")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Advances in Polatuzumab Vedotin-PIIQ Therapy: A Review of Treatment Efficacy in Diffuse Large B Cell Lymphoma and High-Grade B Cell Lymphoma
Authors Abdur Raqib M , Haseeb A , Shafique MA , Fadlalla Ahmed TK , Mustafa MS
Received 6 July 2023
Accepted for publication 13 October 2023
Published 16 October 2023 Volume 2023:14 Pages 323—331
DOI https://doi.org/10.2147/PHMT.S429252
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Moosa Abdur Raqib,1 Abdul Haseeb,2 Muhammad Ashir Shafique,2 Tagwa Kalool Fadlalla Ahmed,3 Muhammad Saqlain Mustafa2
1Department of Medicine, Liaquat College of Medicine & Dentistry, Karachi, Sindh, Pakistan; 2Department of Medicine, Jinnah Sindh Medical University, Karachi, Sindh, Pakistan; 3Department of Medicine, Ahfad University for Women, Omdurman, Sudan
Correspondence: Tagwa Kalool Fadlalla Ahmed, Department of Medicine, Ahfad University for Women, Omdurman, Sudan, Tel +249 969710718, Email [email protected]
Abstract: Polatuzumab vedotin (PV) is an antibody-drug conjugate that has shown promising results in the treatment of diffuse B-cell lymphoma (DLBCL) and high-grade B-cell lymphoma (HGBCL). This abstract summarizes the current understanding of PV’s use in these malignancies based on available clinical data. Multiple clinical trials have evaluated PV as a part of combination therapy regimens in relapsed/refractory DLBCL and HGBCL. The pivotal Phase II study, GO29365, demonstrated that PV in combination with bendamustine and rituximab (BR) significantly improved progression-free survival and overall survival compared to BR alone in patients with relapsed/refractory DLBCL who ineligible for stem cell transplantation were. Subsequently, the US Food and Drug Administration granted accelerated approval to PV in this setting. PV’s mechanism of action involves targeting CD79b, a cell surface receptor expressed in B-cell malignancies, and delivering the cytotoxic agent monomethyl auristatin E to CD79b-expressing cells. This approach enhances the selective killing of cancer cells while sparing normal cells. The safety profile of PV is generally manageable, with adverse events including infusion-related reactions, cytopenia, peripheral neuropathy, and infections. Overall, PV has emerged as a valuable treatment option for patients with relapsed/refractory DLBCL and HGBCL, offering improved outcomes when combined with appropriate chemotherapy regimens. Ongoing research and clinical trials are further exploring PV’s potential in various treatment settings, including frontline therapy and in combination with other novel agents.
Keywords: polatuzumab vedotin, non-Hodgkin lymphoma
Introduction
Between 30 to 40% of non-Hodgkin lymphoma cases globally are diffuse B-cell lymphoma (DLBCL), the most prevalent disease. Patients often have a rapidly expanding nodal or extranodal tumor mass in one or more locations.1 The concept of “high-grade B-cell lymphoma” has historically been used to refer to B-cell lymphomas that are morphologically aggressive, have numerous mitotic figures, frequently display a starry sky pattern, and have a high rate of proliferation, as signified by the word “Ki”. Clinical aggression is linked to particular physical traits. With the revision of the WHO’s (World Health Organization) lymphoma classification in 2017, the phrase “high-grade B-cell lymphoma” experienced a modification. The vast majority of cases in this category belong under the classification of high-grade B-cell lymphomas with MYC changes and BCL2 and/or BCL6, which additionally involves lymphomas with two or three hits or double and triple hit lymphomas. There is no representation elsewhere for high-grade B-cell lymphoma, a less common type among patients.2 Polatuzumab’s therapeutic role for patients with Relapsing and Remitting Diffuse Large B-cell Lymphoma has expanded significantly with the recent FDA approval. This approval pertains to its combination with bendamustine and rituximab, offering an effective treatment option for those who have undergone at least two prior therapies.3 In this review, we will discuss the role of polatuzumab vedotin-piiq a new drug approved by the FDA for the treatment of the above two conditions along with other clinical trials done and treatment regimens followed for the above two diseases.
Mechanism of Action
An example of an antibody-drug conjugate is polatuzumab vedotin-piiq. ADCs are revolutionary drugs that use monoclonal antibodies (mAb) antigen-specificity to target antigens expressed on tumor cells and deliver a powerful cytotoxic payload. With a wider therapeutic window and better pharmacokinetic/pharmacodynamic features, ADCs provide a special opportunity to deliver medicines to tumor cells while minimizing toxicity to normal organs.4 Polatuzumab Vedotin (Genentech, USA) is a conjugate of antibodies and drugs that incorporates the microtubule-disrupting monomethyl auristatin E (MMAE) with an anti-CD79B monoclonal antibody via a peptide linker that can be broken down by the maleimidocaproylvaline-citrulline-paminobenzoyloxycarbonyl protease.5–7
Immune Microenvironment
Beyond its direct cytotoxic effects, the impact of polatuzumab vedotin on the tumor immune microenvironment holds significant importance. The immune microenvironment is a complex network consisting of immune cells, cytokines, and signaling molecules, which can either bolster or hinder tumor growth. Emerging evidence underscores the intricate relationship between the effectiveness of immunotherapeutic agents, like polatuzumab vedotin, and their ability to modulate this immune microenvironment.
Research has indicated that polatuzumab vedotin’s precise delivery of monomethyl auristatin E to CD79b-expressing B-cells not only triggers cancer cell death but also has the potential to impact immune responses. By eliminating malignant B-cells, polatuzumab vedotin may alleviate the immune suppression induced by tumors, leading to improved presentation of tumor antigens to immune cells. This, in turn, could initiate a chain of immune activation events, including enhanced T-cell recognition and recruitment, ultimately contributing to a more robust and enduring anti-tumor immune response.8
Moreover, there is a compelling case for conducting clinical trials that combine polatuzumab vedotin with immunomodulatory agents such as checkpoint inhibitors or immune-stimulating antibodies. These combinations leverage the drug’s capacity to reshape the immune microenvironment, potentially resulting in higher response rates and prolonged disease control. Investigating the interplay between polatuzumab vedotin and immune cells within the tumor microenvironment may yield valuable insights into novel therapeutic strategies that harness the immune system to enhance treatment outcomes.9
In summary, while the discussed clinical trials underscore polatuzumab vedotin’s efficacy in targeting B-cell non-Hodgkin’s lymphoma, it is vital to recognize the broader implications of its actions within the tumor immune microenvironment. Incorporating this perspective on the immune microenvironment could further clarify the mechanisms behind the drug’s therapeutic advantages and inspire innovative approaches to maximize its potential in the treatment of lymphoid malignancies.
Treatment Protocols of Both Diseases
Diffuse Large B Cell Lymphoma
Options for therapy for people with diffuse large B-cell lymphoma are evolving. Over 50% of those diagnosed with diffuse large B-cell lymphoma are presently cured. The management of diffuse large B-cell lymphoma in certain extranodal places, such as the brain, testes, and skin, provides distinct challenges. With Burkitt’s lymphoma treatment regimens, a subset of diffuse large B-cell lymphomas that have a very high proliferation index seem to react better than CHOP-R. CHOP-R-21 is still excellent therapy for the vast majority of patients.10 In eligible individuals, relapsed or refractory illness is often found during the first two years of diagnosis and necessitates more rigorous treatment with high-dose chemotherapy, CD-19-directed chimeric antigen receptor (CAR)-T-cell therapy, or experimental therapy.11 Patients with a double- or triple-hit lymphoma characterized by a MYC and/or BCL2 and/or BCL6 rearrangement revealed by FISH have a poorer prognosis regardless of their basic IPI (international prognostic risk). We typically treat these patients with a dose-adjusted EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin) regimen based on a phase II trial in patients with a MYC rearrangement and a meta-analysis of 11 retrospective studies that demonstrated favorable results with this more intensive treatment regimen.12,13
High Grade B Cell Lymphoma
R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) chemoimmunotherapy is the cornerstone of treatment even if a cure has yet to be discovered.14 Other therapy include Salvage therapy but There is no standard salvage treatment for aggressive lymphoma. DHAP (dexamethasone, cytarabine, cisplatin), ESHAP (etoposide, methylprednisone, cytarabine, cisplatin), mini-BEAM (carmustine, etoposide, cytarabine, melphalan), and ICE (ifosfamide, carboplatin, etoposide) are common second-line regimens. Overall response rates are roughly 60%, with full remission rates ranging from 25% to 35%.15–19 The addition of rituximab to second-line chemotherapy improved outcomes significantly particularly in combination with ICE20 DHAP21 EPOCH.22 This might be part of the therapy for aggressive lymphoma.
Clinical Trials of the Drug Done Previously
NCT01290549
In a Phase I open-label study (NCT01290549), polatuzumab vedotin was given intravenously in cycles of 21 days to patients with R/R B-cell non-Hodgkin’s lymphoma. Toxicity 45 patients with evaluable NHL underwent polatuzumab vedotin 2.4 mg/kg during the exacerbation or expansion phase. There were 23 of them, including 7 complete responses (CR) and 16 partial responses (RP), that had an objective response (OR). A median duration of response (DoR) of 6.2 months and a median progression-free survival (PFS) of 5.7 months was observed in patients undergoing polatuzumab vedotin at a dose of 2.4 mg/kg.23 The same results were similarly obtained by a Phase 1 Japanese experiment (JO29138).24
ROMULUS Phase Ib/II Trial
In a clinical study, either polatuzumab vedotin or pinatuzumab vedotin was given every 21 days along with rituximab until the disease progressed or unacceptable side effects occurred, for a maximum duration of one year. It is noteworthy that the participants included patients who had not responded to four previous treatments, and 78% of those with diffuse large B-cell lymphoma (DLBCL) had shown resistance to their most recent treatment.
Between Sept 27, 2012, and Oct 10, 2013, 81 patients with diffuse large B-cell lymphoma and 42 with follicular lymphoma were recruited and assigned to treatment. Of the patients with diffuse large B-cell lymphoma who received R-pina, 60% achieved an objective response and 26% achieved a complete response. Of the patients in this cohort who received R-pola, 54% achieved an objective response and 21% achieved a complete response. In the follicular lymphoma cohort, of the patients who received R-pina, 62% achieved an objective response and 5% achieved a complete response. Of the patients in this cohort who received R-pola, 70% achieved an objective response and 45% achieved a complete response. Grade 3–5 adverse events occurred in both cohorts, with neutropenia being the most common in both groups receiving R-pina and R-pola.25
Another trial regarding the ROMULUS study investigated the impact of combining polatuzumab vedotin (1.8 mg/kg) with Obinutuzumab in a group of 21 patients with relapsed or refractory (r/r) diffuse large B-cell lymphoma (DLBCL) for a maximum of eight treatment cycles, each spanning 21 days. Out of the 70 patients assessed for safety, 70% (49 patients) encountered a treatment-related adverse event (AE), with the majority falling into the mild category (Group 1/2) comprising 34 out of the 49 occurrences. The most prevalent adverse events, affecting more than 20% of patients, included fatigue (grade 1–3) observed in 43% of patients, diarrhea (grade 1–2) in 34% of patients, nausea (grade 1–3) in 30% of patients, constipation (grade 1–2) in 21% of patients, and headache (grade 1) in 20% of patients.26
Polatuzumab Vedotin + Bendamustine + Rituximab in Relapsed/Refractory DLBCL: Phase 2 Trial Overview
A total of 113 individuals with relapsed/refractory DLBCL who were not suitable for transplantation were enrolled in the study between October 15, 2014, and June 10, 2016. Initially, there were 12 patients in the preliminary safety assessment phase, with 6 receiving pola-BR treatment and 6 receiving pola-BG treatment. In the subsequent phase II portion, 21 participants were in the pola-BG group.
The safety and efficacy of polatuzumab vedotin combined with bendamustine and obinutuzumab (pola-BG) and pola-BR were evaluated in a single-arm cohort of transplantation-ineligible R/R DLBCL patients. Out of the recruited patients, 20 received treatment. Pola-BG and Pola-BR showed acceptable safety profiles in a clinical study. Pola-BR, in a randomly assigned cohort of 80 patients, demonstrated a significantly higher complete response rate (40.0% vs 17.5%) as assessed by an independent review committee (IRC). It also exhibited longer progression-free survival (median 9.5 vs 3.7 months) and overall survival (median 12.4 vs 4.7 months) compared to Pola-BG. These results suggest the potential superiority of Pola-BR in terms of clinical outcomes. The allocation to phase II was done randomly, and each arm of the cohort consisted of 39 participants. Both treatment arms underwent the same course of treatment.27
POLARIX Trial
The standard treatment for Diffuse Large B-cell Lymphoma (DLBCL) is a combination of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP). However, the success rate of curing patients with this regimen is only around 60%. To address this, a research study was conducted using a double-blind, placebo-controlled, international Phase 3 trial. The goal was to assess the effectiveness of a modified version of R-CHOP called pola-R-CHP. In this modified regimen, vincristine was replaced with polatuzumab vedotin. The study focused on individuals with previously untreated intermediate-risk or high-risk DLBCL.
In a study involving 879 patients who were randomized, with 440 in the pola-R-CHP group and 439 in the R-CHOP group, the results after a median follow-up of 28.2 months demonstrated that the percentage of patients who survived without disease progression was notably higher in the pola-R-CHP group compared to the R-CHOP group. Specifically, at the 2-year mark, the survival without progression rates were 76.7% (95% confidence interval [CI], 72.7 to 80.8) in the pola-R-CHP group and 70.2% (95% CI, 65.8 to 74.6) in the R-CHOP group. The hazard ratio for the risk of progression, relapse, or death, adjusted for stratification, was 0.73 according to Cox regression (95% CI, 0.57 to 0.95; P = 0.02).
However, the overall survival rates at 2 years did not exhibit a significant difference between the two groups. The rates were 88.7% (95% CI, 85.7 to 91.6) in the pola-R-CHP group and 88.6% (95% CI, 85.6 to 91.6) in the R-CHOP group. The hazard ratio for the risk of death was 0.94 (95% CI, 0.65 to 1.37; P = 0.75), showing no substantial disparity between the groups. The safety profiles of the two groups were comparable.
For individuals with previously untreated intermediate-risk or high-risk DLBCL, the study concluded that the risk of disease progression, relapse, or death was lower in those treated with pola-R-CHP compared to those treated with R-CHOP. The study was funded by F. Hoffmann–La Roche/Genentech and had the ClinicalTrials.gov identifier NCT03274492.28
Updated Results of a Phase Ib/II Study with Polatuzumab Vedotin in Combination with Obinutuzumab, Cyclophosphamide, Doxorubicin, and Prednisone (G-CHP) for Patients with Previously Untreated Diffuse Large B-Cell Lymphoma (DLBCL)
The study arm’s recruitment phase has been successfully concluded. By March 31, 2017, a group of 21 individuals with untreated DLBCL (57% men) were enrolled in a trial involving a treatment combination of G-CHP and pola at a dose of 1.8 mg/kg. The median age of participants was 67 years (ranging from 28 to 76). Patients had diagnoses of stage I/II disease (3 patients) or stage III/IV disease (18 patients), with an ECOG performance status of 0–1 for 17 individuals. Initial IPI scores were distributed as follows: IPI 0–1 for 3 patients (14%); IPI 2 for 10 patients (48%); IPI 3 for 4 patients (19%); and IPI 4 for 4 patients (19%). At the time of the report, all patients had successfully completed their treatment regimen.
Adverse events (AEs) of all grades occurring in more than 30% of patients, as well as Grade 3/4 AEs occurring in more than one patient, are documented. Among these patients, nine (43%) experienced a total of 31 significant AEs, including occurrences like febrile neutropenia (29%), neutropenia (10%), pneumonia (10%), and others. Peripheral neuropathy was detected in eight individuals (38%), with six experiencing grade 1 and two having grade 2 severity. Four patients (19%) discontinued treatment prematurely due to AEs, which included reasons such as thrombocytopenia after the first treatment cycle, fatal septic shock after the fourth cycle, coronary artery disease after the fourth cycle, and febrile neutropenia after the fifth cycle. Upon completion of the treatment regimen, analysis of effectiveness using PET-CT indicated an overall response rate of 91%, with 81% achieving a complete response (CR) and 10% achieving a partial response (PR). Two individuals who did not respond were considered ineligible due to early withdrawal caused by adverse events (thrombocytopenia and septic shock). With an average duration of 10 months for the trial, no responders showed signs of relapse during the analysis period.
The combined treatment of pola at 1.8 mg/kg and G-CHP demonstrated efficacy and good tolerance in treating previously untreated DLBCL. As anticipated, the most common side effects were neutropenia and peripheral neuropathy.29
A Multicenter Retrospective Analysis of Polatuzumab Vedotin in Patients with Large B-Cell Lymphoma Following CAR T-Cell Treatment
PV is an antibody-drug combination approved for the treatment of relapsed or refractory LBCL. The first registration trial did not include individuals who experienced relapse after CAR T-cell treatment, and data on the use of PV after CAR T-cell therapy is scarce. The trial focused on LBCL patients who experienced relapse or advancement following CAR T-cell treatment and then underwent PV, either with or without rituximab and bendamustine. Over a median follow-up period of 47 weeks, 81% of patients exhibited disease progression or died, with a median progression-free survival of 10 weeks. A multivariate analysis revealed that both bone marrow involvement and increased lactate dehydrogenase levels were associated with decreased progression-free survival.30
Several additional articles and randomized controlled trials (RCTs) warrant discussion and are outlined in the following table, detailing their outcomes and associated side effects.
Adverse Effects
Adverse effects in the clinical study included Grade 3–4 adverse events in 58% of NHL patients, with the most common being neutropenia, anemia, and peripheral sensory neuropathy. Mortality rate was 12%, with deaths primarily attributed to disease progression, treatment-related infections, and deteriorating ascites.23 Other adverse effects seen in different trials and articles are listed in the Table 1.
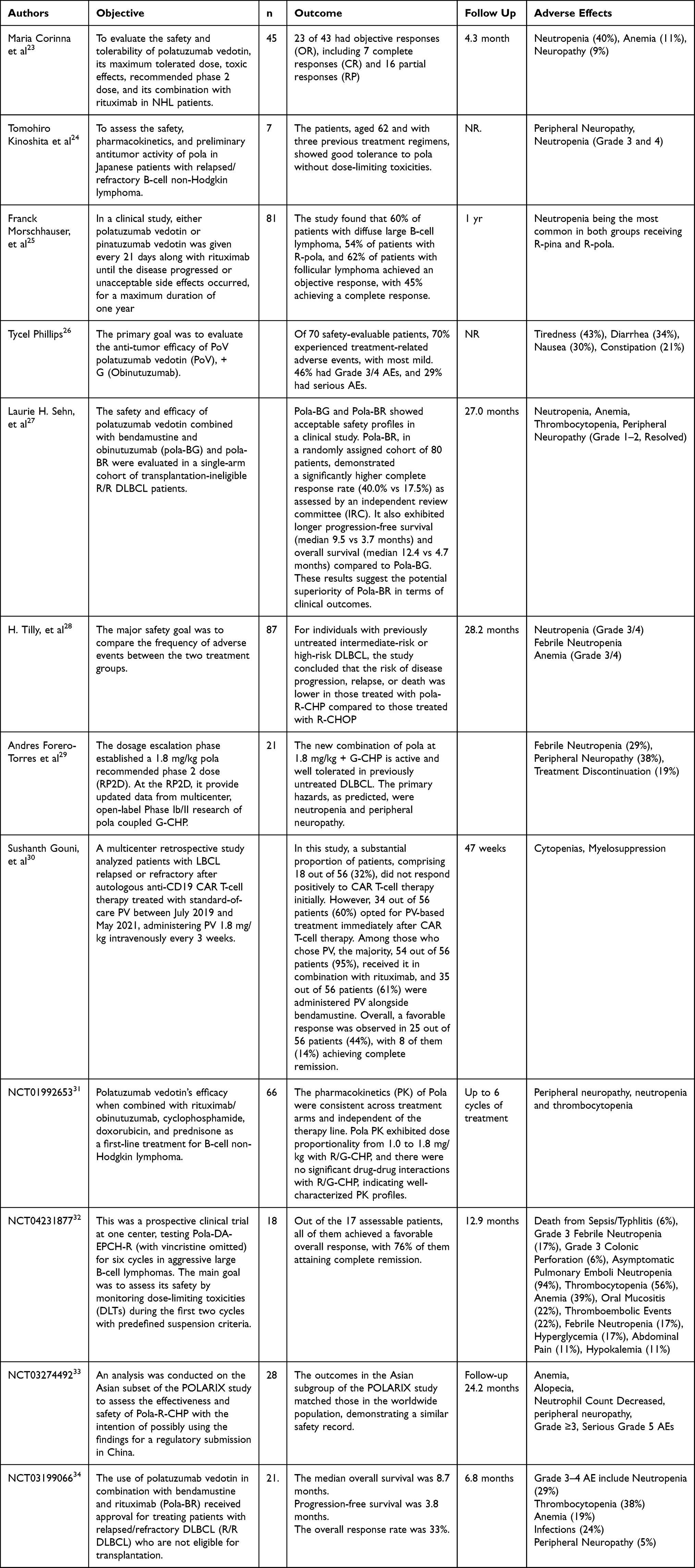 |
Table 1 Summary of Previous Trials |
Conclusion
Polatuzumab vedotin-piiq emerges as a promising therapeutic avenue for the management of diffuse B-cell lymphoma (DLBCL) and high-grade B-cell lymphoma. This antibody-drug conjugate exhibits a targeted approach, directly engaging tumor cells and minimizing harm to healthy organs. Encouraging outcomes from clinical trials, including instances of complete remission, underscore its potential efficacy. Nonetheless, the emergence of side effects such as neutropenia and peripheral sensory neuropathy underscores the importance of vigilant monitoring and comprehensive management strategies. By ushering in renewed optimism for individuals who have encountered setbacks with prior treatments, polatuzumab vedotin-piiq introduces a potential breakthrough. However, comprehensive investigations are imperative to unravel its complete therapeutic landscape. As our understanding deepens, this novel therapeutic approach may unveil further dimensions of its effectiveness, ultimately refining its role in revolutionizing DLBCL and high-grade B-cell lymphoma treatment paradigms.
Disclosure
The authors declare no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
References
1. Li S, Young KH, Medeiros LJ. Diffuse large B-cell lymphoma. Pathology. 2018;50(1):74–87. doi:10.1016/j.pathol.2017.09.006
2. Ok CY, Medeiros LJ. High-grade B-cell lymphoma: a term re-purposed in the revised WHO classification. Pathology. 2020;52(1):68–77. doi:10.1016/j.pathol.2019.09.008
3. Assi R, Masri N, Abou Dalle I, El-Cheikh J, Ghanem H, Bazarbachi A. Polatuzumab vedotin: current role and future applications in the treatment of patients with diffuse large B-cell lymphoma. Clin Hematol Int. 2021;3(1):21. doi:10.2991/chi.k.210305.001
4. Hafeez U, Parakh S, Gan HK, Scott AM. Antibody–drug conjugates for cancer therapy. Molecules. 2020;25(20):4764. doi:10.3390/molecules25204764
5. Bai R, Pettit GR, Hamel E. Binding of dolastatin 10 to tubulin at a distinct site for peptide antimitotic agents near the exchangeable nucleotide and vinca alkaloid sites. J Biol Chem. 1990;265(28):17141–17149. doi:10.1016/S0021-9258(17)44880-0
6. Doronina SO, Toki BE, Torgov MY, et al. Development of potent monoclonal antibody auristatin conjugates for cancer therapy. Nat Biotechnol. 2003;21(7):778–784. doi:10.1038/nbt832
7. Francisco JA, Cerveny CG, Meyer DL, et al. cAC10-vcMMAE, an anti-CD30–monomethyl auristatin E conjugate with potent and selective antitumor activity. Blood. 2003;102(4):1458–1465. doi:10.1182/blood-2003-01-0039
8. Solimando AG, Annese T, Tamma R, et al. New Insights into Diffuse Large B-Cell Lymphoma Pathobiology. Cancers. 2020;12(7):1869. doi:10.3390/cancers12071869
9. Hans CP, Weisenburger DD, Greiner TC, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004;103(1):275–282. doi:10.1182/blood-2003-05-1545
10. Armitage JO, editor. My treatment approach to patients with diffuse large B-cell lymphoma.
11. Melchardt T, Egle A, Greil R. How I treat diffuse large B-cell lymphoma. ESMO open. 2023;8(1):100750. doi:10.1016/j.esmoop.2022.100750
12. Howlett C, Snedecor SJ, Landsburg DJ, et al. Front‐line, dose‐escalated immunochemotherapy is associated with a significant progression‐free survival advantage in patients with double‐hit lymphomas: a systematic review and meta‐analysis. Br J Haematol. 2015;170(4):504–514. doi:10.1111/bjh.13463
13. Dunleavy K, Fanale MA, Abramson JS, et al. Dose-adjusted EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab) in untreated aggressive diffuse large B-cell lymphoma with MYC rearrangement: a prospective, multicentre, single-arm phase 2 study. Lancet Haematol. 2018;5(12):e609–e617. doi:10.1016/S2352-3026(18)30177-7
14. Novo M, Castellino A, Nicolosi M, et al. High-grade B-cell lymphoma: how to diagnose and treat. Expert Rev Hematol. 2019;12(7):497–506. doi:10.1080/17474086.2019.1624157
15. Moskowitz CH, Bertino JR, Glassman JR, et al. Ifosfamide, carboplatin, and etoposide: a highly effective cytoreduction and peripheral-blood progenitor-cell mobilization regimen for transplant-eligible patients with non-Hodgkin’s lymphoma. J Clin Oncol. 1999;17(12):3776–3785. doi:10.1200/JCO.1999.17.12.3776
16. Velasquez WS, Cabanillas F, Salvador P, et al. Effective salvage therapy for lymphoma with cisplatin in combination with high-dose Ara-C and dexamethasone (DHAP). Blood. 1988;71(1):117–122. doi:10.1182/blood.V71.1.117.117
17. Velasquez W, McLaughlin P, Tucker S, et al. ESHAP--an effective chemotherapy regimen in refractory and relapsing lymphoma: a 4-year follow-up study. J Clin Oncol. 1994;12(6):1169–1176. doi:10.1200/JCO.1994.12.6.1169
18. Girouard C, Dufresne J, Imire K, et al. Salvage chemotherapy with mini-BEAM for relapsed or refractory non-Hodgkin’s lymphoma prior to autologous bone marrow transplantation. Ann Oncol. 1997;8(7):675–680. doi:10.1023/A:1008294725992
19. Caballero M, Amigo M, Hernández J, et al. Alternating mini-BEAM/ESHAP as salvage therapy for refractory non-Hodgkin’s lymphomas. Ann Hematol. 1997;74(2):79–82. doi:10.1007/s002770050261
20. Kewalramani T, Zelenetz AD, Nimer SD, et al. Rituximab and ICE as second-line therapy before autologous stem cell transplantation for relapsed or primary refractory diffuse large B-cell lymphoma. Blood. 2004;103(10):3684–3688. doi:10.1182/blood-2003-11-3911
21. Mey UJ, Orlopp KS, Flieger D, et al. Dexamethasone, high-dose cytarabine, and cisplatin in combination with rituximab as salvage treatment for patients with relapsed or refractory aggressive non-Hodgkin’s lymphoma. Cancer Invest. 2006;24(6):593–600. doi:10.1080/07357900600814490
22. Jermann M, Jost L, Taverna C, et al. Rituximab–EPOCH, an effective salvage therapy for relapsed, refractory or transformed B-cell lymphomas: results of a phase II study. Ann Oncol. 2004;15(3):511–516. doi:10.1093/annonc/mdh093
23. Palanca-Wessels MCA, Czuczman M, Salles G, et al. Safety and activity of the anti-CD79B antibody–drug conjugate polatuzumab vedotin in relapsed or refractory B-cell non-Hodgkin lymphoma and chronic lymphocytic leukaemia: a phase 1 study. Lancet Oncol. 2015;16(6):704–715. doi:10.1016/S1470-2045(15)70128-2
24. Hatake K, Kinoshita T, Terui Y, et al. A phase I pharmacokinetic and safety study of polatuzumab vedotin in Japanese patients with relapsed/refractory b-cell non-Hodgkin lymphoma: a comparison with non-Japanese DCS4968g study. Am Soci Clin Oncol. 2016;34(15_suppl):e19070. doi:10.1200/JCO.2016.34.15_suppl.e19070
25. Morschhauser F, Flinn IW, Advani R, et al. Polatuzumab vedotin or pinatuzumab vedotin plus rituximab in patients with relapsed or refractory non-Hodgkin lymphoma: final results from a phase 2 randomised study (ROMULUS). Lancet Haematol. 2019;6(5):e254–e265. doi:10.1016/S2352-3026(19)30026-2
26. Phillips T, Brunvand M, Chen A, et al. Polatuzumab vedotin combined with obinutuzumab for patients with relapsed or refractory non-Hodgkin lymphoma: preliminary safety and clinical activity of a phase Ib/II study. Blood. 2016;128(22):622. doi:10.1182/blood.V128.22.622.622
27. Sehn LH, Herrera AF, Flowers CR, et al. Polatuzumab vedotin in relapsed or refractory diffuse large B-cell lymphoma. J Clin Oncol. 2020;38(2):155. doi:10.1200/JCO.19.00172
28. Tilly H, Morschhauser F, Sehn LH, et al. Polatuzumab vedotin in previously untreated diffuse large B-cell lymphoma. N Engl J Med. 2022;386(4):351–363. doi:10.1056/NEJMoa2115304
29. Forero-Torres A, Kolibaba KS, Tilly H, et al. Polatuzumab vedotin combined with obinutuzumab, cyclophosphamide, doxorubicin, and prednisone (G-CHP) for patients with previously untreated diffuse large B-cell lymphoma (DLBCL): updated results of a phase Ib/II study. Blood. 2017;130:4120.
30. Gouni S, Rosenthal AC, Crombie JL, et al. A multicenter retrospective study of polatuzumab vedotin in patients with large B-cell lymphoma after CAR T-cell therapy. Blood Adv. 2022;6(9):2757–2762. doi:10.1182/bloodadvances.2021006801
31. Shemesh CS, Agarwal P, Lu T, et al. Pharmacokinetics of polatuzumab vedotin in combination with R/G-CHP in patients with B-cell non-Hodgkin lymphoma. Cancer Chemother Pharmacol. 2020;85(5):831–842. doi:10.1007/s00280-020-04054-8
32. Lynch RC, Poh C, Ujjani CS, et al. Polatuzumab vedotin with infusional chemotherapy for untreated aggressive B-cell non-Hodgkin lymphomas. Blood Adv. 2023;7(11):2449–2458. doi:10.1182/bloodadvances.2022009145
33. Song Y, Tilly H, Rai S, et al. Polatuzumab vedotin in previously untreated DLBCL: an Asia subpopulation analysis from the phase 3 POLARIX trial. Blood. 2023;141(16):1971–1981.
34. Vodicka P, Benesova K, Janikova A, et al. Polatuzumab vedotin plus bendamustine and rituximab in patients with relapsed/refractory diffuse large B‐cell lymphoma in the real world. Eur J Haematol. 2022;109(2):162–165. doi:10.1111/ejh.13784
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.