")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 15
Analysis of Childhood Pneumonia: A Comparison Between the Pre- and During the COVID-19 Pandemic in a Reference Hospital in Brazil
Authors Fonseca Lima EJ , Araújo LCCD , Agra KF, Mendoza AJX, Siebra JPDB, dos Santos CS
Received 25 November 2023
Accepted for publication 19 February 2024
Published 1 March 2024 Volume 2024:15 Pages 103—110
DOI https://doi.org/10.2147/PHMT.S451735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Eduardo Jorge Fonseca Lima,1,2 Luiza Campos Corrêa de Araújo,1 Karine Ferreira Agra,2 Ana Julia Xavier Mendoza,1 Julia Pierre de Brito Siebra,1 Carmina Silva dos Santos2,3
1Department of Medicine, Faculdade Pernambucana de Saúde, Recife, Pernambuco, Brazil; 2Lato Sensu Postgraduate Department, Instituto de Medicina Integral Professor Fernando Figueira, Recife, Pernambuco, Brazil; 3Nursing Department, Faculdade Pernambucana de Saúde, Recife, Pernambuco, Brazil
Correspondence: Eduardo Jorge Fonseca Lima, Instituto de Medicina Integral Professor Fernando Figueira, Rua dos Coelhos, N° 300, Boa Vista, Recife, Pernambuco, Brazil, Tel +5581 21224166, Email [email protected]
Introduction: Community-acquired pneumonia (CAP) is one of the most common causes of childhood morbidity and mortality, causing about two million deaths per year worldwide. The complicated CAP (CCAP) results from the worsening of CAP. Their incidence has reduced in the last 30 years due to vaccination. However, the coronavirus disease (COVID-19) pandemic reduced vaccination coverage, resulting in increased incidence of CCAP in 2021 and 2022.
Objective: To analyze the clinical and epidemiological profile of CAP in children under five years of age in two periods: pre- (2018 to 2019) and during the COVID-19 pandemic (2020 to 2022).
Methods: This cross-sectional retrospective study was conducted at the Professor Fernando Figueira Institute of Integral Medicine (IMIP). We analyzed the sociodemographic and clinical variables of children with CAP aged below five years who were admitted to IMIP from 2018 to 2022. Analysis encompassed the Pearson’s Chi-square test, Fischer’s exact test, and Student’s T tests.
Results: A total of 468 children were analyzed: 382 in the pre-pandemic period and 86 during the COVID-19 pandemic. Concerning the antibiotic therapy, the most prescribed was Ampicillin (45.00%) in both periods. The combination of Oxacillin and Ceftriaxone was prescribed in 6.86% of cases in the pre-pandemic period; this value increased to 20.90% during the COVID-19 pandemic. Pleural effusion represented 12.10% of cases in the pre-pandemic period and 24.40% during the COVID-19 pandemic. The presence of pleural empyema went from 1.60% to 8.20%, and necrotizing pneumonia from 1.30% to 5.90% in the respective periods. Regarding ICU admission, 5.30% were admitted during the pre-pandemic period and 34.10% during the COVID-19 pandemic. Clinical suspicion of influenza presented a positivity rate of 17.60%.
Conclusion: Children with CAP presented a higher frequency of complications during the COVID-19 pandemic. Further research is needed to find the cause of increased CAP complications in this period.
Keywords: pneumonia, bacterial, children, COVID-19, pleural effusion
Introduction
Community-acquired pneumonia (CAP) is an infection of the lower airways caused by agents from the community environment, affecting individuals not in contact with hospital germs.1 According to the World Health Organization, CAP is the leading cause of morbidity and mortality in children aged below five years worldwide. Also, CAP causes about two million deaths per year worldwide; most occur in underdeveloped countries.2,3 In Brazil, the mortality of children under five years of age decreased by 90% between 1980 and 2010 due to several interventions, including the implementation of the pneumococcal conjugate vaccine (PCV10) in 2010. However, the disease is still among the main causes of mortality and hospitalization in the country, imposing a substantial burden on the Unified Health System (SUS).4,5
CAP may cause complications that may be related to therapeutic failures, resulting in a longer hospital stay and worse outcomes.1,5 The most frequent complications are pleural effusion, pleural empyema, necrotizing pneumonia, and lung abscess.5,6 Recent studies highlight that the coinfections (viruses and bacteria) may change the epidemiology of CAP.5 According to Johansson et al,6 coinfections represents 20% of cases, leading to more severe pneumonia and requiring longer hospital stay than those caused by an isolated bacterial agent.6
The coronavirus disease (COVID-19) pandemic brought challenges to health systems worldwide.7 Studies conducted in 2020 on COVID-19 in the pediatric population observed that Brazil was the Latin country with the highest disease incidence.8 Also, studies showed that children were less likely to present the severe forms of the disease.8,9 However, the change in the epidemiology of CAP and the direct damage of COVID-19 in the pediatric population was a major public health concern.10
The social distancing was flexible in late 2021 and early 2022. As a result, CAP cases increased and presented severe complications (eg, pleural effusion and refractory CAPs), requiring longer hospital stays.7,9 In addition, an off-season influenza epidemic emerged in the same period, leading the Ministry of Health to question the relationship between the increased cases and the low vaccination coverage in 2020.9,11
Vaccination coverage for influenza and other diseases was hampered during the COVID-19 pandemic.7–9 In 2019, vaccination coverage comprised 73.44% of the world population, 66.78% in 2020, and 56.34% in 2021, being a cause for concern considering the health of the children.12
Literature shows the relationship of COVID-19 with the increased CAP cases via coinfection with other etiological agents, and how the COVID-19 pandemic hampered vaccination rates and increased vulnerability of children to CAP.7–9 Thus, this study aimed to analyze the clinical and epidemiological profile of CAP in children under five years of age in two periods: pre- and during the COVID-19 pandemic. Also, to analyze the association of the increased severe pneumonia during the COVID-19 pandemic, enabling a better understanding of the situation and proposing more efficient interventions to reduce morbidity and mortality for the pediatric population.
Methods
This cross-sectional retrospective study was conducted from August 2022 to August 2023. Patients eligible were children with CAP aged below five years hospitalized at the Instituto de Medicina Integral Prof. Fernando Figueira (IMIP). The study collected data from two periods: the pre-pandemic period (2018 to 2019) and during the COVID-19 pandemic (2020 to 2022).
Inclusion criteria encompassed children aged under five years who presented pneumonia diagnosis confirmed by medical record. Those with unavailable medical record were excluded. Complicated pneumonia (CCAP) was related to the presence of pleural effusion, pleural empyema, lung abscess, and necrotizing pneumonia.5,6
A list of hospitalizations was obtained from the IMIP. Inclusion criteria encompassed all patients with CAP aged below five years hospitalized during the study period whose international code of diseases was related to pneumonia. Next, their medical records were collected for data analysis.
Variables analyzed included demographic (age, sex, race, and nutritional status), clinical, and laboratory data (vaccination schedule status, respiratory rate and oxygen saturation at admission, length of hospital stay [days], antibiotic therapy, and need for ICU admission). The CCAP frequency was compared with the antibiotic therapy used in each period.
For the analysis of COVID-19 and Influenza in CAP, the following situations were considered: clinical suspicion of influenza coinfection, RT-PCR for Influenza, RT-PCR result for influenza, clinical suspicion of confection by COVID-19, RT-PCR for COVID-19, and RT-PCR result for COVID-19.
Kits of the 2019-nCoV real-time polymerase chain reaction (RT-PCR) diagnostic panel were used, following manufacturer instructions (Center for Disease Control and Prevention, USA). They comprised four reagents: primer-probe mixes (2019-nCoV_N1), 2019-nCoV_N2, target human RNAse P gene to detect human nucleic acids, and the nCoVPC (noninfectious positive control material).
Data were plotted in an Excel® spreadsheet and analyzed in SPSS (version 13.0); only valid answers were considered. The results are presented with absolute and relative frequencies. The Chi-square test and Fisher’s exact test for categorical variables verified possible associations. All tests were applied with 95% confidence.
This study followed Resolution 466/12 of the National Health Council and the Declaration of Helsinki, and was approved by the research ethics committee of the IMIP (no. 5.548.941). The committee suggested that the authors collect informed consent from parents (or legal guardians) to use children’s data in this study. If contact was impossible after attempts, the committee authorized the inclusion of data.
Results
A total of 468 patients were included: 382 from the pre-pandemic period and 86 during the COVID-19 pandemic. Demographic variables are presented in Table 1. The two groups were mostly similar; however, the number of patients of the white race increased during the COVID-19 pandemic. Nevertheless, most (> 90.00%) were brown in the two periods.
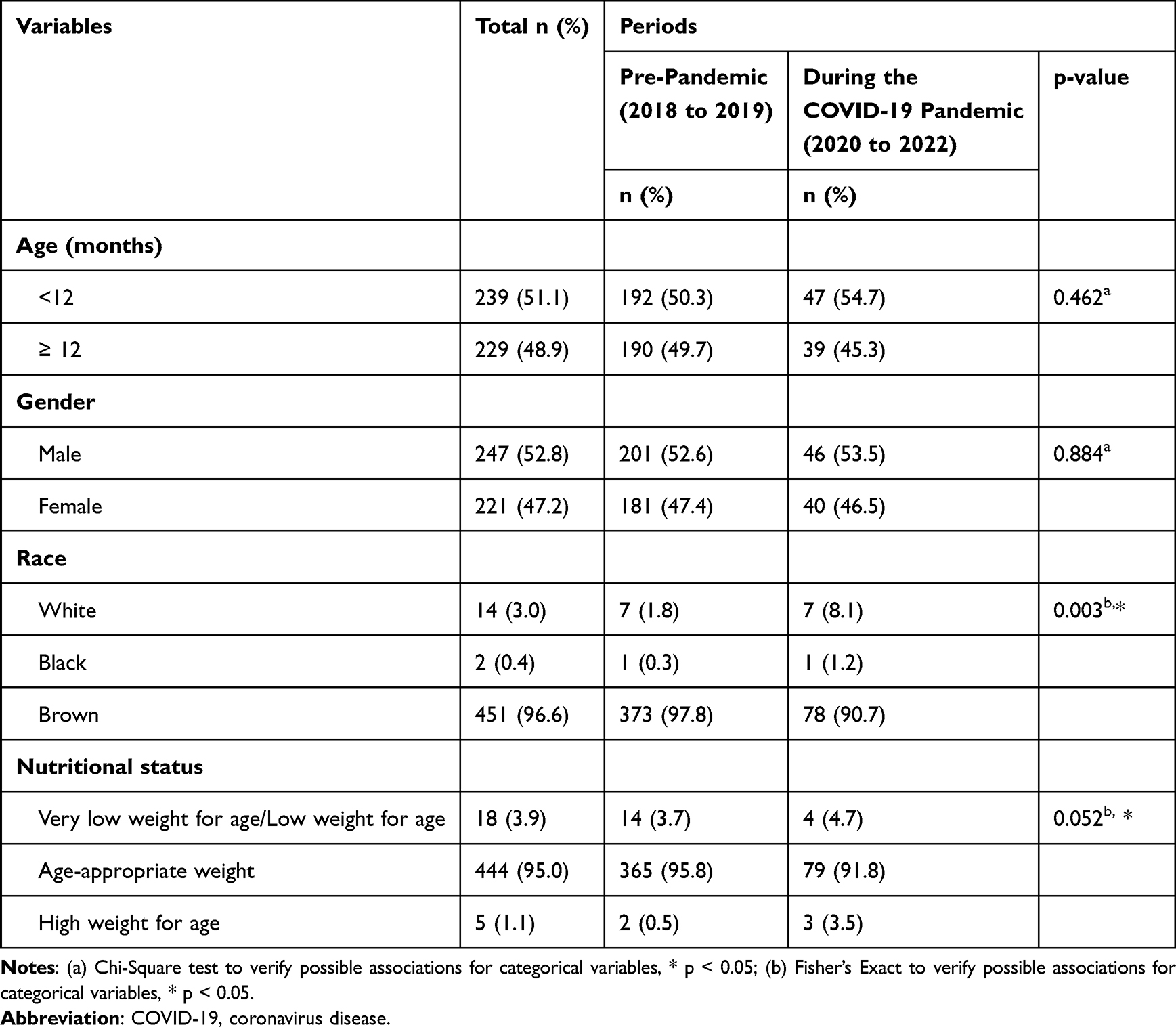 |
Table 1 Epidemiological Characteristics of Patients Under Five Years of Age Hospitalized with Community-Acquired Pneumonia in IMIP from 2018 to 2022 |
Table 2 presents the antibiotic therapy used to treat pneumonia. The Oxacillin and Ceftriaxone combination increased from 7.10% to 20.90% (p < 0.05).
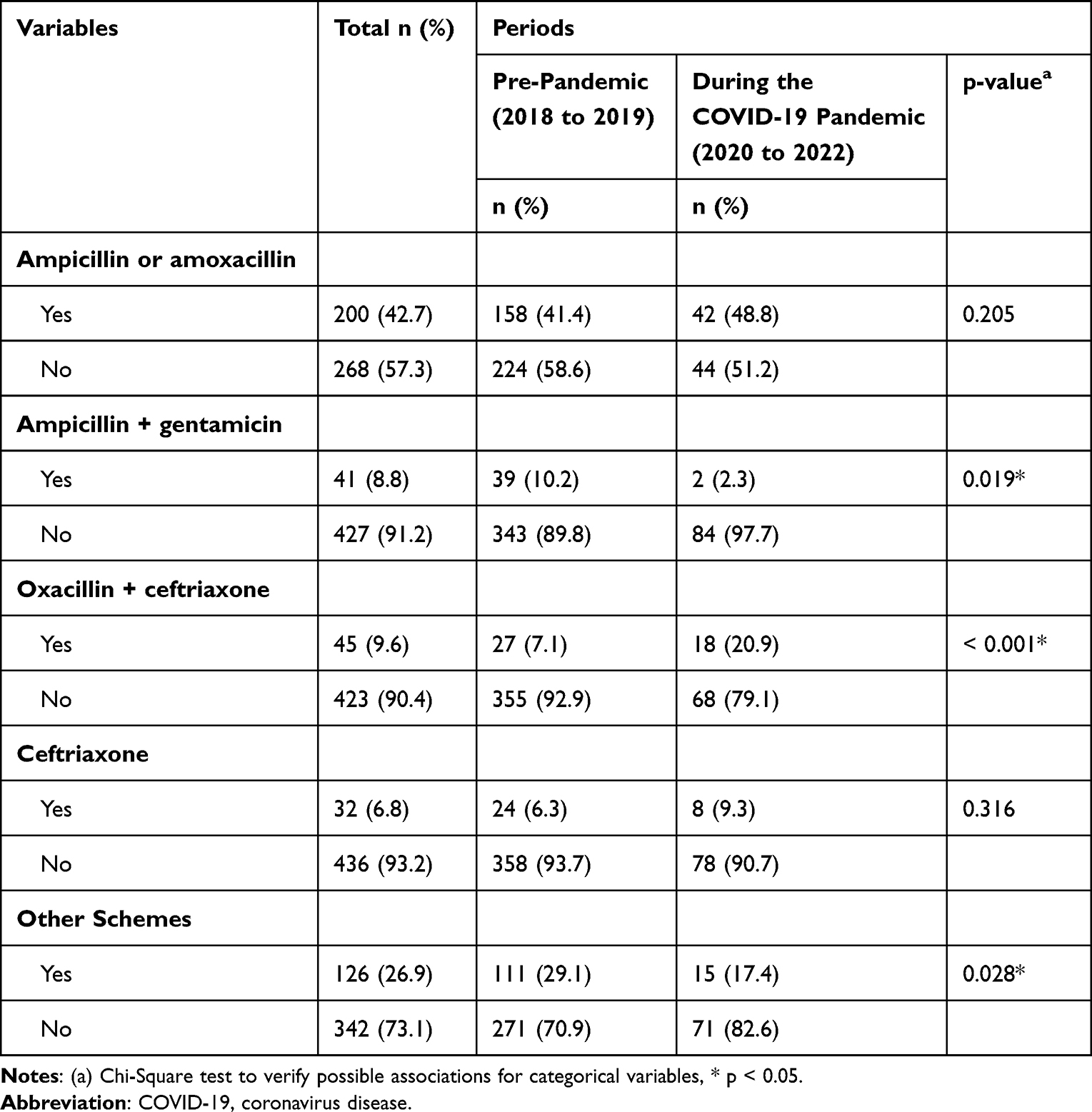 |
Table 2 Antibiotic Therapy for Patients Under Five Years of Age Hospitalized with Community-Acquired Pneumonia Before (2018 and 2019) and During the COVID-19 Pandemic (2020 to 2022). Recife, 2023 |
Table 3 shows the frequency of CCAP and indirect indicators of greater severity (ie, ICU admission and hospitalization period). ICU admission increased from 5.30% (pre-pandemic period) to 34.10% (during the COVID-19 pandemic).
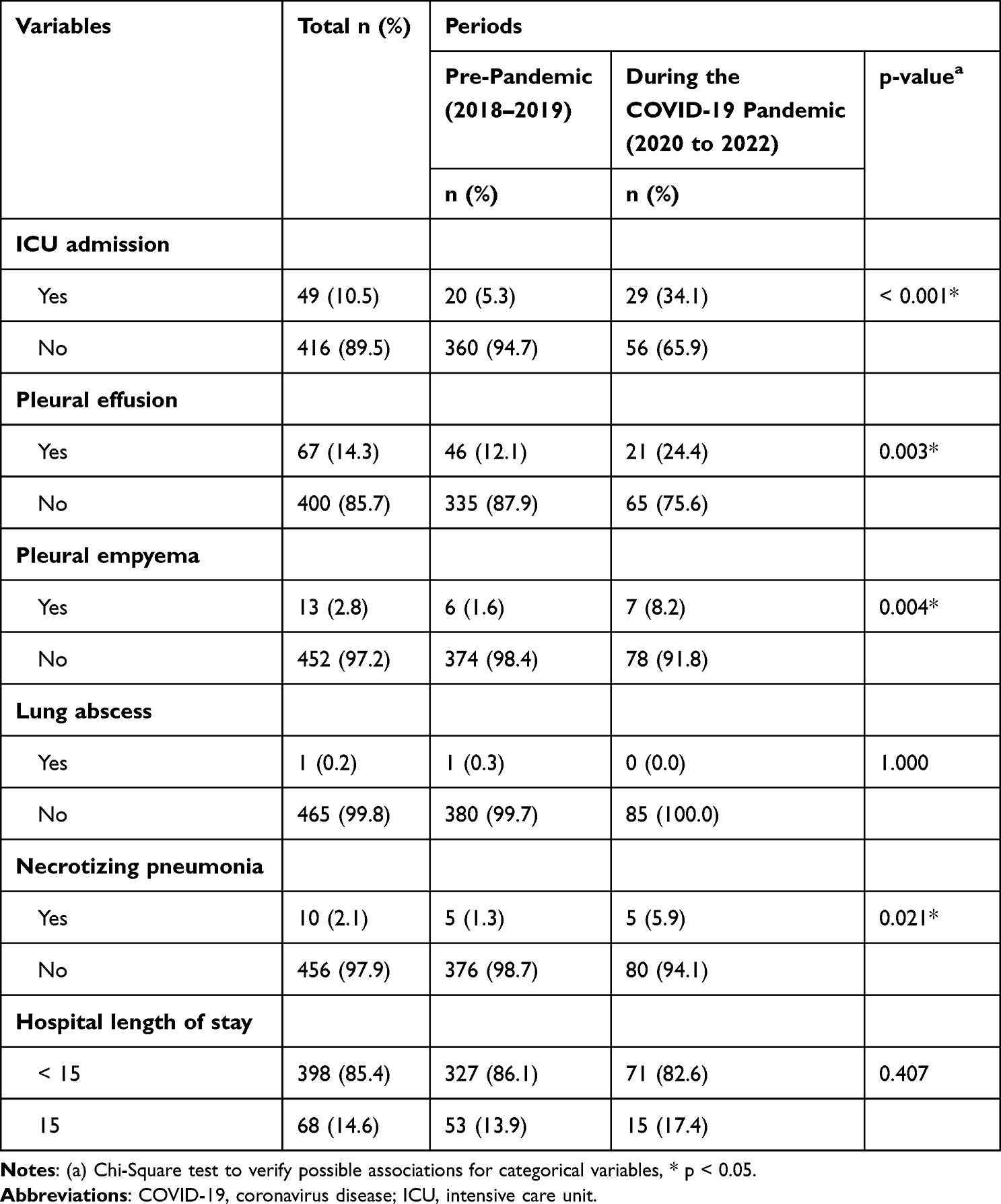 |
Table 3 Frequency of Complicated Pneumonia in Hospitalized Patients Under Five Years of Age Before (2018–2019) and During the COVID-19 Pandemic (2020–2022). Recife, 2023 |
The pleural effusion occurred in 12.10% of cases in the pre-pandemic period and increased to 24.40% during the COVID-19 pandemic. The pleural empyema and necrotizing pneumonia also increased in the same period (1.60% to 8.20% and 1.30% to 5.9%, respectively). All complications were significantly higher during the COVID-19 pandemic.
Table 4 describes the laboratory investigation for viral coinfection by Influenza viruses and COVID-19 during the pandemic. The clinical suspicion of influenza coinfection was presented in 17.6% of the cases. A total of 67 PCR tests for COVID-19 were performed, presenting seven positive cases (10.4%).
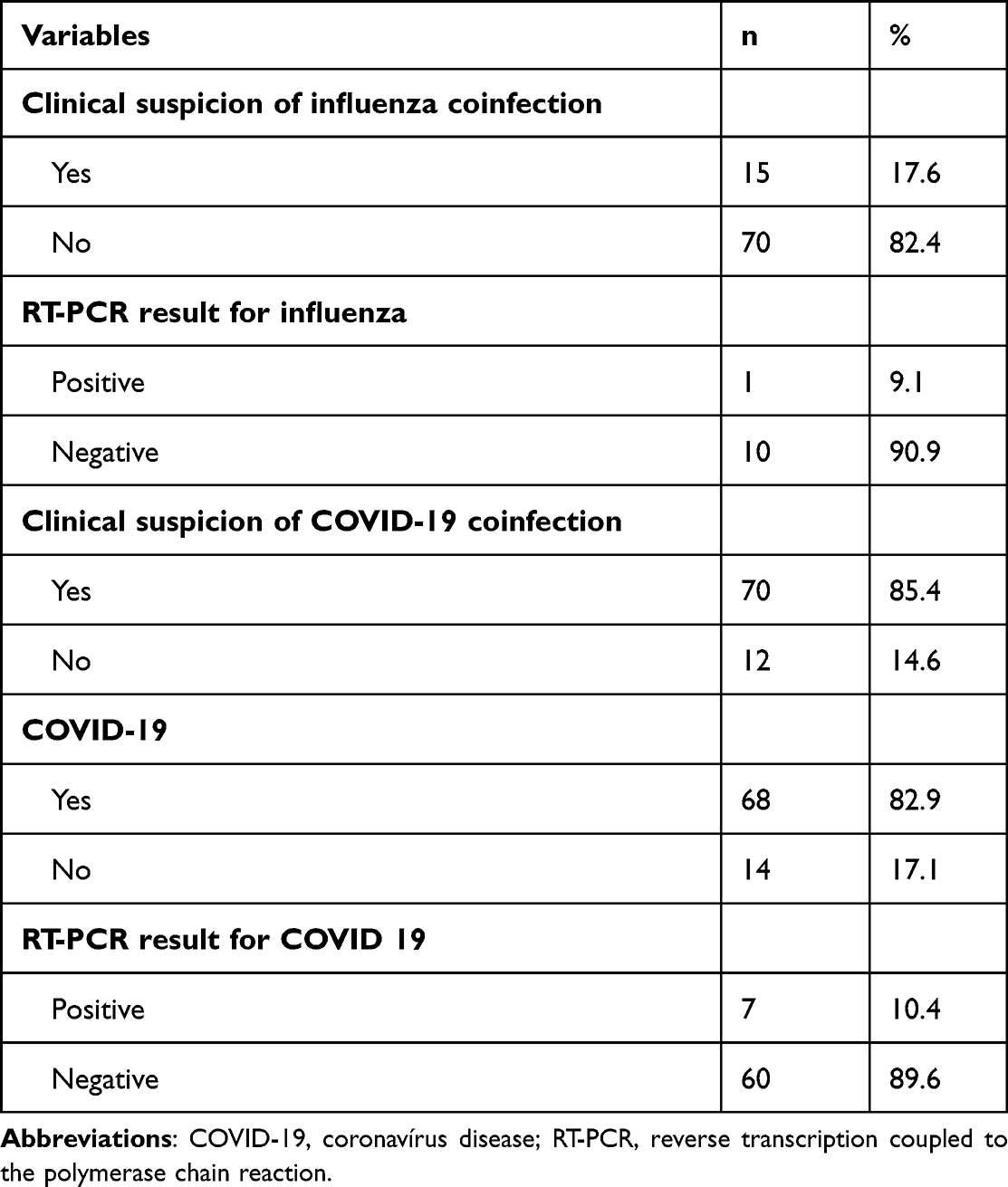 |
Table 4 Investigation of Influenza and COVID-19 Viruses as an Etiological Agent of Pneumonia in Patients Aged Below Five Years Hospitalized During the COVID-19 Pandemic |
Last, the mortality of patients with CAP was 2.2% (55 of 2397 cases) in the pre-pandemic period, increasing to 3.8% (50 of 1294 cases) during the COVID-19 pandemic.
Discussion
This study highlights that pneumonia-related complications were higher during the COVID-19 pandemic than in the pre-pandemic period. Several studies observed reduced hospitalization rates due to CAP during the COVID-19 pandemic worldwide, similarly in Brazil. According to DATASUS, 59,680 and 90,813 hospitalizations due to pneumonia occurred in 2020 and 2021 (respectively) compared with 193,684 cases in 2019.13 This variation may be attributed to the social distancing implemented during the COVID-19 pandemic. The low circulation of people reduced the exposure of children to the etiological agents of CAP.14–16
The epidemiological profile (ie, age, sex, and nutritional status) of the children were similar between the studied periods; however, complications were not related to these variables. A Chinese study17 compared hospitalized patients with CAP before and during the COVID-19 pandemic and found similar results.
The COVID-19 pandemic changed the epidemiology of CAP in the pediatric population, probably due to the low vaccination coverage for pneumococcal conjugate vaccines and influenza. Also, the SARS-CoV-2 interaction with other viruses and bacteria might have contributed to the increased CCAP.6,16 However, this topic is still controversial, requiring more studies with a proper methodology to fill this gap. Previous studies highlighted changes in the CAP epidemiology during the COVID-19 pandemic.17,18 However, studies did not address the difference in the severity of CAP during this period.
The COVID-19 pandemic contributed to the worsening of several diseases, including childhood CAP. The interruption of outpatient healthcare services, the overcrowding of medical emergencies, and the delay in seeking healthcare services during the COVID-19 waves contributed to delayed or inadequate treatment of childhood pneumoniaCAP, leading to more severe cases. The socioeconomic aspects worsened by the pandemic (eg, increased poverty, nutritional disorders, and household crowding) determined greater exposure to domestic pollution and infectious agents during the social distancing may have also been a contributing factor. In addition, many parents or caregivers died due to COVID-19, increasing the hidden impact of the pandemic on children.14–16,19
Regarding the antibiotic therapy prescribed before and during the COVID-19 pandemic, Ampicillin was still the most prescribed antibiotic in about 45% of cases. However, a previous study in the same hospital observed that the combination of Oxacillin + Ceftriaxone was applied only 6.86% of cases,20 contrasting with our results (20.90%). The increased use of this scheme implies the use of higher-spectrum antibiotics, suggesting that cases were more severe.21 According to pediatric guidelines,21,22 the Oxacillin + Ceftriaxone regimen should be used to treat CCAP or in cases that did not improve after the standard regimen with Ampicillin or Amoxicillin.
The presence of complications in pediatrics CAP is well described in the literature.5,6,22 In the present study, pleural effusion (ie, the main complication of CAP) doubled in percentage when comparing the two periods. The frequency of pleural empyema and necrotizing pneumonia also increased in the same period. This finding corroborates the concern about the greater severity of pneumonia, impacting morbidity, mortality, and hospital costs.
The present study also observed increased ICU admissions during the COVID-19 pandemic, possibly due to the clinical worsening of CAP in this period, requiring greater support. Regarding mortality, the rate increased from 2.20% in the pre-pandemic period to 3.80% during the COVID-19 pandemic. A previous study in the same hospital found a mortality rate of 1.55%, suggesting that deaths related to CAP increased during the COVID-19 pandemic.20
A possible explanation for the increased complications associated with CAP is the increased infections by Streptococcus pneumoniae serotypes, which are not included in the Pneumo 10 vaccine (ST19A, ST3, and ST6C). These serotypes were previously described as important causes of invasive pneumococcal disease in countries using PCV10 and PCV13. Another study highlighted the increased prevalence of these serotypes during the COVID-19 pandemic compared with the previous years, corroborating our findings.5
Despite the greater access to confirmatory tests (RT-PCR) during the COVID-19 pandemic, it still needs to be encouraged in the routine of a pediatric hospital. In the present study, the number of confirmatory tests was low, even when clinical suspicion of influenza or COVID-19 was described in the medical record. Regarding COVID-19, 67 RT-PCR tests were performed; 10.4% were positive. Also, virus-bacteria coinfection increases complications of pneumonia. Respiratory viruses facilitate opportunistic infections in the respiratory microbiota, justifying their association with bacterial superinfection. Several mechanisms are involved and well described in the literature.23
Although literature reports reduced vaccination rates before and during the COVID-19 pandemic,12 this information was not analyzed in this study because the vaccination card was often unavailable, and their vaccination status was not correctly filled in the medical record. Thus, these data were not included in the analysis due to a lack of reliability and the possibility of not representing reality.
Conclusion
Children with CAP aged below five years presented a high frequency of CAP and increased mortality during the COVID-19 pandemic. Further research is needed to understand the increased CAP complications observed in this study. Possible reasons are coinfection, decreased vaccine coverage, and lack of pneumococcal serotypes in the 10-valent conjugate vaccine with serotypes 3, 6A/6C, and 19A.
Measures must be implemented to reduce childhood CAP in Brazil, facilitating access to healthcare services for early diagnosis and adequate treatment of complications. Moreover, increased vaccination coverage and socioeconomic improvements in the poorest populations may also contribute to the CAP control during the pandemic period.
Acknowledgments
The authors thank Provatis Academic Services for providing scientific language translation and editing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sociedade Brasileira de Pediatria - Documento Científico. Abordagem Diagnóstica e Terapêutica das Pneumonias Adquiridas na Comunidade Não Complicadas [homepage on the Internet]. Dep Científico Pneumolgia; 2021:1–11. Available from: https://www.sbp.com.br/fileadmin/user_upload/23054d-DC-Pneumonias_Adquiridas_Nao_Complicadas.pdf.
2. Leung AKC, Wong AHC, Hon KL. Community-Acquired Pneumonia in Children. Recent Adv Inflamm Allergy Drug Discov. 2018;403(2):136–144. doi:10.2174/1872213X12666180621163821
3. Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the sustainable development goals. Lancet. 2016;388(10063):3027–3035. doi:10.1016/S0140-6736(16)31593-8
4. Gomes M. Pneumonia adquirida na comunidade: os desafios da realidade brasileira. J Bras Pneumol e Tisiol. 2018;44(4):254–256. doi:10.1590/s1806-37562018000040002
5. Benedictis FM, Kerem E, Chang AB, Colin AA, Zar HJ, Bush A. Complicated pneumonia in children. Lancet. 2020;396(10253):786–798. doi:10.1016/S0140-6736(20)31550-6
6. Corrêa RD, Costa AN, Lundgren F, et al. 2018 recommendations for the management of community acquired pneumonia. J Bras Pneumol. 2018;44(5):405–423. doi:10.1590/s1806-37562018000000130
7. Fundo das Nações Unidas para a Infância (UNICEF). A pandemia de Covid-19 leva a um grande retrocesso na vacinação infantil, mostram novos dados da OMS e do UNICEF [homepage on the Internet]. UNICEF para cada crinaça, Brasil; 2021. Available from: https://www.unicef.org/brazil/comunicados-de-imprensa/pandemia-de-covid-19-leva-A-um-grande-retrocesso-na-vacinacao-infantil.
8. World Health Organization (WHO). Global Immunization News [homepage on the Internet]. Technical Information, East Asia; 2012. Available from: https://cdn.who.int/media/docs/default-source/immunization/gin/archives/gin_january_2012.pdf.
9. Nehab MF, Meirelles AF, Chaves CR, et al. Covid-19 e saúde da criança e do adolescente. Rio de Janeiro: Fiocruz; 2020. Available from: https://portaldeboaspraticas.iff.fiocruz.br/atencao-crianca/covid-19-saude-crianca-e-adolescente.
10. Pandemia de COVID-19 leva a grande retrocesso na vacinação infantil, mostram novos dados da OMS e UNICEF [homepage on the Internet]. OPAS/OMS | Organização Pan-Americana da Saúde; 2021. Available from: https://www.paho.org/pt/noticias/15-7-2021-pandemia-covid-19-leva-grande-retrocesso-na-vacinacao-infantil-mostram-novos.
11. H3N2: novo vírus influenza em circulação no país [homepage on the Internet]. Biblioteca Virtual em Saúde MS. Available from: https://bvsms.saude.gov.br/h3n2-novo-virus-influenza-em-circulacao-no-pais/.
12. Ferreira V Cobertura vacinal no Brasil está em índices alarmantes [homepage on the Internet]. Instituto Oswaldo Cruz; 2022. Available from: https://portal.fiocruz.br/noticia/cobertura-vacinal-no-brasil-esta-em-indices-alarmantes.
13. TabNet Win32 3.0: morbidade Hospitalar do SUS - por local de internação - Pernambuco. Ministério da Saúde - DATASUS; 2021. Available from: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sih/cnv/nipe.def.
14. Alves JC, Lopes CR, Guzzi GP, et al. Impacto da pandemia de COVID-19 na epidemiologia pediátrica. Resid Pediatr. 2020;10(3):1–4.
15. Carvalho MF, Carvalho AA, Martins PL. Impacto da pandemia COVID-19 no perfil de internações pediátricas: análise comparativa dos anos 2018 a 2020. RICM. 2022;6(2):36–40.
16. Dagan R, van der Beek BA, Ben-Shimol S, et al. The COVID-19 pandemic as an opportunity for unravelling the causative association between respiratory viruses and pneumococcus-associated disease in young children: a prospective study. EBioMedicine. 2023;90:104493. doi:10.1016/j.ebiom.2023.104493
17. Zhang LN, Cao L, Meng LH. Pathogenic changes of community-acquired pneumonia in a children’s hospital in Beijing, China before and after COVID-19 onset: a retrospective study. World J Pediatr. 2022;18(11):746–752. doi:10.1007/s12519-022-00592-8
18. Queiroz SP, Espíndola LP, Nogueira BD, Carvalho HO, Cartaxo HB. O impacto da COVID-19 em internações por pneumonia de crianças escolares e pré-escolares. Res Soc Dev. 2022;11(7):e49511730231. doi:10.33448/rsd-v11i7.30231
19. Ferrero F. Impact of the COVID-19 pandemic on the circulation of common respiratory viruses. Arch Argent Pediatr. 2022;120(4):218–219. doi:10.5546/aap.2022.eng.218
20. Lima EJF, Lima DE, Serra GH, Lima MAA, Mello MJ. Prescription of antibiotics in community-acquired pneumonia in children: are we following the recommendations? Ther Clin Risk Manag. 2016;983–988. doi:10.2147/TCRM.S101709
21. Nascimento-Carvalho CM. Community-acquired pneumonia among children: the latest evidence for an updated management. J Pediatr. 2020;96:29–38. doi:10.1016/j.jped.2019.08.003
22. Diretrizes brasileiras em pneumonia adquirida na comunidade em pediatria - 2007. Sociedade Brasileira de Pneumologia e Tisiologia. J Bras Pneumol. 2007;33(suppl 1):s31–s50. doi:10.1590/S1806-37132007000700002
23. Brealey JC, Sly PD, Young PR, Chappell KJ. Viral bacterial co-infection of the respiratory tract during early childhood. FEMS Microbiol Lett. 2015;362(10):fnv062. doi:10.1093/femsle/fnv062
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.