")
Back to Journals » International Journal of Women's Health » Volume 16
Utilization of Antenatal Care Services Within the Context of COVID-19, Security Challenges, and an Unstable Healthcare System at Primary Health Care Centers
Authors Miskeen E
Received 13 September 2023
Accepted for publication 25 November 2023
Published 25 April 2024 Volume 2024:16 Pages 737—747
DOI https://doi.org/10.2147/IJWH.S435894
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Elhadi Miskeen
Department of Obstetrics and Gynaecology, College of Medicine, University of Bisha, Bisha, Saudi Arabia
Correspondence: Elhadi Miskeen, Head Department of Obstetrics and Gynaecology, College of Medicine, University of Bisha, P.O. Box 1290, Bisha, 61922, Saudi Arabia, Email [email protected]
Background: Utilizing antenatal care (ANC) is vital for maternal and neonatal well-being, especially in low-resource settings with healthcare challenges. Identifying factors impacting antenatal care this context, t of current situation in Sudan is crucial for developing strategies to improve maternal care. This study explores ANC utilization amidst COVID-19, security issues, and healthcare instability in primary health care centers in a resource-constrained environment, aiming to enhance maternal care access and quality.
Methods: This is a mixed-methods study. Quantitative data were collected through a retrospective analysis of ANC attendance records before and during the pandemic. Demographic variables were analyzed for their association with ANC utilization. In-depth interviews were conducted to collect qualitative data from pregnant women and healthcare providers. These interviews focused on capturing the experiences, perceptions, and obstacles associated with antenatal care services during the pandemic and within the healthcare system challenges.
Results: Preliminary quantitative analysis revealed a significant decline in ANC utilization during the pandemic. Fear of COVID-19 infection, disrupted transportation, and resource constraints have emerged as significant barriers to ANC attendance. The qualitative findings highlighted the impact of security challenges on healthcare access and the adaptation strategies employed, including mobile ANC clinics and telehealth consultations.
Conclusion: This study illuminates the intricate landscape of ANC utilization in the face of a pandemic, security instability, and healthcare system vulnerability. Policymakers and stakeholders should collaborate to strengthen healthcare systems and ensure the continued provision of essential maternal health services during challenging times.
Keywords: antenatal care, maternal health, COVID-19, healthcare system, primary health care centers, security challenges, low-resource country, healthcare access
Introduction
Improving maternal health is one of the World Health Organization’s (WHO) Millennium Development Goals (MDGs) and assessing progress toward these goals.1 The WHO recommends four antenatal visits for uncomplicated pregnancies beginning within 12 weeks of gestational age.2 These services enhance the health and overall well-being of pregnant women while also increasing the likelihood of receiving care from qualified birth attendants and facilitating effective communication with healthcare providers.3
Access to adequate and timely antenatal care services is the cornerstone of maternal and child health and is pivotal in reducing maternal and infant mortality rates.4 However, the utilization of such services can be significantly influenced by various contextual factors, including external challenges, such as health emergencies, security issues, and healthcare system instability. The outbreak of the COVID-19 pandemic, coupled with pre-existing security challenges and an unstable healthcare system, has posed unprecedented hurdles to maternal health services worldwide.5
In Sudan, antenatal care services provided by primary, secondary, and tertiary health care are the classical standard arrangements. Primary healthcare (PHC) is a basic health unit for ANC services.6
Sudan has a history of political, economic, and healthcare system challenges and faces unique obstacles in providing adequate maternal health care. The nation’s healthcare infrastructure has been further strained by the COVID-19 pandemic, which has disrupted healthcare delivery and created additional barriers to accessing antenatal care services.7 Concurrently, security challenges in some areas of Sudan have exacerbated the difficulties faced by pregnant women seeking essential healthcare.8
The emergence of the COVID-19 pandemic has significantly altered healthcare systems worldwide.9 The need for infection control measures, social distancing, and lockdowns has reduced access to healthcare facilities and changed health-seeking behaviors.10 Pregnant women, who constitute a vulnerable population, may be particularly affected by concerns regarding exposure to the virus. The pandemic’s impact on healthcare services and patient behavior has implications for antenatal care utilization, leading to potential delays in seeking care and compromising maternal and fetal health outcomes.11
The instability of Sudan’s healthcare system, driven by various factors, including economic constraints and inadequate infrastructure, poses additional barriers to accessing antenatal care services. Limited resources, health workforce shortages, and inadequate facilities can result in suboptimal healthcare service delivery, further discouraging pregnant women from seeking care.12
The utilization of ANC at primary healthcare centers was hindered in numerous regions globally. The prevalence of maternal health service usage was observed to be low in various places, such as Ethiopia13 and several developed countries,14 as well as in many African countries like Congo, Sierra Leone, and Uganda.15 The extent of disruption varied across these diverse settings, and it appeared to be qualitatively associated with the stringency of lockdown measures and the perceived attitudes towards the risks posed by COVID-19.
The utilization of ANC was significantly impacted and decreased in the face of security challenges at primary healthcare centers. This was assessed by evaluating the accessibility of antenatal care (ANC) services in primary healthcare facilities in Pakistan,16 revealing a substantial decline in ANC utilization. In India,17 this challenge further complicated efforts to ensure patient safety and equity in ANC services in many low-and middle-income countries.18 Security instability similarly affected ANC utilization in various regions of Sudan.
The utilization of ANC in the unstable health care system at primary health care centers can vary depending on various factors. One study conducted in rural Zambia19 found that the utilization of ANC services was affected by the availability and accessibility of healthcare facilities. In areas with unstable healthcare systems, there may be a lack of well-equipped primary healthcare centers, leading to reduced utilization of ANC services.20
Despite the acknowledged importance of antenatal care, limited research has explored the utilization of such services within the confluence of COVID-19, security challenges, and an unstable healthcare system, particularly in contexts like Sudan.21 We want by this study to address this gap by exploring the intersection of these complex challenges and their impact on the utilization of antenatal care services within primary health care centers in Sudan.
This study examines the utilization of antenatal care services within the challenging context of Sudan, where the COVID-19 pandemic, security challenges, and an unstable healthcare system at primary healthcare centers have posed significant barriers to the provision and utilization of essential maternal healthcare. By understanding the factors affecting antenatal care utilization in this context, we can identify strategies to improve access to and quality of care, ensuring the well-being of pregnant women and their infants. This study aims to shed light on the challenges faced by pregnant women in Sudan while offering insights and recommendations for policymakers and healthcare providers to address these issues effectively. The primary objective of this study was to assess the utilization of antenatal care services in the context of COVID-19, security challenges, and an unstable healthcare system at primary health care centers in Sudan.
Methodology
Study Design
This PHC-based cross-sectional study was conducted from June 2021 to June 2023. This study employed a mixed-methods research design to comprehensively investigate the utilization of antenatal care services within COVID-19, security challenges, and an unstable healthcare system in primary health care centers in Sudan. Integrating qualitative and quantitative approaches allows for a holistic understanding of the complex factors that influence antenatal care utilization.
Study Setting
The study was conducted across selected primary healthcare centers in the Sharge Elneil locality, Khartoum State, Sudan, including areas affected by security challenges. The centers were chosen to represent diverse socioeconomic backgrounds and varying degrees of healthcare system stability.
Theoretical Framework
Integrating a conceptual or theoretical model into research related to the utilization of antenatal care services within the context of COVID-19, security challenges, and an unstable healthcare system at primary health care centers are provide a structured framework for understanding the relationships and factors involved (Figure 1).
 |
Figure 1 Integrating conceptual theoretical model. |
Sampling Strategy
A stratified purposive sampling strategy was employed to ensure representation across geographical regions and security contexts. Fifteen primary health care centers were selected, and within each center, a convenience sample of pregnant women accessing antenatal care services was recruited.
Sampling
Simple random sampling was used to enroll participants. This study randomly investigated pregnant women regarding their utilization of antenatal care services. The sample size determines by: n =Zα/22×p (1–p)/d2 = 384 (minimum sample size). Accordingly, 536 women were enrolled in this study.
Data Collection
Quantitative Data Collection
A structured questionnaire was administered to pregnant women visiting the selected health care centers. To ensure the validity and reliability of the structured questionnaire it share the questionnaire with subject experts. The we collected feedback on the questionnaire’s clarity, relevance, and the appropriateness of the items. We make necessary revisions based on their suggestions.
The questionnaire included sections assessing sociodemographic characteristics, antenatal care utilization patterns, perceived barriers, experiences related to COVID-19, and security challenges. The questionnaire was developed based on validated scales and was adapted to the local context.
Qualitative Data Collection
Focus group discussions (FGD) were conducted with the 23 pregnant women to encourage open discussions and facilitate the exploration of shared experiences and perspectives. The FGD explores the aspects of antenatal care utilization, the impact of COVID-19 and security challenges, and perspectives on the stability of the healthcare system. We choose a skilled facilitator to guide the discussion, ensure all participants have an opportunity to speak, and maintain a constructive and respectful atmosphere.
Data Analysis
Quantitative Data Analysis
Descriptive statistical analysis was performed to summarize the demographic characteristics and antenatal care utilization patterns. A logistic regression analysis was executed to explore the relationship between various factors, encompassing sociodemographic elements, perceptions linked to COVID-19, concerns about security, and the extent of antenatal care utilization. The study data were subjected to various statistical procedures before analysis using STATA BE 17.
Qualitative Data Analysis
Thematic analysis was employed to analyze qualitative data from interviews and focus group discussions. Transcribed data were coded and categorized into themes and sub-themes to capture participants’ experiences, perceptions, and challenges related to antenatal care utilization.
Ethical Considerations
Ethical approval was obtained from the Gezira Institute of Safe Motherhood and Childhood. Informed consent was secured from all participants, underscoring their entitlement to privacy and voluntary engagement. Efforts were made to maintain confidentiality and anonymity of the participants.
Result
This study included 536 pregnant women attending antenatal care, regardless of their age and marital status, after matching the inclusion criteria. Table 1 provides an overview of antenatal care (ANC) service utilization according to various sociodemographic characteristics among the 536 participants. The table presents the distribution of participants who regularly attended ANC services and those who did not, categorized by different variables, including age, educational level, parity, occupation, marital status, and various interruptions related to COVID-19. University graduates (p = 0.00), multiparas (p = 0.01), and unemployed (p = 0.01) attended antenatal care. Several factors significantly hinder regular antenatal care attendance. Significantly, these disruptions resulted from the COVID-19 pandemic, affecting 163 participants (30.4%) (with a p-value = 0.03).
 |
Table 1 Utilization of Antenatal Care Services According to the Characteristics and Issues Leaded to ANC Services Interruption (n=536) |
Additionally, concerns regarding infection during the pandemic disrupted the care of 146 participants (27.2%) (p = 0.01). Public transportation instability also played a role, affecting 262 individuals (p = 0.01). Moreover, services were further interrupted owing to security challenges arising from unstable situations and conflicts. Beyond the influence of the COVID-19 pandemic, the significant reduction in the utilization of ANC services was attributed to challenging security instability, affecting 258 individuals (p = 0.00). The findings are presented in (Table 1).
Logistic regression analysis aimed to explore the relationships between sociodemographic factors, perceptions of COVID-19, security concerns, and the utilization of antenatal care services. Women aged 40–49 years had significantly lower odds of antenatal care utilization compared to women of other age groups (OR=0.56, CI 0.37–0.85, p = 0.007). Women with primary (OR 0.89), secondary (OR 1.12), university (OR 1.28), and post-graduate education (OR 1.45) had odds of antenatal care utilization that were not significantly different from those of illiterate women (p > 0.05). Women who were grand multipara had slightly lower odds of antenatal care utilization than multiparous women (OR=0.76, CI 0.53–1.10, p = 0.141). The odds of antenatal care utilization were not significantly different between the employed and unemployed women (odds ratio [OR] =0.91, CI 0.65–1.29, p = 0.614).
Women who had a perception of COVID-19 had lower odds of antenatal care utilization compared to those without the perception (OR=0.72, CI 0.53–0.98, p = 0.037). This suggests that COVID-19 perceptions may be associated with decreased ANC utilization. Women who expressed security concerns had slightly lower odds of antenatal care utilization than those without security concerns (OR=0.82, CI 0.58–1.16, p = 0.266). (Table 2).
 |
Table 2 Logistic Regression Analysis to Examine the Factor Influence Antenatal Care Utilization (n=536) |
Qualitative Findings
Qualitative interviews were undertaken to delve into the firsthand experiences and perspectives of participants concerning the utilization of ANC services in this particular context. In-depth interviews were conducted to explore pregnant women’s experiences and perceptions of attending ANC services in the context of COVID-19, security challenges, and an unstable healthcare system at primary health care centers in Sudan. The thematic analysis revealed insights into the motivations, challenges, and strategies for ANC attendance (Table 3).
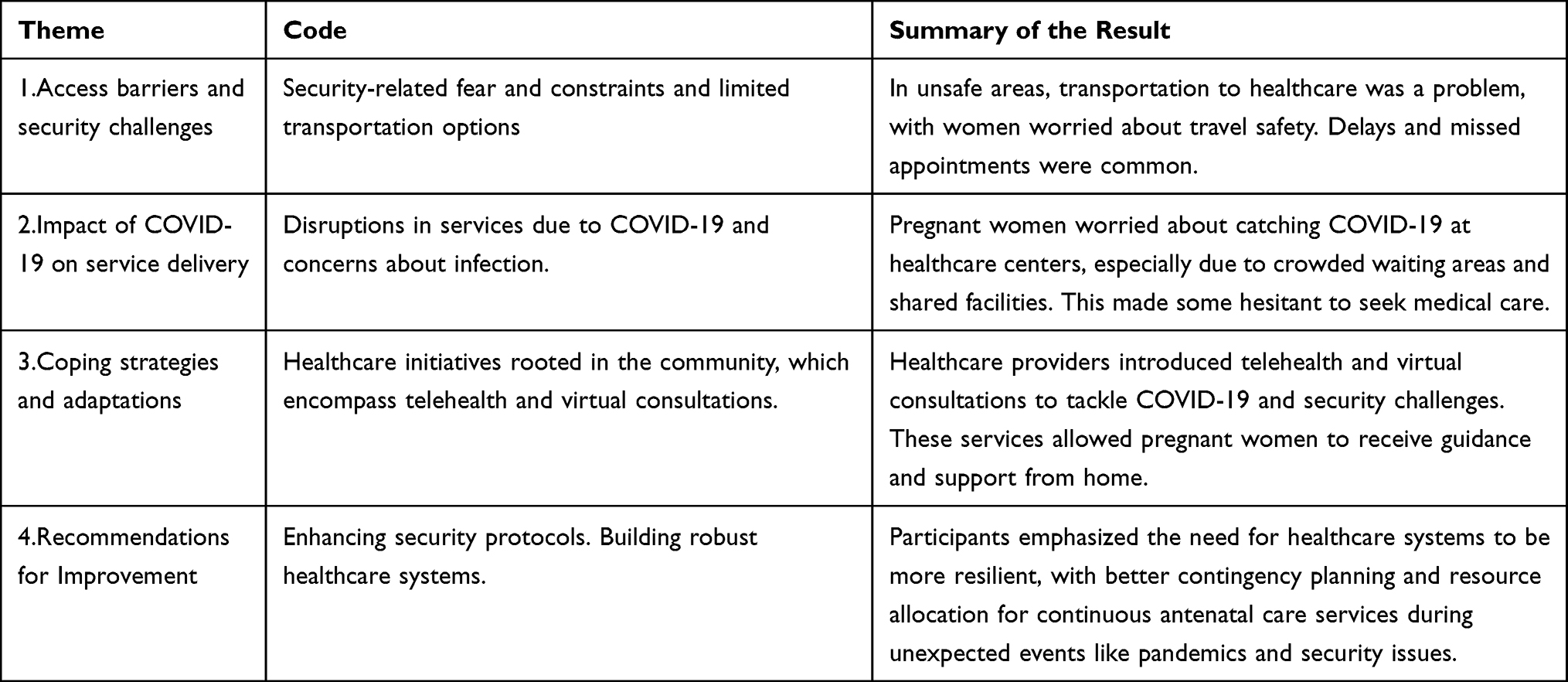 |
Table 3 Summary of Qualitative Result |
Many pregnant women reported significant fear and anxiety associated with attending antenatal care services because of prevailing security challenges. Some participants noted instances of violence and threats near healthcare centers, which deterred them from seeking care in areas with security challenges, access to reliable transportation to healthcare centers is a common barrier. Women expressed concerns about the safety of traveling to and from these centers, which often led to delayed or missed appointments.
Healthcare providers have described disruptions in antenatal care services caused by COVID-19, including the reallocation of resources and staff to respond to the pandemic. These disruptions result in a reduced frequency of antenatal check-ups.
Pregnant women conveyed concerns about the risk of contracting COVID-19 while attending healthcare centers, particularly given crowded waiting areas and shared facilities. These fears sometimes lead to reluctance to seek care.
In areas with unstable healthcare systems, some communities have established local, informal networks to provide basic antenatal care information and support, helping women manage their pregnancies in the absence of reliable healthcare services.
In response to the challenges posed by COVID-19 and security issues, healthcare providers have begun to implement telehealth and virtual consultation services. This allowed pregnant women to receive guidance and support regarding the safety of their homes.
Both pregnant women and healthcare providers emphasized the need for enhanced security measures around healthcare centers, such as increased policing and the establishment of safe zones to ensure the safety of pregnant women seeking care.
Participants suggested the need for more resilient healthcare systems that can adapt to unforeseen challenges, with better contingency planning and resource allocation to ensure continuous antenatal care services during crises, such as pandemics and security issues.
The qualitative findings underscore the resilience of pregnant women in attending ANC services amid the complexities of the COVID-19 pandemic, security challenges, and an unstable healthcare system.
Discussion
This study has uncovered critical insights into the complex landscape of antenatal care in challenging environments. In this discussion, we highlight the key findings and their implications.
The results of this study shed light on the complex interplay between sociodemographic factors, disruptions caused by the COVID-19 pandemic, and security challenges that influence ANC utilization. The outcomes of this study are in line with established literature, underscoring the diverse factors that impact ANC utilization.22–24 These parallels underscore the global nature of these challenges and the need for context-specific intervention. We must address the complexity of the factors influencing ANC utilization, encompassing sociodemographic and external challenges.
Studies have demonstrated the detrimental impact of the pandemic on various healthcare services, in this study the significant reduction in the utilization of ANC services was attributed to challenging security instability. The study revealed that security challenges significantly impede the utilization of antenatal care services. Pregnant women faced fear, anxiety, and even violence when trying to access healthcare facilities. This aligns with research indicating that conflict and insecurity disrupt essential health services, particularly in low-resource settings.25,26 This has profound implications for maternal and child health, as it discourages timely and regular antenatal check-ups. The presence of security concerns necessitates immediate attention from local authorities, possibly through increased policing and the establishment of safe zones around healthcare centers.
The community-based health initiatives, including telehealth and virtual consultations, emerged as innovative solutions to address the challenges presented by COVID-19 and security issues. These adaptations allowed pregnant women to receive the necessary guidance and support without risking exposure. These strategies should be further developed and integrated into healthcare systems as they have proven effective in ensuring care continuity. These adaptations align with global efforts to leverage technology and community engagement to ensure the continuity of essential healthcare services during crises.25,26 Such strategies can potentially improve access to healthcare beyond the pandemic and promote equity and reach. The outcomes of this study are in line with established literature, underscoring the diverse factors that impact ANC utilization.27,28 Health interventions involving communities can have lasting positive effects on healthcare-seeking behaviors and health outcomes.
The study participants strongly advocated for enhanced security measures and resilient healthcare systems. Increased policing and the establishment of safe zones were seen as necessary steps to ensure the safety of pregnant women seeking care. Additionally, participants stressed the importance of healthcare systems being flexible and adaptive to unforeseen challenges, with better contingency planning and resource allocation. These recommendations could serve as a blueprint for healthcare policy and planning in similar regions.29–35 Comprehensive policy and programmatic interventions are essential to address the multifaceted challenges identified in this study.
This study provides essential insights into the utilization of antenatal care services in contexts of COVID-19, security challenges, and unstable healthcare systems. Addressing these challenges necessitates a multifaceted approach involving local authorities, healthcare providers, and communities. It is imperative to prioritize the safety and well-being of pregnant women, promote innovative solutions, and build healthcare systems that are resilient and adaptable in the face of crises.
Limitations
The study’s constraints encompass its cross-sectional design, which hampers the establishment of causal connections, and the potential for bias in participants’ self-reporting. Further research could explore the long-term impact of decreased ANC utilization on maternal and child health outcomes as well as the sustainability of adaptive strategies.
Conclusion
The proposed mixed-methods research design aimed to provide a comprehensive understanding of the utilization of antenatal care services in Sudan within the complex context of COVID-19, security challenges, and an unstable healthcare system. By integrating quantitative and qualitative approaches, this study attempts to capture the multifaceted factors shaping antenatal care utilization and inform policy recommendations that address the unique challenges faced by pregnant women in this context. In Sudan, the situation is more complicated than elsewhere because, in addition to the COVID −19 pandemic, there has been economic, social, and security instability since the Sudanese revolution. Ultimately, this study contributes to a broader understanding of healthcare access within complex contexts, advocating resilient and adaptable healthcare systems that prioritize maternal and neonatal health.
Ethical Consideration
This study was conducted in accordance with the Declaration of Helsinki. Ethical clearance was acquired from the Institutional Review Board (IRB) of the University of Gezira, Institute of Safe Motherhood and Childhood, Sudan. Informed consent was obtained after providing a comprehensive explanation before the commencement of data collection.
Acknowledgments
The author is thankful to the Deanship of Graduate Studies and Scientific Research at University of Bisha for supporting this work through the Fast-Track Research Support Program.
The author would also like to express his gratitude to his colleagues Tuga Hassan and Narmin Ezden for their invaluable efforts in gathering data and spearheading the data collection initiative with the support of the health administration in Sharge Elneil locality, Khartoum State, Sudan.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Whittingham KL, Earle AG, Leyva-de la Hiz DI, Argiolas A. The impact of the United Nations SUSTAINABLE DEVELOPMENT GOALS on corporate sustainability reporting. BRQ Bus Res Q. 2023;26(1):45–61. doi:10.1177/23409444221085585
2. Tikmani SS, Ali SA, Saleem S, et al. Trends of antenatal care during pregnancy in low-and middle-income countries: findings from the global network maternal and newborn health registry. InInSeminars in Perinatology;2019Aug1. Vol. 435: pp.297–307. WB Saunders.
3. World Health Organization. Packages of interventions for family planning, safe abortion care, maternal, newborn and child health. World Health Organization; 2010. Available from: https://apps.who.int/iris/bitstream/handle/10665/70428/WHO_FCH_10.06_eng.pdf.
4. Valdez M, Stollak I, Pfeiffer E, et al. Reducing inequities in maternal and child health in rural Guatemala through the CBIO+ approach of Curamericas: 1. Introduction and project description. Int J Equity Health. 2023;21(2):1–9. doi:10.1186/s12939-022-01752-y
5. Filip R, Gheorghita Puscaselu R, Anchidin-Norocel L, Dimian M, Savage WK. Global challenges to public health care systems during the COVID-19 pandemic: a review of pandemic measures and problems. J Pers Med. 2022;12(8):1295. doi:10.3390/jpm12081295
6. Mohamed SO, Ahmed EM. Prevalence and determinants of antenatal tetanus vaccination in Sudan: a cross-sectional analysis of the multiple indicator cluster survey. Trop Med Int Health. 2022;50(1):1–6. doi:10.1186/s41182-022-00398-4
7. Pilav S, Easter A, Silverio SA, et al. Experiences of perinatal mental health care among minority ethnic women during the COVID-19 pandemic in London: a qualitative study. Int J Environ Res Public Health. 2022;19(4):1975. doi:10.3390/ijerph19041975
8. Aderinto N, Olatunji D. The consequences of Sudan’s armed conflict on public health: a closer look at the devastating impact. IJS Global Health. 2023;6(4):e0179. doi:10.1097/GH9.0000000000000179
9. Frenk J, Chen LC, Chandran L, et al. Challenges and opportunities for educating health professionals after the COVID-19 pandemic. Lancet. 2022;400(10362):1539–1556. doi:10.1016/S0140-6736(22)02092-X
10. Mehta S, Puwar T, Patel Y, et al. Understanding health-seeking behavior of people with diabetes during COVID-19 pandemic: a facility based cross-sectional study conducted in Ahmedabad, India. Clin Diabetol. 2023;12(3):141–149. doi:10.5603/DK.a2023.0013
11. Paudel M, Leghari A, Ahmad AM, et al. Understanding changes made to reproductive, maternal, newborn and child health services in Pakistan during the COVID-19 pandemic: a qualitative study. Sexual Reprod Health Matters. 2022;30(1):2080167. doi:10.1080/26410397.2022.2080167
12. Ebrahim EM, Ghebrehiwot L, Abdalgfar T, Juni MH. Health care system in Sudan: review and analysis of strength, weakness, opportunity, and threats (SWOT analysis). Sudan J Med Sci. 2017;12(3):133–150. doi:10.18502/sjms.v12i3.924
13. Temesgen K, Wakgari N, Debelo BT, et al. Maternal health care services utilization amidstCOVID-19 pandemic in West Shoa zone, central Ethiopia. PLoS One. 2021;16(3):e0249214. doi:10.1371/journal.pone.0249214
14. Aranda Z, Binde T, Tashman K, et al. Disruptions in maternal health service use during the COVID-19 pandemic in 2020: experiences from 37 health facilities in low-income and middle-income countries. BMJ Global Health. 2022;7(1):e007247. doi:10.1136/bmjgh-2021-007247
15. Kasonia K, Tindanbil D, Kitonsa J, et al. The impact of the COVID-19 pandemic on the provision & utilisation of primary health care services in Goma, democratic Republic of the Congo, Kambia district, Sierra Leone & Masaka district, Uganda. PLoS One. 2023;18(6):e0286295. doi:10.1371/journal.pone.0286295
16. Majrooh MA, Hasnain S, Akram J, Siddiqui A, Shah F, Memon Z. Accessibility of antenatal services at primary healthcare facilities in Punjab, Pakistan. J Pak Med Assoc. 2013;63(4):60.
17. Guagliardo MF. Spatial accessibility of primary care: concepts, methods and challenges. Int J Health Geogrs. 2004;3(1):1–3. doi:10.1186/1476-072X-3-3
18. Vasan A, Mabey DC, Chaudhri S, Brown Epstein HA, Lawn SD. Support and performance improvement for primary health care workers in low-and middle-income countries: a scoping review of intervention design and methods. Health Policy Plann. 2017;32(3):437–452. doi:10.1093/heapol/czw144
19. Kyei NN, Campbell OM, Gabrysch S. The influence of distance and level of service provision on antenatal care use in rural Zambia. PLoS One. 2012;7(10):e46475. doi:10.1371/journal.pone.0046475
20. Ambikile JS, Iseselo MK. Mental health care and delivery system at temeke hospital in Dar es Salaam, Tanzania. BMC Psychiatry. 2017;17(109). doi:10.1186/s12888-017-1271-9
21. AlKhaldi M, Abouhala S, Alhalaiqa F, Ibrahim A, Kashash RA, Abusalah A. Health policies of adolescents in the middle East and North Africa: past experiences, current scene, and future strategic directions. InInAdolescent Mental Health in the Middle East and North Africa;2022 May 15: pp. 93–115. Cham: Springer International Publishing.
22. Namatovu HK, Semwanga AR. A systems dynamics approach to understanding the determinants of antenatal care utilization in low-and middle-income countries: a systematic review. Res Anthol Adv Women’s Health Reproductive Rights. 2022;836–856. doi:10.4018/978-1-6684-6299-7.ch044
23. Asim M, Saleem S, Ahmed ZH, et al. We won’t go there: barriers to accessing maternal and newborn care in District Thatta, Pakistan. InHealthcare. 2021;9(10):1314. doi:10.3390/healthcare9101314
24. Tolera H, Gebre-Egziabher T, Kloos H. Using Andersen’s behavioral model of health care utilization in a decentralized program to examine the use of antenatal care in rural western Ethiopia. PLoS One. 2020;15(1):e0228282. doi:10.1371/journal.pone.0228282
25. Fouad FM, Soares L, Diab JL, Abouzeid A. The political economy of health in conflict: lessons learned from three states in the Eastern Mediterranean Region during COVID-19. J Glob Health. 2022;12. doi:10.7189/jogh.12.07001
26. Nesamoney SN, Darmstadt GL, Wise PH. Addressing the impacts of COVID-19 on gender equality and global health security in regions of violent conflict. J Glob Health. 2021;11. doi:10.7189/jogh.11.03074
27. Marston C, Renedo A, McGowan CR, Portela A. Effects of community participation on improving uptake of skilled care for maternal and newborn health: a systematic review. PLoS One. 2013;8(2):e55012. doi:10.1371/journal.pone.0055012
28. Smittenaar P, Ramesh BM, Jain M, et al. Bringing greater precision to interactions between community health workers and households to improve maternal and newborn health outcomes in India. Global Health. 2020;8(3):358–371. doi:10.9745/GHSP-D-20-00027
29. Swanepoel D, Clark JL. Hearing healthcare in remote or resource-constrained environments. J Laryngology Otol. 2019;133(1):11–17. doi:10.1017/S0022215118001159
30. Gamberini C, Angeli F, Ambrosino E. Exploring solutions to improve antenatal care in resource-limited settings: an expert consultation. BMC Pregnancy Childbirth. 2022;22(1):449. doi:10.1186/s12884-022-04778-w
31. Zhang YN, Chen Y, Wang Y, et al. Reduction in healthcare services during the COVID-19 pandemic in China. BMJ Global Health. 2020;5(11):e003421. doi:10.1136/bmjgh-2020-003421
32. Sohrabi C, Alsafi Z, O’neill N, et al. World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int j Surg. 2020;76:71–76. doi:10.1016/j.ijsu.2020.02.034
33. Riley T, Sully E, Ahmed Z, Biddlecom A. Estimates of the potential impact of the COVID-19 pandemic on sexual and reproductive health in low-and middle-income countries. Int Perspect Sex Reprod Health. 2020;46:73–76. doi:10.1363/46e9020
34. Thapa SB, Mainali A, Schwank SE, Acharya G. Maternal mental health in the time of the COVID‐19 pandemic. Acta obstetricia et gynecologica Scandinavica. 2020;99(7):817. doi:10.1111/aogs.13894
35. Babalola OJ, Sesay HW, Blebo LS, et al. The influence of first wave of COVID-19 outbreak on routine healthcare services, Liberia, August 2020: a mixed study approach. BMC Health Serv Res. 2022;22(1):1. doi:10.1186/s12913-022-08074-3
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.