")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 16
Adverse Impact of Systemic Lupus Erythematosus on Pregnancy Outcomes: A Saudi Arabia Retrospective Multi-Center Study
Authors Al Rayes H, AlOudah N, Alsolaimani R, Alharthi A, Attar M, Daghasi H, Albeity A , Afifi AM, AlQahtani A, Alkaff A, Alkhamesi SM, Elnady B
Received 4 November 2023
Accepted for publication 26 January 2024
Published 1 February 2024 Volume 2024:16 Pages 31—41
DOI https://doi.org/10.2147/OARRR.S448186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Hanan Al Rayes,1 Norah AlOudah,1 Roaa Alsolaimani,2,3 Abdulrahman Alharthi,4 Mohammed Attar,4 Hassan Daghasi,4 Abdurahman Albeity,2 Afnan M Afifi,2 Abdulelah AlQahtani,1 Alya Alkaff,5 Sultan M Alkhamesi,3 Basant Elnady4,6
1Department of Rheumatology, Prince Sultan Military Medical City, Riyadh, Saudi Arabia; 2Department of Medicine, King Faisal Specialist Hospital and Research Center, Jeddah, Saudi Arabia; 3Department of Medicine, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 4Department of Rheumatology, Al Hada Armed Forces Hospital, Taif, Saudi Arabia; 5Obstetrics and Gynecology Department, King Faisal Specialist Hospital, and Research Center, Jeddah, Saudi Arabia; 6Rheumatology and Rehabilitation Department, Faculty of Medicine, Benha University, Benha, Egypt
Correspondence: Basant Elnady, Tel +966562387723, Email [email protected]
Objective: The current study aimed to determine the pregnancy outcomes complications in patients with SLE and its association with clinical, laboratory variables, disease activity, and medication use in the Saudi population, as well as pregnancy effect on disease activity.
Methods: A multicenter study included pregnant female patients with Systemic Lupus Erythematosus (SLE) from three tertiary centers in Saudi Arabia. The demographics, clinical, and laboratory variables, SLE disease activity index (SLEDAI), medication before, during, and after pregnancy, planned pregnancy, pregnancy-related outcomes, and complications in comparison to age-matched healthy female controls were noted.
Results: A total of 66 pregnant patients with SLE and 93 healthy age-matched pregnant controls were included in the study. A total of 77.3% had SLEDAI-2K ≤ 4 before conception, and 84.85% of pregnancies were planned. Age of conception, cesarean section, miscarriage, and low birth weight were statistically significant (p < 0.05) higher in SLE patients than in healthy controls. Among all clinical and laboratory variables, SLEDAI-2K > 4 and active lupus nephritis during pregnancy were statistically associated with adverse outcomes (p < 0.05), history of lupus nephritis was not associated with statistically adverse pregnancy outcomes. Higher SLEDAI-2K > 4 was an independent risk at least 4.87 times higher association with adverse pregnancy outcomes. (p < 0.05).
Conclusion: SLE is intricately connected with unfavorable pregnancy outcomes. The preconception of high disease activity stands as a pivotal risk factor for adverse outcomes. Despite the disease remission and meticulous planning, SLE patients frequently grapple with disease exacerbations during pregnancy, culminating in unexpected and unfavorable pregnancy-related outcomes. This underscores the intricate and multifaceted nature of managing SLE during gestation.
Keywords: systemic lupus erythematosus, pregnancy, disease activity
Introduction
Multisystemic autoimmune illness Systemic Lupus Erythematosus (SLE) typically affects females of reproductive age. Pregnancy is a popular concern for individuals with SLE since these women have a normal reproductive rate.1 SLE and pregnancy have mutually harmful effects. In addition to having short- or long-term negative effects on renal function, pregnancy may also enhance the activity of SLE, and can cause difficulties during pregnancy, such as preeclampsia, premature labor, and fetal death, and it can also enhance the activity of the condition. Pregnancy may also have short- or long-term negative effects on renal function.2
High SLE disease activity, as assessed by the SLEDAI during the six months preceding pregnancy, predicted unfavorable maternal and fetal outcomes, such as a flare-up during pregnancy or pre-eclampsia.3 Additionally, results from population-based cohort research revealed a higher risk for fetal problems in SLE pregnancies compared to controls, typically in individuals with an active illness.4 SLE patients have a greater chance of developing pre-eclampsia or eclampsia than people in the general community.5 Prednisone use and the presence of disease-related characteristics including lupus nephritis, and positive anti-phospholipid antibodies are all linked to an elevated risk for pre-eclampsia, according to several studies.6–9 However, there may be inconsistencies in the results produced due to methodological variations and the use of different sample sizes. The likelihood of a lupus flare during pregnancy depends on how active the condition was at the time of conception. While 61–67% of patients with active SLE at the beginning of pregnancy experienced a disease flare, the incidence of flare has been found to range from 7 to 33% in women whose SLE was in remission for at least 6 months before conception. Researchers disagree on whether greater lupus activity is caused by pregnancy or by the illness changing spontaneously.10–12
Despite this, several studies have demonstrated that SLE causes adverse pregnancy outcomes; the diverse results and causes of these difficulties appear to vary from place to region. This study aims to assess characteristics related to pregnancy outcomes in patients with systemic lupus erythematosus (SLE), the primary aim was to evaluate the impact of SLE on pregnancy, namely the obstetric problems and fetal outcomes. The secondary goal was to evaluate how disease activity (as measured by SLEDAI), medications including prednisolone, clinical as well as laboratory characteristics, and planned pregnancy affected the outcome of the pregnancy. Finally, the effect of pregnancy on the disease activity as well.
Patients and Methods
The current study was carried out in three tertiary facilities in Saudi Arabia: Al-Hada Armed Forces Hospital located in Taif, Prince Sultan Military Medical City (PSMMC) in Riyadh, and King Faisal Specialist Hospital and Research Center in Jeddah. This was a multicenter case-control retrospective research in the Saudi population in contrast to healthy, age-matched pregnant women. The primary objective of the study was to assess the influence of Systemic Lupus Erythematosus (SLE) on pregnancy, specifically examining obstetric complications and fetal outcomes. A secondary aim was to analyze the impact of various factors, including disease activity measured by the SLE Disease Activity Index (SLEDAI), medications, clinical and laboratory characteristics, and planned pregnancy, on the overall pregnancy outcomes. Additionally, the study aimed to investigate the reciprocal effect of pregnancy on disease activity in individuals with SLE.
Study Population
Three tertiary hospitals provided data on patients with SLE who were being followed up in the rheumatology clinics between November 2019 and November 2022. The following inclusion criteria were met by participants: Pregnant females over the age of 18, fulfilling the American College of Rheumatology (ACR) SLE criteria 1997,13 having regular follow-up visits in a rheumatology clinic at least every 3–4 months. Age-matched healthy pregnant women were the only controls who met the inclusion criteria.
Incomplete file for the needed datasets and variables, Twin pregnancies, known to have diabetes mellitus, hypertension, chronic renal disease, ovarian surgery, uterine anomalies, prior chemotherapeutic treatment for ectopic pregnancy, and exposure to known or suspected ovary-toxic drugs at least six months before conception were excluded from the study.
Methods
Electronic medical records have been revised for SLE patients who had got pregnant as well as healthy control pregnant females, data for participants in both groups were extracted for clinical and laboratory variables. Data from the clinic visits determined whether the pregnancy was planned by the patient and the rheumatologist and whether medication modification was done or the pregnancy happened spontaneously. The patient-physician planned protocol was defined as prior disease activity control and medication adjustment before conception.
Clinical and laboratory data, demographics, past medical history, and treatments were all gathered for SLE patients using a standardized, automated, and electronically filled form. Laboratory data including anti-nuclear antibodies (ANA) were determined by IIF on HEp-2, anti-double strand DNA (anti-DNA) with IIF on Crithidia luciliae, anti-Ro/SSA, anti-La/SSB, analyzed by ELISA considering titers above the cut-off of the reference laboratory, Beta 2 Glycoprotein 1 (B2GP1), and anticardiolipin (aCL) antibodies (IgG/IgM isotype), analyzed by ELISA, in serum (above the 99th percentile), and LA, according to the guidelines.14 C3 and C4 serum levels were determined as well by nephelometry.
The outcomes of pregnancy in both groups were recorded, including new-onset hypertension, gestational diabetes, and other associated comorbidities, mode of delivery, and miscarriage. Premature birth is described as a delivery that takes place between 20 and 37 weeks during the pregnancy and is referred to as preterm or premature birth.15 Low birth weight (LBW),16 congenital abnormalities, NICU hospitalization, stillbirth, and live birth were among the fetal outcomes. The gestational age was determined for each live birth, and any congenital abnormalities as well as heart block and neonatal lupus were noted.
Disease activity measurement using the SLEDAI-2K. SLEDAI-2K ≤ 4 is considered an inactive disease,17 We chose a sample with at least four measurements of disease activity assessments throughout pregnancy in order to analyze the pattern of lupus during pregnancy. The first within six months before conception, at least one measurement throughout the first and second trimesters, one measurement during the third trimester, and lastly one measurement during the six-month puerperium. Disease activity with new onset lupus nephritis during pregnancy and/or another major organ affected was reported as well. Medications including steroids and immunosuppressive medications were registered both before, during, and after pregnancy.
Ethical Approvals
This study complied with the Declaration of Helsinki and was approved by the local ethics research committee of Al-Hada Armed Forces Hospital located in Taif, Prince Sultan Military Medical City (PSMMC) in Riyadh, and King Faisal Specialist Hospital and Research Center in Jeddah.
Patients were consented to review their medical records. Patients or the public were not involved in the design, conduct, reporting, or dissemination plans of our research.
Statistical Analysis
Descriptive statistics were summarized as numbers and percentages for all categorical variables while mean and standard deviation were used to present all continuous variables. Between comparisons, an independent sample t-test and Fischer Exact test were applied. Based on the significant results, a univariate regression analysis was subsequently performed to determine the independent significant factor associated with SLE pregnancy-related outcomes with odds ratio as well as 95% confidence also being reported. Normality test has been conducted using the Shapiro–Wilk test and Kolmogorov–Smirnov test. The calculated study power was 0.926, which is adequate considering the cutoff point of 0.8. A P-value of less than 0.05 was considered statistically significant. The data were analyzed using Statistical Packages for Social Sciences (SPSS) version 26 (Armonk, NY: IBM Corp, USA).
Results
A total of 66 pregnant patients with SLE and 93 healthy age-matched pregnant controls were included in the study. As seen in Table 1, the patients’ mean ages during pregnancy was 35 (SD 4.98) years old while the mean age at disease onset was 26.2 (SD 4.73) years old. The mean duration of the disease was 6.79 (SD 4.88) years. Hypothyroidism was diagnosed in 21.2% of the patients. Post-kidney transplant and Sjogren syndrome were detected in one patient each. Prednisolone used before and during pregnancy has been reported by 60.6% and 68.2% of patients, respectively. 13.6% with positive B2GP1. One patient had lupus anticoagulation. ACL, anti-DNA, SSA, and SSB were positive in 10.6%, 37.9%, 36.4%, and 15.2%, respectively. 84.8% had planned pregnancies. A total of 51(77.3%) had SLEDAI-2K ≤ 4 before conception however 15 (22.7%) patients had SLEDAI-2K > 4. DMARDs used during pregnancy were reported by 86.4%. The most common DMARDs medication was hydroxychloroquine (HCQ) 57 (86.4%) and azathioprine 18 (27.3%).
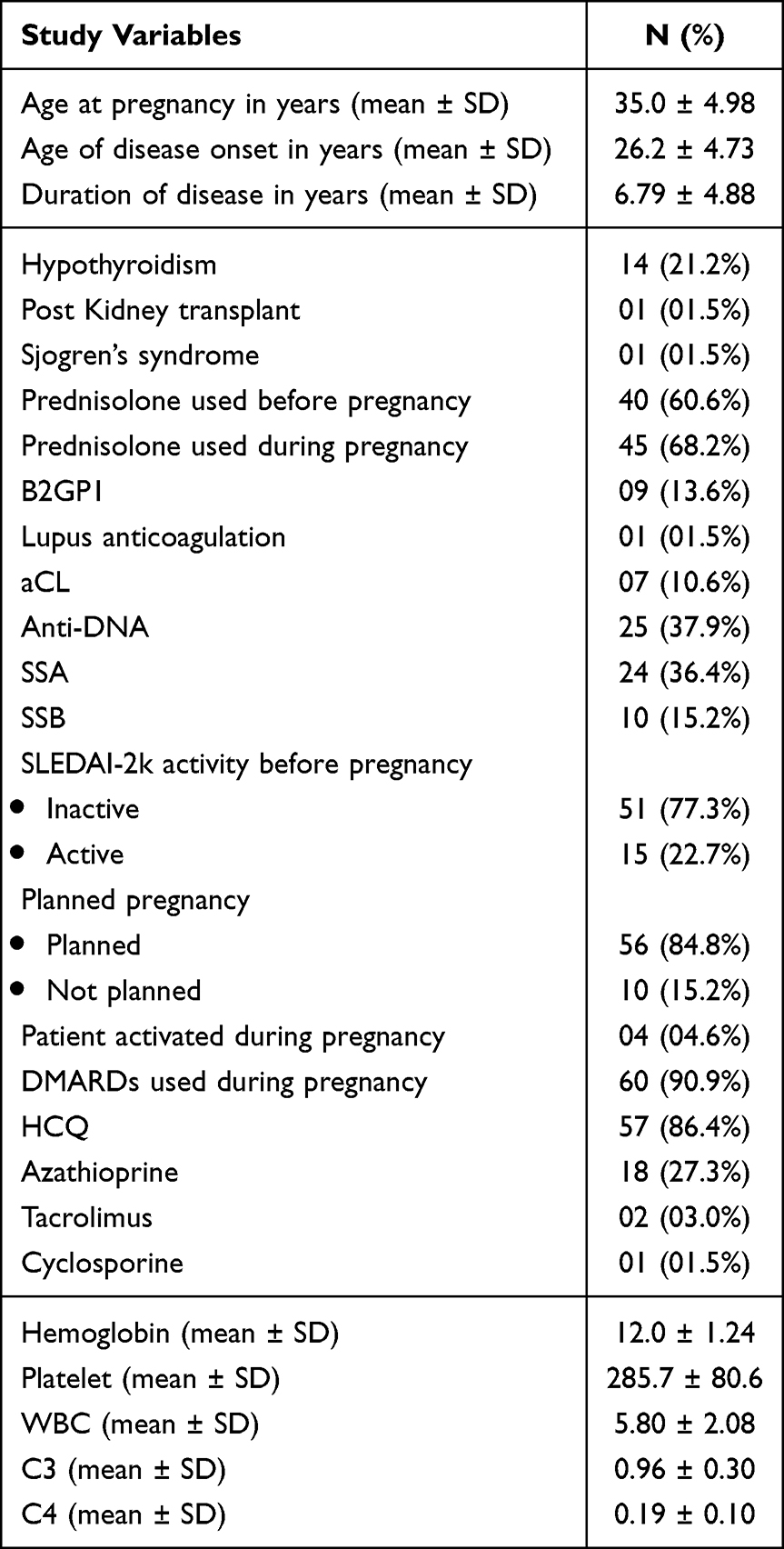 |
Table 1 Baseline and Clinical Characteristics of Patients with Systemic Lupus (n=66) |
The maternal adverse outcomes in our SLE patients, ranked from highest to lowest percentage, included miscarriage (16.7%), preeclampsia (7.6%), hypertension (4.5%), pregnancy gestational diabetes (4.5%), and post-partum hemorrhage (1.5%). Among these outcomes, 79% of pregnancies were planned.
For fetal-related adverse outcomes in our SLE patients, the percentages, from highest to lowest, were as follows: low birth weight (22.7%), preterm birth (15.2%), NICU admission (7.6%), congenital anomalies (6.1%), and stillbirth (3.0%). Among these outcomes, 69.6% of pregnancies were planned.
Older age of conception, cesarean section, miscarriage, and low birth weight were statistically significant (p <0.05) higher in SLE patients rather than in healthy controls, however live birth was statistically higher in the control group (Table 2).
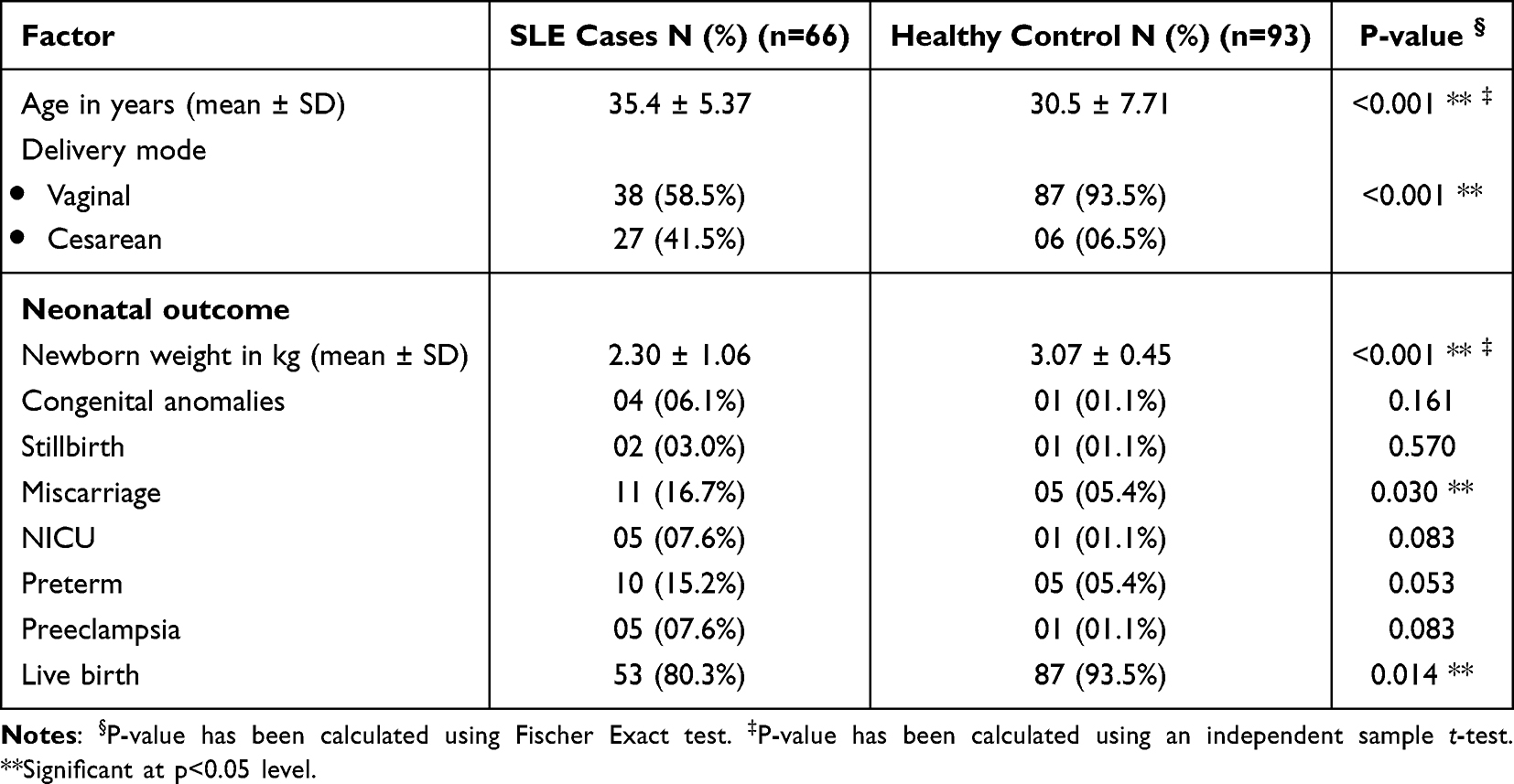 |
Table 2 Comparison Between Pregnancy SLE Group and Healthy Control Group |
In Table 3, Pregnancy adverse-related outcomes were significantly more associated with having currently active lupus nephritis (p=0.026) and those with active SLEDAI-2K activity before pregnancy (p=0.017). No significant relationships were observed between the adverse pregnancy-related outcome in terms of disease duration, age at pregnancy, SLE manifestation, hypothyroidism, history of lupus nephritis, SLEDAI-2K activity during pregnancy, planned pregnancy, prednisolone used before or during pregnancy, DMARDS medication before or during pregnancy, hemoglobin before or after pregnancy, white blood cells |(WBC) before or after pregnancy, C3 before or after pregnancy, C4 before or after pregnancy, 24 hours protein before or after pregnancy, erythrocyte sedimentation rate (ESR) before or after pregnancy, C-reactive protein (CRP) before or after pregnancy, anti-DNA, aCL, lupus anticoagulation, anti-SSA, anti-SSB, and anti-SSA/anti-SSB (all p>0.05), thrombocytopenia was not included as all patients platelets were >150.
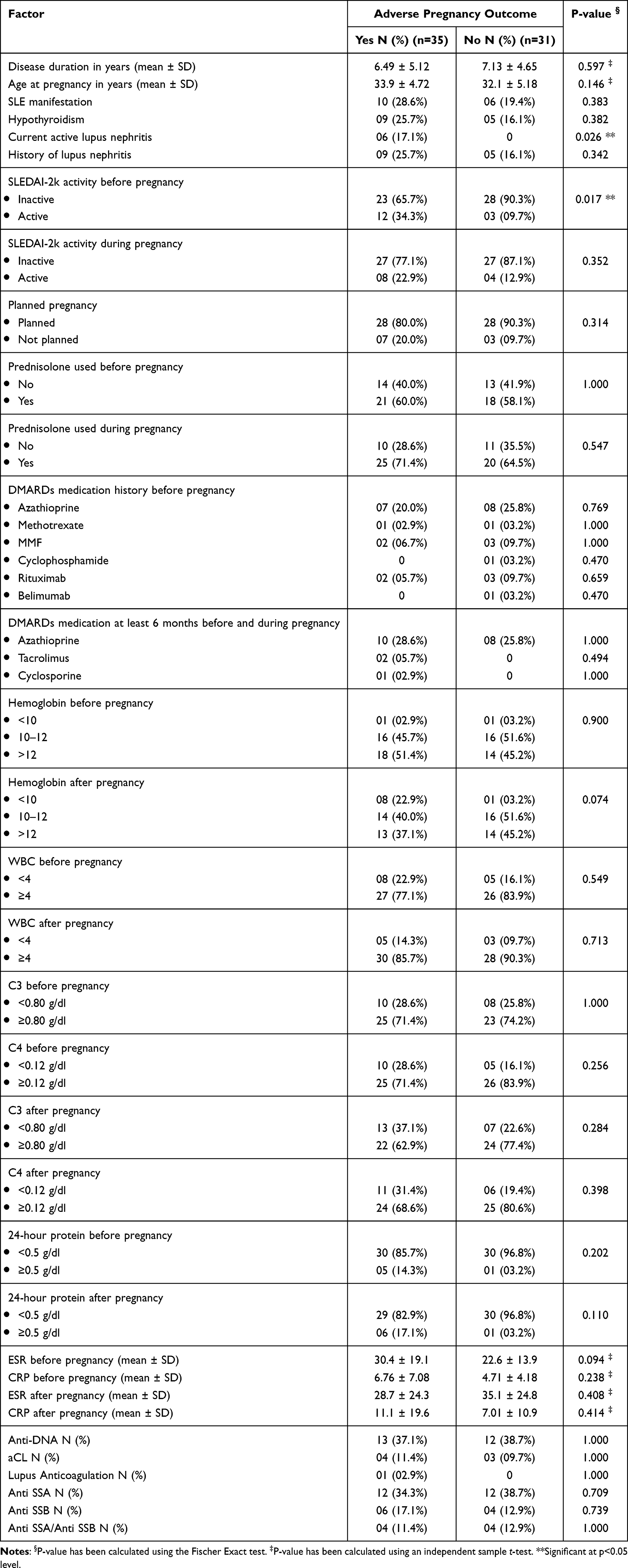 |
Table 3 Relationship Between Clinical Variables and SLE Pregnancy-Related Outcome (n=66) |
In a univariate regression model, active SLEDAI-2k was predicted to increase the risk of having pregnancy adverse-related outcomes by at least 4.87 times higher (OR=4.870; 95% CI=1.225–19.359; p=0.025) as shown in Table 4.
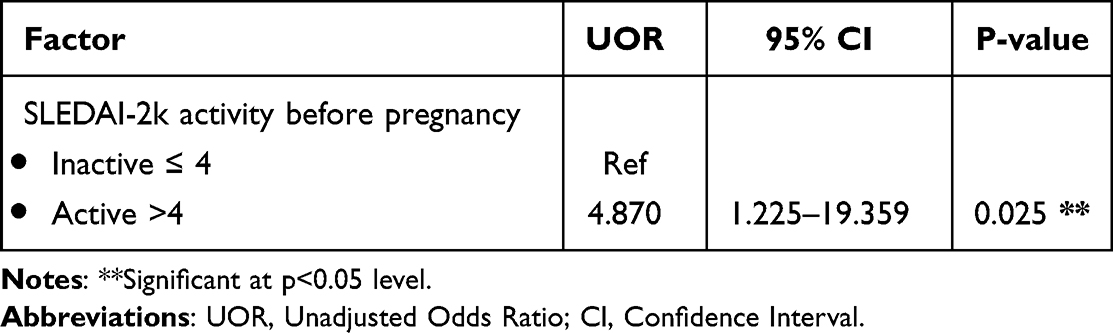 |
Table 4 Multivariate Regression Analysis for the Independent Significant Predictor of SLE Adverse Pregnancy-Related Outcome (n=66) |
In Figure 1, it was revealed that active cases were higher postpartum (45.5%), followed by 3rd trimester (37.9%) and 1st to 2nd trimester (36.4%). Paired t-test indicates that there was a significant difference in SLEDAI-2K disease activity before pregnancy and 9 months of follow-up (p=0.025).
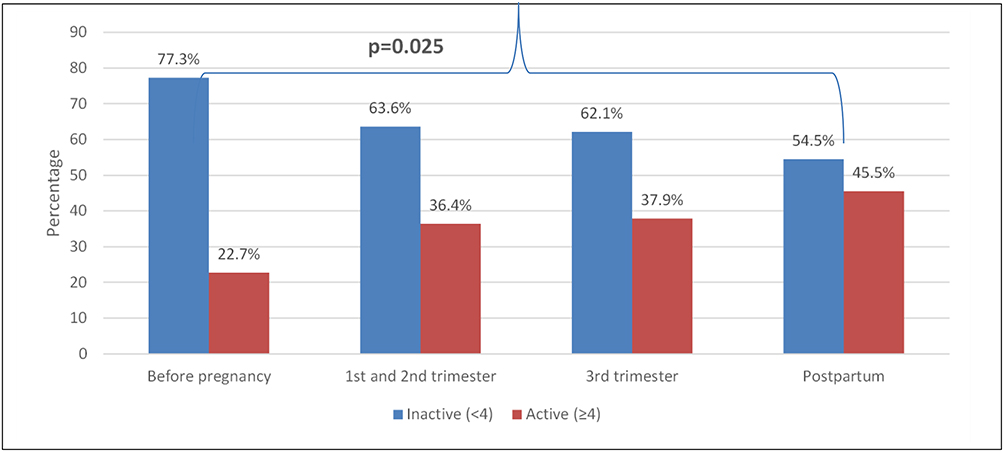 |
Figure 1 Trend of SLEDAI-2k disease activity before pregnancy to 9 months of follow-up. |
Discussion
Systemic lupus erythematosus is an established risk factor for increasing fetal and maternal morbidity and mortality.4 Additionally, pregnancy can exacerbate lupus flares. Several studies have shown that the presence of SLE can negatively impact the outcome of pregnancy, particularly in patients who have active disease.18,19 The development of SLE treatment options and a better perception of pregnancy-lupus interactions drastically improved pregnancy outcomes. Nevertheless, complications may occur as suggested by multiple studies.4,18
The majority of pregnancies in this study were planned pregnancies (84.8%). Most of the patients 77.3% have inactive disease based on SLEDAI-2K prior to conception. In contrast, 22.7% of patients had active disease with SLEDAI-2K > 4.
In this study, we confirmed that pregnancy-related complications are substantially increased among SLE patients compared to the control group. In concordance with the previous studies field,19,20 Likewise, a retrospective cohort investigation that assessed adverse pregnancy outcomes in both healthy control pregnancies and pregnancies affected by Systemic Lupus Erythematosus (SLE) concluded that pregnancies associated with SLE, even in cases marked by uncomplicated conditions and remission, exhibited pregnancy adverse outcomes.21
We agreed with Mehta et al, that patients with SLE have older age at conception,18 Moreover, the SLE group was associated with low birth weight, a higher percentage of miscarriages, a higher rate of caesarian delivery, and significantly fewer live births compared to the control group. Nevertheless, no statistical significance was found regarding congenital anomalies, stillbirth, NICU admissions, preterm and preeclampsia. The presence of lupus nephritis plays a major role in adverse pregnancy and fetal outcomes.4,18,20,22 Previous studies have established the association between active lupus nephritis and adverse pregnancy outcomes mainly fetal losses, premature birth, and maternal hypertension, whereas inactive lupus nephritis history did not adversely affect pregnancy outcomes,8,23–26 our study supports that. The present study demonstrates that patients who had developed active lupus nephritis during pregnancy developed pregnancy complications. Our study confirmed that active lupus nephritis plays a causal role in the increased rate of SLE-related fetal losses and quiescence of renal disease should be obtained prior to conception.27 Pregnancy-related physiological and hormonal changes can cause lupus activity, additionally, a lupus flare’s heightened inflammatory response might seriously complicate pregnancy,28 this is confirmed in our study which revealed that active cases were higher postpartum (45.5%), followed by 3rd trimester (37.9%) and 1st to 2nd trimester (36.4%). A paired t-test indicates that there was a significant difference in SLEDAI-2K disease activity before pregnancy and 9 months of follow-up.
It has been proposed that adverse pregnancy outcomes in SLE patients especially fetal losses were related to hypocomplementemia particularly C3, antiphospholipid antibodies, and pre-pregnancy hypertension.26,29 Similar findings were reported in a meta-analysis conducted by Smyth et al that patients with antiphospholipid antibodies/antiphospholipid syndrome are at higher risk for maternal hypertension and premature birth.8 A previous study showed that the presence of aPL antibodies in patients with SLE significantly affected the rate of pregnancy loss compared to patients without aPL with no effect of hypocomplementemia on pregnancy outcome.30 However, in the present study, there was no significant correlation between hypocomplementemia, aCL antibodies, lupus anticoagulant, and poor pregnancy consequences, this could be justified as the majority of our patients were having diseases controlled and planned with the use of Aspirin (ASA) and antithrombotic therapies in APS patients, this was in agreement with in Kim et al20 study and others,27,31 who mentioned that unfavorable pregnancy outcome was not independently associated with an aPL test result. Given that we effectively addressed the presence of aPL with ASA or low molecular weight heparin, this may be explained by the universal agreement about the value of antithrombotic prophylaxis.
A higher SLEDAI-2K prior to conception was significantly associated with an adverse outcome, nevertheless, current active lupus nephritis was associated with adverse pregnancy outcome but was not identified as an independent risk factor. Univariate regression model, Patients with baseline active SLEDAI-2k were predicted to increase the risk of having pregnancy adverse-related outcomes by at least 4.87 times higher (OR=4.870; 95% CI=1.225–19.359; p=0.025) comparable to Kim et al, the risk increases 4.61 times higher in active SLEDAI-2k (OR=4.61; 95% CI=2.08–10.23; p<0.001).20
Regarding the treatment options, we found no difference in medication used and prednisolone use prior to and during pregnancy, our patients who were using prednisolone before conception were 59% their doses were 5mg, and only 4 patients were on 10 mg. This was in concordance with a recent investigation addressing a mean CS dosage of less than 6 mg/day of prednisone-equivalent during pregnancy was a suitable amount to lower maternal and fetal risk, but they mentioned a history of CYC therapy more likely to develop negative maternal outcomes20 this could be attributed to the number of recruited patients with previous CYC use in our study only 1.5% received CYC before conception however, in their study 14.7%.20
The strength of our study lies in its pioneering nature, being the first multicenter case-control study conducted in Saudi Arabia. A noteworthy feature is its multicenter approach, which provides representation from various regions across the country. Additionally, a substantial proportion of participants were in a state of remission, and their pregnancies were carefully planned. However, we acknowledge several potential limitations. One notable limitation in our study pertains to the relatively modest sample size, a constraint primarily stemming from the formidable challenges encountered in procuring comprehensive data records for inclusion; the mandated collection of complex datasets and variables. Furthermore, the datasets available to us, containing crucial study variables, exhibited a degree of intricacy that amplified the difficulties in our data collection efforts. Furthermore, the fact that SLE patients were older than the control group may be linked to the inherent nature of their disease. Lastly, the selection of the general population in tertiary centers may lead to a higher proportion of high-risk pregnancies. Therefore, we recommend further research to address these gaps and refine our understanding of the complexities surrounding SLE and its impact on pregnancy outcomes.
In conclusion, our study underscores the persistent challenge of adverse pregnancy outcomes in SLE patients, even with our improved comprehension of SLE pathophysiology and advancements in treatment. The prevalence of these outcomes remains elevated compared to the general population, emphasizing the significance of preconception disease activity as a critical risk factor. Notably, our findings reveal that disease activity has the potential to escalate during pregnancy in our patient population. Active lupus nephritis emerges as a notable contributor to increased adverse pregnancy outcomes. As a strategic approach, planned pregnancy during periods of disease inactivity, coupled with vigilant monitoring throughout gestation, emerges as the optimal goal to mitigate both fetal and maternal complications. This conclusion highlights the pressing need for more targeted interventions and personalized care in managing SLE during pregnancy.
Strengths and Limitations of This Study
- This study proposed, to medical records review of the pregnancy outcomes in Saudi patients with SLE from three large tertiary hospitals from different regions of the kingdom.
- This study uncovers unexpected challenges in the complex nature of SLE, despite meticulous planning and optimal disease management, SLE patients still experience adverse pregnancy outcomes as well as disease flares during pregnancy.
- Conception with active disease is an independent risk factor associated with a 4.8-fold increase in adverse pregnancy outcomes.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval Information, Institution(s), and Number(s)
This study complied with the Declaration of Helsinki and was approved by the local ethics research committee of Al-Hada Armed Forces Hospital located in Taif (2022-665), Prince Sultan Military Medical City (PSMMC) in Riyadh (1411), and King Faisal Specialist Hospital and Research Center in Jeddah (2023-47).
Consent for Publication
All authors participated in granting their consent for the publication of the manuscript.
Acknowledgments
The authors gratefully acknowledge the support provided by the studied hospital’s officials for facilitating the research’s administrative aspects as well as the support given by the Saudi Society of Rheumatology.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Meyer O. Making pregnancy safer for patients with lupus. Joint Bone Spine. 2004;71(3):178–182. doi:10.1016/S1297-319X(03)00155-6
2. Chen S, Sun X, Wu B, Lian X. Pregnancy in women with systemic lupus erythematosus: a retrospective study of 83 pregnancies at a single center. Int J Environ Res Public Health. 2015;12(8):9876–9888. doi:10.3390/ijerph120809876
3. Lateef A, Petri M. Systemic lupus erythematosus and pregnancy. Rheum Dis Clin North Am. 2017;43(2):215–226. doi:10.1016/j.rdc.2016.12.009
4. Kwok LW, Tam LS, Zhu T, Leung YY, Li E. Predictors of maternal and fetal outcomes in pregnancies of patients with systemic lupus erythematosus. Lupus. 2011;20(8):829–836. doi:10.1177/0961203310397967
5. Skorpen CG, Lydersen S, Gilboe IM, et al. Influence of disease activity and medications on offspring birth weight, pre-eclampsia and preterm birth in systemic lupus erythematosus: a population-based study. Ann Rheum Dis. 2018;77(2):264–269. doi:10.1136/annrheumdis-2017-211641
6. Chen YJ, Chang JC, Lai EL, et al. Maternal and perinatal outcomes of pregnancies in systemic lupus erythematosus: a nationwide population-based study. Semin Arthritis Rheum. 2020;50(3):451–457. doi:10.1016/j.semarthrit.2020.01.014
7. Simard JF, Arkema EV, Nguyen C, et al. Early-onset preeclampsia in lupus pregnancy. Paediatr Perinat Epidemiol. 2017;31(1):29–36. doi:10.1111/ppe.12332
8. Smyth A, Oliveira GH, Lahr BD, Bailey KR, Norby SM, Garovic VD. A systematic review and meta-analysis of pregnancy outcomes in patients with systemic lupus erythematosus and lupus nephritis. Clin J Am Soc Nephrol. 2010;5(11):2060. doi:10.2215/CJN.00240110
9. Abou-Nassar K, Carrier M, Ramsay T, Rodger MA. The association between antiphospholipid antibodies and placenta mediated complications: a systematic review and meta-analysis. Thromb Res. 2011;128(1):77–85. doi:10.1016/j.thromres.2011.02.006
10. Andrade R, Sanchez ML, Alarcon GS, et al. Adverse pregnancy outcomes in women with systemic lupus erythematosus from a multiethnic US cohort: LUMINA (LVI) [corrected]. Clin Exp Rheumatol. 2008;26(2):268–274.
11. Nili F, McLeod L, O’Connell C, Sutton E, McMillan D. Maternal and neonatal outcomes in pregnancies complicated by systemic lupus erythematosus: a population-based study. J Obstet Gynaecol Can. 2013;35(4):323–328. doi:10.1016/S1701-2163(15)30959-2
12. Cortés-Hernández J, Ordi-Ros J, Paredes F, Casellas M, Castillo F, Vilardell- Tarres M. Clinical predictors of fetal and maternal outcome in systemic lupus erythematosus: a prospective study of 103 pregnancies. Rheumatology. 2002;41(6):643–650. doi:10.1093/rheumatology/41.6.643
13. Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40(9):1725. doi:10.1002/art.1780400928
14. Blencowe H, Cousens S, Oestergaard M, et al. National, regional and worldwide estimates of preterm birth. Lancet. 2012;379(9832):2162–72. Estimates from 2010. doi:10.1016/S0140-6736(12)60820-4
15. American College of Obstetricians and Gynecologists. Perinatal Care at the Threshold of Viability. ACOG Practice Bulletin #38. Washington DC: American College of Obstetricians and Gynecologists; 2002.
16. Pengo V, Tripodi A, Reber G, et al. Update of the guidelines for lupus anticoagulant detection. subcommittee on lupus anticoagulant/antiphospholipid antibody of the scientific and Standardisation Committee Of The International Society On Thrombosis And Haemostasis. J Thromb Haemost. 2009;7(10):1737–1740. doi:10.1111/j.1538-7836.2009.03555.x
17. Gladman DD, Ibanez D, Urowitz MB. Systemic lupus erythematosus disease activity index 2000. J Rheumatol. 2002;29(2):288–291.
18. Mehta B, Jannat-Khah D, Glaser KK, et al. Fetal and maternal morbidity in pregnant patients with Lupus: a 10-year US nationwide analysis. RMD Open. 2023;9(1):e002752. doi:10.1136/rmdopen-2022-002752
19. Clowse MEB, Jamison M, Myers E, James AH. A national study of the complications of lupus in pregnancy. Am J Obstet Gynecol. 2008;199(2):
20. Kim JW, Jung JY, Kim HA, Yang JI, Kwak DW, Suh CH. Lupus low disease activity state achievement is important for reducing adverse outcomes in pregnant patients with systemic lupus erythematosus. J Rheumatol. 2021;48(5):707–716. doi:10.3899/jrheum.200802
21. Phansenee S, Sekararithi R, Jatavan P, Tongsong T. Pregnancy outcomes among women with systemic lupus erythematosus: a retrospective cohort study from Thailand. Lupus. 2018;27(1):158–164. doi:10.1177/0961203317721353
22. Petri M. The Hopkins lupus pregnancy center: ten key issues in management. Rheum Dis Clin North Am. 2007;33(1):33. doi:10.1016/j.rdc.2006.12.007
23. Lucas A, Eudy AM, Gladman D, et al. The association of lupus nephritis with adverse pregnancy outcomes among women with lupus in North America. Lupus. 2022;31(11):1401–1407. doi:10.1177/09612033221123251
24. Georgiou PE, Politi EN, Katsimbri P, Sakka V, Drosos AA. Outcome of lupus pregnancy: a controlled study. Rheumatology. 2000;39(9):1014–1019. doi:10.1093/rheumatology/39.9.1014
25. Gladman DD, Tandon A, Ibañez D, Urowitz MB. The effect of lupus nephritis on pregnancy outcome and fetal and maternal complications. J Rheumatol. 2010;37(4):754–758. doi:10.3899/jrheum.090872
26. Yuen SY, Krizova A, Ouimet JM, Pope JE. Pregnancy Outcome in Systemic Lupus Erythematosus (SLE) is improving: results from a case control study and literature review. Open Rheumatol J. 2009;2(1):89–98. doi:10.2174/1874312900802010089
27. Mecacci F, Bianchi B, Pieralli A, et al. Pregnancy outcome in systemic lupus erythematosus complicated by anti-phospholipid antibodies. Rheumatology. 2009;48(3):246–249. doi:10.1093/rheumatology/ken458
28. Clowse ME. Lupus activity in pregnancy. Rheum Dis Clin North Am. 2007;33(2):237. doi:10.1016/j.rdc.2007.01.002
29. Jiang M, Chang Y, Wang Y, et al. High-risk factors for adverse pregnancy outcomes in systemic lupus erythaematosus: a retrospective study of a Chinese population. BMJ Open. 2021;11(11):e049807. doi:10.1136/bmjopen-2021-049807
30. Al Arfaj AS, Khalil N. Pregnancy outcome in 396 pregnancies in patients with SLE in Saudi Arabia. Lupus. 2010;19(14):1665–1673. doi:10.1177/0961203310378669
31. Tincani A, Bompane D, Danieli E, Doria A. Pregnancy, lupus and antiphospholipid syndrome (Hughes syndrome). Lupus. 2006;15(3):156–160. doi:10.1191/0961203306lu2279rr
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.