")
Back to Journals » Journal of Experimental Pharmacology » Volume 15
Antidiabetic Activities of 80% Methanol Extract and Solvent Fractions of Verbascum Sinaiticum Benth (Scrophulariaceae) Leaves in Mice
Authors Dereje B , Nardos A , Abdela J , Terefe L , Arega M , Yilma TM , Tesfaye T
Received 31 August 2023
Accepted for publication 2 November 2023
Published 9 November 2023 Volume 2023:15 Pages 423—436
DOI https://doi.org/10.2147/JEP.S437991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Beyene Dereje,1 Aschalew Nardos,2 Jemal Abdela,3 Lidet Terefe,2 Melese Arega,4 Terfo Mikre Yilma,5 Tilahun Tesfaye6
1Department of Pharmacology, School of Medicine, College of Medicine and Health Science, Dire Dawa University, Dire Dawa, Ethiopia; 2Department of Pharmacology, School of Pharmacy, College of Medicine and Health Science, Hawassa University, Hawassa, Ethiopia; 3Department of Pharmacology, School of Pharmacy, College of Health and Medical Science, Haramaya University, Harar, Ethiopia; 4Department of Pharmacy, Pawi Health Science College, Pawi, Benishangul, Ethiopia; 5Department of Medicinal Chemistry, School of Pharmacy, College of Health and Medical Science, Haramaya University, Harar, Ethiopia; 6Department of Pharmacy, College of Medicine and Health Science, Ambo University, Ambo, Ethiopia
Correspondence: Beyene Dereje, Email [email protected]; [email protected]
Background: Because of the scarcity, high cost, and severe side effects of current medications, it is necessary to discover novel, safe, and affordable anti-diabetic drugs. The current study was conducted to evaluate the antidiabetic activities of Verbascum sinaiticum Benth leaves in mice.
Methods: Leaf coarse powder was extracted with 80% methanol and then fractionated with n-hexane, ethyl acetate, and distilled water. The glucose-lowering effects of V. sinaiticum at 100, 200, and 400mg/kg were then studied. Glibenclamide was used as a positive control at a dose of 5 mg/kg. For oral glucose tolerance tests and hypoglycemia tests, Tween 2% was used as a negative control, while citrate buffer was used as a negative control for antihyperglycemic investigations. The results from the study were evaluated using one-way ANOVA, and then Tukey’s post hoc multiple comparison test was performed.
Results: Blood glucose levels were significantly reduced by the V. sinaiticum 80% methanol extract at 400 mg/kg (p< 0.05). The blood glucose levels were significantly lowered by the aqueous residue at 400 mg/kg (p< 0.05) and the ethyl acetate fractions at 200 mg/kg (p< 0.01) and 400 mg/kg (p< 0.001); however, none of the fraction extracts resulted in hypoglycemic shock in healthy mice. Higher glucose tolerance was seen in orally glucose-loaded mice after exposure to 80% methanol extracts at 200 and 400 mg/kg (p< 0.05), the aqueous residual fraction at 200 mg/kg (p< 0.01), and the ethyl acetate fraction at 200 and 400 mg/kg (p< 0.05). The ethyl acetate fraction at 200 and 400 mg/kg (p< 0.01), the 80% methanol extract at 400 mg/kg (p< 0.05) and the aqueous residue at 400 mg/kg (p 0.01) significantly lowered blood glucose levels in streptozotocin-induced diabetic mice.
Conclusion: The results of this study revealed that the 80% methanol extract and solvent fractions of V. sinaiticum Benth leaves are endowed with antidiabetic activity.
Keywords: antidiabetic, crude extract, hyperglycemia, hypoglycemia, solvent fraction, streptozotocin, Verbascum sinaiticum Benth
Introduction
A group of metabolic diseases known as diabetes mellitus (DM) are defined by high blood sugar levels brought on by the body’s inability to make or utilize insulin.1 Without treatment, the condition commonly progresses to chronic hyperglycemia, which is associated with long-term damage, dysfunction, and failure of a number of critical organs, including the eyes, kidneys, nerves, heart, and blood vessels.2 According to the International Diabetes Federation (IDF), there were 463 million diabetics in the world between the ages of 20 and 79 in 2019, 537 million by 2022, 643 million by 2030, and 783 million by 2045.3–5
Type 1 diabetes mellitus (T1DM), type 2 diabetes mellitus (T2DM), gestational diabetes mellitus, and other kinds of diabetes are the four categories into which the American Diabetes Association divides diabetes mellitus. The therapy choices for diabetes, whether it is T1DM or T2DM, differ based on the type of diabetes because it is a complex disease with variable clinical symptoms and disease development.6 The type and length of diabetes have an impact on the severity of symptoms. Some individuals with diabetes are asymptomatic, especially those with T2DM in its early stages. Other signs of severe hyperglycemia include polyuria, polydipsia, polyphagia, weight loss, and hazy eyesight, especially in young individuals.7,8
If uncontrolled diabetes is not handled, it can cause ketoacidosis or, in rare instances, nonketotic hyperosmolar syndrome, which can cause stupor, coma, and death.9,10 Insulin and common metabolites such as carbs, lipids, and proteins exhibit aberrant metabolic processes due to their role as anabolic hormones. The low levels of insulin required to achieve an adequate response or overcome insulin resistance in target tissues, primarily skeletal muscles, adipose tissue, and, to a lesser extent, the liver, are to blame for these metabolic abnormalities at the level of insulin receptors, the signal transduction system, and effector enzymes or genes.4,11,12
Diabetes mellitus is increasing in prevalence globally, and by 2023, it is predicted to have a significant economic impact, particularly in nations with scarce resources. Adults are involved in the majority of reported cases. People with type 1 diabetes mellitus (T1DM) are at risk of dying early because of the significant missing prevalence, which also reduces their chances of being saved and having their lives extended.13–15
An estimated 240 million people worldwide have undiagnosed diabetes, with 90% of them residing in low- and middle-income nations. In Africa, Southeast Asia, and the Western Pacific, more than half of diabetes cases go untreated. More than half of the 1.2 million children and teens with type 1 diabetes are under the age of 15. With a prevalence rate of 4.5, diabetes affects 23.6 million Africans between the ages of 20 and 79 and 1.9 million people between the ages of 20 and 79.16 Approximately 1.1 million Ethiopians live with undiagnosed diabetes, which has a prevalence rate of 3.3 and an annual cost of $104.3 per person. By 2022, approximately 6.5% of Ethiopians had type 2 diabetes.17
Diabetes is the world’s seventh-leading cause of death.18 When the body does not produce enough insulin or does not utilize it as effectively as it should, diabetes symptoms develop. Too much blood sugar persists in the bloodstream when there is not enough insulin or when cells cease reacting to insulin. Serious health issues such as heart disease, eye loss, and renal illness may come from this.19 Long-term consequences of diabetes include kidney, eye, foot, nerve, and major and minor blood artery damage, which can result in heart attacks and strokes.20
The good news is that there is a possibility of reducing the likelihood of long-term diabetic problems. It is important to check regularly to detect diabetes-related health risks early, and maintaining healthy blood pressure, cholesterol, blood sugar level, HbA1c, and waist circumference levels is also essential.18,21 Monitoring patients’ cognitive function, promoting vaccinations, caring for overweight patients, educating patients and caregivers, preventing comorbidities, and limiting the risk of repercussions are all part of managing diabetes mellitus.6,17
Despite the fact that there is no known cure for diabetes, antidiabetic medications that have recently received widespread approval allow for the best possible use of therapeutic agents to minimize its effects.22 The use of traditional plant medicine that controls hyperglycemia and averts diabetes-related complications has drawn much attention among the current therapeutic choices, such as hypoglycemic medications and insulin therapy, each of which has particular drawbacks for the management of diabetes.23 The current study’s objective is to examine the anti-diabetic properties of solvent fractions and the crude 80% methanol extract of V. sinaiticum Benth (Scrophulariaceae), which are traditionally believed to be used to treat diabetes.
Materials and Methods
Drugs, Chemicals, and Materials
The chemicals and drugs used in the study were methanol (Alpha Chemika): 99.8%; n-hexane (Sigma‒Aldrich): 99%; ethyl acetate (Sigma‒Aldrich): 99.8%; streptozotocin (Zanosar®, RIEMSER Pharma GmbH); anhydrous citric acid (Sigma‒Aldrich); sodium citrate (MSK); glibenclamide (Daonil®, Sanofi): 5 mg; Tween 80% (Atlas Chemie); glucose powder (Fufeng); and distilled water. The materials and equipment used to perform the present experiment were a rotary evaporator (Rotavapor® R-100 Buchi), measuring cylinder, volumetric flask, beaker, separatory funnel, plastic funnel, conical flask, mini orbital shaker (Stuart), oven (Memmert, Daihan scientific oven), precision balance (Cole Parmer), pH meter, analytical balance (ASR124/E, AS ONE), insulin syringe (Advin Healthcare), lyophilizer (Christ, Alpha 1–4 LDplus), refrigerator, aluminum foil, Whatman No. 1 filter paper (Hahnemuhle Dassel), mortar and pestle (U-Test), marker (Gxin), glucometer and strips (Precisa, FIABiomed™).
Plant Collection and Authentication
Fresh V. sinaiticum leaves were collected from Arsi, Dodota woreda (latitude: 8 19’ 60.00“N and longitude: 39 18’ 60.00” E) approximately 116 km from Addis Ababa on January 16 and 17, 2023. Authentication of the plant was performed by Mr Melaku Wondafrash, a taxonomist at the National Herbarium, College of Natural and Computational Sciences, Department of Biology, Addis Ababa University. A voucher specimen was stored there for future use with the voucher number BD-001, dated January 22, 2023.
Experimental Animals
Healthy adult Swiss albino mice of both sexes, with ages ranging from 6 to 8 weeks and weights varying from 25 to 37 g, were employed in the experiment. Streptozotocin-induced groups were used to assess antihyperglycemic effects, whereas normoglycemic groups were utilized to assess hypoglycemic effects and oral glucose tolerance tests. The mice were provided by the Ethiopian Public Health Institute (EPHI), and all the animals used for the present study were fed standard pellet diets and water ad libitum.24
Animals were kept and maintained under laboratory conditions at a temperature of 22 ± 2°C and a 12-hour light–dark cycle.25,26 The experimental animals were acclimatized to the working lab environment a week before the start of the experiment. All procedures and techniques used in the study were in accordance with the Guide for the Care and Use of Laboratory Animals.27
Preliminary Phytochemical Screening
The availability of secondary metabolites in the plant extract, such as flavonoids, terpenoids, saponins, alkaloids, tannins, steroids, phenolic compounds, and glycosides, was determined by standard procedures and reagents. The tests performed were Wagner’s test for alkaloids, alkaline reagent test for flavonoids, Keller–Kiliani test for cardiac glycosides, ferric chloride test for phenols, foam test for saponins, Salkowski’s test for steroids and triterpenoids, and Braymer’s test for tannins.28,29
Acute Oral Toxicity Test
Five female Swiss albino mice were evaluated for acute oral toxicity using the Organization for Economic Co-operation and Development (425) criteria.30 The mice were fasted but allowed full access to water for 3 hours before and one hour after the injection of an 80% methanol extract of V. sinaiticum leaves. The first mouse was then given 2000 mg/kg of the extract orally, and for the following 4 hours, it was watched for any indications of toxicity or indicators of mortality during the first 24 hours. Based on the results of the first animal, the extract was sequentially given to the following four mice at a dose of 2000 mg/kg because there was no acute toxicity or death within the first 24 hours. The following mice were kept separately and observed for 4 hours with a 30-minute break, followed by daily observation for two weeks for indications of toxicity.
The Crude 80% Methanol Extract and Fraction Preparation
The collected fresh V. sinaiticum Benth leaves were dried at room temperature away from direct sunlight and pounded into a coarse powder. Extraction was carried out with cold maceration for 72 hours at a sufficient volume of plant powder mixed with 80% methanol in a 1:10 (w/v) ratio.31 The samples were then filtered by Whatman No. 1 filter paper using a vacuum-pressurized suction filtration system. Methanol was removed using Rota vapor and evaporated at 40°C. The extract was then lyophilized by freeze-drying to eliminate the water and kept in a freezer at −40°C until it was needed in the experiment.32 Solvents, n-hexane and ethyl acetate, were used to fractionate 90 grams, and a separator funnel produced aqueous residue based on the polarity index of the solvents.
Induction of Diabetes Mellitus
Experimental diabetes was induced using streptozotocin (STZ) in Swiss albino mice. The drug was dissolved in prepared 0.1 M citrate buffer (pH = 4.5). The freshly prepared solution was then administered intraperitoneally at a dose of 60 mg/kg to mice, which were fasted overnight for 14 hours prior to administration.33 Thirty minutes after the administration of streptozotocin, animals were allowed to have free access to food and water. Additionally, animals were allowed to drink a five percent glucose solution 6 hours after the administration of the inducing agent streptozotocin for the next 24 hours to prevent death secondary to hypoglycemic shock.34 Then, animals were screened for the induction of diabetes 72 hours after the STZ injection. Mice that showed fasting blood glucose levels >200 mg/dl were included in the study as diabetic mice.35
Hypoglycemic Effect of V. Sinaiticum in Normoglycemic Mice
Common negative and positive controls were used for both the crude and fractional tests. Group I, the negative control, was given 2% Tween, group II, the positive control, was given glibenclamide 5 mg/kg, and groups III–V were given 100, 200, and 400 mg/kg of the crude 80% extracts, while groups III–XII were given fractional extracts at 100, 200, and 400 mg/kg of n-hexane, the ethyl acetate fraction, and aqueous residue orally after fasting mice for 6 hours to normoglycemic mice. Blood glucose was measured at 0 hours, 1 hour, 2 hours, 3 hours, and 4 hours after treatment.
Oral Glucose Tolerance Test of V. Sinaiticum Extracts
An oral glucose tolerance test was performed 14 hours after the mice had fasted overnight. Common negative and positive controls were used for both the crude and fractional tests. For the crude extracts, group I, the negative control, was given 2% Tween, group II, the positive control, was given glibenclamide 5 mg/kg, and groups III–V were given crude 80% methanol extracts at 100, 200, and 400 mg/kg, respectively, while groups III–XII were given fractional extracts at 100, 200, and 400 mg/kg of n-hexane, ethyl acetate, and aqueous residue. A glucose solution at 2000 mg/kg was administered orally 30 minutes after each dose. Blood glucose was measured at 0, 30, 60, and 120 minutes.
Antihyperglycemic Activity of V. Sinaiticum in Diabetic Mice
The effect of crude 80% methanolic extracts and solvent fractions of V. sinaiticum on STZ-induced diabetic mice was studied following a 14-hour overnight fast. A common negative control, positive control, and normal control were used for both the crude and fractional tests. Group I, the negative control, was given citrate buffer; group II, the normal control, was given Tween 2%; group III, the positive control, was given glibenclamide 5 mg/kg; groups IV–VI were given 100 mg/kg, 200 mg/kg, and 400 mg/kg of crude 80% methanol extract, respectively, while groups IV–XV were given 100 mg/kg, 200 mg/kg, and 400 mg/kg of the n-hexane fractions, ethyl acetate fractions, and aqueous residue fractions, respectively. Blood glucose was measured at 0 hour, 1 hour, 2 hours, 3 hours, and 4 hours after treatment.
Statistical Analysis
The two-tailed hypothesis was analyzed, and the results are presented as the mean ± SEM. One-way ANOVA was used to examine significant differences between treatments and controls, followed by multiple comparisons. Tukey’s post hoc tests were performed with IBM SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY, USA). A difference in mean values with p<0.05 was considered statistically significant.
Ethical Consideration
The experimental procedure of the study was granted permission by the Institutional Review Board of the College of Medicine and Health Science, Hawassa University, dated February 7, 2023, with “Protocol version No. 1, Ref. No. IRB/156/14”. All tests were conducted in a peaceful laboratory setting resembling an animal house. All investigations were carried out in compliance with the Guide for the Care and Use of Laboratory Animals.36
Results
The Yields of Extraction Procedures
A crude 80% methanol extract weighing 162.8 g (17.14%) was obtained from 950 grams of dried and medium-coarsely powdered V. sinaiticum Benth leaves. From the crude 80% methanol extract, 90 grams were fractionated. The aqueous residue fraction, the ethyl acetate fraction, and the n-hexane fraction had yields of 55.17%, 31.77%, and 10.93%, respectively.
Acute Oral Toxicity Tests
According to the results of the acute oral toxicity study, mice that were given up to 2000 mg/kg of an 80% methanol extract of V. sinaiticum Benth leaves did not die within the first 24 hours or over the next 14 days. Therefore, the oral LD50 exceeds 2 g/kg. The physical and behavioral examinations of the experimental mice showed no apparent acute poisoning symptoms, such as loss of appetite, tremors, hair erection, salivation, or diarrhea.
Preliminary Phytochemical Screening Results
The findings show that V. sinaiticum leaves contain alkaloids in both the CME and all solvent fractions. The CME and EAF contain flavonoids, glycosides, phenols, and tannins. The CME and ARF contain saponins. The CME and NHF include steroids. The EAF and NHF contain terpenoids (Table 1).
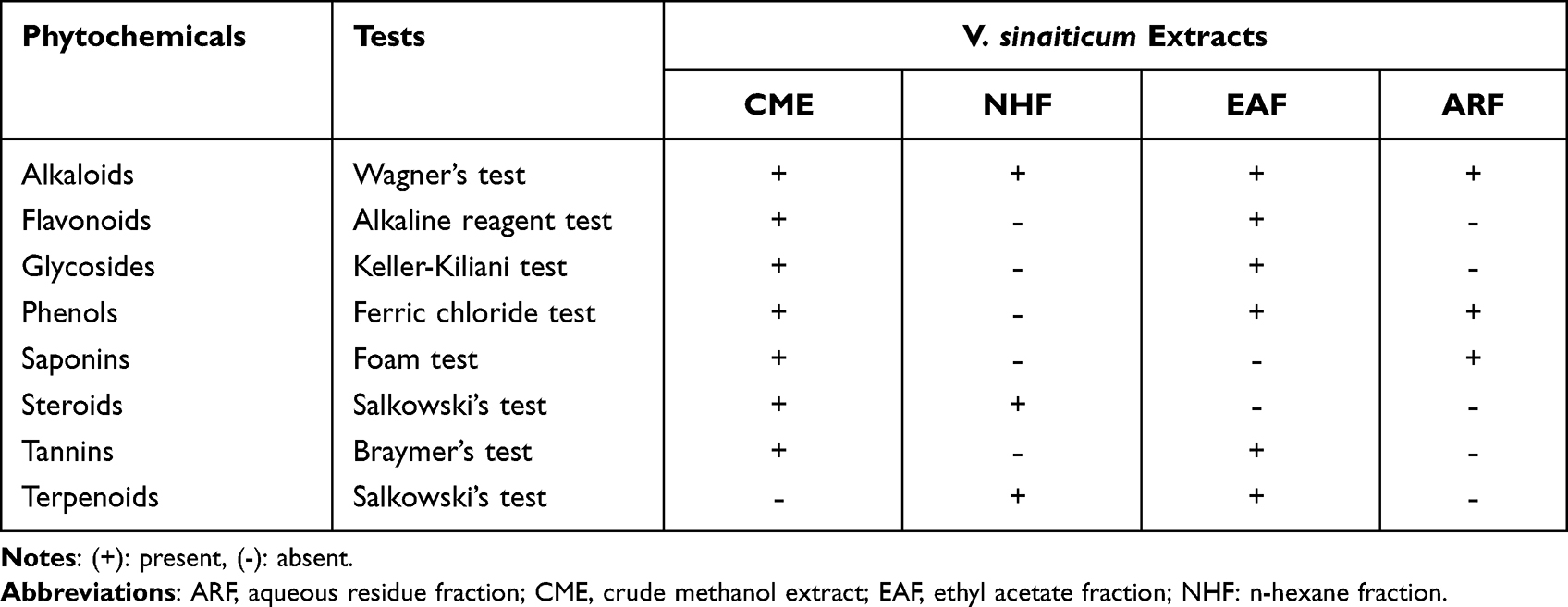 |
Table 1 Preliminary Phytochemical Screening of V. Sinaiticum Leaf Extracts |
Hypoglycemic Effect of V. Sinaiticum in Normoglycemic Mice
Effects of the Crude 80% Methanol Extracts
In comparison to CME 400 mg/kg, the standard drug GLC 5 mg/kg significantly reduced blood glucose levels within the first hour (p<0.05). At the second hour, the CME 400 mg/kg and GLC groups had significantly lower blood glucose levels than the CME 200 mg/kg group (p<0.05). When compared to 100 mg/kg at the third hour, CME 400 mg/kg significantly reduced blood glucose levels (p<0.01). Glibenclamide at 5 mg/kg (p<0.001) and CME at 400 mg/kg (p<0.01) significantly lowered the blood sugar level at the fourth hour. The largest percent reduction in BGL was achieved by GLC 5 mg/kg with 47.54%, followed by CME 400 mg/kg with a 39.77% drop in blood glucose (Table 2).
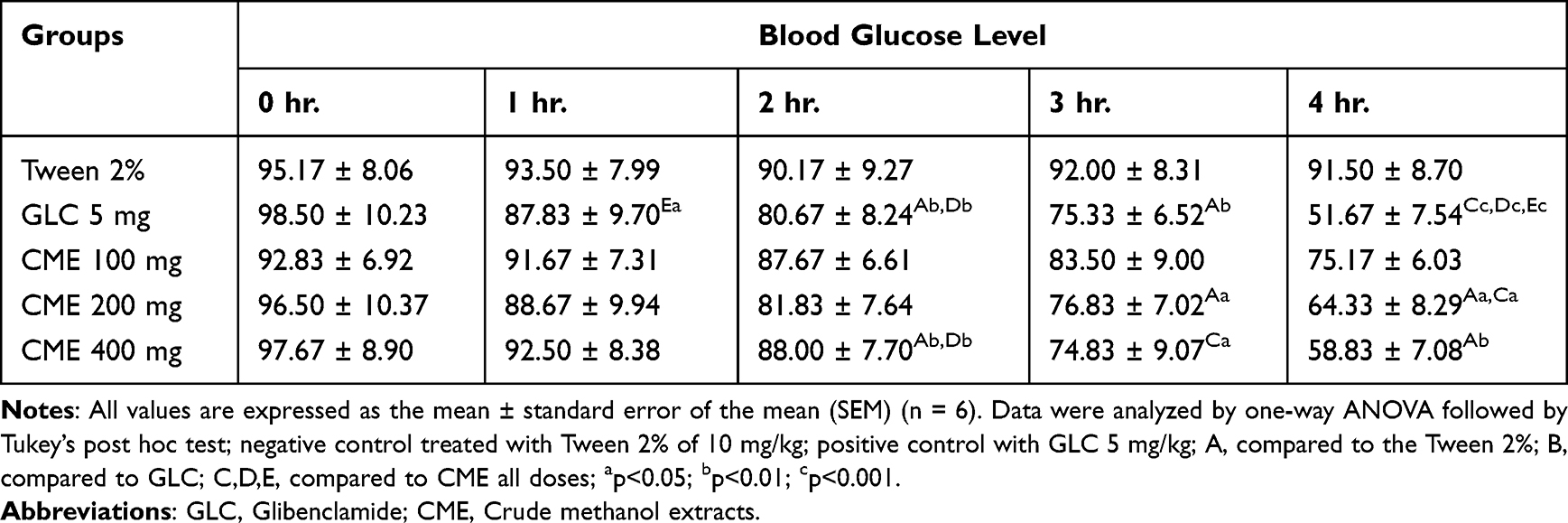 |
Table 2 Hypoglycemic Effect of the Crude 80% Methanol Extracts of V. Sinaiticum Leaves in Normoglycemic Mice |
Effects of the Solvent Fractions
Blood glucose levels at 0 hours showed no statistically significant difference. When compared to GLC, treatment with 200 mg/kg EAF, 400 mg/kg (p<0.001), and 400 mg/kg ARF (p<0.01) significantly reduced blood glucose levels in normoglycemic mice at 1 hour. Compared to mice who received an ARF at 400 mg/kg, mice treated with GLC and EAF at 200 mg/kg showed significantly lower glucose levels after 2 hours (p<0.05). In comparison to 100 mg/kg EAF, 400 mg/kg ARF and 200 mg/kg EAF considerably lowered blood glucose at the third hour (p<0.05).
At 4 hours, mice given GLC had significantly lower blood glucose levels than mice given EAF 200 mg/kg, ARF 200 mg/kg, and NHF 400 mg/kg (p<0.05, p<0.01, and p<0.001, respectively). Blood glucose levels were reduced by 47.54% overall by GLC, 39.26% by 400 mg/kg EAF, and 31.46% by 200 mg/kg EAF. The NHF 100 mg/kg produced unpredictable results, with significantly reduced blood glucose from 0 to 2 hours, an increase from 2 to 3 hours, and then a drop during the 4th hour (Table 3).
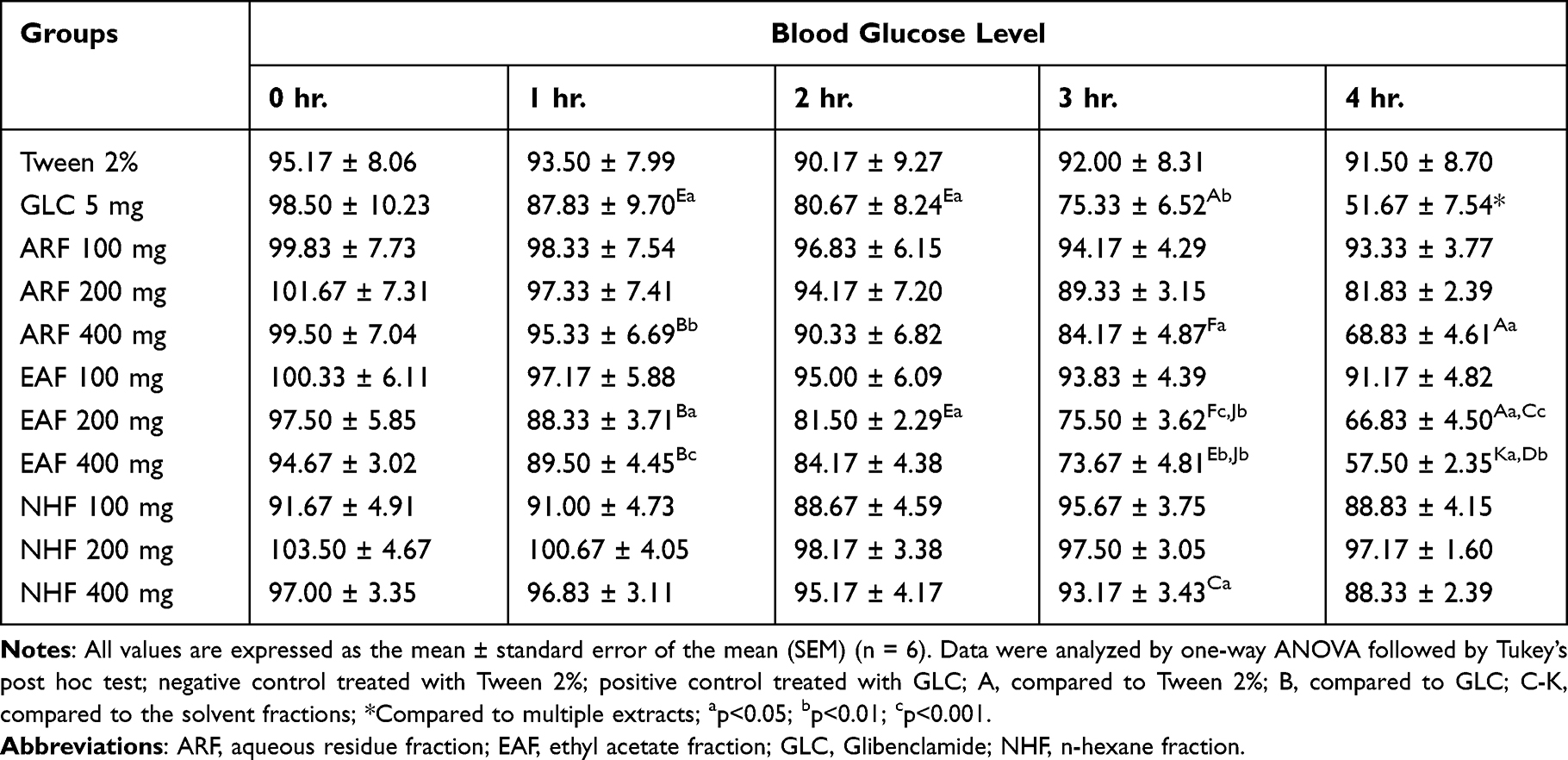 |
Table 3 Hypoglycemic Effect of the Solvent Fractions of V. Sinaiticum Leaves in Normoglycemic Mice |
Oral Glucose Tolerance Tests of V. Sinaiticum Extracts
Effects of the Crude 80% Methanol Extracts
There was no significant difference in baseline blood glucose levels between groups immediately before administration of the negative control, crude methanol extract, or positive control. When compared to the negative control, CME at 200 mg/kg and 400 mg/kg significantly reduced hyperglycemia in the first hour (p<0.05). Similarly, when compared to the negative control group, GLC significantly reduced blood glucose levels 1 hour and 2 hours after oral glucose loading (p<0.01). A within-group study revealed that oral glucose administration to mice resulted in a statistically significant increase in blood glucose levels after 30 minutes, regardless of intervention (p<0.001). CME at 400 mg/kg per body weight reduced blood glucose levels by 42.75%, while dosages of 100 mg/kg and 200 mg/kg per body weight reduced blood glucose levels by 14.56% and 34.28%, respectively (Table 4).
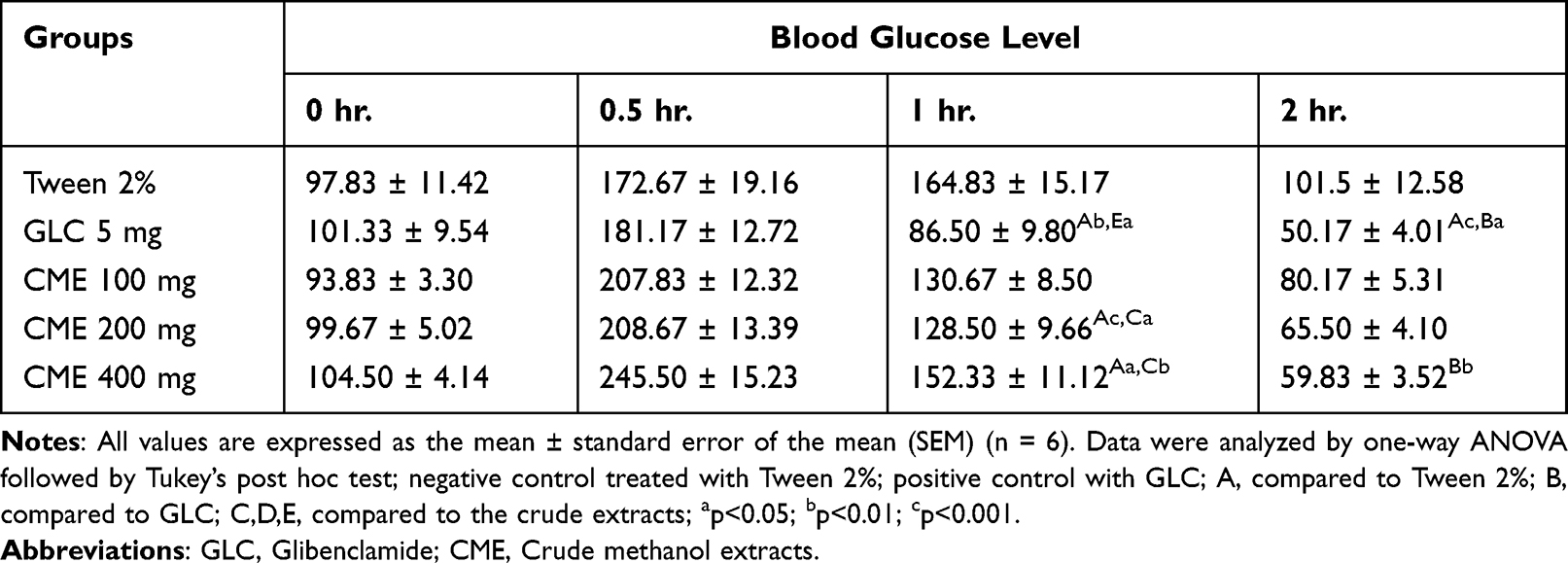 |
Table 4 The Glucose-Lowering Effect of the Crude 80% Methanol Extracts of V. Sinaiticum Leaves in Glucose-Loaded Mice |
Effects of the Solvent Fractions
There were no significant variations in glucose-lowering activity between groups prior to the administration of fractions and controls. ARF at 200 mg/kg significantly lowered blood glucose levels (p<0.01) when compared to NHF at the doses used in the research (p<0.01). GLC at 5 mg/kg (p<0.001) and EAF at 400 mg/kg (p<0.01) significantly reduced the blood glucose level during the first hour when compared to the negative control, according to the dose-between-groups analysis. Similarly, when compared to the negative control group, GLC treatment significantly reduced blood glucose levels 2 hours after oral glucose loading (p<0.001), as well as EAF at 200 mg/kg and 400 mg/kg (p<0.01) and ARF at 200 mg/kg and 400 mg/kg (p<0.05), which tolerated glucose loads significantly better than NHF at 400 mg/kg.
GLC at 5 mg/kg exhibited the highest percentage of overall blood glucose level reduction at 50.49%, followed by EAF 400 mg/kg at 41.81% and EAF 200 mg/kg at 36.91%. The NHF at 200 mg/kg resulted in the lowest percent reduction of 3.72%, whereas the NHF at 100 mg/kg and the tween 2% group demonstrated an increase in blood glucose levels beyond the baseline at 2 hours, indicating a negative reduction percentage (Table 5).
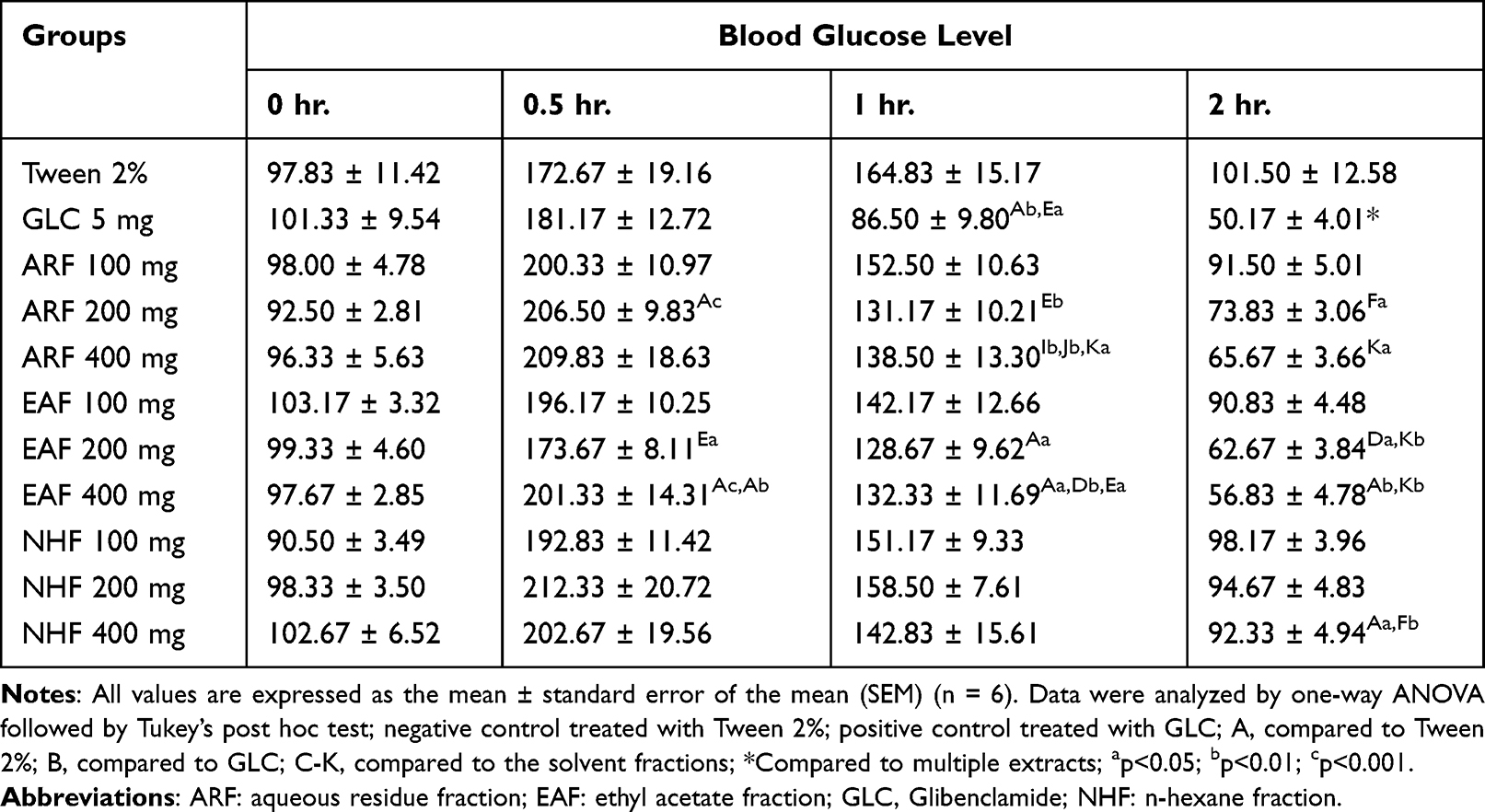 |
Table 5 The Glucose-Lowering Effects of the Solvent Fractions of V. Sinaiticum Leaves in Glucose-Loaded Mice |
Antihyperglycemic Effect of V. Sinaiticum in Diabetic Mice
Effects of the Crude 80% Methanol Extracts
STZ, a diabetes-inducing medication, was given intraperitoneally to mice that had fasted for 14 hours overnight; after 72 hours, 71.43% of the animals developed diabetes mellitus. At 0 hour, there were no significant differences between STZ-induced diabetic mice and normal control mice. At 1 hour, CME 200 mg/kg regulated blood glucose levels significantly better than the standard medicine GLC 5 mg/kg (p<0.01), whereas at 2 and 3 hours, CME at 400 mg/kg significantly lowered blood glucose levels (p<0.05). The percent reductions in blood glucose levels in STZ-induced diabetic mice from 0 to 4 hours were compared between the treatment and control groups. GLC at 5 mg/kg reduced blood glucose levels to the greatest extent (64.09%), followed by CME at 400 mg/kg (51.23%) and CME at 200 mg/kg with 43.51% (Table 6).
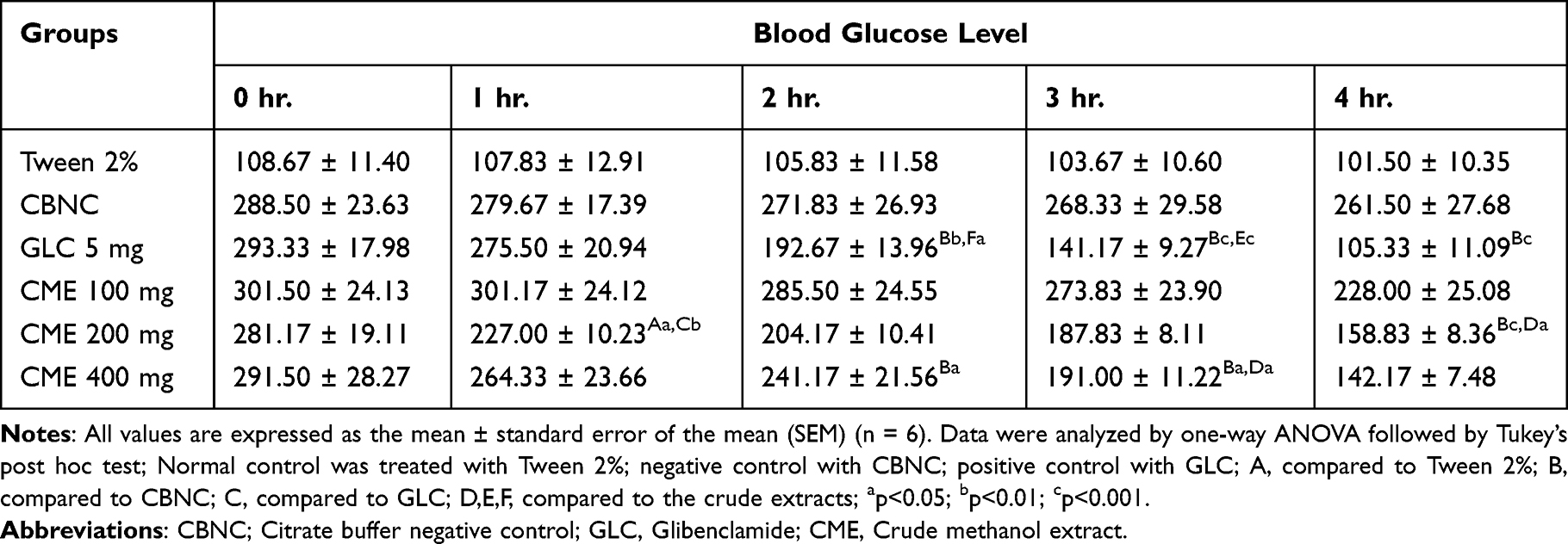 |
Table 6 The Antihyperglycemic Effect of the Crude 80% Methanol Extracts of V. Sinaiticum Leaves in Streptozotocin-Induced Diabetic Mice |
Effects of the Solvent Fractions
The current experiment shows that at 0 hour, there was a significant difference between the STZ-induced diabetes mouse group and the diabetic control group. Furthermore, when compared to ARF 400 mg/kg, EAF 200 mg/kg, 400 mg/kg, and GLC, ARF 200 mg/kg significantly lowered blood glucose levels after 2 hours (p<0.05). Mice administered GLC at 5 mg/kg and an EAF at 200 mg/kg had significantly lower glucose levels after 2 hours than mice given ARF at 200 mg/kg (p<0.05). BGLs were considerably reduced at the third hour by GLC (p<0.001), EAF at 200 mg/kg and 400 mg/kg, and ARF at 200 mg/kg and 400 mg/kg compared to ARF at 100 mg/kg (p<0.05). ARF at 200 mg/kg, 400 mg/kg, and GLC considerably reduced blood glucose levels when compared to NHF at 400 mg/kg (p<0.01).
In comparison to the ARF at 100 mg/kg and the EAF at 100 mg/kg, the EAF at 200 mg/kg (p<0.05) and the ARF at 400 mg/kg (p<0.01) significantly reduced the blood glucose levels at the fourth hour. The investigation findings revealed that GLC had the highest overall percent reduction in blood glucose levels at 64.09%, followed by EAF at 400 mg/kg with a reduction percentage of 52.42%, EAF at 200 mg/kg with a reduction percentage of 45.09%, and ARF at 400 mg/kg with a reduction percentage of 38.30%. The NHF 100 mg/kg treatment had the lowest blood glucose level reduction percentage of all extracts, at 14.85% (Table 7).
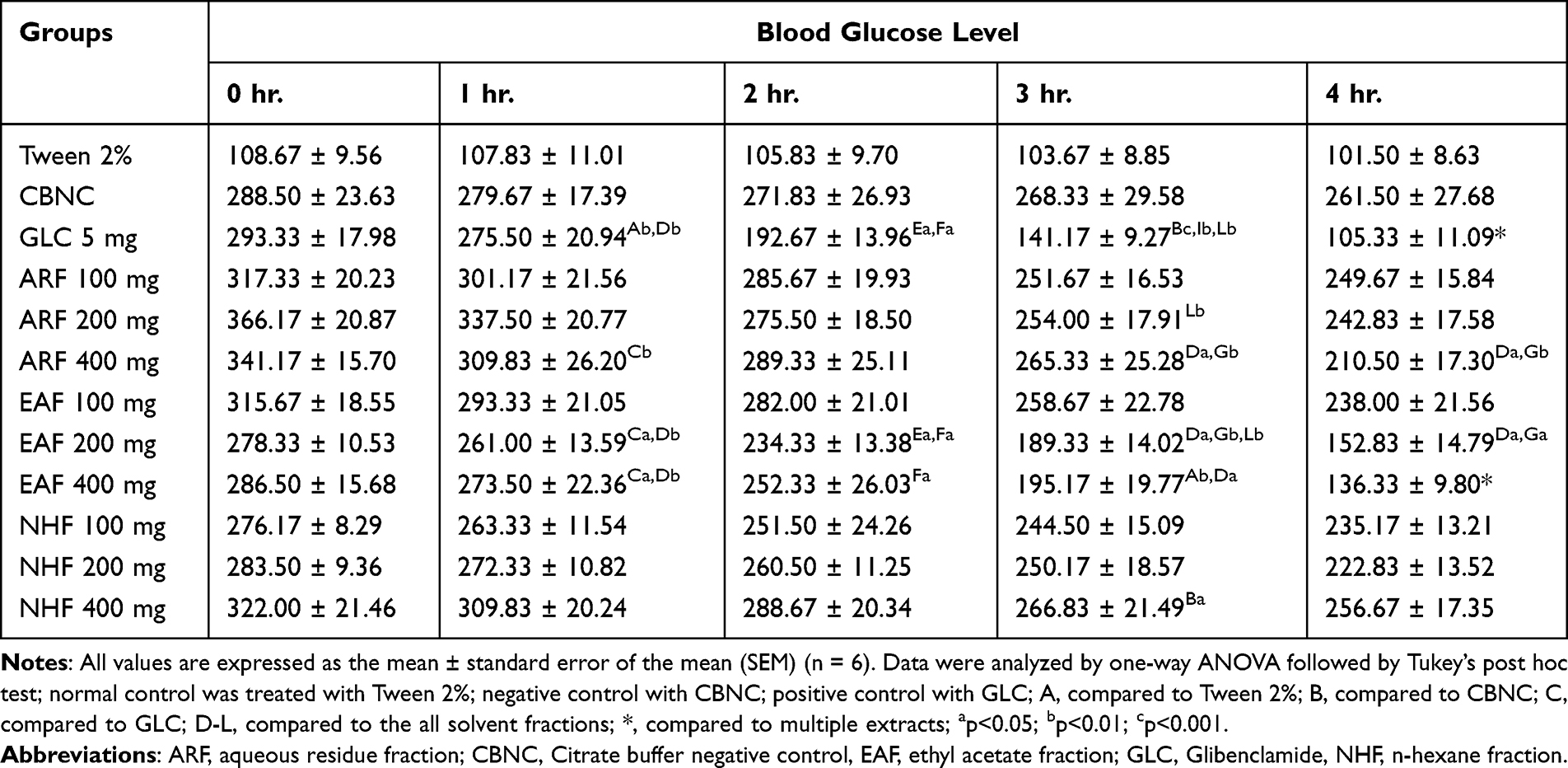 |
Table 7 The Antihyperglycemic Effect of the Solvent Fractions of V. Sinaiticum Leaves in Streptozotocin-Induced Diabetic Mice |
Discussion
The purpose of this study was to assess the anti-diabetic properties of the crude 80% methanol extract and solvent fractions of V. sinaiticum Benth (Scrophulariaceae) leaves in hypoglycemic, oral glucose-loaded, and streptozotocin-induced diabetic mice. Despite the lack of scientific evidence to support the plant’s efficacy and safety, an ethnobotanical study conducted in Dodota woreda, Arsi Zone, Oromia, Ethiopia, claims that V. sinaiticum Benth has a traditional antidiabetic usage.37,38
The crude 80% methanol extract of V. sinaiticum Benth from dried leaves yielded 17.14%. Ninety grams of 80% methanol extracts were fractionated and yielded 55.17% of aqueous residue, 31.77% ethyl acetate, and 10.93% n-hexane fractions, which were comparable to the yields from the previous study. The sum of fractionated extracts accounted for 97.87%, and the remaining 2.13% was most likely left on the container or lost during the fractionation, solvent recovery, and drying procedures. Most of the phytochemicals are available in 80% methanol extracts and ethyl acetate fractions. From previous studies, the important factors affecting the extraction efficiency of plant bioactive compounds, which is the difference observed in crude and fraction availability of terpenoids, might be affected by the type and concentration of solvent, temperature, time, pH, and solid‒liquid ratios.39
The hypoglycemic test in normoglycemic mice showed that crude 80% methanol extract at 200 and 400 mg/kg reduced blood glucose levels significantly at the second and third hours. Different studies show that hypoglycemia is a blood glucose level below 70 mg/dl in laboratory animals.40,41 Therefore, the present study revealed that V. sinaiticum Benth leaf extract and its fractions have mild hypoglycemic activity when compared to normal and standard controls, as mild hypoglycemia defines blood glucose levels between 60 and 80 mg/dl.42
The ethyl acetate fraction at 200 mg/kg exhibited significantly reduced glucose levels after 2 hours when compared to mice given an aqueous residual fraction at 400 mg/kg (p<0.05). At the third hour, an aqueous residue at 400 mg/kg and an ethyl acetate fraction at 200 mg/kg significantly lower blood glucose compared to the ethyl acetate fraction at 100 mg/kg (p<0.05). The plant extract has a lower risk of hypoglycemic shock at the tested dose levels of severe and marked hypoglycemia of less than 40 mg/dl and 40 to 60 mg/dl, respectively.43 A significant reduction in blood glucose levels with some plant extracts might be due to their antioxidant properties or the hypoglycemic activity of phytochemical constituents.44,45
An oral glucose tolerance test is a standard procedure that measures the clearance of an oral glucose load from the body or how quickly exogenous glucose can be cleared from the blood and is used in diagnosing diabetes mellitus.46 It is also used to monitor temporal blood glucose fluctuations in response to an oral glucose challenge.47 In the present study, the crude 80% methanol extracts and solvent fractions were administered orally at 100 mg/kg, 200 mg/kg, and 400 mg/kg. There was no significant difference in baseline blood glucose levels across groups just before the administration of the negative control, crude methanol extract, and positive control. The between-group univariate analysis of variance by post hoc test showed that crude methanol extracts at 200 mg/kg and 400 mg/kg (p<0.05) significantly reduced hyperglycemia in the first hour compared to the negative control from 30 minutes to 2 hours.
Fractions of V. sinaiticum Benth leaves were also tested for oral glucose tolerance using one-way ANOVA and Tukey’s post hoc test. The results of the analysis showed that 30 minutes after glucose administration, a significant glucose tolerance activity was demonstrated by 200 mg/kg of the aqueous residual fraction and 400 mg/kg of the ethyl acetate fraction (p<0.001). At 1 hour after treatment, both the 200 mg/kg ethyl acetate fraction and the 400 mg/kg aqueous residual consistently resisted glucose loading. Compared to all n-hexane fraction doses employed in these investigations, aqueous residue at 200 mg/kg significantly reduced blood glucose levels (p<0.01). At 2 hours, ethyl acetate fractions at 200 mg/kg and 400 mg/kg and aqueous residues at 200 and 400 mg/kg tolerated glucose loads significantly better than the n-hexane fraction of the 400 mg/kg group (p<0.05).
A significant reduction in blood glucose levels might be due to different secondary metabolites of V. sinaiticum Benth, which are responsible for the activities of the extract and its fraction on the loaded glucose in the process of removal from the blood. Therefore, the extract is believed to possess the ability to enhance regulatory mechanisms, indicating a potential advantage of the extract in minimizing hyperglycemia-related complications of diabetes. Extracts’ ability to reduce blood glucose levels following glucose load shows that it might involve an insulin-like action, probably either through enhancing the sensitivity of β-cells to glucose or peripheral glucose utilization.48
Streptozotocin (STZ) was used to induce diabetes mellitus for this investigation. It induces diabetes by entering pancreatic beta cells through the GLUT2 transporter, since it is a glucose analog, and accumulates the alkylating product diazomethane intracellularly, which results in beta cell death by alkylating DNA within these cells.49 STZ is a nitric oxide donor that directly impacts DNA and causes the production of free radicals such as superoxide, which ultimately leads to hydrogen peroxidase and hydroxyl-induced DNA damage through disruption of ATP production in the mitochondria.50
Streptozotocin is a chemical agent that can induce DNA damage and cause a decrease in ATP levels, leading to a reduction in insulin synthesis and secretion from beta cells. Consequently, the subsequent glucose overload activates the protein kinase (PKC) pathways and results in downstream glycation products, resulting in further oxidative stress and cell apoptosis, necrosis, and DNA damage.51 It also includes the accumulation of advanced glycation end products, cytokine secretion, glucose auto-oxidation or diacylglycerol (DAG) production, and increased O2 free radical generation. Thus, it has been suggested that enhanced production of free radicals and oxidative stress are central events in the development of diabetes and its complications. Therefore, the use of antioxidants reduces oxidative stress and alleviates diabetic complications.52
The results of this study show that in streptozotocin-induced diabetic mice, both the crude 80% methanol extract and fractions of V. sinaiticum Benth leaves had an antihyperglycemic effect. Mice were fasted before streptozotocin was administered because glucose can compete with streptozotocin in a fed state, so fasted animals tend to be more susceptible to this chemical.50 In mice treated with crude 80% methanol extracts at 200 mg/kg (p<0.01), 400 mg/kg (p<0.05), and glibenclamide 5 mg/kg (p<0.001), the blood glucose level was significantly reduced from 1 hour to 3 hours. Likewise, in mice treated with ethyl acetate fractions at 200 mg/kg and 400 mg/kg (p<0.01) as well as aqueous residue at 200 mg/kg and 400 mg/kg (p<0.05) of V. sinaiticum, the blood glucose level was significantly reduced at the 1 hour, 2 hour, 3 hour, and 4 hour points of the test.
A previous study showed that the crude aqueous extracts of V. sinaiticum obtained through qualitative phytochemical screening have alkaloids and saponins.53 In the current study, qualitative phytochemical screening of a crude 80% methanol extract of V. sinaiticum Benth leaves showed that it contained alkaloids, flavonoids, glycosides, phenols, steroids, and tannins. The disparity in results between this study and Mergia et al (2016) could be attributed to differences in extraction procedures. Nonpolar or low-polarity solvents, such as hexane, aid in the extraction of terpenoids, fatty acids, and wax, whereas medium-polar solvents, such as acetone, ethyl acetate, butanol, and dichloromethane, aid in the extraction of bioactive compounds such as less polar and polar flavonoids, tannins, and terpenoids. Furthermore, polar flavonoids, tannins, glycosides, saponins, carbohydrates, lectins, amino acids, polypeptides, phenolic acids, and alkaloids are found in highly polar solvents such as ethanol, methanol, and water.54,55
In this study, the crude 80% methanol extract at 200 mg/kg regulated blood glucose levels much better than 5 mg/kg glibenclamide at 1 hour (p<0.01), while at 2 and 3 hours, the 80% methanol extract at 400 mg/kg decreased blood glucose levels significantly (p<0.05). The investigation results showed a reduced blood glucose level at 4 hours, but statistical analysis showed no significant difference between the groups. The rationale could be that the crude 80% methanol extract of V. sinaiticum leaves contains numerous components, such as flavonoids, tannins, and saponins, which can reduce blood glucose levels in a variety of ways.
Saponins in V. sinaiticum may have reduced blood glucose levels in diabetic mice by activating beta cells, suppressing glucose transfer from the stomach to the small intestine, and inhibiting glucose transport across the small intestine’s brush boundary.44 The presence of flavonoids, saponins, and tannins in V. sinaiticum may prevent the loss of beta cells via one or more of the aforementioned processes because the induction of diabetes mellitus involves the destruction of beta cells by autoimmunity through free radicals and oxidative stress, which decrease insulin output. This may explain the stronger antihyperglycemic effects of crude 80% methanol extracts.56
The ethyl acetate fraction at 200 mg/kg and 400 mg/kg (p<0.01) and glibenclamide at 5 mg/kg (p<0.001) notably reduced blood glucose levels at the first and second hours; compared to the aqueous residue at 100 mg/kg. At the third hour, blood glucose levels were significantly lowered by glibenclamide at 5 mg/kg, ethyl acetate fractions at 200 mg/kg and 400 mg/kg, and aqueous fractions at 200 mg/kg and 400 mg/kg compared to an aqueous residue at 100 mg/kg (p<0.05). The blood glucose levels were also significantly lowered by aqueous residual fractions at 200 mg/kg and 400 mg/kg and glibenclamide at 5 mg/kg compared to the n-hexane fraction at 400 mg/kg (p<0.01). In comparison to the aqueous residue at 100 mg/kg, the ethyl acetate fraction at 200 mg/kg and the aqueous residual fraction at 400 mg/kg significantly reduced blood glucose levels at the fourth hour (p<0.05).
The above effects support the fact that V. sinaiticum leaves contain phytochemicals such as flavonoids, tannins, and terpenoids, which can be extracted with the aid of low- and medium-range polarity solvents such as ethyl acetate.57 The antihyperglycemic effect of V. sinaiticum leaf extracts may be due to an antioxidant effect, stimulation of beta cells, or suppression of glucose transfer from the stomach to the small intestine. More antioxidants are required in diabetes to reduce free radical formation and increase radical binding systems because oxidative stress occurs as a result of reactive oxygen species overproduction or decreased antioxidant capacity. It was also stated that terpenes have antioxidant activity.58 The glycemic control of V. sinaiticum may be linked to phytochemicals it possesses and through one or more possible mechanisms.
The current study tested the acute effects of crude 80% methanol extracts of V. sinaiticum Benth leaves and their fractions on three different models: hypoglycemic tests, oral glucose tolerance tests, and streptozotocin-induced diabetic mice. Throughout the trial, no specific phytochemicals or components responsible for diabetes management were found. Repeated-dose studies have not been conducted, and little is known about the long-term administration of medicinal plant extracts. This study did not include quantitative phytochemical screening. Furthermore, only the leaf sections of V. sinaiticum Benth were investigated, leaving the rest accessible for future investigation.
Conclusion
The results of the experiment revealed that the 80% methanolic extracts and solvent fractions of V. sinaiticum Benth leaves have significant glucose-lowering potential in all three models without leading to severe hypoglycemia. The overall antidiabetic efficacy might be correlated with the presence of bioactive secondary metabolites such as alkaloids, flavonoids, tannins, terpenoids, saponins, and phenols. The ethyl acetate fraction was the most active, followed by the aqueous residual fraction. The findings of this study support the traditional use of V. sinaiticum Benth leaf extracts as an antidiabetic agent. However, further studies on pharmacological and histopathological aspects are needed to determine and ascertain the exact mechanism of action against diabetes mellitus disease.
Abbreviations
ADA, American Diabetes Association; ANOVA, analysis of variance; ARF, aqueous residue fraction; CME, crude methanol extract; EAF, ethyl acetate fraction; GLC, glibenclamide; NHF, N-hexane fraction; SEM, standard error of the mean; STZ, streptozotocin.
Data Sharing Statement
The corresponding author will provide all the datasets used and analyzed during the current work upon reasonable request.
Ethical Approval
Ethical approval was obtained from the Institutional Review Board of the College of Medicine and Health Science, Hawassa University, before conducting the experiment (Protocol version Number 1, Ref. No. IRB/156/14).
Acknowledgments
We are very grateful to the School of Pharmacy at Haramaya University for their support and use of their pharmacology laboratory for this study. We would also like to thank the laboratory coordinators and the pharmacology and medicinal chemistry department staff for their unreserved cooperation during the experiment. The full thesis of this manuscript is available on the Hawassa University repository at this link: http://etd.hu.edu.et/handle/123456789/3649.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the School of Pharmacy, College of Medicine and Health Science, Hawassa University.
Disclosure
The authors declare that they have no competing interests.
References
1. ADA. Introduction: standards of medical care in diabetes — 2022. Diabetes Care. 2022;45:2021–2022.
2. Iatcu CO, Steen A, Covasa M. Gut microbiota and complications of type-2 diabetes. Nutrients. 2021;14(1):1–30. doi:10.3390/nu14010166
3. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the international diabetes federation diabetes atlas. Diabetes Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
4. Elsayed NA, Aleppo G, Aroda VR, et al. 2. Classification and diagnosis of diabetes: standards of care in diabetes—2023. Diabetes Care. 2023;46(Suppl 1):S19–40. doi:10.2337/dc23-S002
5. Grulovic N, Rojnic Kuzman M, Baretic M. Prevalence and predictors of diabetes-related distress in adults with type 1 diabetes. Sci Rep. 2022;12(1):15758. doi:10.1038/s41598-022-19961-4
6. Care D, Suppl SS. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2021. Diabetes Care. 2021;44(Supplement 1):1.
7. Monaghan M, Bryant BL, Inverso H, Moore HR, Streisand R. Young children with type 1 diabetes: recent advances in behavioral research. Curr Diab Rep. 2022;22(6):247–256. doi:10.1007/s11892-022-01465-0
8. Karavanaki K, Paschou SA, Tentolouris N, Karachaliou F, Soldatou A. Type 2 diabetes in children and adolescents: distinct characteristics and evidence-based management. Endocrine. 2022;78(2):280–295. doi:10.1007/s12020-022-03172-y
9. Sreedevi A, Krishnapillai V, Menon VB, et al. Uncontrolled blood pressure and associated factors among persons with diabetes: a community based study From Kerala, India. Front Public Heal. 2021;9:778235. doi:10.3389/fpubh.2021.778235
10. Karat S, Lobo AC, Satish D, Devaraj R, Manjooran RR, Nithyanandam S. Uncontrolled diabetes mellitus exacerbated by COVID-19-induced inflammation is the risk factor for COVID-19-associated rhino-orbito-cerebral mucormycosis: a matched pair case‒control study. Indian J Ophthalmol. 2022;70(8):3096–3101. doi:10.4103/ijo.IJO_448_22
11. Craig ME, Hattersley A, Donaghue KC. Definition, epidemiology and classification of diabetes in children and adolescents. Pediatr Diabetes. 2009;10(Suppl 1):3–12. doi:10.1111/j.1399-5448.2009.00568.x
12. Mainieri F, Tagi VM, Chiarelli F. Insulin resistance in children. Curr Opin Pediatr. 2022;34(4):400–406. doi:10.1097/MOP.0000000000001151
13. Kasuga Y, Miyakoshi K, Saisho Y, Ikenoue S, Ochiai D, Tanaka M. Impaired early phase insulin secretion associated with gestational diabetes mellitus in underweight women. J Matern Neonatal Med. 2022;35(12):2411–2413.
14. Gregory GA, Robinson TIG, Linklater SE, et al. Global incidence, prevalence, and mortality of type 1 diabetes in 2021 with projection to 2040: a modeling study. Lancet Diabetes Endocrinol. 2022;10(10):741–760. doi:10.1016/S2213-8587(22)00218-2
15. Ruiz PLD, Chen L, Morton JI, et al. Mortality trends in type 1 diabetes: a multicountry analysis of six population-based cohorts. Diabetologia. 2022;65(6):964–972. doi:10.1007/s00125-022-05659-9
16. IDF Diabetes Atlas. International Diabetes Federation. Diabetes Res Clin Pract. 2021;102:147–148.
17. Zeru MA, Tesfa E, Mitiku AA, Seyoum A, Bokoro TA. Prevalence and risk factors for type-2 diabetes mellitus in Ethiopia: systematic review and meta-analysis. Sci Rep. 2021;11(1):1–15. doi:10.1038/s41598-021-01256-9
18. Rana JS, Khan SS, Lloyd-Jones DM, Sidney S. Changes in mortality in top 10 causes of death from 2011 to 2018. J Gen Intern Med. 2021;36(8):2517–2518. doi:10.1007/s11606-020-06070-z
19. Skyler JS, Bakris GL, Bonifacio E, et al. Differentiation of diabetes by pathophysiology, natural history, and prognosis. Diabetes. 2017;66(2):241–255. doi:10.2337/db16-0806
20. Steenblock C, Hassanein M, Khan EG, et al. Diabetes and COVID-19: short- and long-term consequences. Horm Metab Res. 2022;54(8):503–509. doi:10.1055/a-1878-9566
21. Dereje B, Nardos A. Dopamine 2 agonists for the management of type 2 diabetes: a systematic review and meta‑analysis. J Diabetes Metab Disord. 2023;1–13. doi:10.1007/s40200-023-01230-4
22. Garber AJ, Handelsman Y, Grunberger G, et al. Consensus statement by the American association of clinical endocrinologists and American college of endocrinology on the comprehensive type 2 diabetes management algorithm - 2020 executive summary. Endocr Pract. 2020;26(1):107–139. doi:10.4158/CS-2019-0472
23. Willcox ML, Elugbaju C, Al-Anbaki M, Lown M, Graz B. Effectiveness of medicinal plants for glycemic control in type 2 diabetes: an overview of meta-analyses of clinical Trials. Front Pharmacol. 2021;12:1–13. doi:10.3389/fphar.2021.777561
24. Chaix A, Deota S, Bhardwaj R, Lin T, Panda S. Sex- and age-dependent outcomes of 9-hour time-restricted feeding of a Western high-fat high-sucrose diet in C57BL/6J mice. Cell Rep. 2021;36(7):109543. doi:10.1016/j.celrep.2021.109543
25. Keijer J, Li M, Speakman JR. What is the best housing temperature to translate mouse experiments to humans? Mol Metab. 2019;25:168–176. doi:10.1016/j.molmet.2019.04.001
26. Górska P. Principles in laboratory animal research for experimental purposes. Med Sci Monit Int Med J Exp Clin Res. 2000;6(1):171–180.
27. Garber JC, Barbee RW, Bielitzki JT, et al. National institute of health: guide for the care and use of laboratory animals; 2010;1–218.
28. Shaikh JR, Patil M. Qualitative tests for preliminary phytochemical screening: an overview. Int J Chem Stud. 2020;8(2):603–608. doi:10.22271/chemi.2020.v8.i2i.8834
29. Jaradat N, Hussen F, Al Ali A. Preliminary phytochemical screening, quantitative estimation of total flavonoids, total phenols and antioxidant activity of Ephedra alata Decne. J Mater Environ Sci. 2015;6(6):1771–1778.
30. OECD. Organization of Economic Corporation and Development’s Guideline for the Testing of Chemical No. 425. Manual. 2008;3:27.
31. Altemimi A, Lakhssassi N, Baharlouei A, Watson DG, Lightfoot D. Phytochemicals: extraction, isolation, and identification of bioactive compounds from plant extracts. Plants. 2017;6(4):42. doi:10.3390/plants6040042
32. Larson EC, Pond CD, Rai PP, et al. Traditional preparations and methanol extracts of medicinal plants from Papua New Guinea exhibit similar cytochrome P450 inhibition. Evid Based Complement Alternat Med. 2016;2016:7869710. doi:10.1155/2016/7869710
33. Furman BL. Streptozotocin-induced diabetic models in mice and rats. Curr Protoc. 2021;1(4):1–21. doi:10.1002/cpz1.78
34. Baquer NZ, Kumar P, Taha A, Kale R, Cowsik S, McLean P. Metabolic and molecular action of Trigonella foenum-graecum (fenugreek) and trace metals in experimental diabetic tissues. J Biosci. 2011;36(2):383–396. doi:10.1007/s12038-011-9042-0
35. Tamiru W, Engidawork E, Asres K. Evaluation of the effects of 80% methanolic leaf extract of Caylusea abyssinica (fresen.) fisch. & Mey. on glucose handling in normal, glucose loaded and diabetic rodents. BMC Complement Altern Med. 2012;12(1):1. doi:10.1186/1472-6882-12-151
36. Panel AC, Cohen BJ, Ph D. Guide for laboratory animal facilities and care. ILAR J. 2021;62(3):345–358.
37. Meresa A, Gemechu W, Basha H, et al. Herbal medicines for the management of diabetic mellitus in Ethiopia and Eritrea including their phytochemical constituents. Am J Adv Drug Deliv. 2017;05(01):040–58.
38. Abebe DS, Debella A, Urga K. Medicinal plants and other useful plants of Ethiopia. In: Nairobi (Kenya) Camerapix Publishers International. Nairobi: Nairobi (Kenya) Camerapix Publishers International; 2003:312.
39. Abu Bakar FI, Abu Bakar MF, Abdullah N, Endrini S, Fatmawati S. Optimization of extraction conditions of phytochemical compounds and anti-gout activity of euphorbia hirta L. (Ara Tanah) Using Response Surface Methodology and Liquid Chromatography‒Mass Spectrometry (LC‒MS) Analysis. Evid Based Complement Alternat Med. 2020;2020:4501261. doi:10.1155/2020/4501261
40. Nakhleh A, Shehadeh N. Hypoglycemia in diabetes: an update on pathophysiology, treatment, and prevention. World J Diabetes. 2021;12(12):2036–2049. doi:10.4239/wjd.v12.i12.2036
41. Sen Gupta P, Green AN, Chowdhury TA. Hypoglycemia. BMJ. 2011;342:d567. doi:10.1136/bmj.d567
42. Grant CW, Duclos SK, Moran-Paul CM, et al. Comparative medicine development of standardized insulin treatment protocols for spontaneous rodent models of type 1 diabetes. Comp Med. 2012;62(5):381–390.
43. Kirilmaz OB, Salegaonkar AR, Shiau J, et al. Study of blood glucose and insulin infusion rate in real-time in diabetic rats using an artificial pancreas system. PLoS One. 2021;16(7):1–19. doi:10.1371/journal.pone.0254718
44. Desai SD, Desai DG, Kaur H. Saponins and their Biological Activities. Pharma Times. 2017;41:1–5.
45. Occhiuto C, Aliberto G, Ingegneri M, Trombetta D, Circosta C, Smeriglio A. Comparative evaluation of the nutrients, phytochemicals, and antioxidant activity of two hemp seed oils and their byproducts after cold pressing. Molecules. 2022;27(11):3431. doi:10.3390/molecules27113431
46. Med D M-WPD, Nauck M, Petersmann A, et al. Definition, classification and diagnosis of diabetes mellitus. Diabetologe. 2019;15(2):128–134. doi:10.1007/s11428-019-0460-1
47. Rozman J, Rathkolb B, Neschen S, et al. Glucose tolerance tests for systematic screening of glucose homeostasis in mice. Curr Protoc Mouse Biol. 2015;5(1):65–84. doi:10.1002/9780470942390.mo140111
48. Al-Ishaq RK, Abotaleb M, Kubatka P, Kajo K, Büsselberg D. Flavonoids and their anti-diabetic effects: cellular mechanisms and effects to improve blood sugar levels. Biomolecules. 2019;9(9):1–35. doi:10.3390/biom9090430
49. Graham ML, Janecek JL, Kittredge JA, Hering BJ, Schuurman HJ. The streptozotocin-induced diabetic nude mouse model: differences between animals from different sources. Comp Med. 2011;61(4):356–360.
50. Goyal SN, Reddy NM, Patil KR, et al. Challenges and issues with streptozotocin-induced diabetes - A clinically relevant animal model to understand the diabetes pathogenesis and evaluate therapeutics. Chem Biol Interact. 2016;244(1):49–63. doi:10.1016/j.cbi.2015.11.032
51. Al NAMT, John A, Raza H. Elucidation of molecular mechanisms of streptozotocin-induced oxidative stress, apoptosis, and mitochondrial dysfunction in rin-5F pancreatic β-cells. Oxid Med Cell Longev. 2017;2017:7054272. doi:10.1155/2017/7054272
52. Zeng LY, Liu Y, Han J, Chen J, Liu S, Xi B. O-Methylation of carboxylic acids with streptozotocin. Org Biomol Chem. 2022;20(26):5230–5233. doi:10.1039/D2OB00578F
53. Mergia E, Shibeshi W, Terefe G, Teklehaymanot T. Antitrypanosomal activity of V. sinaiticum Benth. (Scrophulariaceae) against Trypanosoma congolense isolates. BMC Complement Altern Med. 2016;16(1):1–9. doi:10.1186/s12906-016-1346-z
54. Chikezie PC, Ibegbulem CO, Mbagwu FN. Medicinal potentials and toxicity concerns of bioactive principles. Med Aromat Plants. 2015;04(03):1–15.
55. Mosić M, Dramićanin A, Ristivojević P, Milojković-Opsenica D. Extraction as a critical step in phytochemical analysis. J AOAC Int. 2020;103(2):365–372.
56. Yuan H, Zhou P, Peng Z, Wang C. Antioxidant and antibacterial activities of dodecyl tannin derivative linked with 1,2,3-triazole. Chem Biodivers. 2022;19:1.
57. Khentoul H, Bensouici C, Reyes F, et al. Chemical constituents and HRESI-MS analysis of an Algerian endemic plant - Verbascum atlanticum batt. - extracts and their antioxidant activity. Nat Prod Res. 2020;34(20):3008–3012. doi:10.1080/14786419.2019.1602829
58. Zhang P, Li T, Wu X, Nice EC, Huang C, Zhang Y. Oxidative stress and diabetes: antioxidative strategies. Front Med. 2020;14(5):583–600. doi:10.1007/s11684-019-0729-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.