")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 15
Advances in Tumour-Infiltrating Lymphocytes for Triple-Negative Breast Cancer Management
Authors Gorenšek R, Kresnik M, Takač I, Rojko T, Sobočan M
Received 25 November 2022
Accepted for publication 13 August 2023
Published 2 November 2023 Volume 2023:15 Pages 773—783
DOI https://doi.org/10.2147/BCTT.S399157
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Rok Gorenšek,1,2,* Martin Kresnik,1,3,* Iztok Takač,1,4 Tomaž Rojko,1,5 Monika Sobočan1,4
1Faculty of Medicine, University of Maribor, Maribor, Slovenia; 2Department of Oncology, University Medical Centre Maribor, Maribor, Slovenia; 3Department of Emergency Medicine, University Medical Centre Maribor, Maribor, Slovenia; 4Division of Gynecology and Perinatology, University Medical Centre Maribor, Maribor, Slovenia; 5Department of Pathology, University Medical Centre Maribor, Maribor, Slovenia
*These authors contributed equally to this work
Correspondence: Monika Sobočan, University Medical Centre Maribor, Division for Gynecology and Perinatology, Ljubljanska ulica 5, Maribor, 2000, Slovenia, Tel +386 2 321 2195, Email [email protected]
Abstract: Triple negative breast cancer (TNBC) is a subtype of breast cancer which does not express or expresses a minimum amount of estrogen receptors (ER), progesterone receptors (PR) and human epidermal growth factor receptor 2 (HER2) protein. TNBCs include a heterogenic group of cancers that are aggressive, grow rapidly and are associated with poor prognosis and overall survival, mainly attributed to a lack of effective therapeutic targets. For a long time, a major issue with predicting the outcome and prognosis of TNBCs was the lack of an accurate biomarker, a molecule that helps us objectively assess a patient’s health status. In recent times, defining the presence of tumor-infiltrating lymphocytes (TIL) is becoming an indispensable method of determining a patient’s prognosis. TILs are found in tumor tissue and the surrounding stroma and carry a prognostic value. Furthermore, they are known to improve the effect of systemic therapy. With the rise of immunotherapy, the role of TIL in this newer therapeutic option is a topic of increased importance. The goal behind this research article is a comprehensive review of the current literature on the importance of tumor-infiltrating lymphocytes in the prognosis of TNBC.
Keywords: tumor-infiltrating lymphocytes, immunotherapy, prognosis, dysfunction/exhaustion, microenvironment, immunometabolism
Introduction
Triple-negative breast cancer (TNBC) is a subtype of breast cancer that does not express or expresses a minimum amount of estrogen receptors (ER), progesterone receptors (PR) and human epidermal growth factor receptor 2 (HER2) protein.1 It’s a highly aggressive form of breast cancer, punctuated by the fact that the lack of ER, PR and HER2 renders specific endocrine therapies and target therapies obsolete. As such, chemotherapy remains the standard of care (SOC) for TNBC in regards to systemic therapy.2,3 Because of its properties, TNBC patients experience worse overall survival (OS) and progression-free survival (PFS) than those with non-TNBC.4 The 5-year survival rate of TNBC is significantly lower than that of hormone receptor-positive disease.5 In the last decade, however, a great deal of research has been done in order to improve TNBC prognosis and newer treatment options are starting to be used in clinical practice, especially immunotherapy.6
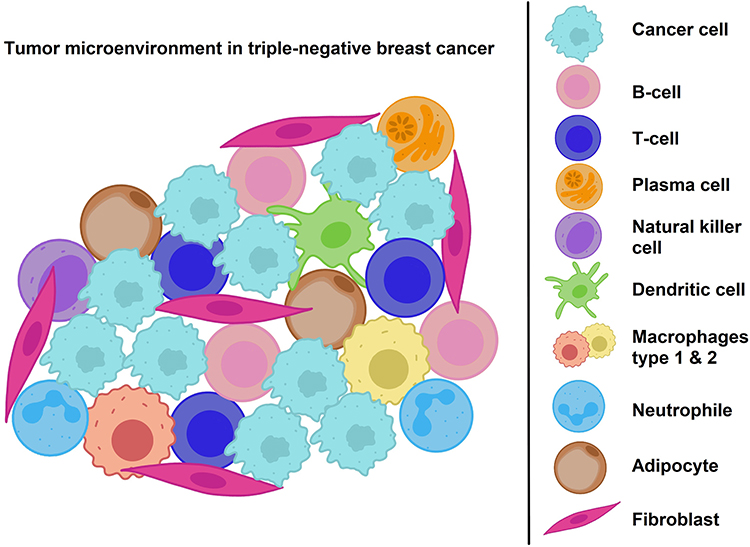 |
Figure 1 Illustration of the tumur microenvironment in triple-negative breast cancer. Notes: Data from Zhou Y, Tian Q, Wang BY, Yang J, Zhao SD, Yang J. The prognostic significance of TILs as a biomarker in triple-negative breast cancer: what is the role of TILs in TME of TNBC? Adapted from Zhou Y, Tian Q, Wang BY, Yang J, Zhao SD, Yang J. The prognostic significance of TILs as a biomarker in triple-negative breast cancer: what is the role of TILs in TME of TNBC. Eur Rev Med Pharmacol Sci. 2021;25(7):2885–2897. Creative Commons.7 |
It has been found that the immune system plays a major part in cancer progression. Transcription factors, cytokines, chemokines, and infiltrating lymphocytes heavily influence tumor growth and progression.8 Analyzing the immune response inside the tumor tissue can help us in predicting disease outcome and plan treatment. In recent years the focus has been on research into tumor-infiltrating lymphocytes (TIL), which have the greatest influence on the management of breast cancer in terms of every cell in the immune system.9,10 They function as a prognostic biomarker, as well as influence the function of chemotherapy and immunotherapy, making them highly important in the treatment of TNBC.3 As such, the aim of this study is to summarize current knowledge of TIL, their properties, their function in tumor tissue, their prevalence in breast cancer patients, and their role in the treatment and prognosis of TNBC. We will be highlighting our current understanding of TIL, as well as the gaps in our knowledge that require further research.
Discussion
Triple-Negative Breast Cancer
TNBC is currently defined as a group of tumors where less than 1% of the cells express ER and PR.3 HER2 protein is defined with the help of immunohistochemistry, where a score of 0/1+ counts as an HER2 negative tumor.11 Furthermore, if TNBCs show signs of epidermal growth factor receptor or cytokeratin 5/6 expression we can count them as part of the bigger group of “basal-like” breast cancers. TNBC represents a molecularly diverse type of breast cancer that is classified according to the revised Lehmann classification. This classification divides TNBC according to grade, local and distant disease progression, age at time of diagnosis and histopathological properties.12,13 The basal-like 1 subtype is characterized by DNA damage response gene expression and an elevated cell cycle, leading to a highly proliferative index. The basal-like 2 subtype has significant expression of growth factors and myoepithelial markers. Both basal types are common in invasive ductal carcinoma. The mesenchymal stem-like subtype expresses genes involved in epithelial mesenchymal transition, as well as genes for cell motility. It also interacts with the extracellular matrix. This molecular subtype is commonly found in medullary and metaplastic carcinoma. The last subtype is the luminal androgen receptor subtype, expressing the luminal gene and characterized by the androgen receptor. It is associated with the apocrine carcinoma. This classification is important not only because it can predict some histopathological properties of TNBC but also because it can predict how a tumor responds to therapy, especially chemotherapy.13 The main characteristics of the four molecular subtypes are shown in Table 1.
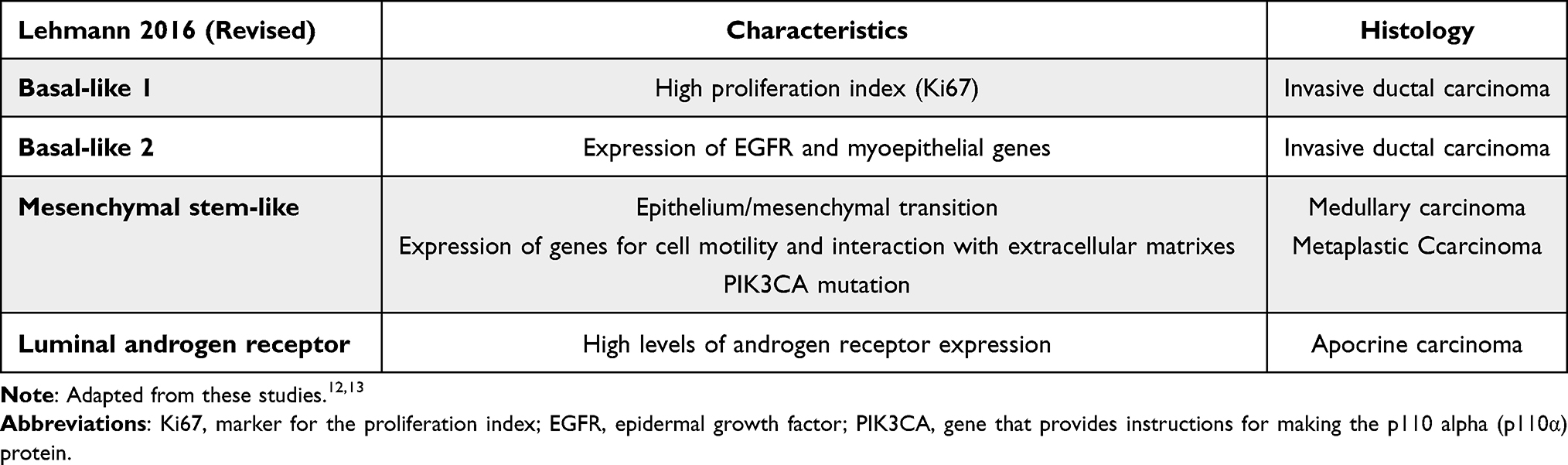 |
Table 1 Molecular Classification of TNBC |
TNBC represented more than 10% of all breast cancers diagnosed.11,14 It regularly affects younger women and is often linked with the BRCA1, BRCA2 and PALB2 gene mutations.5,11,14 TNBC predominantly affects women of African American descent and the probability of death for women of this ethnicity is almost two times higher compared to other races. Along with race, other risk factors include younger age and multiple pregnancies.15 The incidence of breast cancer is higher in developed countries.16 TNBC is linked to a higher grade, higher mitotic index and an advanced stage at diagnosis compared to other subtypes. A quick recurrence is therefore common and that leads to a poor prognosis of the disease.11 Liver, lungs and the central nervous system (CNS) are some of the organs where metastasis is most commonly observed.14 It is often linked with a high tumor mutation burden (TMB).17 Compared to non-TNBC breast cancer patients, TNBC patients experience worse overall survival (OS) and progression-free survival (PFS) rates.4 The TNBC 5-year survival rate is significantly lower than that of the hormone receptor-positive disease.5
TNBC has limited treatment options, because the lack of ER, PR and HER2 renders specific endocrine therapies and target therapies obsolete. As such, chemotherapy remains the standard of care (SOC) for TNBC in regards to systemic treatment.2,3 Prevalent chemotherapies include alkylating agents (eg, cyclophosamide), anthracycline (eg, doxorubicin), anti-microtubule agents (eg, taxane) and anti-metabolite fluorouracils (eg, 5-FU).3 Early TNBC is many times treated with neoadjuvant chemotherapy followed by surgery, which includes mastectomy or breast-conserving surgery (BCS).3,11 BCS is followed by radiotherapy and is mostly used for smaller tumors. This regimen is used in the treatment of other invasive subtypes of breast cancer as well. Mastectomy is the option of choice in more advanced tumors. In advanced TNBC, treated without surgery, the following chemotherapies are used: anti-metabolites capecitabine and gemcitabine, non-taxane microtubule inhibitor eribulin, and DNA cross-linker platinums.11 Neoadjuvant chemotherapy, in particular, has proven itself to be highly effective in improving disease prognosis, shown by the higher pathological remission rate in TNBC than in hormone receptor-positive disease.2 Relapsed/refractory TNBC, however, sees limited benefit from chemotherapy. There is no SOC, responses to treatment are often short in duration and disease relapse and metastases are common. The limited treatment options of TNBC lead to a poor prognosis.3
In the last decade, newer treatment options are starting to be used in clinical practice. Especially prevalent is immunotherapy, which is a type of biological treatment which binds to specific molecular targets to help reduce tumor mass and prevent further growth of the disease, mostly through restoring and strengthening the anti-tumor immune responses that defeat tumor cells.6 Although most of the literature we have read sees these new treatment options as a revolution in the treatment of TNBC, the current use of these agents is mostly limited to programmed cell death protein 1 positive (PD-1+) TNBC. PD-1 and its ligands programmed cell death ligand 1 (PD-L1) and programmed cell death ligand 2 (PD-L2) form a pathway/immune checkpoint that regulates inflammation and leads to inhibition of T cell activation, proliferation, function, and survival within cancer cells. PD-1 is expressed in most cells of the immune system (including lymphocytes, macrophages, natural killer cells and dendritic cells). Most importantly, however, it is highly expressed in cancer-specific T cells. It reduces the regulation of ineffective and harmful immune responses, maintains immune tolerance and is known to interfere with protective immune responses.18,19 Overexpression of PD-1/PD-L1 tumor cells can lead to silencing of the immune system and can evade anti-tumor immune responses.20 PD-L1 expression is defined by the “Combined Positive Score” (CPS) (PD-L1 IHC 22C3 pharm Dx assay), where a score of ≥1 usually represents tumors with high PD-L1 expression.21 It has been found that the PD-1/PD-L1 pathway is highly expressed in TNBC, which is why immunotherapies targeting this specific pathway have been explored, leading to the use of immune-checkpoint inhibitors (ICIs). Following the results of the Impassion 130 trial (NCT02425891) in 2019, the combination approach with atezolizumab and nab-paclitaxel predicted a better prognosis in metastatic patients and was approved by the US Food and Drug administration (FDA) as a first-line treatment in patients with unresectable, locally advanced or metastatic PD-L1-positive TNBC and remains the SOC for these patients. This survival benefit is only seen in PD-L1 positive TNBC patients.3,22 Another ICI, pembrolizumab, was approved in July 2021 following the results of the KEYNOTE-522 study. The trial showed higher pathological complete remission (pCR) rates in stage II or III TNBC patients receiving pembrolizumab along with chemotherapy than in those receiving chemotherapy alone. The percentage of patients without disease progression after 18 months and 36-month event-free survival (EFS) was also higher in the pembrolizumab group.22 In this regimen, immunotherapy is used in combination with chemotherapy as neoadjuvant treatment and continued after surgery as a monotherapy.23 When pembrolizumab was used as a monotherapy in second- or third-line treatment, however, it did not demonstrate superior OS compared to chemotherapy.24 Lastly, olaparib and talazoparib were approved by the FDA in 2018 to treat patients with advanced stage HER2-negative breast cancer and a positive BRCA1 or BRCA2 mutation. Along with olaparib and talazoparib, the diagnostic test to identify germline BRCA-mutated (gBRCAm) breast cancers was also approved. Both immunotherapies showed an increased median PFS in comparison to a physician’s choice of standard therapy and an improved side-effect profile in patient-reported outcomes.3
De-Escalation Therapy
With the recent therapeutic advancements in TNBC whereby newer and more aggressive chemotherapies, immunotherapies and targeted therapies are becoming available, it is important to consider the value of each for the patient. Modern treatment options have helped us to improve the life expectancy of patients with TNBC, but have also increased the chance of side effects. As we enter the era of a more personalized approach to cancer treatment, it has become clear that not all patients profit from or want such aggressive treatment. In the past, we have already de-escalated many radical surgical procedures and could do so for systemic treatment in the future, mainly focusing on using less toxic treatments. Currently, almost every patient receives neoadjuvant or adjuvant chemotherapy as it decreases the chance of recurrence and improves OS. This regimen was proven to be beneficial for patients with aggressive cancer and a high chance of recurrence. Patients with low recurrence rates, however, often see few benefits and experience more toxicities and side effects from this aggressive style of treatment. Therefore, modern medicine strives for a more personalized approach which considers comorbidities, patients’ age and fitness level and focuses more on patients’ quality of life. To identify patients who would benefit from de-escalation treatment, a reliable biomarker is needed.22 Among the possible candidates, we believe TIL could be what we are searching for, which we will be discussing later in this article.
Tumor-Infiltrating Lymphocytes
The immune system plays a major role in cancer progression and prognosis. In the tumor micro-environment (TME) of TNBC the most prominent cells of the immune system are lymphocytes. T lymphocytes comprise around 60% (20% cytotoxic CD8+ T cells and 40% helper CD4+ T cells, CTL and Th cells) of the immune cells of the TME, followed by B cells (20%), natural killer (NK) cells (5%) and macrophages (5%), while the remaining cells are dendritic cells (<1%) (Figure 1).25 Out of all the TME cells, the greatest effect on disease progression and prognosis has been shown with T lymphocytes, amongst all other cells of the immune system.9 T lymphocytes are divided into specific subsets, with different functions in our immune system. We classify the T-cells based on their T cell receptor (TCR sub-unit) and core lineage markers, CD8 and CD4. The αβ TCR complex, in particular, allows the T cells to recognize the major histocompatibility complex (MHC) of target cells. Their main function is terminating infected cells and cancerous cells. CD4+ T lymphocytes encourage antigen presentation, while the cytotoxic CD8+ T lymphocytes directly attack tumor cells as part of the cell-mediated immune response.9,26 Their targets are, predominantly, cells that express the MHC type 1 on their surface.9 Through the secretion of IFN-γ they inhibit the cell cycle and induce cell death. Furthermore, they contribute to macrophage activation.27–29 CD4 T cells can be further divided into CD4 helper cells, which assist CD8 T cells and regulatory CD4 T lymphocytes (T-regs), which regulate tissue inflammation. The function of T-regs is to suppress pathogenic immune responses and to maintain immune homeostasis. With this, they also prevent the development of autoimmunity. They are defined by fork head box P3 (FOXP3) protein expression.30 The TIL infiltrate in TNBC is mostly made up of CD8 T cell infiltrates, leading to their positive prognostic role.31
Assessing TIL
Defining the TIL infiltrate has become an important part of the management of TNBC, due to their role as a strong prognostic biomarker.21 According to the National Cancer Institute (NIH), a biomarker is a biological molecule found in blood, other body fluids, or tissues that is a sign of a normal or abnormal process, or of a condition or disease. A biomarker may be used to see how well the body responds to a treatment for a disease or condition. It is also called a molecular marker or signature molecule.32 According to the FDA-NIH Biomarker Working Group, a prognostic biomarker is one that indicates an increased (or decreased) likelihood of a future clinical event, disease recurrence or progression in an identified population. Prognostic biomarkers are measured at a defined baseline, which may include a background treatment.33 As such, the TIL infiltrate in TNBC is often identified and assessed by pathologists following a standardized set of guidelines first described by Salgaod R. et al in 2015, where they detail both methodological and technological recommendations for evaluating TIL in breast cancer.34 For this purpose, archival formalin-fixed paraffin-embedded (FFPE) tissue is used, stained with hematoxylin and eosin and then observed using light microscopy. Pathologists can then reference a set of reference images, which are published by the International Immuno-Oncology Biomarker Working Group (www.tilsinbreastcancer.org) also known as the TIL working group (TIL-WG). Different zones with different TIL densities are assessed in each tumor, after which a mean of the fields is calculated forming the final TIL score, where the stromal TIL infiltration is expressed in percentages (%). The process is similar to processes for other biomarkers in breast cancer. This standardized set of guidelines leads to excellent interobserver concordance and reproducibility between pathologists, throughout the world.21 Defining TIL in TNBC is still not done routinely, as they do not directly influence tumor staging or choice of therapy. There are however some similar prognostic markers, such as lymphovascular invasion and histological grade, which are routinely included in a pathology report. And with TIL seeming to be able to predict response to ICI, TIL quantity could be considered when staging a tumor in future.34
Value of TIL as Biomarkers in TNBC
In the last decade TIL have been identified as having a positive prognostic role in breast cancer. Furthermore, the influence of TIL on disease prognosis was found to be more significant in TNBC compared to the hormone-positive disease. A bigger TIL infiltration, in patients with TNBC, is a predictor of pCR, disease-free survival (DFS), better OS and better long-term prognosis.20,35 On average, women with basal-like TNBC and CD8+ T lymphocyte presence live 3.5 years longer than those without a CD8+ T lymphocyte infiltrate.31 The effect of TIL on disease prognosis was proven to be significant in early TNBC36 and even in the advanced setting, although not to the same extent.37 In most studies a TIL quantity of 30% and higher was associated with better prognosis and marked as a high TIL tumor.21 In younger patients however the positive prognostic effect was seen even with lower quantities of TIL, leading us to question what the cut off for a high TIL tumor should be.38 Among the TIL subsets, CD8+ lymphocytes are particularly associated with better patient survival in basal like subgroup.9,31 The CD8+ infiltrates have been associated with a better response to therapy as well.39 The role of CD4+ and FOXP3+ infiltrates is still unclear as studies have associated them with both a positive35 and a potentially negative prognostic role.40,41 It is believed that the negative prognostic role of FOXP3+ infiltrates, in particular, could be because of a suppression of the activation of CD8 T cells and CD4 helper T cells.40,41 Despite this effect, most studies find TIL to be a clear positive prognostic marker in TNBC.20 This may be because the TIL infiltrate in TNBC is mostly made up of CD8 T cell infiltrates rather than CD4 T cell infiltrates.31
A positive prognostic role was also shown when predicting response to chemotherapy, which has shown a significantly better effect in TNBC with a large TIL infiltration. In patients with TNBC who were treated with adjuvant anthracycline chemotherapy, the presence of TIL predicted improved OS, DFS and a distant-recurrence free interval (DRFI).42 Part of this effect could be contributed to the fact that some chemotherapeutic drugs were shown to able to induce stress proteins during cell death, which helps with immune recognition of the tumor. For example, doxorubicin can induce secretion of the protein high-mobility-group box 1 (HMGB1), which binds to toll-like receptor (TLR) 4. Together, they promote antigen presentation, T-cell activation, and secretion of IFN-μ. Other chemotherapeutics have shown similar effects. Paclitaxel can increase tumor infiltrating type 1 T lymphocytes and anthracyclines are proven to bolster the type 1 immune response. This means that chemotherapy seems to partly operate as an immunotherapy along with its cytotoxic effect.40 Chemotherapy has been shown to stimulate an immune response against tumor cells, leading to a more significant reduction in tumor mass, which may be the reason it shows good results when combined with immunotherapy.26,43
The increased prognostic value of TIL in TNBC is most likely because it is naturally a subtype with a high level of lymphocyte infiltrate.26,43 TNBC is the subtype with the biggest incidence of invasive tumors, with a lymphocyte infiltration bigger than 50% (lymphocyte predominant breast cancer, LPBC) at the time of diagnosis (20%). Compared to the average of around 11%, it shows a significant difference to other subgroups. The remaining 80% of TNBCs did show at least a partial infiltration with immune cells, either in the tumor itself or the surrounding stroma. The greatest effect on overall survival can be seen with LPBC, which further indicates that a higher TIL infiltration predicts an enhanced effect of chemotherapy.26 In fact, neoadjuvant chemotherapy of carboplatin and anthracycline-plus-taxane combination resulted in a significantly higher pCR rate in LPBC than in non-LPBC (59.9 and 33.8%), respectively.44
Despite the role of TIL as prognostic biomarkers in TNBC, they currently do not influence patient management, as the SOC for most early TNBC remains cytotoxic chemotherapy, regardless of TIL count.3 In comparison to a predictive biomarker (a biomarker used to identify individuals who are more likely than similar individuals without the biomarker to experience a favorable or unfavorable effect from exposure to a medical product or an environmental agent),33 a prognostic marker like TIL has a more subtle and complex role when/if guiding clinicians’ decisions about therapy. In light of this issue, many prognostic tools that incorporate the anatomic stage along with TIL count have been developed. A few examples of this are UK Predict and Adjuvant Online, as well as the prognostic tool developed by the TIL-WG. As of late, TIL are also included in several international guidelines about early-stage TNBC, like the European Society of Medical Oncology (ESMO) Guidelines for early-stage breast cancer as well as the World Health Organization (WHO) Blue Book on breast tumor classification.21
TIL could also help with identifying patients for systemic therapy de-escalation, due to their association with better pCR rates, response to chemotherapy and overall prognosis. As such, they help us in terms of finding patients with a lower chance of recurrence and consequently not needing such aggressive treatment, thus lessening the burden of side effects and improving quality of life. We believe that TIL are currently the most cost-effective, accessible and reliable biomarkers for identifying patients for de-escalation therapy.
Furthermore, TIL are developing a more important role in deciding on a patient’s therapy, as we enter the immune-checkpoint era.
Role of TIL in the Immune-Checkpoint Era
Immune-checkpoint inhibitors are becoming of increased importance in the management of TNBC, even establishing themselves as the SOC for some patients in the advanced setting.3 In combination with chemotherapy, they show promising results in the early stage disease as well. Three recent studies report benefit from using immunotherapy in combination with chemotherapy as a neoadjuvant treatment, namely, the KEYNOTE-522, IMpassion031, and GeparNUEVO studies,7 suggesting a synergetic effect between them. It has become clear that immunotherapy, especially ICI, will become the standard when treating TNBC in the future. As such, there is a need to find a suitable biomarker to help identify patients who respond to immunotherapy and also predicts a good response to chemotherapy. Currently, TIL are showing promising results. TIL have been found to predict high PD-L1 expression and a favorable response to immunotherapy.20,21 The number of TIL has been found as an predictive marker for a response to immune checkpoint blockade (ICB).17 Along with high PD-L1 expression, a high TIL infiltrate was shown to predict a higher chance of responding to pembrolizumab in patients with advanced and metastatic TNBC.14,21 Furthermore, in patients with high PD-L1 expression and high TIL infiltration (≥5%), pembrolizumab was even associated with better survival than chemotherapy. In patients with low TIL infiltration, however, chemotherapy was associated with a better survival. Higher TIL infiltration (≥5%) showed increased benefit of PCR and OS in patients receiving atezolizumab as well.21 The data suggest a more significant anti-tumor immune response with a higher TIL infiltration present, leading to an increased elimination of cancer cells. TIL/PD-L1 appear to be predictive of benefit from PD-L1 inhibition, at least in the advanced setting, which is why Loi et al already believe that the ideal treatment for PD-L1+, CD8+ or TIL+ advanced TNBC would be atezolizumab and nab-paclitaxel up-front. In early-stage TNBC, neoadjuvant treatment of tumors with a higher TIL/PD-L1 expression was linked to higher rates of pCR, regardless of using chemotherapy as a monotherapy or the addition of immunotherapy, although more research still needs to be done.21
We can also speculate that the role TIL play in immunotherapy will only increase in the future, given it is still in the early stages and warrants further research into the underlying mechanisms and properties, not only in TNBC but in other cancers as well. Some of the newest currently ongoing research in the field of TNBC, TIL and immunotherapy are listed in Table 2. Most of the studies listed are researching the effects of immunotherapy on TNBC progression and prognosis. As well as drugs such as nivolumab, pembrolizumab and atezolizumab, which are already approved for use with TNBC patients in some settings, they are testing the efficacy of newer drugs like cabiralizumab. The drugs mentioned are tested mostly as a neoadjuvant treatment combination with chemotherapy in both the early and advanced stages of the disease. Other studies are focusing more on the role of the TME and TIL in TNBC. One study is researching the effect of autologous TIL in pretreated metastatic TNBC. TIL have shown benefits even in advanced disease,37 which makes this an important topic of research to find a potential better treatment option for metastatic TNBC.
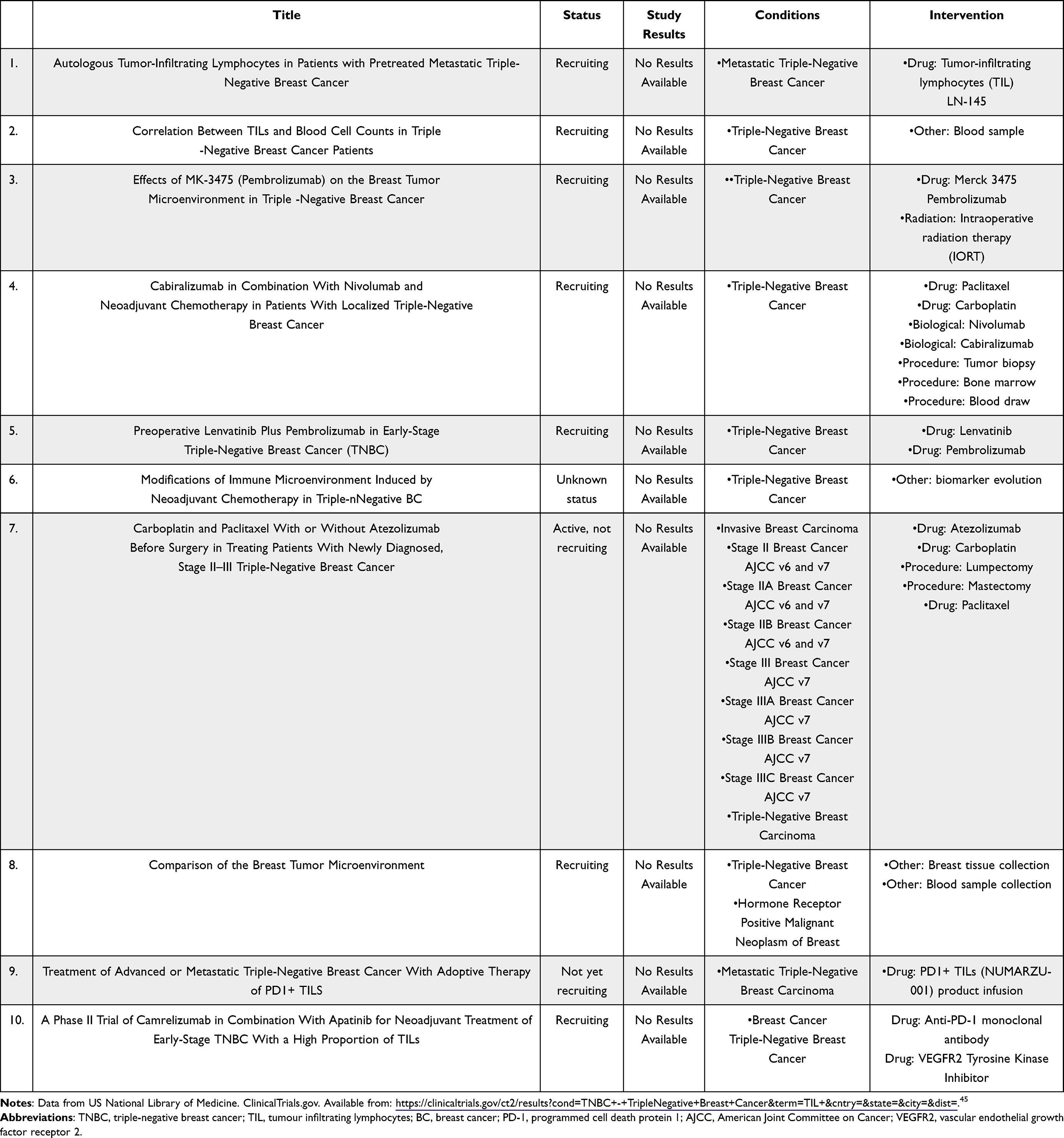 |
Table 2 Some of the Newest Currently Ongoing Research in the Field of TNBC, TIL and Immunotherapy |
Conclusion
Through a review of the current literature we found that TIL have several strengths, making them vital for managing TNBC:
- TIL are currently one of the most reliable prognostic biomarkers in TNBC. They have been linked with an improved clinical outcome in TNBC and a better response to systemic treatment of TNBC.20,35 TILs have the strongest association to breast cancer outcome in TNBC.31 A high number of TIL was asociated with a better DFS and better OS,20,35 in one study even with a better pCR.35 Chemotherapy has been asociated with a increased chance of pCR and improved survival with increased TILs in TNBC25 TIL infiltration is undeniably an independent prognostic marker, that has shown clinical significance even in large-scale meta-analysis.20,35,36
- Patients with a high TIL infiltration were proven to have a lower risk of recurrence and are associated with better pCR rates after neoadjuvant therapy, even in early stage TNBC, making them effective in identifying potential candidates for therapy de-escalation.22
- TIL seem to predict benefit from using immunotherapy, with some researchers advocating that all patients with advanced TNBC who are PD-L1+, CD8+, or TIL+ should receive atezolizumab and nab-paclitaxel.21 As such, TIL could already be seen as not only prognostic biomarkers but predictive ones as well. Additionally, with immunotherapy’s advancement in the future, the role of TIL when planning a patient’s treatment will only grow in the future.
- Defining TIL or a specific subset of TIL (eg, CD8+) on a hematoxylin and eosin slide is relatively cost-effective and done routinely throughout the world; they could therefore replace PD-L1 assays as a companion diagnostic test for atezolizumab and pembrolizumab for patients with advanced TNBC.21
- As it is becoming clear that a combination approach of chemotherapy and immunotherapy will most likely become the standard treatment of TNBC in future, it is vital to use a biomarker that predicts a good response to both. At the time of writing this article, TIL fit this role better than any other potential biomarker, further increasing their importance in the management of TNBC.
Also accounting for the fact that we already routinely include some similar prognostic markers like lymphovascular invasion and histological grade, we firmly believe that TNBC patients would benefit greatly from routinely defining TIL or a specific TIL subset (eg, CD8+). Because of their important role in TNBC management it is also vital to expand our knowledge of TIL in the future, as there is much room for improvement. We still need to define the different TIL subsets, their different effects, and their layout in cancer tissue. Our current understanding about the TME and the interaction of TIL with other cells of the TME is still lacking. Though we know the general composition of the TME,25 the cumulative effect of all the cells of the immune system on disease prognosis is not clearly defined. Moreover, our current knowledge about the interaction between TIL, chemotherapy and immunotherapy is also incomplete. We need to clearly define the interactions between these three factors in order to optimize our treatment options in the future. Finding new drugs and treatment combinations can lead to an even better prognosis for TNBC patients in the future. Furthermore, research is required in the use of TIL autologous transplants as a possible treatment option. This research is still in its early stages but may play an important part of TNBC treatment in coming decades. After reviewing the data we have available now, and as their role will only grow in the future, we firmly believe that routinely defining TIL should be a standard in TNBC management.
Abbreviations
TNBC, triple-negative breast cancer; ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2; PD-L1, programmed death ligand 1; PD-1, programmed cell death receptor 1; DNA, deoxyribonucleic acid; BRCA 1, breast cancer gene 1; PALB2, partner and localizer of BRCA 2; TMB, tumour mutation burden; OS, overall survival; PFS, progression-free survival; BCS, breast conserving surgery; BCT, breast conserving therapy; TME, tumour microenvironment; BC, breast cancer; CT, chemotherapy; TCR, T cell receptor; MHC, major histocompatibility complex ; IFN-γ; interferon gamma; T-reg, regulatory T-lymphocyte; FOXP3, forkhead box P3 protein; TIL, tumour-infiltrating lymphocytes; iTIL, intratumour tumour-infiltrating lymphocytes; 5NP, quintuple -egative breast cancer; pCR, pathological complete response; DRFI, distant recurrence free interval; HMGB1, high mobility group box 1 protein; TLR4, toll-like receptor 4; LPBC, lymphocyte predominant breast cancer; HR, hormone receptor; TIL-B; tumour infiltrating B-cell lymphocyte; BCSS, breast cancer-specific survival; DFI, disease-free survival; APC, antigen presenting cell; NK, natural killer; TNF-α, tumour necrosis factor alpha; ICI, immune checkpoint inhibitor; ICB, immune checkpoint blockade; SOC, standard of care; FDE, US Food and Drug Administration.
Funding
This research was funded by the Slovenian Research Agency, grant number J3-9272 and the Core Research Programme P3-0321, the Internal Research Project Funding of the University Medical Centre Maribor, grant number IRP-2021/01-02, IRP-2019/02-15.
Disclosure
The authors report no conflicts of interest in this work.
References
1. da Silva JL, Cardoso Nunes NC, Izetti P, de Mesquita GG, de Melo AC. Triple negative breast cancer: a thorough review of biomarkers. Crit Rev Oncol Hematol. 2020;145:102855. doi:10.1016/j.critrevonc.2019.102855
2. Yin L, Duan JJ, Bian XW, et al. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Res. 2020;22(1):61. doi:10.1186/s13058-020-01296-5
3. Won K, Spruck C. Triple-negative breast cancer therapy: current and future perspectives (Review). Int J Oncol. 2020;57(6):1245–1261. doi:10.3892/ijo.2020.5135
4. Sporikova Z, Koudelakova V, Trojanec R, Hajduch M. Genetic markers in triple-negative breast cancer. Clin Breast Cancer. 2018;18(5):e841–50. doi:10.1016/j.clbc.2018.07.023
5. Howard FM, Olopade OI. Epidemiology of triple-negative breast cancer. Cancer J. 2021;27(1):8–16. doi:10.1097/PPO.0000000000000500
6. Lyons TG. Targeted therapies for triple-negative breast cancer. Curr Treat Options Oncol. 2019;20(11). doi:10.1007/s11864-019-0682-x
7. Zhou Y, Tian Q, Wang BY, Yang J, Zhao SD, Yang J. The prognostic significance of TILs as a biomarker in triple-negative breast cancer: what is the role of TILs in TME of TNBC? Eur Rev Med Pharmacol Sci. 2021;25(7):2885–2897.
8. Colotta F, Allavena P, Sica A, Garlanda C, Mantovani A. Cancer-related inflammation, the seventh hallmark of cancer: links to genetic instability. Carcinogenesis. 2009;30(7):1073–1081. doi:10.1093/carcin/bgp127
9. Mahmoud SMA, Paish EC, Powe DG, et al. Tumor-infiltrating CD8 + lymphocytes predict clinical outcome in breast cancer. J Clin Oncol. 2011;29(15):1949–1955. doi:10.1200/JCO.2010.30.5037
10. Mouawad R, Spano JP, Khayat D. Lymphocyte infiltration in breast cancer: a key prognostic factor that should not be ignored. J Clin Oncol. 2011;29(15):1935–1936. doi:10.1200/JCO.2011.35.4845
11. Kumar P, Aggarwal R. An overview of triple-negative breast cancer. Arch Gynecol Obstet. 2016;293(2):247–269. doi:10.1007/s00404-015-3859-y
12. Borri F, Granaglia A. Pathology of triple negative breast cancer. Semin Cancer Biol. 2021;72:136–145. doi:10.1016/j.semcancer.2020.06.005
13. Lehmann BD, Jovanović B, Chen X, et al. Refinement of triple-negative breast cancer molecular subtypes: implications for neoadjuvant chemotherapy selection. PLoS One. 2016;11(6):e0157368. doi:10.1371/journal.pone.0157368
14. Bergin ART, Loi S. Triple-negative breast cancer: recent treatment advances. F1000Res. 2019;8:1342. doi:10.12688/f1000research.18888.1
15. Phipps AI, Chlebowski RT, Prentice R, et al. Reproductive history and oral contraceptive use in relation to risk of triple-negative breast cancer. J Natl Cancer Inste. 2011;103(6):470–477. doi:10.1093/jnci/djr030
16. Tao Z, Shi A, Lu C, Song T, Zhang Z, Zhao J. Breast cancer: epidemiology and etiology. Cell Biochem Biophys. 2015;72(2):333–338.
17. Luo C, Wang P, He S, Zhu J, Shi Y, Wang J. Progress and prospect of immunotherapy for triple-negative breast cancer. Front Oncol. 2022; 12:919072.
18. Han Y, Liu D, Li L. PD-1/PD-L1 pathway: current researches in cancer. Am J Cancer Res. 2020;10(3):727–742.
19. Schütz F, Stefanovic S, Mayer L, von Au A, Domschke C, Sohn C. PD-1/PD-L1 pathway in breast cancer. Oncol Res Treat. 2017;40(5):294–297. doi:10.1159/000464353
20. Lotfinejad P, Asghari Jafarabadi M, Abdoli Shadbad M, et al. Prognostic role and clinical significance of Tumor-Infiltrating Lymphocyte (TIL) and Programmed Death Ligand 1 (PD-L1) Expression in Triple-Negative Breast Cancer (TNBC): a Systematic Review and Meta-Analysis Study. Diagnostics. 2020;10(9):704. doi:10.3390/diagnostics10090704
21. Loi S, Michiels S, Adams S, et al. The journey of tumor-infiltrating lymphocytes as a biomarker in breast cancer: clinical utility in an era of checkpoint inhibition. Ann Oncol. 2021;32(10):1236–1244. doi:10.1016/j.annonc.2021.07.007
22. Gupta RK, Roy AM, Gupta A, et al. Systemic therapy de-escalation in early-stage triple-negative breast cancer: dawn of a new era? Cancers. 2022;14(8):1856. doi:10.3390/cancers14081856
23. Schmid P. The use of immunotherapy in triple-negative breast cancer. Clin Adv Hematol Oncol. 2021;19(12):12.
24. Carlino F, Diana A, Piccolo A, et al. Immune-based therapy in triple-negative breast cancer: from molecular biology to clinical practice. Cancers. 2022;14(9):2102. doi:10.3390/cancers14092102
25. Savas P, Salgado R, Denkert C, et al. Clinical relevance of host immunity in breast cancer: from TILs to the clinic. Nat Rev Clin Oncol. 2016;13(4):228–241. doi:10.1038/nrclinonc.2015.215
26. Stanton SE, Adams S, Disis ML. Variation in the incidence and magnitude of tumor-infiltrating lymphocytes in breast cancer subtypes. JAMA Oncol. 2016;2(10):1354. doi:10.1001/jamaoncol.2016.1061
27. Zitvogel L, Galluzzi L, Kepp O, Smyth MJ, Kroemer G. Type I interferons in anticancer immunity. Nat Rev Immunol. 2015;15(7):405–414. doi:10.1038/nri3845
28. Shankaran V, Ikeda H, Bruce AT, et al. IFNγ and lymphocytes prevent primary tumour development and shape tumour immunogenicity. Nature. 2001;410(6832):1107–1111. doi:10.1038/35074122
29. Smyth MJ, Dunn GP, Schreiber RD. Cancer immunosurveillance and immunoediting: the roles of immunity in suppressing tumor development and shaping tumor immunogenicity. Adv Immunol. 2006;90:1–50.
30. Fan Y, He S. The characteristics of tumor microenvironment in triple negative breast cancer. Cancer Manag Res. 2022;14:1–17. doi:10.2147/CMAR.S316700
31. Liu S, Lachapelle J, Leung S, Gao D, Foulkes WD, Nielsen TO. CD8+ lymphocyte infiltration is an independent favorable prognostic indicator in basal-like breast cancer. Breast Cancer Res. 2012;14(2):R48. doi:10.1186/bcr3148
32. National Cancer Institute. Biomarker. Available from: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/biomarker.
33. Understanding Prognostic versus Predictive Biomarkers. FDA-NIH Biomarker Working Group. BEST (Biomarkers, EndpointS, and other Tools) Resource. Available from: https://www.ncbi.nlm.nih.gov/books/NBK402284/.
34. Salgado R, Denkert C, Demaria S, et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: recommendations by an international tils working group 2014. Ann Oncol. 2015;26(2):259–271. doi:10.1093/annonc/mdu450
35. Gao G, Wang Z, Qu X, Zhang Z. Prognostic value of tumor-infiltrating lymphocytes in patients with triple-negative breast cancer: a systematic review and meta-analysis. BMC Cancer. 2020;20(1):179. doi:10.1186/s12885-020-6668-z
36. Ibrahim EM, Al-Foheidi ME, Al-Mansour MM, Kazkaz GA. The prognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancer: a meta-analysis. Breast Cancer Res Treat. 2014;148(3):467–476. doi:10.1007/s10549-014-3185-2
37. Dieci MV, Tsvetkova V, Orvieto E, et al. Immune characterization of breast cancer metastases: prognostic implications. Breast Cancer Res. 2018;20(1):62. doi:10.1186/s13058-018-1003-1
38. de Jong VMT, Wang Y, Opdam M, et al. 159O Prognostic value of tumour infiltrating lymphocytes in young triple negative breast cancer patients who did not receive adjuvant systemic treatment; by the PARADIGM study group. Ann Oncol. 2020;31:S303. doi:10.1016/j.annonc.2020.08.281
39. Seo AN, Lee HJ, Kim EJ, et al. Tumour-infiltrating CD8+ lymphocytes as an independent predictive factor for pathological complete response to primary systemic therapy in breast cancer. Br J Cancer. 2013;109(10):2705–2713. doi:10.1038/bjc.2013.634
40. Stanton SE, Disis ML. Clinical significance of tumor-infiltrating lymphocytes in breast cancer. J Immunother Cancer. 2016;4(1):59. doi:10.1186/s40425-016-0165-6
41. Bates GJ, Fox SB, Han C, et al. Quantification of regulatory t cells enables the identification of high-risk breast cancer patients and those at risk of late relapse. J Clin Oncol. 2006;24(34):5373–5380. doi:10.1200/JCO.2006.05.9584
42. Adams S, Gray RJ, Demaria S, et al. Prognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancers from two Phase III randomized adjuvant breast cancer trials: ECOG 2197 and ECOG 1199. J Clin Oncol. 2014;32(27):2959–2966. doi:10.1200/JCO.2013.55.0491
43. Hornychová H, Melichar B, Tomšová M, Mergancová J, Urminská H, Ryška A. Tumor-infiltrating lymphocytes predict response to neoadjuvant chemotherapy in patients with breast carcinoma. Cancer Invest. 2008;26(10):1024–1031. doi:10.1080/07357900802098165
44. Denkert C et al . (2010). Tumor-Associated Lymphocytes As an Independent Predictor of Response to Neoadjuvant Chemotherapy in Breast Cancer. JCO, 28(1), 105–113. 10.1200/JCO.2009.23.7370
45. U.S. National Library of Medicine. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/results?cond=TNBC+-+TripleNegative+Breast+Cancer&term=TIL+&cntry=&state=&city=&dist=.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.