")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Analyzing Korean Public Health Centers’ Infectious Disease Disaster Response Experiences with a Focus on Business Continuity
Authors Yun EK, Han JW , Kim JO, Jung S , Cha J, Yoo K, Min S, Yang B
Received 6 November 2023
Accepted for publication 23 March 2024
Published 4 April 2024 Volume 2024:17 Pages 789—801
DOI https://doi.org/10.2147/RMHP.S448382
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Eun Kyoung Yun, Jeong-Won Han, Jung Ok Kim, Sungmo Jung, Jeongeun Cha, Keunhee Yoo, Soyoon Min, Boeun Yang
College of nursing science, Kyung Hee University, Seoul, Republic of Korea
Correspondence: Jeong-Won Han, College of Nursing Science, Kyung Hee University, 26, Kyunghee-daero, Dongdaemun-gu, Seoul, 02447, Republic of Korea, Tel/Fax +82-2-961-2123, Email [email protected]
Objective: This study aims to provide basic data for establishing strategies to maintain the core functions of health centers, and enable an effective response to emergency tasks in the event of future infectious disease disasters.
Methods: The participants were 41 workers from two public health centers in Seoul. They all had prior experience in responding to the early and middle stages of the COVID-19 pandemic. Data were collected through Focus Group Discussions, and then analyzed using the deductive method of content analysis.
Results: The participants’ experiences during the infectious disease disaster crisis were examined through ten categories: governance and coordination, information management, human resources, essential medical supplies and equipment, infrastructure, administration, finance and logistics, community engagement and risk communication, delivery of essential services, security, and additional considerations for vulnerable populations. The analysis of the results made it apparent that new systems and policies were imperative for responding appropriately to the concerns and experiences of the public healthcare center staff, and for improving the response to future epidemics.
Conclusion: We found that to prepare for infectious disaster situations in the future, it is necessary for health centers to establish a mid- to long-term business continuity plan to ensure the continuation and stability of their operations. Additionally, it was found that health professionals in public health centers also believe in the necessity of education and training programs on disaster preparedness, based on Business Continuity Planning proposed by the World Health Organization. They deem these essential to sustain routine tasks for the management of the health of local community residents during outbreaks of novel infectious diseases in the future.
Keywords: public health, disaster crisis, qualitative research
Introduction
A public health center is a public institution established in accordance with local health laws; it supports the health, disease management, and hygiene practices of the local residents of a particular area.1 While conducting screening tests, epidemiological investigations, self-quarantine management, and operating vaccination, and residential treatment centers in response to COVID-19, public health centers in Korea had to introduce new tasks.2 Following the enactment of the National Health Promotion Act in 1995, Korean public health centers switched their focus to health promotion projects.3,4 These functional and structural changes significantly enhanced Korean health centers’ readiness and agility to provide healthcare for patients with chronic diseases and the vulnerable, while the readiness to respond to new infectious diseases such as COVID-19 remained relatively low.5 There was social concern about suspending routine work at public health centers.3 Consequently, public health centers and medical institutions in Korean communities were instructed to incorporate Business Continuity Planning (BCP) to restore their routine work.6 However, the disruption to business continuity in the wake of the infectious disease disaster/COVID-19 made it difficult for public health centers to move to the stage of recovery, while simultaneously maintaining routine work.4 Generally, the structure of routine work at public health centers is highly dependent on progress on the tasks executed by projects and teams. Nevertheless, the response to infectious diseases requires a structure with high interdependence and mutual influence between departments and tasks; this makes the continuity of work related to infectious disease response a prerequisite for the recovery of routine work by public health centers.
The outbreak of Severe Acute Respiratory Syndrome, Influenza A virus subtype H1N1, and Middle East Respiratory Syndrome globally resulted in the suspension of core operations of healthcare institutions amid tremendous damage to organizations or countries.6 The new infectious disease pandemic demonstrated that the management of patients with chronic diseases, or treatment plans for quarantined people were not clearly planned. Thus, the World Health Organization (WHO) announced the BCP guidelines to help healthcare institutions respond quickly to emergencies such as infectious diseases, and efficiently return to their core business.7 BCP refers to strategic mitigation, response, and recovery planning to identify potential threats to the organization and their impact on business operations in order to resume core operations at a pre-agreed and acceptable level, and provide an effective organizational resiliency system.8 The International Organization for Standardization/Technical Committee 223 Societal Security has been promoting activities to establish international disaster management standards since 2006. It has emphasized the need for standardization of disaster management with great interest in disaster management system standards.9
The WHO has predicted that even if the virus is eradicated, there are chances that other infectious diseases may occur periodically.10 Therefore, to effectively cope with future crises, medical and public health centers responsible for the health of chronically-ill patients and vulnerable populations in communities require strategies to maintain their core functions even during disasters caused by infectious diseases, and also respond effectively to emergency operations. As a first step in establishing such a strategy, it is essential to systematically explore and understand the experiences of staff in public health centers during general and emergency work in response to infections, and gauge the difficulties they face in the process of responding to the current COVID-19 crisis in terms of business continuity. Therefore, this study aims to analyze the experience of staff while responding to the infectious disease crisis at two public health centers in Seoul, including the one in charge of the first confirmed COVID-19 case in Korea, and provide some basic evidence for establishing policies for BCP to enable responses to possible infectious disease disasters in the future.
Methods
Research Design
This study used deductive content analysis to explore the experiences of public health center health professionals in the early and middle stages of responding to infectious disease crises in terms of work continuity during the new infectious disease pandemic. The public health center presented in this study is public institutions that supports the health, disease management, and hygiene practices of local residents. It is an institution located in an area with a population of over 300,000 community residents.
Research Participants
Focus group discussions were conducted with fifteen nursing officers, nine administrative officers, eight public health officers, three medical technicians, four medical officers, and two pharmaceutical officers who were responding to COVID-19 from two public health centers in Seoul. One was in charge of the first confirmed case of COVID-19 in Korea, while the other had the largest floating population in Korea. Additionally, to select research participants with sufficient experience in responding to infectious disease crises at public health centers, a preliminary meeting was held with the staff of these two public health centers. From among the staff participating in infectious disease response tasks, participants were selected in consideration of their position and level, as well as the tasks related to responding to infectious diseases.
Data Collection
Data were collected through focus group discussions, with 4–5 people per group, considering the position and level of the participants. The discussion commenced with introductions and greetings. The researchers used semi-structured and open-ended questions, and avoided inducing the answers they wanted. To aid the participants’ comprehension, the terms crisis response and business continuity were briefly explained. The main question was, “Tell me about the type of work you performed at the public health center during the COVID-19 pandemic”. The participants were encouraged to talk about the subject as freely as possible, and a list of supplementary questions was also prepared. The supplementary questions were based on the WHO’s proposal of ten main considerations for implementing the BCP:11 governance and coordination, information management, human resources, essential supplies and equipment, facilities, finances, communication and cooperation, provision of essential services, security assurance, and vulnerable populations, and its sub-areas. At the end of the discussion participants’ statements were briefly summarized and evaluated to see if they corresponded with their experiences. The discussions ended when the participants declared that they had nothing more to say. The data were collected in line with quarantine regulations, and the discussions were recorded. The researchers took notes of the main content during and after the discussions. The data were collected in a separate space with the cooperation of the public health center from August 16–30, 2022, and the discussions lasted about two hours. During the discussions, the participants were asked whether they experienced any difficulties or burdens. Afterward, they were given the opportunity to talk about anything else they wanted to express. The data collected comprised transcripts of the recordings made during the discussions and debriefing notes compiled by the researchers immediately after.
Data Analysis
The collected data were analyzed using the deductive method from the qualitative content analysis of Elo and Kynga.12 This method draws valid and reproducible inferences based on the collected data, and can be used to verify them in a new context based on previous theories. This study employed this method to verify the problems of securing business continuity during the response to the actual infectious disease crisis in terms of the BCP (as presented by the WHO; Table 1), targeting the staff of public health centers in Korea. In the first phase, the researchers read the data repeatedly without any conceptual framework or general insight, listened to the recorded data, and thus closely aligned to the data. Subsequently, the meanings highlighted by the data were identified, and appropriate phrases and sentences were derived (line-by-line analysis). In the second step, the data corresponding to the area under study were classified and categorized (sub-categories). In the third step, the contents were stated for each area, concepts or phrases that could reveal the context of the participants were defined (generic category), and finally, the main category was derived and named.
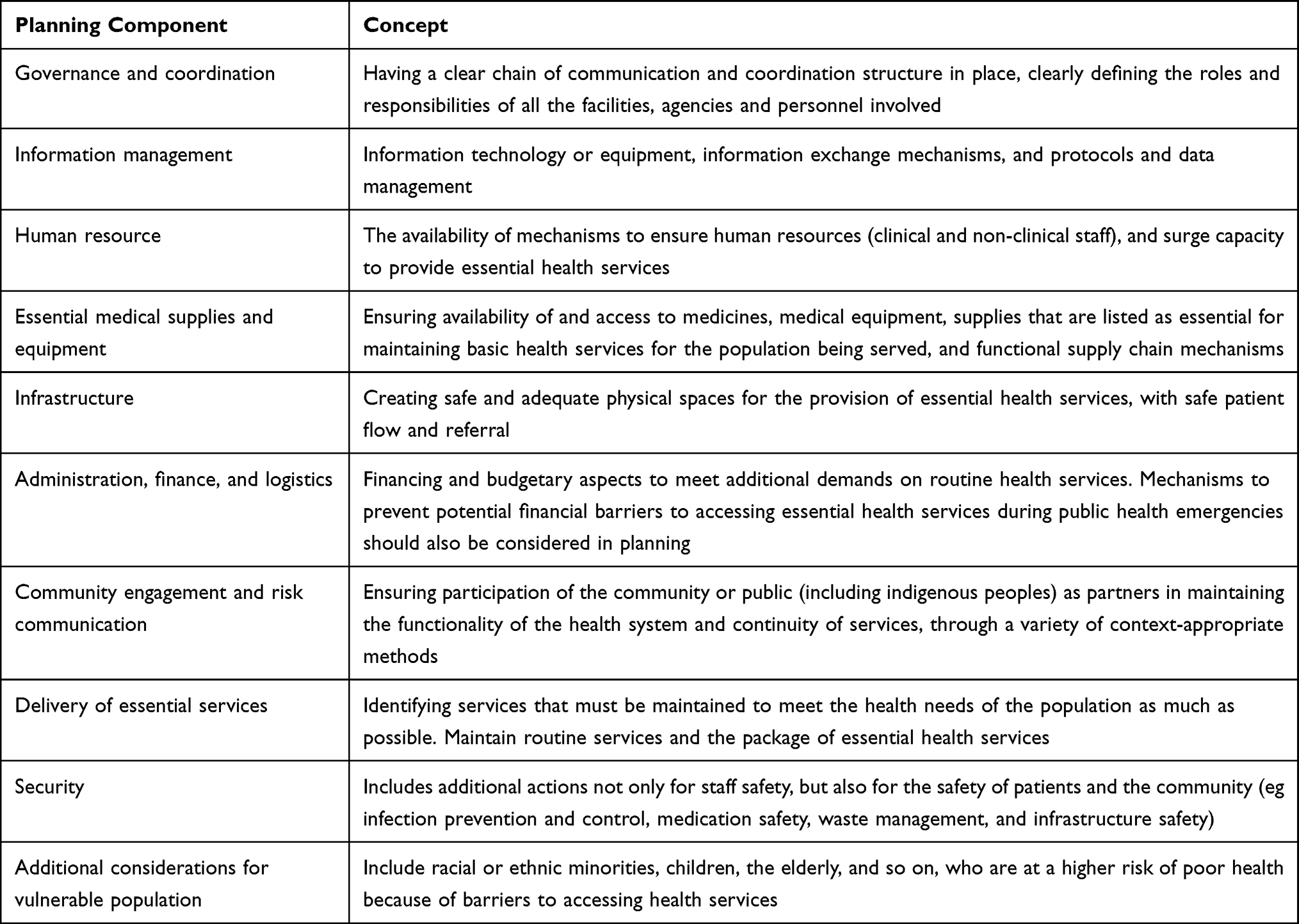 |
Table 1 Identifying Key Actions to Be Taken in the Service Continuity Planning Process |
Research Reliability
This study systematically analyzed and evaluated qualitative research using the three-step process of consolidated criteria for reporting qualitative research presented by the Equator network library.13 Additionally, the researchers conducting this study completed classes and training on qualitative nursing, obtained experience in participating and conducting various qualitative nursing seminars, and responding to COVID-19, or conducting related research. The researchers actively listened to participants’ stories while collecting data without directing their thoughts. They also shared and discussed their memos during data collection and analysis so that the field experience and prior knowledge of the researchers did not prejudice the entire research process.
Results
Participants’ Characteristics
The participants in this study included 41 staff members from two public health centers in Seoul that responded to the COVID-19 infectious disease crisis. Among them, 29 were female and 12 male. The average age was 49.78±7.82 years. The positions were nursing (n=15), administrative (n=9), public health (n=8), medical (n=4), medical technology (n=3), and pharmaceutical (n=2) (Table 2). The roles assigned to each participant in the BCP operation scheme are also listed in Table 2. The role structure for ensuring the continuity of health center operations is based on the participants’ grade level, so that directors are categorized as the strategic level, managers as the tactical level, and team leaders and below as the operational level.
 |
Table 2 Characteristics of All Participants |
Public Health Centers’ Response to Infectious Disease Crises in Terms of Business Continuity
According to this study, the experience of responding to new infectious diseases at public health centers is as follows (Table 3):
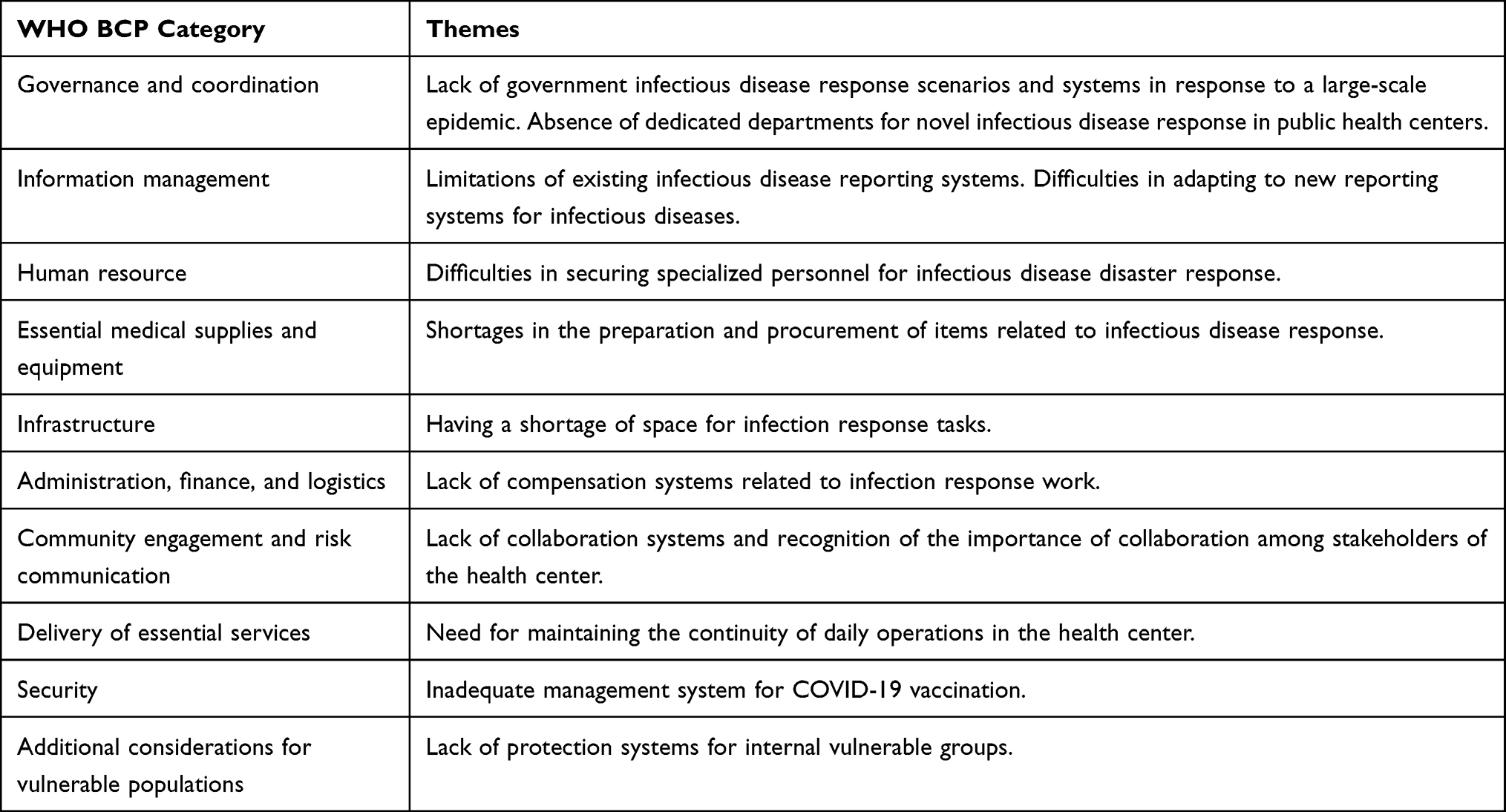 |
Table 3 Category and Themes of Public Health Centers’ COVID-19 Response Focused on Business Continuity |
Governance and Coordination
Insufficient Government Response Scenarios and Systems for Large-Scale Epidemics
The participants in this study were employees of public health centers. Given that government guidelines and laws manage the system and operation of public health centers in Korea, the government’s response scenarios and systems were insufficient for responding appropriately to the large scale epidemic of infectious diseases in the country. The staff at public health centers had difficulty understanding their roles and responsibilities during the pandemic, and thus experienced difficulties in performing and maintaining their duties. Additionally, during the pandemic, it was “all hands on deck” so even administrative staff at public health centers were involved in the response to the infectious disease; therefore, it appears that there is a great need for clear guidelines from the government.
(At the early stages of a large-scale spread of a novel infectious disease) we need a (government) manual. We are doing it this way now, and then when the ward office sends a few more people, we accommodate it. There are 100,000 confirmed cases now, but there were 200,000 cases then. Therefore, we needed to know how many more people would be joining to support us. This information should be included in a manual. If only there was a manual with information on how the workforce could be supplemented or replaced when there is such a meteoric rise in the number of cases. Then, action could be taken immediately, and it would be easy to report to personnel management. (Participant 17)
Absence of a Department Dedicated to Responding to New Infectious Diseases in Public Health Centers
This study found that the participants experienced a rise in work duplication and burden, and a drop in work efficiency, due to the absence of a dedicated department for responding to COVID-19. Before COVID-19, the department of new infectious diseases was operated concurrently with other departments, instead of having a separate one. This was also confirmed by the participants of this study – as below.
(Responding task).Since the departments are diversified, a civil petitioner for example, would need a certificate of quarantine release. Then, it would be important to ask whether they quarantined at a hospital or stayed at home. If so, the issuing department would be different. Furthermore, if the quarantine was done in 2021, the person had to go to a different department, and if it was in 2022, we did it for them.Considering that the departments are diversified, there are two tasks here and two there. I think this is a bit of a problem. (Participant 26)
Information Management
Limitations of the Existing Infectious Disease Reporting System
The participants reported various delays in responding to the new infectious disease with the existing computerized infectious diseases reporting system. Furthermore, as government policies were constantly changing, only limited reporting using the existing computerized system was possible. Therefore, in the early stages of responding to infectious diseases, most involved manual reporting. This additional work led to delays in completing response tasks and taking charge of daily work. There were limitations in responding to the epidemic of infectious diseases and difficulties were compounded by the combination of computerized systems and manual tasks.
Initially, during an epidemiological investigation, I opened the files one by one, called each one individually, and investigated the tracking for almost ten days, including three days prior. I also typed all of them. Then I had to call the people who were in contact with that person and enter all the information into an Excel file; because according to the CDC system, details should be entered individually or uploaded in an Excel file. It took almost 1–2 hours, or sometimes up to 4 hours to investigate one person.If systemized, entries could be made by typing only once. The disease management system was not like that either. The district wanted to help, but their system appeared congested and difficult to use. (Participant 25)
Difficulties in Adapting to the New Infectious Disease Reporting System
In addition to their routine work, the participants faced an additional burden of learning and adapting to the government’s new computerized reporting system for new infectious diseases, without any training or supervision. Consequently, the processing of work was delayed.
There was a new system, a hub system, because of COVID-19. At first, many staff members were dissatisfied.It is not just one system; there was a COVID-19 information management system, along with the new system, so we suffered the inconvenience of using several systems. Additionally, there is information that cannot be found at medical institutions but is visible at public health centers. There were some difficulties because of the asymmetry of information. There were too many confirmed cases, which made it difficult to cope. (Participant 32)
Human Resources
Difficulty in Securing Personnel Dedicated to Infectious Diseases
The participants experienced an explosive increase in infectious disease response work owing to the disease’s large scale and rapid spread. Most of the public health centers’ staff stopped their daily work and participated in response work. However, progress in work, education, and training was hindered as there were many staff members who lacked professional knowledge or skills related to the new disease. Owing to the nationwide spread of the disease, securing a professional workforce and maintaining the response and daily work of public health centers was difficult. Moreover, securing dedicated personnel, notably epidemiological investigators, was challenging during a large-scale infectious disease situation. Additionally, even when personnel were secured, time was required to train them to perform the duties of epidemiological investigators. Furthermore, there was a delay in conferring legal authority for the tasks to substitute personnel. These factors contributed to the inability to respond to the tasks effectively.
Simply having contracted personnel did not solve the problem. All the additional people had to be recruited, managed, and paid; there was too much extra work. Since we were doing that for dozens of people.we constantly had to hire them whenever people quit, citing hardship, and train them, which consumed too much energy. (Participant 4)
The solution to the difficulty in recruiting personnel was to maximize the utilization of existing staff. There was no choice but to extend working hours by offering higher salaries. Although the number of specialized personnel was limited, we made the most of the resident workforce. Given the shortage and limited pool of manpower, we had to find a way to resolve it, no matter what. When there was a shortage of epidemiological investigators, the only option was to expand operations to other areas. We implemented this approach in any region as necessary. (Participant 5)
When an epidemiological investigator was unable to come to work due to circumstances such as infection, they worked from home or a residential care center using a laptop. (participant 15)
Essential Supplies and Equipment
Lack of Preparation and Difficulty in Securing Items Related to Infection Response
The participants required equipment for personal protection, diagnostic tests, and patient transfers due to the extra protocols for work on infectious diseases. However, the infection spread suddenly and on a large scale creating difficulties for the staff in anticipating and securing related items, which led to delays.
In the beginning of 2020, we had no financial support or dedicated budget, and since it was the first time we were experiencing it, we did not know how much money and how much medicine we would need, and whether we required quarantine items, gowns, or masks. We had absolutely no idea whether the basics or just masks were required. However, after a while, I began to predict better. From then on, I stocked items and kept buying what I lacked. (Participant 5)
Facility
Insufficient Space for Infection Response Work
The participants experienced difficulties in carrying out their work due to space constraints, and in operating tasks according to infectious disease policies, such as screening clinics and residential treatment centers. They had to think creatively to resolve and work around the space limitations. As they worked, they found that the time needed to participate in infectious disease response work overshadowed, and increased more than their daily work.
I think the screening clinic needs to be in a separate standardized place. To handle all the work there, I wish there was a separate space in a three-story building that could handle all infection systems with standardization. Otherwise, it is difficult to deal with business quickly, especially on days when the number of confirmed cases increases. (Participant 23)
(To operate the residential treatment centers) we got a new building: the residential treatment center, that was a former hotel. I heard that the hotel was built in 1919. After spraying disinfectants in places like elevators, they asked for money to restore it from damage. So, it was difficult to write an agreement to negotiate like this. (Participant 27)
Finance
Insufficient Compensation System Related to Infection Response Work
The participants found that there were differences in the degree of financial independence of public health centers by region. Thus, they faced difficulties in workforce operation and work maintenance due to conflicts caused by differences in securing infectious disease response personnel and differential compensation for infectious disease response personnel by position and level.
As far as I know, when it comes to securing workforce or things like that, XX district has a high degree of financial independence to manage this it on its own.The money given by the city is the same for all 25 districts. Districts falling short of money must manage with the money given to them; so if you are given money for ten people, you cannot hire more. But XX district has a lot of money. The amount of work is different, but when the city gives money, it is mostly not based on need, but probably based on averages and estimates. (Participant 15)
There were a lot of complaints because of the difference in performance pay, and in fact, there was widespread controversy on our internet bulletin board. It was about paying differentially only to employees in a specific position, level, and work. Everybody suffered from COVID-19; both the ward office and public health centers. The ward office was not convinced either. (participant 30)
In the case of nurses and public health workers, wages greatly differed between contract workers and those who were regular employees. The people inside the organization had to work all night, but they received 2 million won a month, while contract workers were paid 6 million won per month. There was no choice but to leave. Usually, when there is a difference of three times the salary, those who come from outside are paid more if they work three days than regular workers who work 5 or 6 days a week. (Participant 38)
Communication and Cooperation
Lack of Cooperation Between Public Health Centers and Their Stakeholders
The participants in this study argued that in the context of an infectious disease, public health centers and their stakeholders should cooperate in responding to disasters. Cooperation is required to ensure the efficient use of limited resources, and secure a workforce. Smooth communication with community residents and higher-level government agencies is required to reduce citizen complaints.
The public always came first, and the public part almost became a victim to work, and when it became stable, it went over to the private sector. Rather than that, I think that synergistic effects and impacts should be achieved when the private and public sectors respond simultaneously. (Participant 34)
Provision of Essential Services
Recognizing the Need to Maintain Daily Business Continuity of Public Health Centers
The participants noted that their routine work, such as support for fertility, premature baby medical expenses, and maternal and child health projects was disrupted due to the necessity to respond to the infectious disease. Regarding this, the participants recognized that their daily work, such as services directly related to public health, could not be stopped even while the COVID-19 crisis was ongoing. They said they experienced different situations where the public health center’s projects were reduced, suspended, or maintained with the spread of the COVID-19 infection.
Support for medical expenses should not be stopped. Support for infertility medical expenses or support for medical expenses for premature babies and pregnant women who need to take iron and folic acid supplements every month should not be discontinued. Therefore, I had no choice but to continue supporting medical expenses when people applied for it because it could only be done at the public health center. (Participant 8)
First, in our case, we privatized the low birth rate program and then the dementia support and mental health projects, which have now become a more serious problem during COVID-19. Thus, we had to do the best possible because we could not run one-on-one programs or group programs. However, we made videos so people could participate together, and telephone consultations and other things were given. (Participant 34)
Security Assurance
Absence of a COVID-19 Vaccination Management System
It was found that the participants experienced delays in their routine work or were overburdened when the management system was being changed to include better safety, especially while the side effects related to COVID-19 vaccinations were unclear.
In the case of vaccinations, our nurses and doctors made pre-diagnoses and also recruited doctors and nurses when we ran the vaccination center within the system.However, when adverse reactions arose, the doctors and nurses panicked; there were many situations like this. (Participant 8)
Vulnerable Populations
Insufficient Protection System for Vulnerable Staff
The participants reported that protection, and safety measures and systems for vulnerable staff in their organizations were insufficient due to an increase in the number of confirmed cases, even though there were pregnant women and vulnerable staff with mental and psychological problems among the infectious disease response personnel.
We have quite a few pregnant staff, and they went on maternity and sick leave for a while in the middle. There were probably some people who took leave of absence from the epidemiological team due to mental problems, and then there were some who took leave of absence because of work difficulties. Many pregnant people came. After they were hired and said they that they were present for only four weeks, how could I assign them to the night shift (Participant 12)?
Usually, it is depression or parental leave, but sometimes parental leave was also because of depression. Once there is leave of absence, the position must be filled somehow, so staff from departments without heavy workloads were transferred to the vacant positions. Consequently, the staff in charge of COVID-19 and others at the public health center experienced a burnout. This burnout triggered depression. (Participant 30)
Discussion
In the above section, we discussed the ten main categories of considerations to be borne in mind when implementing the BCP proposed by the WHO.11 In this section, we discuss the implications. First, this study found that the participants experienced difficulties in governance and coordination due to the lack of government response scenarios and systems, and the absence of a dedicated department to respond to new infectious diseases in public health centers. In Korea, the organization that is responsible for responding to infectious disease-related crises is the Centers for Disease Control and Prevention, similar to the CDC in the United States. However, since the Minister of Health and Welfare, and mayors and provincial governors have the legal authority and responsibility for infectious disease management, it is a structure that inevitably delays decision-making for establishing an appropriate response system.14 Particularly, given that the initial response is crucial to prevent a large scale and prolonged outbreak in communities, predictions as the case of COVID-19, seem to have been delayed. Accordingly, public health centers had to passively wait for orders from the Centers for Disease Control and Prevention, Ministry of Health and Welfare, and provincial governors, causing a case overload and tardiness in responding to the increasing number of confirmed cases. The passive stance of the public health center can be attributed to the absence of a department dedicated to responding to new infectious diseases within the public health center. The absence of a department in charge of infectious disease response engendered confusion about the roles and responsibilities of those responding to infectious diseases, leading to a situation in which the public health center could not maintain or perform their core tasks efficiently; furthermore, there was no room to maintain the continuity of response tasks in case of emergencies. Therefore, it is necessary to establish governance for rapid response at the regional level, such as establishing a cooperative system between major community organizations and the government, and encouraging experts and residents to participate through various committees.15 For public health centers to fulfill their functions by maintaining continuous emergency work in the event of an infectious disaster, it is necessary to reorganize the government’s organizational structure for responding to infectious disease-related crises. A system to enable public health centers to strengthen their capacity to deal with infectious disasters must be created.
Second, in terms of information management, new tasks related to the infectious disease response appeared due to changes in the reporting system. The participants experienced difficulties with essential supplies and equipment due to a lack of preparation, the securing of supplies related to infection response, and problems related to facilities such as a lack of storage space. These problems are not specific to Korea, but due to the large scale spread of infectious diseases around the world; they had a psychological burden on workers’ safety and work continuity in responding to infectious diseases. The OECD emphasized the need to increase the supply of equipment required to safely diagnose and treat patients, and secure personal protective equipment (masks, face shields, and hand sanitizers) and ventilators necessary for coping with infectious diseases, along with close monitoring to ensure that essential medicines are stably procured.16 Accordingly, considering potential future infectious disease disasters, public health centers should make appropriate plans for resources and budget security, such as information systems, protective equipment, and facilities related to infectious disease response tasks, and prepare for cases where public health center budgets are insufficient. It is also essential to plan for community resource utilization and resource sharing and distribution in case of such budget insufficiency. Screening clinics in Korea require equipment installation considering accessibility and standard design blueprints; but during COVID-19, public health center staff, who also included non-professionals, were required to manage all these aspects somehow.10 Additionally, considering it was difficult for staff to sometimes even organize a space to maintain their work in the event of quarantine, planning and monitoring of space and resources should be conducted periodically by experts, even in normal times, to prepare for future infectious disasters. Moreover, it is challenging to learn and implement a new infectious disease reporting system at the point when a novel infectious disease is spreading on a large scale. Therefore, there is need to consider establishing a system, such as Excel, that allows on-site personnel to handle infectious disease tasks easily and quickly.
Third, we found that the participants experienced difficulties due to a shortage of workforce, while responding to COVID-19. Human resources are essential to maintain medical services, and the personnel in charge of infectious disease control must have scientific expertise and experience in related tasks for responding to infectious diseases.17 Considering the uncertainty of the new infectious disease COVID-19, Korea responded to the pandemic by maintaining the keynote of early termination of infectious diseases through the K-quarantine (test/diagnosis [Test]-epidemiological tracking [Trace]-isolation/treatment [Treat], 3T) strategy.18 Consequently, the necessity to respond to infectious diseases increased, and various other issues such as an increase in the number of confirmed cases, severely ill patients, cases imported from abroad, and confirmed cases occurred simultaneously. Many changes in practice guidelines for responding to infectious diseases were made without the scope of early treatment and vaccines. Additionally, the absolute number of epidemiological investigators capable of responding to the COVID-19 infection disaster was limited due to the lack of vitalization of the government’s infection disaster response specialist training program.19 Considering the lack of medical professionals necessary for the operation of screening clinics, the treatment wings of public health centers across the country were closed. Public health doctors, Korean medicine doctors, and dentists were required to perform the role of epidemiological investigators owing to a lack of epidemiological investigation personnel.4 Thus, non-infectious disease specialists at public health centers participated in response work, experiencing difficulties in business continuity. It was found that the human resources problem went beyond the lack of personnel to respond to infectious diseases, leading to conflicts triggered by differential compensation for infectious disease response personnel by job category and position, and resulting in difficulties in workforce management and job maintenance.
Moreover, protection, safety measures, and systems for pregnant and vulnerable staff with mental and psychological health problems were also insufficient, adding to difficulties in responding to infectious disasters. The problem of human resources for infectious disaster response is gaining attention in Korea and globally, and various educational and training programs to respond to such crises are being conducted. Specialized education is being conducted to suit the roles of medical and non-medical personnel, and the local community.10 Considering the roles of staff in Korean public health centers according to their positions and levels, it is imperative to consider and establish various systems such as education and training for human resources at public health centers, prepare a compensation system, and introduce safety measures for the vulnerable. Additionally, it will be helpful if there is consideration about how and at what point trained human resources should be deployed in terms of continuity of work, and if a program is created that allows all staff to recognize and quickly respond to the crisis.
Finally, the participants recognized that a cooperative system with stakeholders in the public health center is urgently needed for maintaining the infection disaster response work. The development of new vaccines according to the characteristics of new infectious diseases also requires a safety guarantee system for residents and members. Public health centers’ main function and tasks are to deliver public health services for health promotion, prevention, and management.20 Therefore, as the number of complaints from residents in the community exploded due to restrictions on daily work at public health centers and complaints related to COVID-19, quarantine guidelines, vaccinations, and side effects, the centers increased stakeholders’ cooperation and consideration to handle the work with a limited number of staff. However, while this culture has not been formed normally, the infectious disease disaster has been prolonged, leading to more prominent work delays in the public health center. Additionally, Korea applied policies related to residential treatment centers and home treatment, causing many difficulties in resolving resource issues such as quarantine locations and transportation systems with stakeholders.21 Given that public health center staff were in charge of these tasks, the burden of work was exacerbated. Even though inquiries related to vaccination and management of patients with adverse reactions should have been reviewed in cooperation with medical institutions to ensure the safety of community residents, public health centers’ staff handled these, leading to limitations in problem solving. In the future, it is necessary to include these aspects when preparing infectious disaster responses.
The COVID-19 pandemic posed significant challenges with the escalating number of confirmed cases across all countries. These outcomes underscore that viruses know no borders, and that novel infectious diseases can emerge at any time. The resilience and sustainability of healthcare systems depend on their capacity to anticipate and respond to unexpected surges in medical demand, as witnessed during the unprecedented COVID-19 disaster.22 Strengthening this capacity requires enhancements in governance, service delivery, resources, and finances, all of which contribute to the public nature of these areas.23 Despite the challenges in the initial response to COVID-19, countries with robust recovery resilience swiftly restructured their systems. Particularly in European countries such as the United Kingdom, Germany, Italy, and France, various policies were rapidly implemented to address the shortage of healthcare personnel during the first wave of the COVID-19 pandemic. Italy’s Ministry of Health, for instance, devised strategies like recruiting retired healthcare professionals and deploying graduating students to meet the shortage, allocating a budget of €660 million for the recruitment of approximately 20,000 healthcare professionals.24 France also organized groups to recruit a broad range of healthcare professionals, including doctors, nurses, psychologists, and experts from regional health agencies.25 Germany explored collaborative efforts among doctors, the role of auxiliary personnel, and strategies for training substitute personnel to address the long-term shortage of doctors.26 Preparedness for the initial response and the increase in the public nature of healthcare requires systems that periodically check, verify, and prepare the organizational state through measures such as business continuity plans; rather than being formed within a short timeframe.
Based on the ten main categories to be considered when implementing the BCP proposed by the WHO,11 this study conducted a deductive analysis of public health center workers’ COVID-19 crisis response experiences to verify difficulties in securing the business continuity of public health centers. It provides preliminary evidence to establish strategies to maintain the core functions of public health centers and effectively encourage emergency workers to respond to infectious diseases in the event of a future crisis. However, this study has certain limitations in that despite the BCP being introduced to respond to COVID-19 in health and medical institutions, the understanding of participants on the research topic was relatively low owing to the absence of BCP education and programs targeting staff from healthcare institutions. Therefore, the discussion could not elicit more in-depth answers to the topic. Nevertheless, considering the lack of research on BCP in public health centers, this study is significant in providing preliminary evidence for understanding the difficulties of public health center workers’ BCP and suggesting improvements.
Conclusion
This study aimed to explore the experiences of staff in public health centers during their response to the COVID-19 crisis, particularly in terms of establishing strategies for business continuity. Public health centers are responsible for the health of the community; to help with the outbreak of periodically occurring infectious diseases, maintain core functions, and effectively respond to emergency work even in difficult situations. Based on the results of this study, public health center managers need an overall BCP to prepare for such disasters, and separate BCPs for each situation, in addition to related programs, training, education, and response scenarios and systems. Furthermore, it is imperative to conduct a study on a platform to execute and maintain business continuity in response to an infectious disaster. Preparedness for an initial response requires a system that makes periodic checks on the prevailing status over time, instead of something that is formed in a short timeframe as an emergency response. Particularly, training for infectious disease disaster response is crucial for the education and training of medical professionals, including doctors and nurses. It is essential for public health centers and healthcare institutions to be systematically prepared.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to data protection reasons but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board of Kyung Hee University (KHSIRB-22-380 [RA]). All protocols are carried out in accordance with relevant guidelines and regulations. In accordance with HREC requirements, written informed consent was obtained from all participants. Participants were free to withdraw from the study at any time and confirmed their consent for their data to be used in the study and the participant informed consent included publication of anonymized responses.
Acknowledgments
We would like to thank the participants of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Government-wide R&D Fund project for infectious disease research (GFID), Republic of Korea (grant number : HG22C0051).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Korea Institute for Health and Social Affairs [KIHASA]. COVID-19 screening clinic operation experience and improvement direction. Ministry of Health and Welfare, Korea Institute for Health and Social Affairs; 2020. Available from: https://www.prism.go.kr/homepage/entire/researchDetail.do?researchId=1351000-202100014.
2. Park J. Public health, social policies, and the control tower in South Korea. Coronav Polit. 2021;2021:105–126.
3. Park YJ, Huh IS, Lee JK, et al. Application of testing-tracing-treatment strategy in response to the COVID-19 outbreak in Seoul, Korea. J Korean Med Sci. 2020;35(45):1–9. doi:10.3346/jkms.2020.35.e396
4. Na BJ. How impact the pandemic of COVID-19 to the restructuring of public health centers in the future?. Korean Soc Publ Health Med. 2020;5(1):1–10.
5. Bae SS, Lee SW, Kim JI, Lee SM. New approach to strengthening of local public health system. Korean Medical Association Research Institute for Healthcare Policy; 2010. Available from: http://www.dbpia.co.kr/journal/articleDetail?nodeId=NODE02471086.
6. Kim YM. HIV infection control is pushed back by COVID-19; HIV patients at risk. Korean Doctors weekly; 2020. Available from: http://www.docdocdoc.co.kr/news/articleView.html?idxno=2000406.
7. World Health Organization: WHO guidance for business continuity planning. World Health Organization; 2018. Available from: https://apps.who.int/iris/bitstream/handle/10665/324850/WHO-WHE-CPI-2018.60-eng.pdf.
8. Jo HS, Hwang SH, Sim JH, et al. A study on the introduction of the coop in public institutions. National Emergency Management Agency; 2013. Available from: https://dl.nanet.go.kr/SearchDetailView.do?cn=NONB1201421200#none.
9. Lee YS, Ryu SH, Ko HA, Jeong IS. A study on the standard code systematization of disaster environmental information data for earthquakes, fires and fine dusts. J Korean GEO Environm Soc. 2020;20(12):27–32. doi:10.14481/jkges.2019.20.12.27
10. Kim YJ, Kim DH, Lee SH. COVID-19 public health center response, Voices from the field. Seoul Health Air. 2020;3:1–5.
11. World Health Organization. Health service continuity planning for public health emergencies: a handbook for health facilities. World Health Organization; 2021. Available from: https://www.who.int/publications/i/item/9789240033337.
12. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
13. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
14. Ministry of Health and Welfare. Standard manual for infection disease risk management. Ministry of Health and Welfare; 2014. Available from: https://s3.amazonaws.com/s3.documentcloud.org/documents/2095040/untitled.pdf.
15. Na BJ, Kim DH. Improving capability of local public hospital and health center against newly emerging infectious diseases after middle east respiratory syndrome epidemic in Korea. J Korean Med Assoc. 2015;58(8):700–705. doi:10.5124/jkma.2015.58.8.700
16. OECD. Beyond containment: health systems responses to COVID-19 in the OECD. OECD; 2020. Available from: https://www.oecd.org/coronavirus/policy-responses/beyond-containment-%20health-systems-responses-to-covid-19-in-the-oecd-6ab740c0/.
17. Quigley DD, Dick A, Agarwal M, Jones KM, Mody L, Stone PW. COVID-19 preparedness in nursing homes in the midst of the pandemic. J Am Geriatr Soc. 2020;68(6):1164–1166. doi:10.1111/jgs.16520
18. Korea Disease Control and Prevention Agency. Transition of the quarantine system to suit the characteristics of the Omicron. Korea Policy Briefing; 2022. Available from: https://www.korea.kr/news/visualNewsView.do?newsId=148898745.
19. Yoon PH. Current status and problems of epidemiological investigator in Korea. Governors Association of the Republic of Korea; 2021. Available from: https://www.gaok.or.kr/gaok/bbs/B0000008/view.do?nttId=13221&menuNo=200088.
20. Jang SN. Public health center COVID-19 response status and task discussion meeting. YouTube; 2021. Available from: https://youtu.be/7GJBeElNAhE?t=1553.
21. Ouyang H, Jiang H, Huang J, Liu Z. COVID-19 pandemic brings challenges to the management of stroke—the differences between stroke cases admitted to a tertiary hospital before and during COVID-19 Pandemic in China. Risk Manag Healthc Policy. 2023;16:2893–2905. doi:10.2147/RMHP.S435094
22. Baker MG, Kvalsvig A, Verrall AJ. New Zealand’s COVID-19 elimination strategy. Med J Aust. 2020;213(5):198–200. 10.5694/ mja2.50735. doi:10.5694/mja2.50735
23. Nuzzo JB, Meyer D, Snyder M, et al. What makes health systems resilient against infectious disease outbreaks and natural hazards?: Results from a scoping review. BMC Public Health. 2019;19(1):1310. doi:10.1186/s12889-019-7707-z
24. Armocida B, Formenti B, Ussai S, Palestra F, Missoni E. The Italian health system and the COVID-19 challenge. Lancet Public Health. 2020;5(5):e253. doi:10.1016/S2468-2667(20)30074-8
25. Coronavirus. France’s health workers given pay rises worth €8bn. BBC; 2020. Available from: https://www.bbc.com/news/world-europe-53398208.
26. Hix LR, Fernandes SM. An initial exploration of the physician assistant role in Germany. J Physician Assist Educ. 2020;31(1):42–47. doi:10.1097/JPA.0000000000000292
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.