")
Back to Journals » Biologics: Targets and Therapy » Volume 18
Advances with Platelet-Rich Plasma for Bone Healing
Authors Bacevich BM, Smith RDJ, Reihl AM, Mazzocca AD, Hutchinson ID
Received 5 October 2023
Accepted for publication 17 January 2024
Published 25 January 2024 Volume 2024:18 Pages 29—59
DOI https://doi.org/10.2147/BTT.S290341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Shein-Chung Chow
Blake M Bacevich,1 Richard David James Smith,1 Alec M Reihl,1 Augustus D Mazzocca,1,2 Ian D Hutchinson1
1Division of Sports Medicine, Department of Orthopaedic Surgery, Massachusetts General Hospital, Harvard Medical School, Massachusetts General Brigham, Boston, MA, USA; 2Medical Director, Division of Sports Medicine, Department of Orthopaedic Surgery, Massachusetts General Brigham, Boston, MA, USA
Correspondence: Ian D Hutchinson, Division of Sports Medicine, Department of Orthopaedic Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA, Tel +1 781-487-6166, Fax +1 781-487-6826, Email [email protected]
Abstract: Despite significant advances in the understanding and delivery of osteosynthesis, fracture non-union remains a challenging clinical problem in orthopaedic surgery. To bridge the gap, basic science characterization of fracture healing provides a platform to identify and target biological strategies to enhance fracture healing. Of immense interest, Platelet-rich plasma (PRP) is a point of care orthobiologic that has been extensively studied in bone and soft tissue healing given its relative ease of translation from the benchtop to the clinic. The aim of this narrative review is to describe and relate pre-clinical in-vitro and in-vivo findings to clinical observations investigating the efficacy of PRP to enhance bone healing for primary fracture management and non-union treatment. A particular emphasis is placed on the heterogeneity of PRP preparation techniques, composition, activation strategies, and delivery. In the context of existing data, the routine use of PRP to enhance primary fracture healing and non-union management cannot be supported. However, it is acknowledged that extensive heterogeneity of PRP treatments in clinical studies adds obscurity; ultimately, refinement (and consensus) of PRP treatments for specific clinical indications, including repetition studies are warranted.
Keywords: platelet rich plasma, bone regeneration, fracture healing, fractures, ununited
Introduction
Bone healing stands as a complex and pivotal process within the realm of orthopedics, carrying with it substantial clinical and financial burdens. In 2019, the global incidence of bony fractures stood at a staggering 178 million cases, underscoring the pervasive nature of this often-debilitating health concern.1 While the majority of fractures heal successfully, approximately 5–10% of patients encounter a formidable obstacle: non-union.2 The Food and Drug Administration (FDA)3 has defined a non-union as a fracture that persists at 9 months post-injury, exhibiting insufficient signs of healing over three consecutive months. This condition manifests in two distinct forms—hypertrophic non-union, due to inadequate stability at the fracture site, and atrophic non-union, attributed to a deficiency of fracture biology and bone healing.4 The management of fracture non-union is considered on an individualized basis and involves surgical strategies to optimize stability (and strain) at the fracture site while identifying and addressing any deficits in fracture biology manifested in the bone healing response [183]. The costs associated with non-union treatment can be staggering, with tibial non-unions, for example, incurring an approximate cost of $25,556 USD compared to $11,686 USD for tibial fractures without non-union complications.5
The physiological process of bone healing is intrinsically sophisticated, typically progressing through three stages: the inflammatory phase, where hematoma forms and inflammatory cells infiltrate the site; the reparative phase, which involves the formation of a soft callus that gradually mineralizes; and the remodeling phase, where the callus is replaced by mature bone tissue.6 Each of these stages is marked by a distinct cascade of cellular and molecular events, underscoring the potential for therapeutic interventions that can modulate these processes.
Historically, the treatment of bone injuries has evolved from rudimentary splinting techniques to advanced surgical interventions, reflecting a deepening understanding of bone biology and healing processes. In the quest to enhance bone healing, regenerative medicine has introduced several innovative therapies, of which platelet-rich plasma (PRP) therapy has emerged as a significant contender. PRP therapy, in comparison to other regenerative approaches like stem cell therapy or bone morphogenetic proteins (BMPs), offers a unique blend of autologous growth factors and cytokines, potentially reducing the risk of immune rejection and other complications associated with allogeneic or synthetic materials.7 Initially recognized for its role in tissue sealing as fibrin tissue adhesives, PRP subsequently garnered attention for its potential to emulate the initiation of the natural healing cascade.8 The rationale behind PRP therapy lies in its ability to release biologically active factors and adhesion proteins, offering the potential to stimulate the resolution of chronic pathological processes.9 Specifically, PRP is replete with growth factors such as Platelet-Derived Growth Factor (PDGF), Transforming Growth Factor-beta (TGF-β), and Insulin-Like Growth Factor-1 (IGF-1), which are critical mediators in the bone healing process.10 These growth factors and cytokines play key roles in regulating inflammation, angiogenesis, and osteoblastic activity, making them vital to the various phases of bone repair.11–13
Despite promising pre-clinical data supporting the potential of PRP, clinical trials have yet to unequivocally demonstrate its benefits in bone healing. Moreover, the absence of a standardized PRP injection protocol(s) hinders efforts to generalize findings or collate the data of individual studies. Dosage and timing intervals remain uncertain, and the composition of PRP varies widely in terms of leukocyte and platelet count, growth factor concentration, and red blood cell contamination due to patient characteristics and the preparation kit used.8,14 This heterogeneity in PRP formulations further complicates its clinical application to date, given the current absence of a universally accepted PRP injection protocol. Therefore, the aim of this narrative review is to provide a comprehensive platform to evaluate the evidence regarding the use of PRP for bone healing.
Biological Activity of PRP: Influence on the Bone Regeneration Process
The pursuit of optimal strategies for bone healing has driven the exploration of PRP therapy due to its ability to serve as a concentrated source of autologous growth factors and cytokines. Our current understanding of PRP’s biological activity in bone healing has been predominantly centered on three key aspects: inflammatory cytokines, growth factors, and angiogenic factors (Table 1). These factors orchestrate the intricate process of cell signaling, tissue regeneration, and angiogenesis during the bone healing process.
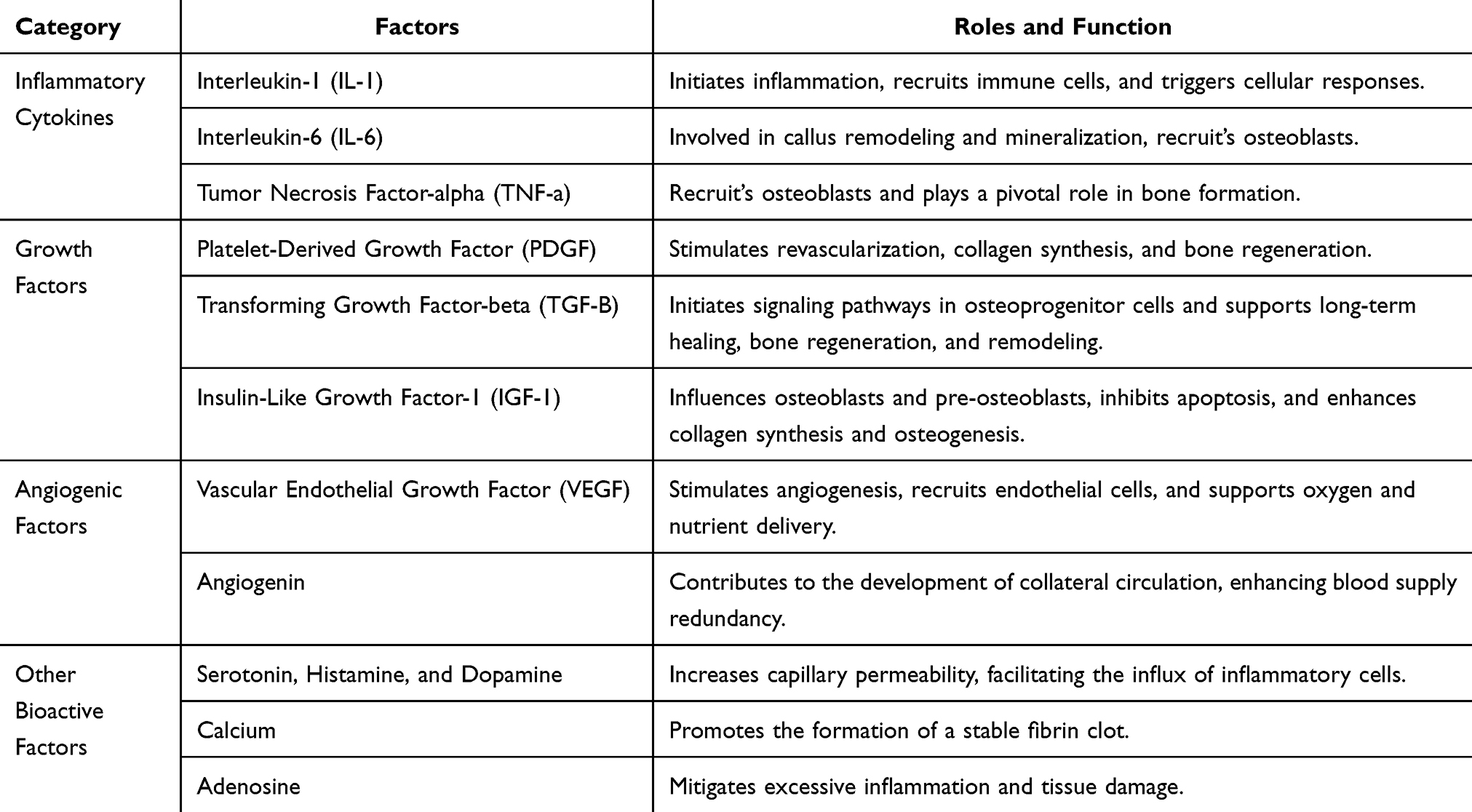 |
Table 1 Function of the Growth Factors and Cytokines Found in PRP on Bone Regeneration |
Inflammatory Cytokines
The initial phase of bone healing is characterized by inflammation, a crucial process that dictates the subsequent stages of repair, and platelets in PRP have been shown to successfully modulate this inflammatory response.10,15 Once activated, the platelets in PRP release a spectrum of inflammatory cytokines from their alpha-granules such as Interleukin-1 (IL-1), Interleukin-6 (IL-6), and Tumor Necrosis Factor-alpha (TNF- α).13,16 These cytokines play pivotal roles in the initiation of fracture repair by recruiting immune cells and initiating a cascade of biochemical and cellular alterations that set the stage for subsequent stages of bone repair. IL-1 stands out as a main regulator of the initial inflammatory responses in bone healing. Its release at the fracture site follows a biphasic pattern, characterized by an initial peak during the onset of the fracture healing process, succeeded by a subsequent peak during the shift from chondrogenesis to osteogenesis in the phase of endochondral maturation.17,18 This cytokine plays a multifaceted role, influencing the recruitment of immune cells to the injury site and initiating a multitude of cellular responses necessary to the bone healing process.19–21 Additionally, TNF-alpha also follows a biphasic pattern in its expression during the healing process and plays a pivotal role in recruiting osteoblasts to the injury site.17,18 These bone-forming cells are crucial for the synthesis of new bone tissue and studies20–22 have indicated that both TNF-α and IL-1β recruit osteoblasts, highlighting their collaborative role in bone regeneration. Furthermore, IL-6 is a multifunctional cytokine involved in bone repair. Studies using IL-6 knockout mice23 have shown that this cytokine plays a role in callus remodeling and mineralization, indicating its significance in the later stages of bone healing. Additionally, IL-6 has been implicated in recruiting osteoblasts, further contributing to bone formation.24,25 Thus, the orchestrated release of inflammatory cytokines in the early phases of bone healing is crucial for initiating the repair process and may be able to be amplified through the application and activation of PRP.
Growth Factors
PRP’s effectiveness in bone healing can be attributed significantly to the rich assortment of growth factors contained in the alpha-granules of platelets. Of the numerous growth factors that have been defined in the literature,26–29 the three that appear to play the most prominent role in bone healing include PDGF, TGF-β, and IGF-1.10 PDGF is a critical growth factor in PRP that plays a pivotal role in the early phases of bone healing by initiating several essential processes upon release from activated platelets. It stimulates revascularization, an essential step in bone repair, by promoting the growth of new blood vessels.11,30 This improved blood supply may facilitate the delivery of oxygen and nutrients to the injury site, accelerating the healing process. PDGF also has a profound impact on collagen synthesis, a key component of bone tissue. It encourages the production of collagen, enhancing the formation of a robust extracellular matrix (ECM) essential for bone regeneration.11,31,32 Moreover, PDGF can directly influence mesenchymal stem cells (MSCs), inducing their migration and osteogenic differentiation.33,34 These MSCs are crucial for generating new bone tissue, making PDGF a potent stimulator of bone formation.
TGF-β is also abundantly present in PRP and holds a multifaceted role in bone healing. It functions by exerting both paracrine and autocrine effects, influencing various cell types involved in long-term healing, bone regeneration, and bone modeling.29 One of TGF-β’s most crucial functions is its ability to initiate the signaling pathway of osteoprogenitor cells, which synthesize BMPs.12 These BMPs have demonstrated the potential to play a pivotal role in regulating the expression of growth factors in bone and cartilage tissue, further promoting bone healing and regeneration.35,36 TGF-β’s influence also extends to fibroblasts and pre-osteoblasts, stimulating the biosynthesis of type I collagen and fibronectin, supporting the formation of a robust ECM.37–39 Additionally, TGF-β promotes the deposition of bone matrix, contributing to the early stages of bone repair.40 Furthermore, it inhibits osteoclast formation and bone resorption, tilting the balance toward bone formation over resorption.41
IGF-1 is another significant component of PRP that plays a vital role in bone regeneration. This growth factor is deposited in bone matrix, endothelial cells, and chondrocytes and is released during the bone regeneration process.42 IGF-1 is responsible for orchestrating the complex interaction between bone formation and bone resorption. IGF-1’s presence in platelets influences osteoblasts and pre-osteoblasts, initiating osteogenesis and inhibiting the apoptosis of bone cells.43 Additionally, IGF-1 affects the expression of mesenchymal collagen enzymes, decreasing their degradation and enhancing collagen synthesis within the ECM. This leads to improved structural integrity and strength in the newly formed bone tissue.43 The growth factors found in PRP, including PDGF, TGF-β, and IGF-1, work synergistically to enhance bone healing. They promote angiogenesis, collagen synthesis, ECM formation, and osteogenesis, contributing to the regeneration and repair of bone tissue. These growth factors play distinct but interconnected roles, collectively facilitating the intricate process of bone healing and regeneration.
Angiogenic Factors
Angiogenesis plays a sustained role in delivering oxygen, nutrients, and precursor cells to the site of injury.44–46 PRP has demonstrated the ability to serve as a potent facilitator of angiogenesis, promoting the formation of new blood vessels that are crucial for supporting the regenerative processes in bone repair. Among the angiogenic factors found within PRP, Vascular Endothelial Growth Factor (VEGF) stands out as a principal driver of neovascularization. VEGF is a signal protein and its primary function is to stimulate angiogenesis.47 Upon the application of PRP to the bone defect site, the release of VEGF from platelets sets in motion a cascade of events. VEGF initiates a signaling cascade, acting as a potent mitogen and chemoattractant for endothelial cells, promoting their proliferation and migration to the area surrounding the bone defect.48–50 Once recruited, endothelial cells start to organize into primitive vascular structures, sprouting and elongating to form capillaries that infiltrate the damaged tissue.48,51 This neovascularization process serves two essential purposes in bone healing. Firstly, it ensures a continuous supply of oxygen and nutrients to the healing site, facilitating the metabolic demands of reparative cells. Secondly, it provides a conduit for the migration of osteoprogenitor cells and mesenchymal stem cells, which are crucial for the formation of new bone tissue.10,52,53
While VEGF primarily influences the growth of new vessels, angiogenin, another angiogenic factor found in PRP, contributes to the development of collateral circulation, which can be particularly relevant in cases where the primary blood supply to a bone defect may be compromised.10 Enhanced blood supply increases the resilience of the healing process, ensuring that adequate resources are available to support the regenerative demands of the damaged bone tissue. In the intricate orchestration of bone healing, angiogenesis is a fundamental process that ensures the delivery of essential resources to the site of injury. PRP therapy, enriched with angiogenic factors such as VEGF and angiogenin, plays a central role in promoting neovascularization and collateral circulation. By stimulating the formation of new blood vessels and alternate circulation pathways, PRP creates an environment conducive to optimal bone regeneration.
Other Bioactive Factors
In addition to growth factors, PRP contains a diverse array of bioactive factors stored within the dense granules of platelets, including serotonin, histamine, dopamine, calcium, and adenosine.54,55 These factors exert fundamental effects on the biologic aspects of wound healing, influencing inflammation modulation and cell function. In the context of PRP therapy, serotonin, histamine, and dopamine contribute to wound healing by increasing capillary permeability. This effect facilitates the influx of inflammatory cells to the site of injury, promoting an initial immune response and the activation of macrophages.56,57 Furthermore, calcium is essential for blood clotting, and its release from platelet granules upon activation is crucial for the formation of a stable fibrin clot at the site of injury.58 The clot not only prevents excessive bleeding but also provides a scaffold for cells involved in tissue repair to attach and proliferate. Additionally, adenosine receptor activation has been shown to modulate inflammation during wound healing, promoting an anti-inflammatory environment.59 Attenuation of local inflammation may be beneficial in the early stages of bone repair, as it may help mitigate excessive inflammation and tissue damage.10,59
PRP Separation: Optimizing Platelet Concentration
Over the past decade, substantial efforts have been devoted to refining PRP preparation techniques, with the aim of optimizing platelet concentration—a critical factor influencing its therapeutic effectiveness in bone healing. While numerous studies have demonstrated PRP’s positive effects on the differentiation and proliferation of human osteoblasts, at present, there exists no unanimous agreement on the ideal PRP dosage. Marx et al initially defined PRP as containing a minimum platelet concentration of 1,000,000 platelets/µL, however, the US Food and Drug Administration (FDA) mandates that PRP products must possess a minimum platelet concentration of 250 × 103/mL.60 Several additional investigators61–63 have also reported that a platelet concentration approximately two times greater than that found in peripheral blood positively affects osteoblast proliferation in vitro and significantly reduces bone healing time. However, Jovani-Sancho et al64 reported that an optimal platelet concentration of four times that of peripheral blood was necessary for optimal results. Other studies65–67 have indicated that concentrations below approximately 0.85 × 109/mL had no significant effect on osteogenesis. In contrast, however, Choi et al68 found that lower PRP concentrations, ranging from 1% to 5% of peripheral blood levels, stimulated the viability and proliferation of osteoblasts. Furthermore, it is crucial to exercise caution when considering platelet concentration, as adverse events have been observed at higher dosages.69–71 Fernandez-Medina et al72 indicated that cell viability and migration assays demonstrated detrimental effects on human osteoblasts when the PRP concentration exceeded 60%. Similarly, Al-Hamed et al61 reported that platelet concentrations greater than 8.21 ± 0.4 × 109/mL inhibited osteogenic proliferation and Graziani et al65 observed that a platelet concentration approximately 3.5 times greater than that of native blood led to a reduction in cell proliferation. These findings underscore the complexity of determining the precise platelet concentration required for optimal bone healing, as different concentrations of PRP may produce varying effects.
Centrifugation separates individual cells within blood based on their individual density gradients, thus the overlaps and proximity of the density of platelets and leukocytes present the possibility of contamination (Figure 1). Similar to other indications, the optimal concentration of leukocytes within PRP for bone healing remains not fully understood. Proponents of incorporating leukocytes argue that the antimicrobial properties of WBCs could mitigate the risk of infection, particularly when PRP is utilized intraoperatively.73–76 Moreover, studies by Zimmermann et al77 have revealed that leukocytes in leukocyte-rich PRP (LR-PRP) contribute significantly to the increased variability of growth factors, such as PDGF-αβ, PDGF-β1, and VEGF, in comparison to leukocyte-poor PRP (LP-PRP). This suggests that the concentration of white blood cells can be manipulated to optimize growth factor levels, potentially influencing the healing process positively. However, critics of leukocyte incorporation argue that the existence of WBCs can result in immediate pain and discomfort post-injection, while their catabolic and proinflammatory attributes may adversely impact the process of articular cartilage recovery as a result of the increased release of proinflammatory cytokines.78–80 Clinical investigations have further validated concerns regarding increased acute swelling and pain after intra-articular LR-PRP injection.81,82 Nevertheless, it is noteworthy that both LR-PRP and LP-PRP have demonstrated statistically significant improvements in clinical outcomes. Recent research, however, has added to this debate by highlighting the importance of matching the type of PRP with the specific clinical context. The prevailing evidence suggests that the choice of leukocyte concentration should be guided by the injection site.73,83 For intra-articular applications, LP-PRP appears to be more beneficial, as indicated in the treatment of knee osteoarthritis. LR-PRP has shown adverse effects on synovial cells, resulting in cell death and proinflammatory mediator production.81,84 In contrast, for the treatment of chronic tendinopathy, leukocyte-rich PRP has demonstrated superiority over leukocyte-poor PRP.85
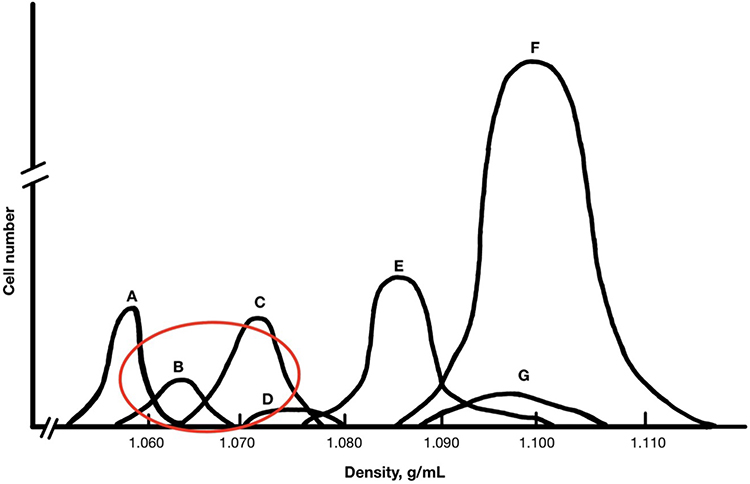 |
Figure 1 Density Gradients of Cells Contained within Blood Aspirate. Notes: (A) Platelets, (B) Monocytes, (C) Lymphocytes, (D) Basophils, (E) Neutrophils, (F) Erythrocytes, (G) Eosinophils. |
Unfortunately, a lack of universal preparation standardization and compositional reporting hampers our ability to collate data from individual studies and to gain consensus on findings. In most cases, blood is drawn from a patient, treated with an anticoagulant, and then centrifuged within an hour of collection. The methods then employed for isolating platelets and growth factors from whole blood can be broadly categorized based on two different distinctions: plasma vs buffy coat-based systems and single-spin vs double-spin processes. Plasma-based systems utilize a slower, shorter spin to isolate plasma and remove WBCs, resulting in platelet 2–3x’s baseline levels (Figure 2A). 69 Contrary, buffy coat-based systems utilize a longer, double spin to isolate a platelet-poor layer (Figure 2B). This allows for an obtained platelet concentration of 3–8x that of baseline levels, however, because of the density it also keeps a concentration of WBCs.69 Furthermore, single-spin processes, represented by many clinically used commercial devices, encompass variations such as low-platelet PRP (PRPLP) and high-platelet PRP (PRPHP). These one-step methods offer a more straightforward and less resource-intensive approach to PRP preparation. Conversely, double-spin processes (PRPDS) have historically been favored in basic science investigations due to their ability to produce PRP with higher platelet concentrations.86 These methods often involve two sequential centrifugation steps, allowing for the separation of platelets from other blood components more effectively. However, recent studies have provided conflicting insights into the strengths and limitations of single-spin and double-spin processes. Notably, Mazzocca et al87 demonstrated that PRPHP produced significantly higher platelet and white blood cell concentrations compared to both the single-step PRPLP and two-step PRPDS procedures. However, no significant differences were observed between PRPLP and PRPDS. Conversely, Saqlian et al88 and Nagata et al89 reported a greater platelet and WBC quantity following PRPDS compared to single-spin techniques. Additionally, when considering specific growth factors, Han Oh et al88 demonstrated that PRPDS resulted in a significantly greater concentration of PDGF and VEGF whereas single-spin methods produced a significantly greater concentration of TGF and FGF. While findings by Mazzocca et al underscore the potential efficacy of one-step procedures and suggest that the increased time required for two-step procedures may not necessarily be advantageous for producing therapeutic PRP preparations, other studies still provide support to the historical superiority of PRPDS.
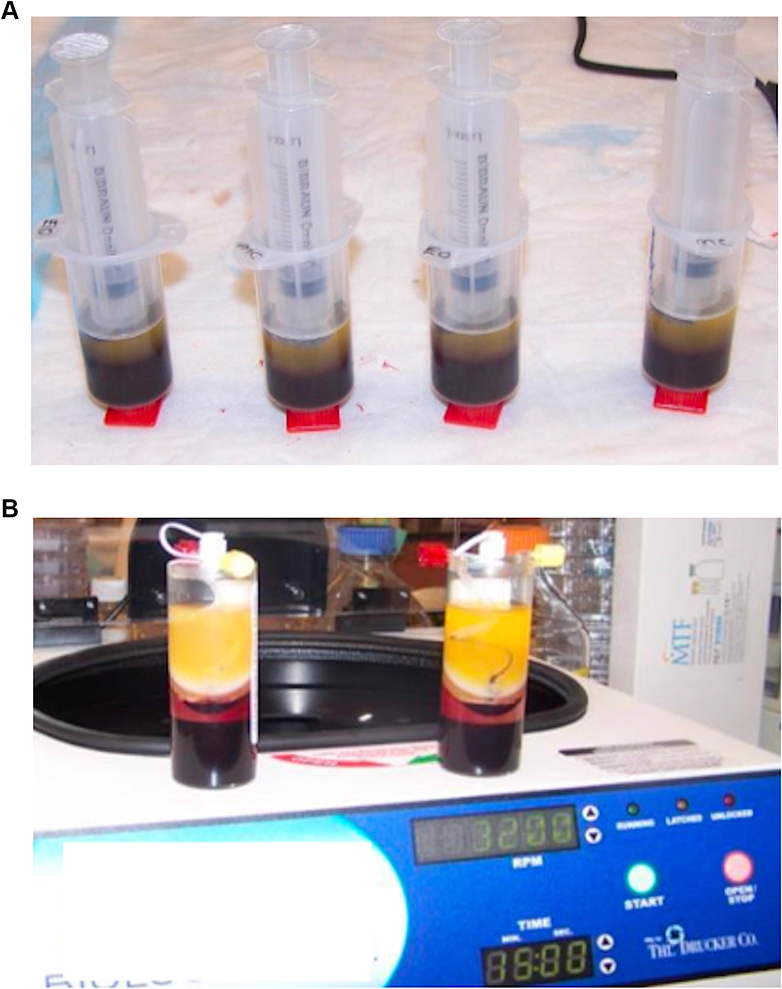 |
Figure 2 (A) Plasma-Based PRP Preparation. (B) Buffy Coat-Based PRP Preparation. |
With the clinical advent of PRP use for bone and soft tissue indications, numerous commercial PRP preparation kits have entered the market. These devices offer the convenience of pre-packaged, standardized protocols, which can be especially beneficial for clinical applications. However, while designed to serve a common purpose, these kits exhibit noteworthy differences in multiple aspects of PRP preparation which manifests as variations in platelet, WBC, and RBC concentrations in the final PRP product. Numerous comprehensive reviews of currently available devices reveal substantial variability in their methodologies and the resultant PRP compositions. Dejnek et al89 extensively evaluated four commonly used commercial PRP systems: Arthrex Autologous Conditioned Plasma (ACP), Mini GPS III, Xerthra, and Dr. PRP. Among the systems evaluated, Mini GPS III notably stood out, yielding significantly higher concentrations of platelets, WBCs, and RBCs compared to the other three systems. Additionally, in a systematic review of the 10 most referenced commercially available PRP systems, Oudelaar et al83 found significant variations in platelet and leukocyte concentrations. The highest concentration of platelets was produced by the Cascade system, while the lowest concentration of platelets was generated by the ACP system. Notably, the GPS III system exhibited a significantly higher concentration of leukocytes compared to other systems. Furthermore, the study reported that the GPS III and SmartPrep systems had the highest platelet enrichment factors, while the ACP, RegenPRP, and Cascade systems showed lower platelet enrichment factors. Furthermore, when analyzing 33 different commercial systems, Fadadu et al73 found a significantly positive correlation between maximum centrifuge spin force, platelet concentration, and PDGF concentration, however, spin time demonstrated no significant relationships. Additionally, 3 of the 33 systems resulted in a platelet count less than that of whole blood. A review by Magalon et al90 also demonstrated that of the 36 PRP preparation systems analyzed, 11 resulted in a final product made up of more RBCs than platelets. These findings emphasize immense variability in commercially available PRP preparation systems. Thus, the choice of a specific commercial device plays a substantial role in determining PRP composition and underscores the importance of selecting the most suitable system based on the intended clinical application. Despite the profound importance of optimizing PRP’s platelet concentration, the challenge of defining a singular optimal value is exacerbated by the variability in research methods employed by past studies.87,91 Consequently, tailoring PRP to individual clinical contexts remains a dynamic process that considers the nature of the injury, the patient’s unique characteristics, and the desired treatment outcomes.
Activation of PRP: Unleashing the Healing Potential
The activation of PRP is an important phase in its therapeutic application, as it serves to transform concentrated platelets into a biologically active state, primed to effectively stimulate the regenerative process. This activation process encompasses two key elements. Firstly, it involves the degranulation of platelets, liberating GFs from α-granules. Secondly, it triggers the cleavage of fibrinogen, initiating matrix formation—a clotting process that facilitates the development of a platelet gel, effectively constraining the secretion of molecules to the designated site.92,93 Consequently, the choice of activator during PRP preparation becomes a critical determinant of its efficacy, influencing both the quantity and release kinetics of GFs from platelets within PRP. Research on the activation of PRP has unveiled a complex interplay of factors that significantly influence its clinical efficacy and therapeutic potential and activation methods have undergone significant development, with multiple techniques devised to unlock the potential of growth factors and other bioactive molecules.
One traditional method of activation involves the addition of bovine thrombin to PRP. Thrombin serves as a rapid activator of platelets, promoting degranulation and facilitating the conversion of fibrinogen into fibrin, resulting in the formation of a stable clot that effectively traps platelets at the target location.94 This entrapment promotes immediate degranulation and the release of growth factors and cytokines. Prior studies have demonstrated that the rapid action of thrombin resulted in an immediate release pattern of approximately 70% of stored growth factors within 10 minutes and nearly 100% released within 1 hour.29,95 While this method offers swift and substantial growth factor activation, it comes with a challenge—released growth factors are swiftly cleared, precluding their long-term stimulatory effects on cells. This concept has been supported by studies that have found that the rapid activation triggered by bovine thrombin results in a reduction in the overall quantity of growth factors accessible at the tissue location over time.69,93 If not promptly utilized upon release, GFs risk degradation before additional tissue receptors become available.95,96 Additionally, bovine thrombin has been shown to carry the potential for complications arising from the generation of antibodies that may result in immune-mediated coagulopathy.86
An alternative approach utilizes calcium chloride to convert autologous prothrombin to thrombin, resulting in platelets being trapped in a fibrin matrix. Numerous studies97,98 have demonstrated that using calcium chloride as an activator can lead to higher concentrations of specific GFs, such as TGF-β(1) and PDGF-AB. Additionally, calcium-based activators have been shown to induce a gradual and extended process of platelet activation, leading to the progressive release of platelet content.93,95 This sustained activation results in the gradual accumulation of endogenous thrombin, facilitating a slower and more extended release of growth factors spanning several days.99 Consequently, this extended-release pattern addresses the need for sustained growth factor delivery necessary for the prolonged nature of bone regeneration.100–102 Additionally, calcium chloride activation was observed to have advantages beyond its release kinetics. Zhuang et al97 demonstrated that calcium chloride can avoid the complications related to antibody formation and immune-mediated coagulopathy associated with bovine thrombin due to the autologous formation of thrombin from prothrombin. However, calcium chloride activation is not without potential shortfalls as well. An excess of calcium has been shown to trigger the swift activation of the clotting cascade, inducing rapid degranulation.102 Additionally, elevated calcium levels may enhance the activity of protein C, protein S, and antithrombin III, potentially destabilizing the fibrin clot and consequently shortening the therapeutic window for platelets.102,103
Fufa et al104 initially proposed the concept of Type-1 collagen as a safe and effective alternative to bovine thrombin for clot activation in PRP. Their initial findings supported this notion by demonstrating a reduction in clot retraction and comparable levels of PDGF-AB and VEGF release. However, recent research has cast some uncertainty on its efficacy. While numerous studies8,95 have observed a more sustained cytokine release pattern with Type-1 collagen compared to bovine thrombin, a contrasting perspective emerged from Cavallo et al,93 indicating that collagen’s platelet-activating capabilities were relatively weak, leading to a lack of clot formation and notably lower GF release compared to bovine thrombin and calcium chloride. While this approach holds promise, further investigations are imperative to elucidate the genuine activation potential of Type-1 collagen in PRP applications.
In some cases, PRP may be applied without exogenous activators. During local infusion, the presence of the natural clotting factor, thrombin, often suffices to activate platelets effectively.105,106 This simplified activation process, however, may lead to variations in growth factor release contingent upon the specific clinical context. Additionally, in a recent meta-analysis99 comparing activated and non-activated PRP, it was observed that non-activated PRP did not yield any substantial clinical improvements in terms of pain relief or functional scores when compared to a placebo. The choice of activator, whether it be calcium chloride, thrombin, collagen, or others, has a profound impact on clot formation, release kinetics, and the therapeutic potential of PRP. Understanding these factors is essential for tailoring PRP preparations to specific clinical needs and optimizing their effectiveness in various medical applications. In the context of bone healing, achieving sustained and controlled release of growth factors is often desirable as this aligns with the gradual and intricate nature of bone regeneration. Ongoing research continues to shed light on this dynamic field, enhancing our ability to harness the therapeutic potential of PRP for improved patient outcomes.
Delivery: Tailoring Application Methods
The manner in which PRP is delivered to the target site also plays a role in optimizing PRP’s therapeutic potential for bone healing. Clinically, PRP is often given through direct injection, topical application, or in combination with a surgical procedure and remains a widely employed and versatile clinical delivery method for bone healing. By injecting PRP directly into the affected site, clinicians can promote a concentrated release of growth factors precisely where they are needed most. Thus, this method expedites the regenerative process by providing a high concentration of growth factors directly to the injury site. Precision of delivery to the targeted tissue using ultrasound may also enhance clinically efficacy.107–109 Additionally, topical application of PRP has gained recognition as an effective clinical approach for surgical or wound site(s), promoting tissue repair, reducing inflammation, and accelerating the healing process.110–112 Furthermore, in addition to standalone PRP delivery, clinicians frequently combine PRP with surgical procedures involving bone grafts. This approach aims to optimize the integration of graft materials and enhance the overall success of the surgical intervention. For instance, PRP may be mixed with bone graft materials such as autografts, allografts, or synthetic grafts before implantation. However, this combination has shown contradicting effects on the enhancement of the graft’s osteogenic potential and ability to accelerate bone healing and reduce the risk of graft rejection.113–116
To address the need for sustained growth factor release, researchers have employed scaffolds as delivery vehicles for PRP. In the context of bone healing, scaffolds can play a critical role in maintaining the integrity of the injury site, preventing migration of PRP, and enabling controlled and sustained release of growth factors.117 Scaffolds such as hydrogels, sponges, and nanofiber-based structures offer the ability to tailor the release kinetics of PRP-derived growth factors.118 Thus, the choice of scaffold material can influence factors like degradation rate, which, in turn, affects the release profile of PRP components. Hydrogels and sponges, composed of materials such as alginate and gelatin, have demonstrated their efficacy as delivery systems for PRP in bone regeneration. These systems offer the advantage of tailorable scaffold degradation, which affects the release of incorporated factors, making them ideal for sustained delivery and enhanced bioavailability of growth factors at the injury site.119 In support of this, Lin et al120 incorporated PRP into an alginate hydrogel, demonstrating that the growth factors released from the hydrogel stimulated the osteogenic differentiation of human MSCs in vitro. Lu et al121 further investigated the growth factor release kinetics of PRP-incorporated alginate hydrogels, showcasing the varying release profiles based on carrier type and the potential of these factors to promote osteoblast-like cell proliferation and activity. In addition to alginate, gelatin, a denatured collagen derivative, has gained attention as a base material for scaffolds in bone healing. Gelatin shares functional groups with collagen, the primary organic component of bone, yet is easier to obtain and less expensive making it an attractive option.119,122 Animal studies by Hokugo et al123,124 have demonstrated that PRP growth factors can be immobilized within gelatin hydrogels, leading to growth factor release correlating with hydrogel degradation. Such studies highlight the potential of hydrogels and sponges to offer controlled and sustained delivery of PRP-derived growth factors, contributing to enhanced bone healing both in vitro and in vivo. Incorporation of bioactive inorganic calcium phosphates, such as carbonated hydroxyapatite (CHA), into PRP-based scaffolds holds significant promise for bone healing and regeneration. Kaur et al125 conducted a study in which they explored the combination of PRP and CHA, finding that this hybrid scaffold yielded significantly enhanced histological bone formation. This suggests that the integration of CHA into PRP delivery systems can enhance the osteogenic potential, potentially accelerating bone healing. Additionally, a study by Liu et al,126 focusing on the inclusion of platelets in calcium phosphate cement, indicated promising outcomes for angiogenesis and osteogenesis. Furthermore, an animal study by Qiu et al127 adds to the growing body of evidence supporting the positive impact of PRP in combination with calcium phosphate cement on bone regeneration by demonstrating favorable results in minipigs. These studies underline the versatile applications of PRP, especially when combined with calcium-based materials, in promoting both vascularization and bone tissue formation. PRP has also been covalently or ionically bonded onto plasma polymers, showcasing enhanced scaffold properties.128 Specifically, it has been reported that the application of poly-ε-caprolactone (PCL) nanofibers coated with PRP substantially enhances the survival and growth of human MSCs.128 These findings emphasize the diverse strategies available for optimizing PRP delivery systems and their potential to enhance bone healing through various approaches, including surface modifications and the development of novel biomaterials.
A Review of Pre-Clinical and Clinical Studies
Vitro Pre-Clinical Studies
This comprehensive review identified 24 in vitro studies that investigated the effects of PRP or a related derivative, on various cell types.31,32,61,67,72,129–147 The diverse spectrum of cell types included osteoblasts, fibroblasts, osteocytes, myocytes, tenocytes, human umbilical vein endothelial cells, bone marrow mesenchymal stem cells, marrow stromal cells, and human osteosarcoma cell lines. Among these studies, 14 (58%)32,61,67,129,136–140,142–144,146,147 of the 24 studies reported PRP increased cell proliferation, 7 studies (29%)67,132,134,135,139,141 reported PRP increased expression of bone-related genes and growth factors, and 5 studies (21%)31,132,143,146,147 reported PRP increased cell migration. Notably, several of these investigations highlighted the effects of PRP were dose-dependent with differing cell responses at different concentrations.61,67,72,142,144,146 In addition, 2 studies (8%)140,141 provided evidence suggesting that PRP has the potential to facilitate osteogenic differentiation of pluripotent stem cells. Furthermore, 1 study (4%)137 reported PRP’s ability to induce tubular formation in human umbilical vein endothelial cells (HUVECs). Another study (4%)145 indicated an increase in osteoblast viability and adhesion following PRP exposure. Conversely, 2 studies (8%)130,131 did not discern any notable impact of PRP on cell behavior. Lastly, 1 study (4%)72 found that concentrations of PRP exceeding 60% decreased cell viability and migration. A summary of the main details of all in-vitro pre-clinical studies can be found in Table 2.
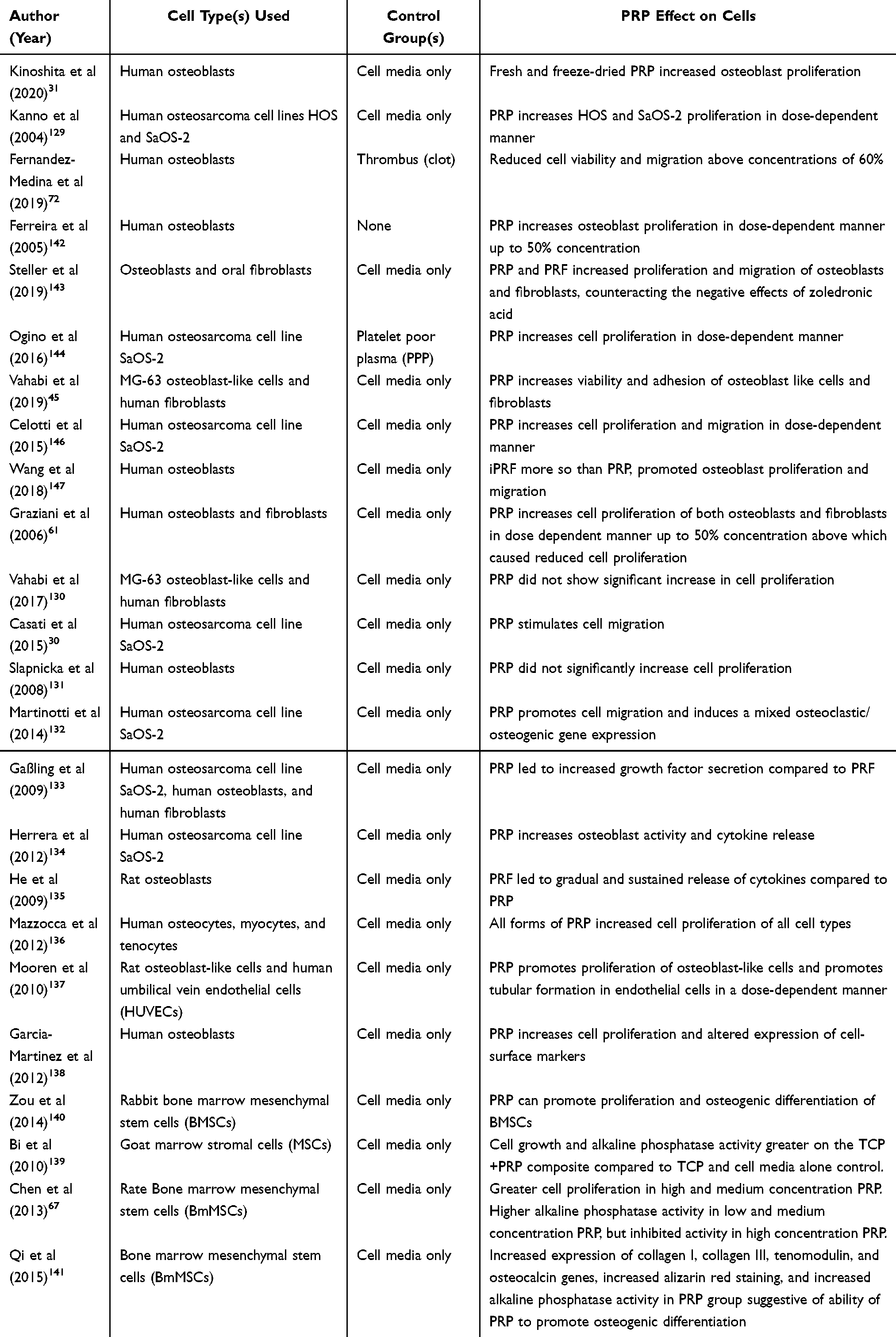 |
Table 2 Effects of PRP on Cell Behavior in vitro |
Vivo Pre-Clinical Studies
A total of sixty pre-clinical in vivo animal studies were identified which investigated the impact of PRP on bone healing.63,67,123,139,141,148–202 The animal models employed in these studies exhibited a notable variation in usage, with rabbits being the most commonly utilized model in 25 studies (42%), followed by rats in 12 studies (20%) and sheep in 8 studies (13%). Conversely, the less frequently employed animal models included goats in 2 studies (3%), pigs in 2 studies (3%), and mice in 1 study (2%). Regarding the bones studied, the tibia was the most frequently examined bone in 23 studies (38%), followed by the femur in 18 studies (30%) and the radius in 11 studies (18%). In contrast, the skull/forehead was among the least studied bone in 3 studies (5%), along with the fibula and metatarsal, each studied in 2 studies (3%).
Out of the 43 in vivo animal studies that incorporated scaffolds-based delivery methods, a variety of scaffold types were employed. Examples included calcium phosphate, bone autograft, bone allograft, gelatin hydrogels, titanium mesh, collagen, ceramic-coated hydroxyapatite, and coral. In several instances, studies compared the effectiveness of PRP delivery with and without a scaffold, with the most favorable outcomes generally observed when PRP was administered alongside a scaffold.123,150,154,161,168,175,176,178 Notably, the dose-dependent response of PRP observed in in vitro studies was also echoed in some of the in vivo experiments.67,190
Of the 45 pre-clinical animal studies that evaluated radiographic bone healing, 36 studies (80%) reported improvements when PRP was employed, whereas 7 studies (16%) did not reveal any radiographic improvement, and 2 studies (4%) even indicated reduced radiographic bone healing. Similarly, out of the 58 pre-clinical animal studies assessing histopathologic bone healing, 43 studies (74%) reported positive outcomes when PRP was applied. Conversely, 13 studies (22%) did not detect any histopathologic improvement, and 2 studies (3%) reported reduced histopathologic bone healing in association with PRP. Biomechanical properties also displayed favorable trends, with 11 out of 13 pre-clinical animal studies (85%) reporting improvements in bone healing when PRP was employed. Only 2 studies (15%) did not observe any biomechanical improvement, and none indicated a reduction in biomechanical properties when PRP was used.
In summary, pre-clinical in vivo animal studies generally demonstrate overall positive effects of PRP on bone healing. However, the substantial variability in study designs and protocols makes direct comparisons challenging. Moreover, several studies combined PRP with other factors like stem cells or scaffolds, complicating the isolation of PRP’s specific effects. Additionally, many studies compared interventions to untreated negative controls, which may not be ideal, and a few studies lacked control groups entirely. Furthermore, subjective evaluations and a lack of statistical comparisons were observed in several studies.152,154,155,158,167,171,198 Lastly, the use of blinded analysis of specimens was inconsistent, with only 20 studies (33%) reporting its implementation. Table 3 presents a concise overview of the key information pertaining to all in-vivo pre-clinical studies.
 |
Table 3 Effects of PRP on Bone Healing in Pre-Clinical in vivo Animal Models |
Vivo Clinical Studies
There were 24 clinical studies that evaluated PRP to treat fractures in human patients (Table 4). 203–226 Among these studies, 11 were prospective randomized control trials, 8 were prospective case series, and 5 were retrospective case series. The bones predominantly examined were the tibia in 9 studies (38%) and the femur in 5 studies (21%). In terms of PRP delivery methods, 11 studies (46%) utilized PRP injection alone at the injury site, while 9 studies (38%) incorporated PRP with a scaffold, such as bone graft. Four studies (17%) involved the injection of PRP in combination with other substances like bone marrow aspirate or stem cells. The average number of patients per study was 52±52, with a range of 10 to 200 patients, and an average follow-up period of approximately 16±15 months (range 2–72 months). Of the clinical studies, 19 (79%) reported favorable clinical outcomes associated with the use of PRP to improve bone healing. Three studies (13%) demonstrated equivocal outcomes, while two studies (8%) indicated negative effects of PRP on bone healing. As with the pre-clinical studies, there is considerable variability among clinical studies, making it challenging to draw direct comparisons between outcomes. Notably, 9 studies (38%) lacked a control group, rendering it impossible to draw definitive conclusions due to the absence of a comparative baseline. Additionally, 14 studies (58%) did not employ any form of randomization in patient assignment to different treatment types within the study. It is worth noting that, to the best of our knowledge, there are no published double-blinded randomized control trials of PRP in the context of bone healing. Considering the existing body of research, which encompasses a reasonable number of patients and follow-up periods, future clinical investigations should prioritize the use of double-blinded randomized control trials to ascertain the true efficacy of PRP in promoting bone healing.
 |
Table 4 Effects of PRP on Bone Healing in Clinical Studies |
Conclusion
Recent evidence gathered in this extensive review of in vitro pre-clinical, in vivo pre-clinical, and clinical studies underscores the growing significance of PRP as a valuable adjunct in the domain of bone healing. In vitro investigations have demonstrated PRP’s potential to stimulate various cell types, promoting proliferation, gene expression, and migration, thereby substantiating its regenerative potential at the cellular level. Pre-clinical animal investigations, despite the inherent diversity in experimental models and methodologies, affirm the positive impact of PRP on radiographic, histopathologic, and biomechanical aspects of bone regeneration. However, the landscape of pre-clinical research reveals the complexity of direct comparisons due to the variable inclusion of adjunctive factors. In the clinical arena, a majority of studies extend support for the beneficial role of PRP in bone healing yet emphasize the demand for more rigorous methodologies to delineate its precise therapeutic potential. Furthermore, investigations delving into dose-dependent PRP effects and the differentiation between PRP formulations concerning platelet concentration and leukocyte content also represent areas meriting further exploration.
Overall, PRP has emerged as a promising adjunctive tool in the context of bone healing, offering multifaceted advantages that encompass augmented cellular responses, accelerated tissue restoration, and potential expedited rehabilitation. However, advancing its integration into evidence-based medical practice necessitates meticulous and standardized clinical investigations, encompassing larger and more diverse patient cohorts, and employing well-defined outcome measures. These endeavors are poised to deepen our comprehension of PRP’s therapeutic implications, particularly in the dynamic field of regenerative medicine, offering renewed optimism for individuals seeking enhanced musculoskeletal recovery.
Abbreviations
PRP, Platelet-Rich Plasma; LR-PRP, Leukocyte-Rich PRP; LP-PRP, Leukocyte-Poor PRP; PRPLP, Low-Platelet PRP; PRPHP, High-Platelet PRP; PRPDS, Double-Spin PRP; FDA, Food and Drug Administration; GF, Growth Factor; IL-1, Interleukin-1; IL-6, Interleukin-6; TNF-α, Tumor Necrosis Factor-alpha; PDGF, Platelet-Derived Growth Factor; TGF-β, Transforming Growth Factor-beta; IGF-1, Insulin-Like Growth Factor-1; ECM, Extracellular Matrix; MSCs, Mesenchymal Stem Cells; BMPs, Bone Morphogenetic Proteins; VEGF, Vascular Endothelial Growth Factor; WBC, White Blood Cell; ACP, Autologous Conditioned Plasma; CHA, Carbonated Hydroxyapatite; PCL, Poly-ε-Caprolactone; HUVEC, Human Umbilical Vein Endothelial Cell.
Disclosure
ADM disclosures include research support and consulting with Arthrex Inc., Naples, FL, as well as consulting and stock interests in Restor3d. All other authors report no conflicts of interest in this work.
References
1. Wu A-M, Bisignano C, James S, et al. Global, regional, and national burden of bone fractures in 204 countries and territories, 1990–2019: a systematic analysis from the Global Burden of Disease Study 2019. Lancet Healthy Long. 2021;2(9):e580–e592. doi:10.1016/S2666-7568(21)00172-0
2. Calori GM, Mazza E, Colombo M, Ripamonti C, Tagliabue L. Treatment of long bone non-unions with polytherapy: indications and clinical results. Injury. 2011;42(6):587–590. doi:10.1016/j.injury.2011.03.046
3. Cunningham BP, Brazina S, Morshed S, Miclau T. Fracture healing: a review of clinical, imaging and laboratory diagnostic options. Injury. 2017;48(Suppl 1):S69–s75. doi:10.1016/j.injury.2017.04.020
4. Bell A, Templeman D, Weinlein JC. Nonunion of the Femur and Tibia: an Update. Orthop Clin North Am. 2016;47(2):365–375. doi:10.1016/j.ocl.2015.09.010
5. Antonova E, Le TK, Burge R, Mershon J. Tibia shaft fractures: costly burden of nonunions. BMC Musculoskelet Disord. 2013;14:42. doi:10.1186/1471-2474-14-42
6. Cruess RL, Dumont J. Fracture healing. Can J Surg. 1975;18(5):403–413.
7. Cole BJ, Seroyer ST, Filardo G, Bajaj S, Fortier LA. Platelet-rich plasma: where are we now and where are we going? Sports Health. 2010;2(3):203–210. doi:10.1177/1941738110366385
8. Everts P, Onishi K, Jayaram P, Lana JF, Mautner K. Platelet-Rich Plasma: new Performance Understandings and Therapeutic Considerations in 2020. Int J Mol Sci. 2020;21(20). doi:10.3390/ijms21207794
9. Collins T, Alexander D, Barkatali B. Platelet-rich plasma: a narrative review. EFORT Open Rev. 2021;6(4):225–235. doi:10.1302/2058-5241.6.200017
10. Zhang N, Wu Y-P, Qian S-J, Teng C, Chen S, Li H. Research Progress in the Mechanism of Effect of PRP in Bone Deficiency Healing. Sci World J. 2013;2013:134582. doi:10.1155/2013/134582
11. Zhang Y, Chen J, Zhong ZM, Yang D, Zhu Q. Is platelet-derived growth factor-BB expression proportional to fibrosis in the hypertrophied lumber ligamentum flavum? Spine. 2010;35(25):E1479–86. doi:10.1097/BRS.0b013e3181f3d2df
12. Panseri S, Russo A, Cunha C, et al. Osteochondral tissue engineering approaches for articular cartilage and subchondral bone regeneration. Knee Surg Sports Traumatol Arthrosc. 2012;20(6):1182–1191. doi:10.1007/s00167-011-1655-1
13. Cachaço AS, Carvalho T, Santos AC, et al. TNF-alpha regulates the effects of irradiation in the mouse bone marrow microenvironment. PLoS One. 2010;5(2):e8980. doi:10.1371/journal.pone.0008980
14. Jamal MS, Hurley ET, Asad H, Asad A, Taneja T. The role of Platelet Rich Plasma and other orthobiologics in bone healing and fracture management: a systematic review. J Clin Orthop Trauma. 2022;25:101759. doi:10.1016/j.jcot.2021.101759
15. Glass GE, Chan JK, Freidin A, Feldmann M, Horwood NJ, Nanchahal J. TNF-alpha promotes fracture repair by augmenting the recruitment and differentiation of muscle-derived stromal cells. Proc Natl Acad Sci U S A. 2011;108(4):1585–1590. doi:10.1073/pnas.1018501108
16. David JP, Schett G. TNF and bone. Curr Dir Autoimmun. 2010;11:135–144. doi:10.1159/000289202
17. Lyras DN, Kazakos K, Verettas D, et al. The effect of platelet-rich plasma gel in the early phase of patellar tendon healing. Arch Orthop Trauma Surg. 2009;129(11):1577–1582. doi:10.1007/s00402-009-0935-4
18. Lyras DN, Kazakos K, Verettas D, et al. The influence of platelet-rich plasma on angiogenesis during the early phase of tendon healing. Foot Ankle Int. 2009;30(11):1101–1106. doi:10.3113/fai.2009.1101
19. Lange J, Sapozhnikova A, Lu C, et al. Action of IL-1beta during fracture healing. J Orthop Res. 2010;28(6):778–784. doi:10.1002/jor.21061
20. Lee Y-M, Fujikado N, Manaka H, Yasuda H, Iwakura Y. IL-1 plays an important role in the bone metabolism under physiological conditions. Int Immunol. 2010;22(10):805–816. doi:10.1093/intimm/dxq431
21. Lange J, Sapozhnikova A, Lu C, et al. Action of IL-1 beta during Fracture Healing. J Orthop Res. 2009;28:778–784. doi:10.1002/jor.21061
22. Spindler KP, Murray MM, Carey JL, Zurakowski D, Fleming BC. The use of platelets to affect functional healing of an anterior cruciate ligament (ACL) autograft in a caprine ACL reconstruction model. J Orthop Res. 2009;27(5):631–638. doi:10.1002/jor.20785
23. Murray MM, Spindler KP, Abreu E, et al. Collagen-platelet rich plasma hydrogel enhances primary repair of the porcine anterior cruciate ligament. J Orthop Res. 2007;25(1):81–91. doi:10.1002/jor.20282
24. Coates BA, McKenzie JA, Yoneda S, Silva MJ. Interleukin-6 (IL-6) deficiency enhances intramembranous osteogenesis following stress fracture in mice. Bone. 2021;143:115737. doi:10.1016/j.bone.2020.115737
25. Palmisano B, Riminucci M, Karsenty G. Interleukin-6 signaling in osteoblasts regulates bone remodeling during exercise. Bone. 2023;176:116870. doi:10.1016/j.bone.2023.116870
26. Alves R, Grimalt R. A Review of Platelet-Rich Plasma: history, Biology, Mechanism of Action, and Classification. Skin Appendage Disord. 2018;4(1):18–24. doi:10.1159/000477353
27. Taschieri S, Lolato A, Ofer M, Testori T, Francetti L, Del Fabbro M. Immediate post-extraction implants with or without pure platelet-rich plasma: a 5-year follow-up study. Oral Maxillofac Surg. 2017;21(2):147–157. doi:10.1007/s10006-017-0609-2
28. Georgakopoulos I, Tsantis S, Georgakopoulos P, et al. The impact of Platelet Rich Plasma (PRP) in osseointegration of oral implants in dental panoramic radiography: texture based evaluation. Clin Cases Miner Bone Metab. 2014;11(1):59–66.
29. Marx RE. Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg. 2004;62(4):489–496. doi:10.1016/j.joms.2003.12.003
30. Kao HK, Chen B, Murphy GF, Li Q, Orgill DP, Guo L. Peripheral blood fibrocytes: enhancement of wound healing by cell proliferation, re-epithelialization, contraction, and angiogenesis. Ann Surg. 2011;254(6):1066–1074. doi:10.1097/SLA.0b013e3182251559
31. Casati L, Celotti F, Negri-Cesi P, Sacchi MC, Castano P, Colciago A. Platelet derived growth factor (PDGF) contained in Platelet Rich Plasma (PRP) stimulates migration of osteoblasts by reorganizing actin cytoskeleton. Cell Adh Migr. 2014;8(6):595–602. doi:10.4161/19336918.2014.972785
32. Kinoshita H, Orita S, Inage K, et al. Freeze-Dried Platelet-Rich Plasma Induces Osteoblast Proliferation via Platelet-Derived Growth Factor Receptor-Mediated Signal Transduction. Asian Spine J. 2020;14(1):1–8. doi:10.31616/asj.2019.0048
33. Ng F, Boucher S, Koh S, et al. PDGF, TGF-beta, and FGF signaling is important for differentiation and growth of mesenchymal stem cells (MSCs): transcriptional profiling can identify markers and signaling pathways important in differentiation of MSCs into adipogenic, chondrogenic, and osteogenic lineages. Blood. 2008;112(2):295–307. doi:10.1182/blood-2007-07-103697
34. Kreja L, Brenner RE, Tautzenberger A, et al. Non-resorbing osteoclasts induce migration and osteogenic differentiation of mesenchymal stem cells. J Cell Biochem. 2010;109(2):347–355. doi:10.1002/jcb.22406
35. Dumic-Cule I, Peric M, Kucko L, Grgurevic L, Pecina M, Vukicevic S. Bone morphogenetic proteins in fracture repair. Int Orthop. 2018;42(11):2619–2626. doi:10.1007/s00264-018-4153-y
36. Lademann F, Hofbauer LC, Rauner M. The Bone Morphogenetic Protein Pathway: the Osteoclastic Perspective. Front Cell Dev Biol. 2020;8:586031. doi:10.3389/fcell.2020.586031
37. Wrana JL, Maeno M, Hawrylyshyn B, Yao KL, Domenicucci C, Sodek J. Differential effects of transforming growth factor-beta on the synthesis of extracellular matrix proteins by normal fetal rat calvarial bone cell populations. J Cell Biol. 1988;106(3):915–924. doi:10.1083/jcb.106.3.915
38. Bonewald LF, Mundy GR. Role of transforming growth factor-beta in bone remodeling. Clin Orthop Relat Res. 1990.
39. Jain NK, Gulati M. Platelet-rich plasma: a healing virtuoso. Blood Res. 2016;51(1):3–5. doi:10.5045/br.2016.51.1.3
40. Beck LS, DeGuzman L, Lee WP, Xu Y, Siegel MW, Amento EP. One systemic administration of transforming growth factor-beta 1 reverses age- or glucocorticoid-impaired wound healing. J Clin Invest. 1993;92(6):2841–2849. doi:10.1172/jci116904
41. Wrotniak M, Bielecki T, Gaździk TS. Current opinion about using the platelet-rich gel in orthopaedics and trauma surgery. Ortop Traumatol Rehabil. 2007;9(3):227–238.
42. Mohan S, Baylink DJ. IGF-binding proteins are multifunctional and act via IGF-dependent and -independent mechanisms. J Endocrinol. 2002;175(1):19–31. doi:10.1677/joe.0.1750019
43. Joseph BK, Savage NW, Daley TJ, Young WG. In situ hybridization evidence for a paracrine/autocrine role for insulin-like growth factor-I in tooth development. Growth Factors. 1996;13(1–2):11–17. doi:10.3109/08977199609034563
44. Noh KC, Park SH, Yang CJ, Lee GW, Kim MK, Kang YH. Involvement of synovial matrix degradation and angiogenesis in oxidative stress-exposed degenerative rotator cuff tears with osteoarthritis. J Shoulder Elbow Surg. 2018;27(1):141–150. doi:10.1016/j.jse.2017.08.007
45. van der Bijl I, Vlig M, Middelkoop E, de Korte D. Allogeneic platelet-rich plasma (PRP) is superior to platelets or plasma alone in stimulating fibroblast proliferation and migration, angiogenesis, and chemotaxis as relevant processes for wound healing. Transfusion. 2019;59(11):3492–3500. doi:10.1111/trf.15535
46. Zhang L, Qiu H, Wang D, et al. Enhanced vascularization and biocompatibility of rat pancreatic decellularized scaffolds loaded with platelet-rich plasma. J Biomater Appl. 2020;35(3):313–330. doi:10.1177/0885328220933890
47. Shibuya M. Vascular Endothelial Growth Factor (VEGF) and Its Receptor (VEGFR) Signaling in Angiogenesis: a Crucial Target for Anti- and Pro-Angiogenic Therapies. Genes Cancer. 2011;2(12):1097–1105. doi:10.1177/1947601911423031
48. Behr B, Tang C, Germann G, Longaker MT, Quarto N. Locally applied vascular endothelial growth factor A increases the osteogenic healing capacity of human adipose-derived stem cells by promoting osteogenic and endothelial differentiation. Stem Cells. 2011;29(2):286–296. doi:10.1002/stem.581
49. Hu K, Olsen BR. The roles of vascular endothelial growth factor in bone repair and regeneration. Bone. 2016;91:30–38. doi:10.1016/j.bone.2016.06.013
50. Yang Y-Q, Tan -Y-Y, Wong R, Wenden A, Zhang L-K, Rabie ABM. The role of vascular endothelial growth factor in ossification. Int J Oral Sci. 2012;4(2):64–68. doi:10.1038/ijos.2012.33
51. Kim ES, Kim JJ, Park EJ. Angiogenic factor-enriched platelet-rich plasma enhances in vivo bone formation around alloplastic graft material. J Adv Prosthodont. 2010;2(1):7–13. doi:10.4047/jap.2010.2.1.7
52. Ball SG, Shuttleworth CA, Kielty CM. Mesenchymal stem cells and neovascularization: role of platelet-derived growth factor receptors. J Cell Mol Med. 2007;11(5):1012–1030. doi:10.1111/j.1582-4934.2007.00120.x
53. Massberg S, Konrad I, Schürzinger K, et al. Platelets secrete stromal cell-derived factor 1alpha and recruit bone marrow-derived progenitor cells to arterial thrombi in vivo. J Exp Med. 2006;203(5):1221–1233. doi:10.1084/jem.20051772
54. Chesney CM, Pifer DD, Byers LW, Muirhead EE. Effect of platelet-activating factor (PAF) on human platelets. Blood. 1982;59(3):582–585.
55. Mehta SK, Tucci MA, Benghuzzi HA. Effect of platelet dense granule contents upon osteoblast viability. Biomed Sci Instrum. 2012;48:288–295.
56. McManus LM, Pinckard RN. PAF, a putative mediator of oral inflammation. Crit Rev Oral Biol Med. 2000;11(2):240–258. doi:10.1177/10454411000110020701
57. Mishra A, Woodall J, Vieira A. Treatment of tendon and muscle using platelet-rich plasma. Clin Sports Med. 2009;28(1):113–125. doi:10.1016/j.csm.2008.08.007
58. Golebiewska EM, Poole AW. Platelet secretion: from haemostasis to wound healing and beyond. Blood Rev. 2015;29(3):153–162. doi:10.1016/j.blre.2014.10.003
59. Hashikawa T, Takedachi M, Terakura M, et al. Involvement of CD73 (ecto-5’-nucleotidase) in adenosine generation by human gingival fibroblasts. J Dent Res. 2003;82(11):888–892. doi:10.1177/154405910308201108
60. Marx RE. Platelet-rich plasma (PRP): what is PRP and what is not PRP? Implant Dent. 2001;10(4):225–228. doi:10.1097/00008505-200110000-00002
61. Graziani F, Ivanovski S, Cei S, Ducci F, Tonetti M, Gabriele M. The in vitro effect of different PRP concentrations on osteoblasts and fibroblasts. Clin Oral Implants Res. 2006;17(2):212–219. doi:10.1111/j.1600-0501.2005.01203.x
62. Mazzucco L, Balbo V, Cattana E, Guaschino R, Borzini P. Not every PRP-gel is born equal Evaluation of growth factor availability for tissues through four PRP-gel preparations: fibrinet®, RegenPRP-Kit®, Plateltex® and one manual procedure. Vox Sanguinis. 2009;97(2):110–118. doi:10.1111/j.1423-0410.2009.01188.x
63. López S, Vilar JM, Sopena JJ, et al. Assessment of the Efficacy of Platelet-Rich Plasma in the Treatment of Traumatic Canine Fractures. Int J Mol Sci. 2019;20(5). doi:10.3390/ijms20051075
64. Jovani-Sancho M, Sheth CC, Marqués-Mateo M, Puche-Torres M. Platelet-Rich Plasma: a Study of the Variables that May Influence Its Effect on Bone Regeneration. Clin Implant Dentistry Relat Res. 2016;18(5):1051–1064. doi:10.1111/cid.12361
65. Al-Hamed FS, Abu-Nada L, Rodan R, et al. Differences in platelet-rich plasma composition influence bone healing. J Clin Periodontol. 2021;48(12):1613–1623. doi:10.1111/jcpe.13546
66. Kawasumi M, Kitoh H, Siwicka KA, Ishiguro N. The effect of the platelet concentration in platelet-rich plasma gel on the regeneration of bone. J Bone Joint Surg Br. 2008;90(7):966–972. doi:10.1302/0301-620x.90b7.20235
67. Chen L, Yang X, Huang G, et al. Platelet-rich plasma promotes healing of osteoporotic fractures. Orthopedics. 2013;36(6):e687–94. doi:10.3928/01477447-20130523-10
68. Choi BH, Zhu SJ, Kim BY, Huh JY, Lee SH, Jung JH. Effect of platelet-rich plasma (PRP) concentration on the viability and proliferation of alveolar bone cells: an in vitro study. Int J Oral Maxillofac Surg. 2005;34(4):420–424. doi:10.1016/j.ijom.2004.10.018
69. DeLong JM, Russell RP, Mazzocca AD. Platelet-rich plasma: the PAW classification system. Arthroscopy. 2012;28(7):998–1009. doi:10.1016/j.arthro.2012.04.148
70. Yamaguchi R, Terashima H, Yoneyama S, Tadano S, Ohkohchi N. Effects of platelet-rich plasma on intestinal anastomotic healing in rats: PRP concentration is a key factor. J Surg Res. 2012;173(2):258–266. doi:10.1016/j.jss.2010.10.001
71. Laver L, Marom N, Dnyanesh L, Mei-Dan O, Espregueira-Mendes J, Gobbi A. PRP for Degenerative Cartilage Disease: a Systematic Review of Clinical Studies. Cartilage. 2017;8(4):341–364. doi:10.1177/1947603516670709
72. Fernández-Medina T, Vaquette C, Ivanovski S. Systematic Comparison of the Effect of Four Clinical-Grade Platelet Rich Hemoderivatives on Osteoblast Behaviour. Int J Mol Sci. 2019;20(24). doi:10.3390/ijms20246243
73. Fadadu PP, Mazzola AJ, Hunter CW, Davis TT. Review of concentration yields in commercially available platelet-rich plasma (PRP) systems: a call for PRP standardization. Reg Anesth Pain Med. 2019. doi:10.1136/rapm-2018-100356
74. Mariani E, Canella V, Cattini L, et al. Leukocyte-Rich Platelet-Rich Plasma Injections Do Not Up-Modulate Intra-Articular Pro-Inflammatory Cytokines in the Osteoarthritic Knee. PLoS One. 2016;11(6):e0156137. doi:10.1371/journal.pone.0156137
75. Anitua E. Plasma rich in growth factors: preliminary results of use in the preparation of future sites for implants. Int J Oral Maxillofac Implants. 1999;14(4):529–535.
76. Kobayashi Y, Saita Y, Nishio H, et al. Leukocyte concentration and composition in platelet-rich plasma (PRP) influences the growth factor and protease concentrations. J Orthop Sci. 2016;21(5):683–689. doi:10.1016/j.jos.2016.07.009
77. Zimmermann R, Jakubietz R, Jakubietz M, et al. Different preparation methods to obtain platelet components as a source of growth factors for local application. Transfusion. 2001;41(10):1217–1224. doi:10.1046/j.1537-2995.2001.41101217.x
78. Xu Z, Yin W, Zhang Y, et al. Comparative evaluation of leukocyte- and platelet-rich plasma and pure platelet-rich plasma for cartilage regeneration. Sci Rep. 2017;7:43301. doi:10.1038/srep43301
79. Yin WJ, Xu HT, Sheng JG, et al. Advantages of Pure Platelet-Rich Plasma Compared with Leukocyte- and Platelet-Rich Plasma in Treating Rabbit Knee Osteoarthritis. Med Sci Monit. 2016;22:1280–1290. doi:10.12659/msm.898218
80. Yin W, Qi X, Zhang Y, et al. Advantages of pure platelet-rich plasma compared with leukocyte- and platelet-rich plasma in promoting repair of bone defects. J Transl Med. 2016;14(1):73. doi:10.1186/s12967-016-0825-9
81. Riboh JC, Saltzman BM, Yanke AB, Fortier L, Cole BJ. Effect of Leukocyte Concentration on the Efficacy of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis. Am J Sports Med. 2016;44(3):792–800. doi:10.1177/0363546515580787
82. Filardo G, Kon E, Pereira Ruiz MT, et al. Platelet-rich plasma intra-articular injections for cartilage degeneration and osteoarthritis: single- versus double-spinning approach. Knee Surg Sports Traumatol Arthrosc. 2012;20(10):2082–2091. doi:10.1007/s00167-011-1837-x
83. Oudelaar BW, Peerbooms JC, Huis In ‘t Veld R, Vochteloo AJH. Concentrations of Blood Components in Commercial Platelet-Rich Plasma Separation Systems: a Review of the Literature. Am J Sports Med. 2019;47(2):479–487. doi:10.1177/0363546517746112
84. Braun HJ, Kim HJ, Chu CR, Dragoo JL. The effect of platelet-rich plasma formulations and blood products on human synoviocytes: implications for intra-articular injury and therapy. Am J Sports Med. 2014;42(5):1204–1210. doi:10.1177/0363546514525593
85. Fitzpatrick J, Bulsara M, Zheng MH. The Effectiveness of Platelet-Rich Plasma in the Treatment of Tendinopathy: a Meta-analysis of Randomized Controlled Clinical Trials. Am J Sports Med. 2017;45(1):226–233. doi:10.1177/0363546516643716
86. Foster TE, Puskas BL, Mandelbaum BR, Gerhardt MB, Rodeo SA. Platelet-rich plasma: from basic science to clinical applications. Am J Sports Med. 2009;37(11):2259–2272. doi:10.1177/0363546509349921
87. Mazzocca AD, McCarthy MB, Chowaniec DM, et al. Platelet-rich plasma differs according to preparation method and human variability. J Bone Joint Surg Am. 2012;94(4):308–316. doi:10.2106/jbjs.K.00430
88. Oh JH, Kim W, Park KU, Roh YH. Comparison of the Cellular Composition and Cytokine-Release Kinetics of Various Platelet-Rich Plasma Preparations. Am J Sports Med. 2015;43(12):3062–3070. doi:10.1177/0363546515608481
89. Dejnek M, Witkowski J, Moreira H, et al. Content of blood cell components, inflammatory cytokines and growth factors in autologous platelet-rich plasma obtained by various methods. World J Orthop. 2022;13(6):587–602. doi:10.5312/wjo.v13.i6.587
90. Magalon J, Brandin T, Francois P, et al. Technical and biological review of authorized medical devices for platelets-rich plasma preparation in the field of regenerative medicine. Platelets. 2021;32(2):200–208. doi:10.1080/09537104.2020.1832653
91. Straum OK. The optimal platelet concentration in platelet-rich plasma for proliferation of human cells in vitro-diversity, biases, and possible basic experimental principles for further research in the field: a review. PeerJ. 2020;
92. Wasterlain A, Braun H, Dragoo J. Contents and Formulations of Platelet-Rich Plasma. Operat Tech Orthop. 2012;22:33–42. doi:10.1053/j.oto.2011.11.001
93. Cavallo C, Roffi A, Grigolo B, et al. Platelet-Rich Plasma: the Choice of Activation Method Affects the Release of Bioactive Molecules. Biomed Res Int. 2016;2016:6591717. doi:10.1155/2016/6591717
94. Smith OJ, Talaat S, Tomouk T, Jell G, Mosahebi A. An Evaluation of the Effect of Activation Methods on the Release of Growth Factors from Platelet-Rich Plasma. Plast Reconstr Surg. 2022;149(2):404–411. doi:10.1097/prs.0000000000008772
95. Harrison S, Vavken P, Kevy S, Jacobson M, Zurakowski D, Murray MM. Platelet activation by collagen provides sustained release of anabolic cytokines. Am J Sports Med. 2011;39(4):729–734. doi:10.1177/0363546511401576
96. Bir SC, Esaki J, Marui A, et al. Angiogenic properties of sustained release platelet-rich plasma: characterization in-vitro and in the ischemic hind limb of the mouse. J Vasc Surg. 2009;50(4):870–879.e2. doi:10.1016/j.jvs.2009.06.016
97. Zhuang YW, Zeng YM, Chen YF, et al. 不同激活剂对人富血小板血浆释放曲线的影响 [The effects of different activators on the release curve of human platelet-rich plasma]. Zhonghua Jie He He Hu Xi Za Zhi. 2018;41(11):868–872. doi:10.3760/cma.j.issn.1001-0939.2018.11.008. Chinese.
98. Toyoda T, Isobe K, Tsujino T, et al. Direct activation of platelets by addition of CaCl2 leads coagulation of platelet-rich plasma. Int J Implant Dentist. 2018;4(1):23. doi:10.1186/s40729-018-0134-6
99. Simental-Mendía M, Ortega-Mata D, Tamez-Mata Y, Olivo CAA, Vilchez-Cavazos F. Comparison of the clinical effectiveness of activated and non-activated platelet-rich plasma in the treatment of knee osteoarthritis: a systematic review and meta-analysis. Clin Rheumatol. 2023;42(5):1397–1408. doi:10.1007/s10067-022-06463-x
100. Sheen JR, Mabrouk A, Garla VV. Fracture Healing Overview. In: StatPearls. StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC.; 2023.
101. Ghiasi MS, Chen J, Vaziri A, Rodriguez EK, Nazarian A. Bone fracture healing in mechanobiological modeling: a review of principles and methods. Bone Reports. 2017;6:87–100. doi:10.1016/j.bonr.2017.03.002
102. Marsell R, Einhorn TA. The biology of fracture healing. Injury. 2011;42(6):551–555. doi:10.1016/j.injury.2011.03.031
103. Kumar V, Madsen T, Zhu H, Semple E. Stability of human thrombin produced from 11 mL of plasma using the thrombin processing device. J Extra Corpor Technol. 2005;37(4):390–395.
104. Fufa D, Shealy B, Jacobson M, Kevy S, Murray MM. Activation of platelet-rich plasma using soluble type I collagen. J Oral Maxillofac Surg. 2008;66(4):684–690. doi:10.1016/j.joms.2007.06.635
105. Mikel S, Maider B, Orlando P, et al. Isolation, Activation, and Mechanism of Action of Platelet-Rich Plasma and Its Applications for Joint Repair. In: Mahmood SC, editor. Regenerative Medicine. IntechOpen; 2019:
106. Kikuchi N, Yoshioka T, Taniguchi Y, et al. Optimization of leukocyte-poor platelet-rich plasma preparation: a validation study of leukocyte-poor platelet-rich plasma obtained using different preparer, storage, and activation methods. J Exper Orthop. 2019;6(1):24. doi:10.1186/s40634-019-0190-8
107. Ali M, Mohamed A, Ahmed HE, Malviya A, Atchia I. The use of ultrasound-guided platelet-rich plasma injections in the treatment of Hip osteoarthritis: a systematic review of the literature. J Ultrason. 2018;18(75):332–337. doi:10.15557/JoU.2018.0048
108. Lam KHS, Hung CY, Hung A. Ultrasound-Assisted Intraosseous Injection of Platelet-Rich Plasma for a Patient With Tibial Plateau Subchondral Bone Marrow Lesion: a Case Presentation and Technical Illustration. Cureus. 2020;12(12):e12312. doi:10.7759/cureus.12312
109. Sağlam G, Çetinkaya Alişar D. Ultrasound-guided versus palpation-guided platelet-rich plasma injection for the treatment of chronic lateral epicondylitis: a prospective, randomized study. Arch Rheumatol. 2023;38(1):67–74. doi:10.46497/ArchRheumatol.2023.9196
110. Carter MJ, Fylling CP, Parnell LK. Use of platelet rich plasma gel on wound healing: a systematic review and meta-analysis. Eplasty. 2011;11:e38.
111. Abdullah BJ, Atasoy N, Omer AK. Evaluate the effects of platelet rich plasma (PRP) and zinc oxide ointment on skin wound healing. Ann Med Surg. 2019;37:30–37. doi:10.1016/j.amsu.2018.11.009
112. Bolton L. Platelet-Rich Plasma: optimal Use in Surgical Wounds. Wounds. 2021;33(8):219–221.
113. Galanis V, Fiska A, Kapetanakis S, Kazakos K, Demetriou T. Effect of platelet-rich plasma combined with demineralised bone matrix on bone healing in rabbit ulnar defects. Singapore Med J. 2017;58(9):551–556. doi:10.11622/smedj.2016095
114. Jensen TB, Rahbek O, Overgaard S, Søballe K. Platelet rich plasma and fresh frozen bone allograft as enhancement of implant fixation. An experimental study in dogs. J Orthop Res. 2004;22(3):653–658. doi:10.1016/j.orthres.2003.10.006
115. Consolo U, Bertoldi C, Zaffe D. Intermittent loading improves results in mandibular alveolar distraction osteogenesis. Clin Oral Implants Res. 2006;17(2):179–187. doi:10.1111/j.1600-0501.2005.01213.x
116. Badr M, Coulthard P, Alissa R, Oliver R. The efficacy of platelet-rich plasma in grafted maxillae. A randomised clinical trial. Eur J Oral Implantol. 2010;3(3):233–244.
117. Sittinger M, Hutmacher DW, Risbud MV. Current strategies for cell delivery in cartilage and bone regeneration. Curr Opin Biotechnol. 2004;15(5):411–418. doi:10.1016/j.copbio.2004.08.010
118. Shakoor S, Kibble E, El-Jawhari JJ. Bioengineering Approaches for Delivering Growth Factors: a Focus on Bone and Cartilage Regeneration. Bioengineering. 2022;9(5):223.
119. Rodriguez IA, Growney Kalaf EA, Bowlin GL, Sell SA. Platelet-rich plasma in bone regeneration: engineering the delivery for improved clinical efficacy. Biomed Res Int. 2014;2014:392398. doi:10.1155/2014/392398
120. Lin SS, Landesberg R, Chin HS, Lin J, Eisig SB, Lu HH. Controlled release of PRP-derived growth factors promotes osteogenic differentiation of human mesenchymal stem cells. Conf Proc IEEE Eng Med Biol Soc. 2006;2006:4358–4361. doi:10.1109/iembs.2006.260847
121. Lu HH, Vo JM, Chin HS, et al. Controlled delivery of platelet-rich plasma-derived growth factors for bone formation. J Biomed Mater Res A. 2008;86(4):1128–1136. doi:10.1002/jbm.a.31740
122. Neffe AT, Loebus A, Zaupa A, Stoetzel C, Müller FA, Lendlein A. Gelatin functionalization with tyrosine derived moieties to increase the interaction with hydroxyapatite fillers. Acta Biomater. 2011;7(4):1693–1701. doi:10.1016/j.actbio.2010.11.025
123. Hokugo A, Ozeki M, Kawakami O, et al. Augmented bone regeneration activity of platelet-rich plasma by biodegradable gelatin hydrogel. Tissue Eng. 2005;11(7–8):1224–1233. doi:10.1089/ten.2005.11.1224
124. Hokugo A, Sawada Y, Hokugo R, et al. Controlled release of platelet growth factors enhances bone regeneration at rabbit calvaria. Oral Surg, Oral Med Oral Pathol Oral Radiol Endod. 2007;104(1):44–48. doi:10.1016/j.tripleo.2006.11.032
125. Kaur P, Maria A. Efficacy of platelet rich plasma and hydroxyapatite crystals in bone regeneration after surgical removal of mandibular third molars. J Maxillofac Oral Surg. 2013;12(1):51–59. doi:10.1007/s12663-012-0382-6
126. Liu X, Wang P, Chen W, Weir MD, Bao C, Xu HH. Human embryonic stem cells and macroporous calcium phosphate construct for bone regeneration in cranial defects in rats. Acta Biomater. 2014;10(10):4484–4493. doi:10.1016/j.actbio.2014.06.027
127. Qiu G, Shi Z, Hhk X, et al. Bone regeneration in minipigs via calcium phosphate cement scaffold delivering autologous bone marrow mesenchymal stem cells and platelet-rich plasma. J Tissue Eng Regen Med. 2018;12(2):e937–e948. doi:10.1002/term.2416
128. Solovieva A, Miroshnichenko S, Kovalskii A, et al. Immobilization of Platelet-Rich Plasma onto COOH Plasma-Coated PCL Nanofibers Boost Viability and Proliferation of Human Mesenchymal Stem Cells. Polymers. 2017;9(12). doi:10.3390/polym9120736
129. Kanno T, Takahashi T, Tsujisawa T, Ariyoshi W, Nishihara T. Platelet-rich plasma enhances human osteoblast-like cell proliferation and differentiation. J Oral Maxillofac Surg. 2005;63(3):362–369. doi:10.1016/j.joms.2004.07.016
130. Vahabi S, Yadegari Z, Mohammad-Rahimi H. Comparison of the effect of activated or non-activated PRP in various concentrations on osteoblast and fibroblast cell line proliferation. Cell Tissue Bank. 2017;18(3):347–353. doi:10.1007/s10561-017-9640-7
131. Slapnicka J, Fassmann A, Strasak L, Augustin P, Vanek J. Effects of activated and nonactivated platelet-rich plasma on proliferation of human osteoblasts in vitro. J Oral Maxillofac Surg. 2008;66(2):297–301. doi:10.1016/j.joms.2007.05.022
132. Martinotti S, Mazzucco L, Balbo V, et al. Platelet-rich plasma induces mixed osteogenic/osteoclastogenic phenotype in osteosarcoma SaOS-2 cells: role of TGF-beta. Curr Pharm Biotechnol. 2014;15(2):120–126. doi:10.2174/1389201015666140604121407
133. Gassling VL, Açil Y, Springer IN, Hubert N, Wiltfang J. Platelet-rich plasma and platelet-rich fibrin in human cell culture. Oral Surg, Oral Med Oral Pathol Oral Radiol Endod. 2009;108(1):48–55. doi:10.1016/j.tripleo.2009.02.007
134. Herrera BS, Coimbra LS, Bastos AS, et al. Platelet-rich plasma stimulates cytokine expression and alkaline phosphatase activity in osteoblast-derived osteosarcoma cells. Arch Oral Biol. 2012;57(9):1282–1289. doi:10.1016/j.archoralbio.2012.03.004
135. He L, Lin Y, Hu X, Zhang Y, Wu H. A comparative study of platelet-rich fibrin (PRF) and platelet-rich plasma (PRP) on the effect of proliferation and differentiation of rat osteoblasts in vitro. Oral Surg, Oral Med Oral Pathol Oral Radiol Endod. 2009;108(5):707–713. doi:10.1016/j.tripleo.2009.06.044
136. Mazzocca AD, McCarthy MB, Chowaniec DM, et al. The positive effects of different platelet-rich plasma methods on human muscle, bone, and tendon cells. Am J Sports Med. 2012;40(8):1742–1749. doi:10.1177/0363546512452713
137. Mooren RE, Hendriks EJ, van den Beucken JJ, et al. The effect of platelet-rich plasma in vitro on primary cells: rat osteoblast-like cells and human endothelial cells. Tissue Eng Part A. 2010;16(10):3159–3172. doi:10.1089/ten.tea.2009.0832
138. García-Martínez O, Reyes-Botella C, Díaz-Rodríguez L, et al. Effect of platelet-rich plasma on growth and antigenic profile of human osteoblasts and its clinical impact. J Oral Maxillofac Surg. 2012;70(7):1558–1564. doi:10.1016/j.joms.2011.06.199
139. Bi L, Cheng W, Fan H, Pei G. Reconstruction of goat tibial defects using an injectable tricalcium phosphate/chitosan in combination with autologous platelet-rich plasma. Biomaterials. 2010;31(12):3201–3211. doi:10.1016/j.biomaterials.2010.01.038
140. Zou J, Yuan C, Wu C, Cao C, Yang H. The effects of platelet-rich plasma on the osteogenic induction of bone marrow mesenchymal stem cells. Connect Tissue Res. 2014;55(4):304–309. doi:10.3109/03008207.2014.930140
141. Qi Y, Niu L, Zhao T, et al. Combining mesenchymal stem cell sheets with platelet-rich plasma gel/calcium phosphate particles: a novel strategy to promote bone regeneration. Stem Cell Res Ther. 2015;6(1):256. doi:10.1186/s13287-015-0256-1
142. Ferreira CF, Carriel Gomes MC, Filho JS, Granjeiro JM, Oliveira Simões CM, Magini Rde S. Platelet-rich plasma influence on human osteoblasts growth. Clin Oral Implants Res. 2005;16(4):456–460. doi:10.1111/j.1600-0501.2005.01145.x
143. Steller D, Herbst N, Pries R, Juhl D, Hakim SG. Positive impact of Platelet-rich plasma and Platelet-rich fibrin on viability, migration and proliferation of osteoblasts and fibroblasts treated with zoledronic acid. Sci Rep. 2019;9(1):8310. doi:10.1038/s41598-019-43798-z
144. Ogino Y, Ayukawa Y, Kukita T, Koyano K. The contribution of platelet-derived growth factor, transforming growth factor-beta1, and insulin-like growth factor-I in platelet-rich plasma to the proliferation of osteoblast-like cells. Oral Surg, Oral Med Oral Pathol Oral Radiol Endod. 2006;101(6):724–729. doi:10.1016/j.tripleo.2005.08.016
145. Vahabi S, Yadegary Z, Karamshahi M. Evaluating the adhesion of human gingival fibroblasts and MG-63 osteoblast-like cells to activated PRP-coated membranes. Cell Tissue Bank. 2019;20(3):339–349. doi:10.1007/s10561-019-09772-9
146. Celotti F, Colciago A, Negri-Cesi P, Pravettoni A, Zaninetti R, Sacchi MC. Effect of platelet-rich plasma on migration and proliferation of SaOS-2 osteoblasts: role of platelet-derived growth factor and transforming growth factor-beta. Wound Repair Regen. 2006;14(2):195–202. doi:10.1111/j.1743-6109.2006.00110.x
147. Wang X, Zhang Y, Choukroun J, Ghanaati S, Miron RJ. Effects of an injectable platelet-rich fibrin on osteoblast behavior and bone tissue formation in comparison to platelet-rich plasma. Platelets. 2018;29(1):48–55. doi:10.1080/09537104.2017.1293807
148. Chaput CD, Patel KV, Brindley GW, et al. Influence of a platelet concentrate on prosthetic bone ingrowth in a rabbit model. J Surg Orthop Adv. 2007;16(4):159–163.
149. Hernandez-Fernandez A, Vélez R, Soldado F, Saenz-Ríos JC, Barber I, Aguirre-Canyadell M. Effect of administration of platelet-rich plasma in early phases of distraction osteogenesis: an experimental study in an ovine femur model. Injury. 2013;44(7):901–907. doi:10.1016/j.injury.2012.10.018
150. Kanthan SR, Kavitha G, Addi S, Choon DS, Kamarul T. Platelet-rich plasma (PRP) enhances bone healing in non-united critical-sized defects: a preliminary study involving rabbit models. Injury. 2011;42(8):782–789. doi:10.1016/j.injury.2011.01.015
151. Kasten P, Vogel J, Geiger F, Niemeyer P, Luginbühl R, Szalay K. The effect of platelet-rich plasma on healing in critical-size long-bone defects. Biomaterials. 2008;29(29):3983–3992. doi:10.1016/j.biomaterials.2008.06.014
152. Kroese-Deutman HC, Vehof JW, Spauwen PH, Stoelinga PJ, Jansen JA. Orthotopic bone formation in titanium fiber mesh loaded with platelet-rich plasma and placed in segmental defects. Int J Oral Maxillofac Surg. 2008;37(6):542–549. doi:10.1016/j.ijom.2008.01.009
153. Kurikchy MQ, Al-Rawi NH, Ayoub RS, Mohammed SS. Histological evaluation of bone healing using organic bovine bone in combination with platelet-rich plasma (an experimental study on rabbits). Clin Oral Investig. 2013;17(3):897–904. doi:10.1007/s00784-012-0751-z
154. Lin BN, Whu SW, Chen CH, et al. Bone marrow mesenchymal stem cells, platelet-rich plasma and nanohydroxyapatite-type I collagen beads were integral parts of biomimetic bone substitutes for bone regeneration. J Tissue Eng Regen Med. 2013;7(11):841–854. doi:10.1002/term.1472
155. Lysiak-Drwal K, Dominiak M, Solski L, et al. Early histological evaluation of bone defect healing with and without guided bone regeneration techniques: experimental animal studies. Postepy Hig Med Dosw. 2008;62:282–288.
156. Malhotra A, Pelletier M, Oliver R, Christou C, Walsh WR. Platelet-rich plasma and bone defect healing. Tissue Eng Part A. 2014;20(19–20):2614–2633. doi:10.1089/ten.TEA.2013.0737
157. Molina-Miñano F, López-Jornet P, Camacho-Alonso F, Vicente-Ortega V. Plasma rich in growth factors and bone formation: a radiological and histomorphometric study in New Zealand rabbits. Braz Oral Res. 2009;23(3):275–280. doi:10.1590/s1806-83242009000300009
158. Nair MB, Varma HK, Menon KV, Shenoy SJ, John A. Reconstruction of goat femur segmental defects using triphasic ceramic-coated hydroxyapatite in combination with autologous cells and platelet-rich plasma. Acta Biomater. 2009;5(5):1742–1755. doi:10.1016/j.actbio.2009.01.009
159. Nather A, Wong KL, David V, Pereira BP. Allografts with autogenous platelet-rich plasma for tibial defect reconstruction: a rabbit study. J Orthop Surg. 2012;20(3):375–380. doi:10.1177/230949901202000324
160. Niemeyer P, Fechner K, Milz S, et al. Comparison of mesenchymal stem cells from bone marrow and adipose tissue for bone regeneration in a critical size defect of the sheep tibia and the influence of platelet-rich plasma. Biomaterials. 2010;31(13):3572–3579. doi:10.1016/j.biomaterials.2010.01.085
161. Orth M, Shadmanov T, Scheuer C, et al. Marble-derived microcalcite improves bone healing in mice osteotomy. Biomed Mater. 2018;14(2):025001. doi:10.1088/1748-605X/aaee54
162. Parizi AM, Oryan A, Shafiei-Sarvestani Z, Bigham AS. Human platelet rich plasma plus Persian Gulf coral effects on experimental bone healing in rabbit model: radiological, histological, macroscopical and biomechanical evaluation. J Mater Sci Mater Med. 2012;23(2):473–483. doi:10.1007/s10856-011-4478-1
163. Rabillard M, Grand JG, Dalibert E, Fellah B, Gauthier O, Niebauer GW. Effects of autologous platelet rich plasma gel and calcium phosphate biomaterials on bone healing in an ulnar ostectomy model in dogs. Vet Comp Orthop Traumatol. 2009;22(6):460–466. doi:10.3415/vcot-09-04-0048
164. Rai B, Oest ME, Dupont KM, Ho KH, Teoh SH, Guldberg RE. Combination of platelet-rich plasma with polycaprolactone-tricalcium phosphate scaffolds for segmental bone defect repair. J Biomed Mater Res A. 2007;81(4):888–899. doi:10.1002/jbm.a.31142
165. Sarkar MR, Augat P, Shefelbine SJ, et al. Bone formation in a long bone defect model using a platelet-rich plasma-loaded collagen scaffold. Biomaterials. 2006;27(9):1817–1823. doi:10.1016/j.biomaterials.2005.10.039
166. Simman R, Hoffmann A, Bohinc RJ, Peterson WC, Russ AJ. Role of platelet-rich plasma in acceleration of bone fracture healing. Ann Plast Surg. 2008;61(3):337–344. doi:10.1097/SAP.0b013e318157a185
167. Souza TF, Andrade AL, Ferreira GT, et al. Healing and expression of growth factors (TGF-β and PDGF) in canine radial ostectomy gap containing platelet-rich plasma. Vet Comp Orthop Traumatol. 2012;25(6):445–452. doi:10.3415/vcot-10-10-0146
168. Sugimori E, Shintani S, Ishikawa K, Hamakawa H. Effects of apatite foam combined with platelet-rich plasma on regeneration of bone defects. Dent Mater J. 2006;25(3):591–596. doi:10.4012/dmj.25.591
169. Zhang ZY, Huang AW, Fan JJ, et al. The potential use of allogeneic platelet-rich plasma for large bone defect treatment: immunogenicity and defect healing efficacy. Cell Transplant. 2013;22(1):175–187. doi:10.3727/096368912x653183
170. Canbeyli İD, Akgun RC, Sahin O, Terzi A, Tuncay İC. Platelet-rich plasma decreases fibroblastic activity and woven bone formation with no significant immunohistochemical effect on long-bone healing: an experimental animal study with radiological outcomes. J Orthop Surg. 2018;26(3):2309499018802491. doi:10.1177/2309499018802491
171. He F, Chen Y, Li J, et al. Improving bone repair of femoral and radial defects in rabbit by incorporating PRP into PLGA/CPC composite scaffold with unidirectional pore structure. J Biomed Mater Res A. 2015;103(4):1312–1324. doi:10.1002/jbm.a.35248
172. Kim YH, Furuya H, Tabata Y. Enhancement of bone regeneration by dual release of a macrophage recruitment agent and platelet-rich plasma from gelatin hydrogels. Biomaterials. 2014;35(1):214–224. doi:10.1016/j.biomaterials.2013.09.103
173. Szponder T, Wessely-Szponder J, Sobczyńska-Rak A, Żylińska B, Radzki RP, Polkowska I. Application of Platelet-rich Plasma and Tricalcium Phosphate in the Treatment of Comminuted Fractures in Animals. Vivo. 2018;32(6):1449–1455. doi:10.21873/invivo.11398
174. Shafiei-Sarvestani Z, Oryan A, Maimandi-Parizi A, Bigham Sadegh A. Histological, Biomechanical and Radiological Evaluation of Bone Repair with Human Platelet Rich Plasma in Rabbit Model. Zahedan J Res Med Sci. 2013;17.
175. Bölükbaşı N, Yeniyol S, Tekkesin MS, Altunatmaz K. The use of platelet-rich fibrin in combination with biphasic calcium phosphate in the treatment of bone defects: a histologic and histomorphometric study. Curr Ther Res Clin Exp. 2013;75:15–21. doi:10.1016/j.curtheres.2013.05.002
176. Chen H, Ji XR, Zhang Q, Tian XZ, Zhang BX, Tang PF. Effects of Calcium Sulfate Combined with Platelet-rich Plasma on Restoration of Long Bone Defect in Rabbits. Chin Med J. 2016;129(5):557–561. doi:10.4103/0366-6999.176981
177. Cho K, Kim JM, Kim MH, Kang SS, Kim G, Choi SH. Scintigraphic evaluation of osseointegrative response around calcium phosphate-coated titanium implants in tibia bone: effect of platelet-rich plasma on bone healing in dogs. Eur Surg Res. 2013;51(3–4):138–145. doi:10.1159/000357197
178. Dallari D, Fini M, Stagni C, et al. In vivo study on the healing of bone defects treated with bone marrow stromal cells, platelet-rich plasma, and freeze-dried bone allografts, alone and in combination. J Orthop Res. 2006;24(5):877–888. doi:10.1002/jor.20112
179. Emilov-Velev K, Clemente-de-Arriba C, Alobera-García M, Moreno-Sansalvador EM, Campo-Loarte J. Bone regeneration in experimental animals using calcium phosphate cement combined with platelet growth factors and human growth hormone. Rev Esp Cir Ortop Traumatol. 2015;59(3):200–210. doi:10.1016/j.recot.2014.07.011
180. Filardo G, Kon E, Tampieri A, et al. New bio-ceramization processes applied to vegetable hierarchical structures for bone regeneration: an experimental model in sheep. Tissue Eng Part A. 2014;20(3–4):763–773. doi:10.1089/ten.TEA.2013.0108
181. Gumieiro EH, Abrahão M, Jahn RS, et al. Platelet-rich plasma in bone repair of irradiated tibiae of Wistar rats. Acta Cir Bras. 2010;25(3):257–263. doi:10.1590/s0102-86502010000300007
182. Hakimi M, Grassmann JP, Betsch M, et al. The composite of bone marrow concentrate and PRP as an alternative to autologous bone grafting. PLoS One. 2014;9(6):e100143. doi:10.1371/journal.pone.0100143
183. Kasten P, Beverungen M, Lorenz H, Wieland J, Fehr M, Geiger F. Comparison of platelet-rich plasma and VEGF-transfected mesenchymal stem cells on vascularization and bone formation in a critical-size bone defect. Cells Tissues Organs. 2012;196(6):523–533. doi:10.1159/000337490
184. Kon E, Filardo G, Delcogliano M, et al. Platelet autologous growth factors decrease the osteochondral regeneration capability of a collagen-hydroxyapatite scaffold in a sheep model. BMC Musculoskelet Disord. 2010;11:220. doi:10.1186/1471-2474-11-220
185. Neves PC, Abib Sde C, Neves RF, et al. Effect of hyperbaric oxygen therapy combined with autologous platelet concentrate applied in rabbit fibula fraction healing. Clinics. 2013;68(9):1239–1246. doi:10.6061/clinics/2013(09)11
186. Oryan A, Meimandi Parizi A, Shafiei-Sarvestani Z, Bigham AS. Effects of combined hydroxyapatite and human platelet rich plasma on bone healing in rabbit model: radiological, macroscopical, hidtopathological and biomechanical evaluation. Cell Tissue Bank. 2012;13(4):639–651. doi:10.1007/s10561-011-9285-x
187. Schneppendahl J, Jungbluth P, Lögters TT, et al. Treatment of a diaphyseal long-bone defect with autologous bone grafts and platelet-rich plasma in a rabbit model. Vet Comp Orthop Traumatol. 2015;28(3):164–171. doi:10.3415/vcot-14-05-0079
188. Thorwarth M, Wehrhan F, Schultze-Mosgau S, Wiltfang J, Schlegel KA. PRP modulates expression of bone matrix proteins in vivo without long-term effects on bone formation. Bone. 2006;38(1):30–40. doi:10.1016/j.bone.2005.06.020
189. Weibrich G, Hansen T, Kleis W, Buch R, Hitzler WE. Effect of platelet concentration in platelet-rich plasma on peri-implant bone regeneration. Bone. 2004;34(4):665–671. doi:10.1016/j.bone.2003.12.010
190. Wiltfang J, Kloss FR, Kessler P, et al. Effects of platelet-rich plasma on bone healing in combination with autogenous bone and bone substitutes in critical-size defects. An animal experiment. Clin Oral Implants Res. 2004;15(2):187–193. doi:10.1111/j.1600-0501.2004.00980.x
191. Yilmaz D, Dogan N, Ozkan A, Sencimen M, Ora BE, Mutlu I. Effect of platelet rich fibrin and beta tricalcium phosphate on bone healing. A histological study in pigs. Acta Cir Bras. 2014;29(1):59–65. doi:10.1590/s0102-86502014000100009
192. Zhong D, Wang CG, Yin K, et al. In vivo ossification of a scaffold combining β-tricalcium phosphate and platelet-rich plasma. Exp Ther Med. 2014;8(5):1381–1388. doi:10.3892/etm.2014.1969
193. Akyildiz S, Soluk-Tekkesin M, Keskin-Yalcin B, et al. Acceleration of Fracture Healing in Experimental Model: platelet-Rich Fibrin or Hyaluronic Acid? J Craniofac Surg. 2018;29(7):1794–1798. doi:10.1097/scs.0000000000004934
194. Batista MA, Leivas TP, Rodrigues CJ, Arenas GC, Belitardo DR, Guarniero R. Comparison between the effects of platelet-rich plasma and bone marrow concentrate on defect consolidation in the rabbit tibia. Clinics. 2011;66(10):1787–1792. doi:10.1590/s1807-593220110007000018
195. Dülgeroglu TC, Metineren H. Evaluation of the Effect of Platelet-Rich Fibrin on Long Bone Healing: an Experimental Rat Model. Orthopedics. 2017;40(3):e479–e484. doi:10.3928/01477447-20170308-02
196. Guzel Y, Karalezli N, Bilge O, et al. The biomechanical and histological effects of platelet-rich plasma on fracture healing. Knee Surg Sports Traumatol Arthrosc. 2015;23(5):1378–1383. doi:10.1007/s00167-013-2734-2
197. Hakimi M, Jungbluth P, Sager M, et al. Combined use of platelet-rich plasma and autologous bone grafts in the treatment of long bone defects in mini-pigs. Injury. 2010;41(7):717–723. doi:10.1016/j.injury.2009.12.005
198. Jungbluth P, Wild M, Grassmann JP, et al. Platelet-rich plasma on calcium phosphate granules promotes metaphyseal bone healing in mini-pigs. J Orthop Res. 2010;28(11):1448–1455. doi:10.1002/jor.21152
199. Lucarelli E, Fini M, Beccheroni A, et al. Stromal stem cells and platelet-rich plasma improve bone allograft integration. Clin Orthop Relat Res. 2005;435:62–68. doi:10.1097/01.blo.0000165736.87628.12
200. Park HC, Kim SG, Oh JS, et al. Early Bone Formation at a Femur Defect Using CGF and PRF Grafts in Adult Dogs: a Comparative Study. Implant Dent. 2016;25(3):387–393. doi:10.1097/id.0000000000000423
201. Raafat SN, Amin RM, Elmazar MM, Khattab MM, El-Khatib AS. The sole and combined effect of simvastatin and platelet rich fibrin as a filling material in induced bone defect in tibia of albino rats. Bone. 2018;117:60–69. doi:10.1016/j.bone.2018.09.003
202. Sindel A, Dereci Ö, Toru HS, Tozoğlu S. Histomorphometric Comparison of Bone Regeneration in Critical-Sized Bone Defects Using Demineralized Bone Matrix, Platelet-Rich Fibrin, and Hyaluronic Acid as Bone Substitutes. J Craniofac Surg. 2017;28(7):1865–1868. doi:10.1097/scs.0000000000003588
203. Bibbo C, Bono CM, Lin SS. Union rates using autologous platelet concentrate alone and with bone graft in high-risk foot and ankle surgery patients. J Surg Orthop Adv. 2005;14(1):17–22.
204. Bielecki T, Gazdzik TS, Szczepanski T. Benefit of percutaneous injection of autologous platelet-leukocyte-rich gel in patients with delayed union and nonunion. Eur Surg Res. 2008;40(3):289–296. doi:10.1159/000114967
205. Calori GM, Tagliabue L, Gala L, d’Imporzano M, Peretti G, Albisetti W. Application of rhBMP-7 and platelet-rich plasma in the treatment of long bone non-unions: a prospective randomised clinical study on 120 patients. Injury. 2008;39(12):1391–1402. doi:10.1016/j.injury.2008.08.011
206. Chiang CC, Su CY, Huang CK, Chen WM, Chen TH, Tzeng YH. Early experience and results of bone graft enriched with autologous platelet gel for recalcitrant nonunions of lower extremity. J Trauma. 2007;63(3):655–661. doi:10.1097/01.ta.0000219937.51190.37
207. Dallari D, Savarino L, Stagni C, et al. Enhanced tibial osteotomy healing with use of bone grafts supplemented with platelet gel or platelet gel and bone marrow stromal cells. J Bone Joint Surg Am. 2007;89(11):2413–2420. doi:10.2106/jbjs.F.01026
208. Galasso O, Mariconda M, Romano G, et al. Expandable intramedullary nailing and platelet rich plasma to treat long bone non-unions. J Orthop Traumatol. 2008;9(3):129–134. doi:10.1007/s10195-008-0021-7
209. Gołos J, Waliński T, Piekarczyk P, Kwiatkowski K. Results of the use of platelet rich plasma in the treatment of delayed union of long bones. Ortop Traumatol Rehabil. 2014;16(4):397–406. doi:10.5604/15093492.1119617
210. Griffin XL, Achten J, Parsons N, Costa ML. Platelet-rich therapy in the treatment of patients with Hip fractures: a single centre, parallel group, participant-blinded, randomised controlled trial. BMJ Open. 2013;3(6). doi:10.1136/bmjopen-2013-002583
211. Kitoh H, Kitakoji T, Tsuchiya H, Katoh M, Ishiguro N. Distraction osteogenesis of the lower extremity in patients with achondroplasia/hypochondroplasia treated with transplantation of culture-expanded bone marrow cells and platelet-rich plasma. J Pediatr Orthop. 2007;27(6):629–634. doi:10.1097/BPO.0b013e318093f523
212. Kitoh H, Kitakoji T, Tsuchiya H, Katoh M, Ishiguro N. Transplantation of culture expanded bone marrow cells and platelet rich plasma in distraction osteogenesis of the long bones. Bone. 2007;40(2):522–528. doi:10.1016/j.bone.2006.09.019
213. Lee DH, Ryu KJ, Kim JW, Kang KC, Choi YR. Bone marrow aspirate concentrate and platelet-rich plasma enhanced bone healing in distraction osteogenesis of the tibia. Clin Orthop Relat Res. 2014;472(12):3789–3797. doi:10.1007/s11999-014-3548-3
214. Liebergall M, Schroeder J, Mosheiff R, et al. Stem cell-based therapy for prevention of delayed fracture union: a randomized and prospective preliminary study. Mol Ther. 2013;21(8):1631–1638. doi:10.1038/mt.2013.109
215. Malhotra R, Kumar V, Garg B, et al. Role of autologous platelet-rich plasma in treatment of long-bone nonunions: a prospective study. Musculoskelet Surg. 2015;99(3):243–248. doi:10.1007/s12306-015-0378-8
216. Mariconda M, Cozzolino F, Cozzolino A, D’Agostino E, Bove A, Milano C. Platelet gel supplementation in long bone nonunions treated by external fixation. J Orthop Trauma. 2008;22(5):342–345. doi:10.1097/BOT.0b013e318172cea5
217. Namazi H, Kayedi T. Investigating the Effect of Intra-articular Platelet-Rich Plasma Injection on Union: pain and Function Improvement in Patients with Scaphoid Fracture. J Hand Microsurg. 2016;8(3):140–144. doi:10.1055/s-0036-1597088
218. Namazi H, Mehbudi A. Investigating the effect of intra-articular PRP injection on pain and function improvement in patients with distal radius fracture. Orthop Traumatol Surg Res. 2016;102(1):47–52. doi:10.1016/j.otsr.2015.11.002
219. Peerbooms JC, Colaris JW, Hakkert AA, et al. No positive bone healing after using platelet rich plasma in a skeletal defect. An observational prospective cohort study. Int Orthop. 2012;36(10):2113–2119. doi:10.1007/s00264-012-1603-9
220. Samy AM. The role of platelet rich plasma in management of fracture neck femur: new insights. Int Orthop. 2016;40(5):1019–1024. doi:10.1007/s00264-015-2844-1
221. Sanchez M, Anitua E, Cugat R, et al. Nonunions treated with autologous preparation rich in growth factors. J Orthop Trauma. 2009;23(1):52–59. doi:10.1097/BOT.0b013e31818faded
222. Say F, Türkeli E, Bülbül M. Is platelet-rich plasma injection an effective choice in cases of non-union? Acta Chir Orthop Traumatol Cech. 2014;81(5):340–345.
223. Sys J, Weyler J, Van Der Zijden T, Parizel P, Michielsen J. Platelet-rich plasma in mono-segmental posterior lumbar interbody fusion. Eur Spine J. 2011;20(10):1650–1657. doi:10.1007/s00586-011-1897-0
224. Tarallo L, Mugnai R, Adani R, Catani F. Treatment of the ulna non-unions using dynamic compression plate fixation, iliac bone grafting and autologous platelet concentrate. Eur J Orthop Surg Traumatol. 2012;22(8):681–687. doi:10.1007/s00590-011-0902-y
225. Wei LC, Lei GH, Sheng PY, et al. Efficacy of platelet-rich plasma combined with allograft bone in the management of displaced intra-articular calcaneal fractures: a prospective cohort study. J Orthop Res. 2012;30(10):1570–1576. doi:10.1002/jor.22118
226. Rodriguez-Collazo ER, Urso ML. Combined use of the Ilizarov method, concentrated bone marrow aspirate (cBMA), and platelet-rich plasma (PRP) to expedite healing of bimalleolar fractures. Strategies Trauma Limb Reconstr. 2015;10(3):161–166. doi:10.1007/s11751-015-0239-x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.