")
Back to Journals » International Journal of Women's Health » Volume 16
A Qualitative Study on the Experience of Assisted Reproductive Technology in Women with Dyspareunia
Authors Wei Q, Wang Z, He Y , Hong X, Shen X, Zhang S
Received 23 November 2023
Accepted for publication 20 March 2024
Published 26 March 2024 Volume 2024:16 Pages 543—553
DOI https://doi.org/10.2147/IJWH.S449830
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Qun Wei, Zilian Wang, Yu He, Xia Hong, Xuling Shen, Songying Zhang
Reproductive Medicine Center, Sir Run Run Shaw Hospital, College of Medicine, Zhejiang University, Hangzhou City, Zhejiang Province, People’s Republic of China
Correspondence: Songying Zhang, Email [email protected]
Objective: This study aims to investigate the phenomenon of sexual intercourse-related fear among women utilizing assisted reproductive technology due to dyspareunia. The primary objective is to offer insights that can inform the development of targeted nursing interventions.
Methods: Employing a purposive sampling approach, a cohort of 23 female patients experiencing dyspareunia and undergoing treatment at the Reproductive Medicine Center of Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, between July 2022 and December 2022, were selected as participants for this research. Semi-structured, in-depth interviews were conducted to gather qualitative data. The Colaizzi 7-step analysis method was subsequently applied to scrutinize the interview transcripts and identify emergent themes.
Results: The analysis yielded five prominent themes: psychological disturbances, incongruent cognitive perceptions, anticipations regarding conception, insufficient adaptive responses, and sexual expectations.
Conclusion: It is imperative for medical practitioners to demonstrate reverence for patients’ sexual beliefs and conditions, attune to their apprehensions, and offer efficacious emotional support. Tailored and multifaceted sexual health knowledge should be dispensed based on patients’ individual requirements and their envisioned sexual experiences, thereby fostering spousal and familial harmony. By prioritizing patients’ sexual well-being, cultivating a compassionate medical milieu, and augmenting the quality of assisted reproductive services, comprehensive improvements can be achieved.
Keywords: dyspareunia, female, assisted reproductive technology, qualitative research
Introduction
Female dyspareunia constitutes a noteworthy concern within the realm of sexual health. This condition is characterized by sexual pain or vaginal discomfort, leading to impaired genital interaction and, at times, rendering sexual intercourse unfeasible.1 The reported global prevalence of dyspareunia among women spans from 3% to 20%.2,3 The etiological landscape of female dyspareunia encompasses both physiological and psychological factors. The former encompass vulvovaginal candidiasis, pelvic inflammatory diseases, and chronic pelvic pain,4 amenable to interventions like medication, hormone therapy, and electrotherapy.5,6 Conversely, psychological factors encompass negative attitudes toward sex, adverse emotions, strained marital relationships, heightened stress, and impaired spousal communication.7 In instances where dyspareunia arises from psychological origins, women must either adapt independently or seek professional intervention, as failure to do so may engender suboptimal sexual encounters and deleteriously impact overall quality of life. Alarmingly, dyspareunia can compromise women’s fertility and marital harmony, potentially precipitating anxiety and depression.8
A burgeoning body of research underscores the far-reaching ramifications of dyspareunia, encompassing not solely sexual challenges, but also detrimental effects on mental well-being and even marital stability.9,10 Within the Chinese context, prevailing traditional norms can lead afflicted women to overlook the treatability of their condition, with certain individuals harboring reluctance to seek assistance.11 A cultural adage resonates: “There are three unfilial acts, of which having no descendants is the gravest”. To meet spousal expectations or fulfill maternal roles, many women afflicted with dyspareunia may forgo seeking treatment, opting instead to engage with reproductive medicine centers in pursuit of successful conception.12
Assisted reproductive technology (ART) encompass methods such as artificial insemination and in vitro fertilization-embryo transfer, intervening at the gametic, zygotic, and embryonic levels to achieve pregnancy.13,14 As a result of multiple drug use (including injections), surgery, and unknown treatment outcomes, women receiving assisted reproductive therapy are reported to be at greater risk for stress, anxiety, and depression.15 However, women with dyspareunia face additional problems. This process necessitates multiple vaginal procedures, including B-ultrasound probe insertions for follicular monitoring, vaginal speculum placements for lavage, gauze packing, and embryo transfer. Women contending with dyspareunia often manifest apprehension, resistance, or outright aversion toward these interventions. Concurrently, the sheer patient volume within reproductive clinics or the brevity of reproductive-related procedures impede succinct communication of the unique needs of dyspareunia patients. Consequently, the diagnostic and therapeutic aspects of ART procedures are compromised, leading some patients to discontinue or forsake assisted reproductive therapy.16 Even when adhering to ART, patients frequently exhibit heightened nervousness during treatment, hampering their ability to cooperate during examinations or surgeries, especially when involving vaginal speculum utilization.17
While prior inquiries have extensively explored the prevailing landscape and influencing factors of female dyspareunia, comparatively scant attention has been devoted to the psychological journey of patients seeking assisted reproductive therapy.18 When women with dyspareunia embark on their quest for conception within reproductive centers, a pivotal query arises concerning the manner in which healthcare practitioners should offer tailored guidance. The present study delves into the experiences of dyspareunia-affected women pursuing ART, with the aim of delineating the support mechanisms sought by patients during treatment. Outcomes of this investigation may furnish medical professionals with empirical insights into assisting women grappling with dyspareunia as they engage with both sexual health and ART. Ultimately, this research has the potential to enrich knowledge, enhance pregnancy prospects, and foster closer spousal relationships for women contending with dyspareunia.
Aim
The primary objective of this investigation was to scrutinize the experiences of female patients afflicted by dyspareunia as they engaged in assisted reproductive therapy. The overarching aim was to facilitate the resolution of fertility challenges among these patients, fostering a healthful perspective on sexuality and accurate sexual knowledge.
Method
Design
This study adopted phenomenological research, which is a kind of qualitative research and is widely used in the fields of humanities and social sciences such as medicine, psychology, nursing, education, etc.19 In the field of nursing, phenomenological research methods are mainly used to explore subjective cognitive aspects or life experiences related to health and illness, such as values and worldviews.20 Phenomenological research can be divided into two categories: descriptive phenomenology and interpretative phenomenology.21 The essence of descriptive phenomenology is to advocate the direct grasp of things and to pursue the understanding of things without any inherent knowledge and prejudice. Interpretative phenomenology, on the other hand, emphasizes the “situational” nature of human reality, that is, each individual’s experience is influenced by the world in which they live. The participants in this study were all undergoing assisted reproductive therapy and were affected by the environment, so the interpretive phenomenology was used.
Participants
The study adopted an objective sampling methodology to select female patients undergoing assisted reproduction and assisted pregnancy treatments for dyspareunia at the reproductive center of our hospital during the period spanning July to December 2022.
Inclusion/Exclusion Criteria
The inclusion criteria encompassed the following: i) Meeting established diagnostic criteria for female sexual dysfunction, specifically diagnosed with dyspareunia by a qualified medical practitioner; ii) Manifesting a desire to partake in assisted reproductive therapy; iii) Expressing willingness to actively engage in this study and collaborate with subsequent follow-up assessments.
Conversely, exclusion criteria were defined as follows: i) Dyspareunia stemming solely from anatomical aberrations of the female vulva or genital tract; ii) Rejection of or withdrawal from the interview process; iii) A documented history of mental disorders; iv) Recent exposure to significant mental trauma or other distressing events.
This study complies with the Declaration of Helsinki. The ethical dimensions of this research were thoroughly reviewed and sanctioned by the Ethics Committee of Sir Run Run Shaw Hospital of Zhejiang University School of Medicine (Approved number: 2023460). Participants were comprehensively apprised that their voluntary withdrawal from the study at any juncture would exert no bearing on their entitlements. Ultimately, a total of 23 patients, who willingly provided informed consent included publication of anonymized responses and exhibited readiness to partake in the study, were included. A summative overview of their information can be found in Table 1.
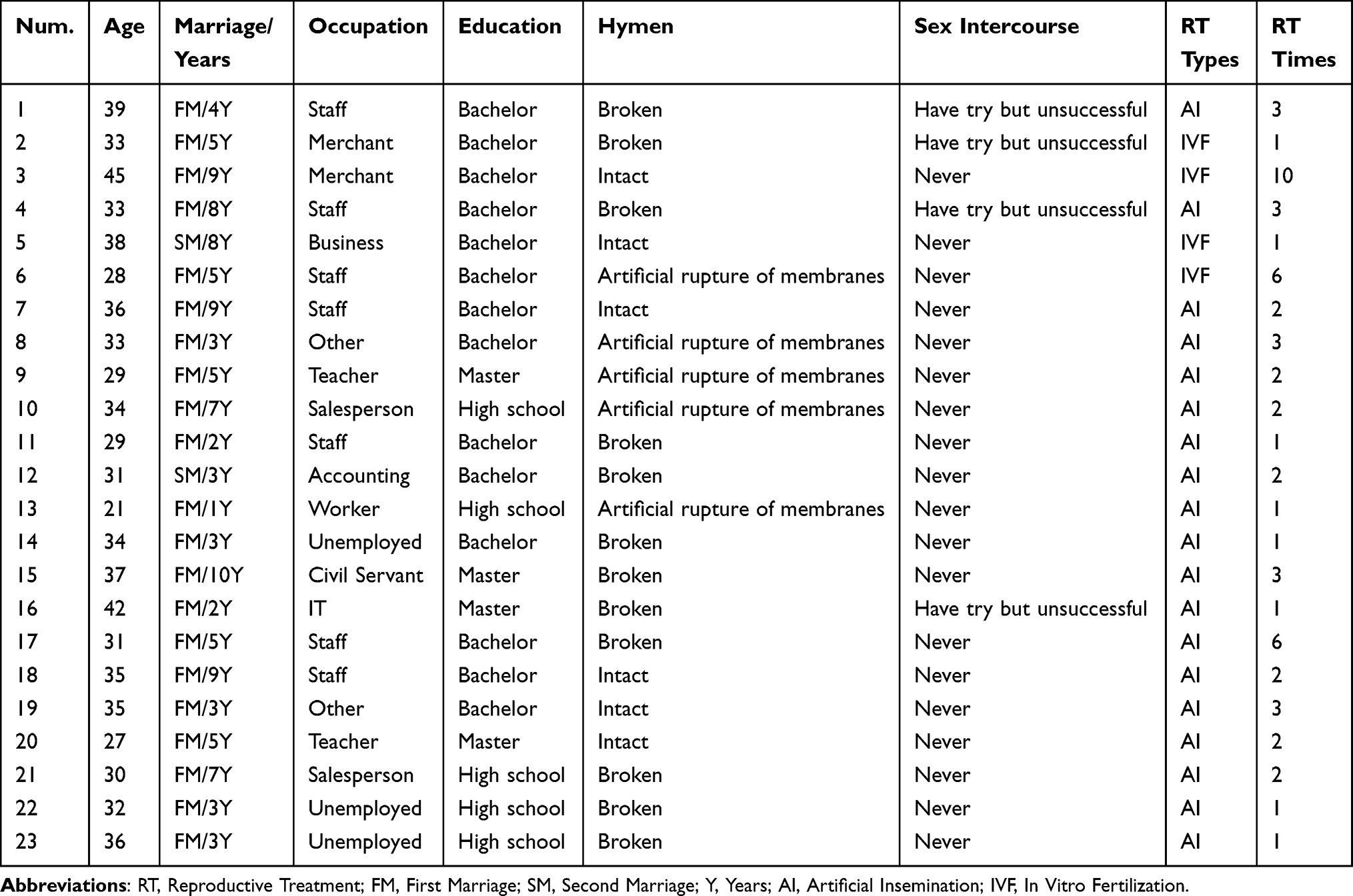 |
Table 1 Characteristics of the Study Participants (N = 23) |
Qualitative Interview Design
Aligned with the research objectives, an interview framework was meticulously developed. This framework underwent successive iterations informed by a synthesis of pertinent literature, insights from reproductive clinical specialists, and input from psychological experts within our institutional milieu. Following preliminary interviews with two patients, refinements were implemented through meticulous deliberation within the research team. The interview protocol encompassed the subsequent inquiries: a. How do you think about the sex life between couples? b. What are your feelings and thoughts when you have sex with your husband and wife? c. How does sexual incompatibility affect your relationship? d. What are your expectations or recommendations for assisted reproductive technology? e. What kind of help do you want the medical staff to provide you?
Procedure
Employing a phenomenological approach inherent to qualitative research, two researchers with proficient training and extensive interview acumen conducted face-to-face, semi-structured interviews. These dialogues transpired within an ambient and secluded clinical setting, conducive to fostering a sense of comfort and openness. The scheduling of interviews occurred subsequent to either the initial or secondary visit to the assisted reproduction clinic. Prior to commencement, participants were presented with the choice of being interviewed jointly with their spouse. Among the participants, two assented to such joint interviews, while one participant was accompanied by her mother, and twenty participants opted for solo interviews. A comprehensive briefing was administered to patients and their accompanying parties, elucidating the study’s objectives, methodologies, confidentiality protocols, and the imperative of audio recording. Notably, two participants declined audio recording, opting solely for note-taking, with the ensuing interview proceeding in accordance with the designated framework.
The interviews were meticulously conducted while attending to the nuances of participants’ expressions, vocal inflections, and non-verbal gestures. To ensure a focused and amenable dialogue, the interviews adhered to a temporal threshold of 30 to 45 minutes.
Data Analysis
The seven steps from the book (Existential-Phenomenological Alternatives for Psychology) are followed by the analysis of the data.22 Subsequent to the interviews, the patients’ responses were cross-verified with them to ensure accuracy and fidelity. Within 24 hours of confirmation, the recorded data was transcribed into textual format and cataloged within the Nvivo software for subsequent analysis. The analytical procedure unfolded as follows: a. Familiarization: both researchers meticulously reviewed the interview transcripts, identifying statements germane to the research inquiry. b. Identifying significant statements: these pertinent statements were subsequently distilled, consolidated, and refined to distill meaningful topics. c. Formulating meanings: recurring topics are encoded. d. Clustering themes: the encoded topics are assembled by virtue of common concepts. e. Developing an exhaustive description: each topic was described in detail. f. Producing the fundamental structure: compare similar topics and their descriptions over and over again to identify and extract similar points of view; then build a theme. g. Seeking verification of the fundamental structure: the themes were returned to the participants for validation to ensure the accuracy of the results. If there is a bias, the researcher must reanalyze it step by step from the first step.
Results
Participants
In this investigation, a total of twenty-three participants were subjected to the interview process. Their ages ranged from 21 to 45 years, with two participants currently engaged in second marriages. Notably, six participants exhibited intact hymens at the time of reproductive treatment (Refer to Table 1).
Thematic Analysis
Psychological Disturbances
Resistance to Sexual Intercourse
Numerous women exhibited a propensity to perceive sexual intercourse as an onerous chore, thus evoking aversion. Some couples grappled with limited sexual knowledge and skills, resulting in profound discomfort and pain during intercourse, consequently precipitating resistance (Refer to Table 2).
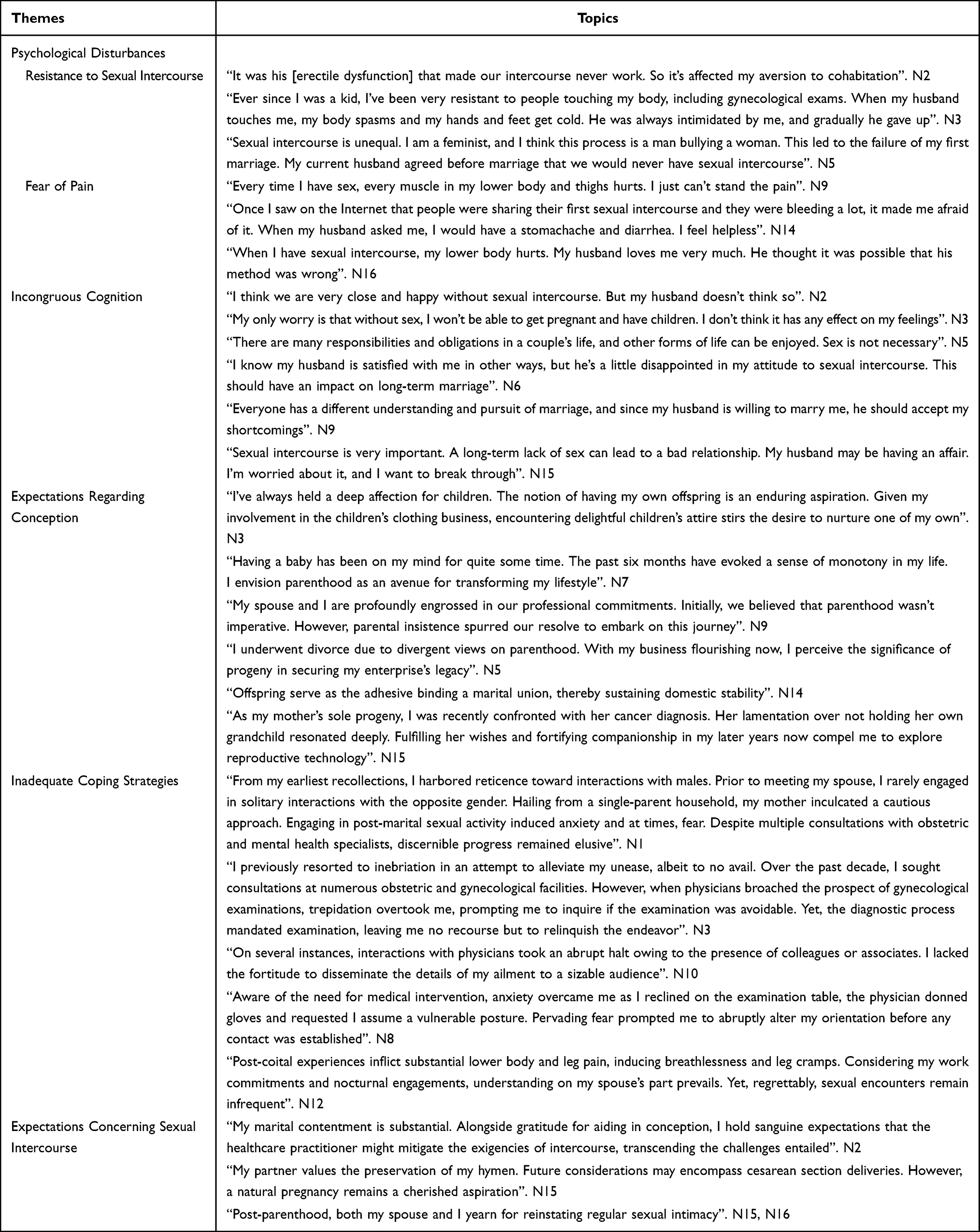 |
Table 2 Results of the Interview (N = 23) |
Participant N2 shared,
It was his [erectile dysfunction] that made our intercourse never work, so it’s affected my aversion to cohabitation.
Participant N3 expounded,
Ever since I was a kid, I’ve been very resistant to people touching my body, including gynecological exams. When my husband touches me, my body spasms and my hands and feet get cold. He was always intimidated by me, and gradually he gave up.
Participant N5, adopting a feminist perspective, noted,
Sexual intercourse is unequal. I am a feminist, and I think this process is a man bullying a woman. This led to the failure of my first marriage. My current husband agreed before marriage that we would never have sexual intercourse.
Fear of Pain
Apprehension regarding pain, specifically lower body discomfort, emerged as a pivotal obstacle to sexual intercourse. Notably, participants reported physiological reactions such as perineal pain, inner thigh discomfort, bodily cramps, cold perspiration, and panic during sexual engagement.
Participant N9 articulated,
Every time I have sex, every muscle in my lower body and thighs hurts. I just can’t stand the pain.
Participant N14 disclosed,
Once I saw on the Internet that people were sharing their first sexual intercourse and they were bleeding a lot, it made me afraid of it. When my husband asked me, I would have a stomachache and diarrhea. I feel helpless.
Participant N16 explicated,
When I have sexual intercourse, my lower body hurts. My husband loves me very much. He thought it was possible that his method was wrong.
Incongruous Cognition
Divergent perspectives regarding sexual intercourse surfaced due to disparate familial roles and dynamics, leading to incongruous perceptions and discordance between partners.
Participant N2 reflected,
I think we are very close and happy without sexual intercourse. But my husband doesn’t think so.
Participant N3 expounded,
My only worry is that without sex, I won’t be able to get pregnant and have children. I don’t think it has any effect on my feelings.
Participant N5 remarked,
There are many responsibilities and obligations in a couple’s life, and other forms of life can be enjoyed. Sex is not necessary.
Participant N6 revealed,
I know my husband is satisfied with me in other ways, but he’s a little disappointed in my attitude to sexual intercourse. This should have an impact on long-term marriage.
Participant N9 postulated,
Everyone has a different understanding and pursuit of marriage, and since my husband is willing to marry me, he should accept my shortcomings.
Participant N15 asserted
Sexual intercourse is very important. A long-term lack of sex can lead to a bad relationship. My husband may be having an affair. I’m worried about it, and I want to break through.
Expectations Regarding Conception
Inquiries regarding fertility expectations during the interviews unveiled a diverse array of motivations underlying patients’ pursuit of assisted reproductive treatment, arising from distinct family dynamics and personal experiences.
Participant N3 expressed,
I’ve always held a deep affection for children. The notion of having my own offspring is an enduring aspiration. Given my involvement in the children’s clothing business, encountering delightful children’s attire stirs the desire to nurture one of my own.
Participant N7 disclosed,
Having a baby has been on my mind for quite some time. The past six months have evoked a sense of monotony in my life. I envision parenthood as an avenue for transforming my lifestyle.
Participant N9 elucidated,
My spouse and I are profoundly engrossed in our professional commitments. Initially, we believed that parenthood wasn’t imperative. However, parental insistence spurred our resolve to embark on this journey.
Participant N5’s narrative revolved around a pivotal shift,
I underwent divorce due to divergent views on parenthood. With my business flourishing now, I perceive the significance of progeny in securing my enterprise’s legacy.
Participant N14 accentuated the role of children as a familial cohesive force, stating,
Offspring serve as the adhesive binding a marital union, thereby sustaining domestic stability.
Participant N15 revealed,
As my mother’s sole progeny, I was recently confronted with her cancer diagnosis. Her lamentation over not holding her own grandchild resonated deeply. Fulfilling her wishes and fortifying companionship in my later years now compel me to explore reproductive technology.
Inadequate Coping Strategies
Participants adopted varied coping mechanisms to grapple with sexual intercourse-related challenges. While some participants acknowledged that they would not have pursued professional intervention if not for fertility concerns, others went to hospital to address their sexual predicament, only to discontinue due to discomfort or anxiety associated with gynecological examinations.
Participant N1 reflected,
From my earliest recollections, I harbored reticence toward interactions with males. Prior to meeting my spouse, I rarely engaged in solitary interactions with the opposite gender. Hailing from a single-parent household, my mother inculcated a cautious approach. Engaging in post-marital sexual activity induced anxiety and at times, fear. Despite multiple consultations with obstetric and mental health specialists, discernible progress remained elusive.
Participant N3 recounted,
I previously resorted to inebriation in an attempt to alleviate my unease, albeit to no avail. Over the past decade, I sought consultations at numerous obstetric and gynecological facilities. However, when physicians broached the prospect of gynecological examinations, trepidation overtook me, prompting me to inquire if the examination was avoidable. Yet, the diagnostic process mandated examination, leaving me no recourse but to relinquish the endeavor.
Participant N10 elucidated,
On several instances, interactions with physicians took an abrupt halt owing to the presence of colleagues or associates. I lacked the fortitude to disseminate the details of my ailment to a sizable audience.
Participant N8 narrated,
Aware of the need for medical intervention, anxiety overcame me as I reclined on the examination table, the physician donned gloves and requested I assume a vulnerable posture. Pervading fear prompted me to abruptly alter my orientation before any contact was established.
Participant N12’s narrative underscored the profundity of her discomfort,
The post-coital experience inflict substantial lower body and leg pain, inducing breathlessness and leg cramps. Considering my work commitments and nocturnal engagements, understanding on my spouse’s part prevails. Yet, regrettably, sexual encounters remain infrequent.
Expectations Concerning Sexual Intercourse
Anticipations regarding post-Assisted Reproductive Technology (ART) sexual experiences surfaced among participants.
Participant N2 conveyed,
My marital contentment is substantial. Alongside gratitude for aiding in conception, I hold sanguine expectations that the healthcare practitioner might mitigate the exigencies of intercourse, transcending the challenges entailed.
Participant N5 delineated personal sentiments,
My partner values the preservation of my hymen. Future considerations may encompass cesarean section deliveries. However, a natural pregnancy remains a cherished aspiration.
Consonant viewpoints emerged among participants N15 and N16, as they voiced,
After becoming parents, both my spouse and I yearn for reinstating regular sexual intimacy.
Discussion
Fulfillment of Fertility Aspirations Through Assisted Reproductive Technology
For women grappling with dyspareunia, the pursuit of parenthood necessitates recourse to Assisted Reproductive Technology (ART) to facilitate conception. Notably, routine gynecological examinations, leucorrhea tests, and follicular interventions, though pivotal in ART, engender profound psychological duress, eliciting feelings of panic and apprehension. Our study’s findings underscore that women with dyspareunia harbor dual expectations—pertaining to both pregnancy and the transformative prospect of sexual intercourse. In the realm of assisted reproduction, healthcare practitioners specializing in this domain are urged to provide holistic care, catering not only to facilitating successful pregnancies but also ameliorating the challenges surrounding sexual engagement.
Sociocultural Influences and Diverse Attitudes Toward Intercourse
The dynamic interplay of socio-economic advancements and cultural evolution, compounded by influences such as religion and personal beliefs, engenders stark divergences in societal attitudes toward sexual intercourse.23 Our investigation accentuates the spectrum of attitudes evident among participants. Upon initial hospital visits, some individuals were entirely abstinent from sexual activity, while others had encountered persistently unsuccessful endeavors. Noteworthy is the presence of cases where couples actively sought alternatives to conventional conception methods, opting for artificial procedures over sexual intercourse to conceive. In this intricate landscape, the impetus for healthcare practitioners lies in respecting patients’ desires and values. A nuanced approach must be adopted, acknowledging diverse marital constructs and medical requisites. For patients favoring asexual-assisted conception, our approach entails strategic collaboration between nurses and physicians, involving processes like abdominal ultrasound monitoring and hormone tests to tailor interventions in consonance with patients’ preferences.24
Cultural Influences on Psychological Well-Being
In Chinese culture, traditional norms exert considerable influence over the perception of psychological states, potentially constraining open dialogue regarding sexual disorders.25 This propensity for silence prevails even when confronted with sexual physiological or psychological discrepancies. Our findings align with this cultural backdrop, with a substantial subset of participants grappling with tension, fear, and rejection when subjected to perineal exposure, gynecological examinations, and speculum utilization. These psychophysiological reactions manifest as direct impediments to the execution of various assisted reproductive methodologies. Empathetic nursing becomes paramount, entailing profound comprehension of patients’ emotional realms. Selection of nurses possessing adept expression and rapport-building capabilities is vital. The establishment of serene, private environments, coupled with compassionate communication, engenders trust and harmonious nurse-patient relationships. Moreover, tailored interventions, such as assigning gentle female practitioners for specific procedures, lend an empathetic touch.
Humanized Nursing Strategies
The effective execution of humanized nursing interventions aims to enhance the efficiency of successful pregnancy and actualize future conjugal intimacy aspirations. Attuned to patients’ intercourse-related challenges, our strategy entails a multi-tiered approach. (1) soothe patients’ emotions and relieve their psychological pressure. Private consultation rooms were provided in the process of treatment and examination, creating a relaxed and friendly atmosphere, patiently asking if they had any discomfort, and allowing their spouse or mother to accompany them during diagnosis and treatment. Patients are advised to play their favorite music or watch videos on their mobile phones during examination or treatment. Carry small objects that they feel safe, throw pillows and other distractions. (2) Carry out operation inspection step by step to relieve pain and pressure. The patient was informed of the steps of gynecological examination and the time required for the operation, and cooperated with the doctor to fully lubricated the examination gloves with lubricating oil. Instructing patients to cross their hands in front of their chest, take chest breathing, and relax the buttock and abdominal muscles can effectively reduce discomfort. A warm gynecological hole was selected to cover the perineum, and the vaginal dilator was gently placed into the vagina. According to the patient’s adaptation, the vagina was gradually expanded to reduce spasm. (3) The use of local lubricants and anesthetics can help to relieve and reduce perineal pain. Eight patients in this study required the use of anesthetics in the vulva during each examination and artificial insemination. According to the patient’s requirements, 10mL lidocaine gel was given to the vulva before the operation, and the intrauterine insemination operation was successfully completed. The patients reported that their pain was relieved, which played a role in local pain relief and psychological suggestion.
Promoting Sexual Education and Communication
Engendering correct sexual attitudes and knowledge through judicious sexual education is vital. Differing attitudes toward and perceptions of sexual intercourse can perpetuate discord and anxieties. Facilitating transparent communication between couples to understand each other’s sexual knowledge, attitudes, and needs can bridge these gaps. Effective communication hinges on encouraging candid expressions of emotions, fostering emotional support, and enhancing the spousal relationship. Furthermore, the provision of educational resources containing pertinent sexual knowledge is indispensable in dispelling misapprehensions and alleviating sexual apprehensions.
Comprehensive Care in Assisted Reproduction
The paramountcy of humanized nursing interventions transcends the realm of mere physiological interventions, encompassing the broader gamut of patients’ psychological and emotional needs. As assisted reproductive technologies advance, healthcare practitioners must expand their purview beyond diagnostic and therapeutic regimens to encompass comprehensive care. Medical practitioners should be sensitive to patientsand#039; psychological sexual needs, provide effective psychological and counseling interventions, and take multidisciplinary approach actions when necessary to promote optimal care outcomes. Such meticulous attention, rooted in empathy and understanding, can substantively augment pregnancy rates and marital satisfaction, engendering contented and harmonious familial units.
Limitations
Firstly, despite we made efforts to recruit participants, this particular group had not received attention before, so we were able to find very few people in the limited time available. Doctors and nurses at the center have already been cultivated to understand this group. In the future, we will implement appropriate treatment and response once a patient with dyspareunia at the first outpatient visit.
Secondly, the aim of this study was to explore the psychological experience of assisted reproductive technology in women with dyspareunia. However, there are still many women with dyspareunia in China who are afraid to seek medical treatment because of their ideological constraints. Now that we are starting to focus on this group, follow-up studies will try to find more women with dyspareunia to help them.
Lastly, the study was conducted at a single center for Reproductive Medicine in China, and most of the patients were from surrounding areas. The results may vary by region. In future studies, patients from different regions should be recruited.
Conclusion
Diverse perceptions of conventional sexual interactions within couples and distinct coping strategies exist among women with dyspareunia. Furthermore, patients exhibited apprehension, fear, and reluctance towards routine gynecological assessments and assisted reproductive procedures. It became evident that patients anticipated a tailored approach to assisted reproductive interventions, attuned to their distinctive requisites. Consequently, an imperative to heighten healthcare professionals’ recognition of the paramount significance of patients’ sexual well-being emerged. A patient-centric perspective mandates the reverence of patients’ sexual psychology and concepts. Effective transmission of accurate sexual perspectives and insights assumes significance, thereby facilitating the implementation of humanized assisted reproductive approaches.
Acknowledgments
We are grateful for all the participants.
Author Contributions
All authors had made significant contributions to the work reported, either in conceptualization, research design, execution, data acquisition, analysis, and interpretation, or in all of these areas; participate in drafting, revising, or critically reviewing articles; approved the version to be released; and agree to be responsible for all aspects of the work. Consensus has been reached on the journal for article submission.
Funding
This study is funded by Medical and Health Technology Project of Zhejiang Province (Grant No. 2024KY112).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gross E, Brubaker L. Dyspareunia in women. JAMA. 2022;327(18):1817–1818. doi:10.1001/jama.2022.4853
2. Hill DA, Taylor CA. Dyspareunia in Women. Am Fam Physician. 2021;103(10):597–604.
3. Tayyeb M, Gupta V. Dyspareunia. In: StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC; 2023.
4. Moscicki P, Bachmann GA. Characterization of female sexual dysfunction associated with spinal pathology and surgery. Sexual Med Rev. 2022;10(4):493–498. doi:10.1016/j.sxmr.2022.01.003
5. Fernández-Pérez P, Leirós-Rodríguez R, Marqués-Sánchez MP, Martínez-Fernández MC, de Carvalho FO, Maciel LYS. Effectiveness of physical therapy interventions in women with dyspareunia: a systematic review and meta-analysis. BMC Womens Health. 2023;23(1):387. doi:10.1186/s12905-023-02532-8
6. Nappi RE, Tiranini L, Martini E, Bosoni D, Righi A, Cucinella L. Medical treatment of female sexual dysfunction. Urol Clin North Am. 2022;49(2):299–307. doi:10.1016/j.ucl.2022.02.001
7. Ertem DH, Ayan Saatçioğlu Ş, Bingol A, et al. Factors influencing sexual functions in Turkish female patients with migraine. Agri J Turkish Soc Algol. 2020;32(4):193–201.
8. Boerner KE, Rosen NO. Acceptance of vulvovaginal pain in women with provoked vestibulodynia and their partners: associations with pain, psychological, and sexual adjustment. J Sex Med. 2015;12(6):1450–1462. doi:10.1111/jsm.12889
9. Moyneur E, Dea K, Derogatis LR, Vekeman F, Dury AY, Labrie F. Prevalence of depression and anxiety in women newly diagnosed with vulvovaginal atrophy and dyspareunia. Menopause. 2020;27(2):134–142. doi:10.1097/GME.0000000000001450
10. Burri A, Hilpert P, Williams F. Pain catastrophizing, fear of pain, and depression and their association with female sexual pain. J Sex Med. 2020;17(2):279–288. doi:10.1016/j.jsxm.2019.10.017
11. Stones RW, Padmadas SS, Guo S, Brown JJ, Zhao F, Li B. Dyspareunia, urinary sensory symptoms, and incontinence among young Chinese women. Arch Sex Behav. 2006;35(5):561–567. doi:10.1007/s10508-006-9070-2
12. Zhang N, Sun S, Zheng Y, et al. Reproductive and postsurgical outcomes of infertile women with deep infiltrating endometriosis. BMC Womens Health. 2022;22(1):83. doi:10.1186/s12905-022-01666-5
13. Guan H, Tang H, Pan L, Song H, Tang L. Pregnancy predictors in unexplained infertility after intrauterine insemination. J Gynecol Obstetr Hum Reprod. 2021;50(8):102071. doi:10.1016/j.jogoh.2021.102071
14. Wu H, Zhou P, Lin X, Wang S, Zhang S. Endometrial preparation for frozen-thawed embryo transfer cycles: a systematic review and network meta-analysis. J Assist Reprod Genet. 2021;38(8):1913–1926. doi:10.1007/s10815-021-02125-0
15. Purewal S, Chapman SCE, van den Akker OBA. Depression and state anxiety scores during assisted reproductive treatment are associated with outcome: a meta-analysis. Reprod Biomed Online. 2018;36(6):646–657. doi:10.1016/j.rbmo.2018.03.010
16. Clayton AH, Harsh V. Sexual function across aging. Curr Psychiatry Rep. 2016;18(3):28. doi:10.1007/s11920-016-0661-x
17. Qiao J, Feng HL. Assisted reproductive technology in China: compliance and non-compliance. Transl Pediatr. 2014;3(2):91–97. doi:10.3978/j.issn.2224-4336.2014.01.06
18. Thomas HN, Neal-Perry GS, Hess R. Female Sexual Function at Midlife and Beyond. Obstet Gynecol Clin North Am. 2018;45(4):709–722. doi:10.1016/j.ogc.2018.07.013
19. Rietmeijer CBT, Veen M. Phenomenological research in health professions education: tunneling from both ends. Teach Learn Med. 2022;34(1):113–121. doi:10.1080/10401334.2021.1971989
20. Deliktas A, Korukcu O, Aydin R, Kabukcuoglu K. Nursing students’ perceptions of nursing metaparadigms: a phenomenological study. J Nurs Res. 2019;27(5):e45. doi:10.1097/jnr.0000000000000311
21. Lopez KA, Willis DG. Descriptive versus interpretive phenomenology: their contributions to nursing knowledge. Qual Health Res. 2004;14(5):726–735. doi:10.1177/1049732304263638
22. Colaizzi P. Psychological research as the phenomenologist views it. In: Valle RS, King M, editors. Existential Phenomenological Alternatives for Psycholog. New York: Oxford University Press; 1978.
23. Weitzman A, Mallory AB. Racial, socioeconomic, and attitudinal disparities in trajectories of young women’s willingness to refuse unwanted sex. J Adolesc Health. 2019;64(6):746–752. doi:10.1016/j.jadohealth.2018.12.002
24. Kaseki H, Kaseki S, Shimizu M, Hayashi A, Suganuma N. Indication of intravaginal insemination for infertility treatment in couples with sexual dysfunction. Reprod Med Biol. 2021;20(2):241–245. doi:10.1002/rmb2.12376
25. Yan E, Wu AM, Ho P, Pearson V. Older Chinese men and women’s experiences and understanding of sexuality. Culture Health Sexual. 2011;13(9):983–999. doi:10.1080/13691058.2011.605471
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.