")
Back to Journals » Infection and Drug Resistance » Volume 17
Antifungal Selection for the Treatment of Onychomycosis: Patient Considerations and Outcomes
Received 27 November 2023
Accepted for publication 24 February 2024
Published 4 March 2024 Volume 2024:17 Pages 819—843
DOI https://doi.org/10.2147/IDR.S431526
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Sandip Patil
Eden Axler, Shari R Lipner
Weill Cornell Medicine, Department of Dermatology, New York, NY, 10021, USA
Correspondence: Shari R Lipner, Weill Cornell Medicine, Department of Dermatology, 1305 York Avenue, New York, NY, 10021, USA, Tel +1 646-962-3376, Fax +1 646-962-0033, Email [email protected]
Abstract: Onychomycosis, a common fungal nail infection, affects > 20% of adults over age 60 and > 50% of people over age 70. Onychomycosis may cause pain, psychosocial problems, and secondary infections, therefore meriting treatment. This review describes the range of treatment modalities, including FDA-approved systemic drugs and topical therapies. Additionally, new and emerging oral and topical therapies are discussed. We emphasize the importance of tailoring onychomycosis therapy to individual patient characteristics, comorbidities, preferences, extent of nail involvement, and fungal species, such that physicians may optimize treatment outcomes, patient satisfaction, and safety.
Keywords: dermatophyte, nail infection, topical therapy, systemic treatment, fungal susceptibility, treatment guidelines
Introduction
Onychomycosis is a fungal nail infection caused by species that consume keratin, as well as non-dermatophyte molds and yeasts.1 Treatment is challenging due to high recurrence rates, patient compliance, thick nail plate barrier, biofilm formation, and emerging antifungal resistance.2 Food and Drug Administration (FDA) approved treatment options for onychomycosis include systemic and topical antifungals.3 As well, many non-FDA-approved and newer treatments have emerged for treating this condition. Patients with onychomycosis may be apprehensive of treatment due to perceived risks and long treatment courses. Optimal treatment for individual patients is determined by considerations of efficacy, safety, comorbidities, compliance, and cost.4 In this review we discuss current and novel treatment options for onychomycosis to assist physicians in informed treatment decisions.
Etiology
Onychomycosis is predominantly caused by Trichophyton rubrum, followed by Trichophyton mentagrophytes and Epidermophyton floccosum. Dermatophytes account for 90% of toenail and 50% of fingernail infections. Candida albicans represents 2% of cases, primarily in fingernails.5 Nondermatophyte molds, including Fusarium, Aspergillus, Acremonium, Scytalidium, and Scopulariopsis brevicaulis, make up about 8% of infections.5,6
Materials and Methods
Searches for peer-reviewed journal articles were conducted on August 8th, 2023 and January 19th, 2024 using the PubMed/MEDLINE database with the search terms “onychomycosis treatment”, “itraconazole onychomycosis”, “terbinafine onychomycosis”, “griseofulvin onychomycosis”, “fluconazole onychomycosis”, “efinaconazole onychomycosis”, “voriconazole onychomycosis”, “posaconazole onychomycosis”, “fosravuconazole onychomycosis”, “amorolfine onychomycosis”, “ciclopirox onychomycosis”, “tavaborole onychomycosis”, and “luliconazole onychomycosis”. Additionally, reference lists from identified articles were examined to identify further relevant literature. A comprehensive review of over 4000 articles was conducted, with a focus on prioritizing randomized clinical trials and pivotal trials. Studies were excluded if they were not relevant, were overshadowed by more current or larger studies, or were not in English. Studies were not excluded based on the date of publication.
Oral Therapy
Griseofulvin
Griseofulvin was FDA-approved in 1959, making it the first oral agent available for treating onychomycosis.7,8 While once the agent of choice, its use declined due to its longer treatment duration, lower efficacy, and higher recurrence rates compared to other oral antifungals.9,10 Today griseofulvin is now rarely used for onychomycosis treatment.9
Griseofulvin prevents the formation of intracellular microtubules, disrupts the mitotic spindle, and prevents fungal cell division.7 The drug reaches the infection site through uptake by newly produced nail, necessitating continuous treatment as the nail grows out.6 Consequently, griseofulvin is prescribed for extended durations in onychomycosis treatment, with recommended daily doses ranging from 500–1000mg for 6–9 months for fingernails and 12–18 months for toenails, aligned with average nail growth rates.11,12 This prolonged treatment duration results in challenges related to low patient compliance.11,12
Efficacy
Griseofulvin’s spectrum of activity is limited to dermatophytes, and it is not effective against other species or mixed-organism infections.6,13 In a prospective study with 122 onychomycosis patients treated with griseofulvin, mycological cure rates were 29% for toenails and 80% for fingernails, while clinical cure rates were 3% for toenails and 40% for fingernails.14
Safety
Common side effects of griseofulvin include gastrointestinal disturbance, nausea, vomiting, diarrhea, and headache. Nausea and rashes occur in 8–15% of patients (Table 1).12 Less common adverse effects include photosensitivity, fixed drug eruption, petechiae, pruritus, and urticaria.11 Griseofulvin has been associated with relapses of acute intermittent porphyria in two patients in remission.15 One patient was a 51-year-old man who experienced a marked increase of urine pyrrole excretion on his fifth day of griseofulvin treatment. The second patient was a 43-year-old male who experienced a marked increase in urine pyrrole excretion on the first day of treatment with griseofulvin.16 Griseofulvin has also been linked to flares of systemic lupus erythematosus (SLE) and other connective tissue disorders.17 A 22-year-old woman prescribed griseofulvin for an unknown indication (total dose of less than 1g) experienced a fatal exacerbation of SLE after 7 days of treatment.18 It is recommended that physicians conduct thorough medication reviews and avoid prescribing griseofulvin to patients with contraindications.
 |
Table 1 Safety of Oral and Topical Onychomycosis Treatment in Specific Patient Populations |
Special Populations
Pregnancy
Griseofulvin is classified as FDA category C.11 A 1987 paper reported 2 cases of conjoined twins by mothers who had taken griseofulvin early in pregnancy for fungal infections, though this association has not been confirmed.19 It is recommended that female patients wait one month after completing treatment before trying to conceive. In the package insert, caution is advised for men attempting conception within 6 months because griseofulvin was associated with abnormalities in mouse sperm cells.20 However, further studies are required in humans to assess the impact of griseofulvin on sperm quality.
Children
Griseofulvin is not FDA-approved for onychomycosis treatment in children. In a systematic review of systemic antifungals in the treatment of pediatric onychomycosis, 6.3% (n=16) of children experienced complete clearance with griseofulvin with no adverse events reported.21 There are no US guidelines on the treatment of pediatric onychomycosis; However, it is no longer recommended given its lower efficacy and lower compliance compared to other agents.22
Drug Interactions
Griseofulvin induces cytochrome-P450 enzymes and interacts with drugs metabolized through this mechanism.11 It may reduce the therapeutic efficacy of warfarin by increasing its metabolism, necessitating weekly warfarin monitoring.23 Griseofulvin may decrease the therapeutic efficacy of oral contraceptives and salicylates.24
Itraconazole
Itraconazole inhibits 14a-demethylase in the ergosterol biosynthesis pathway, which disrupts the fungal membrane permeability and causes accumulation of lanosterol and other 14α-methyl sterols.25 It was FDA-approved in 1995 for dermatophyte onychomycosis treatment, with oral dosing of 200mg daily for 12 weeks for toenails and two treatment pulses of 200mg twice daily for 1 week separated by 3 weeks for fingernails.4,26 Itraconazole demonstrates broad-spectrum activity against dermatophytes, non-dermatophyte molds, and candida species. The oral formulation of itraconazole has 55% bioavailability, though maximal absorption occurs in acidic gastric environments. Therefore, efficacy may be decreased with histamine H2 blockers and proton pump inhibitors, with maximum absorption after a meal.27,28
Efficacy
Several pivotal trials have evaluated the efficacy of itraconazole for onychomycosis.29–40 Toenail and fingernail complete cure rates for onychomycosis are 47% and 14% with mycological cure rates of 61% and 54%, respectively.41 A multi-center study assessed intermittent itraconazole therapy for 683 onychomycosis patients in two groups (group A, 635 patients, 400mg/day for 1 week a month for 3 months) (group B, 48 patients, fingernail involvement, 400mg/day for 1 week a month for 2 months). Group A achieved clinical and mycological cure rates of 91.4% and 85.3% for fingernails, respectively and 89.0% and 68.4% for toenails, respectively. Group B achieved clinical and mycological cure rates of 84.4% and 77.1% for fingernails respectively.42 In a prospective study by Ramos-e-Silva et al including 72 patients treated with itraconazole (200mg twice a day for seven days a month) for 4 months for onychomycosis, 77.8% of patients were culture negative at treatment completion. Group 1 (0 to 5.9 mm of healthy nail) had an average clinical improvement of 88.36% and group 2 (more than 6mm of healthy nail) had an average improvement of 36.64% (P<0.001).43 In a meta-analysis of 1741 toenail onychomycosis patients treated with continuous itraconazole (200mg/day for 3 months), 12-month clinical cure rate, clinical response rate, and mycological cure rates were 52%±9, 86%±2, and 74%±3%, respectively.44
Safety
Common adverse effects of itraconazole include headache (10%), rhinitis (9%), upper respiratory tract infections (8%), sinusitis, injury (both 7%), diarrhea, dyspepsia, flatulence, abdominal pain, dizziness, rash (all 4%), cystitis, urinary tract infection, liver function abnormality, myalgia, nausea (all 3%), increased appetite, constipation, gastritis, gastroenteritis, pharyngitis, asthenia, fever, pain, tremor, herpes zoster, and abnormal dreaming (2%).45 In the aforementioned trial by Ramos-e-Silva et al43 including 72 onychomycosis patients, headache, nausea, and abdominal pain occurred in 0.05% of patients. Another prospective study with 646 onychomycosis patients treated with itraconazole (200mg twice daily for one week a month for 2–3 months) reported adverse events in 4.6% of patients, most commonly nausea, anorexia, gastrointestinal upset, malaise, and xerostomia. Two patients had mild, asymptomatic, transient elevations of liver enzymes that returned to normal after treatment cessation. Two patients developed edema.46 More serious, rare side effects include hypertriglyceridemia, elevated transaminases, and hepatic injury.41 Liver enzyme monitoring is recommended before treatment initiation and every 4–6 weeks during treatment.
Itraconazole may rarely lead to adverse cardiovascular events and should be avoided in patients with evidence of ventricular dysfunction, such as congestive heart failure (CHF) or a history of CHF.45 A retrospective study of adverse events related to itraconazole using the FAERS database between September 1991-April 2001 identified 58 cases of CHF, though 43 of these patients had risk factors such as concomitant hypertension, coronary artery disease, or valvular heart disease that may confound this association.47 Therefore, it is advisable to consult a cardiologist before initiating itraconazole in patients with risk factors for heart disease, such as diabetes mellitus, history of a cerebrovascular event, or hypertension.41
Special Populations
HIV
As oral itraconazole absorption is pH dependent, HIV patients with achlorhydria and mucosal damage may experience decreased absorption.27 Itraconazole should be prescribed with caution in HIV patients taking protease inhibitors due to the possibility of medication interactions. A 34-year-old HIV patient taking saquinavir and ritonavir who began itraconazole 100mg twice daily, increased to 200mg twice daily, for disseminated histoplasmosis developed cheilitis, pruritus, and a widespread eczematous reaction which resolved upon itraconazole discontinuation.48 Itraconazole may be safe in this population, though monitoring for adverse reactions is warranted.
Diabetics
Onychomycosis affects up to one-third of diabetic patients, particularly those over the age of 65 years.49 Itraconazole has less than 0.03% renal excretion, and therefore may be prescribed for diabetics with renal impairment. In a prospective, randomized trial involving 27 diabetic patients with onychomycosis receiving itraconazole 200mg twice daily for one week a month for 3 months, only one patient experienced itraconazole-associated elevation of liver function tests and withdrew from the study. Therefore, treatment with itraconazole may be considered safe in the diabetic population with onychomycosis.49 Of note, most diabetic drugs and insulin are not metabolized by the same cytochrome P-450 enzymes as itraconazole.49
Pregnancy
Itraconazole is classified as FDA category C, meaning there were embryotoxic and teratogenic effects in animal studies, and therefore the human risk is possible. A prospective cohort study of 206 pregnant women exposed to itraconazole vs 207 women not exposed to itraconazole in the first trimester (mean dose 182.23–62.58, mean duration 6.9–6.4 days) found no differences in major congenital anomalies in the exposed group vs unexposed group (1.8% vs 2.1%), respectively. However, differences were noted in the rates of live births, spontaneous abortion, and termination of pregnancy (79.1% vs 91.8%), (11.2% vs 4.8%), (9.2% vs 3.4%), P<0.05), in exposed vs non-exposed, respectively.50 In a retrospective study with 229 pregnant women exposed to itraconazole, 198 during the first trimester, there was no increased risk of fetal malformation.51 Despite these findings, itraconazole should not be prescribed to pregnant women or women contemplating pregnancy.45 Contraception should be used during and for 2 months following treatment. Itraconazole is excreted into breast milk and should be avoided in lactating mothers.45
Children
Itraconazole is not FDA-approved for onychomycosis treatment in the pediatric population but has been used off-label with good efficacy. In an observational study of 12 children (10–17 years old) with severe, long-standing onychomycosis treated with itraconazole (200mg daily for 12 weeks), clinical cure was 83% and mycological cure was 83% in 2–4 months. No laboratory abnormalities or adverse events were reported.52 In a retrospective review of 17 pediatric patients (ages 3–14) treated with itraconazole pulse therapy for onychomycosis (5mg/kg/d for 1 week a month, 3–5 cycles), 94% of patients achieved clinical cure, with no reported adverse events.53 A systematic review with 77 pediatric onychomycosis patients treated with itraconazole showed complete clearance rates of 82.7% for continuous itraconazole and 68.4% for pulsed itraconazole.21 One case of ataxia was reported, although the dose was not specified.21 Reported adverse events in pediatric patients taking itraconazole (>1%) include gastrointestinal symptoms (nausea, vomiting, or abdominal pain), rash, dizziness, sleepiness, headache, and transaminase elevations, though these events are usually mild and transient and most children can continue their course of treatment.54
Drug Interactions
Itraconazole inhibits CYP-3A4, and medication interactions should be checked before prescribing. A retrospective analysis of adverse events associated with itraconazole from January 1993-June 2019 using the FAERS database found that drug-drug interactions were the most common adverse event.55 Life-threatening QT prolongation and death may occur if itraconazole is prescribed concurrently with the class IA antiarrhythmic quinidine or the class III anti-arrhythmic dofetilide.45 A retrospective study analyzing adverse drug events reported to the World Health Organization monitoring center between 2015–2019 identified 22 cases of torsades de pointes linked to itraconazole, with 19 of the cases associated with concurrent use of an interacting medication.56 Therefore, itraconazole should be avoided in patients with risk factors for QT prolongation or a secondary medication that could potentiate these effects. Itraconazole may increase concentrations of benzodiazepines alprazolam, diazepam, midazolam, and triazolam, exacerbating sedation.41 HMG-CoA reductase inhibitors such as atorvastatin, cerivastatin, lovastatin, and simvastatin are metabolized by CYP34A, and itraconazole may increase their plasma concentrations and potentiate rhabdomyolysis.55
Terbinafine
FDA approved in 1996 for the treatment of onychomycosis, terbinafine is now recommended as first-line onychomycosis treatment by the British Association of Dermatologists.4,57 Terbinafine, a synthetic allylamine, competitively inhibits squalene epoxidase, disrupting ergosterol synthesis and leading to intracellular squalene accumulation, which has fungicidal effects.58 In vitro, terbinafine has broad-spectrum antifungal activity against dermatophytes and some activity against yeasts and non-dermatophyte molds.59 Dosing is 250mg once daily for 6 weeks for fingernail onychomycosis and 12 weeks for toenail onychomycosis.60
Efficacy
Pivotal randomized control trials (RCT) demonstrate the efficacy of terbinafine for onychomycosis treatment,29–36,61–66 with mycological and complete cure rates of 70% and 38%, respectively.67 In the IRON-CLAD trial (N=504) of toenail onychomycosis in patients ages 18–75 years-old treated with terbinafine 250mg for 12 weeks, with or without nail debridement, efficacy was greater in the debridement group; mycological cure was 67.6% vs 62.6% (95% CI-4.0–1.3), clinical cure was 55.3% vs 52.3% (95% CI −6.0–1.2), and complete cure was 37.8% vs 32.5% (95% CI −3.0–1.4) with debridement vs without, respectively.68 In a Cochrane review of 10,200 patients with toenail onychomycosis, terbinafine was superior to placebo for clinical cure (RR 6.00, 95% CI 3.96–9.08) and mycological cure (RR 4.45, 95% CI 2.47–8.33) (complete cure not reported).69 In a meta-analysis of 20 RCTs on treatment of onychomycosis with terbinafine 250mg for 3–4 months, average mycological cure was 78%±6-76%±3 and average clinical cure was 69%±7-66%±5.70
Terbinafine showed superior efficacy to other oral antifungal medications in head-to-head trials. In the LION study of toenail onychomycosis, mycological cure rate (76%) was higher for terbinafine 250mg/day compared to itraconazole 400mg/day (38%) at 72 weeks (P<0.0001).30,62 In a 5-year follow-up study of 151 patients 18–75 years old with toenail onychomycosis, mycological cure for terbinafine was 46% versus 13% for itraconazole (P<0.001).29 In a meta-analysis comparing efficacy of continuous terbinafine for 12 weeks with intermittent itraconazole for toenail onychomycosis (taken 1 in every 4 weeks for 12 weeks), including 1181 patients, terbinafine treated vs itraconazole treated patients had higher mycological cure rates (OR 2.3, 95% CI, 1.7 to 3.0, P≤0.0001).71
Safety
Terbinafine undergoes hepatic first-pass metabolism followed by renal clearance, necessitating caution in patients with liver or kidney disease. Common adverse effects of terbinafine include headache (12.9%), gastrointestinal symptoms (5.6%), dyspepsia (4.3%), abdominal pain (2.4%), nausea (2.6%), flatulence (2.2%), dermatological symptoms including rash (5.6%), pruritus (2.8%), and urticaria (1.1%). Liver enzyme abnormalities occurred in 3.3% of patients, and taste and visual disturbances in 2.8% and 1.1%, respectively.60 In a retrospective study of adverse effects associated with terbinafine from January 1993 to June 2019 using the Federal Drug Administration Adverse Event Reporting System (FAERS) database (11,658 cases), “ageusia/dysgeusia” occurred in 12%, ‘AST/ALT elevations’ in 6%, and ‘pruritus’ in 6%.55
Taste alterations associated with terbinafine use are reported in 0.6–2.8% of patients, which is usually reversible.72,73 Though the exact mechanism is unclear, terbinafine-induced taste disturbance may be related to inhibition of cytochrome p-450-dependent enzymes, resulting in taste receptor dysfunction.74 In a post-marketing survey of 10,361 onychomycosis patients treated with oral terbinafine, reversible taste disturbances were reported in 0.6% of patients, with a mean taste recovery time of 42 days (range 2–186 days).75 A case-control study of 87 patients with terbinafine-induced taste loss and 362 controls taking terbinafine without taste loss identified low body mass index (BMI) (RR: 12.8, 95% CI 1.9–88.6), a history of taste loss (P<0.007), and older age (RR: 4.4, 95% CI 1.4–16.1) as risk factors.76
The mechanism of terbinafine associated hepatotoxicity is not fully understood, though one hypothesis posits that terbinafine metabolites bind to hepatobiliary proteins, inducing an immune reaction.77 Baseline liver function tests are recommended for all patients before treatment initiation. In a multicenter, prospective study from 1998–2007, out of 1198 patients with liver failure, only 3 cases were attributed to terbinafine.78 A retrospective analysis of 4309 patients taking terbinafine from 2006–2016 identified 4 cases of grade 2 or higher ALT elevations (0.2%) and 1 case of grade 2 or higher AST elevations (0.1%). Six patients (0.14%) discontinued treatment due to grade 1 to 3 LFT abnormalities, though transaminase elevations resolved after treatment discontinuation.79 Therefore, interim laboratory monitoring is not recommended in healthy adults taking terbinafine.
Although terbinafine induced hepatotoxicity is rare, patient fear and misinformation surrounding the medication is rampant. Terbinafine-induced liver injury occurs in 1 in 50,000–120,000 prescriptions, which is similar to the lifetime risk of an American death from an earthquake (1 in 130,171).80,81 In the National Library of Medicine Liver Toxicity Database, <1% of patients prescribed terbinafine experienced aminotransferase elevations.80 In a study evaluating 35 websites based on the accountability, quality, readability, display, support, and transparency of their terbinafine-related information, only 51.4% of websites had accurate information regarding terbinafine-related hepatotoxicity, and only 20.0% of websites mentioned that hepatotoxicity was rare.82,83 Therefore, understanding misconceptions that patients may have regarding terbinafine and educating patients to make informed treatment decisions may combat these falsehoods.
Pulse Dosing
Pulse dosing of terbinafine has been studied as a treatment for onychomycosis. In a randomized trial comparing pulse dosing (500mg daily, 1 week per month for 3 months) to continuous terbinafine (250mg daily for 3 months) with 306 onychomycosis patients, mycological cure (70.9% vs 58.7%, P=0.03, RR=1.21 (95% CI, 1.02–1.43)), clinical cure (44.6% vs 29.3%, P=0.007, RR=1.52 (95% CI, 1.11–2.07)), and complete cure (40.5% vs 28.0%; P=0.02, RR=1.45 (95% CI, 1.04–2.01)) were higher for continuous vs pulse dosing, with no difference in tolerability (P=0.65).63 Two identical, double-blind trials compared the efficacy of continuous vs pulse dosing of terbinafine for 2005 total onychomycosis patients. In trial I, complete cure rates for continuous and pulsed regimens were 25.6% vs 19.8% (−5.8%; 95% CI 11.8–0.07) and mycological cure rates were 57.9% vs 42.8% (−15.2%; 95% CI −22.2-(-)8.2), respectively. In trial II complete cure rates were 29.6% vs 23.7% (−5.0%; 95% CI −12-0.1) and mycological cure rates were 55.6% vs 50.5% (−5.1%; 95% CI −11.9–1.7) for continuous and pulsed courses, respectively. The rate and types of adverse events were similar in both groups.33 Therefore, since available data suggests higher efficacy for continuous dosing, with a similar side effect profile, continuous terbinafine dosing is preferred over pulse dosing for the treatment of onychomycosis.
Special Populations
Diabetics
Diabetes mellitus is a risk factor for developing toenail onychomycosis. In a multicenter study of 550 diabetic patients, there was a 2.77-fold greater prevalence of onychomycosis in diabetics vs the general population.84 Since terbinafine is renally cleared, it is recommended that kidney function is checked in all patients before initiating treatment. In a prospective randomized trial of patients with diabetes mellitus who had onychomycosis, patients treated with continuous terbinafine (250mg once daily for 12 weeks) vs pulsed itraconazole (200mg twice daily, 1 week on, 3 weeks off, for 12 weeks), showed mycological cure in 88.2% of terbinafine-treated patients vs 79.3% of itraconazole-treated patients (P>0.05), with no adverse events or medication interactions reported.85 A review analyzing published data regarding safety and efficacy of terbinafine in high-risk populations (HIV, diabetes, and immunosuppression) found no differences in mycological cure (64% vs 73%, respectively) or clinical cure (37% vs 45%, respectively) in diabetic vs nondiabetic patients (p-value not reported).86 Therefore, terbinafine is a safe and effective treatment option for this population.
HIV
Based on a multi-center observational study, the prevalence of onychomycosis in HIV-positive patients was 23.2% (N=500) vs 6.9% in immunocompetent patients (N=2001).87 In a prospective study including ten HIV-positive patients treated with 250mg terbinafine for onychomycosis over 12 weeks, mycological cure was achieved in 3 patients, with negative culture in seven patients at 48-week follow-up. One patient withdrew from this study due to a terbinafine-induced drug rash.88 In a second study, 21 HIV-positive patients with onychomycosis were treated with 250mg terbinafine for 16 weeks, with clinical cure achieved by 50%, partial improvement by 25%, with 2 therapeutic failures, and 7 mycological cures (4 withdrawals, 3 deaths due to HIV illness). Ten months following treatment, 13 participants achieved clinical and mycological cure. No drug-drug interactions, laboratory abnormalities, or serious adverse events related to terbinafine were reported.89 Therefore, if there are no other contraindications to its use, terbinafine may be safely used in this population.
Pregnancy and Lactation
There is insufficient data regarding teratogenicity and pregnancy outcomes associated with terbinafine and it is classified as FDA category B, meaning there are no adequate studies in humans, though animal studies have not demonstrated teratogenicity. Therefore, its use is not recommended during pregnancy. In a retrospective study of 942 terbinafine-exposed pregnancies, there was no association between oral or topical terbinafine use in pregnancy and risk of preterm birth, small for gestational age, low birth weight, or stillbirth.90 In a cohort study of 54 women exposed to terbinafine in the first trimester (mean duration 32±9 days), there was no increased risk of major malformations above the baseline risk of 1–3%.91 Terbinafine is excreted into breast milk, and treatment is not recommended while breastfeeding.4
Children
Based on a multicenter survey study of 2500 children, ages 0–18, the prevalence of onychomycosis in the North American pediatric population was 0.16%.92 Terbinafine is not FDA-approved for the treatment of onychomycosis in children but is often used off-label. In children, it is dosed by weight (<25kg: 125mg daily, 25–35 kg:187.5mg daily, >35kg: 250mg daily), with treatment duration identical to adult treatment duration (6 weeks for fingernails and 3 months for toenails).93 A systematic review with 52 pediatric onychomycosis patients demonstrated 78.8% complete cure rate with continuous terbinafine. Adverse events were acute urticaria (n = 1), agranulocytosis (n = 1), anorexia (n = 2), epigastric pain (n = 2), tiredness (n = 1), and vesiculopustular eruption (n = 1).21,94 In a retrospective studying assessing the frequency of abnormal laboratory tests in 1403 pediatric patients prescribed terbinafine for superficial fungal infections, only 1.7% had abnormal monitoring LFT results, and 4.4% had abnormal monitoring blood count. In all cases, values normalized within 4 weeks of treatment completion, will all abnormalities being mild (grade 1) and asymptomatic.95 Therefore, interval monitoring is not necessary for healthy children taking terbinafine for onychomycosis treatment.
Transplant Patients
Immunosuppressed transplant patients are at increased risk for developing onychomycosis, necessitating caution due to potential drug-drug interactions with terbinafine. Terbinafine influences the metabolism of cyclosporine, and drug level monitoring is recommended for patients taking these medications concominantly.96 A prospective study assessing treatment with terbinafine 250mg/day in 30 renal transplant patients with onychomycosis found a mycological cure rate of 85.7% at 12 weeks with no significant laboratory changes.97 In a prospective study of 11 transplant patients (kidney, heart, or lung) treated with 250mg terbinafine daily for 12 weeks for onychomycosis, cyclosporine levels decreased at 4, 8, and 12 weeks (P<0.05). Terbinafine was well tolerated, with no reported adverse events or signs of graft rejection.96 In a retrospective analysis of 13 kidney transplant recipients treated with terbinafine 250mg for onychomycosis for 12 weeks (9, 3, and 1 patients taking tacrolimus, cyclosporine or everolimus, respectively), 8 patients had 10–20% clinical improvement and 3 patients had 20–45% clinical improvement at 3 months post-treatment. A year after treatment completion, 9 patients were re-examined, and all had clinical and mycological cure. Three patients experienced adverse events during treatment including loss of taste (n=1), nausea and vomiting (n=1), and tachycardia (n=1). No laboratory abnormalities were reported during or following treatment.98 Treatment with terbinafine may be considered in transplant patients, though cyclosporine medication levels should be monitored throughout treatment.
Drug Interactions
Terbinafine inhibits CPY-2D6, but there are few associated drug-drug interactions and no absolute drug contraindications.41,99 Caffeine clearance is decreased by 19% and cyclosporine clearance is decreased by 15% with terbinafine.87 Terbinafine may increase plasma concentrations of imipramine, desipramine, amitriptyline, nortriptyline, and paroxetine, and may induce thirst, nausea, and vertigo when taken together with these medications.100 A case report of an older female prescribed the antipsychotic perphenazine along with terbinafine for onychomycosis developed extrapyramidal symptoms including akathisia and gait disturbances.100,101 Terbinafine also decreases clearance of beta-blockers. A 63-year-old man on metoprolol experienced symptomatic bradycardia after beginning terbinafine 250mg for onychomycosis.102 Therefore, it is important for physicians to perform thorough medication reviews prior to prescribing terbinafine and monitor for adverse drug-drug interactions throughout treatment.
Fluconazole
Fluconazole, an azole antifungal, inhibits lanosterol-14-α-demethylase, an enzyme important for the synthesis of ergosterol, a component of fungal cell walls.103 Fluconazole is approved for the treatment of onychomycosis in Europe.104 Although not FDA-approved for the treatment of onychomycosis, it is commonly prescribed off-label in the USA, Australia, and Canada.
Fluconazole is active against dermatophytes and candida species, but not non-dermatophyte molds, and may be detected in the nail plate within two weeks of initiating treatment.105,106
Efficacy
Based on a meta-analysis of 5 studies evaluating optimal fluconazole dosing for onychomycosis, taking into consideration mycological, clinical, and complete cure rates, as well as safety, the efficacies of 150mg, 300mg, and 450mg for 12–48 weeks duration were comparable, though 150mg for at least 6 months was recommended due to the fewest adverse events (Table 2).107 A prospective study of 74 onychomycosis patients treated with 150mg of fluconazole per week for 3–12 months showed a clinical response of 95% after three months and 96% after 11 months, with 52% of patients experiencing complete clinical cure. Mycological cure was achieved for 88% of fingernails and 79% of toenail.108 In a prospective study by Smith et al of 16 onychomycosis patients treated with 100mg of oral fluconazole daily for six months, all subjects had clinical improvement based on visual assessment score (VAS) (P=0.005).109 The cure rate, defined as improved appearance of nails and increased VAS score without evidence of relapse, was 64%.109 A prospective study of 11 patients treated with 300mg of fluconazole once weekly for onychomycosis with concurrent use of a topical antifungal to the feet (econazole nitrate cream 1%, sulconazole nitrate cream 1%, ciclopirox olamine lotion 1%, or terbinafine cream 1%) reported 100% clinical cure in mean of 6 months for toenails and 3.7 months for fingernails, with concurrent resolution of all cases of tinea pedis.110
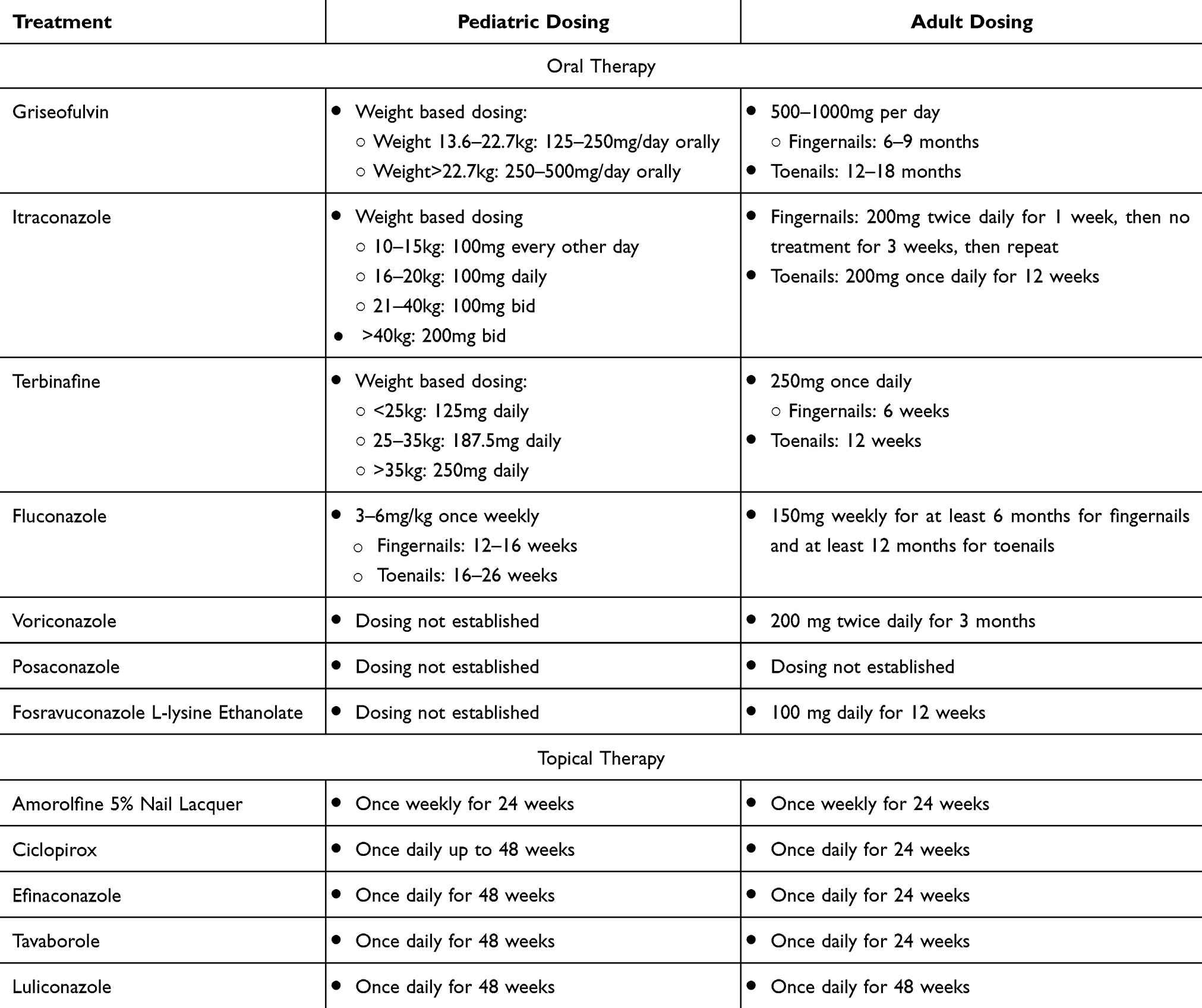 |
Table 2 Pediatric and Adult Dosing for Oral and Topical Onychomycosis Treatment |
Safety
In a clinical trial of 602 patients treated with fluconazole for systemic fungal infections, who were immunocompromised or receiving multiple concomitant medications, side effects occurring in more than 1% of patients included nausea (3.7%), headache (1.9%), skin rash (1.8%), vomiting (1.7%), abdominal pain (1.7%), and diarrhea (1.5%).111 In the aforementioned trial by Smith et. Al of 16 onychomycosis patients treated with 100mg fluconazole for six months, one patient withdrew from the study due to palpitations. Other reported adverse reactions in this study include facial pruritus, nocturia, fever, diaphoresis, and nausea. No patients had significant elevations in AST, ALT, or alkaline phosphatase levels after two months of treatment.109 In LiverTox, an online source for information on liver injury attributable to prescription and non-prescription medications, 1990–2017, there was only a single case of fatal hepatotoxicity (n=1) with fluconazole use, with transient, mild elevations of aminotransferases occurring in up to 5% of patients. In LiverTox, ALT elevations above 8 times the upper limit of normal occurred in less than 1% of patients.80
Special Populations
Pregnancy and Lactation
Fluconazole is categorized as an FDA category D due to evidence of risk in pregnancy.41 Administration of high-dose fluconazole in animal studies has been associated with congenital malformations.112 There have been 5 reported cases of newborns with craniofacial and skeletal abnormalities after first-trimester exposure to high-dose fluconazole (400–800mg daily).113 An analysis of 5382 pregnant women exposed to fluconazole and 13,246 unexposed women at weeks 7–22 of gestation showed an increased risk of spontaneous abortion compared to unexposed women (HR, 1.48; 95% CI, 1.23–1.77).114 An analysis of stillbirths (n=7832), congenital abnormalities (226,599), and spontaneous abortions (320,868) using data from the Quebec Pregnancy Cohort between 1998–2015 found that use of low-dose fluconazole (< 150mg) and high-dose fluconazole (>150mg) were both associated with an increased risk of spontaneous abortion (OR 2.23; OR 3.20).115 Exposure to low-dose fluconazole during the first trimester did not appear to increase the risk of major congenital malformations or stillbirth.115 Fluconazole is excreted into human breast milk and should be avoided in lactation.111
Children
Fluconazole is not FDA-approved for pediatric onychomycosis treatment, and no clinical trials have specifically assessed its safety and efficacy in this population. A systematic review including 6 pediatric onychomycosis patients treated with fluconazole reported that 66.7% of patients had complete cure with no reported adverse events.21
Drug Interactions
Fluconazole inhibits CYP-2C9 and CYP-3A4, therefore there are many potential drug-drug interactions. In a retrospective analysis of the FAERS database, the most common adverse event with fluconazole was drug-drug interactions. It may increase concentrations of sulfonylurea anti-diabetic agents, potentially leading to hypoglycemia.55 Fluconazole may also elevate warfarin levels, increasing the risk of bleeding. A 71-year-old female on warfarin who was prescribed fluconazole 200mg once daily for a candida wound infection experienced an increase of prothrombin time from 16 to 65 seconds and developed a sublingual hematoma.116 Fluconazole may cause QT interval prolongation, potentially causing torsade de pointes, therefore co-administration with any medication that may also prolong the QT interval is contraindicated.111 A comprehensive review of patient medications is essential prior to treatment initiation.
Voriconazole
Voriconazole, a synthetic triazole, was FDA-approved in 2002 for treating invasive aspergillosis, nonneutropenic candidemia, deep tissue candida infections, scedosporiosis, fusariosis, and esophageal candidiasis in refractory or intolerant patients.117–119 Its mechanism involves the inhibition of cytochrome P450 lanosterol 14a-demethylase (CYP51), leading to the accumulation of sterol precursors that disrupt fungal cell membrane integrity.118 In vitro and in vivo studies have demonstrated its efficacy against dimorphic fungi, yeasts, and opportunistic filamentous fungi, including dermatophytes.120
Efficacy
The effectiveness of voriconazole in treating onychomycosis has been supported by case reports. A 52-year-old male liver transplant patient, unresponsive to itraconazole and terbinafine, received voriconazole (200 mg twice daily) for 3 months, resulting in clinical cure. No recurrence was observed during the 8-month post-treatment monitoring period.117 In another case, a 30-year-old female with Scytalidium dimidiatum onychomycosis and cutaneous fungal infection underwent oral voriconazole therapy (400 mg twice a day loading dose, followed by 200 mg twice a day maintenance dose) for 3 months, achieving mycological cure at 12 weeks with some residual nail plate hyperpigmentation.121
Safety
Common side effects, as per the package insert, include fever (5.7%), nausea (5.4%), and rash (5.3%).122 Additional adverse effects encompass hepatotoxicity, visual disturbances, and phototoxicity. The overall incidence of transaminases greater than twice the upper limit of normal across therapeutic studies is noted at 12.4% (20/1655 patients) according to the manufacturer’s package insert. In a 2010 meta-analysis, transaminases greater than twice the upper limit of normal occurred in up to 20% of voriconazole-treated patients, which often did not necessitate therapy discontinuation.122,123 Visual disturbances, such as altered color discrimination and blurred vision, may manifest in the first week of therapy but typically diminish over time. Patients starting therapy in an outpatient setting should be cautious about driving due to potential visual disturbances. Additionally, patients are advised to avoid direct sunlight to prevent photosensitivity reactions.124 For onychomycosis patients, it is recommended to obtain liver function tests, kidney function assessments, and complete blood counts before initiating treatment.
Special Populations
Pregnancy and Lactation
Voriconazole is categorized as FDA category D.125 A case report detailed the successful use of voriconazole in a 28-year-old pregnant woman at 16 weeks of gestation for invasive aspergillosis without maternofetal adverse effects.125 However, the manufacturer reports embryotoxic/teratogenic effects in rabbits and rats at doses 0.3 and 6 times the recommended human dose, which may result in cleft palate, hydronephrosis, reduced ossification, and fetal mortality.125
Children
Voriconazole, a broad-spectrum triazole antifungal, is FDA-approved for patients 2 years and older with invasive aspergillosis, candidemia in non-neutropenic patients, deep tissue candida infections, esophageal candidiasis, and serious fungal infections or refractory to other therapies. However, its efficacy, safety, and dosing in the pediatric onychomycosis population have not been established.
Liver Failure
For patients with mild to moderate hepatic impairment (Child-Pugh class A and B), voriconazole dosage should be reduced by 50%. Close monitoring for potential drug toxicity is advised. In severely hepatic impaired patients (Child-Pugh class C), it is recommended to avoid voriconazole.118
Renal Failure
Metabolism of voriconazole occurs in the liver, and therefore, the oral form does not necessitate dose adjustment in patients with renal impairment. However, it is advised to conduct creatinine and renal function tests before and during treatment.118
Drug Interactions
Since voriconazole undergoes metabolism through hepatic cytochrome P450 enzymes, it is necessary to assess potential drug interactions before prescribing. Contraindications include coadministration with ritonavir, rifampin, St. John’s wort, carbamazepine, or long-acting barbiturates.126
Posaconazole
Posaconazole, an itraconazole analog with a 1.3-dioxolone backbone, was FDA-approved in 2006 for treating invasive aspergillosis, oropharyngeal candidiasis, and resistant oropharyngeal candidiasis. It is not approved for onychomycosis or superficial fungal infections, though it has been used off label.118,127 Posaconazole is a synthetic triazole and inhibits fungal 14α-ergosterol demethylase, exhibiting broad-spectrum activity against various fungi, including strains resistant to fluconazole, Cryptococcus neoformans, Trichosporon species, Zygomycetes, and dermatophytes.127
Efficacy
In a phase 2B RCT with 200 onychomycosis patients aged 18–75 by Elewski et al, six treatment regimens were randomized, including posaconazole (oral suspension) at 100, 200, or 400 mg once daily for 24 weeks. All posaconazole arms had a significantly greater proportion of patients with complete cure at week 48 compared to placebo (P<0.012). Posaconazole 200 mg/24 weeks and 400 mg/24 weeks achieved numerically higher clinical cure rates (54.1% and 45.5%) than terbinafine (37%), though no statistically significant differences were observed. All posaconazole arms significantly differed from placebo in achieving negative mycology results at week 48 (P<0.001).128 In a case report, a patient with severe dermatophytosis due to CARD9 deficiency, unresponsive to multiple antifungal treatments, achieved complete clinical remission of skin and nail lesions with 3 months of posaconazole therapy (400mg bid for 1 month, followed by 200mg tid for 2 months), and continued posaconazole for 8 months led to complete clinical remission.129
Safety
Common adverse reactions to posaconazole include diarrhea, nausea, fever, vomiting, headache, coughing, and hypokalemia.130 In Elewski et al’s RCT, 24% of patients experienced treatment-related adverse events, with diarrhea (3%), nausea (3%), and dizziness and headache (2%) being the most reported. Eleven patients discontinued treatment due to treatment-related adverse events, primarily related to liver function (4%), abdominal pain (0.5%), asthenia, dizziness, and somnolence (0.5%).128 In a network meta-analysis of 21 studies assessing the efficacy of monotherapy for dermatophyte toenail onychomycosis, posaconazole at 200 mg daily for 24 weeks had a higher likelihood of discontinuation due to any AE compared to terbinafine and continuous itraconazole therapies.131
Special Populations
Pregnancy and Lactation
Prescribing posaconazole (pregnancy category C) to pregnant women or nursing mothers should be avoided unless the benefits outweigh the risks.118
Children
Posaconazole lacks FDA approval for children under 13 but has been used off-label for those with cystic fibrosis. Due to limited data on safety and efficacy in this age group, it is not recommended for onychomycosis treatment in children.132
Liver Failure
As per Livertox, 2–12% of posaconazole users experience transient, mild, and asymptomatic elevations in serum aminotransferase levels. These elevations are typically self-limited and rarely necessitate discontinuation of the medication.80 Regular liver function tests should be conducted at the beginning and throughout posaconazole therapy.130
HIV
A 64-year-old HIV-positive patient, unresponsive to itraconazole and terbinafine, achieved onychomycosis treatment success with posaconazole 800mg daily for 1 week each month for four months. Clinical and mycological cures were attained, and the patient remained relapse-free during a 1-year and 4-month follow-up period. No adverse events were observed.133
Drug Interactions
Posaconazole inhibits CYP3A4 and is contraindicated with the following drugs: sirolimus, CYP3A4 substrates (pimozide, quinidine, HMG-CoA reductase inhibitors, and ergot alkaloids).130
Fosravuconazole L‐lysine Ethanolate
Fosravuconazole L-lysine ethanolate (F-RVCZ), a ravuconazole (RVCZ) prodrug developed for improved pharmacokinetics and bioavailability compared to RVCZ, is approved for onychomycosis treatment in Japan (not in the USA).118 F-RVCZ achieves 100% bioavailability after oral administration, along with excellent skin and nail tissue retention.134,135 The antifungal mechanism of RVCZ involves ergosterol biosynthesis inhibition, potent against a broad spectrum of dermatophytes and pathogenic fungi, including Trichophyton, Candida, Aspergillus, and Cryptococcus.136,137
Efficacy
In a Phase III RCT by Watanabe et al including 153 patients with onychomycosis, F-RVCZ (100 mg) showed a higher complete cure rate at week 48 (59.4%) compared to placebo (5.8%) (P<0.001), with a mycological cure rate of 82.0% vs 20.0% for placebo (P<0.001).136 A prospective study including 37 elderly patients using F-RVCZ (100mg) for 12 weeks resulted in a substantial decrease in percentage nail plate involvement from 86.6% to 28.1% (P<0.01), with a clinical cure rate of 29.7%.134 In a retrospective study by Inoue et al including 36 patients, F-RVCZ (100mg) taken daily for an average of 11.3 weeks showed clinical cure in 11.1% and 33.3% at 24 and 48 weeks.138
Safety
In the study by Inoue et al, adverse events led to treatment discontinuation in 16.6% of cases, with elevated liver enzymes (13.8%) and nausea/abdominal discomfort (2.7%). Six patients withdrew from treatment due to adverse events.138 In the study by Watanabe et al, abdominal discomfort was the most common adverse event (4.0%) with F-RVCZ. Laboratory abnormalities included increased liver function test values, with γ‐GT elevations in 15.8%, ALT in 8.9%, AST in 7.9%, and blood alkaline phosphatase in 2.0%. All laboratory abnormalities were mild to moderate and resolved after treatment completion.136
Special Populations
Clinical data are not available on RVCZ use in children, pregnant women, and nursing mothers. No clinical information is available for dose adjustment in patients with hepatic and renal impairment.118
Drug Interactions
RVCZ demonstrates decreased inhibition of CYP3A4 compared to itraconazole. Additionally, it exhibits negligible inhibitory effects on CYP2C8, CYP2C19, CYP2D6, CYP1A2, and CYP2C9, and therefore has minimal concern for drug interactions.134,135
Topical Therapy
Amorolfine 5% Nail Lacquer
Amorolfine 5% Nail Lacquer, a morpholine derivative that inhibits ergosterol synthesis, gained European approval in 1991 and is approved for onychomycosis treatment in Australia, Brazil, Russia, Germany, and the UK, though it is not approved for the treatment of onychomycosis in the United States or Canada.139 The concentration increases from 5% to 27% with solvent evaporation.140 Treatment duration varies (6–12 months) based on infection severity, site, and nail plate growth. Application involves filing and cleansing the nail, and clinical/mycological assessment every 3 months is recommended until cure is achieved.140 Amorolfine is dosed weekly and may improve patient compliance compared to daily ciclopirox.139
Efficacy
In a retrospective study including 53 Neoscytalidium dimidiatum-related onychomycosis cases treated twice weekly with 5% amorolfine nail lacquer, 89.3% achieved mycological cure, and 50% achieved complete cure in a median time of 112 and 176 days, respectively.141 Another prospective study by Reinel et al142 with 456 patients using amorolfine 5% nail lacquer for up to 6 months for onychomycosis showed complete cure rates of 54.2% (twice weekly) vs 46.0% (once weekly), with mycological cure rates at 76.1% and 70.6% for twice and once weekly dosing, respectively.142 Additionally, in a randomized trial of 160 patients comparing once and twice-weekly amorolfine 5% treatment for 6 months for onychomycosis, mycological cure rates were 71.2% and 75.3%, and complete cure rates were 46.1% and 61.8% after 3 months post-treatment, once and twice weekly, respectively.143
Safety
Common side effects of amorolfine include burning, itching, redness, irritation, and pain.139 In a randomized trial by Reinel et al,142 only 4 out of 456 patients reported mild local irritation. Plasma levels of amorolfine were undetectable (below 0.5 ng/mL) in all 19 patients tested.
Special Populations
Pregnancy and Lactation
Amorolfine, at doses ≥10 mg/kg/day, caused increased resorptions in pregnant rats and rabbits (Category B3), suggesting embryotoxicity. The impact on human embryotoxicity is unclear, with no ongoing human trials, and the package insert advises against its use during pregnancy or breastfeeding.144
Children
Amorolfine is not licensed for children under 12 in Europe. However, a case report describes the successful treatment of a 16-month-old with onychomycosis, using 5% amorolfine nail lacquer once a week for 12 weeks, then once every two weeks for another 12 weeks. No recurrence or adverse events were reported during a half-year follow-up.145
Ciclopirox
Ciclopirox, a synthetic hydroxypyridone, chelates metal-dependent enzymes, interfering with critical metabolic and energy-producing processes in microbial cells. It has broad spectrum activity against dermatophytes, yeast, and non-dermatophyte molds, as well as gram-positive and gram-negative bacteria, including resistant staphylococcus aureus strains.146 Ciclopirox nail lacquer topical solution 8%, was approved by the FDA in 1999 for the treatment of mild to moderate onychomycosis without lunular involvement in immunocompetent patients.147 It is recommended that the medication is removed weekly with acetone and has higher efficacy when accompanied by weekly clippings and debridement.4 The lacquer’s concentration gradient allows penetration of all nail layers. It exceeds the minimum inhibitory concentration for fungal species within 24 hours of application, with minimal systemic absorption.140,148 As the lacquer evaporates, the concentration gradient increases from 8% to 34%, enhancing penetration. The prolonged contact period between the nail and the active ingredient contributes to its efficacy.149
Efficacy
Two identical RCTs, each with over 200 subjects, evaluated ciclopirox nail lacquer topical solution 8% applied daily for 48 weeks compared to a placebo vehicle for onychomycosis. In study I, mycological cure rates were 29% for active drug vs 11% for placebo (P=0.002), and in study II the mycological cure rate was for active drug 36% vs 9% for placebo (P<0.001).150 In an open, non-comparative study of 36 patients with onychomycosis following a 9-month regimen of ciclopirox, 22% had complete cure of the toenails, while 14% experienced marked clinical improvement with complete mycological cure.151 Per package insert, mycological cure rates for toenail onychomycosis are 29–36%, with complete cure rates 5.5–8.5% (Table 3).4
 |
Table 3 Toenail Onychomycosis Cure Rates for Oral and Topical Treatment |
Combination therapy of ciclopirox with a systemic antifungal medication for onychomycosis was evaluated in a randomized study of eighty patients. Patients received either oral terbinafine 250mg/day for 16 weeks or a combination of oral terbinafine 250mg/day for 16 weeks plus topical ciclopirox daily for 9 months, with mycological cure rates of 88.2% for the combination therapy group vs 64.7% for terbinafine‐only group (p<0.05). No significant difference was noted in the complete cure rate (67.6% terbinafine only vs 50% combination, P>0.05)).152
Safety
Due to minimal systemic absorption, ciclopirox nail lacquer topical solution 8% demonstrates a minimal side effect profile. In the two aforementioned clinical trials, the most commonly reported mild effect was mild, transient irritation. Overall, 1.8% of patients using ciclopirox nail lacquer topical solution 8% reported nail changes as an adverse event, including nail discoloration, nail shape changes, and ingrown toenails.153 A retrospective study of adverse events due to ciclopirox using the FAERS database found that 10.2% of patients experienced application site discoloration.55 Other reported adverse events include localized burning, periungual erythema, and application site reactions.4
Special Populations
Pregnancy and Lactation
Ciclopirox is classified as FDA category B. While animal studies have not reported maternal toxicity, fetotoxicity, or teratogenicity, there have been no human studies.91 It should not be used in pregnant women.91 There is limited data regarding ciclopirox use during breastfeeding, therefore women should not use ciclopirox during lactation.
Children
Ciclopirox is FDA-approved for onychomycosis treatment in children 12 years and older. In a prospective, vehicle-controlled study of 35 pediatric patients receiving ciclopirox daily for 32 weeks for onychomycosis, 70% of patients in the ciclopirox group achieved mycological cure (negative culture) vs 20% in the vehicle group (P=0.31), and 60% achieved effective treatment (IGA score of 2 or less plus negative culture) vs 20% in the vehicle group (P=0.06) at week 12. Those with poor response to vehicle were crossed over to active drug at week 12. Reversible nail discoloration was the only reported adverse event, which resolved after treatment.154
Diabetic Patients
In an observational study, 215 diabetic patients who applied ciclopirox nail lacquer topical solution 8% daily for up to 6 months for onychomycosis, there was a reduction nail surface area involvement from 64.3% at baseline to 25.7% at 6 months.155 Another study including 49 type II diabetic patients with onychomycosis receiving insulin or oral hypoglycemic therapy reported clinical improvement in 63.4% of patients using ciclopirox nail lacquer topical solution 8% for 48 weeks, with mycological cure in 54.3%.156 Ciclopirox may be used in individuals with diabetes and exhibits comparable efficacy to the general population.
Efinaconazole
Efinaconazole 10% was FDA approved for treatment of onychomycosis in 2014. It is a triazole antifungal that inhibits ergosterol synthesis by blocking 14α-demethylase.157 It exhibits activity against dermatophytes, non-dermatophyte molds, and candida both in vitro and in vivo.4 The drug has a 7-fold higher unbound keratin fraction and a higher release rate from keratin than ciclopirox or amorolfine, which correlates with greater nail penetration and fungicidal activity.158,159
Efficacy
In a multicenter, open-label study involving 200 patients with onychomycosis treated with efinaconazole 10% daily for up to 72 weeks, complete cure rates were 31.1% and mycological cure rate were 61.6%.160 Pooled data from two phase III clinical trials with 1655 participants showed higher complete cure rates compared to vehicle (study 1:17.8% vs 3.3%, study 2: 15.2% vs 5.5%, P<0.001), and higher mycological cure rates for active drug compared to vehicle (study 1: 55.2% vs 16.8%, study 2: 53.4% vs 16.9%, P< 0.001).161 Patients concurrently treated for tinea pedis and onychomycosis had higher rates of complete and mycological cure rates (29.4% and 56.2%, respectively) compared to those who were not treated for tinea pedis (16.1% and 45.2%) (P < 0.001).162
Efinaconazole is effective in treating dermatophytomas, defined as subungual hyperkeratotic fungal masses oftentimes with biofilms. In an open-label study of 19 participants with dermatophytomas treated with efinaconazole daily for 48 weeks, mycological cure rate was 100% at week 52, with mean time to resolution of 16 weeks.163
Safety
Efinaconazole has demonstrated a favorable safety profile. In a prospective study of 62 patients receiving efinaconazole for 48 weeks for onychomycosis, the only treatment-related adverse event was ingrown toenails.164 In the aforementioned multicenter study, the most common adverse events were contact dermatitis (5%) and application site erythema (0.9%).160 Efinaconazole was not associated with erythema, swelling, burning, itching, or vesiculation.161 A retrospective study of adverse events associated with efinaconazole using the FAERS database 2014–2019 found that the most common adverse events were nail discoloration (10.6%), and skin erythema (8.6%).55 There were three case reports of confirmed allergic contact dermatitis due to efinaconazole.165–167
Special Populations
Pregnancy and Lactation
No clinical trials have evaluated efinaconazole’s efficacy in pregnant patients, therefore it is classified as FDA category C.159 Efinaconazole was detected in the milk of nursing rats in animal studies, warranting caution in lactating patients.159 Use of efinaconazole should be avoided in pregnancy and lactation.168
Children
Efinaconazole is FDA approved for treating onychomycosis in children ages 6 and older. In a multicenter, open-label study with 52 pediatric onychomycosis patients treated with efinaconazole 10% for 48 weeks, mycological cure rates were 65%, complete cure rates were 40%, and clinical cure rates were 42%. While there are no head to head studies, these cure rates are considerably higher than those in the adult cohort (complete cure: 15.2%-17.8%; mycological cure: 53.4–55.2%), which may be attributed to faster nail growth, shorter duration of infection, less nail damage over time, and shorter nail length, or trial design.169 The most common adverse events were local and included ingrown toenail (2.3%), application-site dermatitis (2.2%), application-site vesicles (1.6%), and application-site pain (1.1%).164
Diabetic Patients
Efinaconazole has shown efficacy for onychomycosis treatment in diabetic patients. A post-hoc analysis with 36 diabetic patients with onychomycosis reported mycological cure in 58.33% and clinical cure in 11.11%, with no association between hemoglobin A1C and efficacy endpoints.170 In a post-hoc analysis of two-phase III studies with diabetic patients with onychomycosis, efinaconazole demonstrated higher complete cure and mycological cure rates compared to vehicle at week 52 (13.0% vs 3.7%) and (56.5% vs 14.8%, P=0.016), respectively.171
Tavaborole
Tavaborole is a boron-based molecule and a highly specific fungal protein synthesis inhibitor. It targets fungal LeuRS, which inhibits tRNA function and inhibits fungal protein synthesis.172 Tavaborole topical solution 5% was FDA approved in 2014 for mild to moderate onychomycosis cases and is applied once daily for 48 weeks.173 Tavaborole penetrates the nail bed, with 250-fold greater penetration than ciclopirox in a cadaver study (P<0.05).174 In vitro studies have demonstrated that tavaborole has efficacy against Trichophyton rubrum, Trichophyton mentagrophytes, Epidermophyton floccosum, Microsporum audouinii, Malassezia furfur, Candida albicans, Fusarium solani, and Aspergillis fumigatus.172
Efficacy
In two phase III randomized, vehicle-controlled studies (n=1194) for onychomycosis patients aged 18 years or older, mycological cure rates were 31.1–35.9% vs 7.2–12.2% in the treatment vs vehicle groups and complete cure was 6.5–9.1% vs 0.5–1.5% in the treatment vs vehicle groups (P<0.001). Completely or almost clear nail cure rate was 26.1–27.5% with tavaborole vs 9.3–14.6% with vehicle (P<0.001).175 A post-hoc analysis of a Phase II randomized vehicle-controlled tavaborole trials for onychomycosis found that of 102 patients with dermatophytomas, 24.4% achieved complete resolution of dermatophytomas with tavaborole, vs 0% of patients treated with vehicle.176 A Cochrane review reported that tavaborole was superior to vehicle for onychomycosis treatment in achieving mycological cure (RR 3.40, 95% CI 2.34–4.93) and complete cure (RR 7.40, 95% CI 2.71–20.24), but noted a higher risk of adverse events compared to vehicle (RR 3.82, 95% CI 1.65–8.85) based on two studies.177
Safety
In the aforementioned phase III clinical trials, the adverse event rate in the tavaborole group was similar to the vehicle group. Most reported adverse events were mild or moderate in severity, including exfoliation (2.7%), erythema (1.6%), and dermatitis (1.3%).175 A meta-analysis of monotherapy treatment for onychomycosis ranked tavaborole 5% and placebo both as the least likely to cause adverse events.178 In a retrospective analysis of adverse events with topical onychomycosis medications using the FAERS database, the most common adverse events were application site erythema (16.4%), and application site pain (8.3%).153
Special Populations
Pregnancy and Lactation
Tavaborole is classified as FDA category C. In animal studies, exposure to high doses of tavaborole were associated with maternal toxicity, embryo-fetal resorption, skeletal malformations, and variations in skeletal ossification in rats and rabbits.41 Studies examining the risks of tavaborole in human pregnancy are lacking, and there is no data regarding the excretion of the drug into breast milk. Tavaborole should not be used during pregnancy or lactation.
Children
Tavaborole is FDA-approved for onychomycosis treatment in children ages 6 and older. In an open-label study of pediatric patients (age 6–17 years old) applying tavaborole for 48 weeks for onychomycosis treatment, 8.5% achieved complete cure at week 52, and 36.2% of patients achieved mycological cure.179 The most common adverse events were erythema (13%), scaling (11.1%), induration/edema (9.3%), pruritus (5.6%), and oozing and crusting (3.7%).179
Luliconazole
Luliconazole, an imidazole antifungal, gained approval in Japan in 2005 and from the FDA in November 2013 for treating interdigital tinea pedis, tinea cruris, and tinea corporis in individuals aged 18 and above.180 It is not yet approved for onychomycosis treatment in the US. Its mechanism of action is the inhibition of sterol 14a-demethylase.181 In both in vitro and in vivo studies, luliconazole demonstrated broad-spectrum activity against dermatophyte and non-dermatophyte pathogens, with lower minimum inhibitory concentrations compared to other antifungal drugs including terbinafine, bifonazole, clotrimazole, miconazole, and amorolfine hydrochloride.182 Notably, its low binding affinity for keratin allows easy release from the nail plate, facilitating penetration into the nail bed.182
Efficacy
In a double-blind, randomized study by Watanabe et al, 293 patients with onychomycosis received either luliconazole 5% nail solution or a vehicle once daily for 48 weeks. At week 48, luliconazole showed a significantly higher complete cure rate for onychomycosis (14.9%) compared to the vehicle (5.1%) (P=0.012). The luliconazole group also exhibited a higher rate of negative direct microscopy (45.4%) compared to the vehicle group (31.2%) (P=0.026).183
Safety
In the randomized trial by Watanabe et al,183 the most common adverse drug reactions with luliconazole included dry skin (6.7%), contact dermatitis (5.2%), paronychia (4.1%), and eczema (3.1%). Another open-label study with 24 patients using luliconazole 10% for onychomycosis for 36 days showed fewer side effects (11.3%) compared to the vehicle (16.9%). Application site reactions, including general reactions, pruritus, and pain, were reported in two patients with 1% luliconazole cream but did not require discontinuation.184 Additionally, one case of allergic contact dermatitis from luliconazole in a 59-year-old patient treated for tinea pedis has been reported.185
Special Populations
Pregnancy and Lactation
There is a lack of research on luliconazole’s safety during pregnancy and breastfeeding (FDA category C). Therefore, it is advisable to avoid using this drug in individuals in these populations.
Children
The FDA has expanded the approval of luliconazole cream for patients aged 12 and older with interdigital tinea pedis and tinea cruris, and for patients aged 2 and older with tinea corporis caused by Trichophyton rubrum and Epidermophyton floccosum. However, the safety and efficacy of the drug in children for onychomycosis have not been studied.
Conclusion
The landscape of onychomycosis treatment encompasses a range of oral and topical therapies. When a patient seeks treatment for confirmed positive onychomycosis, a shared dialogue between the patient and the physician is imperative. Before initiating treatment, a thorough evaluation of medical history and potential medication interactions is required for all patients. Additionally, patients are informed about the benefits and drawbacks of oral therapy, which commonly include gastrointestinal upset, rash, or headaches. It is crucial to discuss more serious but rare side effects such as hepatic injury. Addressing initial hesitations and dispelling misconceptions about the safety of oral therapy, particularly regarding the perceived risk of liver complications, is an essential aspect of patient education. For patients undergoing oral therapy, a baseline CBC/CMP should be conducted. Terbinafine is recommended as the first-line oral therapy (Figure 1). Topical treatment is reasonable for patients with few nails affected and/or limited nail plate involvement or for patients with contraindications to oral therapy. It is important to communicate the lower efficacy rates compared to oral therapy, along with potential side effects such as application site erythema. Of the FDA-approved topical treatments, efinaconazole has high efficacy rates.
 |
Figure 1 Algorithm of First-Line Therapeutic Recommendations for Confirmed Onychomycosis. Notes: Data from Lipner et al.57 Mild disease: <20% nail involvement, moderate disease: 21–60% nail involvement, severe disease: 61–100% nail involvement. All medication selections are based on medication with the highest mycological and clinical cure rates along with the lowest side effect profile. In all patients, age, severity of disease, interacting medications, comorbidities, and patient preferences must be considered. Tinea pedis must be evaluated for and treated in all patients with confirmed onychomycosis. In pregnant patients, wait until after pregnancy to treat. Avoid in breastfeeding patients. |
Abbreviations
FDA, Food and Drug Administration; RCT, Randomized Control Trial; RR, Relative Risk; FAERS, Federal Drug Administration Adverse Event Reporting System; BMI, Body Mass Index; CI, Confidence interval; HIV, Human Immunodeficiency Virus; CHF, Congestive Heart Failure; SLE, systemic lupus erythematosus.
Data Sharing Statement
Data sharing is not applicable to this article as no new data was created or analyzed in this study.
Funding
No funding was utilized in the preparation of this manuscript.
Disclosure
Eden Axler reports no conflicts of interest in this work. Dr Shari Lipner reports grants from Moberg Pharmaceuticals, Belle Torus Corporation; personal fees from Hoth Therapeutics, Ortho Dermatologics, and Eli Lilly, outside the submitted work. Dr. Lipner has also served as a consultant for Ortho-Dermatologics, Eli Lilly, Moberg Pharmaceuticals, and BelleTorus Corporation.
References
1. Veiga FF, Gadelha MC, da Silva MRT, et al. Propolis extract for onychomycosis topical treatment: from bench to clinic. Front Microbiol. 2018;9:779. doi:10.3389/fmicb.2018.00779
2. Nickles MA, Lio PA, Mervak JE. Complementary and alternative therapies for onychomycosis: a systematic review of the clinical evidence. Skin Appendage Disorders. 2022;8(4):269–279. doi:10.1159/000521703
3. Lipner S, Scher RK. Onychomycosis: current and future therapies. Cutis. 2014;93(2):60–63.
4. Lipner SR, Scher RK. Onychomycosis: treatment and prevention of recurrence. J Am Acad Dermatol. 2019;80(4):853–867. doi:10.1016/j.jaad.2018.05.1260
5. Bodman MA, Krishnamurthy K. Onychomycosis. In: StatPearls. StatPearls Publishing LLC.; 2023.
6. Elewski BE. Onychomycosis: pathogenesis, diagnosis, and management. Clin Microbiol Rev. 1998;11(3):415–429. doi:10.1128/cmr.11.3.415
7. Gupta AK, Shear NHO. Going for cure. Can Fam Physician. 1997;43:299–305.
8. Aris P, Wei Y, Mohamadzadeh M, Xia X. Griseofulvin: an Updated Overview of Old and Current Knowledge. Molecules. 2022;27(20):7034. doi:10.3390/molecules27207034
9. Baran R, Gupta AK, Piérard GE. Pharmacotherapy of onychomycosis. Expert Opin Pharmacother. 2005;6(4):609–624. doi:10.1517/14656566.6.4.609
10. Falotico JM, Lipner SR. Updated perspectives on the diagnosis and management of onychomycosis. Clin Cosmet Invest Dermatol. 2022;15:1933–1957. doi:10.2147/ccid.S362635
11. Olson JM, Troxell T. Griseofulvin. In: StatPearls. StatPearls Publishing LLC; 2023.
12. Ameen M, Lear JT, Madan V, Mohd Mustapa MF, Richardson M. British Association of Dermatologists’ guidelines for the management of onychomycosis 2014. Br J Dermatol. 2014;171(5):937–958. doi:10.1111/bjd.13358
13. Piérard GE, Arrese-Estrada J, Piérard-Franchimont C. Treatment of onychomycosis: traditional approaches. J Am Acad Dermatol. 1993;29(1):S41–5. doi:10.1016/s0190-9622(08)81836-1
14. Davies RR, Everall JD, Hamilton E. Mycological and clinical evaluation of griseofulvin for chronic onychomycosis. Br Med J. 1967;3:5563):464–8. doi:10.1136/bmj.3.5563.464
15. Griseofulvin. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. National Institute of Diabetes and Digestive and Kidney Diseases; 2012.
16. Redeker AG, Sterling RE, Bronow RS. Effect of griseofulvin in acute intermittent porphyria. JAMA. 1964;188(5):466–468. doi:10.1001/jama.1964.03060310066017
17. Watsky MS, Lynfield YL. Lupus erythematosus exacerbated by griseofulvin. Cutis. 1976;17(2):361–363.
18. Madhok R, Zoma A, Capell H. Fatal exacerbation of systemic lupus erythematosus after treatment with griseofulvin. Br Med J Clin Res Ed. 1985;291:6490):249–50. doi:10.1136/bmj.291.6490.249
19. Rosa FW, Hernandez C, Carlo WA. Griseofulvin teratology, including two thoracopagus conjoined twins. Lancet. 1987;1(8525):171. doi:10.1016/s0140-6736(87)92015-0
20. Ko EM, Lowry RB, Martin RH. Analysis of sperm karyotypes in a patient treated with griseofulvin. Arch Androl. 2007;53(3):157–160. doi:10.1080/01485010701314024
21. Gupta AK, Paquet M. Systemic antifungals to treat onychomycosis in children: a systematic review. Pediatr Dermatol. 2013;30(3):294–302. doi:10.1111/pde.12048
22. Sajeed M, Wei L, Murdan S. What can GP data tell us about the treatment of onychomycosis in the UK? Skin Health Dis. 2022;2(1):e84. doi:10.1002/ski2.84
23. Okino K, Weibert RT. Warfarin-griseofulvin interaction. Drug Intell Clin Pharm. 1986;20(4):291–293. doi:10.1177/106002808602000417
24. Katz HI. Systemic antifungal agents used to treat onychomycosis. J Am Acad Dermatol. 1998;38(5):S48–52. doi:10.1016/s0190-9622(98)70484-0
25. De Beule K, Van Gestel J. Pharmacology of itraconazole. Drugs. 2001;61:27–37. doi:10.2165/00003495-200161001-00003
26. Ricardo JW, Lipner SR. Recommendations for treatment of nail lichen planus during the COVID-19 pandemic. Dermatol Ther. 2020;33(4):e13551. doi:10.1111/dth.13551
27. Slain D, Rogers PD, Cleary JD, Chapman SW. Intravenous itraconazole. Ann Pharmacother. 2001;35(6):720–729. doi:10.1345/aph.10262
28. Rodgers P, Bassler M. Treating onychomycosis. Am Fam Physician. 2001;63(4):663–72, 677–8.
29. Sigurgeirsson B, Olafsson JH, Steinsson JB, Paul C, Billstein S, Evans EG. Long-term effectiveness of treatment with terbinafine vs itraconazole in onychomycosis: a 5-year blinded prospective follow-up study. Arch Dermatol. 2002;138(3):353–357. doi:10.1001/archderm.138.3.353
30. Sigurgeirsson B, Billstein S, Rantanen T, et al. Study: efficacy and tolerability of continuous terbinafine (Lamisil) compared to intermittent itraconazole in the treatment of toenail onychomycosis. Lamisil vs. Itraconazole in Onychomycosis. Br J Dermatol. 1999;141(56):5–14. doi:10.1046/j.1365-2133.1999.00008.x
31. Gupta AK, Konnikov N, Lynde CW. Single-blind, randomized, prospective study on terbinafine and itraconazole for treatment of dermatophyte toenail onychomycosis in the elderly. J Am Acad Dermatol. 2001;44(3):479–484. doi:10.1067/mjd.2001.110874
32. De Backer M, De Keyser P, De Vroey C, Lesaffre E. A 12-week treatment for dermatophyte toe onychomycosis: terbinafine 250 mg/day vs. itraconazole 200 mg/day--a double-blind comparative trial. Br J Dermatol. 1996;134(46):16–17. doi:10.1111/j.1365-2133.1996.tb15653.x
33. Sigurgeirsson B, Elewski BE, Rich PA, et al. Intermittent versus continuous terbinafine in the treatment of toenail onychomycosis: a randomized, double-blind comparison. J DermatolTreat. 2006;17(1):38–44. doi:10.1080/09546630500504713
34. Bräutigam M. Terbinafine versus itraconazole: a controlled clinical comparison in onychomycosis of the toenails. J Am Acad Dermatol. 1998;38(5):S53–6. doi:10.1016/s0190-9622(98)70485-2
35. Ranawaka RR, Nagahawatte A, Gunasekara TA, Weerakoon HS, de Silva SH. Randomized, double-blind, comparative study on efficacy and safety of itraconazole pulse therapy and terbinafine pulse therapy on nondermatophyte mold onychomycosis: a study with 90 patients. J DermatolTreat. 2016;27(4):364–372. doi:10.3109/09546634.2015.1119781
36. Degreef H, Del Palacio A, Mygind S, Ginter G, Pinto Soares A, Zuluaga de Cadena A. Randomized double-blind comparison of short-term itraconazole and terbinafine therapy for toenail onychomycosis. Acta Derm Venereol. 1999;79(3):221–223. doi:10.1080/000155599750011020
37. Maddin S, Quiring J, Bulger L. Randomized, placebo-controlled, Phase 3 study of itraconazole for the treatment of onychomycosis. J Drugs Dermatol. 2013;12(7):758–763.
38. Odom RB, Aly R, Scher RK, et al. A multicenter, placebo-controlled, double-blind study of intermittent therapy with itraconazole for the treatment of onychomycosis of the fingernail. J Am Acad Dermatol. 1997;36(2):231–235. doi:10.1016/s0190-9622(97)70286-x
39. Zhang L, Xu H, Shi Y, Yu J, Tao Y, Li X. An exploration of the optimum dosage and number of cycles of itraconazole pulse therapy for severe onychomycosis. Mycoses. 2018;61(10):736–742. doi:10.1111/myc.12799
40. Havu V, Brandt H, Heikkilä H, et al. A double-blind, randomized study comparing itraconazole pulse therapy with continuous dosing for the treatment of toe-nail onychomycosis. Br J Dermatol. 1997;136(2):230–234.
41. Ricardo JW, Lipner SR. Safety of current therapies for onychomycosis. Expert Opin Drug Saf. 2020;19(11):1395–1408. doi:10.1080/14740338.2020.1829592
42. Haneke E, Abeck D, Ring J. Safety and efficacy of intermittent therapy with itraconazole in finger- and toenail onychomycosis: a multicentre trial. Mycoses. 1998;41(11–12):521–527. doi:10.1111/j.1439-0507.1998.tb00716.x
43. Ramos-e-Silva M, Marques SA, Gontijo B, Zaitz C, Campbell I, Veloso ST. Efficacy and safety of itraconazole pulse therapy: Brazilian multicentric study on toenail onychomycosis caused by dermatophytes. J Eur Acad Dermatol Venereol. 1998;11(2):109–116. doi:10.1111/j.1468-3083.1998.tb00762.x
44. Gupta AK, De Doncker P, Scher RK, et al. Itraconazole for the treatment of onychomycosis. Int J Dermatol. 1998;37(4):303–308. doi:10.1046/j.1365-4362.1998.00360.x
45. Sporanox (itraconazole) capsules. PriCara; 2023. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020083s040s041s044lbl.pdf.
46. Wang DL, Wang AP, Li RY, Wang R. Therapeutic efficacy and safety of one-week intermittent therapy with itraconazole for onychomycosis in a Chinese patient population. Dermatology. 1999;199(1):47–49. doi:10.1159/000018177
47. Ahmad SR, Singer SJ, Leissa BG. Congestive heart failure associated with itraconazole. Lancet. 2001;357(9270):1766–1767. doi:10.1016/s0140-6736(00)04891-1
48. MacKenzie-Wood AR, Whitfeld MJ, Ray JE. Itraconazole and HIV protease inhibitors: an important interaction. Med J Aust. 1999;170(1):46–47. doi:10.5694/j.1326-5377.1999.tb126872.x
49. Albreski DA, Gross EG. The safety of itraconazole in the diabetic population. J Am Podiatr Med Assoc. 1999;89(7):339–345. doi:10.7547/87507315-89-7-339
50. De Santis M, Di Gianantonio E, Cesari E, Ambrosini G, Straface G, Clementi M. First-trimester itraconazole exposure and pregnancy outcome: a prospective cohort study of women contacting teratology information services in Italy. Drug Saf. 2009;32(3):239–244. doi:10.2165/00002018-200932030-00006
51. Bar-Oz B, Moretti ME, Bishai R, et al. Pregnancy outcome after in utero exposure to itraconazole: a prospective cohort study. Am J Obstet Gynecol. 2000;183(3):617–620. doi:10.1067/mob.2000.105962
52. Ginter G. Mycoses in Children, Systemic Treatment. Acta Derm Venereol. 1998;7(98):3–4.
53. Huang PH, Paller AS. Itraconazole pulse therapy for dermatophyte onychomycosis in children. Arch Pediatr Adolesc Med. 2000;154(6):614–618. doi:10.1001/archpedi.154.6.614
54. Gupta AK, Cooper EA, Ginter G. Efficacy and safety of itraconazole use in children. Dermatol Clin. 2003;21(3):521–535. doi:10.1016/s0733-8635(03)00030-5
55. Wang Y, Lipner SR. Retrospective analysis of adverse events with systemic onychomycosis medications reported to the United States food and drug administration. J DermatolTreat. 2021;32(7):783–787. doi:10.1080/09546634.2019.1708242
56. Salem M, Reichlin T, Fasel D, Leuppi-Taegtmeyer A. Torsade de pointes and systemic azole antifungal agents: analysis of global spontaneous safety reports. Glob Cardiol Sci Pract. 2017;2017(2):11. doi:10.21542/gcsp.2017.11
57. Lipner SR, Joseph WS, Vlahovic TC, et al. Therapeutic recommendations for the treatment of toenail onychomycosis in the US. J Drugs Dermatol. 2021;20(10):1076–1084. doi:10.36849/jdd.6291
58. Bhatia A, Kanish B, Badyal DK, Kate P, Choudhary S. Efficacy of oral terbinafine versus itraconazole in treatment of dermatophytic infection of skin - A prospective, randomized comparative study. Indian J Pharmacol. 2019;51(2):116–119. doi:10.4103/ijp.IJP_578_17
59. Garcia-Effron G, Gomez-Lopez A, Mellado E, Monzon A, Rodriguez-Tudela JL, Cuenca-Estrella M. In vitro activity of terbinafine against medically important non-dermatophyte species of filamentous fungi. J Antimicrob Chemother. 2004;53(6):1086–1089. doi:10.1093/jac/dkh228
60. LAMISIL (terbinafine hydrochloride) tablets. Novartis pharmaceuticals corporation; 2023.
61. Tavakkol A, Fellman S, Kianifard F. Safety and efficacy of oral terbinafine in the treatment of onychomycosis: analysis of the elderly subgroup in improving results in onychomycosis-concomitant lamisil and debridement (IRON-CLAD), an open-label, randomized trial. Am J Geriatr Pharmacother. 2006;4(1):1–13. doi:10.1016/j.amjopharm.2005.12.012
62. Evans EG, Sigurgeirsson B. Double blind, randomised study of continuous terbinafine compared with intermittent itraconazole in treatment of toenail onychomycosis. The LION Study Group. BMJ. 1999;318(7190):1031–1035. doi:10.1136/bmj.318.7190.1031
63. Warshaw EM, Fett DD, Bloomfield HE, et al. Pulse versus continuous terbinafine for onychomycosis: a randomized, double-blind, controlled trial. J Am Acad Dermatol. 2005;53(4):578–584. doi:10.1016/j.jaad.2005.04.055
64. Billstein S, Kianifard F, Justice A. Terbinafine vs. placebo for onychomycosis in black patients. Int J Dermatol. 1999;38(5):377–379. doi:10.1046/j.1365-4362.1999.00713.x
65. Svejgaard EL, Brandrup F, Kragballe K, et al. Oral terbinafine in toenail dermatophytosis. A double-blind, placebo-controlled multicenter study with 12 months’ follow-up. Acta Derm Venereol. 1997;77(1):66–69. doi:10.2340/0001555555776669
66. Bräutigam M, Nolting S, Schopf RE, Weidinger G. German randomized double-blind multicentre comparison of terbinafine and itraconazole for the treatment of toenail tinea infection. Br J Dermatol. 1996;134(46):18–21. doi:10.1111/j.1365-2133.1996.tb15654.x
67. Gupta AK, Stec N, Summerbell RC, et al. Onychomycosis: a review. J Eur Acad Dermatol Venereol. 2020;34(9):1972–1990. doi:10.1111/jdv.16394
68. Jennings MB, Pollak R, Harkless LB, Kianifard F, Tavakkol A. Treatment of toenail onychomycosis with oral terbinafine plus aggressive debridement: IRON-CLAD, a large, randomized, open-label, multicenter trial. J Am Podiatr Med Assoc. 2006;96(6):465–473. doi:10.7547/0960465
69. Kreijkamp-Kaspers S, Hawke K, Guo L, et al. Oral antifungal medication for toenail onychomycosis. Cochrane Database Syst Rev. 2017;7(7):Cd010031. doi:10.1002/14651858.CD010031.pub2
70. Gupta AK, Ryder JE, Johnson AM. Cumulative meta-analysis of systemic antifungal agents for the treatment of onychomycosis. Br J Dermatol. 2004;150(3):537–544. doi:10.1046/j.1365-2133.2003.05728.x
71. Trivedi NA, Shah PC. A meta-analysis comparing efficacy of continuous terbinafine with intermittent itraconazole for toenail onychomycosis. Indian J Dermatol. 2010;55(2):198–199. doi:10.4103/0019-5154.62746
72. Doty RL, Haxel BR. Objective assessment of terbinafine-induced taste loss. Laryngoscope. 2005;115(11):2035–2037. doi:10.1097/01.Mlg.0000181462.08683.0c
73. Doty RL, Bromley SM. Effects of drugs on olfaction and taste. Otolaryngol Clin North Am. 2004;37(6):1229–1254. doi:10.1016/j.otc.2004.05.002
74. Duxbury AJ, Oliver RJ, Pemberton MN. Persistent impairment of taste associated with terbinafine. Br Dent J. 2000;188(6):295–296. doi:10.1038/sj.bdj.4800461
75. O’Sullivan DP, Needham CA, Bangs A, Atkin K, Kendall FD. Postmarketing surveillance of oral terbinafine in the UK: report of a large cohort study. Br J Clin Pharmacol. 1996;42(5):559–565. doi:10.1111/j.1365-2125.1996.tb00110.x
76. Stricker BH, Van Riemsdijk MM, Sturkenboom MC, Ottervanger JP. Taste loss to terbinafine: a case-control study of potential risk factors. Br J Clin Pharmacol. 1996;42(3):313–318. doi:10.1046/j.1365-2125.1996.04105.x
77. Kyriakidis I, Tragiannidis A, Munchen S, Groll AH. Clinical hepatotoxicity associated with antifungal agents. Expert Opin Drug Saf. 2017;16(2):149–165. doi:10.1080/14740338.2017.1270264
78. Reuben A, Koch DG, Lee WM. Drug-induced acute liver failure: results of a U.S. multicenter, prospective study. Hepatology. 2010;52(6):2065–2076. doi:10.1002/hep.23937
79. Stolmeier DA, Stratman HB, McIntee TJ, Stratman EJ. Utility of laboratory test result monitoring in patients taking oral terbinafine or griseofulvin for dermatophyte infections. JAMA Dermatol. 2018;154(12):1409–1416. doi:10.1001/jamadermatol.2018.3578
80. National Institute of Diabetes and Digestive and Kidney Diseases. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. National Institute of Diabetes and Digestive and Kidney Diseases; 2012.
81. Vanderweil SG, Yang C, Pagani K, Chuprin J, Bernhard J, Harris JE. Assessing risk amid uncertainty inside and outside the dermatology clinic. J Am Acad Dermatol. 2023;89:864–866. doi:10.1016/j.jaad.2023.06.038
82. Ishack S, Miller RC, Lipner SR. Insights into the ”fear factor” regarding terbinafine-associated hepatoxicity in an assessment of online information. J Am Acad Dermatol. 2022;86(6):e269–e271. doi:10.1016/j.jaad.2022.02.006
83. Kang R, Lipner S. Evaluation of onychomycosis information on the internet. J Drugs Dermatol. 2019;18(5):484–487.
84. Gupta AK, Konnikov N, MacDonald P, et al. Prevalence and epidemiology of toenail onychomycosis in diabetic subjects: a multicentre survey. Br J Dermatol. 1998;139(4):665–671. doi:10.1046/j.1365-2133.1998.02464.x
85. Gupta AK, Gover MD, Lynde CW. Pulse itraconazole vs. continuous terbinafine for the treatment of dermatophyte toenail onychomycosis in patients with diabetes mellitus. J Eur Acad Dermatol Venereol. 2006;20(10):1188–1193. doi:10.1111/j.1468-3083.2006.01698.x
86. Cribier BJ, Bakshi R. Terbinafine in the treatment of onychomycosis: a review of its efficacy in high-risk populations and in patients with nondermatophyte infections. Br J Dermatol. 2004;150(3):414–420. doi:10.1046/j.1365-2133.2003.05726.x
87. Gupta AK, Ryder JE, Lynch LE, Tavakkol A. The use of terbinafine in the treatment of onychomycosis in adults and special populations: a review of the evidence. J Drugs Dermatol. 2005;4(3):302–308.
88. Nandwani R, Parnell A, Youle M, et al. Use of terbinafine in HIV-positive subjects: pilot studies in onychomycosis and oral candidiasis. Br J Dermatol. 1996;134(46):22–24. doi:10.1111/j.1365-2133.1996.tb15655.x
89. Herranz P, García J, De Lucas R, et al. Toenail onychomycosis in patients with acquired immune deficiency syndrome: treatment with terbinafine. Br J Dermatol. 1997;137(4):577–580. doi:10.1111/j.1365-2133.1997.tb03789.x
90. Andersson NW, Thomsen SF, Andersen JT. Exposure to terbinafine in pregnancy and risk of preterm birth, small for gestational age, low birth weight, and stillbirth: a nationwide cohort study. J Am Acad Dermatol. 2021;84(3):763–767. doi:10.1016/j.jaad.2020.10.034
91. Patel VM, Schwartz RA, Lambert WC. Topical antiviral and antifungal medications in pregnancy: a review of safety profiles. J Eur Acad Dermatol Venereol. 2017;31(9):1440–1446. doi:10.1111/jdv.14297
92. Gupta AK, Chang P, Del Rosso JQ, Adam P, Hofstader SL. Onychomycosis in children: prevalence and management. Pediatr Dermatol. 1998;15(6):464–471. doi:10.1046/j.1525-1470.1998.1998015464.x
93. Tosti A, Piraccini BM, Iorizzo M. Management of onychomycosis in children. Dermatol Clin. 2003;21(3):507–509. doi:10.1016/s0733-8635(03)00034-2
94. Feldstein S, Totri C, Friedlander SF. Antifungal therapy for onychomycosis in children. Clin Dermatol. 2015;33(3):333–339. doi:10.1016/j.clindermatol.2014.12.010
95. Wang Y, Lipner SR. Retrospective analysis of abnormal laboratory test results in pediatric patients prescribed terbinafine for superficial fungal infections. J Am Acad Dermatol. 2021;85(4):1042–1044. doi:10.1016/j.jaad.2021.01.073
96. Jensen P, Lehne G, Fauchald P, Simonsen S. Effect of oral terbinafine treatment on cyclosporin pharmacokinetics in organ transplant recipients with dermatophyte nail infection. Acta Derm Venereol. 1996;76(4):280–281. doi:10.2340/0001555576280281
97. Lee KH, Kim YS, Kim MS, Chung HS, Park K. Study of the efficacy and tolerability of oral terbinafine in the treatment of onychomycosis in renal transplant patients. Transplant Proc. 1996;28(3):1488–1489.
98. Moreno-Sabater A, Ouali N, Chasset F, et al. Severe onychomycosis management with oral terbinafine in a kidney transplantation setting: clinical follow-up by image analysis. Mycoses. 2021;64(3):309–315. doi:10.1111/myc.13220
99. Saarikoski T, Saari TI, Hagelberg NM, et al. Effects of terbinafine and itraconazole on the pharmacokinetics of orally administered tramadol. Eur J Clin Pharmacol. 2015;71(3):321–327. doi:10.1007/s00228-014-1799-2
100. Mikami A, Hori S, Ohtani H, Sawada Y. Analysis of the mechanism of prolonged persistence of drug interaction between terbinafine and amitriptyline or nortriptyline. Biol Pharm Bull. 2017;40(7):1010–1020. doi:10.1248/bpb.b16-01004
101. Park YM. Prolonged Drug-Drug Interaction between Terbinafine and Perphenazine. Psychiatry Invest. 2012;9(4):422–424. doi:10.4306/pi.2012.9.4.422
102. Bebawi E, Jouni SS, Tessier AA, Frenette AJ, Brindamour D, Doré M. A metoprolol-terbinafine combination induced bradycardia. Eur J Drug Metab Pharmacokinet. 2015;40(3):295–299. doi:10.1007/s13318-014-0205-x
103. Brown SJ. Efficacy of fluconazole for the treatment of onychomycosis. Ann Pharmacother. 2009;43(10):1684–1691. doi:10.1345/aph.1M165
104. Leung AKC, Lam JM, Leong KF, et al. Onychomycosis: an Updated Review. Recent Pat Inflamm Allergy Drug Discov. 2020;14(1):32–45. doi:10.2174/1872213x13666191026090713
105. Pakshir K, Kamali M, Nouraei H, Zomorodian K, Motamedi M, Mahmoodi M. Molecular characterization and antifungal activity against non-dermatophyte molds causing onychomycosis. Sci Rep. 2021;11(1):20736. doi:10.1038/s41598-021-00104-0
106. Gupta AK, Scher RK, Rich P. Fluconazole for the treatment of onychomycosis: an update. Int J Dermatol. 1998;37(11):815–820. doi:10.1046/j.1365-4632.1998.00564.x
107. Gupta AK, Drummond-Main C, Paquet M. Evidence-based optimal fluconazole dosing regimen for onychomycosis treatment. J DermatolTreat. 2013;24(1):75–80. doi:10.3109/09546634.2012.703308
108. Montero-Gei F, Robles-Soto ME, Schlager H. Fluconazole in the treatment of severe onychomycosis. Int J Dermatol. 1996;35(8):587–588. doi:10.1111/j.1365-4362.1996.tb03666.x
109. Smith SW, Sealy DP, Schneider E, Lackland D. An evaluation of the safety and efficacy of fluconazole in the treatment of onychomycosis. South Med J. 1995;88(12):1217–1220. doi:10.1097/00007611-199512000-00006
110. Assaf RR, Elewski BE. Intermittent fluconazole dosing in patients with onychomycosis: results of a pilot study. J Am Acad Dermatol. 1996;35(2):216–219. doi:10.1016/s0190-9622(96)90327-8
111. Diflucan (fluconazole) tablets. Pfizer Inc; 2023. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/020083s062lbl.pdf.
112. Zhang Z, Zhang X, Zhou YY, Jiang CM, Jiang HY. The safety of oral fluconazole during the first trimester of pregnancy: a systematic review and meta-analysis. Bjog. 2019;126(13):1546–1552. doi:10.1111/1471-0528.15913
113. Kaplan YC, Koren G, Bozzo P. Fluconazole exposure during pregnancy. Can Fam Physician. 2015;61(8):685–686.
114. Mølgaard-Nielsen D, Svanström H, Melbye M, Hviid A, Pasternak B. Association between use of oral fluconazole during pregnancy and risk of spontaneous abortion and stillbirth. JAMA. 2016;315(1):58–67. doi:10.1001/jama.2015.17844
115. Paquette VC, Elwood C. The safety of oral fluconazole therapy in pregnancy. Cmaj. 2019;191(7):E177–e178. doi:10.1503/cmaj.190079
116. Seaton TL, Celum CL, Black DJ. Possible potentiation of warfarin by fluconazole. Dicp. 1990;24(12):1177–1178. doi:10.1177/106002809002401207
117. Nofal A, Fawzy MM, El-Hawary EE. Successful treatment of resistant onychomycosis with voriconazole in a liver transplant patient. Dermatol Ther. 2020;33(6):e14014. doi:10.1111/dth.14014
118. Gupta AK, Talukder M, Venkataraman M. Review of the alternative therapies for onychomycosis and superficial fungal infections: posaconazole, fosravuconazole, voriconazole, oteseconazole. Int J Dermatol. 2022;61(12):1431–1441. doi:10.1111/ijd.15999
119. Scott LJ, Simpson D. Voriconazole: a review of its use in the management of invasive fungal infections. Drugs. 2007;67(2):269–298. doi:10.2165/00003495-200767020-00009
120. Perea S, Fothergill AW, Sutton DA, Rinaldi MG. Comparison of in vitro activities of voriconazole and five established antifungal agents against different species of dermatophytes using a broth macrodilution method. J Clin Microbiol. 2001;39(1):385–388. doi:10.1128/jcm.39.1.385-388.2001
121. Spriet I, Lambrecht C, Lagrou K, Verhamme B. Successful eradication of Scytalidium dimidiatum-induced ungual and cutaneous infection with voriconazole. Eur J Dermatol. 2012;22(2):197–199. doi:10.1684/ejd.2011.1616
122. Levine MT, Chandrasekar PH. Adverse effects of voriconazole: over a decade of use. Clin Transplant. 2016;30(11):1377–1386. doi:10.1111/ctr.12834
123. Wang JL, Chang CH, Young-Xu Y, Chan KA. Systematic review and meta-analysis of the tolerability and hepatotoxicity of antifungals in empirical and definitive therapy for invasive fungal infection. Antimicrob Agents Chemother. 2010;54(6):2409–2419. doi:10.1128/aac.01657-09
124. Johnson LB, Kauffman CA. Voriconazole: a new triazole antifungal agent. Clin Infect Dis. 2003;36(5):630–637. doi:10.1086/367933
125. Shoai Tehrani M, de Fontbrune F S, Roth P, et al. Case report of exposure to voriconazole in the second and third trimesters of pregnancy. Antimicrob Agents Chemother. 2013;57(2):1094–1095. doi:10.1128/aac.00899-12
126. VFEND (voriconazole) oral suspension. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/021266s032lbl.pdf.
127. Gupta AK, Tomas E. New antifungal agents. Dermatol Clin. 2003;21(3):565–576. doi:10.1016/s0733-8635(03)00024-x
128. Elewski B, Pollak R, Ashton S, Rich P, Schlessinger J, Tavakkol A. A randomized, placebo- and active-controlled, parallel-group, multicentre, investigator-blinded study of four treatment regimens of posaconazole in adults with toenail onychomycosis. Br J Dermatol. 2012;166(2):389–398. doi:10.1111/j.1365-2133.2011.10660.x
129. Jachiet M, Lanternier F, Rybojad M, et al. Posaconazole treatment of extensive skin and nail dermatophytosis due to autosomal recessive deficiency of CARD9. JAMA Dermatol. 2015;151(2):192–194. doi:10.1001/jamadermatol.2014.2154
130. Noxafil (posaconazole) Label. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/022003s018s020,0205053s002s004,0205596s001s003lbl.pdf
131. Gupta AK, Venkataraman M, Bamimore MA. Relative impact of traditional vs. newer oral antifungals for dermatophyte toenail onychomycosis: a network meta-analysis study. Br J Dermatol. 2023;189(1):12–22. doi:10.1093/bjd/ljad070
132. Lavigne S, Fisher BT, Ellis D, Zaoutis TE, Downes KJ. Posaconazole Administration in Hospitalized Children in the United States. J Pediatric Infect Dis Soc. 2019;8(5):481–484. doi:10.1093/jpids/piy119
133. Al-Hatmi AM, Bonifaz A, Calderón L, et al. Proximal subungual onychomycosis caused by Fusarium falciforme successfully cured with posaconazole. Br J Dermatol. 2015;173(1):253–255. doi:10.1111/bjd.13589
134. Noguchi H, Matsumoto T, Kimura U, et al. Fosravuconazole to treat severe onychomycosis in the elderly. J Dermatol. 2021;48(2):228–231. doi:10.1111/1346-8138.15651
135. Shimoyama H, Yo A, Sei Y, Kuwano Y. Treatment Outcome with Fosravuconazole for Onychomycosis. Mycopathologia. 2021;186(2):259–267. doi:10.1007/s11046-021-00540-6
136. Watanabe S, Tsubouchi I, Okubo A. Efficacy and safety of fosravuconazole L-lysine ethanolate, a novel oral triazole antifungal agent, for the treatment of onychomycosis: a multicenter, double-blind, randomized phase III study. J Dermatol. 2018;45(10):1151–1159. doi:10.1111/1346-8138.14607
137. Nakano M, Aoki Y, Yamaguchi H. Drug properties of fosravuconazole L-lysine ethanolate (NAILIN(®) Capsules 100 mg), a new oral azole therapeutic for onychomycosis: an analysis based on non-clinical and clinical trial data. Nihon Yakurigaku Zasshi. 2019;153(2):79–87. doi:10.1254/fpj.153.79
138. Inoue T, Watabe D, Tsunemi Y, Amano H. Outcome of fosravuconazole treatment for onychomycosis refractory to topical antifungal agents. J Dermatol. 2023;50(8):1014–1019. doi:10.1111/1346-8138.16824
139. Gupta AK, Ryder JE, Baran R. The use of topical therapies to treat onychomycosis. Dermatol Clin. 2003;21(3):481–489. doi:10.1016/s0733-8635(03)00025-1
140. Tabara K, Szewczyk AE, Bienias W, et al. Amorolfine vs. ciclopirox - lacquers for the treatment of onychomycosis. Postepy Dermatol Alergol. 2015;32(1):40–45. doi:10.5114/pdia.2014.40968
141. Bunyaratavej S, Leeyaphan C, Rujitharanawong C, Surawan TM, Muanprasat C, Matthapan L. Efficacy of 5% amorolfine nail lacquer in Neoscytalidium dimidiatum onychomycosis. J DermatolTreat. 2016;27(4):359–363. doi:10.3109/09546634.2015.1109029
142. Reinel D. Topical treatment of onychomycosis with amorolfine 5% nail lacquer: comparative efficacy and tolerability of once and twice weekly use. Dermatology. 2009;184(Suppl. 1):21–24. doi:10.1159/000247612
143. Reinel D, Clarke C. Comparative efficacy and safety of amorolfine nail lacquer 5% in onychomycosis, once-weekly versus twice-weekly. Clin Exp Dermatol. 1992;17 Suppl 1:44–49. doi:10.1111/j.1365-2230.1992.tb00278.x
144. Amorolfine 5% Medicated nail lacquer, package leaflet: information for the user. Available from: https://www.medicines.org.uk/emc/files/pil.7414.pdf.
145. Chen S, Ran Y-P, Dai Y-L, Lama J, Hu W-Y. Case of infantile onychomycosis successfully cured by 5% amorolfine nail lacquer. J Paediatr Child Health. 2014;50(11):933–934. doi:10.1111/jpc.12740
146. Bohn M, Kraemer KT. Dermatopharmacology of ciclopirox nail lacquer topical solution 8% in the treatment of onychomycosis. J Am Acad Dermatol. 2000;43(4 Suppl):S57–69. doi:10.1067/mjd.2000.109072
147. Geizhals S, Lipner SR. A timeline of onychomycosis therapy and future directions. Skinmed. 2020;18(6):367–371.
148. Bohn M, Kraemer K. The dermatopharmacologic profile of ciclopirox 8% nail lacquer. J Am Podiatr Med Assoc. 2000;90(10):491–494. doi:10.7547/87507315-90-10-491
149. Gupta AK, Baran R. Ciclopirox nail lacquer solution 8% in the 21st century. J Am Acad Dermatol. 2000;43(4 Suppl):S96–102. doi:10.1067/mjd.2000.109068
150. Gupta AK, Fleckman P, Baran R. Ciclopirox nail lacquer topical solution 8% in the treatment of toenail onychomycosis. J Am Acad Dermatol. 2000;43(4 Suppl):S70–80. doi:10.1067/mjd.2000.109071
151. Shemer A, Nathansohn N, Trau H, Amichai B, Grunwald MH. Ciclopirox nail lacquer for the treatment of onychomycosis: an open non-comparative study. J Dermatol. 2010;37(2):137–139. doi:10.1111/j.1346-8138.2009.00773.x
152. Avner S, Nir N, Henri T. Combination of oral terbinafine and topical ciclopirox compared to oral terbinafine for the treatment of onychomycosis. J DermatolTreat. 2005;16(5–6):327–330. doi:10.1080/09546630500420183
153. Wang Y, Lipner SR. Retrospective analysis of adverse events with topical onychomycosis medications reported to the United States food and drug administration. Arch Dermatol Res. 2020;312(8):581–586. doi:10.1007/s00403-020-02044-7
154. Seebacher C, Nietsch KH, Ulbricht HM. A multicenter, open-label study of the efficacy and safety of ciclopirox nail lacquer solution 8% for the treatment of onychomycosis in patients with diabetes. Cutis. 2001;68(2 Suppl):1.
155. Brenner MA, Harkless LB, Mendicino RW, Page JC. Ciclopirox 8% nail lacquer topical solution for the treatment of onychomycosis in patients with diabetes: a multicenter, open-label study. J Am Podiatr Med Assoc. 2007;97(3):195–202. doi:10.7547/0970195
156. Friedlander SF, Chan YC, Chan YH, Eichenfield LF. Onychomycosis does not always require systemic treatment for cure: a trial using topical therapy. Pediatr Dermatol. 2013;30(3):316–322. doi:10.1111/pde.12064
157. Tatsumi Y, Nagashima M, Shibanushi T, et al. Mechanism of action of efinaconazole, a novel triazole antifungal agent. Antimicrob Agents Chemother. 2013;57(5):2405–2409. doi:10.1128/aac.02063-12
158. Sugiura K, Sugimoto N, Hosaka S, et al. The low keratin affinity of efinaconazole contributes to its nail penetration and fungicidal activity in topical onychomycosis treatment. Antimicrob Agents Chemother. 2014;58(7):3837–3842. doi:10.1128/aac.00111-14
159. Lipner SR, Scher RK. Efinaconazole in the treatment of onychomycosis. Infect Drug Resist. 2015;8:163–172. doi:10.2147/idr.S69596
160. Iozumi K, Abe M, Ito Y, et al. Efficacy of long-term treatment with efinaconazole 10% solution in patients with onychomycosis, including severe cases: a multicenter, single-arm study. J Dermatol. 2019;46(8):641–651. doi:10.1111/1346-8138.14935
161. Elewski BE, Rich P, Pollak R, et al. Efinaconazole 10% solution in the treatment of toenail onychomycosis: two phase III multicenter, randomized, double-blind studies. J Am Acad Dermatol. 2013;68(4):600–608. doi:10.1016/j.jaad.2012.10.013
162. Gupta AK, Cernea M. How effective is efinaconazole in the management of onychomycosis? Expert Opin Pharmacother. 2016;17(4):611–618. doi:10.1517/14656566.2016.1146687
163. Wang C, Cantrell W, Canavan T, Elewski B. Successful treatment of dermatophytomas in 19 patients using efinaconazole 10% solution. Skin Appendage Disord. 2019;5(5):304–308. doi:10.1159/000495042
164. Gupta AK, Venkataraman M, Shear NH, Piguet V. Labeled use of efinaconazole topical solution 10% in treating onychomycosis in children and a review of the management of pediatric onychomycosis. Dermatol Ther. 2020;33(4):e13613. doi:10.1111/dth.13613
165. Fujimoto K, Yamaguchi H, Otsuka Y, Mayumi N, Saeki H. Contact dermatitis caused by efinaconazole and luliconazole. J Nippon Med Sch. 2021;88(3):253–257. doi:10.1272/jnms.JNMS.2021_88-312
166. Hirohata A, Hanafusa T, Mabuchi-Kiyohara E, Ikegami R. Contact dermatitis caused by efinaconazole solution for treatment of onychomycosis. Contact Dermatitis. 2015;73(3):190–192. doi:10.1111/cod.12414
167. Oiso N, Tatebayashi M, Kawada A. Allergic contact dermatitis caused by efinaconazole: positive patch test reactions up to 0.1% pet. Contact Dermatitis. 2017;76(1):53–54. doi:10.1111/cod.12643
168. Jublia (efinaconazole) topical solution, 10%. Valent Pharmaceuticals; 2023. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/203567s009lbl.pdf.
169. Eichenfield LF, Elewski B, Sugarman JL, et al. Efinaconazole 10% topical solution for the treatment of onychomycosis in pediatric patients: open-label Phase 4 study. J Am Acad Dermatol. 2021;84(4):1140–1142. doi:10.1016/j.jaad.2020.06.1004
170. Shofler D, Hamedani E, Seun J, Navarrete R, Thamby R, Harkless L. Efficacy and safety of efinaconazole 10% solution in the treatment of onychomycosis in diabetic patients. Clin Podiatr Med Surg. 2020;37(2):401–407. doi:10.1016/j.cpm.2019.12.015
171. Vlahovic TC, Joseph WS. Efinaconazole topical, 10% for the treatment of toenail onychomycosis in patients with diabetes. J Drugs Dermatol. 2014;13(10):1186–1190.
172. Elewski BE, Tosti A. Tavaborole for the treatment of onychomycosis. Expert Opin Pharmacother. 2014;15(10):1439–1448. doi:10.1517/14656566.2014.921158
173. Jinna S, Finch J. Spotlight on tavaborole for the treatment of onychomycosis. Drug Des Devel Ther. 2015;9:6185–6190. doi:10.2147/dddt.S81944
174. Hui X, Baker SJ, Wester RC, et al. In Vitro penetration of a novel oxaborole antifungal (AN2690) into the human nail plate. J Pharm Sci. 2007;96(10):2622–2631. doi:10.1002/jps.20901
175. Elewski BE, Aly R, Baldwin SL, et al. Efficacy and safety of tavaborole topical solution, 5%, a novel boron-based antifungal agent, for the treatment of toenail onychomycosis: results from 2 randomized phase-III studies. J Am Acad Dermatol. 2015;73(1):62–69. doi:10.1016/j.jaad.2015.04.010
176. Aly R, Winter T, Hall S, Vlahovic T. Topical tavaborole in the treatment of onychomycosis complicated by dermatophytoma: a post-hoc assessment of phase II subjects. J Drugs Dermatol. 2018;17(3):347–354.
177. Foley K, Gupta AK, Versteeg S, Mays R, Villanueva E, John D. Topical and device-based treatments for fungal infections of the toenails. Cochrane Database Syst Rev. 2020;1(1):Cd012093. doi:10.1002/14651858.CD012093.pub2
178. Gupta AK, Foley KA, Mays RR, Shear NH, Piguet V. Monotherapy for toenail onychomycosis: a systematic review and network meta-analysis. Br J Dermatol. 2020;182(2):287–299. doi:10.1111/bjd.18155
179. Rich P, Spellman M, Purohit V, Zang C, Crook TJ. Tavaborole 5% topical solution for the treatment of toenail onychomycosis in pediatric patients: results from a phase 4 open-label study. J Drugs Dermatol. 2019;18(2):190–195.
180. Khanna D, Bharti S. Luliconazole for the treatment of fungal infections: an evidence-based review. Core Evid. 2014;9:113–124. doi:10.2147/ce.S49629
181. Gregoriou S, Kyriazopoulou M, Tsiogka A, Rigopoulos D. Novel and investigational treatments for onychomycosis. J Fungi. 2022;8:1.
182. Scher RK, Nakamura N, Tavakkol A. Luliconazole: a review of a new antifungal agent for the topical treatment of onychomycosis. Mycoses. 2014;57(7):389–393. doi:10.1111/myc.12168
183. Watanabe S, Kishida H, Okubo A. Efficacy and safety of luliconazole 5% nail solution for the treatment of onychomycosis: a multicenter, double-blind, randomized phase III study. J Dermatol. 2017;44(7):753–759. doi:10.1111/1346-8138.13816
184. Jones T, Tavakkol A. Safety and tolerability of luliconazole solution 10-percent in patients with moderate to severe distal subungual onychomycosis. Antimicrob Agents Chemother. 2013;57(6):2684–2689. doi:10.1128/aac.02370-12
185. Shono M. Allergic contact dermatitis from luliconazole. Contact Dermatitis. 2007;56(5):296–297. doi:10.1111/j.1600-0536.2006.01023.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.