")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 15
A Case Report of a Maxillary Second Molar with Two Distinct Palatal Canals, Confirmed by CBCT
Authors Al-Qudah A , Afaneh A, Hassouneh L
Received 20 July 2023
Accepted for publication 21 September 2023
Published 26 September 2023 Volume 2023:15 Pages 199—203
DOI https://doi.org/10.2147/CCIDE.S431563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Aladdin Al-Qudah, Asem Afaneh, Layla Hassouneh
Department of Conservative Dentistry, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Aladdin Al-Qudah, Department of Conservative Dentistry, Jordan University of Science and Technology, P.O. Box 3030, Irbid, 22110, Jordan, Email [email protected]
Abstract: Cases of unusual and complex root canal morphology could be difficult to diagnose and treat. This report describes the diagnosis and management of a rare maxillary right second molar (tooth #17) with two distinct palatal canals. The tooth was diagnosed with irreversible pulpitis and symptomatic apical periodontitis. Non-surgical root canal treatment was performed. Accurate diagnosis and comprehensive treatment of cases with unusual root canal morphology can be achieved by evaluation of periapical radiographs at different angulations, advanced magnification techniques, and the Cone Beam Computed Tomography (CBCT) scanning. Clinicians should be aware that two separate palatal canals could exist in maxillary second molar teeth.
Keywords: two palatal canals, root canal morphology, maxillary molar, cone beam computed tomography
Introduction
A comprehensive knowledge and consideration of the different variations in the root canal morphology of human dentition is essential for the clinical success of root canal treatment.1 Such variations and complexities in root canal anatomy have been thoroughly investigated in the literature, and their significance is strongly emphasized.1–3 However, rare anatomical variations can be challenging due to its uncommon appearance and insufficient knowledge of the dental operator.
One of the most important factors contributing to failure of root canal treatment is incomplete instrumentation or obturation of missed root canals.4 Maxillary molars present one of the most complicated root canal anatomies.1,2 The presence of three roots with three individual canals (mesio-buccal, disto-buccal, and palatal) is the most common appearance in maxillary second molars (MSMs), followed by the presence of three roots with four canals. The fourth canal is often found in the mesiobuccal root and is commonly referred to a second mesio-buccal (MB) canal.2,5,6 Some unusual root and canal morphology of MSMs has been reported in the dental literature. Ashraf et al reported MSM with only two roots (distal and mesial roots) with two canals in each root.7 Ozcan and coworkers showed the presence of 3 canals in the MB root.8 Five roots with 5 canals have also been reported.9 Other authors reported the presence of two palatal roots.10 Marco A. Versiani et al, 2023 reported the presence of a palato-mesiobuccal canal in an extracted 3-rooted MSM, scanned using micro-computed tomography.11 Versiani et al, 2012 investigated 4 –rooted MSMs selected from a pool of extracted teeth, using micro-computed tomography.12 They found that all roots presented one canal except MB root which presented 2 canals in 24% of cases. Zeng et al, 2016 reported a MSM with 4 roots (1 palatal, 1 MB and 2 DB) and 5 canals (2MB, 2 DB and 1 palatal).13 Nosrat et al, 2017 presented a series of 5 maxillary molars (4 first molars and 1 second molar) with bifurcated palatal canals (type 1–2 canal configuration).14
Earlier root canal classification systems did not report cases of two palatal canals in the maxillary molars.1,15 Few studies and case reports reported a rare appearance of two palatal canals/roots (bifurcated canals) in maxillary molars showing a low incidence of 0.73–2%.5,16,17
Cone beam computed tomography (CBCT) is a modern and effective method that is being widely used in dentistry.2 In contrary to traditional radiography, CBCT can provide 3-dimensional (3D) illustration of teeth, which can aid in analyzing the internal and external tooth anatomy and provide a more precise imaging of the root and canal system.18 It is a non-invasive technique and produces images with a higher resolution compared to conventional radiographs.18
Although maxillary molars have been reported to be associated with several morphological variations, the appearance of two palatal canals is considered a rare phenomenon.16,17 In this report, we describe a maxillary right second molar requiring root canal treatment, with a rare morphological occurrence of two separate palatal canals in a single palatal root (Vertucci type IV canal configuration).1 Previous studies reported bifurcated canals, double roots or variations in MB and DB roots.13,14 The present case illustrates a clinical case with CBCT images, whereas previous studies conducted radiographic evaluation or extracted teeth analysis.12,17
Clinical Report
A 23-yr-old female, who is medically fit, was referred by the dental emergency clinic for endodontic treatment of the right MSM. The patient attended the emergency clinic at Jordan University of Science & Technology (JUST) after developing spontaneous pain in the right maxillary posterior quadrant. The pain was described to last for few hours and occur more frequently at night. A thorough clinical and radiographic examination was conducted, by a dentist in the emergency dental department, to determine the source of pain.
Clinical examination revealed that tooth was grossly destructed, tender to percussion, and elicited an intense, lingering pain on cold test. Other teeth in the right quadrants showed normal response to percussion and cold test. There was no history of trauma to the head region and no occlusal factors that could affect her symptoms. Periodontal probing of the sulcus of the right MSM resulted in normal depths of 2 to 3 mm. A periapical radiograph of the tooth showed widening of the apical lamina dura associated with the palatal root. However, no anatomical variations were noticed or reported by the referrer dentist (Figure 1a).
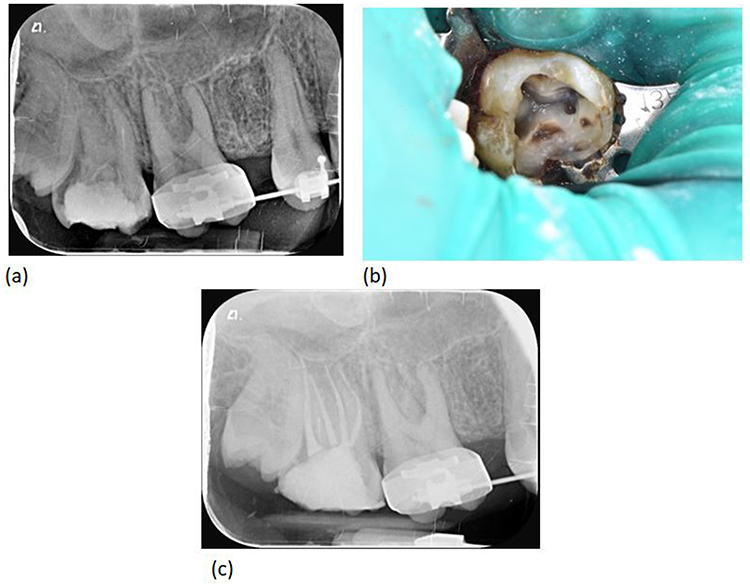 |
Figure 1 Clinical and radio-graphical presentation of tooth #17. (a) Pre-operative periapical radiograph showing widening of the apical lamina dura associated with the palatal root for tooth #17. (b) Access cavity of tooth #17 under rubber dam isolation, revealing 2 buccal and 2 palatal canal orifices. (c) Post-operative periapical radiograph revealing complete obturation of all canals (mesio-buccal, disto-buccal, mesio-palatal, and disto-palatal canals). |
The diagnosis of the tooth was irreversible pulpitis with symptomatic apical periodontitis and the patient was given a local anesthetic of 2% lidocaine with 1:100,000 epinephrine. Under rubber dam isolation, caries removal, access cavity preparation and pulpal extirpation were performed to relieve pain and the patient was referred to the endodontic post-graduate clinics at JUST for root canal treatment.
The patient attended the post-graduate dental clinics 1 week after the emergency visit. A thorough clinical and radiographic examination was conducted by an endodontic resident; one of the authors of this manuscript, who also carried out RCT for the tooth. The patient was given a local anesthetic of 2% lidocaine with 1:100,000 epinephrine. Under rubber dam isolation, temporary restoration was removed and access cavity was exposed. Two buccal canals and one palatal canal orifices were initially observed clinically. The palatal canal was found in the floor of pulp chamber at a more mesial location, compared to its usually observed position in other maxillary molars. In addition, the morphology of the pulp chamber dictated further distopalatal extension of the access cavity preparation. Hence, further deroofing of the pulp chamber was carried out under magnification (OPMI PICO; Carl Zeiss, Gottingen, Germany) and a second palatal canal orifice was identified (Figure 1b). The pre-operative periapical radiographic evaluation did not propose this occurrence. The canal was initially negotiated with a manual file #10, and subsequently files were inserted into the canals and working length was obtained using apex locator (Dentaport ZX, J. Morita Co., Tokyo, Japan).
After negotiating the canals with manual files #10–15, all canals were prepared using Protaper Gold rotary files (Dentsply, Sirona) until file F2 and irrigated with 2.5% sodium hypochlorite. Apical preparations of all canals were completed to size 30/0.04 using profile rotary files (Dentsply, Sirona). A master cone radiograph was taken using Gutta Percha points size 30/0.04, and canals were obturated using lateral condensation technique and AH Plus root canal sealer (Dentsply, Sirona). The postoperative radiograph revealed two that tooth # 17 possessed 4 canals with completely separate apical course (Figure 1c). The treatment was completed in a single visit.
A post-operative “limited field-of- view” CBCT scan was taken to confirm and analyze the unusual anatomy of tooth #17 (Figure 2a–c). The potential benefits as well as potential risks were discussed with the patient beforehand, and informed consent was obtained. At one-month follow-up, patient was satisfied with the treatment and showed no signs or symptoms. Institutional approval was not required to publish the case details.
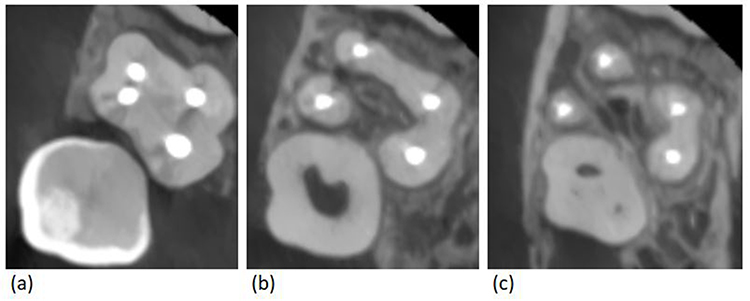 |
Figure 2 Post-operative Cone Beam Computed Tomography scan (axial sections) for tooth #17. (a) Coronal root view showing 4 obturated canals. (b) Mid root view showing separate mesio-buccal canal in addition to disto-buccal, mesio-palatal, and disto-palatal canals. (c) Apical root view showing two separate mesio-buccal and disto-buccal roots, and one bifid palatal root encasing two palatal canals. |
Discussion
The success of root canal treatment in cases with unexpected root canal morphology requires proper diagnosis, careful inspection of clinical radiographs, use of magnification, and most importantly thorough knowledge of the dental anatomy and its various modifications.2,4
Despite the wide range of variations in the reported root and canal morphology of MSM teeth, the presence of two palatal canals is considered a rare occurrence. MSMs most commonly have one palatal root with a single canal. The existence of two palatal canals/roots in MSM’s is rare, but should be considered by dental practitioners, to aid in proper diagnosis and effective treatment of such cases. In the current case, several factors aided in the diagnosis and treatment of a second palatal canal; knowledge, skills and proficiency of the operator, careful inspection of pulp chamber floor under magnification, and evaluation of periapical radiographs at different angulations. The use of CBCT scanning postoperatively confirmed the diagnosis of two separate palatal canals.
A CBCT scan taken before treatment, during treatment or post-treatment is helpful in evaluating complex and unusual root canal anatomies.2,17 Recently, the use of CBCT scanning is recommended as the imaging method of choice for endodontic treatment of cases with unusual or complicated anatomy, as 2-dimensional imaging is not predictable in terms of revealing the actual number of roots and canals.19 In the present case, the two palatal canals were clinically identified after complete de-roofing of the pulp chamber, as they were two separate and distinct canals extending all the way from pulp chamber to root apex (Vertucci type IV). Other canal configurations can be more difficult to identify clinically or by using conventional 2-D radiography. These are the configurations where canal branching occurs in the middle or apical thirds of the canal (Vertucci type III and V). In such cases, the use of CBCT scanning is more predictable in revealing the actual number of canals.
In the current case, CBCT scan was not taken preoperatively or during treatment, as a CBCT machine was not available in the dental facility where treatment was carried out. However, “limited field-of- view (FOV)” CBCT was taken postoperatively to confirm the anatomical findings and exclude other variations or treatment complications. CBCT systems with a limited FOV have a lower radiation dose than several other conventional 3D radiography methods. Such scans reduce the volume of exposed tissue, and therefore, the effective radiation dose. With the limited FOV scans, practitioners are no longer required to radiate the entire face, but they can take a radiograph of the specific anatomic region; the upper right molar area in the present case. Therefore, the ALARA (as low as reasonably achievable) principle was observed in the present report.
The CBCT scan demonstrated that the 4th canal observed in the periapical radiograph was a second palatal canal and not an MB2. The scan also excluded the presence additional canals or other complex canal configurations. Based on the CBCT findings, and according to the new classification system of root canal morphology proposed by Ahmed et al,2 the tooth is described as3 17 MB1 DB1 P2; meaning that the right MSM has three roots (MB: mesiobuccal; DB: distobuccal; P: palatal) in which the palatal root encases two separate canals each with an independent orifice and foramen (Figure 2a–c).
Variations in root canal anatomy must always be taken into consideration before starting treatment. In addition, careful clinical and radiographic examinations are necessary for accurate identification of all root canals. In maxillary second molar teeth, the root canal system typically consists of 3 or 4 canals. The fourth canal is often found in the mesiobuccal root. However, in the present case, a fourth canal was found in the palatal root and extends all the way from pulp chamber to root apex.
Conclusions
The case presented shows that two separate and distinct canals may occur in the palatal root of maxillary second molar teeth.
Abbreviations
MSM, Maxillary Second Molar; RCT, Root Canal Treatment; CBCT, Cone Beam Computed Tomography; MB, Mesio-Buccal; JUST, Jordan University of Science & Technology.
Consent for Publication
The participant/patient gave written informed consent for her personal or clinical details along with any identifying images to be published in this study.
Funding
This study was conducted without external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589–599. doi:10.1016/0030-4220(84)90085-9
2. Ahmed H, Versiani M, De‐Deus G, Dummer P. A new system for classifying root and root canal morphology. Int Endod J. 2017;50(8):761–770. doi:10.1111/iej.12685
3. Fenelon T, Parashos P. Prevalence and morphology of C‐shaped and non‐C‐shaped root canal systems in mandibular second molars. Aust Dent J. 2022;67:S65–S75. doi:10.1111/adj.12925
4. García-Guerrero C, Delgado-Rodríguez CE, Molano-González N, et al. Predicting the outcome of initial non-surgical endodontic procedures by periapical status and quality of root canal filling: a cohort study. Odontology. 2020;108:697–703. doi:10.1007/s10266-020-00494-z
5. Stone LH, Stroner WF. Maxillary molars demonstrating more than one palatal root canal. Oral Surg Oral Med Oral Pathol. 1981;51(6):649–652. doi:10.1016/S0030-4220(81)80017-5
6. Khadilkar I, Nangia D, Chawla A, et al. 3D geometric analysis of second mesiobuccal canal in permanent maxillary first molar tooth. Aust Endod J. 2023;49(1):140–148.
7. Ashraf H, Dianat O, Hajrezai R, Paymanpour P, Azadnia S. Endodontic treatment of a double-rooted maxillary second molar with four canals: a case report. Iran Endod J. 2014;9(4):304.
8. Ozcan E, Aktan AM, Arı H. A case report: unusual anatomy of maxillary second molar with 3 mesiobuccal canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107(1):e43–e6. doi:10.1016/j.tripleo.2008.09.006
9. Kottoor J, Hemamalathi S, Sudha R, Velmurugan N. Maxillary second molar with 5 roots and 5 canals evaluated using cone beam computerized tomography: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109(2):e162–e5. doi:10.1016/j.tripleo.2009.09.032
10. Ulusoy Öİ, Görgül G. Endodontic treatment of a maxillary second molar with 2 palatal roots: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104(4):e95–e7. doi:10.1016/j.tripleo.2007.05.027
11. Versiani MA, Taşdemir T, Keleş A. Identification and characterization of a previously undiscovered anatomical structure in maxillary second molars: the palato-mesiobuccal canal. J Endod. 2023;49:730–734. doi:10.1016/j.joen.2023.03.013
12. Versiani MA, Pécora JD, de Sousa-Neto MD. Root and root canal morphology of four-rooted maxillary second molars: a micro–computed tomography study. J Endod. 2012;38(7):977–982. doi:10.1016/j.joen.2012.03.026
13. Zeng C, Shen Y, Guan X, Wang X, Fan M, Li Y. Rare root canal configuration of bilateral maxillary second molar using cone-beam computed tomographic scanning. J Endod. 2016;42(4):673–677. doi:10.1016/j.joen.2015.12.028
14. Nosrat A, Verma P, Hicks ML, Schneider SC, Behnia A, Azim AA. Variations of palatal canal morphology in maxillary molars: a case series and literature review. J Endod. 2017;43(11):1888–1896. doi:10.1016/j.joen.2017.04.006
15. Al Shalabi R, Omer O, Glennon J, Jennings M, Claffey N. Root canal anatomy of maxillary first and second permanent molars. Int Endod J. 2000;33(5):405–414. doi:10.1046/j.1365-2591.2000.00221.x
16. Shahi S, Yavari HR, Rahimi S, Ahmadi A. Root canal configuration of maxillary first permanent molars in an Iranian population. JODDD. 2007;1(1):1. doi:10.5681/joddd.2007.001
17. Zheng QH, Wang Y, Zhou XD, Wang Q, Zheng GN, Huang DM. A cone-beam computed tomography study of maxillary first permanent molar root and canal morphology in a Chinese population. J Endod. 2010;36(9):1480–1484. doi:10.1016/j.joen.2010.06.018
18. Karobari MI, Noorani TY, Halim MS, Ahmed HMA. Root and canal morphology of the anterior permanent dentition in Malaysian population using two classification systems: a CBCT clinical study. Aust Endod J. 2021;47(2):202–216. doi:10.1111/aej.12454
19. Fayad MI, Nair M, Levin MD, et al. AAE and AAOMR joint position statement: use of cone beam computed tomography in endodontics 2015 update. JOOO. 2015;120(4):508–512.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.