knowledge of eOC from their family, friends, or the media. However, despite being aware of eOC, a majority of respondents 368 (93.21%) lacked knowledge on the cost of eOC. Table 3 provides the answers to various statements about respondent attitudes towards eOC.
 |
Table 2 Distribution of Awareness of Elective OC |
 |
Table 3 Distribution of Attitude Towards Using Elective OC for Reproduction |
The overall trend indicated that respondents generally hold a positive or neutral attitude towards eOC. For instance, 264 (59.73%) respondents strongly agreed or agreed that women without cancer or infertility should be permitted to utilize eOC in China. Similarly, 247 (55.88%) respondents strongly agreed or agreed that unmarried women should have access to eOC. Furthermore, 209 (47.29%) respondents strongly agreed or agreed that the government should establish policies regarding the use of eOC for reproductive purposes. When specifically addressing male participants, the majority also expressed either a neutral stance or a positive outlook on their partners utilizing eOC.
Table 4 presents data on the inclination of respondents towards fertility desire by eOC. The majority of women expressed no desire to reproduce through eOC with only 51 respondents answering affirmatively to this question. Among these 51 women, reasons cited included a lack of a partner (22), unstable relationships (7), and job or financial constraints (18).
 |
Table 4 Women Fertility Desire Using Elective OC |
Table 5 presents the distribution of attitudes, stratified by awareness of eOC. We combined the responses of “I heard of it but do not understand” with “I have not heard of it” to form the “no group” to capture individuals who possessed some knowledge and understanding about the procedure. Among the respondents, 244 were aware of OC, while 198 were not. Overall, individuals who had prior knowledge exhibited a more positive attitude towards eOC compared to participants without awareness. The majority of responses in the group with limited knowledge about eOC were neutral.
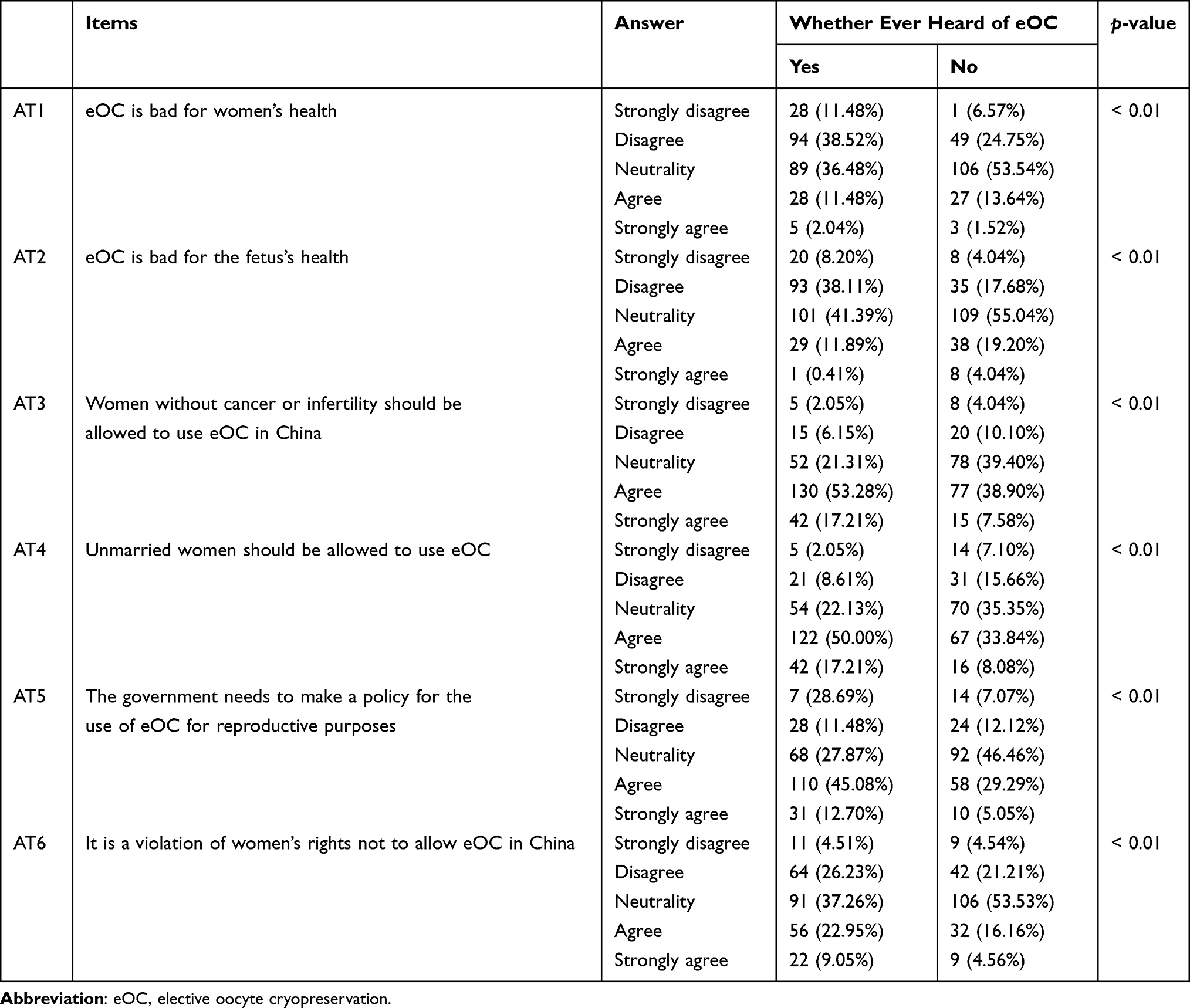 |
Table 5 Distribution of Attitude Stratified by Awareness Whether Ever Heard of Elective OC |
By conducting a Chi-square analysis, we identified the variables that exhibited statistical significance in relation to awareness. However, no significant differences in awareness were found among different age groups (see Supplementary Table 1). Subsequently, a multinomial regression model was constructed. The dependent variable was whether or not participants had heard of eOC where “I did not hear of eOC” was the reference category. The independent variables were gender, education level, presence of one child in the family, and region. Furthermore, a stratified analysis was performed based on gender (Table 6). After controlling for access to information, the analysis found that being female, older age groups, and being single had greater likelihoods of increased awareness than their counterparts. The awareness of participants who accessed information from any source had a higher relative probability of having good awareness levels compared to participants who did not access the information. The effect of access to information stratified on different genders could not be done due to the small sample size. Undergraduates exhibited significantly higher levels of cognitive understanding, as indicated by their increased familiarity and comprehension, compared to high school students (relative risk ratio = 1.44, confidence interval = 0.48,4.29). The level of eOC awareness was higher among participants who were the only child in their families regardless of gender.
 |
Table 6 Multinomial Regression for Factors Associated with Awareness of Elective OC |
The dependent variable was set as the attitude towards eOC, with positive attitude serving as the reference. Gender, parental status, monthly income, region of residence, awareness of eOC, source of knowledge about eOC, and knowledge of the cost of eOC were included as independent variables (Supplementary Table 2). Multinomial regression analysis revealed no significant differences in attitudes (Supplementary Table 3).
Supplementary Table 4 shows that females who have a higher number of children had higher intention of fertility desire compared to those without having child
Discussion
Currently, the acceptability of eOC is an ongoing discussion in China.17,24,25 At the same time, discussions are being conducted on how the health care system should deal with ART in general, and more specifically, whether it should be covered by public health insurance. Sound ART policies in general, and OC policies in particular, will need to be based in part on the estimates of the demand for these services and the attitudes among population groups towards reproductive technologies. The results of this study may contribute to the development of a sound policy in China.
The data in our study generally showed a quite positive attitude towards eOC among the participants surveyed in this study. Only about 10% thought eOC should not be allowed, and only 15% thought that unmarried women should not be allowed to use it. However, it is also clear that nearly half of participants did not know or did not understand the details of the eOC procedure. The relationship between risk perception and attitude is complicated. Some researchers concluded that a negative relationship exists between knowledge and risk perception.26 In this current study at least, limited knowledge of eOC indicated the participants could not understand the risk of eOC, which may mislead one’s attitude. Further research to explore the relationship of awareness and risk perception of eOC may be warranted. The government, media, and special institutions of China should fully inform citizens on the risks of eOC because this technology may bring biological risks to individuals such as ovarian hyperstimulation syndrome.27,28 When a woman freezes her eggs for a long period to be used at an older age, she faces the same risks as women who become pregnant at an older age.29,30
We should also note that in our study, there was very little knowledge on the cost of eOC. Based on data from other countries, eOC is quite expensive. In the UK, women pay £2800–3900 per ovulation promotion cycle and £330–1345 for a follow-up visit plus consultation fees. The cost of egg freezing is calculated separately according to the freezing time.31 Cost-effective analysis of eOC or medical OC in China is lacking. There is insufficient evidence to help policy makers alter the current policy.
Although the use of eOC requires medical technology, it is not a therapeutic procedure, and it may be expensive. Furthermore, eOC does not fall under the category of basic medical services. The principles of health allocation are to make health resources available to the vulnerable and to patients who need health resources to save or prolong life.32,33 From the perspective of cost-effectiveness and quality of adjusted life years, the allocation of health resources should focus on technology with social benefits and the promotion of health, but not delayed fertility without a medical purpose. Therefore, some observers believe hospitals in China are not currently suitable for eOC because this technology is not a therapeutic procedure.
There are still a lot of issues concerning health accessibility and equality of public health resources in China. Although many developed countries offer eOC, many disparities in health care access and quality of medical resources exist in developing countries.34 Within China, the allocation of health resources is unbalanced among the provinces and between the developed provinces and developing areas.24–27 Therefore, basic medical services should be the priority of health resources in China.
Our data showed that the participants lacked knowledge of eOC and not that many participants were willing to use this technology. Our data also suggested that policy-makers need to pay attention to the possible consequences of allowing eOC. Furthermore, those who want eOC should be required to pay for the procedure. However, at the present time, a sufficient physical or regulatory infrastructure is not available to ensure that private provision of services would be responsibly introduced. If eOC is allowed using one’s private funds, the government needs to strengthen the infrastructure for such services as well as a regulatory framework, so that women are not taken advantage of by nefarious providers. Furthermore, the providers must be prevented from misusing public funds and facilities.
Conclusion
In our study, few participants knew the cost of eOC but around half of participants thought they fully understood eOC. Even though about half of participants agreed that single women or women without cancer could use eOC, most females did not have a fertility desire by eOC. More debate is needed to determine the possibility of allowing eOC in public hospitals. The debates also need to focus on the ethical, legal, and social aspects and how to regulate eOC while protecting the reproductive freedom of healthy women. More research needs to be conducted on the ethical, legal, and social implications. Prudence should be exercised while arguments for and against eOC are heard from jurists, ethicists, sociologists, policy-makers, and even the public.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the first authors, without undue reservation.
Ethics Approval and Informed Consent
Ethical approval of this study was obtained from the Ethics Committee of Binzhou Medical University (REC NO. (2022-212). Informed consent was obtained from all study participants on an electronic questionnaire. The study complies with the Declaration of Helsinki.
Acknowledgments
Chenge Liao and Xiaomei Zhai are co-correspondence authors for this study. We are grateful to all participants enrolled in this study. We also want to express our gratitude to the Humanities and Social Sciences research project of Ministry of Education (19YJCZH100) and Inner Mongolia Department of Education Humanities and Social Sciences General project (NJSY19108).
Funding
This study was funded by the Humanities and Social Sciences research project of Ministry of Education (19YJCZH100) and Inner Mongolia Department of Education Humanities and Social Sciences General project (NJSY19108).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Noyes N, Labella PA, Grifo J, Knopman JM. Oocyte cryopreservation: a feasible fertility preservation option for reproductive age cancer survivors. J Assist Reprod Genet. 2010;27(8):495–499. doi:10.1007/s10815-010-9434-3
2. Bedoschi G, Oktay K. Current approach to fertility preservation by embryo cryopreservation. Fertil Steril. 2013;99(6):1496–1502. doi:10.1016/j.fertnstert.2013.03.020
3. Jain JK, Paulson RJ. Oocyte cryopreservation. Fertil Steril. 2006;86(4 Suppl):1037–1046. doi:10.1016/j.fertnstert.2006.07.1478
4. Practice Committees of the American Society for Reproductive Medicine and the Society for Assisted Reproductive Technology. Mature oocyte cryopreservation: a guideline. Fertil Steril. 2013;99(1):37–43. doi:10.1016/j.fertnstert.2012.09.028
5. Cho HW, Lee S, Min KJ, et al. Advances in the treatment and prevention of chemotherapy-induced ovarian toxicity. Int J Mol Sci. 2020;21(20):7792. doi:10.3390/ijms21207792
6. Tao T, Del Valle A. Human oocyte and ovarian tissue cryopreservation and its application. J Assist Reprod Genet. 2008;25(7):287–296. doi:10.1007/s10815-008-9236-z
7. Harwood KA. On the ethics of social egg freezing and fertility preservation for nonmedical reasons. Medicoleg Bioethic. 2015;5:59–67. doi:10.2147/MB.S66444
8. Shkedi-Rafid S, Hashiloni-Dolev Y. Egg freezing for non-medical uses: the lack of a relational approach to autonomy in the new Israeli policy and in academic discussion. J Med Ethics. 2012;38(3):154–157. doi:10.1136/medethics-2011-100088
9. Pritchard N, Kirkman M, Hammarberg K, et al. Characteristics and circumstances of women in Australia who cryopreserved their oocytes for non-medical indications. J Reprod Infant Psychol. 2017;35(2):108–118. doi:10.1080/02646838.2016.1275533
10. Katsani D, Paraschou N, Panagouli E, et al. Social egg freezing-a trend or modern reality? J Clin Med. 2024;13(2):390. doi:10.3390/jcm13020390
11. Inhorn MC. The egg freezing revolution? Gender, technology, and fertility preservation in the twenty-first century. In: Scott RA, Buchmann M, editors. Emerging Trends in the Social and Behavioral Sciences. Hoboken: John Wiley & Sons, Inc.; 2017:1–14.
12. Varlas VN, Bors RG, Albu D, et al. Social Freezing: pressing Pause on Fertility. Int J Environ Res Public Health. 2021;18(15):8088. doi:10.3390/ijerph18158088
13. Bhatia R, Campo-Engelstein L. The biomedicalization of social egg freezing: a comparative analysis of European And American professional ethics opinions and US news and popular media. Sci Technol Hum Val. 2018;43(5):864–887. doi:10.1177/0162243918754322
14. Beauchamp T, Childress J. Principles of biomedical ethics: marking its fortieth anniversary. Am J Bioeth. 2019;19(11):9–12. doi:10.1080/15265161.2019.1665402
15. Gao DR, Shi XW. Ethical considerations on social egg freezing for single women. Chin Med Ethics. 2023;36(3):288–292. doi:10.12026/j.issn.1001-8565.2023.03.09
16. Shi JY, Zeng J. Legal regulation and countermeasures on single females’ egg freezing. J Shandong Women’s Univ. 2023;1–10(3):129.
17. Xie Y, Zhai X. An ethical debate on non-medical oocyte cryopreservation. Med Philos. 2023;44(17):21–25. doi:10.12014/j.issn.1002-0772.2023.17.05
18. Gazette Min Health PRC. Notice of the Ministry of Health on the revision of technical specifications, basic standards and ethical Principles related to human assisted reproductive technology and human sperm banks. Gazette Min Health PRC. 2003.
19. Grandy K. Freeze frame: media coverage of Apple’s and Facebook’s egg-freezing employee benefit. Gend Manag. 2019;34(5):384–397. doi:10.1108/GM-07-2018-0080
20. Campo-Engelstein L, Aziz R, Darivemula S, Raffaele J, Bhatia R, Parker WM. Freezing fertility or freezing false hope? A content analysis of social egg freezing in US print media. AJOB Empir Bioethics. 2018;9(3):181–193. doi:10.1080/23294515.2018.1509153
21. Hong YH, Park JW, Kim H, et al. A survey on the awareness and knowledge about elective oocyte cryopreservation among unmarried women of reproductive age visiting a private fertility center. Obstet Gynecol Sci. 2019;62(6):438–444. doi:10.5468/ogs.2019.62.6.438
22. Stoop D, Nekkebroeck J, Devroey P. A survey on the intentions and attitudes towards oocyte cryopreservation for non-medical reasons among women of reproductive age. Hum Reprod. 2011;26(3):655–661. doi:10.1093/humrep/deq367
23. Walker Z, Lanes A, Ginsburg E. Oocyte cryopreservation review: outcomes of medical oocyte cryopreservation and planned oocyte cryopreservation. Reprod Biol Endocrin. 2022;20(1):1–14. doi:10.1186/s12958-021-00884-0
24. Lanyi Y, Xiaomei Z. Oocyte cryopreservation for non-medical reasons: ethical and regulatory concerns in China. Dev World Bioeth. 2023. doi:10.1111/dewb.12418
25. Ren Y, Xie Y, Xu Q, et al. University students’ fertility awareness and its influencing factors: a systematic review. Reprod Health. 2023;20(1):1–12. doi:10.1186/s12978-023-01628-6
26. Zhong Y, Liu W, Lee TY, Zhao H, Ji J. Risk perception, knowledge, information sources and emotional states among COVID-19 patients in Wuhan, China. Nurs Outlook. 2021;69(1):13–21. doi:10.1016/j.outlook.2020.08.005
27. Jahromi BN, Parsanezhad ME, Shomali Z, et al. Ovarian hyperstimulation syndrome: a narrative review of its pathophysiology, risk factors, prevention, classification, and management. Iran J Med Sci. 2018;43(3):248–260. doi:10.30476/IJMS.2018.40535
28. Tureck RW, García CR, Blasco L, Mastroianni L. Perioperative complications arising after transvaginal oocyte retrieval. Obstet Gynecol. 1993;81(4):591–593.
29. Frederiksen LE, Ernst A, Brix N, et al. Risk of adverse pregnancy outcomes at advanced maternal age. Obstet Gynecol. 2018;131(3):457–463. doi:10.1097/01.aoa.0000542378.64975.41
30. Alteri A, Pisaturo V, Nogueira D, D’Angelo A. Elective egg freezing without medical indications. Acta Obstet Gyn Scan. 2019;98(5):647–652. doi:10.1111/aogs.13573
31. Gürtin ZB, Tiemann E. The marketing of elective egg freezing: a content, cost and quality analysis of UK fertility clinic websites. Reprod Biomed Soc Online. 2021;12:56–68. doi:10.1016/j.rbms.2020.10.004
32. Persad G, Wertheimer A, Emanuel EJ. Principles for allocation of scarce medical interventions. Lancet. 2009;373(9661):423–431. doi:10.1016/S0140-6736(09)60137-9
33. Munthe C, Fumagalli D, Malmqvist E. Sustainability principle for the ethics of healthcare resource allocation. J Med Ethics. 2021;47(2):90–97. doi:10.1136/medethics-2020-106644
34. Haakenstad A, Yearwood JA, Fullman N, et al. Assessing performance of the healthcare access and quality index, overall and by select age groups, for 204 countries and territories, 1990–2019: a systematic analysis from the Global Burden of Disease Study 2019. Lancet Glob Health. 2022;10(12):e1715–e1743. doi:10.1016/S2214-109X(22)00429-6
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.