")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
A Thematic Analysis Investigating the Inaugural Psychosis REACH Family Ambassador Peer Training Program
Authors Vaswani-Bye A , McCain C, Blank JM, Tennison ME, Kopelovich SL
Received 25 July 2023
Accepted for publication 15 December 2023
Published 8 February 2024 Volume 2024:20 Pages 233—245
DOI https://doi.org/10.2147/NDT.S432255
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Akansha Vaswani-Bye, Chris McCain, Jennifer M Blank, Mackenzie E Tennison, Sarah L Kopelovich
Department of Psychiatry and Behavioral Sciences, University of Washington, Seattle, WA, USA
Correspondence: Akansha Vaswani-Bye, Department of Psychiatry and Behavioral Sciences, University of Washington, Box 359911, 325 Ninth Ave, Seattle, WA, 98104, USA, Tel +1 206-744-9346, Fax +(206) 744-3236, Email [email protected]
Purpose: Caregivers of loved ones with psychosis are tasked with navigating a barren care landscape for their loved ones and for themselves. The dearth of resources they face has a negative impact on outcomes for caregivers and their loved ones. The Psychosis REACH program, based on principles from Cognitive Behavioral Therapy for psychosis was developed as a community-based resource for families to address this care gap. A role for family peers called the Psychosis REACH Family Ambassadors (pRFAs) was developed to reinforce skill learning for caregivers by utilizing a task-sharing approach. This qualitative study sought to better understand pRFAs’ experiences in the inaugural training cohort of this program.
Patients and Methods: Eleven pRFAs participated in semi-structured interviews with research coordinators via teleconference. Questions assessed the quality of the training, challenges and facilitators experienced in their role, and ways in which the program could be improved and expanded. Using thematic analysis, members of the research team coded interviews individually, discussed codes until consensus was reached, and iteratively developed themes based on codes that clustered based on meaning or content.
Results: This process identified 5 key themes: The development of hope and recovery, the development of solidarity networks, the challenges of navigating boundaries, preferred pedagogical strategies, and the need for more support.
Conclusion: Overall, the themes developed from this qualitative analysis demonstrate the value and feasibility of developing a caregiver peer network of pRFAs trained in recovery-oriented care and CBTp-informed skills to support other caregivers. Additionally, they highlight the challenges associated with being in the role of a pRFA and further efforts needed to align training content and learning management systems to the needs of pRFA trainees. These findings highlight the importance of expanding access to family peer training programs for the wellbeing of caregivers and loved ones with psychosis alike.
Keywords: family interventions for psychosis, task-sharing, peer workforce development, family caregivers, cognitive behavioral therapy for psychosis
Introduction
Policies of psychiatric deinstitutionalization and increased use of psychotropic medications in the 1960s moved care for individuals with serious mental illnesses into communities.1 However, these policies were not followed by the development and implementation of accessible community and evidence-based psychosocial interventions. In this contextual landscape, individuals with psychosis often do not have easy access to care and experience social isolation and loneliness.2–4 Their social networks are largely comprised of family members5 who, when involved in their lives and care, have been shown to have a profoundly positive impact on recovery and quality of life indicators, including better treatment outcomes,6 fewer hospital admissions,7 shorter inpatient stays,8 overall improvement in quality of life,9 better work and role performance,10 reduced substance use,11 potentially reduced mortality,12 enhanced adherence to treatment, and reduced relapse rates (as much as 40%13). In a resource-poor landscape of care, family caregivers often take on roles akin to frontline workers. Some estimates suggest that they can spend approximately 20 hours a week on caregiving activities, providing high levels of unpaid care.14 Caregivers are rarely trained by professionals on how best to care for their loved ones experiencing a psychotic disorder, and as a result are vulnerable to high rates of burnout, chronic stress, emotional and physical health conditions, financial stress, stigma, and isolation.15,16 Unequipped with skills to respond to their loved one, they are more likely to fall into unhelpful communication patterns characteristic of hostility, overinvolvement, or criticism, which have been found to negatively impact their loved one’s illness course.17 It is thus integral to support caregivers who are navigating the challenges that caring for a loved one with psychosis entails in facilitating recovery.
As such, Family Interventions for psychosis (FIp) are considered an integral component of a comprehensive treatment plan for individuals with psychosis by organizations like the National Institute for Health and Care Excellence in the United Kingdom18 and the American Psychiatric Association19 in the United States, and meta-analyses have highlighted the importance and effectiveness of FIp.20,21 However, family engagement by service providers in the United States is rare.22–24 A federal audit recently estimated that fewer than 2% of American families receive FIp.25 To increase family engagement and support, more recently developed early intervention programs (eg, NAVIGATE, OnTrack NY) in the United States include family education as an integral part of a multidisciplinary treatment program. But even within these programs, engaging families consistently is an issue – for instance, one study reported that only 29% of families attended 5 or more appointments.26 Barriers to family participation in serious mental illness care have been identified at multiple levels - at the provider level, there is often a lack of training and incentivization to involve families, at the client level, familial estrangement or mistrust may restrict the family’s access to FIp, and at the family level, competing responsibilities or patient privacy laws may impede participation.27
One novel programmatic approach to bolstering the accessibility of FIp is Psychosis Recovery by Enabling Adult Carers at Home (Psychosis REACH28,29). Psychosis REACH trains caregivers in recovery-oriented psychoeducation, high-yield communication strategies, problem-solving, and coping skills derived from cognitive behavioral therapy for psychosis (CBTp), and caregiver self-care. Psychosis REACH bypasses clinical bottlenecks by delivering the intervention directly to community members. It is available as a resource to families regardless of whether their loved ones are engaged in treatment. The program is designed to combat the stigma surrounding psychosis, empower caregivers to reconnect and relate more effectively with their loved ones experiencing psychosis, and mitigate caregiver burnout. The training was piloted in Canada28 and subsequently refined by CBTp and FIp experts in the United States in collaboration with families providing care for loved ones with psychosis. The refined Psychosis REACH training was launched in the United States in 2019 in partnership with the University of Washington. Since then, Psychosis REACH has been iteratively refined based on program evaluation data and stakeholder input, including that of a formal Family and Caregiver Advisory Board. An initial evaluation of Psychosis REACH on trainee outcomes demonstrated reductions in symptoms of depression and anxiety, expressed emotion, caregiver burden, and psychosis-related stigma both immediately after the training and at 4-month follow-up. Examination of trainees’ self-confidence in executing the cognitive and behavioral techniques demonstrated during the workshop revealed a statistically significant reduction in self-perceived skill mastery at 4-month follow-up.29
To both address this decay in skills acquisition and capitalize on the unique benefits offered by peer learning and support within the mental health field,30 we developed a role for Psychosis REACH-trained family members to serve as sources of emotional support and peer coaches to community members once they complete the Psychosis REACH core training. Participants from the first Psychosis REACH training cohort were invited to apply to co-develop the role and serve as the inaugural training cohort of Psychosis REACH Family Ambassadors (pRFAs). The process of co-production with families was critical as involving lived experience stakeholders is more likely to generate knowledge that is relevant, useful, usable, and used.31 Participants were selected on the basis of interest and capacity to work with other family members, availability to participate in a 24-month training program with Psychosis REACH trainers, and prior experience working with other families in similar roles. To inform ongoing model development and evaluation, we engaged in a qualitative analysis of our inaugural cohort of pRFAs. Here we present a thematic analysis of interviews with the inaugural cohort of pRFAs to inform iterative program development.
Materials and Methods
Recruitment of Study Participants
All study procedures were reviewed and approved by the University of Washington Institutional Review Board and as such the study complies with the Declaration of Helsinki. Participants came from a purposive sample of caregivers who participated in the inaugural pRFA training program (N=21). All participants resided in Washington State in the United States. At the end of pRFA training, participants were asked to participate in a one-on-one interview with a research coordinator from the study team who was not involved in training and consultation meetings. In total, 11 pRFAs participated in interviews (response rate = 52.38%). Table 1 presents descriptive statistics of the final sample.
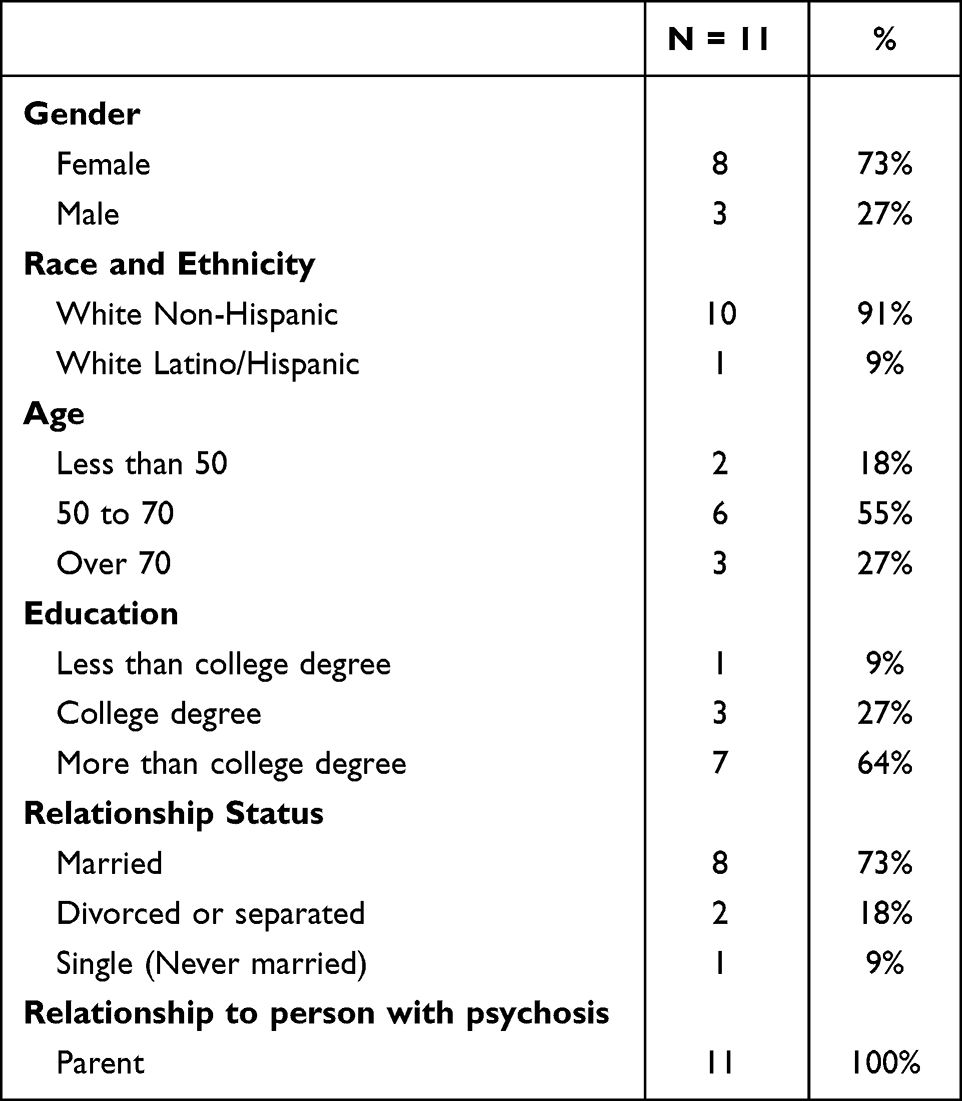 |
Table 1 Demographics of Family Ambassadors |
Interview Procedure
All interviews were conducted on a secure virtual teleconference platform. Prior to the start of each interview, interviewers gathered informed consent from participants, including consent for publication of anonymized responses. Interviewers used a semi-structured interview protocol consisting of open-ended questions and ad-hoc follow-up questions based on responses. On average, interviews lasted 45 minutes. Questions were designed to gather information from participant pRFAs about their experience being part of the inaugural pilot pRFA training program. Specifically, the goal was to collect feedback about the training process designed to teach pRFAs how to support other family members in learning Psychosis REACH concepts and skills.
Questions focused on aspects of the training that pRFAs found most and least valuable, their understanding of the role and scope of a pRFA, the work that they engaged in within the community as a part of their role, the challenges, and barriers encountered, their views on what could be added to the training to better support the pRFA role and their vision of how this program could have the biggest impact on families. Interviews were recorded, de-identified, and transcribed prior to analysis.
Data Analysis
An analytic team of two research coordinators and one psychologist with qualitative experience conducted qualitative data analysis utilizing a thematic analysis approach.32,33 Thematic analysis is considered a useful method for examining the perspectives of different research participants, highlighting similarities and differences, and generating unexpected insights.32 The team systematically and iteratively developed a codebook to identify key themes related to the pRFA experience in three phases. In Phase 1 (Familiarization), members of the team read each transcript twice to familiarize themselves with the data. During this phase, team members noted and reflected upon personal responses to the content, analytic ideas, and data insights. In Phase 2 (Coding), the research coordinators each coded half of the individual transcripts (5–6 transcripts each). Research coordinators met regularly with the psychologist to review, discuss, and revise codes as necessary until consensus was reached among the full team. The psychologist served as an auditor of the final codebook. In Phase 3 (Theme-Building), initial themes were generated by clustering codes that appeared to share core ideas or concepts. Themes were further developed and reviewed by comparing the initial themes against the full dataset in an iterative process.
Results
Through the thematic analysis process we identified five themes organized around core concepts. Overall, the themes developed from this qualitative analysis demonstrate the value and feasibility of developing a caregiver peer network of pRFAs trained in recovery-oriented care and CBTp-informed skills to support other caregivers. Additionally, they highlight the challenges associated with being in the role of a pRFA and further efforts needed to align training content and learning management systems to the needs of pRFA trainees.
Theme 1: The Psychosis REACH Program Supported the Development of “Hope and Recovery” for Families
When reflecting on the skills that are integral to the Psychosis REACH training, pRFAs often first identified the ways in which the skills had impacted their own lives in meaningful ways. Some expressed global changes in overall family dynamics, such as:
I don’t say this lightly. It changed our family. I mean, I felt like we lived in a war zone prior to attending Psychosis REACH.
This description of a “war zone” illustrates sentiments that many pRFAs expressed about their personal experience with psychosis and the ways in which the skills integral to this program impacted them. pRFAs described navigating treatment options, supporting illness exacerbations, managing interruptions in their personal and professional lives, and the emotional work of maintaining relationships during period of increased family stress.
Some pRFAs discussed how small changes in relationships were indicative of hope and change:
But he didn’t call me “mom” for a really long time. And now he calls us mom and dad. Well, to me, these gems of things that we’ve been learning have really made him feel like he’s part of our family again.
Another indication of hope was that several pRFAs reported envisioning a better future for families and loved ones because of the recovery-oriented education that is foundational to this program. This element of the program seemed to engender a sense of optimism that things could be different, and equipped them with a sense of agency and possibility:
I see it as a hope. I had no hope when I came to REACH. REACH gave me hope. Yeah. And most of these families-- most of these families have no hope. They’ve lost it. And suddenly, my story is a story of hope. My son should have been dead, and I probably should have been dead, too, but instead, we laugh.
Moreover, pRFAs attested to the effects the Psychosis REACH principles and learning had on the caregivers to whom they provided peer support:
So they would describe that a technique actually worked or a change in the relationship between themselves and their loved one when they-- I mean, I did not hear anyone say, “What a flop.”
pRFAs also shared their hopefulness about the impact that dissemination of Psychosis REACH could have on other families across the country because of its effectiveness in their own and others’ lives:
What you guys are doing is so fantastic, we are so lucky, and some of the people that I have talked to who live in Durham, North Carolina, or Florida, they are so happy that they were able to take the training online, and so the momentum is growing, I know. It’s just going to be powerful.
Finally, beyond their direct participation, some pRFAs found the mere existence of the program hopeful. Given the historical disenfranchisement of families receiving treatment for serious mental illness, the fact that researchers and academic medical centers were focusing on the needs of families was meaningful to participants:
I was just trying to think of how I would express to you that all of us, as family members, deal with an aspect of health which is not appropriately resourced almost anywhere but especially here. And to have a group of really exciting young researchers who are even interested in this area gives us such hope and a general feeling of being cared about.
Theme 2: Development of Solidarity Networks: Education and Skill-Building in Community
Many pRFAs endorsed prominent isolation in their experience of caregiving before attending Psychosis REACH. They found a strong sense of community in the program, both within their own training cohort and with the family members they coached, which functioned as an antidote to the isolation they had experienced prior to Psychosis REACH.
Several pRFAs described the intangible benefit of learning alongside peers who bring both similar experiences and different perspectives:
It wasn’t just what was being presented by the [training] team, but it was the enrichment that came from the other family ambassadors as well.
pRFAs distinguished the solidarity they found in peer relationships from the kind of support they got from professionals. They emphasized the shared nature of suffering as caregivers which led to a unique bond:
You’re just not going to get it [from professionals]. You get it from people who are suffering through the same things that you are.
Within the framework of pRFA groups, pRFAs discussed finding a quick sense of solidarity and connection with other caregivers:
We walk through life and we don’t look like we would have any sort of pressure like we do. And she looked just like a working mom, and she put her smile on every day and yeah, did the best she could, but she opened up about her son enough, so I thought, “I know you, I know you.”
The sentiment that their experience is a hidden one is indicative of a sense of isolation that was alleviated by the feeling of mutuality. pRFAs reported that in their roles as peers, they were able to address concerns and challenges that professionals or others in the community might not discern. Given that their sense of isolation was further compounded by the ongoing Covid-19 pandemic, this sense of connection and mutuality was especially healing for pRFAs:.
I have to say that given that it’s COVID and a lot of us are isolated, this has been a lifeline for me
Theme 3: Navigating Boundaries Within a Peer Role: Being a pRFA is a Balancing Act
Overall, the pRFAs reported clarity about the scope of the pRFA role, role expectations (ie, running groups, engaging in reflective listening, engaging families in guided rehearsals of Psychosis REACH skills), and prescribed limitations on the role (ie, case management, advice-giving, or addressing concerns related to violence risk). The pRFAs noted that training and written materials about the role were clear and empowered them to assert those boundaries in their work:
I really appreciated the manual, that it does have some really clear definitions and structure, and if the conversation gets to de-escalation or whatever. If there are certain things that come up, it’s not your role to address those things.
While the programmatic expectations were clear, pRFAs often discussed navigating similar predicaments as the caregivers to whom they were providing support and navigating these complexities could sometimes be challenging. Some participants found it more challenging to navigate boundaries around the scope of the pRFA role because of their own lived experience or identity:
[Being a physician] made sticking to the role of Family Ambassador more difficult, and so I’d often have to monitor the sort of power hierarchy issues that are sort of rampant in medicine trying to make sure that I was coming from a perspective of a peer having been through this… sort of stepping back from the ordinary physician role, which is to think that I have all the answers.
pRFAs’ responses emphasized the need for the program to accommodate the shifting needs inherent in caring for a loved one navigating a psychotic disorder, which can be characterized by periods of relapse. This flexibility was identified as necessary for the pRFAs whose capacity to run and recruit for groups varied dynamically with their life circumstances:
I got too much on my plate right now; personal, family and my own issues with my son that I can’t take on anything more than I’m doing, which is you have no idea. It’s just quite a bit.
Given the personal nature of the work, connecting with other caregivers was an emotional experience that sometimes led to feelings of burnout. This seemed more likely when the pRFA was simultaneously supporting a loved through a challenging period and fulfilling their role as a pRFA:
The number one challenge or barrier for me is probably the mental fatigue I suffered by already having to deal with my current situation with my son, who has a mental health issue. So a person only has so much capacity. And, you know, you’re not used to serving a bunch of people obviously at one time. So the mental capacity and already serving a loved one kind of makes you feel a little stretched, I guess.
pRFAs also acknowledged that the degree of participation of caregivers was predicated on whether crises were occurring in their lives. Some found that succeeding in the pRFA role required them to moderate their interactions according to the capacity and unique needs of the families they were supporting and appreciated that the program allowed them to do so:
Given the predictable chaos that a lot of people’s families are in, episodic illness of our loved ones, it certainly varies. So some people that I had intense contact with during times of crisis for probably four or five months. There’s still one that I meet along the lines, I think, most carefully of what we’re supposed to be doing every two weeks for a couple of hours. And then, there’s some that we’re very intense for a period of time who [later] completely disappeared.
Some pRFAs felt that, because of how their more in-depth training with the Psychosis REACH program had shaped their understanding of psychosis, they had a different perspective on the nature of mental illness and the utility of CBTp-informed skills. It was challenging for some to navigate working with caregivers who blamed loved ones for their symptoms, or did not readily adopt a recovery orientation:
Many families think, “Well, they’re just choosing to be like this.” And I kind of want to hit them on the head or something because nobody would choose to be in psychosis. And that has been extremely challenging for me to find compassion in that for the family members.
Finally, some pRFAs expressed complex feelings around the boundaries involved in interacting with expert clinician trainers. Some noted that it was challenging to have access to expert clinicians to support them in their role as peer trainers but not for the treatment of their own family:
It’s like if you are dying of thirst and you’re in a room and there’s a well and there’s a sign on it that says, “This well is not for your personal use…” It’s to be in a meeting with [the training team] and what you want to say is, “Please help my son.” And you can’t. It’s a difficult thing.
Theme 4: Preferred Pedagogical Strategies
Since all training activities and most connections with caregivers were virtual, the pRFA role by design required a degree of comfort with communication technology. The training and consultation team provided pRFAs with a wide range of electronic resources including online forums, written materials, and archival videos. pRFAs acknowledged the theoretical utility of these materials, but often felt that they were not pragmatically useful, and reported a lack of confidence in accessing asynchronous materials on the learning management system used to facilitate learning. In addition, some pRFAs felt they spent too much time navigating these resources and articulated the need for more support from the training team in managing technical challenges. Some pRFAs did not access them at all, preferring other modes of learning and some suggested that the training team could have scaffolded exposure to the manual instead of presenting it in its entirety:
I know we have [the virtual] manual. I know I read it at the beginning. There were [sic] probably twice that I looked for things in it, but it’s so rich in resources that I think I still haven’t begun to think of all the ways I could apply it and use it. So it’s one of the things that I would probably need a nudge, something to look for or that it was going to be the focus the next week, so I would have a reason to go back into it.
Participants recurrently reported that repetition of training materials was a helpful element of the learning approach. A particularly useful practice pRFAs noted was attending the foundational Psychosis REACH live training more than once:
Well, actually it was the third time I did the training. I do not really know specifically. I just know that I felt like I learned the things rather than just hearing the things.
Others appreciated the extensive opportunity to practice skills in consultation calls which included repetition of core training concepts:
Well, what was very valuable was having access to the excellent trainers and staff at UW and their contractors to further disseminate and reinforce information that we learned in the FIRST skills basic training that I attended.
Finally, others mentioned that they were motivated to review written materials to continually refresh their own understanding:
Some of the ones about redirecting discussion, creating boundaries, whose story was whose, were really excellent, and I had to keep reading them, again and again, to try to incorporate them.
By far, pRFAs identified the most useful modes of learning as those geared towards direct, interpersonal interaction:
I’m more people-oriented. I can interact with people. I can talk to people. I can explain my role. I can talk about my situation and what I’ve learned and how I apply it. I can do all those things best one-on-one or in a group. And so those two things were the most helpful to me.
pRFAs felt that role-plays and interactive discussions with the caregivers they were working with was an essential means of translating the theoretical material from Psychosis REACH trainings into practical application strategies:
I think practice dialogue (is the most useful) because that always seemed to be that they want concrete ways of communication. I think that that’s what a lot of people are looking for. And just also understanding when you’re practicing dialogue, you are realizing,“Oh, goodness, I haven’t been doing that at all.”
Beyond skill acquisition, role-play enabled participants to build a more empathic understanding of their loved one’s experience as well as experience firsthand the emotional effects of improved communication:
And then even during our training, one of the role-plays we had to do with a partner, we had to pretend to be our child and then the other parent had to try to de-escalate us or work with us in some way. And it was amazing to me how being empathetic and listening - I was really getting ramped up in being angry - and my partner [de-identified], just by listening in and responding to me in an empathetic way I could just feel my anger go down, which I thought was really powerful.
Theme 5: Need for More Support in Implementing the pRFA Role
Several pRFAs noted that participating in the inaugural cohort of pRFAs also came with some challenges. Within their role, pRFAs had to not only organize and initiate groups, but also learn how to incorporate the Psychosis REACH skills into their meetings while managing group dynamics with family members at different stages in their caregiving journeys.
Structurally, pFRAs expressed that additional support would have helped in all three phases: initiating groups, running groups, and ending groups. First, many pRFAs were not able to form sustainable groups, and wondered whether this was linked to caregivers’ desire to connect with pRFAs who were relatable in terms of identity and background variables. As one pRFA described it:
Can I relate to you? Right. Do you have a child that looks like my child? The more you can find the people who are more squarely in the space you are in, the more you feel like they can understand. That’s just natural.
In response to these challenges with initiating groups, many pRFAs instead facilitated other types of support, such as individual sessions or email correspondence. pRFAs expressed disappointment at this predicament and expressed that more support from the team could help facilitate group formation. Second, pRFAs who successfully launched groups disclosed that sustaining their group posed unique challenges both experientially and logistically. As one pRFA described:
I don’t have a huge number of groups, and mine are just ongoing. This is just for four weeks because they don’t seem to be learning the skills, or I’m not good at teaching it. I don’t know. I am a little hard on myself at times.
Experientially, many expressed a desire for ongoing feedback on their group facilitation skills from the training team for issues like managing dropouts, responding to difficult questions, and locating resources for families who were geographically remote from them. Some respondents expressed uncertainty about how to respond to the ideological, familial, social, cultural, clinical, geographic, and economic differences between family members. For example, some caregivers had close connections with their loved one, whereas others were not on speaking terms.
Some families were also navigating crisis situations, which had the potential to trigger pRFAs’ adverse experiences with their own loved ones. The quote below illustrates the tension that some pRFAs felt between responding to the needs that caregivers identify (in this case, addressing substance use), and managing their own emotions related to hardships they experienced with their loved ones:
Something that I missed so much and it’s like a huge chunk of what’s missing from this program, and that is drug use, substance abuse, addiction because that adds. My son is also-- he was never a needle or heroin user until he moved to the [location]. Well, now he’s on methadone because I told him, I said, “I’m not going to give you ultimatums. I love you. I want you in my life, but I will tell you, I know for sure that I do not know how long I can take this.”
Logistically, pRFAs also requested more concrete operational support for the pRFA-led groups in the form of developing agenda templates and syllabi. Respondent pRFAs said that this additional structural support from the training team would have engendered greater confidence, especially when they were first starting to work with families.
Finally, after groups had run their course, respondents reported challenges with identifying how or when to end pRFA meetings with families:
I don’t know. It’s hard for me to just cut it off completely.
pRFAs reported that the intimate nature of the meetings and the vulnerability of group members created bonds that they were reticent to disband. Such concerns highlight the tension in the intimacy of the peer role that is encompassed by pRFAs.
Discussion
We engaged in a thematic analysis of data from semi-structured interviews with a self-selecting sample of the inaugural cohort of family caregivers who were trained as pRFAs. De-identified data were independently reviewed by researchers who were not involved in the inaugural pRFA training.
Approximately half of the inaugural cohort of pRFAs elected to participate in the research interviews. Participants were homogenous in their racial and ethnic identities and relationship to their loved one experiencing a psychotic disorder, but varied in their gender identity, age, highest level of education, and marital status.
Overall, five key themes about pRFAs’ experience were identified. The five themes include: The development of hope and recovery, the development of solidarity networks, the challenges of navigating boundaries, preferred pedagogical strategies, and the need for more support. Across themes, a consistent finding was that the Psychosis REACH program, and specifically the principles and skills to which pRFAs were introduced, enabled the pFRAs and the caregivers they supported to reconnect with loved ones and understand their experiences more deeply. This was facilitated by their ability to apply the education and skills they learned toward more collaborative and adaptive relationships. This is a promising finding as healthy relationships are a key protective factor in the recovery from a psychotic disorder.34 For instance, social interactions provide an individual experiencing paranoid ideation with opportunities to discuss both, their concerns and alternative explanations with trusted people in their lives.35 Families trained in Psychosis REACH are guided in communication strategies like befriending, normalization, reflective listening, and identifying a shared goal as a precursor to helping their loved one begin to make sense of challenging experiences and develop new skills to progress toward valued goals and outcomes.
Relatedly, isolation among people experiencing psychosis can also be a function of stigma at both individual (eg, beliefs about the label of psychosis) and institutional or structural levels (eg, social effects of long-term psychiatric hospitalization, lack of resources for reintegration into the community, or unemployment).36,37 Leveraging caregiver involvement and advocacy to resist the effects of stigma within relational dyads and to create systemic change is a model used successfully in other areas where caregiver involvement is warranted. For instance, parents of children with developmental disabilities have used parent-to-parent mentoring and peer support to mobilize toward advocating for increased development of services using a rights-based discursive framework.38 This is more likely to occur when caregivers feel a sense of community and solidarity with one another, as most pRFAs found the program created for themselves and the caregivers they connected with.
Further, research indicates that caregivers’ perceptions of mental illness or feelings of powerlessness about their loved one’s diagnosis can lead them to experience increased stress, depression, and negative self-perceptions of their own abilities to effect change.39 Additionally, when the relationship between the caregiver and loved one is emotionally challenging, caregivers are more likely to believe that loved ones’ symptoms are linked to deliberate intentions, which can lead to increased blame,40 or maladaptive responses at the expense of the relationship. This has been found to negatively impact both caregivers’ and loved ones’ sense of well-being.41 As an antidote to these caregiver states, the pRFAs discussed the aspects of the program that led to a) more helpful attributions (eg, psychosis is not their or their loved one’s fault), b) collaborative and relationally oriented interaction patterns, and c) a hope-oriented mindset. These included many important moments of learning the philosophy of recovery that is foundational to the Psychosis REACH program, specific skills to improve trust and communication with their loved ones, and skills to manage their own emotions. The feelings of hope generated in this program may be an important mediator for positive caregiving relationships. This may be linked to positive relationship appraisal that focuses on the loved one needing help with problems that can be addressed by working together as a team.39
In addition to individuals with psychosis, caregivers of people living with psychosis also report significant isolation15 and this was also a key finding in the present analysis. The pRFAs noted that the caregivers they met really needed a space to be heard, understood, and listened to, highlighting that their isolation found at least partial relief within this program. pRFAs positioned themselves as mutual aid workers42 whilst connecting with caregivers, in groups or individual meetings, by respecting the expertise and lived experience of all parties in their interactions. Additionally, pRFA participants were also engaged in advocacy efforts43 as they normalized mental illness, engaged in social and political action by supporting others in a similar situation, and sharing their personal stories. This finding suggests that engaging caregiver peers in supporting other caregivers is an important step toward replacing stigmatizing beliefs about psychosis with self-affirming beliefs, which is considered a central feature of effective stigma reduction campaigns.44 Finally, having a community of other pRFA trainees provided a network of people with different perspectives to learn from. This had a positive impact on coping skills, distress reduction and feelings of empowerment, as found in other mutual assistance interventions.45
The barriers that pRFAs discussed were linked closely to the perception that the technology used to support their learning was not user-friendly. Research suggests that older adult learners, like our participants, prefer e-learning modules that present information step-by-step and contain practice questions and examples.46 The learning management system used in this pilot training was utilized more as an information repository, rather than a learning engagement tool and it was perceived as more overwhelming than useful. Additionally, participants reported that practicing the skills rather than just hearing about them was a more effective pedagogical approach. These perspectives suggest that a shift in e-learning tools that scaffold information and provide more opportunities to practice skills during live consultation calls may be a more productive direction to facilitate learning and retention in future iterations of training. Finally, participants mentioned that they needed more support with the logistical requirements of the pRFA role, especially in terms of initiating and sustaining skills-focused groups. This finding implies that this is an area where more structural and pragmatic support from the training and implementation team is warranted.
Another challenge pRFAs described was the emotional and cognitive demands of being peer volunteers whilst navigating their own role as caregivers. Their perspectives on this matter are important to understand in the context of the barren service landscape for families impacted by psychosis. As highlighted in the introduction, less than 2% of families receive FIp so it is possible that pRFAs were the only support the caregivers they met with could access. Additionally, peer workers report similar levels of burnout to mental health professionals47,48 Further understanding of and responsiveness to the risk of burnout is an important consideration for future iterations of the pRFA training program. Finally, even when FIp are available, research suggests that they do not fully account for caregivers’ understandable emotional responses to their loved ones’ diagnosis as they tend to be more focused on the person with psychosis.49 Our research suggests that pRFAs can supplement deficiencies in clinic-based FIp offered to families navigating psychosis, but that they also would benefit from care contexts that provide FIp that includes psychoeducation, skills training, and emotional support.
Limitations
Limitations of this study include several aspects of representation. All participants in the inaugural training cohort resided in one state in the United States (Washington) and perspectives of pRFAs from other parts of the country were not included. Additionally, caregivers who took part in groups run by pFRAs were not interviewed, and thus their experiences can only be viewed through the lenses of the pFRAs. Our participants were quite homogenous in terms of their identified racial/ethnic backgrounds (see Table 1) – all identified as White, and one as Latino/Hispanic. Moreover, all participants were parents of a loved one with psychosis, the majority were married, over 50 years old, had at least a college degree, and identified as women. Therefore, findings may be missing important implications from a diversity and equity perspective and from the perspective of other forms of caregiving relationships.
Conclusion
Psychosis REACH has been iteratively developed for and with families who support individuals experiencing psychotic symptoms. The purpose of this study was to understand the inaugural training experience of the caregiver peer role we developed called the pRFA, to support families in implementation of skills, and to inform future iterations of both training models and processes, thus enhancing intervention and implementation co-production. Additionally, it provided useful information about skills-focused and peer-delivered approaches to FIp, and our findings suggest that it is important to increase access to family peer interventions in both clinical and community-based settings to ensure that caregivers of individuals with psychosis are supported in their pursuit of recovery for their loved one, irrespective of engagement with treatment teams.
Holistically, our analysis lends support to the value and feasibility of developing a caregiver peer network that can enhance the translation of psychosis caregiver education and skills training to community members. This model is consistent with a task sharing approach, which has been identified as a viable and effective global mental health strategy.50 Additionally, our analysis spotlighted important challenges associated with being in the role of a pRFA and the additional efforts needed to align training content and modalities to the needs of pRFAs. Although pRFAs were forthcoming in their report of the nuanced challenges they experienced in their training and delivery of pRFA functions, they also expressed gratitude, a sense of satisfaction from the community they built, and the changes they were able to help other caregivers foster with their loved ones. Thus, this study adds to the literature by a) highlighting the needs of caregiver peer workers that should be addressed in current and future peer workforce programs, and b) addressing important implications for collaborations between caregivers and professionals to support individuals with psychosis through recovery.
Acknowledgments
We sincerely thank all the families who participated in the inaugural pRFA program and appreciate their time, expertise, lived experience wisdom, and generosity in co-constructing this program with us. We are also grateful for our colleagues at the University of Washington for their continued support and our collaborating partners in Psychosis REACH implementation, Drs. Turkington and Hardy.
Disclosure
Dr Sarah Kopelovich reports grants from University of Washington, and grants from Washington State Health Care Authority, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Erickson B. Deinstitutionalization through optimism: the community mental health act of 1963. Am J Psychiatry Resid J. 2021;16(4):6–7. doi:10.1176/appi.ajp-rj.2021.160404
2. Giacco D, Palumbo C, Strappelli N, Catapano F, Priebe S. Social contacts and loneliness in people with psychotic and mood disorders. Compr Psychiatry. 2016;66:59–66. doi:10.1016/j.comppsych.2015.12.008
3. Stefanidou T, Wang J, Morant N, Lloyd-Evans B, Johnson S. Loneliness in early psychosis: a qualitative study exploring the views of mental health practitioners in early intervention services. BMC Psychiatry. 2021;21(1):134. doi:10.1186/s12888-021-03138-w
4. Velthorst E, Fett AJ, Reichenberg A, et al. The 20-year longitudinal trajectories of social functioning in individuals with psychotic disorders. Am J Psychiatry. 2017;174(11):1075–1085. doi:10.1176/appi.ajp.2016.15111419
5. Palumbo C, Volpe U, Matanov A, Priebe S, Giacco D. Social networks of patients with psychosis: a systematic review. BMC Res Notes. 2015;8:560. doi:10.1186/s13104-015-1528-7
6. Glick ID, Stekoll AH, Hays S. The role of the family and improvement in treatment maintenance, adherence, and outcome for schizophrenia. J Clin Psychopharmacol. 2011;31(1):82–85. doi:10.1097/JCP.0b013e31820597fa
7. Pitschel-Walz G, Leucht S, Bauml J, Kissling W, Engel RR. The effect of family interventions on relapse and rehospitalization in schizophrenia - A meta-analysis. Schizophr Bull. 2001;27(1):73–92. doi:10.1093/oxfordjournals.schbul.a006861
8. Pfammatter M, Junghan UM, Brenner HD. Efficacy of psychological therapy in schizophrenia: conclusions from meta-analyses. Schizophr Bull. 2006;32(Suppl 1):S64–S80. doi:10.1093/schbul/sbl030
9. Evert H, Harvey C, Trauer T, Herrman H. The relationship between social networks and occupational and self-care functioning in people with psychosis. Soc Psychiatry Psychiatr Epidemiol. 2003;38(4):180–188. doi:10.1007/s00127-003-0617-4
10. Brekke JS, Mathiesen SG. Effects of parental involvement on the functioning of noninstitutionalized adults with schizophrenia. Psychiatr Serv. 1995;46(11):1149–1155.
11. Clark RE. Family support and substance use outcomes for persons with mental illness and substance use disorders. Schizophr Bull. 2001;27(1):93–101. doi:10.1093/oxfordjournals.schbul.a006862
12. Revier CJ, Reininghaus U, Dutta R, et al. Ten-year outcomes of first-episode psychoses in the MRC AESOP-10 study. J Nerv Ment Dis. 2015;203(5):379–386. doi:10.1097/NMD.0000000000000295
13. Knapp M, Andrew A, McDaid D, et al. Investing in Recovery: Making the Business Case for Effective Interventions for People with Schizophrenia and Psychosis. London: London School of Economics and Political Science; 2014.
14. Flyckt L, Lothman A, Jorgensen L, Rylander A, Koernig T. Burden of informal care giving to patients with psychoses: a descriptive and methodological study. Int J Soc Psychiatry. 2013;59(2):137–146. doi:10.1177/0020764011427239
15. Hayes L, Hawthorne G, Farhall J, O’Hanlon B, Harvey C. Quality of life and social isolation among caregivers of adults with schizophrenia: policy and outcomes. Community Ment Health J. 2015;51(5):591–597. doi:10.1007/s10597-015-9848-6
16. Kadakia A, Catillon M, Fan Q, et al. The economic burden of schizophrenia in the United States. J Clin Psychiatry. 2022;83(6):43278. doi:10.4088/JCP.22m14458
17. Bogojevic G, Ziravac L, Zigmund D. Impact of expressed emotion on the course of schizophrenia. Eur Psychiatry. 2015;30:390. doi:10.1016/S0924-9338(15)30309-6
18. National Institute For Clinical Excellence. Psychosis and schizophrenia in adults: prevention and management: clinical guideline [CG178]. Available from: https://www.nice.org.uk/guidance/cg178.
19. Keepers GA, Fochtmann LJ, Anzia JM, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia. Am J Psychiatry. 2020;177(9):868–872. doi:10.1176/appi.ajp.2020.177901
20. Camacho-Gomez M, Castellvi P. Effectiveness of family intervention for preventing relapse in first-episode psychosis until 24 months of follow-up: a systematic review with meta-analysis of randomized controlled trials. Schizophr Bull. 2020;46(1):98–109. doi:10.1093/schbul/sbz038
21. Rodolico A, Bighelli I, Avanzato C, et al. Family interventions for relapse prevention in schizophrenia: a systematic review and network meta-analysis. Lancet Psychiatry. 2022;9(3):211–221. doi:10.1016/S2215-0366(21)00437-5
22. Hjarthag F, Persson K, Ingvarsdotter K, Ostman M. Professional views of supporting relatives of mental health clients with severe mental illness. Int J Soc Psychiatry. 2017;63(1):63–69. doi:10.1177/0020764016682268
23. Lavoie-Tremblay M, Bonin JP, Bonneville-Roussy A, et al. Families’ and decision makers’ experiences with mental health care reform: the challenge of collaboration. Arch Psychiatr Nurs. 2012;26(4):e41–50. doi:10.1016/j.apnu.2012.04.007
24. Marshall T, Solomon P. Provider contact with families of adults with severe mental illness: taking a closer look. Fam Process. 2004;43(2):209–216. doi:10.1111/j.1545-5300.2004.04302006.x
25. McCance-Katz EF, Hargan F, Carson ED, et al. Interdepartmental Serious Mental Illness Coordinating Committee (ISMICC). 2017 Report to Congress: “The Way Forward: federal Action for a System That Works for All People Living with Serious Mental Illness (SMI) and Serious Emotional Disturbance (SME) and Their Families and Caregivers.” U.S. Department of Health and Human Services (DHHS), December 13, 2017. Available at https://www.samhsa.gov/sites/default/files/programs_campaigns/ismicc_2017_report_to_congress.pdf.
26. Glynn S, Gingerich S, Meyer-Kalos P, et al. T255. Who participated in family work in the US raise-etp first episode sample? Schizophrenia Bulletin. 2018;44(Suppl 1):S216–S217. doi:10.1093/schbul/sby016.531
27. Landeweer E, Molewijk B, Hem MH, Pedersen R. Worlds apart? A scoping review addressing different stakeholder perspectives on barriers to family involvement in the care for persons with severe mental illness. BMC Health Serv Res. 2017;17(1):349. doi:10.1186/s12913-017-2213-4
28. Turkington D, Gega L, Lebert L, et al. A training model for relatives and friends in cognitive behaviour therapy (CBT) informed care for psychosis. Cogent Psychol. 2018;5(1):1–15. doi:10.1080/23311908.2018.1497749
29. Kopelovich SL, Stiles B, Monroe-DeVita M, Hardy K, Hallgren K, Turkington D. Psychosis REACH: effects of a brief CBT-informed training for family and caregivers of individuals with psychosis. Psychiatr Serv. 2021;72(11):1254–1260. doi:10.1176/appi.ps.202000740
30. Mead S, Hilton D, Curtis L. Peer support: a theoretical perspective. Psychiatr Rehabil J. 2001;25(2):134–141. doi:10.1037/h0095032
31. Graham ID, McCutcheon C, Kothari A. Exploring the frontiers of research co-production: the Integrated Knowledge Translation Research Network concept papers. Health Res Policy Syst. 2019;17(1):88. doi:10.1186/s12961-019-0501-7
32. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
33. Clarke V, Braun V. Thematic analysis: a practical guide. Thematic Analysis. 2021;1–100.
34. Fett AJ, Hanssen E, Eemers M, Peters E, Shergill SS. Social isolation and psychosis: an investigation of social interactions and paranoia in daily life. Eur Arch Psychiatry Clin Neurosci. 2022;272(1):119–127. doi:10.1007/s00406-021-01278-4
35. Freeman D, Garety PA, Kuipers E, Fowler D, Bebbington PE. A cognitive model of persecutory delusions. Br J Clin Psychol. 2002;41(Pt 4):331–347. doi:10.1348/014466502760387461
36. Brouwers EPM. Social stigma is an underestimated contributing factor to unemployment in people with mental illness or mental health issues: position paper and future directions. BMC Psychol. 2020;8(1):36. doi:10.1186/s40359-020-00399-0
37. Xanthopoulou PD, Mbanu J, Chevalier A, Webber M, Giacco D. Social isolation and psychosis: perspectives from people with psychosis, family caregivers and mental health professionals. Community Ment Health J. 2022;58(7):1338–1345. doi:10.1007/s10597-022-00941-x
38. Szlamka Z, Tekola B, Hoekstra R, Hanlon C. The role of advocacy and empowerment in shaping service development for families raising children with developmental disabilities. Health Expect. 2022;25(4):1882–1891. doi:10.1111/hex.13539
39. Kuipers E, Onwumere J, Bebbington P. Cognitive model of caregiving in psychosis. Br J Psychiatry. 2010;196(4):259–265. doi:10.1192/bjp.bp.109.070466
40. Barrowclough C, Hooley JM. Attributions and expressed emotion: a review. Clin Psychol Rev. 2003;23(6):849–880. doi:10.1016/S0272-7358(03)00075-8
41. Onwumere J, Kuipers E, Bebbington P, et al. Patient perceptions of caregiver criticism in psychosis: links with patient and caregiver functioning. J Nerv Ment Dis. 2009;197(2):85–91. doi:10.1097/NMD.0b013e3181960e57
42. Steinberg DM. The Mutual-Aid Approach to Working with Groups: Helping People Help One Another.
43. Schaffer MA. Speaking up: how family members advocate for relatives living with a mental illness. Community Ment Health J. 2021;57(8):1547–1555. doi:10.1007/s10597-021-00775-z
44. Corrigan PW. Lessons learned from unintended consequences about erasing the stigma of mental illness. World Psychiatry. 2016;15(1):67–73. doi:10.1002/wps.20295
45. Dixon LB, Lucksted A, Medoff DR, et al. Outcomes of a randomized study of a peer-taught Family-to-Family Education Program for mental illness. Psychiatr Serv. 2011;62(6):591–597. doi:10.1176/ps.62.6.pss6206_0591
46. Pappas MA, Demertzi E, Papagerasimou Y, Koukianakis L, Voukelatos N, Drigas A. Cognitive-based e-learning design for older adults. Soc Sci-Basel. 2019;8(1):6. doi:10.3390/socsci8010006
47. Park SG, Chang BH, Mueller L, Resnick SG, Eisen SV. Predictors of employment burnout among VHA peer support specialists. Psychiatr Serv. 2016;67(10):1109–1115. doi:10.1176/appi.ps.201500239
48. Janouskova M, Vlckova K, Harcuba V, Kluckova T, Motlova J, Bankovska Motlova L. The challenges of inter-role conflicts for peer support workers. Psychiatr Serv. 2022;73(12):1424–1427. doi:10.1176/appi.ps.202100566
49. Lavis A, Lester H, Everard L, et al. Layers of listening: qualitative analysis of the impact of early intervention services for first-episode psychosis on carers’ experiences. Br J Psychiatry. 2015;207(2):135–142. doi:10.1192/bjp.bp.114.146415
50. Stevens C, Tosatti E, Ayer L, et al. Helpers in Plain Sight: A Guide to Implementing Mental Health Task Sharing in Community-Based Organizations. RAND; 2015.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.