")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Analysis of Centralized Efficiency Improvement Practices in Australian Public Health Systems
Authors Walters JK, Sharma A, Boyce J, Harrison R
Received 11 August 2023
Accepted for publication 10 November 2023
Published 15 November 2023 Volume 2023:15 Pages 313—326
DOI https://doi.org/10.2147/JHL.S435035
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
James Kenneth Walters,1 Anurag Sharma,2 Jamie Boyce,1 Reema Harrison3
1HealthShare NSW, NSW Health, St Leonards, NSW, Australia; 2School of Population Health, UNSW, Sydney, NSW, Australia; 3Centre for Health Systems and Safety Research, Australian Institute of Health Innovation, Macquarie University, North Ryde, NSW, Australia
Correspondence: James Kenneth Walters, Email [email protected]
Aim: Analysis of centralized efficiency improvement practices in Australian public health systems.
Introduction: Public health systems seek to maximize outcomes generated for resources used through efficiency improvement (EI) in response to funding and demand pressures. Despite this focus, evidence for EI approaches at the whole-of-system level is lacking in the literature. There is an urgent need for evidence-based approaches to centralized EI to address these pressures. This study aims to address this gap by answering the research question “How is EI conceptualized and managed by central public health system management entities in Australia?”.
Material and Methods: Document analysis was selected due to its suitability for systematically searching and appraising health system documentation, with this study following Altheide’s approach focusing on whole-of-system strategic plan and management framework documents originating from Australian public health organizations.
Results: Conceptualization of efficiency varied substantially with no consistent definition identified, however common attributes included resource use, management, service and delivery. Forty-two of 43 documents contained approaches associated with improving efficiency at the whole of system level.
Discussion: While no comprehensive framework for centralized EI was evident, we identified nine core approaches which together characterize centralized EI. Together these approaches represent a comprehensive evidence-based approach to EI at the whole of system level.
Conclusion: The approaches to whole-of-system EI identified in this study are likely to be highly transferable across health systems internationally with approaches including strategic priority setting, incentivization, performance support, use of EI evidence, digital enablement and workforce capability development.
Keywords: efficiency, public health, health management
Introduction
Public health systems internationally continue to be challenged by increasing demand for health care, compounded by pressures to enhance health outcomes amidst the current climate of uncertainty and tightening government finances.1–3 These pressures necessitate a focus on maximizing value in terms of health outcomes achieved for resources invested.4 Health systems therefore require cost-specific improvement practices that do not negatively impact either the quality of outcomes achieved or the experiences of staff and consumers. Despite this requirement, efficiency and cost are not always consistently connected to care quality and experiences in the context of improvement, with many approaches focusing largely on reducing cost and achieving budget results with little regard to other outcomes.5,6 Our recent rapid systematic review of 82 publications found that inefficiencies in public health systems can be driven by a range of factors including workforce pressures, waste, low-value activity, limited evidence for efficient practices and reactive approaches to cost control, as well as shortfalls in conceptualization of efficiency among healthcare workers.7,8 Health system managers must be cautious when seeking to manage service cost alone, as this can lead to false representations of efficiency, unsustainable short-term improvements and detrimental impacts to service quality and stakeholder experience.7,8
Value is addressed in differing ways between health systems internationally with a three-fold focus on patient, technical and allocative value in the UK, a focus on integrating fragmented system elements to improve performance and outcomes in the US, and a balance between health outcomes, efficiency and experience in Australia. The World Health Organization describes efficiency as cutting across the broad health system goals of equity, access and outcomes; improved efficiency should enable greater outcomes to be achieved with the same or fewer resources while also contributing to health system’s financial stability.9 Despite different ways of characterizing value, the underlying theme of maximizing health outcomes for resources invested remains consistent.10,11 Where resources are limited, the importance of maximizing outcomes achieved with available resources is key to ensuring health systems are able to respond to requirements for performance improvement, transformation and reform.3,12 This further heightens the imperative for public health systems to understand how to undertake deliberate, coordinated action to improve efficiency.13
The inclusion of efficiency in health system performance management frameworks and indicators is commonplace in health systems internationally, however frameworks for centralized EI management in public health systems at the whole-of-system level are lacking in the literature.8,14 In practice, the extent to which EI priorities translate to the policy and performance frameworks required to operationalize them is unclear.15,16 The consistency with which EI targets and processes are defined and included within common governance and management instruments such as budgets, service level agreements and key performance indicators at a whole-of-system level is also unclear.17 This results in a lack of clarity as to how EI is positioned by system management policies and frameworks in public health systems, as well as uncertainty of the extent to which system-wide EI is linked to service quality, experience and value outcomes.8 To address this issue, there may be potential for centralized approaches to support planned, coordinated efficiency improvement (EI) across healthcare systems and organisations internationally; however, evidence of such models in the literature is limited.8,10 This results in a lack of guidance for individuals and teams involved in EI work at a whole of system level.8,18 This further heightens the imperative for public health systems to understand how to undertake deliberate, coordinated action to improve efficiency.13
The Australian public healthcare system is distinguished by a complex array of funding and service responsibilities split between the Federal and State governments. Service cost and price are set independently at a Federal level, while State governments administrate funding and performance management for Local Hospital Networks within each state which manage delivery of tertiary care health services within their jurisdictions, with funding administered by State governments who are also responsible for their performance management.19 The State Department or Ministry of Health acts as a statewide system management entity, utilizing policy and performance frameworks implemented to agree and monitor performance against activity and financial performance metrics.20 These federal and state-based systems within the Australian public health system provide examples of centralized multi-state governance models which are explored in this study in the context of EI. As evidence for such centralized models in the literature is extremely limited in this context, the Australian system provides a unique opportunity to address this gap in the literature by exploring current practices for centralized EI at the whole of system level.
In the context of ever-increasing demand and constrained resources, there is an urgent need to understand how public health systems are responding to the contemporary challenges posed by increasing requirements for improved outcomes, experiences and efficiency.3 To address the knowledge gap regarding how health systems may support EI practices, a document analysis was undertaken in the Australian healthcare system. The document analysis sought to identify how Australian public health systems centrally define and manage EI at the whole-of-system level through documented processes, priorities and performance requirements. This study aims to answer the research question “How is EI conceptualized and managed through policy and performance frameworks across central public health system management entities in Australia?”.
This study contributes to the gap in the literature on whole-of-system approaches to EI by identifying and synthesizing definitions and approaches to system-wide, centralized EI in Australian public health systems. This provides a consolidated view of how efficiency is currently conceptualized, established as a strategic priority and centrally driven through performance management frameworks. The findings of this study can be applied to public health systems internationally within the context of value-based care, providing evidence for the importance of and scope for including EI in the governance mechanisms by which healthcare organisations design and deliver services while driving improvements in outcomes gained for resources invested.
Materials and Methods
Document analysis was selected due to its suitability for systematically searching and appraising health system documentation, such as strategic and policy documents, relevant to addressing the research question.21–23 This study followed Altheide’s approach to document analysis due to its application in contemporary healthcare document analysis studies, with the unit of analysis being any specific content relating to EI, measurement, support or conceptualization.23–25 The study is reported using the Standard for Reporting Qualitative Research (SPQR) guideline.26
Identification and document selection
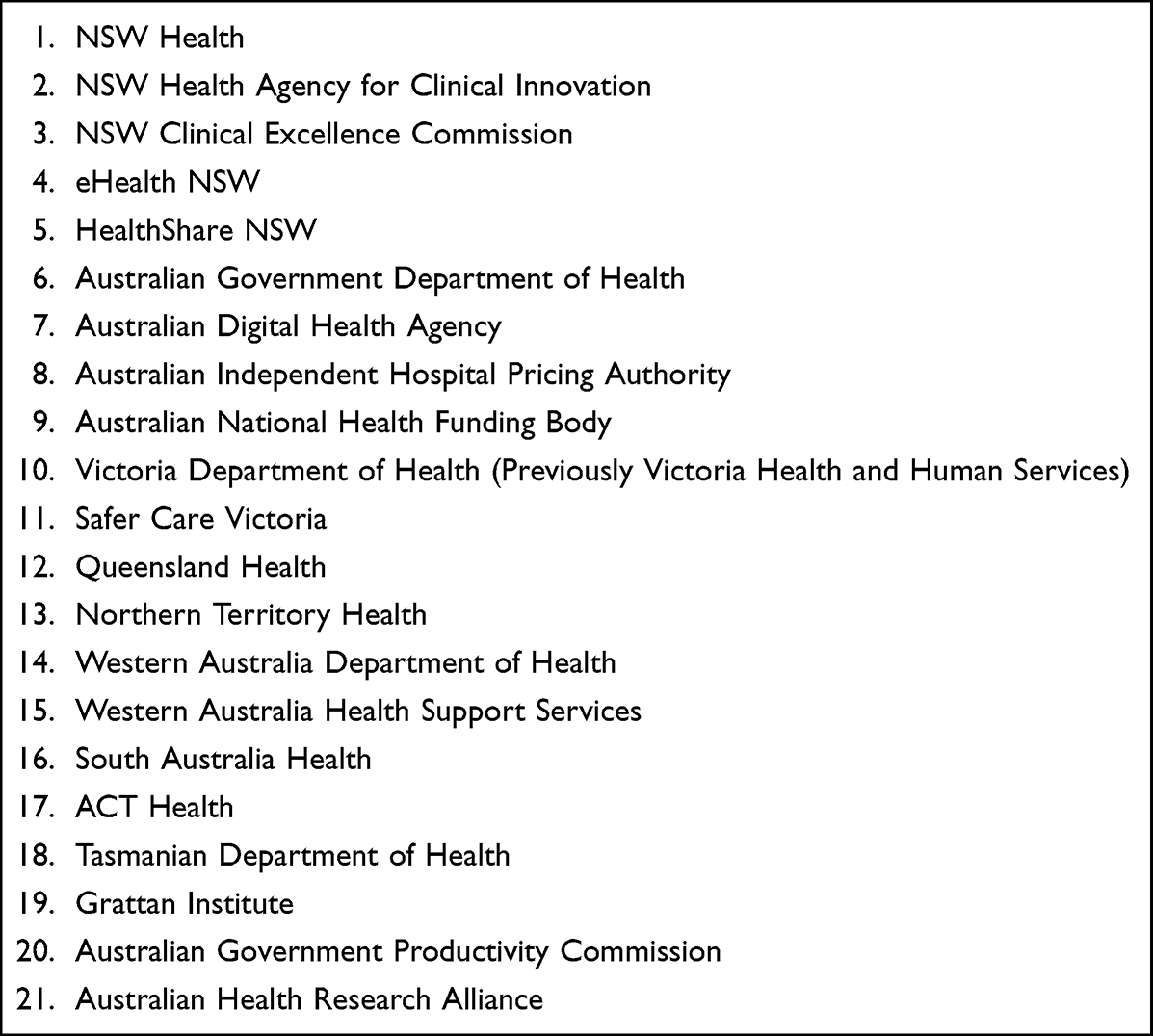
To ensure all relevant data sources were searched, a list of departments and agencies meeting eligibility criteria was compiled with each identified source systematically searched. A list of search terms based on a recent literature review was agreed by the authors and applied by one author (JW) to each website to identify an initial range of documents for potential inclusion.8 These terms included efficient/efficiency, value performance and finance/financial in combination with improvement and support. Each website was also hand-searched for potentially relevant documents. The list of websites searched is outlined in Box 1 below:
 |
Box 1 Search Strategy |
The websites of the following organisations were searched to identify policy, strategic and framework documents relevant to centralized EI in public health systems. The search was restricted to Australian Federal and State public health administration entities. Key websites included central system management, performance and policy entities. Search terms included efficiency, value, performance and finance in combination with improvement and support. A timeframe of 2010 onwards was applied. Documents focusing on environmental rather than financial sustainability and documents classified as guidelines, plans and reports were excluded.
Eligibility Criteria
Inclusion Criteria
Sources: Strategic, policy and framework documents which set out system governance and priorities from Australian State, Territory and Federal health system administration departments and associated agencies were eligible, as such entities lead strategic, policy and guideline setting across organisations within their broader systems.
Document type and publication date: Documents published from 2010 onwards were included to broadly align with the current paradigm of value-based healthcare and explore contemporary material. Documents labelled as policies, strategic plans and frameworks were included as these represent the instruments of health system management.
Content: Eligible content related to conceptualization of EI, principles and processes of improvement and alignment of EI with other strategic and service outcomes were included in the analysis.
Exclusion Criteria
Documents originating from organisations supervised by State, Territory and Federal departments fitting the definition of Local Hospital Networks (LHNs) under the National Health Reform Agreement were excluded in order to maintain the focus of this study on centralized system-wide approaches, as central ministries and departments are responsible for system management of Local Hospital Networks under the Agreement.19 As such, documents originating from single facilities within these broader geographical organisations were excluded. Reference guides, project plans, presentations and communications material were excluded in addition to documents without clear content relating to EI when examined were excluded.
Data Extraction and Analysis
One author (JW) manually analyzed each document for content specifically referring to efficiency and extracted relevant information according to the eligibility criteria, with a data extraction record used to document findings. The following data were extracted: Organisation, system/service level, title, year published, document type, document function and core content relating to EI. The data extraction record was used to systematically analyze the data from each reviewed document. A second author (JB) independently conducted a manual analysis of the documents, with JB and JW meeting to compare results to validate the accuracy and comprehensiveness of the extracted data. A narrative synthesis approach was applied to the extracted data to address the research question, establishing key themes for structured exploration of extracted content.27,28 The data extraction record enabled the analysis to proceed by grouping information specific to efficiency definitions and central support approaches in separate groups to address both elements of the research question. All data in each group were systematically examined and findings condensed into boxes to provide a concise representation of the complexity of data extracted. These findings were discussed and agreed upon by the authors prior to being finalized.
Results
The search covered websites across 21 organisations, yielding a set of 53 documents, which the authors screened and collectively discussed to determine suitability for inclusion based on inclusion/exclusion criteria. One duplicate was removed. Forty-three documents from 18 organisations were included in the final review. Two documents were published in 2022, 13 in 2021, four in 2020, five in 2019 and 2018, three in 2017, five in 2016, three in 2015 and three in 2013. Twenty-three of the 43 included documents were classified as frameworks, while the remaining 20 documents were classified as strategic plans. The primary purpose of 20 documents was to outline organizational strategic priorities, nine were developed to improve or recommend capability in specific practice areas, 10 set out management frameworks and the remaining four set out business rules and legislative requirements for public health system administration.
Characterizing Efficiency
Sixteen documents (30%) provided a definition of efficiency, while the remaining 32 (70%) did not. Efficiency measures were specified in just over half (n = 27) of documents. Document focus areas related to EI were identified in almost all documents (n = 42) and 33 documents referred directly to improving efficiency. Specific measures relating to efficiency were identified in 24 documents. Of the 21 organisations included in the study, relevant documents were included from 18 organisations, while searches of websites of the remaining five organisations did not identify any documents, with content specifying or related to EI at whole-of-system or centralized levels. Thirty-six documents were obtained from public health system management organisations, three from government health administration organisations, three from non-government organisations and two from public health system supporting organisations. A list of included documents is shown in Table 1 below:
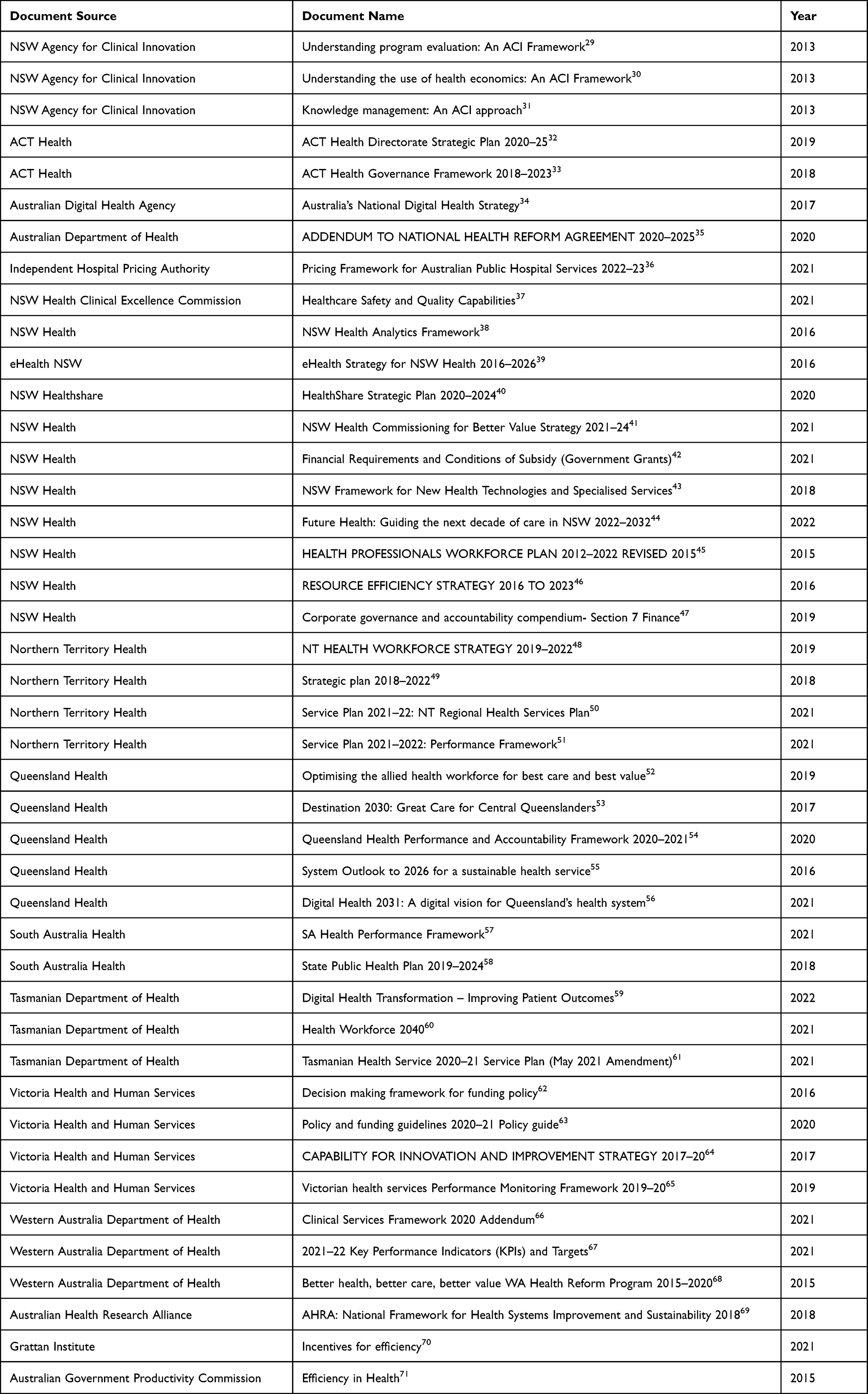 |
Table 1 List of Included Documents |
Defining Efficiency
Twenty definitions for efficiency were identified in total. Efficiency was defined using a range of terms, with no two definitions being identical or closely similar. This included variations in the definition between documents originating from the same organisation. Despite the variation in definitions, several common terms were identified. The term “resources” was identified in 10 definitions, “service” in six definitions, “deliver” in seven, “management” in three and “value” in two. Financial terms appeared in six definitions, with “cost” identified four times and “budget” identified twice. Additionally, two documents from the same organisation provided a related definition of value as “outcomes and experience relative to the costs of achieving them”.41,44 All definitions identified in the analysis are shown in Box 2 below:
 |
Box 2 Definitions of Efficiency |
Improving Efficiency
42 of 43 documents contained approaches associated with improving efficiency at the whole of system level, of which 29 used the term efficiency directly. No comprehensive framework or approach for centralized public health system support or management of EI was identified. A range of high-level themes were identified including establishing strategic priorities, including efficiency in system performance management frameworks, improving infrastructure efficiency, driving change through funding models and financial incentives, data and analytics, staff capability development and use of evidence. Establishing efficiency and sustainability as strategic priorities was identified in six documents, as was establishing EI performance measures and targets. Specific digital enablement and workforce capability approaches to EI were identified in 13 documents. A summary list of approaches is provided in Table 2.
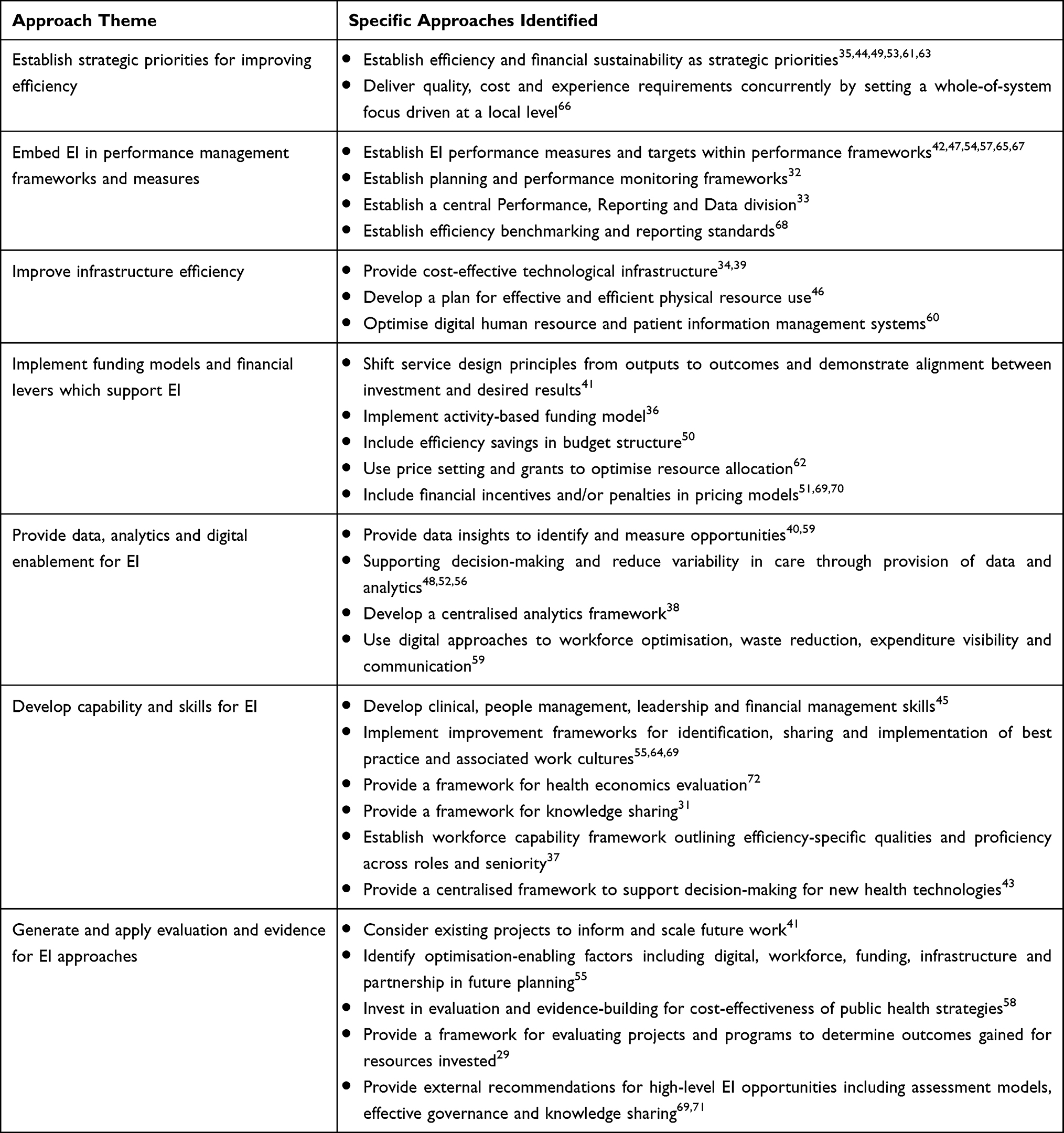 |
Table 2 Summary of System-Level Management Approaches to EI |
Establish Strategic Priorities for Improving Efficiency
The identification of EI as a strategic priority was identified at a federal level as a key reform principle as well as at a state level in documents from obtained from the Northern Territory, Queensland, Tasmania, New South Wales and Victoria. Recommendations were made for improving efficiency including development of models and methods to assess effectiveness, efficiency and cost-effectiveness of models of care as well as optimizing knowledge translation, scalability, implementation, adoption and diffusion of best practice.35,53 It was suggested that collaboration with internal and external partners can build shared accountability for service deliverables, thereby promoting value with a focus on outcomes and sustainability.44 Strategic priorities also supported EI through setting a strategic direction to establish a system-wide efficiency plans and performance measures to achieve efficient and sustainable services where these were not already in place.49,61,65
Embed EI in Performance Management Frameworks and Measures
The inclusion of efficiency elements in performance management and system governance documents was identified in documents from the state public health systems of New South Wales, Queensland, South Australia, Victoria, Western Australia and the Australian Capital Territory. This included the specification of performance metrics, the service area each metric related to and the frequencies at which they were to be reported.42,47,57,65,67,68 This was also supported by an overarching focus on effective resource allocation and utilization.54 Use of a centralized function to coordinate and report on EI requirements across the public health system was identified as a driver of these functions.33,42
Improve Infrastructure Efficiency
Improving the efficiency of infrastructure was a direction noted in documents arising from supporting agencies in New South Wales, Tasmania and the Australian Digital Health Agency with a specific digital, resource or workforce focus, as opposed to being identified in overarching strategic plans and performance frameworks arising from frontline service agencies. This included striving towards digitally enabled models of care and asset management to drive improved accessibility, quality, safety and efficiency.34,46 Also included was the importance of providing information and communications technology which promotes workforce engagement, streamlines workflows and enables timely access to information.39,46,60
Implement Funding Models and Financial Levers Which Support EI
A mix of state, supporting and independent advisory organisations across New South Wales, the Northern Territory, the Independent Hospital Pricing Authority, Victoria, the Australian Health Research Alliance and the Grattan Institute advocated for the use of funding models and levers to promote EI. Changing service design from outputs to outcomes was suggested as a fundamental shift towards efficiency.41 Activity-based funding models were represented as a catalyst for improving efficiency up to a common standard.36 Including efficiency savings in budgets was identified as a means to link EI and financial performance, while grants were recognized as a means to support smaller or unique services.50,62 The use of financial incentives and penalties to encourage more efficient practices while discouraging less efficient practices was recommended from an independent advisory perspective.69,70
Provide Data, Analytics and Digital Enablement for EI
Documents from supporting agencies promoted the use of data to provide insights and identify opportunities to improve and measure efficiency.40,59 It was suggested that workforce optimization, reduced waste, visibility over expenditure, access to funding and staff communication could all be digitally enabled to promote EI.40 In turn, decision-making could also be improved through access to data across areas including access, waste, variability, staffing and future planning.48,52,56 One document from New South Wales suggested that consistent application of data insights could be supported through the use of a statewide analytics framework.38
Develop Capability and Skills for EI
Documents from Queensland, New South Wales, Victoria and the Australian Health Research Alliance identified the need to develop workforce EI skills to identify and measure opportunities, use data and analytics and ensure consistent EI approaches across the system.38,55,56 This included both clinical and financial management skills, supported by improvement frameworks and cultures.30,45,64 Frameworks for knowledge management, quality and technology assessment were similarly presented.31,37,43 The capability for collaboration and partnership-building was also identified as an enabler of EI.55,69 Training and development in the use of EI implementation tools represents an additional focus area for central capability development.
Generate and Apply Evidence for EI Approaches
South Australia, Queensland, New South Wales as well as federal and advisory agencies promoted the importance of generating and applying evidence for EI. This included the use of current and past projects to inform future work and the use of data to inform continuous improvement.41 Understanding factors which are associated with EI and was considered within the context of evidence-based EI.55,58 Three documents advocated and provided approaches for specific work towards building evidence for efficient and cost-effective practices.37,58,69 The Australian Government Productivity Commission proposed detailed areas to investigate for EI opportunities on the basis of a comprehensive review including pharmaceutical subsidy review, technology assessment process review and sharing of assessment findings and including a safety and quality aspects in price-setting.71 This study did not identify the application of any case studies or examples of centralized EI being used in practice for the purpose of informing future strategic or governance document development, representing an opportunity for future such documents to be informed by examples of previous evidence and experience.
Discussion
Efficiency has been recognized as a pillar of health service quality and value for decades, with the link between resources used and outcomes achieved being well established as hallmarks of efficiency.4,73 The theme of Australian public health systems seeking to achieve greater or improved health outcomes for resources invested by improving efficiency was a common theme across the strategic plans and system management frameworks included in this study, with 43 documents from 18 organisations making direct reference to improving efficiency. Only 3 organisations included in the document search did demonstrate efficiency-related content in documents matching the inclusion criteria. This indicates that the strategic prioritization of EI and the management of public health systems in a way which drives EI at a whole of system level are commonly established within Australian public health organisations.
Despite this high-level consensus on the inclusion of EI in strategic plans and system management frameworks, the way in which efficiency is defined across the system-level documents of Australian public health organisations is highly variable. Not only was a standard definition not identified, no two organisations or even any two documents from the same organisation defined efficiency in the same terms. This is at odds with the literature, in which definitions for efficiency in the context of healthcare are reasonably consistent.8 At a higher level, the conceptualization of efficiency is more consistent across the documents included in this study, with several core themes evident across the range of identified definitions including resource use, service delivery, management and finances. These align well with contemporary definitions of efficiency and its central role within value.4,8 Additionally, the desired impacts of improved efficiency were highlighted across the range of definitions identified, demonstrating that the purpose of improving efficiency is to maximize the use of resources to deliver the right mix and amount of sustainable high-quality services.4
For a range of the public health organisations included in the study to formally prioritize EI, efficiency was specified as a strategic priority and was subsequently included in performance management frameworks, with performance measures and targets required to achieve this priority clearly articulated. These themes were apparent in six strategic plans and six management frameworks, respectively, from the set of documents included in this study. These represent enabling steps which set the course of action for public health organisations towards improving efficiency, thereby supporting the development and implementation of service agreements and specific actions aimed at meeting performance targets.17,20 This also underpins the development of system-wide policy to set a balance between resource use and outcomes achieved.74 Centralized performance teams and reporting processes were identified to drive EI at a whole of system level to meet specified efficiency-related strategic priorities and performance targets.20,75
The utility of funding levers for supporting EI was noted across seven documents. This was underpinned by linking resources invested with outcomes achieved, activity delivered and investment impact. Financial incentives, penalties and grants were identified as mechanisms to incentivize targeted efficiency improvements, as was including the realization of efficiency benefits as a part of operating budgets. This can allow public health organizations to direct the use of fiscal resources in a manner which promotes efficiency, prioritizes the achievement of efficiency targets and encourages increases in desired activity and/or reductions in low-value activity.76,77 A challenge was also recognized in relation to linking outcomes with financial levers, as outcome-based performance measures require further development.44 Four documents highlighted the pursuit of cost-effective infrastructure, physical resources and information management systems as directions for improving efficiency, providing further insights into the potential for EI to be driven at an organisation-wide level through effective information and asset management processes.12
Six documents recognized the requirement for public health organisations to develop EI capability and skills of their workforces. Key to this direction was the provision of data and analytics, highlighting the scope for digital enablement of EI. This included EI decision support, opportunity identification and performance monitoring. Beyond digital supports, workforce development directions also included management and leadership skill development, knowledge sharing frameworks and delineation of efficiency skills required across various levels of seniority. These approaches are likely to promote stakeholder engagement in EI processes by ensuring efficiency messaging is made relevant and accessible for clinical and management staff, promoting staff involvement in EI decision-making and providing evidence of improvements achieved.78,79
Further to the association between sharing knowledge of EI approaches and their performance with improved EI engagement, six documents identified actions aimed at generating and applying evidence for successful EI strategies. These included investing in evaluation of current and past projects to identify lessons to apply in the future and identifying factors which support EI such as digital enablement, funding, infrastructure and partnerships. The use of this information to inform future projects was recommended, while common opportunities for EI in health organisations were also identified. Such use of evidence to improve resource utilization and outcomes realization is a key element of value.4,10 This also links with the theme of developing capability and skills for EI, with evidence for approaches which collectively improve cost, quality and experience linked with stakeholder engagement in EI strategies.80,81
While each definition of efficiency identified in this study was different, a range of common elements across definitions can be used to infer how efficiency is currently defined in practice. These included generally a focus on maximizing resource use to achieve the best and most appropriate health outcomes, concepts which align closely with how value is currently conceptualized and the inclusion of efficiency as a core element of value.4,73 Public health organisations seeking to specify efficiency-related content in system-level documentation should align with these concepts when defining efficiency within their local context. Although efficiency is consistently defined in the literature, the wide variation in definitions used in practice identified through this research highlights a need for a consistent definition for efficiency in the context of public health systems to be used in practice. By consolidating the range of definitions identified through this study, we propose the following definition: the optimal use of resources to maximize and balance clinical, cost and experience outcomes.
With EI recognized as an integral component in addressing the challenge of meeting increasing demand for outcomes with limited resources, the generation and application of evidence to identify and implement EI approaches which have proven to be successful is likely to be a key enabling factor.3,12 Public health systems and organisations internationally can establish EI as a strategic and operational priority by embedding a focus on efficiency in strategic plans, performance management frameworks and service agreements.16,20 This can be extended to including EI-specific funding levers such as incentivization and grants, which can support organisations to direct resources and service delivery towards more efficient activities and away from less-efficiency and lower-value activities.82 Public health organisations seeking to establish EI as a strategic priority can consider these approaches as tools to motivate and manage towards change, using system management instruments such as service level agreements, budget structures and performance management frameworks to implement change.
In addition to setting strategic, funding and performance management priorities for EI, this study identified three additional themes for supporting EI across the public health systems. These were providing data and analytics to enable EI, develop staff capability and skills for EI and generate evidence for EI. These three themes are closely linked and mutually supportive for two reasons. Firstly, developing and sharing EI knowledge, data and evidence in a digitally enabled manner can facilitate the use of this information across the system or organisation, allowing replication and scaling of successful approaches. Secondly, this can be further promoted by investing in developing the capability of staff at all levels across the organisation to understand, engage with and lead EI work using data and evidence as key enablers. As staff engagement with EI is a key factor in EI success, equipping staff with the skills, information and evidence to drive EI will be a key determinant of EI performance.8,83 Specific digital health and workforce plans can set out key timelines and actions to deliver this support. These enabling factors can support public health systems to achieve sustainable efficiency improvements which also improve service quality and stakeholder experience.74
Although the structure of health systems varies internationally, the imperatives to improve value, respond to increasing demand pressures and ensure capacity for reform by maximizing outcomes achieved for resources invested are shared across many public health systems.3 This comes with a caveat, as performance measures for outcomes are in their infancy and are likely to vary across systems.44,71 As each public health system sets out its strategic planning and governance documents according to its unique structural, funding and service delivery requirements, the approaches identified in this study may be used to inform specific approaches for EI which may be included in these documents. The approaches to whole-of-system EI identified in this study are likely to be highly transferable across health systems internationally with the key themes of funding levers, digital enablement and workforce capability development being widely established areas of practice.8 The importance of building and applying evidence for EI approaches specific to the unique attributes of international health systems will support EI success at a local level.13
Conclusions
This study addresses the gap in evidence regarding the efficiency-specific content and tools to support EI practice identified in the strategic plans and system management frameworks of Australian public health systems. It is evident that efficiency is commonly held as a strategic and operational priority across Australian public health systems, with efficiency-specific directions identified in the system-level plans and frameworks from 18 of 21 organisations included in this study. While significant variation in individual definitions of efficiency was noted, most definitions related to the use of resources to deliver services and outcomes. This provides further evidence of the role of efficiency within the current focus on value.
Health systems can establish improving efficiency as a whole-of-system priority through the inclusion of efficiency aims and performance targets within strategic plans and performance management processes. The use of funding levers such as incentives and grants, as well as the provision of cost-effective resource and information management processes can, be used to direct efforts towards specific outcomes, enable change and reduce waste. Health systems can enable their workforces to understand and work towards improved efficiency by developing skills and capabilities and by providing data and analytics to identify opportunities, support decisions and measure impact. Investing in the generation and application of evidence for approaches which improve efficiency can allow public health organisations to benefit from learnings and experience to drive future improvements. Through deliberate, well-supported and clearly articulated EI initiatives, public health systems can support the maximization of outcomes and value achieved for resources invested.
Ethics and Data Sharing Statements
This research did not require review or approval by an institutional review board or ethics committee as all information used in this research was publicly available.
Acknowledgments
This research was supported by an Australian Government Research Training Program Scholarship. This research was undertaken as a part of a Doctor of Public Health degree at the University of New South Wales, jointly supervised by A/Prof Anurag Sharma and A/Prof Reema Harrison.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Mr James Kenneth Walters reports non-financial support from NSW Health, during the conduct of the study and financial support from HealthShare NSW to meet the Article Processing Charge for publication of this work. The authors report no other conflicts of interest in this work.
References
1. Blank JL, Eggink E. The impact of policy on hospital productivity: a time series analysis of Dutch hospitals. Health Care Manag Sci. 2014;17(2):139–149. doi:10.1007/s10729-013-9257-8
2. Ellen ME, Wilson MG, Velez M, et al. Addressing overuse of health services in health systems: a critical interpretive synthesis. Health Res Policy Syst. 2018;16(1):48. doi:10.1186/s12961-018-0325-x
3. Maniatopoulos G, Hunter D, Best A. Editorial. J Health Organ Manag. 2020;34(3):233–236. doi:10.1108/JHOM-05-2020-367
4. Porter ME. Value in Health Care. N Engl J Med. 2010;363(26):2477–2481. doi:10.1056/NEJMp1011024
5. Akinci F, Patel PM. Quality improvement in healthcare delivery utilizing the patient-centered medical home model. Hosp Top. 2014;92(4):96–104. doi:10.1080/00185868.2014.968493
6. Chen KK, Harty JH, Bosco JA. It is a brave new world: alternative payment models and value creation in total joint arthroplasty: creating value for tjr, quality and cost-effectiveness programs. J Arthroplasty. 2017;32(6):1717–1719. doi:10.1016/j.arth.2017.02.013
7. Bosch X, Moreno P, Lopez-Soto A. The painful effects of the financial crisis on Spanish health care. Int J Health Serv. 2014;44(1):25–51. doi:10.2190/HS.44.1.c
8. Walters JK, Sharma A, Malica E, Harrison R. Supporting efficiency improvement in public health systems: a rapid evidence synthesis. BMC Health Serv Res. 2022;22(1):1–11. doi:10.1186/s12913-022-07694-z
9. Papanicolas I, Rajan D, Karanikolos M, Soucat A, Figueras J. Health System Performance Assessment: A Framework for Policy Analysis. Geneva: World Health Organization; 2022.
10. Koff E, Lyons N. Implementing value-based health care at scale: the NSW experience. Med J Aust. 2020;212(3):104–6 e1. doi:10.5694/mja2.50470
11. Woolcock K; Australian Healthcare and Hospitals Association. Value Based Health Care: Setting the Scene for Australia. Deeble Institute for Health Policy Research; 2019:323–325.
12. Ansmann L, Vennedy V, Hillen HA, et al. Resource dependency and strategy in healthcare organizations during a time of scarce resources: evidence from the metropolitan area of cologne. J Health Organ Manag. 2020;35(9):211–227. doi:10.1108/JHOM-12-2020-0478
13. Bennett CC. Are we there yet? A journey of health reform in Australia. Med J Aust. 2013;199(4):251–255. doi:10.5694/mja13.10839
14. Braithwaite J, Hibbert P, Blakely B, et al. Health system frameworks and performance indicators in eight countries: a comparative international analysis. SAGE Open Med. 2017;5:1–10.
15. Anstey MH, Elshaug AG, Russell LM, Wells S. Can we learn anything from health care in the United States? Med J Aust. 2014;200(9):526–528. doi:10.5694/mja13.11357
16. Zhang X, Tone K, Lu Y. Impact of the local public hospital reform on the efficiency of medium-sized hospitals in japan: an improved slacks-based measure data envelopment analysis approach. Health Serv Res. 2018;53(2):896–918. doi:10.1111/1475-6773.12676
17. Harris C, Green S, Elshaug AG. Sustainability in health care by allocating resources effectively (share) 10: operationalising disinvestment in a conceptual framework for resource allocation. BMC Health Serv Res. 2017;17(1):632. doi:10.1186/s12913-017-2506-7
18. Allin S, Grignon M, Wang L. The determinants of efficiency in the Canadian health care system. Health Econ Policy Law. 2016;11(1):39–65. doi:10.1017/S1744133115000274
19. Department of Health. Addendum to National Health Reform Agreement 2020–25. Canberra: Commonwealth of Australia; 2020.
20. Anderson T, Catchlove B. Health and hospital reform in Australia -a local health district’s perspective. World Hosp Health Serv. 2012;48(3):21.
21. Bowen GA. Document analysis as a qualitative research method. Qual Res J. 2009;9(2):27–40. doi:10.3316/QRJ0902027
22. Dalgish SL, Khalid H, McMahon SA. Document analysis in health policy research: the READ approach. Health Policy Plan. 2020;25(10):1424–1431.
23. Chauhan A, Walpola RL, Manias E, et al. How do health services engage culturally and linguistically diverse consumers? An analysis of consumer engagement frameworks in Australia. Health Expect. 2021;24(5):1747–1762. doi:10.1111/hex.13315
24. Altheide DL. Qualitative Media Analysis. Thousand Oaks, CA: SAGE Publications Inc; 1996.
25. Esbati A, Barnes M, Henderson A, Legislation TJ. Policies and guidelines related to breastfeeding and the baby friendly health initiative in Australia: a document analysis. Aust Health Rev. 2018;44(4):72–81. doi:10.1071/AH16067
26. O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
27. Popay J, Roberts H, Sowden A, et al.Guidance on the conduct of narrative synthesis in systematic reviews: a product from the ESRC methods programme. Lancaster University. 2006;1:b9
28. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
29. NSW Agency for Clinical Innovation. Understanding Program Evaluation: An ACI Framework 2013.2013. Sydney (AU): AIHW.
30. NSW Agency for Clinical Innovation. Understanding the Use of Health Economics: An ACI Framework. Sydney (AU); 2014.
31. NSW Agency for Clinical Innovation. Knowledge Management: An ACI Approach. Sydney (AU): ACI; 2013.
32. ACT Health. ACT Health Directorate Strategic Plan 2020–25. Canberra (AU): ACT Health; 2019.
33. ACT Health. ACT Health Governance Framework 2018–2023. Canberra (AU): ACT Health; 2018.
34. Australian Digital Health Agency. Australia’s National Digital Health Strategy. Canberra (AU): ADHA; 2017.
35. Australian Department of Health. Addendum to National Health Reform Agreement 2020–2025. Canberra (AU): ADH; 2020.
36. Independent Hospital Pricing Authority. Pricing Framework for Australian Public Hospital Services 2022–23. Sydney (AU): IHPA; 2021.
37. NSW Health Clinical Excellence Commission. Healthcare Safety and Quality Capabilities. Sydney (AU): CEC; 2021.
38. NSW Health. NSW Health Analytics Framework. Sydney (AU): NSW Health; 2016.
39. NSW Health. eHealth Strategy for NSW Health 2016–2026. Sydney (AU): eHealth NSW; 2016.
40. Healthshare. HealthShare Strategic Plan 2020-2024. Sydney (AU): Healthshare; 2020.
41. NSW Health. NSW Health Commissioning for Better Value Strategy 2021-24. Sydney (AU): NSW Health; 2021.
42. NSW Health. Financial Requirements and Conditions of Subsidy (Government Grants). Sydney (AU): NSW Health; 2021.
43. NSW Health. NSW Framework for New Health Technologies and Specialised Services. Sydney (AU): NSW Health; 2018.
44. NSW Health. Future Health: Guiding the Next Decade of Care in NSW 2022-2032. Sydney (AU): NSW Health; 2022.
45. NSW Health. Health Professionals Workforce Plan 2012-2022 Revised 2015. Sydney (AU): NSW Health; 2015.
46. NSW Health. Resource Efficiency Strategy 2016 to 2023. Sydney (AU): NSW Health; 2016.
47. NSW Health. Corporate Governance & Accountability Compendium- Section 7 Finance. Sydney (AU): NSW Health; 2019.
48. Northern Territory Health. NT Health Workforce Strategy 2019 - 2022. Darwin (AU): NT Health; 2019.
49. Northern Territory Health. Strategic Plan 2018-2022. Darwin (AU): NT Health; 2018.
50. Northern Territory Health. Service Plan 2021-22: NT Regional Health Services Plan. Darwin (AU): NT Health; 2021.
51. Northern Territory Health. Service Plan 2021-2022: Performance Framework. Darwin (AU): NT Health; 2021.
52. Queensland Health. Optimising the Allied Health Workforce for Best Care and Best Value. Brisbane (AU): QLD Health; 2019.
53. Queensland Health. Destination 2030: Great Care for Central Queenslanders. Brisbane (AU): QLD Health; 2017.
54. Queensland Health. Queensland Health Performance and Accountability Framework 2020-2021. Brisbane (AU): QLD Health; 2020.
55. Queensland Health. System Outlook to 2026 for a Sustainable Health Service. Brisbane (AU): QLD Health; 2016.
56. Queensland Health. Digital Health 2031: A Digital Vision for Queensland’s Health System. Brisbane (AU): QLD Health; 2021.
57. South Australia Health. SA Health Performance Framework. Adelaide (AU): SA Health; 2021.
58. South Australia Health. State Public Health Plan 2019-2024. Adelaide (AU): SA Health; 2018.
59. Tasmanian Department of Health. Digital Health Transformation – Improving Patient Outcomes. Hobart (AU): Tas Health; 2022.
60. Tasmanian Department of Health. Health Workforce. Hobart (AU): Tas Health; 2021.
61. Tasmanian Department of Health. Tasmanian Health Service 2020-21 Service Plan (May 2021 Amendment). Hobart (AU): Tas Health; 2021.
62. Victoria Health and Human Services. Decision Making Framework for Funding Policy. Melbourne (AU): Vic HHS; 2016.
63. Victoria Health and Human Services. Policy and Funding Guidelines 2020–21 Policy Guide. Melbourne (AU): Vic HHS; 2020.
64. Victoria Health and Human Services. CAPABILITY for INNOVATION and IMPROVEMENT STRATEGY 2017–20. Melbourne (AU): Vic HHS; 2017.
65. Victoria Health and Human Services. Victorian Health Services Performance Monitoring Framework 2019–20. Melbourne (AU): Vic HHS; 2019.
66. Western Australia Department of Health. Clinical Services Framework 2020 Addendum. Perth (AU): WA DoH; 2021.
67. Western Australia Department of Health. Key Performance Indicators (KPIs) and Targets. Perth (AU): WA DoH; 2021.
68. Western Australia Department of Health. Better Health, Better Care, Better Value WA Health Reform Program 2015–2020. Perth (AU): WA DoH; 2015.
69. Australian Health Research Alliance. National Framework for Health Systems Improvement and Sustainability. Sydney (AU): AHRA; 2018.
70. Grattan Institute. Incentives for Efficiency. Carlton (AU): GI; 2021.
71. Australian Government Productivity Commission. Efficiency in Health. Canberra (AU): AGPC; 2015.
72. NSW Agency for Clinical Innovation. Understanding the Use of Health Economics: An ACI Framework. Sydney (AU): ACI; 2013.
73. Medicine Io. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: The National Press; 2001
74. Akinleye DD, McNutt L, VLazariu V, McLaughlin CC. Correlation between hospital finances and quality and safety of patient care. PLoS One. 2019;14(8):e0219124. doi:10.1371/journal.pone.0219124
75. Hassanain M. An Overview of the Performance Improvement Initiatives by the Ministry of Health in the Kingdom of Saudi Arabia. Inquiry. 2017;54:46958017707872. doi:10.1177/0046958017707872
76. Elshaug AG, Rosenthal MB, Lavis JN, et al. Levers for addressing medical underuse and overuse: achieving high-value health care. Lancet. 2017;390(10090):191–202. doi:10.1016/S0140-6736(16)32586-7
77. Schakel HC, Wu EH, Jeurissen P. Fiscal rules, powerful levers for controlling the health budget? Evidence from 32 OECD countries. BMC Public Health. 2018;18(1):300. doi:10.1186/s12889-018-5198-y
78. Elshaug AG, Moss JR, Tunis SR, Hiller JE. Challenges in Australian policy processes for disinvestment from existing, ineffective health care practices. Australia and New Zealand health policy. Aust New Zeal Health Pol. 2007;4(1):23–30
79. Wolfenden L, Bolsewicz K, Grady A, et al. Optimisation: defining and exploring a concept to enhance the impact of public health initiatives. Health Res Policy Syst. 2019;17(108):doi:10.1186/s12961-019-0502-6
80. Gans D, Kominski GF, Roby DH, et al. Better Outcomes, Lower Costs: Palliative Care Program Reduces Stress, Costs of Care for Children with Life-Threatening Conditions. UCLA Center for Health Policy Research; 2012.
81. Ament SMC, Gillissen F, Moser A, et al. Factors associated with sustainability of 2 quality improvement programs after achieving early implementation success. A qualitative case study. J Eval Clin Pract. 2017;23(6):1135–1143. doi:10.1111/jep.12735
82. Kamarainen VJ, Peltokorpi A, Torkki P, Tallbacka K. Measuring healthcare productivity - from unit to system level. Int J Health Care Qual Assur. 2016;29(3):288–299. doi:10.1108/IJHCQA-04-2015-0050
83. Allin S, Veillard J, Wang L, Grignon M. How can health system efficiency be improved in Canada? Healthcare Policy. 2015;11(1):33.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.