")
Back to Journals » Infection and Drug Resistance » Volume 17
A Risk Model for 28-Day in-Hospital Mortality in 173 COVID-19 Patients Admission to ICU: A Retrospective Study
Authors Hua Y , Zhou Y, Qin Z, Mu Y , Wang T , Ruan H
Received 30 October 2023
Accepted for publication 5 March 2024
Published 23 March 2024 Volume 2024:17 Pages 1171—1184
DOI https://doi.org/10.2147/IDR.S447326
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Sandip Patil
Yiting Hua,1,2,* Yutong Zhou,1,2,* Ziyue Qin,1,2 Yuan Mu,1,2 Ting Wang,1,2 Haoyu Ruan1,2
1Department of Laboratory Medicine, the First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 2Branch of National Clinical Research Center for Laboratory Medicine, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haoyu Ruan; Ting Wang, Department of Laboratory Medicine, the First Affiliated Hospital, Nanjing Medical University, 300 Guang Zhou Road, Nanjing, Jiangsu Province, 210029, People’s Republic of China, Email [email protected]; [email protected]
Background: The surge in the number of patients diagnosed with COVID-19 since China’s open-door policy has placed a huge burden on the public healthcare system, especially the intensive care system. This study’s objective was to discover possible clinical outcome predictors in COVID-19 patients treated in intensive care units (ICUs) and to provide useful information for future preventative efforts and therapies.
Methods: This retrospective study included 173 COVID-19 critically ill patients and reviewed the 28-day survival outcome in the First Affiliated Hospital of Nanjing Medical University. Competing risk analysis was performed to predict the cumulative incidence function (CIF) of mortality in hospital. The independent prognostic factors were identified by applying the Fine–Gray proportional subdistribution hazard model. Receiver operating characteristic (ROC) curves were used to evaluate model efficacy, and calibration curves were used to validate the model. Finally, we compared the competing risk model with the traditional proportional hazards model (Cox regression model) using CIF.
Results: Of these 173 patients, 66 (38.2%) survived, 55 (31.8%) died, and 52 (30.0%) discharged. In univariate analysis, 12 variables were significantly correlated with mortality. In multivariate analysis, Age, Neutrophil ratio, Direct Bilirubin (DBIL) and Renal disease were independent predictors of 28-day outcome. The ROC curve of the multivariate prediction model showed an AUC (area under the curve) of 0.790. The results of the calibration curve and the concordance index (C-index) show that the model has good discriminatory power. The competing risk model we applied was more accurate than the Cox model.
Conclusion: We presented a more accurate multivariate prediction model for 28-day in-hospital mortality for ICU COVID-19 patients using a competing risk model.
Keywords: COVID-19, 28-day mortality, competing-risk analysis, ICU
Introduction
COVID-19 pandemic has been one of the most severe problems for contemporary medicine and public health systems worldwidely since its emergency.1,2 Symptoms vary in COVID-19 patients, ranging from asymptomatic to severe pneumonia, acute respiratory distress syndrome (ARDS), respiratory failure, or multi-organ failure.3 According to early epidemiological reports, 80% of cases have only mild symptoms, 20% required hospitalization, and 4% further required intensive care unit treatment.4 ICU COVID-19 patients demand more inclination of medical resources such as respiratory support, including invasive mechanical ventilation (IMV), noninvasive mechanical ventilation (NIV), and high-flow nasal cannula (HFNC) oxygen therapy, as well as specialized nursing staff, causing higher public health care burden.5,6 Since December 2022, China has begun its epidemic liberalization policy. The number of infections has surged accordingly, which has brought huge burden on the health care system. ICUs have been fully loaded and even overloaded for patients with COVID-19.7 Early identification of risk factors for critically ill patients with COVID-19 can help make medical decision for timely and effective management.8,9
There have been many investigations trying to discover risk factors for the deaths of COVID-19 patients.10–15 In a retrospective study including 2529 patients, researchers established a risk model of COVID-19 to predict in-hospital mortality and complications, and identify high-risk patients with poor prognosis,16 which included old age, history of heart disease, lymphocyte ratio, Procalcitonin (PCT), and D-D dimers. Stephen, et al17 developed a simple and practical 4C Mortality Score based on basic epidemiologic, clinical, and laboratory data to predict mortality among hospitalized patients with COVID-19. For COVID-19 ICU patients, Cheng, et al18 combined chest radiographs and clinical data to build a deep learning model to predict mortality. Amir, et al19 focused on a combined systemic inflammation index which reflected the prognosis of patients with COVID-19 infection admitted to the ICU. Finally, they identified age and derived neutrophils/(leukocytes minus neutrophils) ratio (dNLR) as valuable predictors of mortality in ICU hospitalized COVID-19 patients. David, et al20 used samples from a large multicenter cohort of COVID-19 critically ill patients to construct a blood miRNA classifier that could be used to predict all-cause mortality in the ICU. The clinical outcome predictors for the mortality of ICU COVID-19 patients were still unclear. Here, we underwent a competing risk analysis to discover the potential risks for 28-day in-hospital mortality for ICU critically ill patients with COVID-19.
In the study, we defined patients who automatically discharged prior to the day 28 as a competing event since it precluded the occurrence of the event of interest (ie, 28-day mortality in hospital). In practice, the discharged group have a certain risk of death for the severity of illnesses and giving-up of treatment, but the possibility to survive for the improvement of the disease. If this property was simply ignored, the incidence of mortality might be inevitably biased. Therefore, it is better to perform the competing risk model than conventional Cox model since the competing risks model has taken the discharged group into account and calculated their subdistribution risk probabilities, which undoubtedly make our results more accurate.21 Here, Fine-Gray model was chosen to define independent risk factors of ICU COVID-19 patients prognosis and to predict the cumulative incidence of mortality, aiming to contribute to clinical practice.
Materials and Methods
Study Design and Patients
We retrospectively assessed routine epidemiologic, clinical, and laboratory data at first admission to ICU of COVID-19 critically ill patients and reviewed the 28-day survival outcome in the First Affiliated Hospital of Nanjing Medical University between December 2022 to January 2023. Real-Time Polymerase Chain Reaction (RT-PCR) assays and CT scans were used to confirm SARS-CoV-2 infection. The following were the inclusion criteria: (1) Adults above the age of 18, (2) ICU admission. Cases with significant data gaps were excluded. Finally, we included 173 patients in our study. The main goal of the study was to identify the risk factors that influence in-hospital mortality after ICU admission at 28 days. The study was carried out in accordance with the principles outlined in the Declaration of Helsinki and were approved by the Ethics Committee of the First Affiliated Hospital of Nanjing Medical University, Nanjing, China (2023-SR-516). Informed consents of enrolled patients were obtained.
Data Collection
We reviewed all the electronic medical records to collect demographic data, medical history, epidemiological exposure, comorbidities, as well as the first laboratory results from the hospital management software at ICU admission. All data were saved in electronic form and examined retrospectively.
Outcome
The primary outcome of this study is the survival time, defined as the duration from the date of admission to ICU until the date of death. At the date of data extraction, patients remained hospitalized were considered as right censored, whereas those discharged alive from the hospital were thought to be the competing events to death.
Statistical Analysis
Quantitative variables were presented as mean ± standard deviation and compared using independent samples ANOVA test for normally distributed variables. For skewed distributions, the data are presented as the median (interquartile range) and compared using Kruskal-wallis nonparametric test. Categorical variables were described as counts and percentages and compared using the chi-square test as appropriate. Restricted cubic splines (RCS) were used to reveal non-linear associations between some variables and in-hospital mortality, and to determine optimal cut-off values. CIF was applied to present the risk of in-hospital mortality following ICU admission. For each potential predictor, we also plotted Nelson-Aalen curves. In order to discover independent predictors, we used the Fine-Gray proportional subdistribution hazard approach after incorporating the potential predictors. For each predictor, the subdistribution hazard ratios (sdHRs) and 95% confidence intervals (95% CIs) were calculated.22 The AUC of the ROC was used to assess prediction performance.23 The calibration curve plots the fit of the average prediction estimates to the actual observations.24 Finally, we compared the Fine-gray model with the Cox model to predict the cumulative incidence of in hospital mortality in ICU. The statistical significance level was set at P ≤ 0.05. R software (version 4.3.0) was used to analyze all of the data.
Results
Univariate Analysis of in-Hospital Mortality Based on Competing Risk Regression Model
A total of 173 ICU patients with confirmed SARS-CoV-2 infection were included in this study. In conclusion, 66 (38.2%) patients survived, 55 (31.8%) died, and 52 (30.0%) discharged alive from the hospital. Their baseline characteristics are presented in Table 1.
 |
Table 1 Demographics, Blood Parameters, Comorbidities and Outcomes of 173 Patients with ICU COVID-19 Patients |
The variable Systolic Blood Pressure (SBP), Lymphocyte ratio, Basophil ratio, Neutrophil ratio, Alkaline phosphatase (ALP), Urea, Na and K did not have a linear relationship with 28-day mortality outcomes, we used RCS to determine their non-linear association with 28-day mortality in hospital and to find optimal cut-off values (Figure 1). For those variables that are normally distributed, we use the mean truncation, whereas for those skewed distributions, we use the median truncation. The cut-off values of all variables were shown in Supplementary Table 1. We presented the estimates of the hazard ratio (HR) of in-hospital mortality of different clinical characteristics in Figure 2. In the univariate analysis, ICU patients with older Age (sdHR = 3.40, P < 0.001), increased Respiratory rate (RR) (sdHR = 2.07, P = 0.013), Neutrophil-to-lymphocyte ratio (NLR) (sdHR = 1.93, P = 0.017), Neutrophil to albumin ratio (NAR) (sdHR = 2.36, P = 0.002), Neutrophil ratio (NE%) (sdHR = 2.87 P = 0.005), DBIL (sdHR = 1.73, P = 0.044), coexisting Renal Disease (sdHR = 2.22, P = 0.003) and Coagulation Disease (sdHR = 2.95, P < 0.001) had higher cumulative incidence of in-hospital mortality in ICU COVID-19 patients. Besides, decreased Lymphocyte ratio (LY%) (sdHR = 0.55, P = 0.028), Basophil ratio (BA%) (sdHR = 0.53, P = 0.021), Albumin (ALB) (sdHR = 0.52, P = 0.017) and Anion gap (A.G) (sdHR = 0.51, P = 0.016) were related to significantly higher cumulative incidence of in-hospital mortality. The related Nelson-Aalen curves for the prospective predictors were shown in Figure 3.
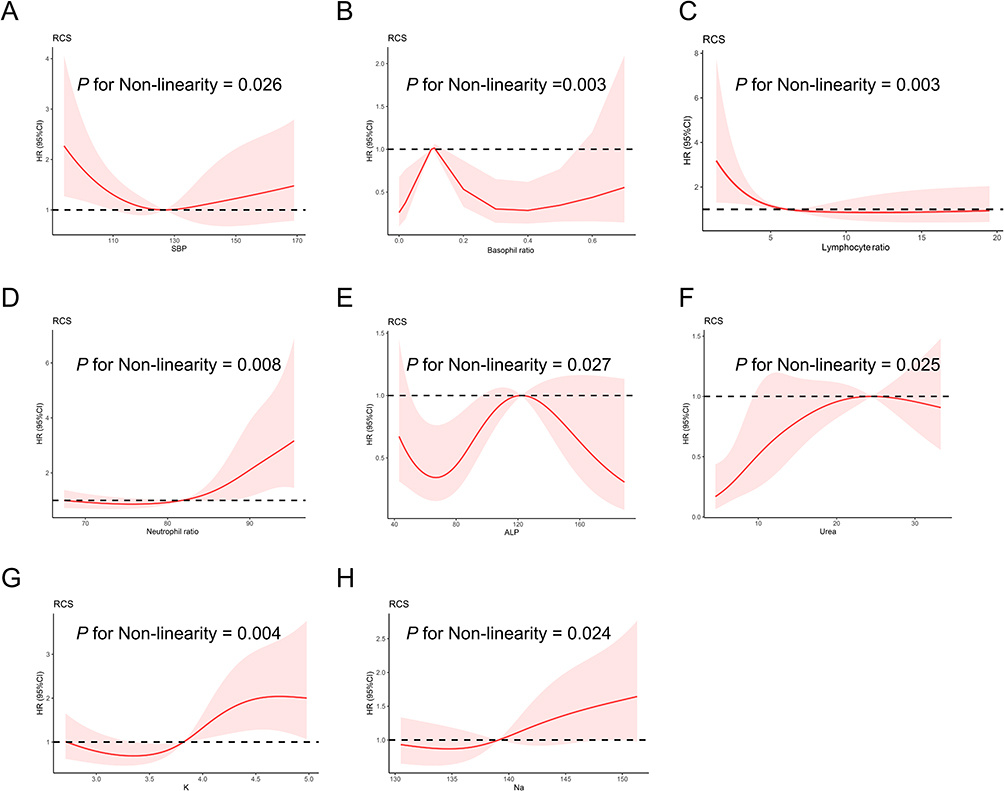 |
Figure 1 Restricted cubic spline (RCS) of no-liner association between some variables and in-hospital mortality. Association of some variables with in-hospital mortality. (A) SBP, (B) Basophil ratio, (C) Lymphocyte ratio, (D) Neutrophil ratio, (E) ALP, (F) Urea, (G) K, (H) Na. Abbreviation: SBP Systolic blood pressure; ALP Alkaline Phosphatase. |
 |
Figure 2 Univariate and multivariate analysis of in-hospital mortality. Abbreviations: RR, Respiratory rate; NLR, Neutrophil-to-lymphocyte ratio; NAR, Neutrophil to albumin ratio; LY%, Lymphocyte ratio; NE%, Neutrophil ratio; BA%, Basophil ratio; DBIL, Direct bilirubin; ALB, Albumin; A.G, Anion gap. |
 |
Figure 3 Cumulative incidence function curves of death for ICU COVID-19 patients grouped by different characteristics. Cumulative incidence function curves of death by different characteristics. (A) Age, (B) Respiratory rate, (C) NLR, (D) NAR, (E) Lymphocyte ratio, (F) Neutrophil ratio, (G) Basophil ratio, (H) DBIL, (I) ALB, (J) A.G, (K) Renal Disease, (L) Coagulation Disease. Abbreviations: NLR, Neutrophil-to-lymphocyte ratio; NAR, Neutrophil to albumin ratio; DBIL, Direct bilirubin; ALB, Albumin; A.G, Anion gap. |
Multivariate Analysis for in-Hospital Mortality Post-ICU Admission in COVID-19 Patients
Possible predictors (Age, RR, NLR, NAR, LY%, NE%, BA%, DBIL, ALB, A.G, Renal Disease, and Coagulation Disease) identified in the univariate analysis (P ≤ 0.05) were included in the Fine-Gray proportional subdistribution hazard approach. According to the result of multivariable analysis (Figure 2), the following four factors are independent predictors of in-hospital mortality (P < 0.05): Age, NE%, DBIL, and Renal Disease. The risk of in-hospital mortality was higher in older patients (sdHR = 3.27, P < 0.001). The cumulative incidence of in-hospital mortality was higher in patients with increased DBIL (sdHR = 2.07, P = 0.011), increased NE% (sdHR = 2.59, P = 0.033) and the presence of Renal Disease (sdHR = 1.89, P = 0.025).
ROC Curves, Calibration Curves and C-Index of the Multivariate Prediction Model for 28-Day in-Hospital Mortality
The ROC curve of the multivariate prediction model to predict 28-day hospital mortality was shown in Figure 4 and AUC is 0.790 (95% CI = 0.720–0.860; Cut-off value = 0.297; sensitivity = 80.0%; specificity = 69.0%), showing better prediction performance (Table 2).
 |
Table 2 Comparison of ROC Curves of Multivariate Model with Other Univariate Variables |
 |
Figure 4 ROC curve of the multivariate prediction model for 28-day prediction. Abbreviations: ROC, Receiver operating characteristic; AUC, Area under the curve. |
The calibration curves of prediction model were displayed in Figure 5. The calibration curves were well fitted, showing high consistencies between the predicted and observed mortality probability. The 28-day C-indexe for the multivariate prediction model predicting the 28-day mortality in hospital was 0.750, which indicated the good discrimination ability of the multivariate prediction model.
 |
Figure 5 Calibration curves of the multivariate prediction model for 28-day prediction. |
Comparison Between Fine-Gray Model and Cox Model
Finally, we predicted the cumulative mortality of patients with higher Age, DBIL, NE% and in presence of Renal Disease by Fine-gray model and Cox model respectively. As previously mentioned, in the presence of competing events, if the traditional Cox model was still used, it would overestimate mortality and bias the results (Figure 6).
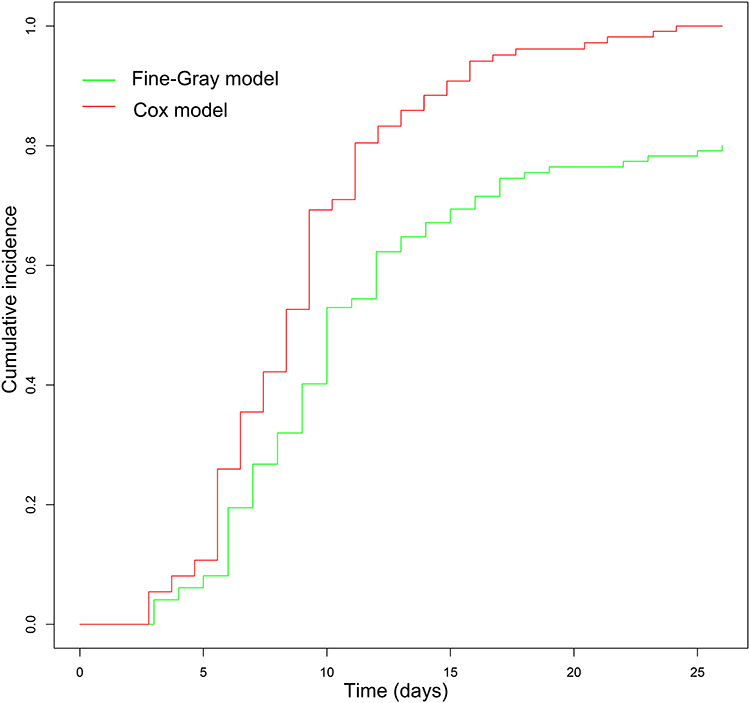 |
Figure 6 The cumulative mortality of patients with higher age, direct bilirubin, neutrophil ratio and in presence of renal disease by fine-gray model and Cox model. |
Discussion
In our study, we retrospectively analyzed 173 critically ill COVID-19 patients receiving treatment in ICU. To determine the predictors of the 28-day in-hospital mortality, a competing risk analysis was conducted. Finally, we identified that Age, Neutrophil ratio, DBIL and Renal Disease were four independent risk factors of in-hospital mortality post-ICU admission for COVID-19 patients and develop a risk model of 28-day in-hospital mortality by the Fine-Gray proportional subdistribution hazard approach. The model showed a favorable accuracy and accordance in predicting the mortality with a favorable AUC (0.790) and a high C-index (0.750).
Age is one of the most important risk factors for COVID-19, and it has been confirmed by overwhelming evidence worldwide.2,25,26 A meta-analysis by Andrew, et al27 showed an exponential relationship between age and COVID-19 infection fatality rate (IFR). Age-specific IFRs were very low in children and younger adults, but gradually increased to 1.4% at age 65, 4.6% at age 75, and up to 15% at age 85.27 Infected individuals with older age tended to have more comorbidities and low resistance to pathogenic infections.28 Besides, aging tended to cause an increase in baseline inflammation, the immune system of older adults might be in a chronic pro-inflammatory state which could contribute to infection-induced tissue damage.25,29
Our study discovered that Neutrophil ratio was independent risk factor for in-hospital mortality of ICU COVID-19 patients. Excessive inflammatory responses tend to stimulate neutrophil production.30 Researchers believe that in susceptible individuals, neutrophils produce excessive amounts of Reactive Oxygen Species (ROS), exacerbating the host’s immunopathologic response and leading to more severe disease. ROS impair the function of lung cells and red blood cell, which may be the main cause of hypoxic respiratory failure in critically ill patients with COVID.31 Despite the many studies30,32,33 identifying the value of NLR for prognostic prediction of COVID-19, we did not find it. We may need to expand our sample size to validate it.
DBIL level is a significant biomarker for monitoring liver injury.34 SARS-CoV-2 can also bind to receptor ACE2 on the bile ducts, leading to cholangiocyte injury and the increase of DBIL level. A retrospective study in the United States showed that patients with abnormal DBIL were at higher risk of ICU admission and death.35 Ding, et al36 showed that DBIL levels in deceased COVID-19 patients were significantly higher than that in discharged patients. This evidence suggests that DBIL is a noteworthy predictor of COVID-19 related mortality.
Patients with Renal complications had a higher mortality rate. A meta-analysis demonstrates that chronic kidney disease is associated with severe COVID-19 infection.37 A large prospective cohort study with COVID-19 admitted to 250 hospitals in the UK found that patients with latent CKD have a 66% increased likelihood of developing AKI.38 In fact, SARS-CoV-2 can affect the kidneys both directly and indirectly.39,40 The virus can enter renal cells by binding to membrane-bound ACE2 receptors on the apical membranes of glomerular podocytes and proximal tubular cells, destroy renal epithelial cells and disrupt the balance of the renin-angiotensin system.41,42 Besides, SARS-CoV-2 indirectly causes renal damage through cytokine storms and activation of coagulation pathways, and leads to sepsis, hemodynamic instability, and hypoxemia.6
The novelty of our study is that we performed survival analysis using a competing risk model. It could fully take competing risk events into consideration and make the outcomes more objective. Moreover, the variables incorporated in our model are readily available in clinical practice. Nevertheless, this study has several limitations. First, the number of patients was insufficient which limited the statistical power of this explorative study. Second, we did not have access to more complete and comprehensive data on inflammatory cytokines such as CRP, IL-6, etc. Third, COVID-19 is an evolving phenomenon, showing a downward trend in overall mortality. Our mortality prediction models for a specific time period and population need to be validated externally to ensure their continuous availability. Fourth, the immune status and treatment-related data were not access, which might cause an elevated NLR and confound the results.
Conclusion
We presented the results of a multivariable prediction model for mortality of ICU COVID-19 patients. Ultimately, we identified that Age, Neutrophil ratio, Direct Bilirubin and Renal Disease at admission to ICU were independently associated with in-hospital mortality for ICU COVID-19 patients and develop a risk model of 28-day in-hospital mortality with high levels of accuracy and robustness.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the corresponding authors, without undue reservation.
Funding
This work was supported by the National Natural Science Foundation of China (82102489), Young Scholars Fostering Fund of the First Affiliated Hospital of Nanjing Medical University (PY2022032), Special Fund project of Laboratory Medicine Research of Jiangsu Medical Association (SYH-3201160-0056).
Disclosure
Ting Wang and Haoyu Ruan are co-corresponding authors. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Rahmandad H, Lim TY, Sterman J. Behavioral dynamics of COVID-19: estimating underreporting, multiple waves, and adherence fatigue across 92 nations. Syst Dyn Rev. 2021;37(1):5–31. doi:10.1002/sdr.1673
2. Kuo CL, Pilling LC, Atkins JC, et al. COVID-19 severity is predicted by earlier evidence of accelerated aging. medRxiv. 2020;2:3.
3. Abbasi-Oshaghi E, Mirzaei F, Farahani F, Khodadadi I, Tayebinia H. Diagnosis and treatment of coronavirus disease 2019 (COVID-19): laboratory, PCR, and chest CT imaging findings. Int J Surg. 2020;79:143–153. doi:10.1016/j.ijsu.2020.05.018
4. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in china: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
5. Grigonis AM, Mathews KS, Benka-Coker WO, Dawson AM, Hammerman SI. Long-term acute care hospitals extend ICU capacity for COVID-19 response and recovery. Chest. 2021;159(5):1894–1901. doi:10.1016/j.chest.2020.12.001
6. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
7. Wang Z, Wu P, Wang L, et al. Marginal effects of public health measures and COVID-19 disease burden in China: a large-scale modelling study. PLoS Comput Biol. 2023;19(9):e1011492. doi:10.1371/journal.pcbi.1011492
8. Kwok KO, Huang Y, Tsoi MTF, et al. Epidemiology, clinical spectrum, viral kinetics and impact of COVID-19 in the Asia-Pacific region. Respirology. 2021;26(4):322–333. doi:10.1111/resp.14026
9. Kim L, Garg S, O’Halloran A, et al. Risk factors for intensive care unit admission and in-hospital mortality among hospitalized adults identified through the US coronavirus disease 2019 (COVID-19)-Associated Hospitalization Surveillance Network (COVID-NET). Clin Infect Dis. 2021;72(9):e206–e214. doi:10.1093/cid/ciaa1012
10. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
11. Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020;18(4):844–847. doi:10.1111/jth.14768
12. Barbaro RP, MacLaren G, Boonstra PS, et al. Extracorporeal membrane oxygenation support in COVID-19: an international cohort study of the extracorporeal life support organization registry. Lancet. 2020;396(10257):1071–1078. doi:10.1016/S0140-6736(20)32008-0
13. Chen T, Wu D, Chen H, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ. 2020;368:m1091. doi:10.1136/bmj.m1091
14. Khalid A, Ali Jaffar M, Khan T, et al. Hematological and biochemical parameters as diagnostic and prognostic markers in SARS-COV-2 infected patients of Pakistan: a retrospective comparative analysis. Hematology. 2021;26(1):529–542. doi:10.1080/16078454.2021.1950898
15. Wu C, Chen X, Cai Y, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 Pneumonia in Wuhan, China. JAMA Intern Med. 2020;180(7):934–943. doi:10.1001/jamainternmed.2020.0994
16. Shang Y, Liu T, Wei Y, et al. Scoring systems for predicting mortality for severe patients with COVID-19. EClinicalMedicine. 2020;24:100426. doi:10.1016/j.eclinm.2020.100426
17. Knight SR, Ho A, Pius R, et al. Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: development and validation of the 4C Mortality Score. BMJ. 2020;370:m3339.
18. Cheng J, Sollee J, Hsieh C, et al. COVID-19 mortality prediction in the intensive care unit with deep learning based on longitudinal chest X-rays and clinical data. Eur Radiol. 2022;32(7):4446–4456. doi:10.1007/s00330-022-08588-8
19. Tahavvori A, Mosaddeghi-Heris R, Ghanbari Sevari F, et al. Combined systemic inflammatory indexes as reflectors of outcome in patients with COVID‑19 infection admitted to ICU. Inflammopharmacology. 2023;31(5):2337–2348. doi:10.1007/s10787-023-01308-8
20. de Gonzalo-Calvo D, Molinero M, Benítez ID, et al. A blood microRNA classifier for the prediction of ICU mortality in COVID-19 patients: a multicenter validation study. Respir Res. 2023;24(1):159. doi:10.1186/s12931-023-02462-x
21. Angriman F, Ferreyro BL, Harhay MO, Wunsch H, Rosella LC, Scales DC. Accounting for competing events when evaluating long-term outcomes in survivors of critical illness. Am J Respir Crit Care Med. 2023;208(11):1158–1165. doi:10.1164/rccm.202305-0790CP
22. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Statis Assoc. 1999;94(446):496–509. doi:10.1080/01621459.1999.10474144
23. Obuchowski NA, Bullen JA. Receiver operating characteristic (ROC) curves: review of methods with applications in diagnostic medicine. Phys Med Biol. 2018;63(7):07TR01. doi:10.1088/1361-6560/aab4b1
24. Brien WF, Crawford L, Raby A, Richardson H. In-house calibration of the international sensitivity index or calibration curve for determination of the international normalized ratio. Arch Pathol Lab Med. 2004;128(3):308–312. doi:10.5858/2004-128-308-ICOTIS
25. Chen Y, Klein SL, Garibaldi BT, et al. Aging in COVID-19: vulnerability, immunity and intervention. Ageing Res Rev. 2021;65:101205. doi:10.1016/j.arr.2020.101205
26. Zhu N, Zhang D, Wang W, et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa2001017
27. Levin AT, Hanage WP, Owusu-Boaitey N, Cochran KB, Walsh SP, Meyerowitz-Katz G. Assessing the age specificity of infection fatality rates for COVID-19: systematic review, meta-analysis, and public policy implications. Eur J Epidemiol. 2020;35(12):1123–1138. doi:10.1007/s10654-020-00698-1
28. Shaw AC, Joshi S, Greenwood H, Panda A, Lord JM. Aging of the innate immune system. Curr Opin Immunol. 2010;22(4):507–513. doi:10.1016/j.coi.2010.05.003
29. Gao YD, Ding M, Dong X, et al. Risk factors for severe and critically ill COVID-19 patients: a review. Allergy. 2021;76(2):428–455. doi:10.1111/all.14657
30. Liu Y, Du X, Chen J, et al. Neutrophil-to-lymphocyte ratio as an independent risk factor for mortality in hospitalized patients with COVID-19. J Infect. 2020;81(1):e6–e12. doi:10.1016/j.jinf.2020.04.002
31. Laforge M, Elbim C, Frère C, et al. Tissue damage from neutrophil-induced oxidative stress in COVID-19. Nat Rev Immunol. 2020;20(9):515–516. doi:10.1038/s41577-020-0407-1
32. Cai J, Li H, Zhang C, et al. The neutrophil-to-lymphocyte ratio determines clinical efficacy of corticosteroid therapy in patients with COVID-19. Cell Metab. 2021;33(2):258–269.e253. doi:10.1016/j.cmet.2021.01.002
33. Bedel C, Korkut M. Neutrophil-to-lymphocyte ratio and covid-19. Shock. 2021;56(5):874. doi:10.1097/SHK.0000000000001712
34. Yadav DK, Singh A, Zhang Q, et al. Involvement of liver in COVID-19: systematic review and meta-analysis. Gut. 2021;70(4):807–809. doi:10.1136/gutjnl-2020-322072
35. Bender JM, Worman HJ. Coronavirus disease 2019 and liver injury: a retrospective analysis of hospitalized patients in New York City. J Clin Transl Hepatol. 2021;9(4):551–558. doi:10.14218/JCTH.2020.00171
36. Ding ZY, Li GX, Chen L, et al. Association of liver abnormalities with in-hospital mortality in patients with COVID-19. J Hepatol. 2021;74(6):1295–1302. doi:10.1016/j.jhep.2020.12.012
37. Henry BM, Lippi G. Chronic kidney disease is associated with severe coronavirus disease 2019 (COVID-19) infection. Int Urol Nephrol. 2020;52(6):1193–1194. doi:10.1007/s11255-020-02451-9
38. Sullivan MK, Lees JS, Drake TM, et al. Acute kidney injury in patients hospitalized with COVID-19 from the ISARIC WHO CCP-UK Study: a prospective, multicentre cohort study. Nephrol Dial Transplant. 2022;37(2):271–284. doi:10.1093/ndt/gfab303
39. Chu KH, Tsang WK, Tang CS, et al. Acute renal impairment in coronavirus-associated severe acute respiratory syndrome. Kidney Int. 2005;67(2):698–705. doi:10.1111/j.1523-1755.2005.67130.x
40. Soleimani M. Acute kidney injury in SARS-CoV-2 infection: direct effect of virus on kidney proximal tubule cells. Int J Mol Sci. 2020;21(9):3275. doi:10.3390/ijms21093275
41. Donnelly CA, Ghani AC, Leung GM, et al. Epidemiological determinants of spread of causal agent of severe acute respiratory syndrome in Hong Kong. Lancet. 2003;361(9371):1761–1766. doi:10.1016/S0140-6736(03)13410-1
42. Thomas G. Renin-angiotensin system inhibitors in COVID-19. Cleve Clin J Med. 2020. doi:10.3949/ccjm.87a.ccc009
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.