")
Back to Journals » Research and Reports in Urology » Volume 15
What are the Most Important Objectives of Patients Undergoing Radical Prostatectomy? A Narrative Review
Authors Virk A , Treacy PJ, Thanigasalam R, Leslie S
Received 10 October 2023
Accepted for publication 6 December 2023
Published 19 December 2023 Volume 2023:15 Pages 563—569
DOI https://doi.org/10.2147/RRU.S444033
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Guglielmo Mantica
Amandeep Virk,1 Patrick-Julien Treacy,2 Ruban Thanigasalam,1– 3 Scott Leslie1– 3
1Department of Uro-Oncology, Chris O’Brien Lifehouse, Sydney, NSW, Australia; 2The Institute of Academic Surgery at Royal Prince Alfred Hospital, Sydney, NSW, Australia; 3Faculty of Medicine and Health, University of Sydney, Sydney, NSW, Australia
Correspondence: Amandeep Virk, Chris O’Brien Lifehouse, 119-143 Missenden Road, Camperdown, Sydney, NSW, 2050, Australia, Tel +61421233369, Email [email protected]
Purpose: This study aimed to evaluate what objectives are most important to men undergoing radical prostatectomy to allow treating physicians to personalize perioperative counselling and improve patient quality of life outcomes.
Materials and Methods: A predefined search protocol of the Medline and Embase databases was performed from database inception to May 2023. The search was limited to English language and full text. All articles with a specific consideration of patient objectives, preferences or reasons for decision to undergo radical prostatectomy were included for review.
Results: Ten articles out of 375 screened met inclusion criteria for review. All 10 articles utilized a qualitative design and originated across 5 countries across the developed world. A common theme of men placing importance on having their tumor physically removed was found. Methodologies allowing free response beyond predefined categories identified a breadth of considerations including personal circumstance, personal belief and current function in the decision-making process. An investigation on radical prostatectomy performed robotically found some men placed preference on the quicker treatment time with surgery compared to radiation therapy, reflective of shorter recovery times with the robotic approach.
Conclusion: Variability in results across studies highlights the heterogeneity in patient preferences. Directed investigation of patient objectives with an open-ended questioning approach would personalize the perioperative experience and may improve patient satisfaction and quality of life outcomes.
Keywords: prostate cancer, prostatectomy, robotic surgery, objectives, preferences, goals, quality of life
Introduction
Prostate cancer is the most common cancer diagnosed in men in Australia and the second most common cause of cancer-related death after lung cancer.1 The treatment options for localized prostate cancer include radical prostatectomy, radical radiotherapy and deferred treatment by way of active surveillance.2,3 Radical prostatectomy can be performed by open, laparoscopic or robot assisted surgical approaches.
Evidence from the ProtecT trial, reflective across guidelines for the management of prostate cancer, show radical prostatectomy and radical radiotherapy to have the highest reduction in risk of disease progression and metastatic disease development.2,3 Thus, in the appropriately selected patient group, considering comorbidities and life expectancy, they remain the mainstay of treatment.
Evidence has shown the impact of radical prostatectomy and of radical radiation therapy on urinary function, sexual function and bowel function. Radiation therapy has been shown to be associated with more issues with bowel function while the urinary function and sexual function sequelae of radical prostatectomy have been found to have a greater impact on quality of life in comparison.3
Quality of life is therefore an important factor in the shared decision-making process when considering radical treatment such as radical prostatectomy. Robotic radical prostatectomy is becoming increasingly available to patients in the public system in Australia and has the benefit of being less invasive and is associated with quicker recovery times.4
We sought to understand the objectives men who elect to undergo radical prostatectomy have, with emphasis on robotic surgery where data are available. This will allow treating physicians to better elicit men’s objectives and personalize their perioperative counselling and treatment. We hypothesize that this would improve patient quality of life outcomes and satisfaction.
Materials and Methods
A key word search was performed of the Medline and Embase databases making use of MeSH terms where applicable. Search terms were based around the key words “prostatectomy” and “patient objectives” or “preferences” or “goals”. The search was limited to English language and full text. The search was performed with no time specifiers from database inception to the date of search, May 2023.
The articles generated were exported to EndNote 9.3.3 and duplicates were removed. The remaining articles were screened by title and abstract for relevance and inclusion in the review. The screening process for relevance was kept broad to encompass any paper reporting on decision-making to increase capture. In instances of uncertain relevance, the full text was assessed. Where conference abstracts were identified, subsequent full text publication was searched for and included if available. See Figure 1 for a full search schematic.
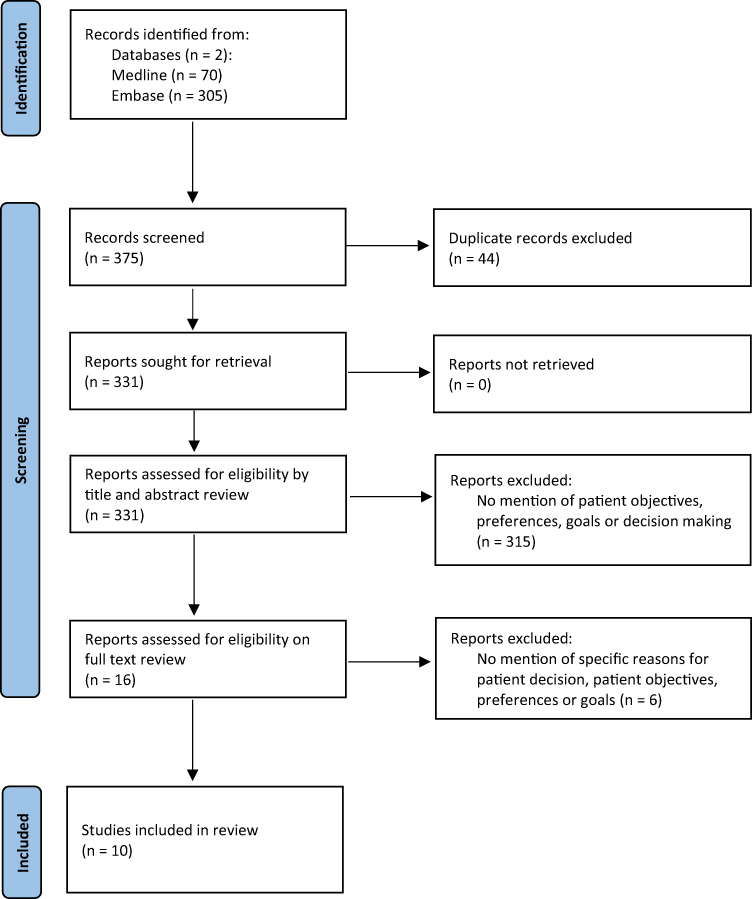 |
Figure 1 Identification of studies for review. Notes: PRISMA figure adapted from Page et al.5 Creative Commons. |
The full text of all included articles was retrieved and appraised. The details of the included articles, type of research and a summary of their relevant findings were tabulated for review in Excel 2023.
Results
The search was performed in May 2023 yielding 375 articles across Medline and Embase combined. After removal of duplicates, 331 articles remained. Title and abstract search identified 16 relevant articles. Two of the articles were conference abstracts and the full text of their subsequent publications were identified and included.
Full text review found 10 articles which included an analysis or consideration of specific reasons for patient decision, preference, objective or goals and included radical prostatectomy as a treatment. Of the 10 articles, all dealt with patient preference or treatment objectives by way of qualitative study design. Investigative methods used were questionnaires, semi-structured interviews, time trade-off scenarios or discrete choice experiments. The articles originated from 5 countries across the developed world (North America, Europe and Australia) between 1996 and 2020. Please see Table 1 for a summary of key findings of the articles reviewed.
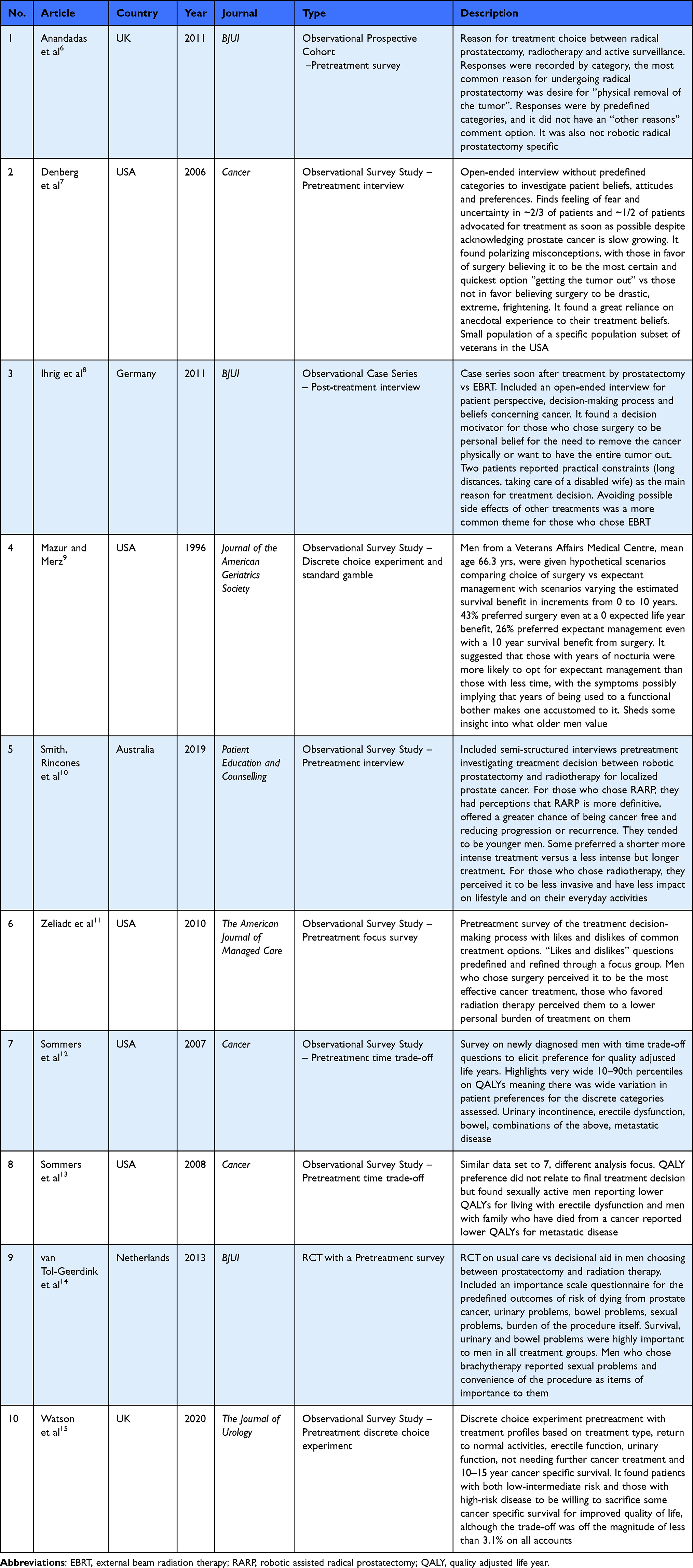 |
Table 1 Summary of Articles Reviewed |
Discussion
Understanding patient objectives and preference for outcomes when undergoing radical prostatectomy is of interest as urologists increasingly focus on quality of life outcomes as a measure of care. In the Australian setting, with the increasing availability of robotic surgery in the public setting, this is of particular significance. This line of inquiry may be best suited to qualitative methodologies to achieve a broad understanding which may be further followed up with quantitative methods. This approach is evident with the results of the review identifying 10 qualitative investigations, sometimes alongside a quantitative analysis of an intervention to improve patient decision-making.
We identified 6 studies utilizing a survey method pretreatment or soon after treatment through questionnaires or interviews (study number 1, 2, 3, 5, 6, 9) (Table 1). Three of these studies used predefined questions or categories with focus on commonly known benefits or side effects of treatment options (study 1, 6, 9) (Table 1). These studies found that men who chose surgery wanted their tumor physically removed and wanted the most effective oncological option. Men favoring brachytherapy placed emphasis on burden of treatment or sexual function. These studies did not differentiate whether surgery was performed by open, laparoscopic or robotic techniques. Impact of the quicker recovery time and associated lower burden of treatment with robotic surgery on patient preference and decision-making could not be assessed in these papers.4
Three studies used semi-structured interview approaches allowing more patient flexibility in answering, beyond discrete categories (study 2, 3, 5) (Table 1). Men in these studies again perceived surgery as the most definitive option and chose surgery with the desire of having their tumor physically removed again. Motivating factors for decision-making amongst an American veteran population in study 2 were anecdotal experience and personal beliefs about surgery.7 Interestingly in these investigations, additional reasons men considered were practical constraints such as distance to treatment or needing to care for a family member. The Australian study particularly looked at robotic prostatectomy vs radiotherapy.10 It found some men wanted the shorter, more intense treatment offered by surgery rather than radiotherapy.10 This reflects the quicker recovery time with robotic surgery compared to open surgery. Men who chose radiotherapy in this study still often cited less impact on everyday lifestyle or daily activities.10 This may be due to the urinary side effects of surgery or the recovery time with surgery. A drawback of more open questions can be less specific answers.
Four studies used time trade-off tools or discrete choice experiments to elicit patient preferences and objectives for treatment (study 4, 7, 8, 10) (Table 1). They had varying results with study 4 finding older men with years of symptoms would choose expectant management, indicating older men become accustomed to their symptoms.9 It contrarily found that some men would prefer surgery even with a zero expected life year benefit, suggesting the strong influence personal belief or preference can have.9 Study 8 found that sexually active men reported lower quality adjusted life years for living with erectile dysfunction and men who have had a family member die of a cancer report lower quality adjusted life years for metastatic disease.13 This highlights the variation in men’s preference based on their personal circumstance and function. Study 7 acknowledged the wide percentiles (10–90th) they found in investigating quality adjusted life years for the categories of urinary incontinence, erectile dysfunction, bowel symptom and metastatic disease. This represents the wide variation prevalent in patient preferences and objectives.12
Of the 10 articles reviewed, all were on populations within the developed world and preferences and reasons for treatment choice may not be reflective of men and their circumstances in developing countries. Difference in health care access, education and cultural beliefs may be variables to consider for broader extrapolation. Additionally, 2 of the studies were amongst the American veteran’s community which again may have particularities in the population group which are less generalizable.7,9
Only one article looked at the treatment choice of robotic prostatectomy in particular. Men who preferred surgery in this study did mention a preference for the shorter more intense treatment modality.10 This is likely reflective of the perceived quicker recovery with surgery in the robotic era.4 This variation calls for updated investigation into men’s treatment preferences with the changing benefit to risk profile of surgery, which is now increasingly performed robotically.
With the existing literature focusing on men’s treatment decision-making and outcome preferences, a direct investigation into men’s specific objectives for surgery would capture men’s personal goals. Studies which asked questions beyond predefined categories found variety in response indicating heterogeneity in men’s personal decision-making factors and this should be further explored.
Direct questioning of objectives (DQO) is a novel approach to assessing quality of life and patient objectives.16–18 This approach was first developed and applied by Detsky et al in 1983 in assessing patient quality of life on home TPN.16 It was later employed by Mcleod et al in 1991 in assessing perceived quality of life of patients with ulcerative colitis pre and post surgery, and again employed by Byrne et al in 2002 in studying the quality of life of patients with neuropathic fecal incontinence.17,18 Detsky et al and Mcleod et al both performed the DQO technique alongside the more commonly performed techniques of time trade-off and category scaling demonstrating concordance in the results of the novel DQO technique with these other techniques which have been shown to be reliable and valid in other applications.16,17
This would be a novel application in the field of urology. It would allow inquiry into men’s self-identified objectives in a directed interview allowing free response.16–18 Category scaling can then be used, as performed in previous applications, to assess men’s self-rated importance of their objectives.16–18 This would elicit men’s objectives beyond the commonly studied categories of urinary, bowel, hormonal and sexual function and would also assess for alignment with these commonly studied domains. This would be a more personalized approach and can also be used to direct preoperative counselling. With iterative application in the postoperative setting, it can also be used to track men’s quality of life postoperatively based on their own objectives. A specific investigation into robotic radical prostatectomy would further be of interest, with the increasing availability of the robotic platform.
Conclusions
Men undergoing radical prostatectomy for localized prostate cancer place a high emphasis on having their tumor physically removed and having the most definitive oncological outcome. Factors men consider in the decision-making process include practical constraints, personal beliefs and circumstance, current urinary and sexual function and anecdotal experience. Age has an impact on choice and the availability of the robotic platform for surgery may also impact choice. The wide variation in results and wide percentiles found in some studies represents the heterogeneity in patient preference and objective. Open and direct investigation of patient objectives will personalize patient counselling and the perioperative experience, and this may improve patient satisfaction and quality of life outcomes.
Data Sharing Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
This investigation was performed following the principles of the Declaration of Helsinki. Ethics Committee approval was not required as the study did not involve human participants or animal care or use.
Funding
The authors declare no funding.
Disclosure
The authors declare no competing interests.
References
1. Australian Institute of Health and Welfare. Cancer data in Australia [Internet]. Canberra: Australian Institute of Health and Welfare; 2022. Available from: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia.
2. EAU Guidelines. Edn. presented at the EAU Annual Congress Milan 2023. ISBN 978-94-92671-19-6; 2023. Available from: http://uroweb.org/guidelines/compilations-of-all-guidelines/.
3. National Institute for Health and Care Excellence (NICE). Prostate cancer: diagnosis and management – intervention comparisons; 2019. Available from: https://www.nice.org.uk/guidance/ng131/evidence/g-active-surveillance-radical-prostatectomy-or-radical-radiotherapy-in-people-with-localised-prostate-cancer-pdf-6779081780.
4. Coughlin GD, Yaxley JW, Chambers SK, et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: 24-month outcomes from a randomised controlled study. Lancet Oncol. 2018;19(8):1051–1060. doi:10.1016/S1470-2045(18)30357-7
5. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372(71). doi:10.1136/bmj.n71
6. Anandadas CN, Clarke NW, Davidson SE, et al. Early prostate cancer--which treatment do men prefer and why? BJU Int. 2011;107(11):1762–1768. doi:10.1111/j.1464-410X.2010.09833.x
7. Denberg TD, Melhado TV, Steiner JF. Patient treatment preferences in localized prostate carcinoma: the influence of emotion, misconception, and anecdote. Cancer. 2006;107(3):620–630. doi:10.1002/cncr.22033
8. Ihrig A, Keller M, Hartmann M, et al. Treatment decision-making in localized prostate cancer: why patients chose either radical prostatectomy or external beam radiation therapy. BJU Int. 2011;108(8):1274–1278. doi:10.1111/j.1464-410X.2011.10082.x
9. Mazur DJ, Merz JF. How older patients’ treatment preferences are influenced by disclosures about therapeutic uncertainty: surgery versus expectant management for localized prostate cancer. J Am Geriatr Soc. 1996;44(8):934–937. doi:10.1111/j.1532-5415.1996.tb01863.x
10. Smith A, Rincones O, Sidhom M, et al. Robot or radiation? A qualitative study of the decision support needs of men with localised prostate cancer choosing between robotic prostatectomy and radiotherapy treatment. Patient Educ Couns. 2019;102(7):1364–1372. doi:10.1016/j.pec.2019.02.017
11. Zeliadt SB, Moinpour CM, Blough DK, et al. Preliminary treatment considerations among men with newly diagnosed prostate cancer. Am J Manag Care. 2010;16(5):e121–e130.
12. Sommers BD, Beard CJ, D’Amico AV, et al. Decision analysis using individual patient preferences to determine optimal treatment for localized prostate cancer. Cancer. 2007;110(10):2210–2217. doi:10.1002/cncr.23028
13. Sommers BD, Beard CJ, D’Amico AV, Kaplan I, Richie JP, Zeckhauser RJ. Predictors of patient preferences and treatment choices for localized prostate cancer. Cancer. 2008;113(8):2058–2067. doi:10.1002/cncr.23807
14. van Tol-Geerdink JJ, Willem Leer J, Weijerman PC, et al. Choice between prostatectomy and radiotherapy when men are eligible for both: a randomized controlled trial of usual care vs decision aid. BJU Int. 2013;111(4):564–573. doi:10.1111/j.1464-410X.2012.11402.x
15. Watson V, McCartan N, Krucien N, et al. Evaluating the trade-offs men with localized prostate cancer make between the risks and benefits of treatments: the COMPARE Study. J Urol. 2020;204(2):273–280. doi:10.1097/JU.0000000000000754
16. Detsky A, McLaughlin J, Abrams H, et al. Quality of life of patients on long-term total parenteral nutrition at home. J Gen Intern Med. 1986;1(1):26–33. doi:10.1007/BF02596321
17. McLeod R, Churchill D, Lock A, Vanderburgh S, Cohen Z. Quality of life of patients with ulcerative colitis preoperatively and postoperatively. Gastroenterology. 1991;101(5):1307–1313. doi:10.1016/0016-5085(91)90081-U
18. Byrne C, Pager C, Rex J, Roberts R, Solomon M. Assessment of quality of life in the treatment of patients with neuropathic fecal incontinence. Dis Colon Rectum. 2002;45(11):1431–1436. doi:10.1007/s10350-004-6444-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.