")
Back to Journals » Eye and Brain » Volume 14
Adults Born Small for Gestational Age at Term Have Thinner Peripapillary Retinal Nerve Fiber Layers Than Controls
Authors Fieß A , Brandt M , Mildenberger E, Urschitz MS, Wagner FM, Grabitz SD, Hoffmann EM, Pfeiffer N , Schuster AK
Received 21 July 2022
Accepted for publication 18 October 2022
Published 25 November 2022 Volume 2022:14 Pages 127—135
DOI https://doi.org/10.2147/EB.S383231
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Margaret Wong-Riley
Achim Fieß,1 Marilena Brandt,1 Eva Mildenberger,2 Michael Siegfried Urschitz,3 Felix Mathias Wagner,1 Stephanie Desiree Grabitz,1 Esther Maria Hoffmann,1 Norbert Pfeiffer,1 Alexander Konrad Schuster1
1Department of Ophthalmology, University Medical Center of the Johannes Gutenberg University Mainz, Mainz, Germany; 2Division of Neonatology, Department of Pediatrics, University Medical Center of the Johannes Gutenberg-University Mainz, Mainz, Germany; 3Division of Pediatric Epidemiology, Institute for Medical Biostatistics, Epidemiology and Informatics, University Medical Center of the Johannes Gutenberg University Mainz, Mainz, Germany
Correspondence: Achim Fieß, Department of Ophthalmology, Medical Center of the Johannes Gutenberg University Mainz, Langenbeckstr. 1, Mainz, 55131, Germany, Tel +49-6131-17-5150, Fax +49-6131-17-8495, Email [email protected]
Purpose: Prenatal growth restriction is associated with impaired neurodevelopment in childhood. This study investigated the effects of being born small for gestational age (SGA) on peripapillary retinal nerve fiber layer (pRNFL) thickness in adults born at term.
Methods: A retrospective cohort study was conducted with a prospective ophthalmologic examination of participants born at full-term (gestational age ≥ 37 weeks) between 1969 and 2002. All participants were examined with spectral-domain optical coherence tomography and grouped according to their birth weight in correlation to gestational age as former moderate (birth weight (BW) percentile 3rd to < 10th) and severe SGA (< 3rd percentile), normal (10th-90th percentile, AGA), and moderately (> 90th to 97th percentile) and severely (> 97th percentile) large for gestational age (LGA) adults (18 to 52 years).
Results: Overall, 547 eyes of 285 individuals (age 29.9± 9.4 years, 151 females) born at term were included. Multivariable regression analyses revealed a strong association between a lower global pRNFL thickness in the severe SGA (B=− 8.99 [95%-CI: − 12.68; − 5.30] μm; p< 0.001) and in the moderate SGA groups (B=− 6.40 [95%-CI: − 10.29; − 2.50] μm; p=0.001) compared to the reference AGA group.
Conclusion: Our results indicate that restricted fetal growth affects neurologic tissue development of the optic nerve head, particularly in individuals born severely SGA at term. This indicates that fetal growth restriction may exert disturbances in the development of neurologic tissue, which persists in adulthood.
Keywords: birth weight, small for gestational age, large for gestational age, peripapillary retinal nerve fiber layer, optic nerve head, epidemiology
Introduction
Impaired fetal growth has important long-term effects on the central nervous system1 and can lead to reduced neurological and intellectual outcomes in childhood.2,3 Growth restriction at birth is classified as severely small-for-gestational-age (SGA) when birth weight is <3rd percentile and as moderately SGA when BW is between the 3rd and <10th percentile in relation to gestational age.4 Every year, about 30 million infants are born SGA.4
Magnetic resonance imaging (MRI) studies have shown that SGA children have a decreased total brain volume and reduction of the cortical gray matter.3,5 Some authors even reported a correlation between brain structure and the peripapillary retinal nerve fiber layer (pRNFL), which can be measured precisely with optical coherence tomography (OCT).6 The optic nerve head is part of the CNS and pRNFL measurements provide a unique non-invasive and contact-less view on neuronal tissue, potentially on neuronal degeneration of the CNS, such as in multiple sclerosis,7 Parkinson´s disease,8 and Alzheimer´s disease.9 From an ophthalmological perspective, it is of particular importance to analyze factors that have been associated with thinner pRNFL, as this measure is of major importance in diagnosing different optic neuropathies, such as glaucoma in adulthood, a leading cause of vision loss and blindness in developed countries.10 In recent reports in infants,11,12 children13–15 and young adults,16 an association was observed between preterm birth and pRFNL thinning. Furthermore, in a recent study, the authors showed that pRNFL measured in infants can predict visual acuity at 9 months, which provided direct evidence for the importance of measuring pRNFL.5
However, there is a lack of data comparing pRNFL thickness in term children born SGA and large for gestational age (LGA). A Spanish research group reported that children born SGA before term and at term showed alterations in retinal structure compared to children born appropriate for gestational age.17–20 Recently within the Gutenberg Health Study, we observed a thinner pRNFL in individuals born preterm and at term with low birth weight (<2500 g) compared to individuals born normal birth weight (2500–4000 g) in middle and late adulthood.21 However, the results of this study were limited because gestational age was not documented. Therefore, no data exists about the exclusive long-term effects of being born SGA on pRNFL independent of prematurity. Premature birth is a risk factor affecting individuals´ neurodevelopmental outcomes and optic disc shape,1,13 but it is unclear whether term individuals born SGA are also at increased risk. Thus, the present study is the first to analyze the long-term effects of different degrees of fetal growth restriction and supernutrition in individuals born at term in adulthood. It was hypothesized that impaired fetal growth is linked to a thinner pRNFL in individuals born SGA at term than controls.
Materials and Methods
Study Population
The present study is a retrospective single-center cohort study with a prospective ophthalmologic examination at the University Medical Center of the Johannes Gutenberg-University Mainz in Germany (UMCM). A comprehensive ophthalmologic examination was conducted, and a detailed questionnaire was completed of individuals born SGA, AGA and LGA at term in the UMCM between 1969 and 2002 now aged between 18 and 52 years. There were 40 individuals born severe SGA (BW percentile <3rd), 40 moderate SGA (3rd to <10th percentile), 40 severe LGA (BW percentile >97th), 40 moderate LGA (BW percentile >90th to 97th), and 140 AGA (BW percentile between 10th and 90th), all with a gestational age ≥37 weeks in the study. The participants were aged matched invited to take part in the study. The study measurements were obtained between 2019 and 2021, as well as a review of the childrens´ and their mothers´ birth records.
Written informed consent was obtained from all study participants before they entered into the study complying with Good Clinical Practice, Good Epidemiological Practice, and the ethical principles of the Declaration of Helsinki. The study protocol and documents were approved by the local ethics committee of the Medical Chamber of Rhineland-Palatinate, Germany (reference no. 2019-14161; original vote: 29.05.2019, latest update: 02.04.2020).
Assessment of Pre- and Postnatal History
The medical birth records were reviewed, and data regarding gestational age, birth weight, placental insufficiency, breastfeeding, maternal smoking, gestational diabetes, and preeclampsia were collected.
Exposure: Birth Weight Percentile
Birth weight percentile was calculated based on birth weight in correlation to gestational age.22 BW percentile was categorized into severe SGA (BW percentile <3; group 1), moderate SGA (BW percentile 3rd to <10th group 2), AGA (BW percentile 10th to 90th; group 3), moderate LGA (BW percentile >90th to 97th; group 4), and severe LGA (BW percentile >97th percentile; group 5). All individuals were born full-term (gestational age ≥37 weeks).
Ophthalmologic Examination
Each participant completed an extensive ophthalmologic examination. In brief, objective refraction and distant-corrected visual acuity were measured in both eyes (ARK-1s, NIDEK, Oculus, Wetzlar, Germany). The spherical equivalent was calculated by spherical correction value plus half the cylindrical power.
The pRNFL was measured by spectral-domain optical coherence tomography (SD-OCT). Briefly, a circular peripapillary scan of 12° diameter centered on the optic disc with eye tracking with a standard 7.7 mm corneal curvature and ametropia of 0 diopter was performed. Automatic segmentation of the retinal nerve fiber layer was performed with the Heidelberg Eye Explorer Software tool (HEYEX version 6.13.3.0). Software algorithms calculated global and sectorial pRNFL thickness (superonasal, nasal, inferonasal, inferotemporal, temporal, superotemporal) from circle scan data. The pRNFL measurements were adjusted for ocular magnification by integrating corneal curvature and spherical equivalent,23 the same parameters used in the HEYEX software for adjustment of ocular magnification as reported previously.21 Each SD-OCT examination was conducted in non-mydriatic eyes and every scan was checked by an experienced investigator for decentration and segmentation errors. In the case that OCT scans showed decentration or segmentation error, this examination was excluded. In addition, only high-quality images with a high signal strength >15 dB were included in the present study. In a previous study, Wu et al observed intraclass correlation coefficients for repeated pRNFL measurements from 0.977 (T) to 0.990 (G and inferior-nasal sector) in normal eyes.24
Covariates
The following covariates were considered as factors potentially affecting the main outcome measures, namely, age (years), sex (female), gestational age (weeks), birth weight (kg), birth weight percentile (categories), placental insufficiency (yes), preeclampsia (yes), and breastfeeding (yes) and maternal cigarette smoking during pregnancy (yes).
Statistical Analysis
Descriptive statistics were computed for the main outcome measures, pRNFL thickness for the global measure, and the six sectors (superonasal, nasal, inferonasal, inferotemporal, temporal, and superotemporal). Absolute and relative frequencies were calculated for dichotomous parameters, mean and standard deviation were calculated for approximately normally distributed data, otherwise median and interquartile range were computed. Linear regression models with general estimating equations (GEE) were used to assess associations and account for correlations between the corresponding eyes of one individual. In model #1, the main outcome measures were tested in univariate analysis with gestational age (weeks), birth weight percentile (categories), breastfeeding (yes), preeclampsia (yes), and placental insufficiency (yes). In model #2, the associations with these parameters were assessed in a multivariable model. Maternal cigarette smoking during pregnancy was tested in a univariate model due to the small number of smokers. A sensitivity analysis was performed with the inclusion of cigarette smoking during pregnancy (yes) in the multivariable model. A potential relationship between global pRNFL and visual acuity (in logMAR) was tested and Spearman correlation coefficient was computed for right eyes. This is an explorative study, and no adjustment for multiple testing was performed. The statistical analysis was performed using commercial software (IBM SPSS 20.0; SPSS, Inc., Chicago, IL, USA).
Results
Participant Characteristics
A total of 547 eyes of 285 individuals born at term were included in the present study (aged 29.9±9.4 years; 151 females). The recruitment efficacy proportion was 52.6% in all SGA and LGA individuals and 48.3% in AGA study participants. There were 39 participants (74 eyes) with <3rd BW percentile, 38 participants (73 eyes) with 3rd–<10th BW percentile, 132 participants (253 eyes) with BW percentile 10–90th; 36 participants (70 eyes) with BW percentile >90–97th and 40 participants (77 eyes) with BW percentile >97th. Table 1 presents the peri- and postnatal parameters and descriptive characteristics. The age at examination did not differ between the different SGA, LGA, and AGA groups. Overall, in 15 participants and 53 eyes, measurements of pRNFL were not possible or excluded because of low scan quality.
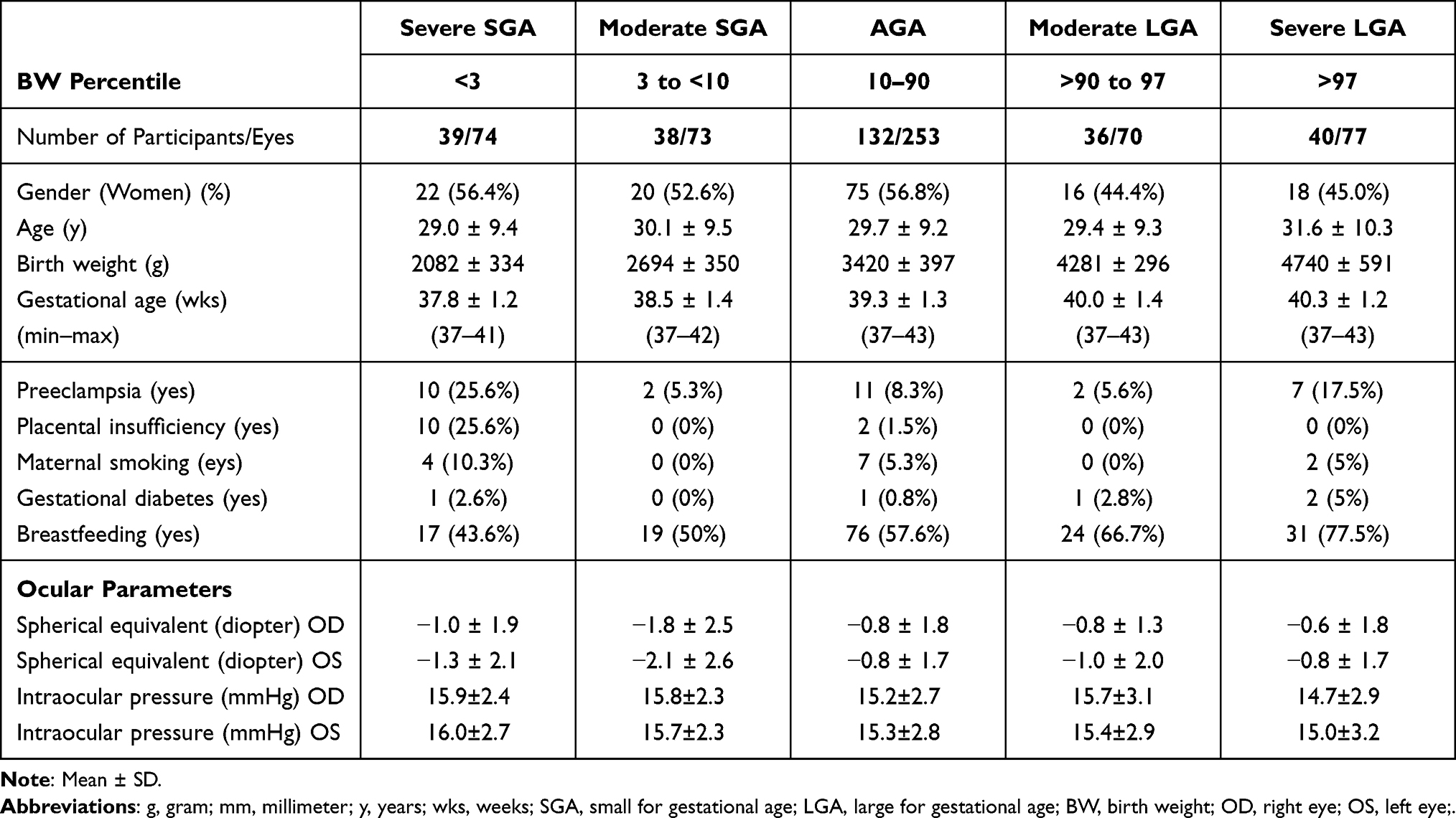 |
Table 1 Characteristics of the Study Sample (n=285) Stratified by Severe and Moderate SGA and LGA Groups |
SGA, AGA and LGA Group
Severe SGA individuals showed the lowest global pRNFL thickness, followed by the moderate SGA group for both right and left eyes (Table 2). Descriptively smaller pRNFL was particularly observed in the SGA groups in the nasal sectors, while the differences were less pronounced in the temporal sectors (Figure 1). The lower BW percentile and thinner global pRNFL showed a nearly linear relationship up to the 25th percentile (Figure 2).
 |
Table 2 Peripapillary Retinal Nerve Fiber Layer Thickness for Each Segment (n=285) and the SGA, AGA, and LGA Study Groups |
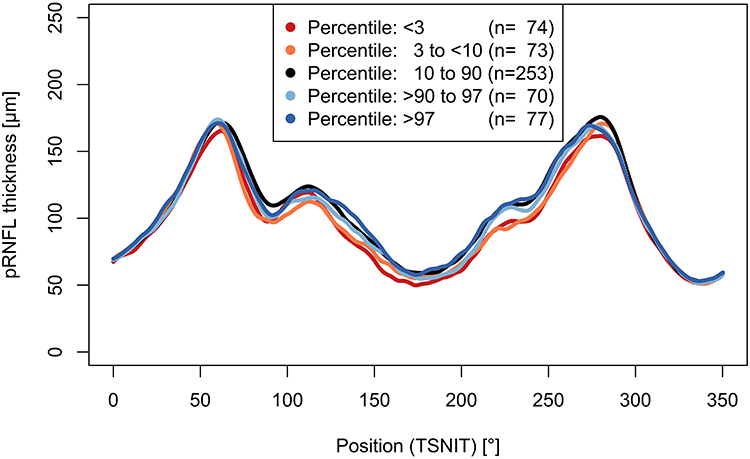 |
Figure 1 Peripapillary retinal nerve fiber layer thickness profile for the different birth weight percentile (SGA, LGA, and AGA) groups. The SGA groups revealed lower pRNFL thickness, especially in the nasal sectors. |
 |
Figure 2 Scatterplot of global peripapillary retinal nerve fiber layer thickness with (A) gestational age, (B) birth weight, and (C) birth weight percentile (n=285). Participants with birth weight percentile below 25 showed lower pRNFL thickness than controls. |
Uni- and Multivariable Analyses
In the multivariable analyses, there was a strong association between low global pRNFL thickness and severe SGA (B=−8.99 [95%-CI: −12.68; −5.298] µm; p<0.001) and in moderate SGA, respectively (B=−6.40 [95%-CI: −10.30; −2.50] µm; p=0.001). This association was more evident in the nasal sectors than the temporal sectors. In contrast, no significant association was observed between global pRNFL and moderate and severe LGA. Uni- and multivariable analyses for the global sector are described in Table 3 and for the different subsectors in Supplementary Tables 1 and 2.
 |
Table 3 Linear Associations of Global Peripapillary Retinal Nerve Fiber Layer Thickness with the Different Birth Weight Percentile Groups (n = 285) and Other Covariates |
None of the other covariates showed an association with global and sectorial pRNFL thickness in multivariable analyses (Table 3 and Supplementary Tables 1 and 2). Furthermore, no correlation was observed between pRNFL thickness and the best corrected visual acuity in the right eyes. Maternal smoking during pregnancy was marginally associated with global pRNFL thickness (p=0.05) in univariate analysis.
Discussion
The present study provides new information regarding the effects of prenatal growth restriction on the neuronal tissue of the optic nerve head as part of the CNS in individuals born at term. Individuals born moderately and severely SGA showed significantly thinner pRNFL measurements in adulthood than controls, with the lowest pRNFL thickness observed in the severe SGA group, particularly in the nasal sectors. This data indicates that fetal growth restriction may exert disturbances in the development of neurologic tissue, which persists in adulthood.
Our study provides a novel approach to investigate pRNFL in a relatively homogeneous cohort of individuals born at term with different degrees of fetal growth restriction, demonstrating that individuals born moderately and severely SGA showed a thinner pRNFL thickness in a dose–response manner in most sectors. There are almost exclusively data available about the effects of growth restriction on pRNFL development in former preterm individuals during infancy,11,12 childhood,13–15 and early adulthood16 and the existing data are inconclusive while nearly no data exist about the effects of growth restriction on pRNFL in soley term individuals.
Some authors reported a thinner pRNFL in children born SGA before and at term in comparison to children born AGA,18,19 while others found no significant differences between these two groups in childhood.17 It is well known that low gestational age is associated with a thin pRNFL in childhood,13 thus, previous reports did not differentiate the effects of prematurity and fetal growth restriction because both have in common low birth weights. Pueyo et al described that children born SGA at term aged 5 to 6 years showed a thinner pRNFL compared to children born AGA at term.20 However, the long-term effects of impaired growth on pRNFL in adulthood in individuals born at term are still unknown. In a recent population-based report of the Gutenberg Health Study, the authors observed in individuals with a low birth weight (<2500 g) a thinner pRNFL compared to individuals with normal birth weight (2500g to 4000 g). However, this data is limited, as gestational age was not surveyed, thus former preterm participants were not excluded. Consequently, the present study is the first highlighting that adults born SGA at term have a thin pRNFL potentially reflecting general changes of the CNS due to impaired growth independent of prematurity.
There are different reports demonstrating the effects of impaired fetal growth on neurostructural and neurodevelopment in preterm infants.25 Impaired fetal growth in these preterm individuals is linked to a smaller cerebral brain volume and a reduction of cortical white and grey matter volume after birth,26 which is still present at 12 months postnatal27 and in childhood.17 Preterm infants frequently experience an early growth restriction in combination with a higher rate of perinatal complications, while the neurodevelopmental outcome in childhood is comparable between SGA children born preterm and SGA children born at term. A correlation was shown between cerebral visual pathway changes, brain atrophy, and a reduction of pRNFL thickness in adults with multiple sclerosis28 corresponding to functional impairment. Rothmann et al observed a relationship between brain damage and thinning of the pRNFL in very preterm infants.6 To date, there is no proven explanation for the pathophysiologic association between alterations of the optic nerve head and variations in regional brain volumes. Some authors assume that a retrograde trans-synaptic degeneration may contribute to this relationship in individuals born preterm, particularly in the case of perinatal adverse events.29 Pueyo et al17 hypothesized that impaired growth and neurological lesions at an early stage of neurodevelopment may lead to retinal changes. They assume that impaired intrauterine growth during fetal development leads to both altered retinal structure formation and abnormal adaptive mechanisms.
There is evidence that maternal cigarette smoking leads to lower pRNFL thickness in childhood and optic nerve atrophy,30,31 while Shen et al12 found no association between maternal smoking and pRNFL. We did find that smoking during pregnancy was marginally associated with global pRNFL thickness (p=0.05) in univariate analysis. However, the number of children with maternal smoking during pregnancy in our cohort was relatively low, which limits our findings.
The present data is of clinical importance because nearly every 10th newborn worldwide is affected by prenatal impaired growth. As the severe SGA group showed the lowest pRNFL thickness, one may speculate that these individuals are at the greatest risk of neurodevelopmental deficits. This hypothesis is supported by the fact that there is already evidence that severe SGA individuals have reduced neurological and intellectual outcomes in childhood.2 Thus, pRNFL measurements could potentially be used as a biomarker to identify children born SGA with increased risk of CNS alterations, which should be examined in a future prospective study but was beyond the scope of this study as brain imaging and neurological testings were not performed.
Strengths and Limitations
A limitation of the present study is its single-center hospital-based study design. Furthermore, it was not possible to contact every former newborn of the UMCM and some individuals declined to participate in the present study. The major strength of the present study is that only former full-term newborns with different degrees of prenatal growth restriction as indicated by differing birth weight percentile represent a relatively homogenous sample with a small range of gestational age. Another strength is the detailed assessment of perinatal history and review of medical records of all participants and their mothers, thus, we were able to calculate a detailed and specific multivariable model with the inclusion of various perinatal parameters potentially affecting pRNFL. Furthermore, all examinations were conducted in accordance with strict standard operating procedures.
Conclusion
This study provides the first data about the relationship between fetal growth restriction and alterations of the neuronal tissue of the optic nerve head as part of the CNS in adulthood. A low birth weight percentile is associated with lower pRNFL in individuals born at term aged 18 to 52 years, indicating that fetal growth restriction has lifelong effects on the neuronal tissue of the CNS potentially contributing to an increased risk of abnormal neurodevelopment.
Access to Data, Responsibility, and Analysis
AF had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Statistical analyses were performed by AF. The analysis presents clinical data of a cohort. This project constitutes a major scientific effort with high methodological standards and detailed guidelines for analysis and publication to ensure scientific analyses are on the highest level. Therefore, data are not made available for the scientific community outside the established and controlled workflows and algorithms. To meet the general idea of verification and reproducibility of scientific findings, we offer access to data at the local database upon request at any time. Interested researchers make their requests to the coordinating PI (Achim Fieß; [email protected]). More detailed contact information is available at the homepages of the UM (www.unimedizin-mainz.de).
Acknowledgments
The whole study team thanks all participants who took part in this study, which includes an enthusiastic team to explore perinatal factors on long-term eye development. This study contains parts of the thesis of Marilena Brandt.
Funding
All authors: Dr Fieß is supported by the Intramural Research Funding (Stufe I) of the University Medical Center of Johannes Gutenberg-University Mainz. The present study was supported by the Ernst-und Berta-Grimmke Stiftung and the Else Kröner-Fresenius-Stiftung. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Schuster AK holds the professorship for ophthalmic healthcare research endowed by “Stiftung Auge” and financed by “Deutsche Ophthalmologische Gesellschaft” and “Berufsverband der Augenärzte Deutschlands e.V.”. Brandt M, Mildenberger E, Urschitz MS, Wagner F, Grabitz S, Hoffmann EM, Pfeiffer N: none.
Disclosure
Pfeiffer N receives financial support and grants from Novartis, Ivantis, Santen, Thea, Boehringer Ingelheim Deutschland GmbH & Co. KG, Alcon, and Sanoculis. Schuster AK receives research support from Allergan, Bayer, Heidelberg Engineering, PlusOptix and Novartis. Dr Achim Fieß reports grants from Ernst and Berte Grimmke Foundation, grants from Else Kröner Fresenius Stiftung, grants from Stufe 1 Support of the University Medical Center Mainz, during the conduct of the study. Professor Esther Maria Hoffmann reports personal fees, non-financial support from Heidelberg Engineering, personal fees, non-financial support from Allergan, personal fees from Santen, personal fees from ORA, personal fees from AbbVie, outside the submitted work. The authors declare that they have no other competing interests.
References
1. Fieß A, Kolb-Keerl R, Schuster AK, et al. Correlation of morphological parameters and visual acuity with neurological development in former preterm children aged 4–10 years. Acta Ophthalmol. 2018;96(8):e1010–e1017. doi:10.1111/aos.13755
2. Figueras F, Gratacós E. Update on the diagnosis and classification of fetal growth restriction and proposal of a stage-based management protocol. Fetal Diagn Ther. 2014;36(2):86–98. doi:10.1159/000357592
3. Miller SL, Huppi PS, Mallard C. The consequences of fetal growth restriction on brain structure and neurodevelopmental outcome. J Physiol. 2016;594(4):807–823. doi:10.1113/JP271402
4. Chiavaroli V, Castorani V, Guidone P, et al. Incidence of infants born small- and large-for-gestational-age in an Italian cohort over a 20-year period and associated risk factors. Ital J Pediatr. 2016;42:42. doi:10.1186/s13052-016-0254-7
5. De Bie HM, Oostrom KJ, Boersma M, et al. Global and regional differences in brain anatomy of young children born small for gestational age. PLoS One. 2011;6(9):e24116. doi:10.1371/journal.pone.0024116
6. Rothman AL, Sevilla MB, Mangalesh S, et al. Thinner retinal nerve fiber layer in very preterm versus term infants and relationship to brain anatomy and neurodevelopment. Am J Ophthalmol. 2015;160(6):1296–1308.e1292. doi:10.1016/j.ajo.2015.09.015
7. Sotirchos ES, Gonzalez Caldito N, Filippatou A, et al. Progressive multiple sclerosis is associated with faster and specific retinal layer atrophy. Ann Neurol. 2020;87(6):885–896. doi:10.1002/ana.25738
8. Unlu M, Gulmez Sevim D, Gultekin M, Karaca C. Correlations among multifocal electroretinography and optical coherence tomography findings in patients with Parkinson’s disease. Neurol Sci. 2018;39(3):533–541. doi:10.1007/s10072-018-3244-2
9. Cunha JP, Proença R, Dias-Santos A, et al. OCT in Alzheimer’s disease: thinning of the RNFL and superior hemiretina. Graefes Arch Clin Exp Ophthalmol. 2017;255(9):1827–1835. doi:10.1007/s00417-017-3715-9
10. Bourne RR et al. (2018). Prevalence and causes of vision loss in high-income countries and in Eastern and Central Europe in 2015: magnitude, temporal trends and projections. Br J Ophthalmol, 102(5), 575–585. 10.1136/bjophthalmol-2017-31125810.1136/bjophthalmol-2017-311258.supp110.1136/bjophthalmol-2017-311258.supp2
11. Shen LL, Mangalesh S, McGeehan B, et al. Birth weight is a significant predictor of retinal nerve fiber layer thickness at 36 weeks postmenstrual age in preterm infants. Am J Ophthalmol. 2020;222:41–53. doi:10.1016/j.ajo.2020.08.043
12. Shen LL, Mangalesh S, Michalak SM, et al. Associations between systemic health and retinal nerve fibre layer thickness in preterm infants at 36 weeks postmenstrual age. Br J Ophthalmol. 2021;bjophthalmol-2021–319254. doi:10.1136/bjophthalmol-2021-319254
13. Fieß A, Christian L, Janz J, et al. Functional analysis and associated factors of the peripapillary retinal nerve fibre layer in former preterm and full-term infants. Br J Ophthalmol. 2017;101(10):1405–1411. doi:10.1136/bjophthalmol-2016-309622
14. Tariq YM, Pai A, Li H, et al. Association of birth parameters with OCT measured macular and retinal nerve fiber layer thickness. Invest Ophthalmol Vis Sci. 2011;52(3):1709–1715. doi:10.1167/iovs.10-6365
15. Wang XY, Huynh SC, Rochtchina E, Mitchell P. Influence of birth parameters on peripapillary nerve fiber layer and macular thickness in six-year-old children. Am J Ophthalmol. 2006;142(3):505–507. doi:10.1016/j.ajo.2006.03.052
16. Fieß A, Schäffler A, Mildenberger E, et al. Peripapillary retinal nerve fiber layer thickness in adults born extremely, very, and moderately preterm with and without ROP: results from the Gutenberg Prematurity Eye Study (GPES). Am J Ophthalmol. 2022;244:88–97.
17. Pueyo V, Pérez T, González I, et al. Retinal structure assessed by OCT as a biomarker of brain development in children born small for gestational age. Br J Ophthalmol. 2017;101(9):1168–1173. doi:10.1136/bjophthalmol-2016-309790
18. Oros D, Altermir I, Elia N, et al. Pathways of neuronal and cognitive development in children born small-for-gestational age or late preterm. Ultrasound Obstetr Gynecol. 2014;43(1):41–47. doi:10.1002/uog.12556
19. Pueyo V, Gonzalez I, Altemir I, et al. Microstructural changes in the retina related to prematurity. Am J Ophthalmol. 2015;159(4):797–802. doi:10.1016/j.ajo.2014.12.015
20. Pueyo V, Oros D, Valle S, et al. Axonal loss and cognitive deficits in term infants with normal umbilical artery Doppler born small-for-gestational age. Ultrasound Obstetr Gynecol. 2012;40(3):297–303. doi:10.1002/uog.11215
21. Fieß A, Nickels S, Urschitz MS, et al. Association of birth weight with peripapillary retinal nerve fiber layer thickness in adulthood—results from a population-based study. Invest Ophthalmol Vis Sci. 2020;61(8):4. doi:10.1167/iovs.61.8.4
22. Voigt M, Fusch C, Olbertz D. Analysis of the Newborn Collective of the Federal Republic of Germany 12. Communication: Presentation of close-meshed percentile values (curves) for the body measurements of newborns. Geburtsh Frauenheilk. 2006;66:956–970. doi:10.1055/s-2006-924458
23. Garway-Heath DF, Rudnicka AR, Lowe T, Foster PJ, Fitzke FW, Hitchings RA. Measurement of optic disc size: equivalence of methods to correct for ocular magnification. Br J Ophthalmol. 1998;82(6):643–649. doi:10.1136/bjo.82.6.643
24. Wu H, de Boer JF, Chen TC. Reproducibility of retinal nerve fiber layer thickness measurements using spectral domain optical coherence tomography. J Glaucoma. 2011;20(8):470–476. doi:10.1097/IJG.0b013e3181f3eb64
25. Meher S, Hernandez-Andrade E, Basheer SN, Lees C. Impact of cerebral redistribution on neurodevelopmental outcome in small-for-gestational-age or growth-restricted babies: a systematic review. Ultrasound Obstetr Gynecol. 2015;46(4):398–404. doi:10.1002/uog.14818
26. de Bie HM, Oostrom KJ, Delemarre-van de Waal HA. Brain development, intelligence and cognitive outcome in children born small for gestational age. Horm Res Paediatr. 2010;73(1):6–14. doi:10.1159/000271911
27. Padilla N, Falcón C, Sanz-Cortés M, et al. Differential effects of intrauterine growth restriction on brain structure and development in preterm infants: a magnetic resonance imaging study. Brain Res. 2011;1382:98–108. doi:10.1016/j.brainres.2011.01.032
28. Gordon-Lipkin E, Chodkowski B, Reich DS, et al. Retinal nerve fiber layer is associated with brain atrophy in multiple sclerosis. Neurology. 2007;69(16):1603–1609. doi:10.1212/01.wnl.0000295995.46586.ae
29. Jacobson L, Hellström A, Flodmark O. Large cups in normal-sized optic discs: a variant of optic nerve hypoplasia in children with periventricular leukomalacia. Arch Ophthalmol. 1997;115(10):1263–1269. doi:10.1001/archopht.1997.01100160433007
30. Pueyo V, Güerri N, Oros D, et al. Effects of smoking during pregnancy on the optic nerve neurodevelopment. Early Hum Dev. 2011;87(5):331–334. doi:10.1016/j.earlhumdev.2011.01.042
31. Ashina H, Li XQ, Olsen EM, Skovgaard AM, Larsen M, Munch IC. Association of maternal smoking during pregnancy and birth weight with retinal nerve fiber layer thickness in children aged 11 or 12 years: the Copenhagen child cohort 2000 eye study. JAMA Ophthalmol. 2017;135(4):331–337. doi:10.1001/jamaophthalmol.2017.0043
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.