")
Back to Journals » Open Access Journal of Sports Medicine » Volume 14
Athlete Sleep Behavior Questionnaire in Japanese (ASBQ-J): An Adaptation and Validation Study
Authors Tsukahara Y , Kodama S, Kikuchi S, Day C
Received 21 August 2023
Accepted for publication 2 November 2023
Published 16 November 2023 Volume 2023:14 Pages 89—97
DOI https://doi.org/10.2147/OAJSM.S431820
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff
Yuka Tsukahara,1 Satoshi Kodama,2 Saaya Kikuchi,1 Carly Day3,4
1Department of Sports Medicine, Tokyo Women’s College of Physical Education, Kuitachi, Tokyo, Japan; 2Department of Neurology, Graduate School of Medicine, The University of Tokyo, Bunkyo, Tokyo, Japan; 3Department of Health and Kinesiology, Purdue University, West Lafayette, IN, USA; 4Franciscan Physician Network, West Lafayette, IN, USA
Correspondence: Yuka Tsukahara, Department of Sports Medicine, Tokyo Women’s College of Physical Education, 4-30-1 Fujimidai Kunitachi, Tokyo, 1868668, Japan, Tel +8180-3688-6128, Fax +81471-60-6112, Email [email protected]
Purpose: The Athlete Sleep Behavior Questionnaire (ASBQ) is an 18-item self-reported questionnaire that can be used to screen for sleep disorders in athletes and assess environmental, behavioral, and sports-related factors along with sleep disorders. This study aimed to analyze the reliability and validity of the ASBQ translated into Japanese (ASBQ-J).
Patients and Methods: 111 female collegiate athletes completed both the initial test and retest. Independent variables were what kind of sports they perform, level as an athlete, grade (freshman, sophomore, junior, senior), and age. The reliability of the survey was assessed using Cronbach’s alpha and intraclass correlation, and Pearson’s correlation coefficient was calculated to determine the correlation between the total ASBQ scores and three components which were routine/environmental, behavioral, and sports factors.
Results: A total of 37.8% of athletes had ASBQ scores equal or less than 36 indicating good sleep. However, 19.8% of athletes scored more than 42, indicating poor sleep. Cronbach alpha was 0.62 and 0.65 for test and retest, respectively. Intraclass correlation was 0.78 (P < 0.01), indicating sufficient internal consistency and test–retest validity. Mean ASBQ scores were 38.5 ± 5.0 and 37.0 ± 6.5 for test and retest, respectively, and it was not significantly different between the two groups (P = 0.37). The correlation coefficients between the ASBQ-J and component scores were all statistically significant (all P < 0.01).
Conclusion: ASBQ-J is a reliable questionnaire for assessing sleep disorders in athletes whose primary language is Japanese.
Keywords: collegiate athlete, female athlete, performance level, survey
Introduction
Insomnia is more prevalent in athletes than in the general population.1 Athletes can be under considerable psychological pressure including anxiety and depression that can affect their sleep patterns.2 Sleep deprivation has been reported to be associated with a high risk of injury due to decreased attention and impaired judgment.3 Specifically, less than 8 hours of sleep per night was associated with increased injury risk in adolescent athletes.4 A correlation between sleep and performance has been reported including improved accuracy with sleep extension and decreased power with sleep deprivation.4–6 Therefore, although adequate sleep is essential for athletes, 42% of college athletes in the United States have poor sleep quality.7 In addition, sleep disorders may overlap with other medical conditions. Difficulty sleeping can be due to untreated or undertreated asthma and gastroesophageal reflux disease.8,9 Thus, whether athletes have any type of sleep disorder needs to be accurately diagnosed. Furthermore, it has been reported that premenstrual and menstrual periods are associated with insomnia and poor sleep quality, and although assessing sleep disorders is important for all athletes, female athletes need to be screened for sleep disorders.10
Finding an easy screening tool for sleep in athletes is imperative as it is often impractical to perform actigraphy or overnight sleep studies due to cost, compliance, time demands, and adequate staff to interpret. There are many questionnaires regarding sleep, such as the Pittsburgh Sleep Quality Index, which have been translated into different languages and used to evaluate sleep length, habitual sleep efficiency, sleep latency, sleep disruption, daytime dysfunction, sleep medication use, and subjective sleep quality over the preceding month.11–14 However, these questions are not specific to athletes, and some are related to working environments that are not applicable to student-athletes.12 Athlete Sleep Behavior Questionnaire (ASBQ) by Driller et al consists of 18 questions that examine sleep behavior using a 5-point scale (1: never, 2: rarely, 3: sometimes, 4: frequently, and 5: always). The range of scores was between 18 and 90 with higher scores indicating poor sleep behaviors.15 The three main categories included were routine/environmental factors (naps, consistent bedtimes, and travel), behavioral factors (medications, alcohol, and late-night technology use), and sports-related factors (late-night training, pain, and worrying about performance). Sleep disorders were calculated by adding these numbers, and scores less than or equal to 36 characterized good sleep behavior, scores above 42 characterized poor sleep behavior, and scores between 37 and 42 characterized moderate sleep behavior. The ASBQ demonstrated low-to-moderate correlations with other sleep questionnaires and high test–retest consistency and has been used in elite athletes.15–17 Mason et al has reported that sleep difficulty measured by ASBQ scores were associated with injury status. However, the survey was conducted in English, and although it has been translated into Turkish, Portuguese, and French, few surveys have been performed on non-English-speaking athletes, including Japanese athletes, who reportedly have low sleep duration.18–21 Although general sleep questions can be the same, there are certain cultural differences among athletes’ personal backgrounds, which may affect some questions and their answers. In this study, we aimed to translate the ASBQ into Japanese (ASBQ-J), assess its validity, test the reliability of the translated Japanese survey, and investigate the characteristics of the results obtained from Japanese female athletes. We hypothesized that the validity would be high but could be lower than that of the original ASBQ, owing to the effect of cultural backgrounds. In addition, as elite athletes have been reported to have sleep disorders, we hypothesized that the performance level of the athlete is also correlated with ASBQ-J scores.22,23
Materials and Methods
Translation of the Survey
Ethical Considerations
This prospective study was approved by the Ethics Committee of the Tokyo Women’s College of Physical Education (approval number: 2022–75) and complied with the ethical principles of the Declaration of Helsinki. All athletes provided electronical written informed consent prior to participating in the study.
Forward Translation
First, permission was obtained from the original authors to translate the survey into the Japanese language. Two physicians, bilingual in English and Japanese who specialize in sports medicine (YT) and neurology (SK) with an experience of more than 10 years in these fields translated the original ASBQ from English to Japanese.24 Given potential differences in cultures, translations were reviewed by the athletes, coaches, and an American physician specializing in sports medicine (CD). The two Japanese physicians discussed whether there were any differences in their translations, and when they were not resolved, third translator, who has an experience of more than 20 years of translating not involved in the initial translation was asked to provide an opinion.25
Backward Translation
To ensure accurate translation, the English questionnaire, which was translated into Japanese, was back-translated into English.26 This was performed by two independent translators whose native language was English and who worked at a translation company with more than 20 years of experience in translating without knowing the purpose of the translation.
Expert Committee
The expert committee specializing in physical education, sports medicine, and neurology (two females and one male) reviewed the finalized version of the questionnaire and the translated version; when there were any discrepancies that needed to be resolved, forward and backward translations were repeated until the discrepancies were resolved.
Pilot Study
The survey was then distributed to 42 female athletes, as this number is sufficient according to a previous study.27 The respondents were interviewed verbally using an open-ended question on their thoughts about the questionnaire and whether they understood all the questions, whether there was any confusion regarding the questions, and if there were any questions that did not make any sense. This process was repeated until the final version of the questionnaire was completed. The time required to complete the ASBQ-J was 2–3 min. Details of both the original and Japanese versions of the ASBQ are presented in Figure 1.
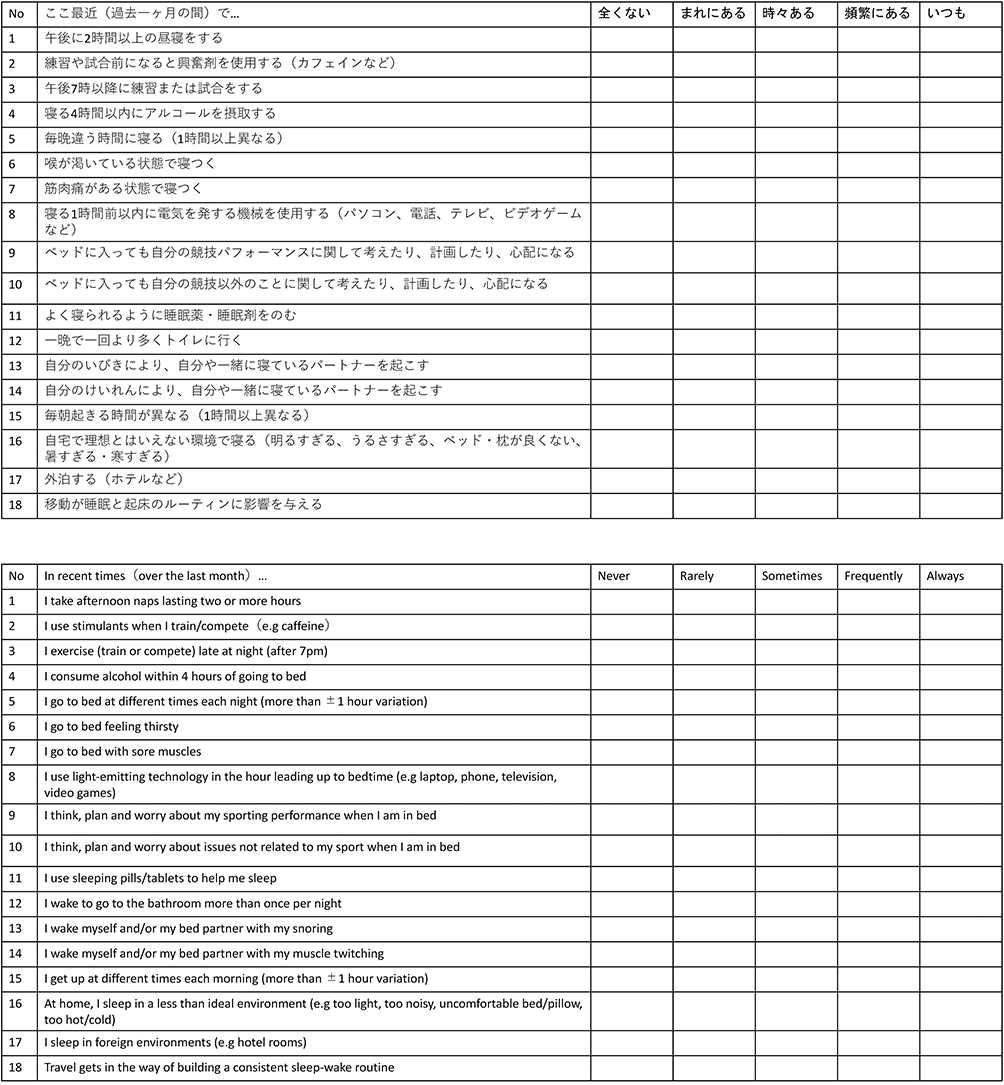 |
Figure 1 Details of both the original and Japanese versions of the ASBQ. Adapted and translated with permission from Driller MW, Mah CD, Halson SL. Development of the athlete sleep behavior questionnaire: a tool for identifying maladaptive sleep practices in elite athletes. Sleep Science. 2018;11(1):37. Creative Commons.15 |
Distribution of the Survey
Following completion of the pilot study, the linkable anonymized ASBQ-J was sent to 437 female collegiate athletes in a single institution in Japan electronically and google form was used as the platform. Since the ASBQ consisted of 18 questions, and the number of participants required was reported to be five times the number of questions, we calculated that more than 90 participants were needed in this study; thus, we performed the survey using 17 different types of sports teams.26 Athletes were asked what kind of sports they perform, their level as an athlete, their grade (freshman, sophomore, junior, senior), and their age, in addition to the questions in the ASBQ-J. The survey was first administered to the athletes on the first week of February 2023. To assess the test–retest consistency, the survey was again administered to the same group one month later which is different from the original survey (7 days) to avoid the retest being too close to the test for the participants to remember their responses or the gap between the test and being too long that their daily schedule, including their sleep, had changed.15 The study protocol was approved by the Ethics Review Procedures Concerning Research with Human Subjects Group of the authors’ affiliated institutions (approval number 2022-15) and was conducted in accordance with the tenets of the Declaration of Helsinki.
Statistical Analyses
All data were analyzed using Stata 16.1 (Stata Corporation, TX, USA). Comparison of national level athletes to non- national level athletes were performed using independent sample t-tests. Internal consistency was measured by calculating Cronbach’s alpha and McDonald’s omega. To investigate the test–retest reliability, intraclass correlation (ICC) coefficients were measured. Correlations between the total ASBQ-J score and three components (environmental, behavior and sports factors) were evaluated using Pearson’s correlation coefficients to investigate the homogeneity of the ASBQ-J scores for both national and non-national level athletes. ICC values less than 0.5, between 0.5 and 0.75, between 0.75 and 0.9, and greater than 0.9 are indicative of poor, moderate, good, and excellent reliability, respectively. Furthermore, Pearson’s correlation coefficients less than 0.2, between 0.2 and 0.39, between 0.4 and 0.59, between 0.6 and 0.79, and greater than 0.8 are indicative of very weak, weak, moderate, strong, and very strong.
Results
ASBQ-J was distributed to athletes from a single institution majoring in physical education twice a month apart. A total of 401 athletes from 17 different types of sports teams responded. The response rate was 54.9% for the first survey and 41.4% for the second survey. A total of 111 athletes participating in 14 different sports completed both the first and second surveys, and their data were analyzed. The mean age of the respondents who completed both the first and second survey was 20.4 ± 0.9 years-old, and the grades of the respondents were freshmen 35.1% (N = 39), sophomore 27.9% (N = 31), junior 31.5% (N = 35), and senior 5.4% (N = 6). A total of 46.8% (N = 52) of the athletes were competing at the national or international level. Mean ASBQ-J scores were 37.5±5.8 and 35.5±6.0 during the first and second survey, respectively, and were not significantly different between national- and non-national-level athletes (36.1±5.7 and 34.9±6.2, respectively p = 0.30) according to the t-tests. The ASBQ-J scores and its components during the first and second surveys with the comparisons between the national and non-national levels are listed in Table 1 and none of the components were statistically different between national and non-national level athletes during both the first and second survey. A total of 37.8% of athletes had ASBQ-J scores equal or less than 36 indicating good sleep. However, almost one in five athletes (19.8%) scored more than 42, indicating that they have poor sleep. The majority of athletes (99.0%) answered that they had never taken any medication to aid sleep, and 90.1% of athletes answered that they sometimes had sore muscles that affected their sleep. Furthermore, most athletes (96.4%) answered that they did not wake up during sleep because of snoring. Among the 18 questions, there were no significant differences in the response for 17 questions between national- and non-national-level athletes; however, national-level athletes answered that they took fewer naps than their non-national-level counterparts. Details of the ASBQ-J results are shown in Figure 2.
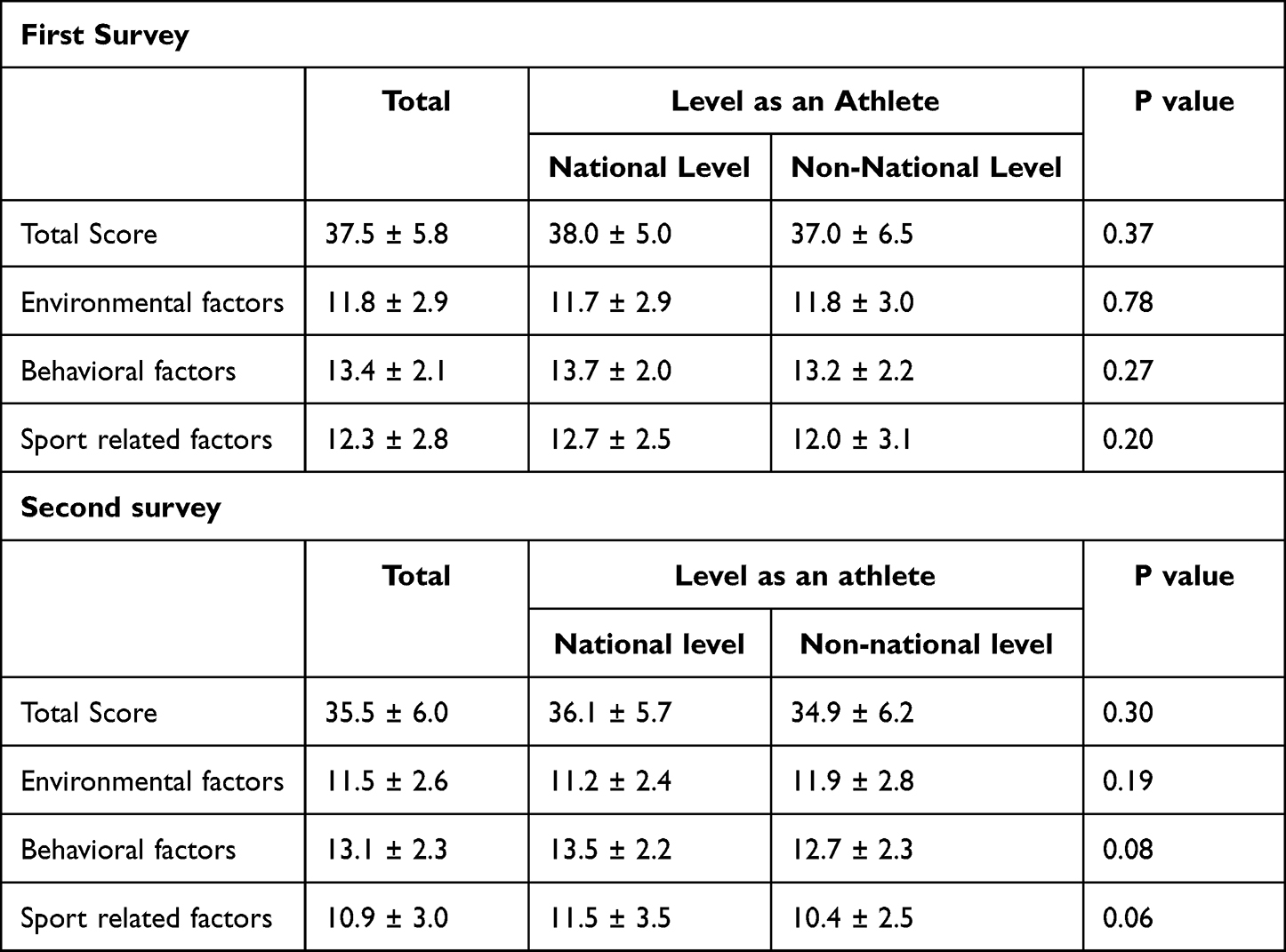 |
Table 1 Results of ASBQ-J |
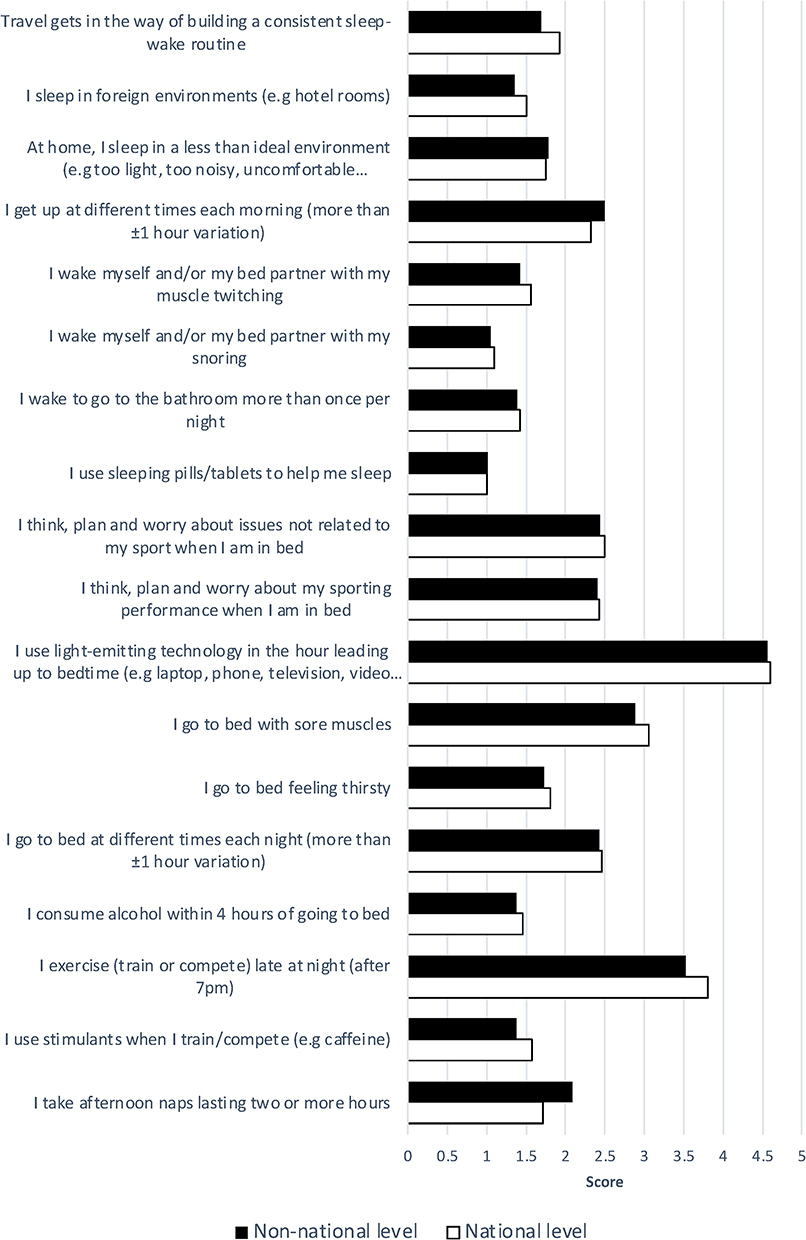 |
Figure 2 Details of the ASBQ-J results. |
Reliability
Cronbach’s alpha coefficient, which reflects internal consistency, was 0.62 for the first and 0.65 for the second survey. In addition, McDonald’s Omega was 0.54 for the first and 0.65 for the second survey. For test–retest reliability, the ICC value was 0.78 (95% CI, 0.64–0.86), thus indicating high reliability (P < 0.001). In addition, the ICC values for all three factors, namely environmental, behavioral, and sports-related factors, were above 0.7, when all athletes were combined. Test–retest validity results are listed in Table 2. Pearson’s correlations between the total ASBQ-J score and three component scores were all high and statistically significant but were mostly higher in non-national-level athletes than in their national-level counterparts. The correlation coefficients between the ASBQ-J and component scores are listed in Table 3.
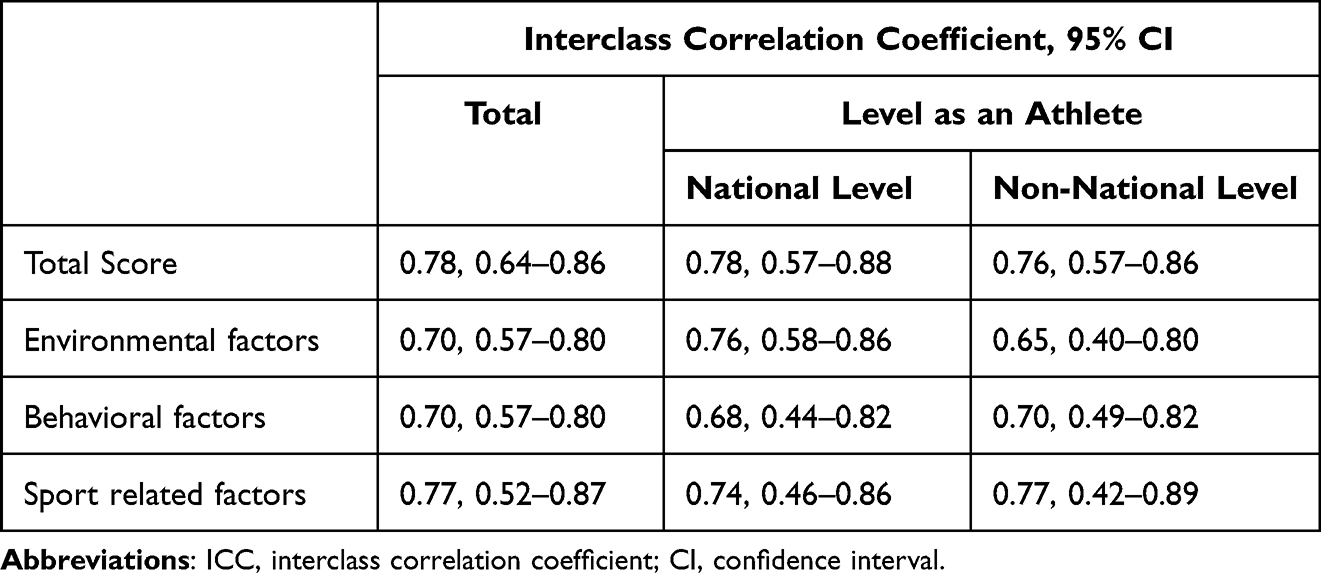 |
Table 2 Results of Test-Retest Reliability |
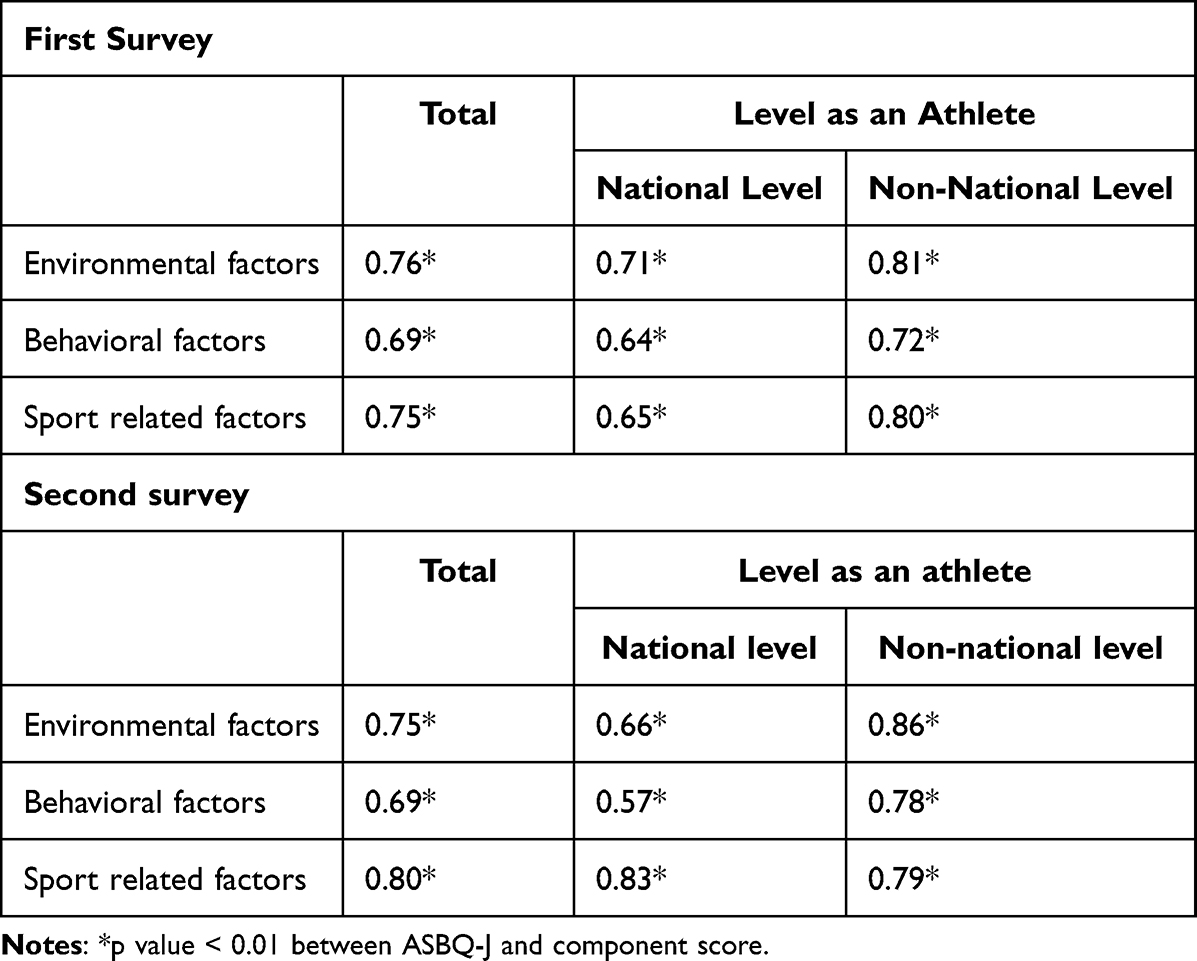 |
Table 3 Correlation Coefficients Between the ASBQ-J and Component Scores |
Discussion
This study translated the ASBQ into Japanese and validated the Japanese version. We performed both forward and backward translations, followed by a discussion with the experts, and modified wording based on the cultural context. Response rate was felt to be good, possibly due to ease of completing the short survey. The questions were easily comprehensible, regardless of the athlete’s educational background. However, certain words were reworded as the transcultural adaptations were necessary; for example, in Japanese the word “travel” could mean “leisure” rather than travel for competition.28
Contrary to our hypothesis, the Cronbach’s alpha coefficient (0.62 and 0.65 during the first and second survey, respectively) was slightly higher than that in the study by Driller et al (0.63), indicating that the internal consistency was slightly higher than the original survey in English and lower than the Brazilian version, which was 0.78.15,19 According to Terwee et al, although a value of more than 0.7 is preferable, values between 0.6 and 0.7 can be considered as satisfactory.29 In addition, test–retest reliability was sufficiently high, despite the survey being conducted 4 weeks apart, which is longer than the gap in previous studies, thereby indicating that the scores remained stable over those 4 weeks.15,19 Thus, our results establish that the ASBQ-J is reliable. In addition, the ICC was high for both national- and non-national-level athletes, along with a higher overall test–rested reliability in non-national-level athletes than in national-level athletes, suggesting that the ASBQ-J can be used for a wide range of athletes, although the primary author recommended its use in elite athletes.15 In addition, as the Pearson’s correlation between ASBQ-J scores and the components was high for all components, good validity of the linguistic constructs was noted.
The majority of the athletes reported having sore muscles that disrupted their sleep, which is higher than in the previous studies.15,19 It was not specified whether the sore muscles were due to injury, overtraining, or another cause.21 Thus, in future studies, researchers should consider identifying the cause of the muscle soreness which may better help target solutions to this problem that could be affecting their sleep. Overall, there were no significant differences between national- and non-national-level athletes. This could be because the athletes belonged to a single institution.
In this study, the average ASBQ-J scores were lower than those in previous studies.15,19,30 However, our study participants used less stimulants, alcohol, and medications than that in the study by Driller et al.15 This corresponds to the results of previous studies from Japan. For example, Hoshikawa et al reported that the use of medications to aid sleep was 1.6% in elite female athletes, and the usage of caffeine in Japanese athletes was lower than that in other elite athletes.30–33 Furthermore, it is possible that general environmental differences and possibly cultural differences in Japan could have played a role. Compared with the study by Driller et al, in our participants, the frequency of training at night was higher.15 However, this could be explained by another previous study that indicated that the training hours were longer in Japanese athletes than in American athletes competing at the same level.21,30
This study has some limitations. First, the survey was only performed on non-minor female athletes and further studies on male and minor athletes are required, as sex may play a role in sleep disorders and distributing the survey to athletes in multiple levels are also required.34 For example, since sleep apnea is less prevalent in females compared to their male counterparts, almost none of the athletes reported difficulty in sleeping due to snoring.35 Second, as the number of athletes who completed the survey in two different time frames was close to half, there may be a selection bias, and future studies are required for a more diverse population. Third, the participants in this study were from a single institution and to compare the results with previous studies, it is necessary to distribute the survey to different institutions because it is challenging to conclude whether the results in this study reflect the cultural differences between Japan and other countries or solely are a characteristic of this specific institution. In addition, we did not validate the diagnostic accuracy of the survey by asking the athletes whether they had any sleep disorders, and we were also not able to determine the stage of the sporting season when the survey was distributed due to the variety of sports.
The Japanese ASBQ was modified to represent the cross-cultural adaptation and will be an important tool for Japanese athletes to assess their sleep behaviors. The internal consistency was higher than that of the study performed by the original authors, and the validity was sufficiently accurate. Prospectively, it may aid athletes in acquiring a healthy sleep environment. The ease of distributing and scoring an interpretation of the ASBQ will make it possible for athletes, coaches, and medical practitioners to evaluate sleep disorders in athletes and will be able to address the problems easily, thereby leading to early intervention. In fact, Driller et al utilized ASBQ for individualized sleep hygiene education.17 Future studies with participants from diverse populations are required to build stronger evidence for the use of the ASBQ in athletes.
Conclusion
Athletes of all levels have poor sleep behaviours. The Japanese version of the ASBQ has been validated with sufficient internal consistency and test–retest validity. This is a simple and reliable tool for screening Japanese athletes with poor sleep behaviours. Although it cannot be used to make a diagnosis, it will be helpful not only for athletes but also for coaches, parents, and medical personnel to assess the sleep hygiene of the athletes.
Acknowledgments
We thank all the athletes who participated in this study.
Disclosure
Dr Carly Day reports travel reimbursement for Board of Directors meetings from American Medical Society for Sports Medicine, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Gupta L, Morgan K, Gilchrist S. Does elite sport degrade sleep quality? A systematic review. Sports Med. 2017;47(7):1317–1333. doi:10.1007/s40279-016-0650-6
2. Grandner MA, Hall C, Jaszewski A, et al. Mental health in student athletes: associations with sleep duration, sleep quality, insomnia, fatigue, and sleep apnea symptoms. Athl Train Sports Health Care. 2021;13(4):e159–e167. doi:10.3928/19425864-20200521-01
3. Gao B, Dwivedi S, Milewski MD, Cruz AI. Lack of sleep and sports injuries in adolescents: a systematic review and meta-analysis. J Pediatr Orthop. 2019;39(5):e324–e333. doi:10.1097/BPO.0000000000001306
4. Milewski MD, Skaggs DL, Bishop GA, et al. Chronic lack of sleep is associated with increased sports injuries in adolescent athletes. J Pediatr Orthop. 2014;34(2):129–133. doi:10.1097/BPO.0000000000000151
5. Mah CD, Mah KE, Kezirian EJ, Dement WC. The effects of sleep extension on the athletic performance of collegiate basketball players. Sleep. 2011;34(7):943–950. doi:10.5665/SLEEP.1132
6. Watson AM. Sleep and athletic performance. Curr Sports Med Rep. 2017;16(6):413–418. doi:10.1249/JSR.0000000000000418
7. Mah CD, Kezirian EJ, Marcello BM, Dement WC. Poor sleep quality and insufficient sleep of a collegiate student-athlete population. Sleep Health. 2018;4(3):251–257. doi:10.1016/j.sleh.2018.02.005
8. Shibli F, Skeans J, Yamasaki T, Fass R. Nocturnal gastroesophageal reflux disease (GERD) and sleep: an important relationship that is commonly overlooked. J Clin Gastroenterol. 2020;54(8):663–674. doi:10.1097/MCG.0000000000001382
9. Reiter J, Ramagopal M, Gileles Hillel A, Forno E. Sleep disorders in children with asthma. Pediatr Pulmonol. 2022;57(8):1851–1859. doi:10.1002/ppul.25264
10. Day C, Nishino N, Tsukahara Y. Sleep in the Athlete. Clin Sports Med. 2023. doi:10.1016/j.csm.2023.06.007
11. Suleiman KH, Yates BC, Berger AM, Pozehl B, Meza J. Translating the Pittsburgh Sleep Quality Index into Arabic. West J Nurs Res. 2010;32(2):250–268. doi:10.1177/0193945909348230
12. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
13. Shochat T, Tzischinsky O, Oksenberg A, Peled R. Validation of the Pittsburgh Sleep Quality Index Hebrew translation (PSQI-H) in a sleep clinic sample. I Med Assoc J. 2007;9(12):853.
14. Bertolazi AN, Fagondes SC, Hoff LS, et al. Validation of the Brazilian Portuguese version of the Pittsburgh Sleep Quality Index. Sleep Med. 2011;12(1):70–75. doi:10.1016/j.sleep.2010.04.020
15. Driller MW, Mah CD, Halson SL. Development of the athlete sleep behavior questionnaire: a tool for identifying maladaptive sleep practices in elite athletes. Sleep Science. 2018;11(1):37. doi:10.5935/1984-0063.20180009
16. Mason J, Stewart A, Kniewasser C, Zech A. Tracking sleep in the field: sleep quality and sleep behaviours of elite track and field athletes during preparation and competition. J Sports Sci. 2022;40(24):2741–2749. doi:10.1080/02640414.2023.2191089
17. Driller MW, Lastella M, Sharp AP. Individualized sleep education improves subjective and objective sleep indices in elite cricket athletes: a pilot study. J Sports Sci. 2019;37(17):2021–2025. doi:10.1080/02640414.2019.1616900
18. Baize D, Meriaux-Scoffier S, Chrétien A, Hayotte M, Piponnier E, d’Arripe-Longueville F. Sleep assessment in competitive athletes: development and validation of French Versions of the Athens Insomnia Scale and the Athlete Sleep Behavior Questionnaire. Sleep Science. 2023;16(02):183–196. doi:10.1055/s-0043-1770803
19. Facundo LA, Albuquerque MR, Esteves AM, et al. Cross-cultural adaptation of the Brazilian version of the athlete sleep behavior questionnaire. Sleep Sci. 2021;14(Spec 2):150–157. doi:10.5935/1984-0063.20200105
20. Darendeli A, Diker G, Çinar Z. Athlete sleep behavior questionnaire-Turkish version: study of validity and reliability. J Turk Sleep Med. 2019;6(2):43–48.
21. Tsukahara Y, Mason RA, Macznik A. Training and physiological characteristics of American and Japanese female track and field athletes. J Sports Med Phys Fitness. 2022;62(9). doi:10.23736/S0022-4707.22.13045-8
22. Dunican IC, Walsh J, Higgins CC, et al. Prevalence of sleep disorders and sleep problems in an elite super rugby union team. J Sports Sci. 2019;37(8):950–957. doi:10.1080/02640414.2018.1537092
23. Nedelec M, Aloulou A, Duforez F, Meyer T, Dupont G. The variability of sleep among elite athletes. Sports Med - Open. 2018;4(1):1–13. doi:10.1186/s40798-018-0151-2
24. Hendricson WD, Jon Russell I, Prihoda TJ, et al. Development and initial validation of a dual-language English–Spanish format for the arthritis impact measurement scales. Arthritis Rheum. 1989;32(9):1153–1159. doi:10.1002/anr.1780320915
25. Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol. 1993;46(12):1417–1432. doi:10.1016/0895-4356(93)90142-N
26. Tsang S, Royse CF, Terkawi AS. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J Anaesth. 2017;11(Suppl 1):S80–S89. doi:10.4103/sja.SJA_203_17
27. Perneger TV, Courvoisier DS, Hudelson PM, Gayet-Ageron A. Sample size for pre-tests of questionnaires. Qual Life Res. 2015;24(1):147–151. doi:10.1007/s11136-014-0752-2
28. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
29. Terwee CB, Bot SD, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42. doi:10.1016/j.jclinepi.2006.03.012
30. Driller MW, Suppiah H, Rogerson D, Ruddock A, James L, Virgile A. Investigating the sleep habits in individual and team-sport athletes using the Athlete Sleep Behavior Questionnaire and the Pittsburgh Sleep Quality Index. Sleep Sci. 2022;15(1):112–117. doi:10.5935/1984-0063.20210031
31. Hoshikawa M, Uchida S, Hirano Y. A subjective assessment of the prevalence and factors associated with poor sleep quality amongst elite Japanese athletes. Sports Med - Open. 2018;4(1):1–13. doi:10.1186/s40798-018-0122-7
32. Tabata S, Yamasawa F, Torii S, et al. Use of nutritional supplements by elite Japanese track and field athletes. J Int Soc Sports Nutr. 2020;17(1):1–8. doi:10.1186/s12970-020-00370-9
33. Del Coso J, Muñoz G, Muñoz-Guerra J. Prevalence of caffeine use in elite athletes following its removal from the world anti-doping agency list of banned substances. Appl Physiol Nutr Metab. 2011;36(4):555–561. doi:10.1139/h11-052
34. Abd Rahim H, Zawi MK. Study of sleep behaviour of adolescent athletes sports school Malaysia Sabah. Malaysian J Soc Sci Humanit. 2022;7(3):e001382–e001382. doi:10.47405/mjssh.v7i3.1382
35. Swinbourne R, Gill N, Vaile J, Smart D. Prevalence of poor sleep quality, sleepiness and obstructive sleep apnoea risk factors in athletes. Eur J Sport Sci. 2016;16(7):850–858. doi:10.1080/17461391.2015.1120781
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.