")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 16
Antibody-Drug Conjugates in Breast Cancer: A Comprehensive Review of How to Selectively Deliver Payloads
Authors Monteiro MR , Nunes NCC, Junior AADS, Fêde ABDS, Bretas GDO, Souza CDP, Mano M, da Silva JL
Received 4 November 2023
Accepted for publication 10 February 2024
Published 28 February 2024 Volume 2024:16 Pages 51—70
DOI https://doi.org/10.2147/BCTT.S448191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Mariana Ribeiro Monteiro,1,2 Natalia Cristina Cardoso Nunes,3 Aumilto Augusto da Silva Junior,4 Angelo Bezerra de Souza Fêde,5 Gustavo de Oliveira Bretas,6 Cristiano de Pádua Souza,7 Max Mano,8 Jesse Lopes da Silva6,9,10
1Instituto Americas, São Paulo, Brazil; 2Hospital Samaritano, São Paulo, Brazil; 3Instituto Americas, Rio de Janeiro, Brazil; 4Hospital Santa Catarina Paulista, São Paulo, Brazil; 5DASA Oncologia, São Paulo, Brazil; 6Grupo Oncoclínicas, Rio de Janeiro, Brazil; 7Hospital do Câncer de Barretos, São Paulo, Brazil; 8Grupo Oncoclínicas, São Paulo, Brazil; 9Divisão de Pesquisa Clínica e Desenvolvimento Tecnológico, Instituto Nacional do Câncer, Rio de Janeiro, Brazil; 10Hospital da Força Aérea do Galeão, Rio de Janeiro, Brazil
Correspondence: Mariana Ribeiro Monteiro, Email [email protected]
Abstract: Antibody-drug conjugates (ADCs) have surfaced as a promising group of anticancer agents employing the precise targeting capacity of monoclonal antibodies to transport highly effective cytotoxic payloads. Compared to conventional chemotherapy, they aim to selectively eradicate cancer cells while minimizing off-target toxicity on healthy tissues. An increasing body of evidence has provided support for the efficacy of ADCs in treating breast cancer across various contexts and tumor subtypes, resulting in significant changes in clinical practice. Nevertheless, unlocking the full potential of these therapeutic agents demands innovative molecular designs to address complex clinical challenges, including drug resistance, tumor heterogeneity, and treatment-related adverse events. This thorough review provides an in-depth analysis of the clinical data on ADCs, offering crucial insights from pivotal clinical trials that assess the efficacy of ADCs in diverse breast cancer settings. This aids in providing a comprehensive understanding of the current state of ADCs in breast cancer therapy, while also providing valuable perspectives for the future.
Keywords: breast cancer, cancer therapy, target therapy, antibody–drug conjugates, ADCs
Introduction
Breast cancer (BC) poses a significant global public health challenge.1 Historically, the conventional non-selective approach of chemotherapeutic agents has led to concerns regarding toxicity and the premature activation of resistance mechanisms.2 Recent advances in understanding carcinogenesis, tumor heterogeneity, and metastasis process have provided opportunities for the development of more targeted and less toxic anticancer agents.3 In the early 20th century, Paul Ehrlich advocated for the creation of therapeutic agents that could selectively target specific cancer cell antigens while minimizing harm to surrounding cell populations.4
To enhance the therapeutic index, defined as the range between the minimum effective dose and the maximum tolerated dose, antibody-drug conjugates (ADCs) have emerged as a promising strategy. ADCs comprise a monoclonal antibody (mAbs) linked to a potent cytotoxic payload via a chemical linker, offering a more targeted delivery system.5 Employing a “Trojan horse” approach, these agents ease the transportation of chemotherapy to precise targets, theoretically reducing systemic toxicity in comparison to traditional chemotherapeutic agents.6
The improvement of ADCs has involved enhancing each vital component: the antibody, cytotoxic payload, and linker. Multiple crucial considerations have been addressed to enhance the efficacy of ADCs. Regarding the antibody component (typically human IgG1), emphasis is placed on high tumor specificity, extended circulation life, rapid internalization, with or without immune activation, and minimal immunogenicity. Furthermore, for the payload, critical factors include high potency, diverse mechanisms of action (eg, microtubule inhibition and direct DNA damage), and optimal drug antibody ratio. Specific payloads like deruxtecan in trastuzumab deruxtecan (T-DXd) can also induce bystander killing effects, as the drug diffuses from targeted to untargeted cells due to its unique chemistry.7 The linker and conjugation chemistries are crucial in linking the mAbs and the payload, ensuring homogeneity, and determining whether cleavable or non-cleavable linkers are used based on payload characteristics. The design of the linker is pivotal in controlling drug release from the antibody, influencing physicochemical properties, stability in circulation, and potency. ADCs need to limit payload exposure to normal tissues to minimize general toxicities.8
Acquired resistance and adverse events represent limitations to the efficacy of ADCs in breast cancer treatment. Improvements in the diverse components of ADCs will be pivotal in enhancing both the efficacy and safety of these agents.9 To address these challenges, various innovative ADCs formats have emerged, including bispecific ADCs, probody–drug conjugates, immune-stimulating ADCs, protein-degrader ADCs, and dual-drug ADCs. Probody-drug conjugates are expected to provide increased tumor specificity, whereas bispecific ADCs and dual-drug ADCs have the potential to address drug resistance and tumor heterogeneity, aspects that significantly influence treatment responses. The association between tumor heterogeneity and ADCs resistance encompasses selective pressures induced by intense ADCs treatment, promoting the survival of resistant clones with specific attributes. These clones may exhibit distinct characteristics, such as mutations in target proteins or related signaling pathways, changes in drug metabolism, activation of alternative signaling pathways, and the existence of cancer stem-like cells.10 Combining immune-stimulating ADCs and protein-degrading ADCs with current treatment regimens has the potential to facilitate multimodal treatment, potentially through several distinct mechanisms of action.11
This comprehensive review thoroughly examines the primary clinical data of ADCs that have significantly transformed clinical practices across the various BC subtypes and settings. Herein, the latest clinical research advances, innovative biomarkers, and strategies to address resistance are meticulously scrutinized.
HER2-Positive Breast Cancer
Ado-trastuzumab emtansine (T-DM1) was the first ADC approved for the treatment of HER2-positive BC. T-DM1 is composed of the mAb trastuzumab, linked to a maytansinoid toxin, DM1, which inhibits tubulin polymerization. The DM1 is connected to the mAb by a non-cleavable stable thioether (N-maleimidomethyl) linker. T-DM1 has a drug-antibody ratio (DAR) of 3.5:1.12 It retains the functions of the trastuzumab, including antibody-dependent cellular cytotoxicity and signaling inhibition, in conjunction with the antitumoral effects of the payload (Figure 1).13 T-DM1 received FDA approval in 2013 for use in patients with previously treated HER2-positive metastatic BC.
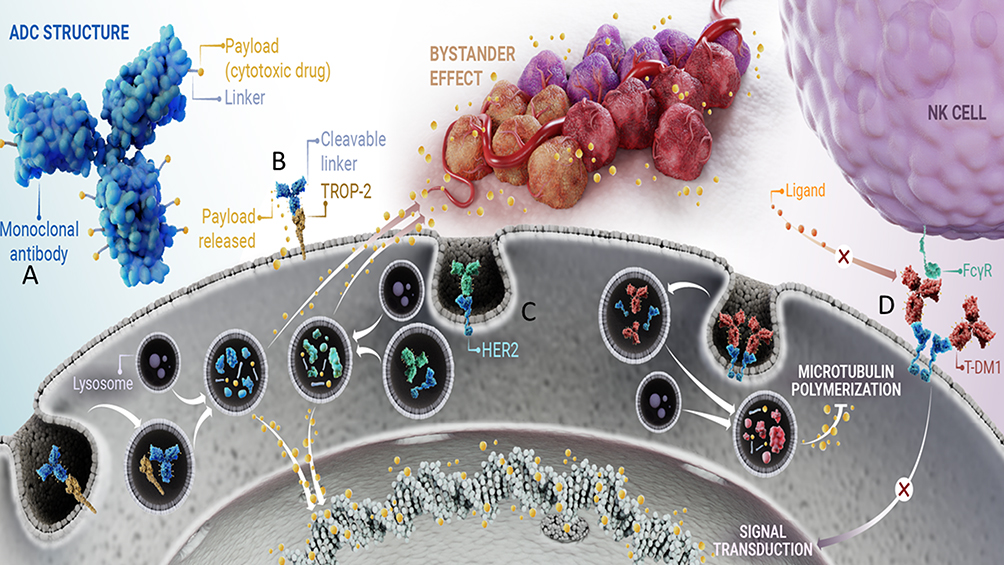 |
Figure 1 Structure and Mechanism of Action of Antibody-Drug Conjugates in the Treatment of Breast Cancer. Note: (A) The figure displays the components of Antibody-Drug Conjugates (ADCs), comprising the antibody, linker, and payload. (B). Sacituzumab Govitecan targets TROP-2-expressing cancer cells using the humanized antibody RS7. Following cellular internalization, the topoisomerase I inhibitor SN-38 is released, leading to DNA damage-mediated apoptosis. (C) Trastuzumab-Deruxitecan (T-DXd), another ADC, binds to HER2 on tumor cells and undergoes internalization. Intracellular linker cleavage by lysosomal enzymes ensues, liberating the membrane-permeable DXd. Once released, DXd enters the nucleus, causing DNA damage and inducing apoptotic cell death. Notably, the high membrane permeability of the payload enables a cytotoxic bystander effect on neighboring tumor cells, regardless of their HER2 expression levels. (D) Trastuzumab emtansine (T-DM1), a representative ADC, binds to HER2 via the Fc receptor. Upon internalization of the TDM-1/HER2 complex by endosomes, subsequent degradation occurs within lysosomes, leading to the release of emtansine. Emtansine then binds to microtubules, impeding their polymerization. Additionally, TDM-1 inhibits downstream HER2 signaling, resulting in the prevention of cell proliferation and the induction of apoptosis. Moreover, TDM-1 binds to natural killer (NK) cells through Fc gamma receptors (FcƴR), eliciting cell death via immune system activation. |
The EMILIA trial demonstrated that T-DM1 markedly improved progression-free survival (PFS) and overall survival (OS) compared to lapatinib and capecitabine. The objective response rate (ORR) was 43.6% versus 31%, and the median PFS was 9.6 versus 6.4 months (Hazard Ratio, HR 0.65, p<0.001). In the second interim analysis, the median OS was 30.9 versus 25.1 months (HR 0.68, p<0.001), demonstrating the superiority of the experimental arm.14 Similarly, the TH3RESA trial showed that T-DM1 improved significantly both PFS (median 6.2 versus 3.3 months; HR 0.52, p<0.0001) and OS (22.7 versus 15.8 months; HR 0.68, p=0.0007) compared to treatment of physician’s choice (TPC) in later lines. The ORR was 31% versus 9%.15 The results of the MARIANNE trial suggested T-DM1 as a feasible first-line therapeutic option for metastatic HER2-positive BC, exhibiting non-inferiority in comparison to the combination of trastuzumab and taxane.16 However, the CLEOPATRA trial results indicated that the addition of pertuzumab to trastuzumab and taxane significantly prolonged PFS (HR 0.62, 95% Confidence interval, CI, 0.51–0·75) and OS (HR 0.69, 95% CI, 0.58–0.82), and this regimen has been considered the standard first-line treatment for metastatic HER2-positive BC so far.17
Shifting the focus to the early-stage scenario, the neoadjuvant administration of T-DM1 plus pertuzumab did not meaningfully improve the pathological complete response (pCR) rate in comparison to the administration of trastuzumab, pertuzumab, and chemotherapy, as demonstrated by the KRISTINE trial.18 However, in the adjuvant setting, in patients who have not achieved pCR after neoadjuvant treatment, the KATHERINE trial revealed a decreased risk of invasive BC recurrence. The published results in 2019 revealed a 3-year invasive disease-free survival (iDFS) of 88.3% for patients who received T-DM1 compared to 77% for those in the control arm who received trastuzumab (HR 0.5, p<0.001).19 With a follow-up of 8.1 years, OS data presented in December 2023 at the San Antonio Breast Cancer Symposium revealed OS of 89.1% in the T-DM1 arm and 84.4% in the trastuzumab arm. T-DM1 is generally well-tolerated, with manageable adverse events (AEs) such as gastrointestinal toxicity, thrombocytopenia, and a mild to moderate increase in liver enzymes, mostly categorized as grade 1/2.20
Trastuzumab deruxtecan (T-DXd) is a recently approved ADC for the treatment of previously treated metastatic BC in patients with HER2-positive status.21 T-DXd comprises a humanized anti-HER2 IgG1 mAb, a cleavable tetrapeptide-based linker, and a payload. The payload is a topoisomerase I inhibitor, an exatecan derivative, known as deruxtecan. T-DXd exhibits a high DAR of 8:1, which results in the delivery of a higher concentration of the cytotoxic drug than T-DM1. The bystander effect of T-DXd arises from the release of cytotoxic payload from the targeted cells, after ADCs internalization and degradation. The payload then is able to act on the target cell and on surrounding (or bystander) cells, which may or may not express the HER2 antigen, thereby instigating a potent paracrine effect. Such an effect justifies the tumor response in HER2-low or HER2-heterogeneous BC (Figure 1).22,23
T-DXd was approved by the FDA in December 2019 based on the results of the DESTINY-Breast01 (DB01) study, which is a Phase II, two-part, open-label, single-group study. The study enrolled HER2-positive metastatic BC patients who had previously received two or more anti-HER2 therapies in the metastatic setting and had previously been treated with T-DM1. The study demonstrates an impressive ORR of 60.9%, a median PFS of 16 months and a 2-year OS rate of 58%.24 Subsequently, the Phase III DESTINY-Breast-02 (DB02) trial confirmed these findings by demonstrating considerable improvement in ORR (69.7% versus 29.2%), in PFS (median 17.8 versus 6.9 months, HR 0.35, p<0.0001), and OS (median 39.2 versus 26.5 months; HR 0.66, p=0.0021) in patients treated with T-DXd compared to TPC.25 The phase III DESTINY-Breast03 (DB03) study also showed superiority of T-DXd compared to T-DM1 in second-line treatment for HER2-positive unresectable or metastatic BC. Treatment with T-DXd resulted in a higher ORR (79.7% versus 34.2%), and a statistically significant improvement in PFS (median 25.1 versus 7.2 months; HR 0.26, p<0.001) that was across all prespecified subgroups, including patients with brain metastases. In recently updated results, OS was also significantly improved (2-year OS rate of 77.4% versus 69.9%; HR 0.64, p=0.0037).26
T-DXd has exhibited activity against brain metastases, as revealed in a subgroup analysis of the DB01 and DB03 trials.26,27 However, patients with untreated or progressing brain metastases were excluded from both study protocols. In contrast, two small Phase II clinical trials, namely the DEBBRAH and TUXEDO-1, have reported high intracranial ORR among patients with active brain metastases and HER2-positive BC. The efficacy of T-DXd in the central nervous system is being further evaluated by the ongoing phase III DB12 trial, which is investigating patients with previously treated metastatic HER2-positive breast cancer, with or without brain metastases.28,29
The incidence of AEs associated with T-DXd, however, is considerable. Gastrointestinal and hematological toxicities are the most frequently observed AEs, regardless of its severity. Notably, interstitial lung disease (ILD)/pneumonitis is a worrisome toxicity associated with T-DXd. In a meta-analysis, 10.8% of the patients had ILD of any grade and 1.8% grade ≥3.30
In summary, T-DXd has demonstrated high response rates, prolonged duration of response, and longer survival after progression to first-line treatment. However, data on first-line treatment and earlier settings are still lacking. Several phase III randomized clinical trials are currently underway. DESTINY-Breast05 (DB-05) study is investigating the iDFS of T-DXd compared to T-DM1 in high-risk HER2-positive BC patients without pCR in the post-neoadjuvant setting.31 Similarly, the DESTINY-Breast11 (DB-11) trial is assessing the efficacy of T-DXd in a neoadjuvant setting for high-risk, early HER2-positive BC.32 In the first-line treatment of HER2 metastatic BC, the DESTINY-Breast09 (DB-09) trial is comparing the efficacy and safety of T-DXd alone or in combination with pertuzumab to standard taxane, trastuzumab and pertuzumab.33 The results of these studies are eagerly awaited and have the potential to further modify the treatment sequencing of HER2-positive metastatic BC.
Table 1 provides a comprehensive summary of the findings from the primary studies published on ADCs in the HER2-positive BC context. It highlights the significant results that have led to noteworthy changes in clinical practices in recent years. Table 2 describes the future prospects for treating HER2-positive BC with new ADCs, which will be detailed later in this review.
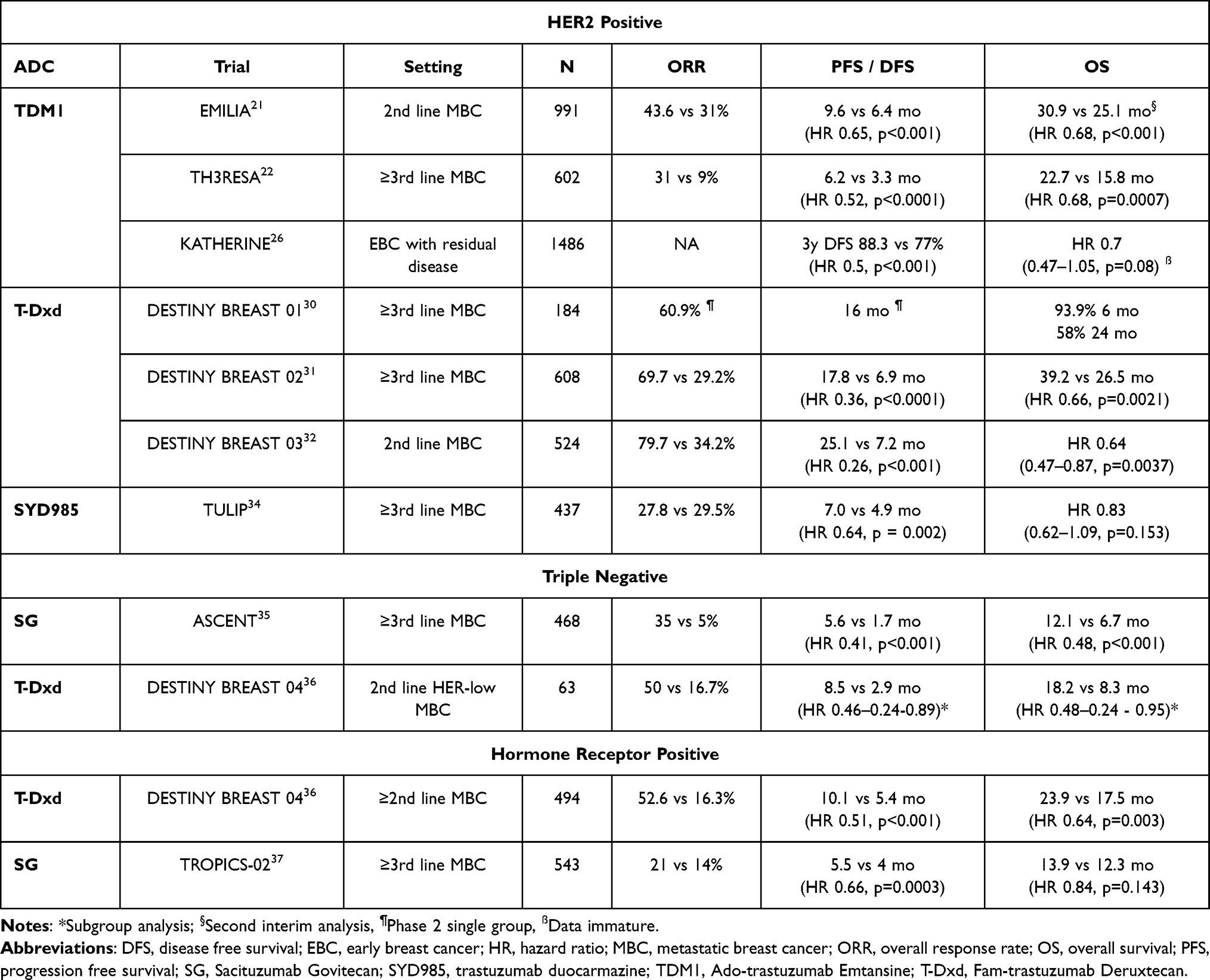 |
Table 1 Pivotal Trials with ADCs for Breast Cancer Treatment |
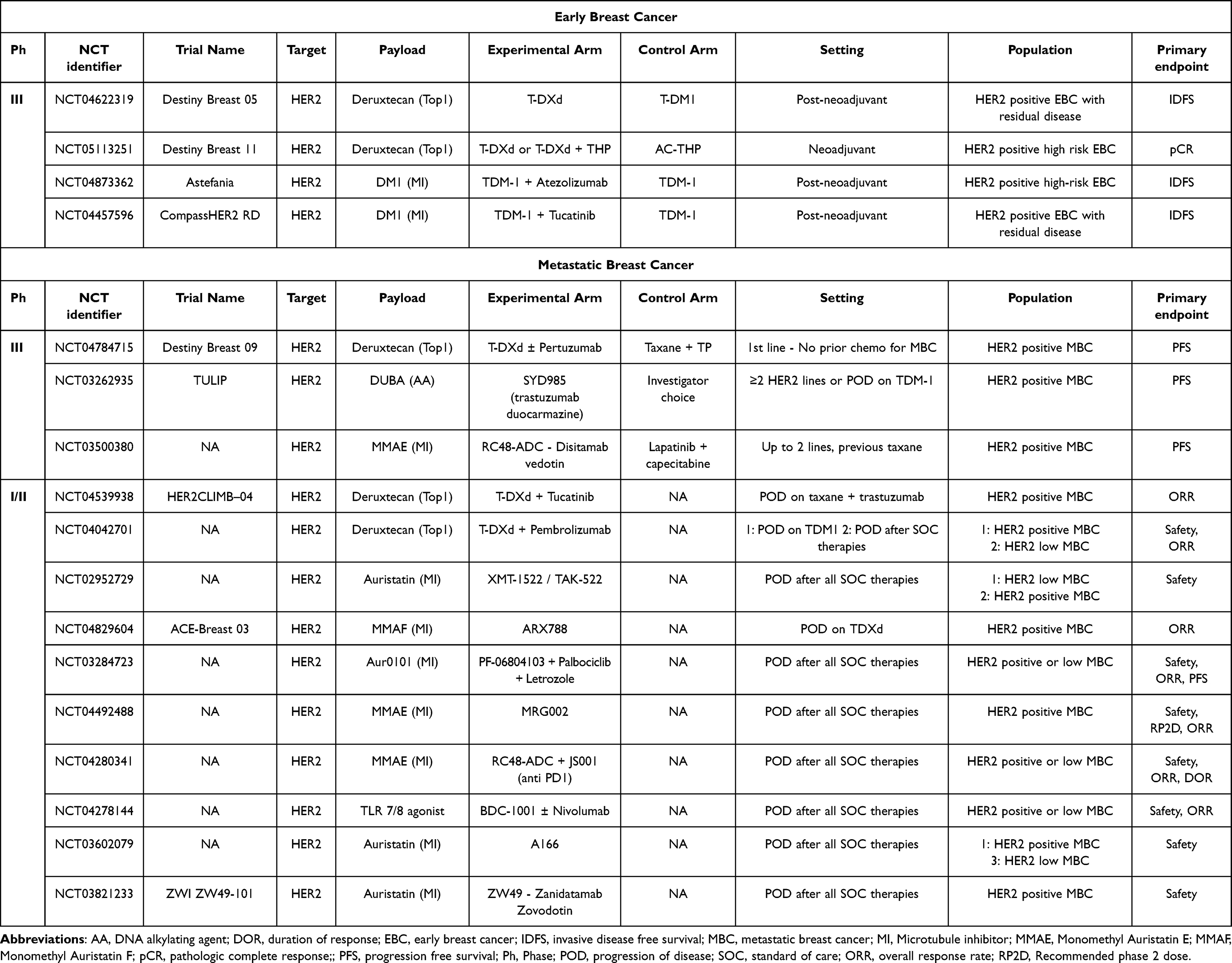 |
Table 2 Ongoing Trials: HER2-Positive Breast Cancer |
Triple-Negative Breast Cancer
Triple negative breast cancer (TNBC) accounts for approximately 10–15% of all BC cases.38 Although there have been marked advances in the understanding of molecular biology and its corresponding therapeutic modalities, the prognosis for patients with TNBC remains largely unfavorable.39 In this context, numerous pharmacological agents have been evaluated in TNBC patients, including anti-programmed cell death protein 1/programmed death-ligand 1 (PD1/PDL1) checkpoint inhibitors, poly (ADP-ribose) polymerase (PARP) inhibitors, and ADCs.6
Sacituzumab Govitecan (SG) was the first ADC that has been approved for the treatment of TNBC.40 SG consists of a fully human IgG1 mAb targeting tumor-associated trophoblast antigen 2 (Trop-2) conjugated to SN-38 (7-ethyl-10-hydroxycamptothecin), a topoisomerase I–inhibiting drug that has demonstrated potent efficacy in previous clinical trials. Trop-2 is a transmembrane calcium signal transducer that is highly expressed in multiple tumor types, including more than 90% of TNBC cases. Similar to T-DXd, SG also exhibits a bystander effect, delivering the membrane-permeable active drug SN-38 to adjacent tumor cells (Figure 1).41 The high DAR of SG, with 7.6 molecules of SN-38 conjugated to each antibody via a unique hydrolysable and proprietary linker, CL2A, is noteworthy.42
In the phase III ASCENT trial, a total of 529 patients with previously treated TNBC, who had received two or more lines of systemic therapy, were randomly assigned to receive either SG or TPC based on conventional chemotherapy regimen, which typically included capecitabine, eribulin, gemcitabine, or vinorelbine.43 The study was successful in demonstrating significant improvements in both PFS (median 5.6 versus 1.7 months; HR 0.41, P<0.001) and OS (median 12.1 versus 6.7 months; HR 0.48, P<0.001) with SG as compared to chemotherapy. Additionally, SG showed a higher ORR of 35% compared to 5% in the control group. The most frequently reported grade 3 or higher adverse events were neutropenia, leukopenia, diarrhea, and anemia.
T-DXd is another treatment option of ADC for TNBC, particularly in patients with HER2 expression by immunohistochemistry (IHC) levels 1+ or 2+/ISH negative, also known as HER2-low BC. The DESTINY-Breast04 (DB-04) trial has shown superiority of T-DXd over TPC chemotherapy in patients with HER2-low BC.44 In an exploratory analysis performed in a small subset of patients with TNBC (n=63), the median PFS was 8.5 months with T-DXd versus 2.9 months with standard therapy (HR 0.46; 95% CI, 0.24 to 0.89), the median OS was 18.2 versus 8.3 months (HR 0.48; 95% CI, 0.24 to 0.95) and ORR was 50% versus 16.7%, suggesting strong activity in this population. As of August 5, 2022, the FDA has approved T-DXd for the treatment of unresectable or metastatic HER2-low BC in patients who have previously received chemotherapy in the metastatic setting or developed disease recurrence during or within six months of completing adjuvant chemotherapy, without restrictions for the TNBC patient population.45
Table 1 also presents data from the primary studies published on ADCs in the TNBC context. Recent studies in TNBC have explored the use of novel ADCs in combination with other chemotherapy agents, immunotherapy, PI3K/AKT/m-TOR inhibitors, and PARP inhibitors, with promising results (Table 3).
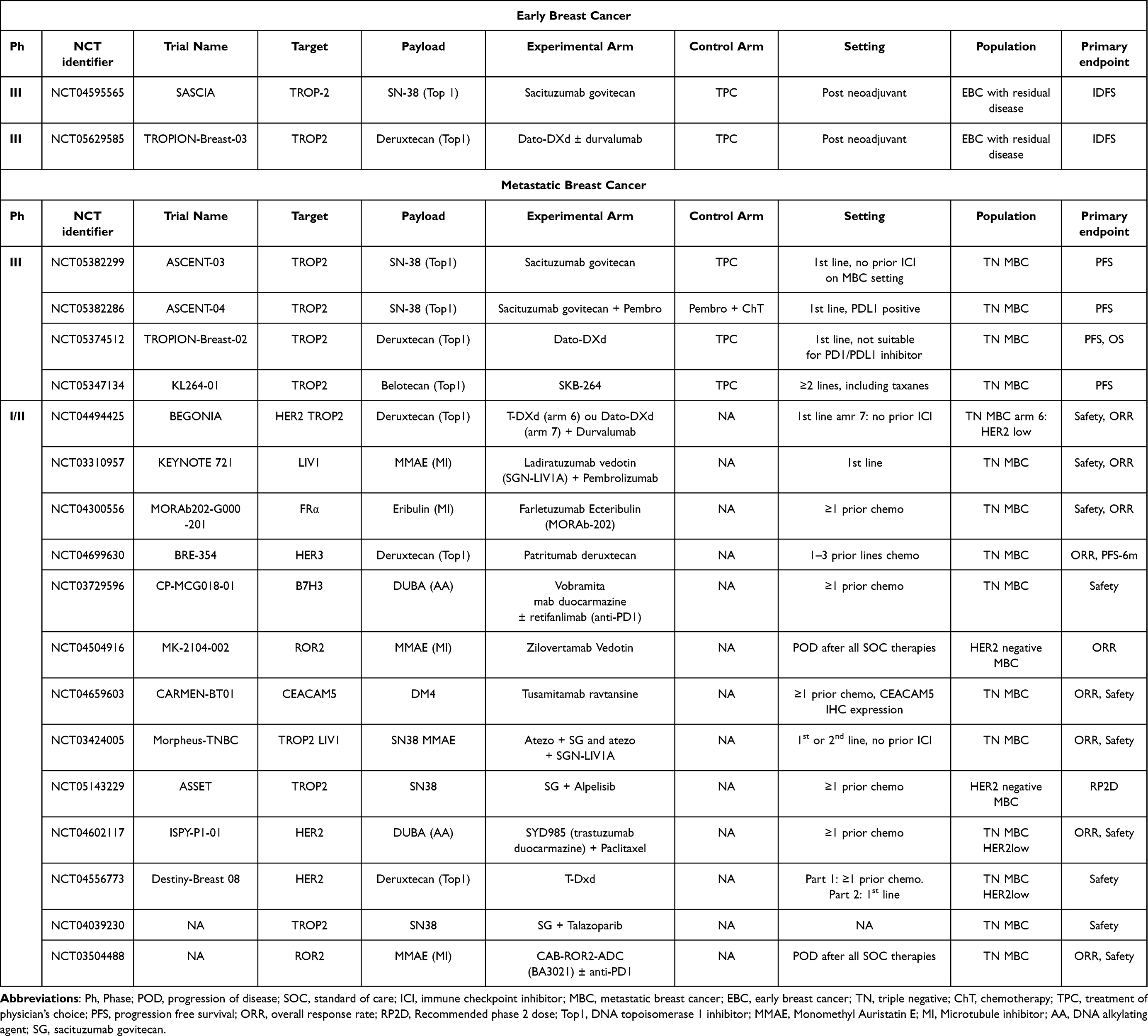 |
Table 3 Ongoing Trials: Triple Negative Breast Cancer |
Hormone Receptor Positive Breast Cancer
Approximately 70% of BC are classified as hormone receptor (HR)-positive and HER2-negative.46 The backbone treatment for advanced HR-positive HER2-negative BC involves endocrine therapy combined with target therapy. In recent years, cyclin-dependent kinase (CDK) 4/6 inhibitors have become the standard first-line therapy for these patients, given their ability to achieve a median OS of up to 57 months.47 However, managing this subtype of BC beyond CDK4/6 inhibitor progression remains challenging. In cases where patients have rapidly progressing disease or immediately life-threatening visceral metastatic disease, chemotherapy is an option as a first-line treatment.48 Indeed, response rates to later lines of endocrine therapy are low due to intrinsic or acquired resistance, with median PFS of approximately 4–5 months in HR-positive/HER2-negative metastatic BC in later lines.35,36,49
Approximately 50–80% of HER2-low BC are HR-positive, and this characteristic may change upon disease progression.50 Based on DB-04 data, practice-changing information has emerged.44 The median treatment duration was 8.2 months with T-DXd compared to 3.5 months with TPC (chemotherapy). At a median follow-up of 18.4 months, T-DXd demonstrated a significant improvement in PFS (median 10.1 versus 5.4 months; HR 0.51, p<0.001), OS (median 23.9 versus 17.5 months; HR 0.64, p=0.003), and ORR (52.6% versus 16.3%) compared with chemotherapy.
Another ADC that may be considered a treatment option for patients with HR-positive/HER2-negative BC is SG. Trop-2 is commonly upregulated in malignant breast tissues and HR-positive/HER2-negative BC has shown significantly higher Trop-2 expression than other subtypes.35 SG has demonstrated promising single-agent activity in a cohort of 54 HR-positive/HER2-negative metastatic BC patients. The patients had received a median of three prior lines of endocrine therapy (range 1–6) and two of chemotherapies (range 0–9) in the metastatic setting. SG monotherapy had a confirmed ORR of 31% and a clinical benefit (complete response, partial response, and stable disease) with duration of more than 6 months in 48% of patients. Median duration of response (DOR) was 7.4 months.51
In TROPICS-02, a global phase III trial, 543 patients were randomly assigned to SG versus TPC (eribulin, vinorelbine, capecitabine, or gemcitabine). Patients had received 2–4 prior lines of therapy, including endocrine therapy and CDK4/6 inhibitors. TROPICS-02 was positive for its primary endpoint, with a statistically significantly improvement in PFS (median 5.5 versus 4 months; HR 0.66, p=0.0003).52 In the second interim analysis, with approximately 350 death events, a statistically significant improvement in OS (median 14.4 versus 11.2 months; HR 0.79, p=0.02) was demonstrated. The benefit was seen across most of the prespecified subgroups, including patients who received at least three prior lines of chemotherapy for metastatic disease, that had visceral disease, and who were aged 65 or older. ORR was 21% versus 14% (Odds Ratio 1.63, CI 1.03–2.56; p=0.035), and the trial also demonstrated a benefit in time to deterioration of global health score/quality of life of 4.3 versus 3 months (HR 0.75; p=0.006) and time to deterioration of fatigue of 2.2 versus 1.4 months (HR 0.73; p=0.002) in favor of SG group as compared to TPC group.53 These results, though of only modest clinical relevance, pave the way for further development of SG use in the HR-positive/HER2-negative BC setting.
Table 1 additionally showcases information derived from the original studies published on advanced HR-positive HER2-negative BC setting. Most ongoing studies in this subset of patients involve ADCs targeting HER2 and TROP2. The association with hormonal therapies, as well as new targets are explored and summarized in Table 4.
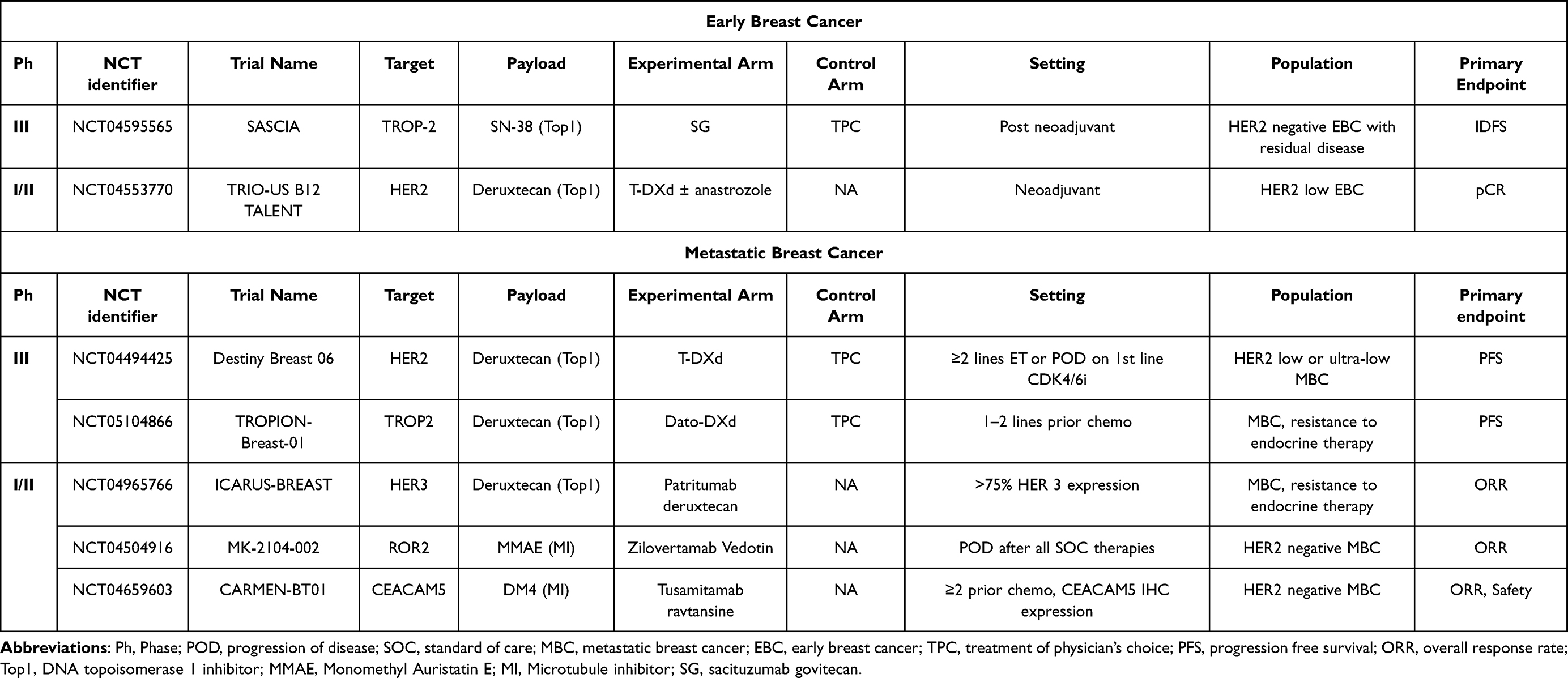 |
Table 4 Ongoing Trials: Hormone Receptor Positive Breast Cancer |
Biomarkers for ADCs
Several ADCs have demonstrated improvements irrespective of biomarker-based prediction of treatment response and potential resistance mechanisms. Nonetheless, it is anticipated that target antigens should be overexpressed on cancer cells to improve activity. However, mechanisms other than targets have been studied as a way to predict or increase the efficacy of new ADCs.
Interestingly, in some cancers from other sites, such as non-small cell lung cancer, HER2 protein expression may not be the most appropriate biomarker, and HER2 mutations have shown to be a more useful biomarker for some patients.50 The findings of the study conducted by Li et al54 suggest that HER2 ubiquitination and internalization, rather than its overexpression, play crucial roles in the endocytosis process and subsequent efficacy of certain ADCs, such as T-DM1 and T-DXd, in both lung cancer cell lines and patient-derived xenograft models. These results were translated into a 51% of response rate in a clinical trial involving 49 patients with ERBB2/HER2-amplified or mutant lung cancers who were treated with T-DM1. Additionally, in a Phase 1 study (DS8201-A-J101), T-DXd demonstrated promising antitumor activity in patients with tumors carrying HER2 mutations, with confirmed responses observed in 9 out of 19 patients (47.4%).55 The molecular changes occurring in the HER2 receptor due to HER2 mutations hold significant potential for the advances of novel anti-HER2 therapeutics with higher efficacy. These genetic modifications present auspicious prospects for the exploration and creation of more potent agents specifically designed to target HER2 and counteract its aberrant signaling pathways.56
A fascinating proposal has recently emerged to expand the concept of HER2 categorical status in BC as a gradual spectrum, leading to the potential for HER2 targeting in HER2 “ultra-low” subgroups (ie, tumors with a score of 0, exhibiting incomplete and faint staining in ≤10% of tumor cells) due to increasing understanding of the intra-tumor heterogeneity phenomena.57 In this context, the limitations of IHC for HER2 testing have prompted researchers to develop more precise and reliable methods based on artificial intelligence (AI), such as Gustavson et al’s novel HER2 Quantitative Continuous Score using deep learning-based image analysis, which has the potential to improve the prediction of patients outcomes with T-DXd.37 Recently, the HER2Complete® program, an AI-based software product, has gained popularity in the digital pathology community for its objective and reproducible ability to detect HER2 expression levels in HER2-zero and HER2-low cases, although it is not yet approved for diagnostic procedures.58
Furthermore, investigators have examined alternative technologies, such as the quantitative immunofluorescence linked to a standardized mass spectrometry HER2 array introduced by Moutafi et al, which measures absolute quantities of HER2 protein on traditional histology sections.59 Additionally, Kennedy et al have employed immunoaffinity enrichment in combination with multiple reaction monitoring-mass spectrometry (immuno-MRM-MS), demonstrating enhanced consistency with existing assays, particularly at lower HER2 expression levels.60 Xu et al also proposed that molecular techniques like mRNA could be valuable in accurately characterizing HER2-low cancer for making treatment decisions, owing to their broader dynamic scope.61 These approaches may offer more reliable and accurate HER2 testing for guiding treatment decisions in patients with BC.
Several trials evaluating ADCs efficacy were designed without specific biomarker selection. For instance, SG and enfortumab vedotin (EV) were tested in tumors with previously unknown overexpression of their target antigens (Trop-2 and Nectin-4, respectively), despite their results demonstrating efficacy regardless of the level of antigen expression.40,62 In the ASCENT trial, patients with high Trop-2 expression had a better PFS and ORR than patients with low Trop-2 expression, but SG outperformed chemotherapy in all subgroups.63 Although Trop-2 is not currently used as a biomarker, better assays for Trop-2, as well as additional ADC options, may alter this concept in the future. The activity of EV may also be influenced by Nectin-4 expression, although clinical confirmation is lacking.64
Current Understanding of Mechanisms of Resistance to ADCs
This review has previously highlighted the mechanism of action of ADCs and their effectiveness in the treatment of BC. However, it has been observed that many patients will inevitably develop resistance to these drugs, resulting in recurrence or disease progression. Treatment resistance can manifest at the outset of therapy, referred to as primary resistance, or after exposure to the drug for several months, known as secondary resistance. Considering the three components of an ADC, it is important to note that the mechanism of resistance can arise from the antibody, the linker or the payload. This section will focus on the three ADCs approved for BC treatment (T-DM1, T-DXd and SG) and examine their primary mechanisms of resistance, as well as potential solutions to overcome resistance.
Several potential mechanisms of resistance to T-DM1 have been proposed, primarily related to the disruption of trastuzumab-mediated effects or the intracellular metabolism of T-DM1.65 The first mechanism is the subversion of trastuzumab-mediated effects. HER2 loss, which includes HER2 downregulation, subtype switching, and clonal selection, is a known resistance mechanism for trastuzumab.66 Additionally, T-DM1 does not possess a bystander effect and thus relies on higher HER2 expression in tumor cells to bind the drug. With prolonged exposure to T-DM1, a decreased HER2 expression relative to prior cells may result in resistance.67 The second mechanism is the reduced binding of T-DM1. HER-2 is a transmembrane protein, and T-DM1 binding depends on the molecular fit of trastuzumab with the extracellular subdomain. If the protein becomes truncated for any reason, it can cause impairment by reducing DM1 internalization and its effects.68 Dysregulation of PI3K signaling is another potential resistance mechanism. PIK3CA mutations are associated with reduced pCR rates in primary HER2-positive BC.69 However, clinical studies have evaluated response rates regarding PI3K status (mutated/wild). In the TH3RESA and EMILIA trials, it was observed that T-DM1 could overcome this resistance. These data suggest that altering the PI3K pathway could lead to resistance to lapatinib, pertuzumab, and trastuzumab but not to T-DM1.70,71 However, in the adjuvant setting, data from the KATHARINE trial failed to show any predictive value (of greater benefit from TDM1 over trastuzumab) of PI3K mutations, gene expression levels of HER2 or immune activation pathways.72 Finally, increased drug efflux is another potential mechanism of resistance for many ADCs. One of the mechanisms by which BC cells acquire drug resistance to T-DM1 is increased expression of ADC transporters, which actively efflux the drug out of cells.67
Currently, meaningful data about resistance to T-DXd comes from the translational analysis of the DAISY trial.73 Whole exome sequencing was performed on some BC biopsies at baseline and after clinical progression. Biomarkers for response and resistance are being sought. ERBB2/HER2 gene amplification is not associated with clinical response to T-DXd, and no other driver alterations have been associated with resistance. Since T-DXd has a bystander effect, it appears to be less reliant on high HER2 expression in tumor cells to bind the drug, as evidenced by the drug’s benefit in HER2-low BC.44 Findings of hemizygous deletion of ERBB2 (6%) in baseline biopsies of non-responders suggest that this deletion may be associated with primary resistance. In contrast, mutations in SLX4, observed in 20% (2/10) of biopsies of progression and corroborated by in vitro experiments, appear to be associated with secondary resistance. Further studies are required to confirm these potential biomarkers.
The modulation of therapeutic efficacy and patient selection for SG may be influenced by the lower expression of Trop-2, as observed in the ASCENT trial. Patients with metastatic TNBC and high or intermediate Trop-2 expression apparently demonstrated higher ORR (44% and 39%, respectively) compared to those with low Trop-2 expression (22%).68 Another study analyzing somatic alterations in SG-treated patients indicated that alterations in Trop-2 (antibody) or SN-38 (payload) might contribute to resistance mechanisms against this class of drugs. The analysis revealed that resistance to SG due to topoisomerase-1 payload alterations could lead to cross-resistance to ADCs with similar payloads; however, using a different payload with the same antibody could be beneficial. Conversely, resistance resulting from Trop-2 alteration would likely lead to cross-resistance to other Trop-2-directed ADCs, but not to non-Trop-2-directed ADCs, irrespective of payload.74
In general, the composition of ADCs (linker, payload, and antibody) offers the prospect of modifying some elements to create novel compounds that can overcome resistance. Manipulation of any of these components would enable the development of potential drugs against various tumor types. As new ADCs gain clinical approval, novel resistance mechanisms may emerge, and new approaches to overcoming tumor cell resistance may be identified.
Future Perspectives
Numerous ADCs with distinct configurations, targets, and payloads are currently under careful examination for different subtypes of BC. A multitude of additional ADCs specifically designed to target HER2 are presently under investigation in Phase I and II clinical trials, with comprehensive information available in Table 2, compiling their respective particulars. They are categorized based on the antibody used (including those exhibiting higher affinity for HER2 compared to trastuzumab), the nature of the linker (whether it is cleavable or non-cleavable), and the specific payload employed. Other ADCs have incorporated novel cytotoxic agents, such as auristatin derivatives known for their potent inhibition of microtubules, even at low doses. The ongoing development of these new ADCs poses the challenge of achieving improved blood stability, reduced adverse effects, and the employment of more potent antibodies.
Improvements in the diverse components of ADCs are essential for enhancing their efficacy and safety. Various innovative ADC formats have been developed, including bispecific ADCs, probody–drug conjugates, immune-stimulating ADCs, protein-degrader ADCs, and dual-drug ADCs.11 Bispecific ADCs present promising therapeutic possibilities, targeting a wider spectrum of antigens and showing potential safety and activity enhancements. However, potential pitfalls must be cautiously considered, such as the risk of unintended receptor activation and agonistic activity.75 Probody–drug conjugates offer potential in targeting antigens with undesirable levels of expression in nonmalignant tissues. Nevertheless, their potential in effectively targeting specific cancer subtypes requires further elucidations through preclinical and clinical research.76
Immune-stimulating ADCs show potential as a new class of cancer immunotherapy, with initial clinical trial results showing promise, but further research is crucial to optimize their efficacy and safety profiles.77 Antibody-directed protein degraders have the potential to offer unique therapeutic interventions for cancer patients. However, further studies are needed to identify safe and potentially effective conjugates.78 The clinical potential of dual-drug ADCs has been explored further, showing synergistic antitumor activity and immunological memory in some cases. Nonetheless, not all studies testing dual-drug ADCs have demonstrated meaningful synergistic effects, hence demonstrating the need for further research and evaluation.79
Trastuzumab duocarmazine (SYD985) is an ADC containing a humanized anti-HER2 monoclonal antibody linked chemically to a duocarmycin compound through a cleavable linker, yielding a DAR of 2.8:1. Notably, the duocarmazine payload is present as a cell-permeable pro-drug (seco-duocarmycin-hydroxybenzamide-azaindole - seco-DUBA) that undergoes enzymatic cleavage by proteases within intracellular lysosomes post-internalization. The resulting active toxin (DUBA) subsequently acts by alkylating the DNA, causing DNA damage and eventual cell demise. Additionally, this ADC demonstrates cytotoxicity through a bystander effect mechanism.80 In a phase I study81 involving patients with treatment-refractory locally advanced or metastatic solid tumors displaying variable HER2 status, SYD985 exhibited a promising ORR of 33% in HER2-positive BC. Consequently, the FDA accepted a biologics license application (BLA) for SYD985 in July 2022, seeking approval for the treatment of patients with HER2-positive unresectable locally advanced or metastatic BC. The BLA submission is based on the pivotal phase III TULIP trial, which was presented at the European Society for Medical Oncology (ESMO) in 2021.82 In this trial, SYD985 demonstrated a significant improvement in PFS as compared to TPC in the specified patient population, fulfilling the primary endpoint with a nearly 40% reduction in the risk of centrally reviewed disease progression (median PFS of 7 versus 4.9 months, HR 0.64, p = 0.002).
An emerging avenue of research involves bispecific ADCs, which have the potential to bind to two different regions of target proteins simultaneously. A prime example of such is zanidatamab zovodotin (ZW49), an anti-HER2 biparatopic antibody that selectively targets extracellular domains 2 and 4 of the HER2 protein. This unique configuration results in multiple mechanisms of action, including dual HER2 signal blockade, enhanced antibody binding, receptor clustering, removal of HER2 from the cell surface, and potent effector function. Recently published data from a study involving heavily pretreated HER2-positive metastatic breast cancer patients revealed an ORR of 13%, with 38% achieving stable disease.83
Disitamab vedotin (RC-48) represents a novel anti-HER2 ADC that comprises disitamab, a novel anti-HER2 Mab, conjugated to monomethyl auristatin E (MMAE) via a cleavable linker. This ADC has obtained regulatory approval in China for the treatment of gastric and urothelial cancers. Notably, it exhibits a higher binding affinity for HER2 targets compared to trastuzumab, facilitating enhanced endocytosis. The linker used, Mc-VC-pa, confers increased stability in human plasma and demonstrates efficient cleavage mediated by human cathepsin enzymes. Despite possessing a lower DAR of 4:1 as opposed to the 8:1 ratio of T-DXd, RC-48 exhibits remarkable cytotoxicity even at very low concentrations.34 In a Chinese clinical trial involving 118 patients with metastatic BC, the ORR was found to be 42.9% for HER2-positive cases and 39.6% for HER2-low cases.84 Currently, an ongoing phase II study is comparing the efficacy of RC48 with capecitabine + lapatinib in patients with locally advanced or metastatic HER2-positive breast cancer presenting with liver metastasis.
A166 is an ADC composed of trastuzumab conjugated to the potent payload duostatin-5. Preliminary efficacy data from a phase I trial were initially presented in 2020, with subsequent updates shared at the ASCO meetings in 2021 and 2022.85 The most frequently observed grade ≥ 3 adverse events included corneal epitheliopathy, blurred vision, and ulcerative keratitis. A166 demonstrated an impressive objective response rate (ORR) of 73.91% (17/23; 95% CI, 51.59–89.77) and 68.57% (24/35; 95% CI, 50.71–83.15) in the 4.8 mg/kg and 6.0 mg/kg dose cohorts, respectively. The median PFS was reported as 12.3 months (95% CI, 6.0 - not reached) in the 4.8 mg/kg cohort and 9.4 months (95% CI, 4.0–10.4) in the 6.0 mg/kg cohort.
XMT-1522 represents a novel anti-HER2 ADC that incorporates a human IgG1 anti-HER2 mAb (HT-19) targeting domain IV of the HER2 protein. Importantly, this epitope is distinct from the trastuzumab-binding site, ensuring non-competitive binding with trastuzumab for HER2. In a phase I dose escalation trial involving patients with HER2-expressing breast, lung, and gastric tumors, XMT-1522 demonstrated a noteworthy disease control rate of 83%.86
An overview of ongoing clinical trials investigating ADCs for the treatment of TNBC is provided in Table 3. Patritumab deruxtecan (U3-1302) represents an ADC consisting of a recombinant fully human monoclonal antibody targeting HER3, conjugated to a linker incorporating a topoisomerase I inhibitor. The BRE-354 phase II trial aims to assess the efficacy of U3-1402 in patients with metastatic BC, specifically focusing on the TNBC population. Eligible patients in the TNBC subgroup should have received one to three prior lines of chemotherapy in the metastatic setting. The primary endpoints of the study are the ORR of U3-1402 as a single agent and the six-month PFS in patients with metastatic BC.87 In December 2021, this drug was granted breakthrough therapy designation by the FDA for patients with metastatic EGFR-mutated non-small cell lung cancer.
The TROPION-PanTumor01 trial is a phase I trial that showed encouraging response rates (ORR 32%), median PFS 4.4 months and median OS 13.5 months in heavily pretreated metastatic TNBC patients treated with datopotamab deruxtecan (DS-1062), a Trop-2 directed ADC.88 The BEGONIA phase Ib/II trial showed that the combination of DS-1062 with durvalumab reached an ORR of 73.6% in previously untreated metastatic TNBC patients, regardless of PD-L1 expression.89 TROPION-Breast02 study is a phase III trial currently enrolling patients with metastatic or inoperable TNBC who are not eligible for treatment with anti-PD-1/PD-L1 agents. This study aims to compare the efficacy of DS-1062 versus TPC. The primary endpoints of the study are PFS and OS in these patient populations. The results of this study are highly anticipated, as it may offer an alternative treatment option for patients who are not candidates for first-line immunotherapy treatment.90
Another ADC targeting Trop-2 is SKB264, which utilizes 2-methylsulfonyl pyrimidine as the linker to conjugate its payload (KL610023), a belotecan-derivative topoisomerase I inhibitor. The KL264-01 trial is a randomized, open-label, multicenter phase III trial that aims to compare the efficacy of SKB264 versus TPC in patients with unresectable locally advanced, recurrent, or metastatic TNBC who have received more than two lines of treatment. The primary endpoint of the study is PFS, based on a planned enrollment of 254 patients.91
Ladiratuzumab vedotin (SGN-LIV1A), a humanized IgG1 antibody that specifically targets the LIV-1 proteins expressed in approximately 90% of breast cancer cells. Its payload consists of the potent microtubule inhibitor known as monomethyl auristatin E (MMAE).92 SGN-LIV1A is being evaluated both as a monotherapy and in combination with immunotherapy agents.93,94 Trastuzumab duocarmazine (SYD985), previously mentioned, is also being examined in combination with Paclitaxel in the context of TNBC (NCT04602117).95,96 Another noteworthy ADC is MGC018, which employs an anti-B7-H3 antibody linked to a duocarmycin payload. This agent is currently being investigated in an expansion cohort phase II trial that includes TNBC patients, and results from this study are anticipated in the coming years.97 BA3021, an ADC targeting ROR2 (CAB-ROR2-ADC) and utilizing MMAE as its payload, is being assessed in a phase 1/2 trial to evaluate its safety and efficacy in patients with advanced solid tumors. The subsequent phase II component of the study aims to determine the drug’s effectiveness as a monotherapy and in combination with immunotherapy.98
Additionally, a novel ADC called tusamitamab ravtansine (SAR408701) selectively targets CEACAM5 and is being evaluated in a multi-cohort, phase II trial involving patients with CEACAM5-positive solid tumors. Cohort A of this study includes patients with metastatic breast cancer who have undergone at least two prior cytotoxic chemotherapy regimens for non-TNBC or at least one regimen for TNBC, with a maximum of four regimens in the locally recurrent or metastatic setting. Although the trial was not explicitly designed for the TNBC population, it will provide valuable insights into the efficacy of this new ADC in this particular subgroup.99 Farletuzumab ecteribulin (MORAb-202) represents another ADC consisting of the humanized anti-FRα monoclonal antibody, farletuzumab, conjugated to the cytotoxic microtubule inhibitor eribulin. This drug will be evaluated in a multicenter, open-label phase 1/2 trial involving selected tumor types, including TNBC.100
Finally, an intracellular adhesion molecule-1 highly enriched on cell surface of TNBC patients (ICAM1) is being investigated as a new target in this poor prognostic population. An ICAM1 ADC conjugated with MMAE was identified as the optimal formulation to achieve efficacy and safety, and further studies are awaited for testing it in the TNBC population.101
Conclusions
In summary, traditional ADCs such as T-DM1, T-DXd, and SG have already been incorporated into BC treatment protocols across various settings. As technological advances progress, the development of personalized ADCs is expected to become a reality in the future. This involves creating tailored combinations of antibodies, linkers, and payloads based on individual patient tumor antigens and other characteristics to overcome resistance mechanisms. However, the primary challenge is efficiently producing personalized ADCs within reasonable timeframes and at reasonable costs. Additionally, future developments will be able to explore potential synergies between checkpoint inhibitors, tyrosine kinase inhibitors, and ADCs.
Biomarkers play a crucial role in the design and optimization of ADCs for BC treatment. Although some ADCs have shown efficacy regardless of biomarker-based predictions, identifying robust predictive biomarkers remains crucial. Following this, conventional understanding of HER2 overexpression as a biomarker for ADC efficacy is now being questioned, given the emergence of next-generation anti-HER2 ADCs that demonstrate activity even in tumors with low levels of HER2 expression. Due to limitations associated with current biomarker assessment methods, such as IHC, there is ongoing exploration of more precise and reliable techniques based on AI and molecular approaches.
Ethics Approval
As a literature data review, there was no need for approval by the local institutional review board.
Acknowledgments
The authors express their sincere gratitude to Dr. Jose Bines for his invaluable collaboration and insightful input throughout the development of this manuscript. His expertise and guidance have significantly enhanced the quality of our work. Additionally, the authors would like to acknowledge Novartis for their contribution in creating the images used in this article. Their support in visually presenting the data has greatly enriched the overall presentation and impact of our findings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that this study has received no financial support.
Disclosure
Dr Gustavo Bretas reports personal fees, non-financial support from Daiichi Sankyo, AstraZeneca, Roche, and Eli-Lilly, outside the submitted work. Dr Max Mano reports personal fees for lectures, advisory boards and/or travel grants from AstraZeneca, Daiichi-Sankyo, Roche (also Principal Investigator for clinical trials), Novartis, Lilly, Pfizer (also Principal Investigator for clinical trials), Gilead, MD Health, and MSD, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Falzone L, Salomone S, Libra M. Evolution of cancer pharmacological treatments at the turn of the third millennium. Front Pharmacol. 2018;9:1300. doi:10.3389/fphar.2018.01300
3. Twelves C, Jove M, Gombos A, Awada A. Cytotoxic chemotherapy: still the mainstay of clinical practice for all subtypes metastatic breast cancer. Crit Rev Oncol Hematol. 2016;100:74–87. doi:10.1016/j.critrevonc.2016.01.021
4. Strebhardt K, Ullrich A. Paul Ehrlich’s magic bullet concept: 100 years of progress. Nat Rev Cancer. 2008;8(6):473–480. doi:10.1038/nrc2394
5. Chau CH, Steeg PS, Figg WD. Antibody–drug conjugates for cancer. Lancet. 2019;394(10200):793–804. doi:10.1016/S0140-6736(19)31774-X
6. Lambert JM, Berkenblit A. Antibody–drug conjugates for cancer treatment. Annu Rev Med. 2018;69(1):191–207. doi:10.1146/annurev-med-061516-121357
7. Rugo HS, Bianchini G, Cortes J, Henning JW, Untch M. Optimizing treatment management of trastuzumab deruxtecan in clinical practice of breast cancer. ESMO Open. 2022;7(4):100553. doi:10.1016/j.esmoop.2022.100553
8. Mahmood I. Clinical pharmacology of antibody-drug conjugates. Antibodies Basel Switz. 2021;10(2):20. doi:10.3390/antib10020020
9. Loganzo F, Sung M, Gerber HP. Mechanisms of resistance to antibody-drug conjugates. Mol Cancer Ther. 2016;15(12):2825–2834. doi:10.1158/1535-7163.MCT-16-0408
10. García-Alonso S, Ocaña A, Pandiella A. Resistance to antibody-drug conjugates. Cancer Res. 2018;78(9):2159–2165. doi:10.1158/0008-5472.CAN-17-3671
11. Tsuchikama K, Anami Y, Ha SYY, Yamazaki CM. Exploring the next generation of antibody–drug conjugates. Nat Rev Clin Oncol. 2024;21:1–21. doi:10.1038/s41571-023-00821-7
12. Michel LL, Bermejo JL, Gondos A, Marmé F, Schneeweiss A. T-DM1 as a new treatment option for patients with metastatic HER2-positive breast cancer in clinical practice. Anticancer Res. 2015;35(9):5085–5090.
13. Boyraz B, Sendur MAN, Aksoy S, et al. Trastuzumab emtansine (T-DM1) for HER2-positive breast cancer. Curr Med Res Opin. 2013;29(4):405–414. doi:10.1185/03007995.2013.775113
14. Verma S, Miles D, Gianni L, et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N Engl J Med. 2012;367(19):1783–1791. doi:10.1056/NEJMoa1209124
15. Krop IE, Kim SB, Martin AG, et al. Trastuzumab emtansine versus treatment of physician’s choice in patients with previously treated HER2-positive metastatic breast cancer (TH3RESA): final overall survival results from a randomised open-label Phase 3 trial. Lancet Oncol. 2017;18(6):743–754. doi:10.1016/S1470-2045(17)30313-3
16. Perez EA, Barrios C, Eiermann W, et al. Trastuzumab emtansine with or without pertuzumab versus trastuzumab plus taxane for human epidermal growth factor receptor 2–positive, advanced breast cancer: primary results from the phase III MARIANNE study. J Clin Oncol. 2017;35(2):141–148. doi:10.1200/JCO.2016.67.4887
17. Swain SM, Miles D, Kim SB, et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): end-of-study results from a double-blind, randomised, placebo-controlled, phase 3 study. Lancet Oncol. 2020;21(4):519–530. doi:10.1016/S1470-2045(19)30863-0
18. Hurvitz SA, Martin M, Jung KH, et al. Neoadjuvant trastuzumab emtansine and pertuzumab in human epidermal growth factor receptor 2-positive breast cancer: three-year outcomes from the phase III KRISTINE study. J Clin Oncol off J Am Soc Clin Oncol. 2019;37(25):2206–2216. doi:10.1200/JCO.19.00882
19. von Minckwitz G, Huang CS, Mano MS, et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med. 2019;380(7):617–628. doi:10.1056/NEJMoa1814017
20. Kowalczyk L, Bartsch R, Singer CF, Farr A. Adverse events of trastuzumab emtansine (T-DM1) in the treatment of HER2-positive breast cancer patients. Breast Care Basel Switz. 2017;12(6):401–408. doi:10.1159/000480492
21. Narayan P, Osgood CL, Singh H, et al. FDA approval summary: fam-trastuzumab deruxtecan-nxki for the treatment of unresectable or metastatic HER2-positive breast cancer. Clin Cancer Res off J Am Assoc Cancer Res. 2021;27(16):4478–4485. doi:10.1158/1078-0432.CCR-20-4557
22. Nguyen X, Hooper M, Borlagdan JP, Palumbo A. A review of fam-trastuzumab deruxtecan-nxki in HER2-positive breast cancer. Ann Pharmacother. 2021;55(11):1410–1418. doi:10.1177/1060028021998320
23. Tamura K, Tsurutani J, Takahashi S, et al. Trastuzumab deruxtecan (DS-8201a) in patients with advanced HER2-positive breast cancer previously treated with trastuzumab emtansine: a dose-expansion, phase 1 study. Lancet Oncol. 2019;20(6):816–826. doi:10.1016/S1470-2045(19)30097-X
24. Modi S, Saura C, Yamashita T, et al. Trastuzumab deruxtecan in previously treated HER2-positive breast cancer. N Engl J Med. 2020;382(7):610–621. doi:10.1056/NEJMoa1914510
25. André F, Park YH, Kim SB, et al. Trastuzumab deruxtecan versus treatment of physician’s choice in patients with HER2-positive metastatic breast cancer (DESTINY-Breast02): a randomised, open-label, multicentre, phase 3 trial. Lancet. 2023;1:1.
26. Hurvitz SA, Hegg R, Chung WP, et al. Trastuzumab deruxtecan versus trastuzumab emtansine in patients with HER2-positive metastatic breast cancer: updated results from DESTINY-Breast03, a randomised, open-label, phase 3 trial. Lancet. 2023;401(10371):105–117. doi:10.1016/S0140-6736(22)02420-5
27. Jerusalem G, Park YH, Yamashita T, et al. Trastuzumab deruxtecan in HER2-positive metastatic breast cancer patients with brain metastases: a DESTINY-breast01 subgroup analysis. Cancer Discov. 2022;12(12):2754–2762. doi:10.1158/2159-8290.CD-22-0837
28. Bartsch R, Berghoff AS, Furtner J, et al. Trastuzumab deruxtecan in HER2-positive breast cancer with brain metastases: a single-arm, phase 2 trial. Nat Med. 2022;28(9):1840–1847. doi:10.1038/s41591-022-01935-8
29. Pérez-García JM, Vaz Batista M, Cortez P, et al. Trastuzumab deruxtecan in patients with central nervous system involvement from HER2-positive breast cancer: the DEBBRAH trial. Neuro-Oncol. 2023;25(1):157–166. doi:10.1093/neuonc/noac144
30. Guo Z, Ding Y, Wang M, Liu J, Zhai Q, Du Q. Safety of trastuzumab deruxtecan: a meta-analysis and pharmacovigilance study. J Clin Pharm Ther. 2022;47(11):1837–1844. doi:10.1111/jcpt.13777
31. Daiichi Sankyo, Inc. A phase 3, multicenter, randomized, open-label, active-controlled study of trastuzumab deruxtecan (T-DXd) versus trastuzumab emtansine (T-DM1) in participants with high-risk HER2-positive primary breast cancer who have residual invasive disease in breast or axillary lymph nodes following neoadjuvant therapy (DESTINY-Breast05). clinicaltrials.gov; 2023. Available from: https://clinicaltrials.gov/ct2/show/NCT04622319.
32. AstraZeneca. A phase 3 open-label trial of neoadjuvant trastuzumab deruxtecan (T-DXd) Monotherapy or T-DXd followed by thp compared to ddac-thp in participants with high-risk HER2-positive early-stage breast cancer (DESTINY-Breast11). clinicaltrials.gov; 2023. Available from: https://clinicaltrials.gov/ct2/show/NCT05113251.
33. AstraZeneca. Phase III study of trastuzumab deruxtecan (T-DXd) with or without pertuzumab versus taxane, trastuzumab and pertuzumab in HER2-positive, first-line metastatic breast cancer (DESTINY-Breast09). clinicaltrials.gov; 2023. Available from: https://clinicaltrials.gov/ct2/show/NCT04784715.
34. Shi F, Liu Y, Zhou X, Shen P, Xue R, Zhang M. Disitamab vedotin: a novel antibody-drug conjugates for cancer therapy. Drug Deliv. 2022;29(1):1335–1344. doi:10.1080/10717544.2022.2069883
35. Vidula N, Yau C, Rugo HS. Trop2 gene expression (Trop2e) in primary breast cancer (BC): correlations with clinical and tumor characteristics. J Clin Oncol. 2017;35(15_suppl):1075. doi:10.1200/JCO.2017.35.15_suppl.1075
36. Bardia A, Mayer IA, Diamond JR, et al. Efficacy and safety of anti-trop-2 antibody drug conjugate sacituzumab govitecan (IMMU-132) in heavily pretreated patients with metastatic triple-negative breast cancer. J Clin Oncol off J Am Soc Clin Oncol. 2017;35(19):2141–2148. doi:10.1200/JCO.2016.70.8297
37. Gustavson M, Haneder S, Spitzmueller A, et al. Abstract PD6-01: novel approach to HER2 quantification: digital pathology coupled with AI-based image and data analysis delivers objective and quantitative HER2 expression analysis for enrichment of responders to trastuzumab deruxtecan (T-DXd; DS-8201), specifically in HER2-low patients. Cancer Res. 2021;81(4_Supplement):1.
38. Zagami P, Carey LA. Triple negative breast cancer: pitfalls and progress. NPJ Breast Cancer. 2022;8(1):95. doi:10.1038/s41523-022-00468-0
39. Trivers KF, Lund MJ, Porter PL, et al. The epidemiology of triple-negative breast cancer, including race. Cancer Causes Control CCC. 2009;20(7):1071–1082. doi:10.1007/s10552-009-9331-1
40. Wahby S, Fashoyin-Aje L, Osgood CL, et al. FDA approval summary: accelerated approval of sacituzumab govitecan-hziy for third-line treatment of metastatic triple-negative breast cancer. Clin Cancer Res. 2021;27(7):1850–1854. doi:10.1158/1078-0432.CCR-20-3119
41. Kwapisz D. Sacituzumab Govitecan-hziy in Breast Cancer. Am J Clin Oncol. 2022;45(7):279–285. doi:10.1097/COC.0000000000000919
42. Weiss J, Glode A, Messersmith WA, Diamond J. Sacituzumab govitecan: breakthrough targeted therapy for triple-negative breast cancer. Expert Rev Anticancer Ther. 2019;19(8):673–679. doi:10.1080/14737140.2019.1654378
43. Bardia A, Hurvitz SA, Tolaney SM, et al. Sacituzumab govitecan in metastatic triple-negative breast cancer. N Engl J Med. 2021;384(16):1529–1541. doi:10.1056/NEJMoa2028485
44. Modi S, Jacot W, Yamashita T, et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387(1):9–20. doi:10.1056/NEJMoa2203690
45. Narayan P, Dilawari A, Osgood C, et al. US food and drug administration approval summary: fam-trastuzumab deruxtecan-nxki for human epidermal growth factor receptor 2-low unresectable or metastatic breast cancer. J Clin Oncol off J Am Soc Clin Oncol. 2023;2023:JCO2202447.
46. Howlader N, Altekruse SF, Li CI, et al. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J Natl Cancer Inst. 2014;106(5):dju055. doi:10.1093/jnci/dju055
47. Lobbezoo DJA, van Kampen RJW, Voogd AC, et al. Prognosis of metastatic breast cancer subtypes: the hormone receptor/HER2-positive subtype is associated with the most favorable outcome. Breast Cancer Res Treat. 2013;141(3):507–514. doi:10.1007/s10549-013-2711-y
48. Matutino A, Joy AA, Brezden-Masley C, Chia S, Verma S. Hormone receptor-positive, HER2-negative metastatic breast cancer: redrawing the lines. Curr Oncol Tor Ont. 2018;25(Suppl 1):1.
49. McAndrew NP, Finn RS. Clinical review on the management of hormone receptor-positive metastatic breast cancer. JCO Oncol Pract. 2022;18(5):319–327. doi:10.1200/OP.21.00384
50. Li BT, Shen R, Buonocore D, et al. Ado-trastuzumab emtansine for patients With HER2-mutant lung cancers: results from a phase II basket trial. J Clin Oncol off J Am Soc Clin Oncol. 2018;36(24):2532–2537. doi:10.1200/JCO.2018.77.9777
51. Bardia A, Diamond JR, Vahdat LT, et al. Efficacy of sacituzumab govitecan (anti-Trop-2-SN-38 antibody-drug conjugate) for treatment-refractory hormone-receptor positive (HR+)/HER2- metastatic breast cancer (mBC). J Clin Oncol. 2018;36(15_suppl):1004. doi:10.1200/JCO.2018.36.15_suppl.1004
52. Rugo HS, Bardia A, Marmé F, et al. Sacituzumab govitecan in hormone receptor–positive/human epidermal growth factor receptor 2–negative metastatic breast cancer. J Clin Oncol. 2022;40(29):3365–3376. doi:10.1200/JCO.22.01002
53. Rugo HS, Bardia A, Marmé F, et al. LBA76 Overall survival (OS) results from the phase III TROPiCS-02 study of sacituzumab govitecan (SG) vs treatment of physician’s choice (TPC) in patients (pts) with HR+/HER2- metastatic breast cancer (mBC). Ann Oncol. 2022;33:1.
54. Li BT, Michelini F, Misale S, et al. HER2-mediated internalization of cytotoxic agents in ERBB2 amplified or mutant lung cancers. Cancer Discov. 2020;10(5):674–687. doi:10.1158/2159-8290.CD-20-0215
55. Tsurutani J, Iwata H, Krop I, et al. Targeting HER2 with trastuzumab deruxtecan: a dose-expansion, phase i study in multiple advanced solid tumors. Cancer Discov. 2020;10(5):688–701. doi:10.1158/2159-8290.CD-19-1014
56. Heymach J, Negrao M, Robichaux J, et al. OA02.06 A Phase II trial of poziotinib in EGFR and HER2 exon 20 mutant non-small cell lung cancer (NSCLC). J Thorac Oncol. 2018;13(10):S323–S324. doi:10.1016/j.jtho.2018.08.243
57. Venetis K, Crimini E, Sajjadi E, et al. HER2 low, ultra-low, and novel complementary biomarkers: expanding the spectrum of HER2 positivity in breast cancer. Front Mol Biosci. 2022;9. doi:10.3389/fmolb.2022.834651
58. Paige answers call to better identify breast cancer patients with low expression of HER2. 2022. Available from: https://www.businesswire.com/news/home/20220623005253/en/Paige-Answers-Call-to-Better-Identify-Breast-Cancer-Patients-with-Low-Expression-of-HER2.
59. Moutafi M, Robbins CJ, Yaghoobi V, et al. Quantitative measurement of HER2 expression to subclassify ERBB2 unamplified breast cancer. Lab Investig J Tech Methods Pathol. 2022;102(10):1101–1108. doi:10.1038/s41374-022-00804-9
60. Kennedy JJ, Whiteaker JR, Kennedy LC, et al. Quantification of human epidermal growth factor receptor 2 by immunopeptide enrichment and targeted mass spectrometry in formalin-fixed paraffin-embedded and frozen breast cancer tissues. Clin Chem. 2021;67(7):1008–1018. doi:10.1093/clinchem/hvab047
61. Xu K, Bayani J, Mallon E, et al. Discordance between Immunohistochemistry and Erb-B2 receptor tyrosine kinase 2 mRNA to determine human epidermal growth factor receptor 2 low status for breast cancer. J Mol Diagn JMD. 2022;24(7):775–783. doi:10.1016/j.jmoldx.2022.04.002
62. Hoffman-Censits JH, Lombardo KA, Parimi V, et al. Expression of nectin-4 in bladder urothelial carcinoma morphologic variants, and nonurothelial histotypes. Appl Immunohistochem Mol Morphol AIMM. 2021;29(8):619–625. doi:10.1097/PAI.0000000000000938
63. Bardia A, Tolaney SM, Punie K, et al. Biomarker analyses in the phase III ASCENT study of sacituzumab govitecan versus chemotherapy in patients with metastatic triple-negative breast cancer. Ann Oncol off J Eur Soc Med Oncol. 2021;32(9):1148–1156. doi:10.1016/j.annonc.2021.06.002
64. Chu CE, Sjöström M, Egusa EA, et al. Heterogeneity in NECTIN4 expression across molecular subtypes of urothelial cancer mediates sensitivity to enfortumab vedotin. Clin Cancer Res off J Am Assoc Cancer Res. 2021;27(18):5123–5130. doi:10.1158/1078-0432.CCR-20-4175
65. Hunter FW, Barker HR, Lipert B, et al. Mechanisms of resistance to trastuzumab emtansine (T-DM1) in HER2-positive breast cancer. Br J Cancer. 2020;122(5):603–612. doi:10.1038/s41416-019-0635-y
66. Branco FP, Machado D, Silva FF, et al. Loss of HER2 and disease prognosis after neoadjuvant treatment of HER2+ breast cancer. Am J Transl Res. 2019;11(9):6110–6116.
67. Li G, Guo J, Shen BQ, et al. Mechanisms of acquired resistance to trastuzumab emtansine in breast cancer cells. Mol Cancer Ther. 2018;17(7):1441–1453. doi:10.1158/1535-7163.MCT-17-0296
68. Sung M, Tan X, Lu B, et al. Caveolae-mediated endocytosis as a novel mechanism of resistance to trastuzumab emtansine (T-DM1). Mol Cancer Ther. 2018;17(1):243–253. doi:10.1158/1535-7163.MCT-17-0403
69. Loibl S, Majewski I, Guarneri V, et al. PIK3CA mutations are associated with reduced pathological complete response rates in primary HER2-positive breast cancer: pooled analysis of 967 patients from five prospective trials investigating lapatinib and trastuzumab. Ann Oncol off J Eur Soc Med Oncol. 2016;27(8):1519–1525. doi:10.1093/annonc/mdw197
70. Baselga J, Lewis Phillips GD, Verma S, et al. Relationship between Tumor Biomarkers and Efficacy in EMILIA, a phase iii study of trastuzumab emtansine in HER2-positive metastatic breast cancer. Clin Cancer Res off J Am Assoc Cancer Res. 2016;22(15):3755–3763. doi:10.1158/1078-0432.CCR-15-2499
71. Kim SB, Wildiers H, Krop IE, et al. Relationship between tumor biomarkers and efficacy in TH3RESA, a phase III study of trastuzumab emtansine (T-DM1) vs. treatment of physician’s choice in previously treated HER2-positive advanced breast cancer. Int, J, Cancer. 2016;139(10):2336–2342. doi:10.1002/ijc.30276
72. Denkert C, Lambertini C, Fasching PA, et al. Biomarker Data from the Phase III KATHERINE Study of Adjuvant T-DM1 versus trastuzumab for residual invasive disease after neoadjuvant therapy for HER2-positive breast cancer. Clin Cancer Res off J Am Assoc Cancer Res. 2023;29(8):1569–1581. doi:10.1158/1078-0432.CCR-22-1989
73. Mosele MF, Lusque A, Dieras VC, et al. LBA72 Unraveling the mechanism of action and resistance to trastuzumab deruxtecan (T-DXd): biomarker analyses from patients from DAISY trial. Ann Oncol. 2022;33:1.
74. Coates JT, Sun S, Leshchiner I, et al. Parallel genomic alterations of antigen and payload targets mediate polyclonal acquired clinical resistance to sacituzumab govitecan in triple-negative breast cancer. Cancer Discov. 2021;11(10):2436–2445. doi:10.1158/2159-8290.CD-21-0702
75. Beishenaliev A, Loke YL, Goh SJ, et al. Bispecific antibodies for targeted delivery of anti-cancer therapeutic agents: a review. J Control Release off J Control Release Soc. 2023;359:268–286. doi:10.1016/j.jconrel.2023.05.032
76. Desnoyers LR, Vasiljeva O, Richardson JH, et al. Tumor-specific activation of an EGFR-targeting probody enhances therapeutic index. Sci Transl Med. 2013;5(207):207ra144. doi:10.1126/scitranslmed.3006682
77. Fang S, Brems BM, Olawode EO, Miller JT, Brooks TA, Tumey LN. Design and characterization of immune-stimulating imidazo[4,5-c]quinoline antibody-drug conjugates. Mol Pharm. 2022;19(9):3228–3241. doi:10.1021/acs.molpharmaceut.2c00392
78. Pillow TH, Adhikari P, Blake RA, et al. Antibody conjugation of a chimeric BET degrader enables in vivo activity. ChemMedChem. 2020;15(1):17–25. doi:10.1002/cmdc.201900497
79. Tang C, Zeng Y, Zhang J, et al. One-Pot assembly of dual-site-specific antibody-drug conjugates via glycan remodeling and affinity-directed traceless conjugation. Bioconjug Chem. 2023. doi:10.1021/acs.bioconjchem.3c00048
80. Xu Z, Guo D, Jiang Z, et al. Novel HER2-targeting antibody-drug conjugates of trastuzumab beyond T-DM1 in breast cancer: trastuzumab deruxtecan(DS-8201a) and (Vic-)Trastuzumab Duocarmazine (SYD985). Eur J Med Chem. 2019;183:111682. doi:10.1016/j.ejmech.2019.111682
81. QuantumLeap Healthcare Collaborative. ISPY-P1.01: evaluating the safety of weekly paclitaxel with trastuzumab duocarmazine (SYD985) in patients with metastatic cancer: a Phase I/Ib Trial. clinicaltrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT04602117.
82. Byondis BV. A multi-centre, open-label, randomized clinical trial comparing the efficacy and safety of the antibody-drug conjugate SYD985 to physician’s choice in patients with HER2-positive unresectable locally advanced or metastatic breast cancer. clinicaltrials.gov; 2022. Available from: https://clinicaltrials.gov/ct2/show/NCT03262935.
83. Jhaveri K, Han H, Dotan E, et al. 460MO Preliminary results from a phase I study using the bispecific, human epidermal growth factor 2 (HER2)-targeting antibody-drug conjugate (ADC) zanidatamab zovodotin (ZW49) in solid cancers. Ann Oncol. 2022;33:S749–50. doi:10.1016/j.annonc.2022.07.589
84. Wang J, Liu Y, Zhang Q, et al. RC48-ADC, a HER2-targeting antibody-drug conjugate, in patients with HER2-positive and HER2-low expressing advanced or metastatic breast cancer: a pooled analysis of two studies. J Clin Oncol. 2021;39(15_suppl):1.
85. Hu X, Zhang J, Liu R, et al. Phase I Study of A166, a novel antibody-drug conjugate in advanced HER2-expressing solid tumors. In Review; 2022. Available from: https://www.researchsquare.com/article/rs-2179560/v1.
86. Hamilton EP, Barve MA, Bardia A, et al. Phase 1 dose escalation of XMT-1522, a novel HER2-targeting antibody-drug conjugate (ADC), in patients (pts) with HER2-expressing breast, lung and gastric tumors. J Clin Oncol. 2018;36(15_suppl):2546. doi:10.1200/JCO.2018.36.15_suppl.2546
87. SCRI Development Innovations, LLC. A Phase II Study of U3-1402 in patients with metastatic breast cancer. clinicaltrials.gov; 2022. Available from: https://clinicaltrials.gov/ct2/show/NCT04699630.
88. Daiichi Sankyo Co., Ltd. Phase 1, two-part, multicenter, open-label, multiple dose, first-in-human study of DS-1062a in subjects with advanced solid Tumors (TROPION-PanTumor01). clinicaltrials.gov; 2022. Available from: https://clinicaltrials.gov/ct2/show/NCT03401385.
89. AstraZeneca. A Phase IB/II, 2-stage, Open-label, multicenter study to determine the efficacy and safety of durvalumab (MEDI4736) + Paclitaxel and Durvalumab (MEDI4736) in combination with novel oncology therapies with or without paclitaxel for first-line metastatic triple negative breast cancer. clinicaltrials.gov; 2023. Available from: https://clinicaltrials.gov/ct2/show/NCT03742102.
90. AstraZeneca. A phase 3, open-label, randomised study of datopotamab deruxtecan (Dato-DXd) versus investigator’s choice of chemotherapy in patients who are not candidates for PD-1/PD-L1 inhibitor therapy in first-line locally recurrent inoperable or metastatic triple-negative breast cancer (TROPION Breast02). clinicaltrials.gov; 2022. Available from: https://clinicaltrials.gov/ct2/show/NCT05374512.
91. Sichuan Kelun Pharmaceutical Research Institute Co., Ltd. A randomized, controlled, open-label, multi-center phase iii clinical trial of skb264 for injection versus investigator selected regimens in patients with unresectable locally advanced, recurrent or metastatic triple-negative breast cancer who have failed second-line or above prior standard of care. clinicaltrials.gov; 2022. Available from: https://clinicaltrials.gov/ct2/show/NCT05347134.
92. Cortés J, Diab S, Basho RK, et al. 357TiP SGNLVA-002: single arm, open-label, phase Ib/II study of ladiratuzumab vedotin (LV) in combination with pembrolizumab for first-line treatment of triple-negative breast cancer. Ann Oncol. 2020;31:S393. doi:10.1016/j.annonc.2020.08.459
93. Modi S, Pusztai L, Forero A, et al. Abstract PD3-14: phase 1 study of the antibody-drug conjugate SGN-LIV1A in patients with heavily pretreated triple-negative metastatic breast cancer. Cancer Res. 2018;78(4_Supplement):PD3–14. doi:10.1158/1538-7445.SABCS17-PD3-14
94. Seagen Inc. Single arm, open label phase 1b/2 Study of SGN-LIV1A in combination with pembrolizumab for first-line treatment of patients with unresectable locally-advanced or metastatic triple-negative breast cancer. clinicaltrials.gov; 2022. Available from: https://clinicaltrials.gov/ct2/show/NCT03310957.
95. PharmD BP. FDA to Review [Vic-]Trastuzumab Duocarmazine for HER2-positive metastatic breast cancer. MPR. 2022. Available from: https://www.empr.com/home/news/drugs-in-the-pipeline/fda-to-review-vic-trastuzumab-duocarmazine-for-her2-positive-metastatic-breast-cancer/.
96. QuantumLeap Healthcare Collaborative. ISPY-P1.01: evaluating the safety of weekly paclitaxel with trastuzumab duocarmazine (syd985) in patients with metastatic cancer: a phase I/Ib trial. clinicaltrials.gov; 2021. Available from: https://clinicaltrials.gov/ct2/show/NCT04602117.
97. Shenderov E, Mallesara GHG, Wysocki PJ, et al. 620P MGC018, an anti-B7-H3 antibody-drug conjugate (ADC), in patients with advanced solid tumors: preliminary results of phase I cohort expansion. Ann Oncol. 2021;32:S657–9. doi:10.1016/j.annonc.2021.08.1133
98. BioAtla, Inc. A Phase 1/2 Safety and Efficacy Dose Escalation / Dose Expansion Study of a CAB-ROR2-ADC, alone and in combination with a pd-1 inhibitor, in patients with advanced solid tumors (Ph1) and Melanoma and NSCLC Patients (Ph2). clinicaltrials.gov; 2022. Available from: https://clinicaltrials.gov/ct2/show/NCT03504488.
99. Sanofi. Open-label, multi-cohort, phase 2 trial, evaluating the efficacy and safety of tusamitamab ravtansine (SAR408701) monotherapy and in combination in patients with CEACAM5-positive advanced solid tumors. clinicaltrials.gov; 2022. Available from: https://clinicaltrials.gov/ct2/show/NCT04659603.
100. Eisai Inc. A multicenter, open-label phase 1/2 trial evaluating the safety, tolerability, and efficacy of MORAb-202, a Folate Receptor Alpha (FRα)-Targeting Antibody-drug Conjugate (ADC) in subjects with selected tumor types. clinicaltrials.gov; 2022. Available from: https://clinicaltrials.gov/ct2/show/NCT04300556.
101. Guo P, Huang J, Zhu B, et al. A rationally designed ICAM1 antibody drug conjugate eradicates late-stage and refractory triple-negative breast tumors in vivo. Sci Adv. 2023;9(18):eabq7866. doi:10.1126/sciadv.abq7866
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.