")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Using a Double Syringe Sterile System for MSK Aspiration/Injection Procedures Eliminates Risk of Iatrogenic Infection
Authors Lazarescu AE , Hogea BG , Andor BC, Totorean A, Cojocaru DG, Negru M, Bolintineanu LA, Patrascu Jnr JM, Misca LC, Sandesc MA, Patrascu Snr JM
Received 3 May 2022
Accepted for publication 29 September 2022
Published 29 October 2022 Volume 2022:18 Pages 1029—1036
DOI https://doi.org/10.2147/TCRM.S372676
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Adrian Emil Lazarescu,1– 3 Bogdan Gheorghe Hogea,2– 4 Bogdan Corneliu Andor,2– 4 Alina Totorean,2,5 Dan Grigore Cojocaru,2,3 Marius Negru,6 Laura A Bolintineanu,7 Jenel Marian Patrascu Jnr,2– 4 Liviu C Misca,2– 4 Mihai A Sandesc,2– 4 Jenel Marian Patrascu Snr2– 4
1Department of Anatomy and Embriology, University of Medicine and Pharmacy “victor Babes” Timișoara, Timisoara, Romania; 2 2nd Clinic of Orthopedics and Traumatology, County Emergency Hospital “Pius Branzeu” Timisoara, Timisoara, Romania; 3Profesor Teodor Sora’ Research Center, University of Medicine and Pharmacy “Victor Babes” Timișoara, Timisoara, Romania; 4Department of Orthopedics and Traumatology, University of Medicine and Pharmacy “Victor Babes” Timișoara, Timisoara, Romania; 5Department of Medical Recovery, University of Medicine and Pharmacy “Victor Babes” Timișoara, Timisoara, Romania; 6Department of Pediatric Surgery, University of Medicine and Pharmacy “Victor Babes” Timișoara, Timisoara, Romania; 7Department of Pathophysiology, University of Medicine and Pharmacy “Victor Babes” Timișoara, Timisoara, Romania
Correspondence: Bogdan Gheorghe Hogea, Tel +40744363188, Email [email protected]
Introduction: Diverse musculo-skeletal pathology can be treated conservatively by different types of injections and in most cases, results are significantly better if the existing inflammatory fluid is aspirated prior to injection of medication solutions. The present study analyses an original technique which uses infusion therapy accessories to create two types of closed sterile double syringe systems, and compares the benefits of using such a system in aspiration/injection procedures to classic aspiration injection technique that implies changing and connecting multiple syringes to the same needle, thus increasing the risk for septic complications. The aim of the present study is to minimize therapeutic risk of iatrogenic septic complications during aspiration/injection procedures.
Methods: 1024 patients underwent aspiration/injection procedures in our clinic using the double syringe system between 2015 and 2020. During the early stages of the study, the second type of assembly was rendered impractical so the study continued with analyzing a single type of double syringe system using a three way infusion therapy device which is readily available, and allows the assembly of a closed sterile system with a single, two-step procedure technique. Iatrogenic local septic complications were followed by means of a six week clinical follow-up evaluation with additional investigations only if necessary.
Results: In 1024 procedures we report 0% incidence of iatrogenic septic complications, or other types of complications and recommend this technique in a vast array of rheumatic, orthopedic or traumatic conditions that require aspiration/injection procedures.
Discussion: The double syringe system is practical, easy to use, it completely eliminates the risk of iatrogenic infection due to manipulation errors, and significantly simplifies the technique for sonography guided aspiration/injection procedures for musculo-skeletal pathology.
Keywords: musculo-skeletal injections, aspiration/injection technique, double syringe system, iatrogenic infection, rheumatology, joint pathology
Background/Objective
Many pathological conditions resulting from musculo-skeletal (MSK) injuries or chronic degenerative joint and tendon pathology require local corticosteroid injections or different types of medication which are administered locally, like hialuronic acid.1–4 It has been shown that these types of injections have better results if the inflammatory fluid, present at the site of injection, is aspired before injecting the medicine, instead of adding the medication onto an already high pressure effusion.5,6 Weitoft et al demonstrates that aspiration of the synovial fluid before injection of the corticosteroid solution significantly reduces arthritis relapse and leads to better results, concluding that “arthrocentesis shall be included in the intra-articular corticosteroid injection procedures”.5 The same applies to visco-elastic supplementation procedures.2 Zhang et al demonstrates that all scores are significantly improved if joint injection of hyaluronic acid is preceded by aspiration.6 Producers and experts recommend aspiration of joint fluid before injecting the hyaluronic acid solution as well.7,8 Taking all this into consideration, it is interesting to see that aspiration before musculo-skeletal injections is not routinely done in clinical settings. We find that the reason is represented by the associated septic risk that comes with manipulating syringes during intra-articular injections9 potentially compromising the sterility of the procedure leading to severe septic complications.
Whatever the clinical situation, aspiration/injection of symptomatic Baker cyst,10 acute tenosynovitis11 or visco-supplementation procedures,6 aspiration of the existing pathological fluid followed by injection of the medication solutions implies changing syringes during the procedure, in the sense that the fluid is aspirated, the needle is left in place and the syringe changed for the one with the substance meant to be injected in the first place.12 However, holding the needle in place and changing syringes is not recommended unless it can be achieved in completely sterile conditions to avoid joint contamination with dramatic consequences that follow, like acute septic arthritis which can even be fatal.13
The field of MSK imaging guided procedures has become impressively vast and the reason for this is accuracy of the injections and visual certainty that the solution is administered at the perfect location to ensure optimal results for the patient and the specific pathology.14–16 Direct visualization also ensures aspiration success and facilitates joint procedures which are becoming fairly common in the clinical setting. On the other hand, handling the probe and performing the procedure at the same time can be technically challenging especially because of the need to change syringes while leaving the needle in place. Usually an assistant is required to hold the probe in place while the physician handles the needle and syringes. Even so, switching syringes, being carefully not to dislocate the tip of the needle, keeping your eyes at the screen as well, can lead to human error with contamination of the syringe and dramatic consequences, with infection rate considered to be 1 in 3000 to 1 in 100,000 after joint injections.17 Furthermore, in most septic complications following joint or tendon injection the cause is considered to be faulty technique.17 It is important to differentiate septic arthritis and pseudoseptic arthritis that can sometimes occur after visco-supplementation procedures and resolves with rest and conservative treatment.18
The aim of the present study is to propose an original technique and demonstrate that the double syringe system (DSS.) completely eliminates the risk of iatrogenic infection in aspiration/injection procedures performed in various joint pathology, by eliminating the potentially unsecure gesture of switching syringes with the needle left in place at the injection site.
Materials and Methods
Study Design
The present study follows one single potential complication that results from musculo-skeletal aspiration/injection procedures and this is iatrogenic septic complications resulting from the technical difficulty of switching the aspiration syringe with the final injection syringe with the needle left in place, while also holding the sonography probe in some situations. The study compares two different assemblies that allow the connection of two syringes, using ready available intra-venous (i.v.) administration accessories (Figure 1).
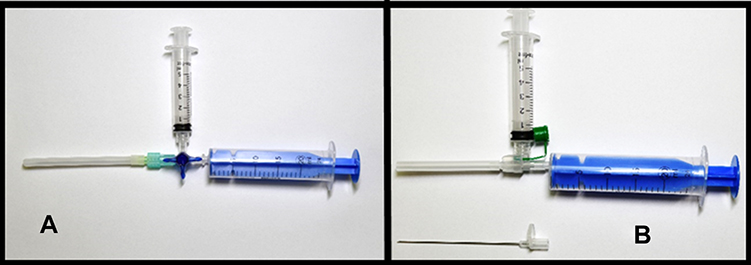 |
Figure 1 (A) double syringe system type A using the three way stopcock Discofix-3, with a 5 mL syringe for treatment solution and a 20 mL syringe for aspiration; (B) double syringe system type B using a standard i.v. catheter with aspiration syringe connected after placing the needle in place and removal of the guide needle. |
The present study is strictly designed to demonstrate two original aspiration/injection techniques using sterile i.v. administration accessories to create a closed sterile system that avoids manipulating the needle or syringes during the procedure. The present study is not designed to discuss the type of medication administered or any kind of outcome following these procedures, but only focus on reducing the risk of iatrogenic septic complications at the site of injection.
Sample
The study group consists of 1024 patients (Table 1), who were admitted to our Clinique for intra articular injection of visco-elastic solutions. All patient were already under observation for either coxarthrosis or gonarthrosis, unilateral or bilateral or both hip and knee pathology, mild or moderate forms of the disease with indication for conservative treatment and surgical indication when clinical symptoms deteriorate. In this group of patients some of them were diagnosed with associated musculo-skeletal pathology that also had indications for aspiration/injection procedures and were treated accordingly: shoulder subacromial bursitis 15%, symptomatic Baker cyst 14%, calcific supraspinatus tendinopathy 10%, tenosynovitis (with significant amount of fluid in the tendon sheath) 9%, synovial cyst 6%, suprapatelar bursitis 2% (Table 1). However, the type of pathology, the type of medication administered and clinical results do not make the subject of the present study.
 |
Table 1 Study Group Characterization |
The only parameter followed in the present study is iatrogenic infection after MSK aspiration/injection procedures using the DSS. The study was conducted following the Declaration of Helsinki of 1975 revised in 2013. All participants signed a written consent for the procedure and the study was authorized by the ethical committee of the University of Medicine and Pharmacy Victor Babes Timisoara Nr. 8/2015, and also by the ethics committee of the Emergency County Hospital “Pius Branzeu” Timisoara Nr.242/20.APR.2021.
Technique
A sterile technique is mandatory in any joint/tendon injection. In order to achieve this the research team used a one time application of alcohol on a large area surrounding the site of the procedure followed by a minimum of three applications of surgical iodopovidone on a large area around the puncture site, with adequate time for drying so that the solution penetrates the deep layers of the skin in order to avoid other potential sources of iatrogenic contamination. We selected two assemblies for a double syringe system in order to allow aspiration/injection procedures with a completely closed sterile system, using common intra-venous administration accessories.
Double Syringe System Type A (DSSA)
The first type of assembly (Figure 1A) uses a three way stopcock designed for infusion therapy (Discofix-3 produced by B.Braun) which allows for two syringes to be connected to one single needle (24 Gauge) but also allows the physician to control flow, alternatively for each syringe.
Double Syringe System Type B (DSSB)
The second type of assembly (Figure 1B) also uses an administration accessory designed for infusion therapy which is known as peripheral IV catheter (Vasofix Safety Pur produced by BBraun) with a 24 Gauge needle.
Assembly of the sterile components was done before preparing the site of injection, all components were handled with sterile gloves. For the aspiration syringe we used a 20–50 mL syringe depending on the amount of fluid expected to be aspirated and for medication a 5 mL syringe was prefilled with the medication solution before connecting it to the assembly. Once the system assembly is completed, attention is directed to preparing the site of injection. Because all procedures were assisted by sonography, a piece of tape was used to separate the sterile field from the probe field where gel was applied.
System A Technique
The entire assembly is mounted before the procedure starts using sterile gloves and sterile field. The stopcock is set in aspiration position to only allow the aspiration syringe to be connected to the needle (Figure 2A). After local preparation the needle is placed in position and aspiration is completed first (Figure 2B). The stopcock is then oriented to block the aspiration syringe and open the treatment syringe so the treatment solution can be injected (Figure 2C). The treatment is injected and the entire assembly removed (Figure 2D) followed by compressive dressing for 30 min.
 |
Figure 2 (A) system is set for aspiration after the needle will be in place, red arrows demonstrate the direction of the aspirate from tip of needle towards the aspiration syringe; (B) aspiration is completed and stopcock is rotated clockwise. The red arrow indicates the 90 degree rotation of the stopcock, to block the aspiration syringe and open the injection syringe; (C) treatment solution can be administered without changing needle tip location. The red arrows indicate the direction of injectate flow from medication syringe to the tip of the needle location; (D) double syringe system at the end of the procedure. |
System B Technique
The treatment syringe is connected before the procedure. After the needle is placed, the guide needle is removed and the aspiration syringe attached. After the aspiration is completed the final treatment solution is injected. During aspiration, the second syringe needs to be fixed by hand so that the negative pressure resulting from the viscosity of the pathological fluid does not lead to aspiration of the medication solution instead of the content of the pathological collection.
After all aspiration/injection procedures, the patients were advised to rest for 3 to 5 days, use local cryotherapy for 1 to 3 days and address the clinic if any adverse effects were noticed. Otherwise they were instructed to return for the six week follow-up clinical exam to evaluate any potential signs of septic local complications. Six week visit protocol included clinical examination and only in case of any clinical signs that suggest local complications, further imagistic imaging like plain radiographs, MSK sonography and magnetic resonance imaging according to the clinical situation, as decided by the physician.
Results
DSSB is far less practical and efficient because of the inability to block the syringes individually. Because of this, at the moment of aspiration (because aspirate fluids are usually of higher viscosity than the injection solution) the injection solution was aspirated in the second syringe. To avoid this, the physician needs to hold and manually lock the injection syringe. Also because i.v. catheters have the guide needle, the aspiration syringe would have to be connected after needle placement which led to the loss of the main objective of our study, specifically to avoid manipulating syringes after needle placement. In addition the flexible plastic tube that is left in place was not as reliable as a standard needle. These technical difficulties justified stopping the DSSB procedures and to continue our study using only the DSSA which completely met the initial objectives of our study design: a system that is easy to use, practical and a completely closed sterile system that is also relatively inexpensive.
In all 1020 procedures that were done in the present study using the DSSA, the success rate of the procedure was 100% with aspiration followed by injection from the second syringe using the i.v. three way stopcock designed for infusion therapy (Disco-Fix produced by B.Braun) (Figure 1A). 4 procedures with system type B were successful but with unnecessary technical difficulties that are completely eliminated by using the DSSA.
In 1024 procedures the infection rate was 0% (Table 1). At six weeks, the follow-up clinical examination revealed normal anatomy with the complete absence of clinical signs of infection like local redness, edema, high temperature, etc. Because of this, no further imaging investigations were solicitated by the physicians that conducted the follow-up clinical examination. Most patients described local tenderness for 1–3 days which is usually noted in MSK injections that did not need treatment besides local cryotherapy and rest. We observed mild inflammation of the joint in 2 cases following injection of hyaluronic acid but this is usually observed when injecting visco-elastic substances, regardless of the technique used, and symptoms resolution was achieved in 10 to 14 days with conservative treatment. Following visco-elastic supplementation 88% of patients declared significant articular functional and pain improvements, with the remaining 12% declaring stationary evolution at the six week mark (Table 1). Following local corticosteroid injection for bursitis or tenosynovitis, 92% of patients declared major improvement in pain and function at six weeks but in these cases patients also continued with physical therapy and other conservative treatments (Table 1).
Discussions
Results demonstrate that the DSS completely removes the risk of joint contamination due to syringe manipulation errors during the aspiration/injection procedure. In all visco-supplementation procedures for arthritis, experts and producers recommend aspiration of the existing joint fluid7,24 before injecting medication solutions.
The potential indications for using the DSS under sonography guidance are vast, ranging from joint injections,5,6 conservative treatment of ganglion cysts (Figure 3) 19 and Baker cyst in particular,10 bursitis,20 to rare pathology like intra-neural ganglion cyst21 or intra-spinal synovial cyst22,23 and many other clinical situations that require an aspiration/injection procedure.
 |
Figure 3 Technique presentation for aspiration/injection procedure of a wrist synovial cyst; (A) approach and needle placement was done after understanding local anatomy with sonography, with wide skin preparation and sterile technique under local anesthesia; (B) aspiration of cyst content; (C) injection of corticosteroid after aspiration is completed; (D) 6 week follow-up visit with clinical assessment (patient used compressive bandage during activities after the procedure). |
The technique described brings many advantages and benefits to the field of MSK injections. Current techniques imply changing syringes while leaving the needle in place, but the technique described in the present study completely eliminates syringe manipulation during the procedure, making it safer for the patient and easier for the physician, in comparison with techniques found in the literature. Furthermore, when assembling the DSSA each component is chosen with regard to the pathological situation, like type of needle or syringe dimensions. Sonography guidance of minimally invasive procedures is a constantly developing field, and quickly becoming standard practice (Figure 4). A practical improvement of the technique is much needed in aspiration/injection procedures.
 |
Figure 4 Sonography images collected from our series of patients; (A) image obtained during vasco-supplementation of the Hip using the convex probe, with obvious thickening of the joint capsule and small quantity of intra articular fluid; (B) image obtained from a patient suffering from Milwaukee Shoulder arthropathy were evacuation was attempted (with no success due to high viscosity of intra articular deposits) before local steroid injection. |
The limitations of the present study consist of the comparative nature of the study between two original techniques without adding a control group in which the procedure would be done by a standard technique that implies changing needles during the procedure. Authors avoided this in their daily practice and have decided to use data in the current literature regarding septic complication rates of this procedure, rather than recreating a study group in which such severe complications are likely to emerge.
The economic impacts of the present results are twofold: all necessary components of the DSSA are readily available as infusion therapy accesories and it also lowers healthcare costs by avoiding unnecessary hospital admissions and hospital stay (by suggesting a safe sterile technique easily achieved in a clinical office setting).
Conclusions
The DSSA is a powerfull tool with 0% iatrogenic infection rate that makes aspiration/injection procedures safer for the patient and technically effortless for the physician, thus offering a much needed solution to lower the clinical risk of complications and allow aspiration/injection procedures to gain popularity in clinical practice, while avoiding unnecessary hospital admissions. Using this technique, sterile conditions can be achieved in a clinical office setting, reducing cost and making aspiration/injection procedures widely accessible.
The present study concludes that using the i.v. catheter is not as practical and efficient as using the three way stopcock designed for infusion therapy (Figure 1A).
Abbreviations
MSK, musculo-skeletal; I.V, intra-venous; DSS, double syringe system; DSSA, double syringe system type A; DSSB, double syringe system type B.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Ethics Review Board of of the University of Medicine and Pharmacy Victor Babes Timisoara nr 8/2015, and also by the ethics committee of the Emergency County Hospital “Pius Branzeu” Timisoara nr. 242/20.APR.2021.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Funding
This research received no external funding.
Disclosure
The authors declare no conflict of interest.
References
1. Bellamy N, Campbell J, Robinson V, Gee T, Bourne R, Wells G. Viscosupplementation for the treatment of osteoarthritis of the knee. Cochrane Database Syst Rev. 2006;CD005321. doi:10.1002/14651858.CD005321.pub2
2. Yaftali NA, Weber K. Corticosteroids and hyaluronic acid injections. Clin Sports Med. 2019;38:1–15. doi:10.1016/j.csm.2018.08.006
3. Liu SH, Dube CE, Eaton CB, Driban JB, McAlindon TE, Lapane KL. Longterm effectiveness of intra articular injections on patient-reported symptoms in knee osteoarthritis. J Rheumatol. 2018;45:1316–1324. doi:10.3899/jrheum.171385
4. Bedard NA, DeMik DE, Glass NA, Burnett RA, Bozic KJ, Callaghan JJ. Impact of clinical practice guidelines on use of intra-articular hyaluronic acid and corticosteroid injections for knee osteoarthritis. J Bone Joint Surg Am. 2018;100:827–834. doi:10.2106/JBJS.17.01045
5. Weitoft T, Uddenfeldt P. Importance of synovial fluid aspiration when injecting intra-articular corticosteroids. Ann Rheum Dis. 2000;59:233–235. doi:10.1136/ard.59.3.233
6. Zhang Q, Zhang T. Effect on pain and symptoms of aspiration before hyaluronan injection for knee osteoarthritis: a prospective, randomized, single-blind study. Am J Phys Med Rehabil. 2016;95:366–371. doi:10.1097/PHM.0000000000000403
7. Conrozier T, Monfort J, Chevalier X, et al. EUROVISCO recommendations for optimizing the clinical results of viscosupplementation in osteoarthritis. Cartilage. 2020;11:47–59. doi:10.1177/1947603518783455
8. Bhadra AK, Altman R, Dasa V, et al. Appropriate use criteria for hyaluronic acid in the treatment of knee osteoarthritis in the United States. Cartilage. 2017;8:234–254. doi:10.1177/1947603516662503
9. Dooley P, Martin R. Corticosteroid injections and arthrocentesis. Can Fam Physician. 2002;48:285–292.
10. Smith MK, Lesniak B, Baraga MG, Kaplan L, Jose J. Treatment of popliteal (baker) cysts with ultrasound-guided aspiration, fenestration, and injection: long-term follow-up. Sports Health. 2015;7:409–414. doi:10.1177/1941738115585520
11. Jose J, Silverman E, Kaplan L. Symptomatic ganglion cyst of the popliteus tendon treated with ultrasound-guided aspiration and steroid injection: a case report. Sports Health. 2011;3:393–395. doi:10.1177/1941738111406223
12. Wang SZ, Wu DY, Chang Q, Guo YD, Wang C, Fan WM. Intra-articular, single-shot co-injection of hyaluronic acid and corticosteroids in knee osteoarthritis: a randomized controlled trial. Exp Ther Med. 2018;16:1928–1934. doi:10.3892/etm.2018.6371
13. Manfreda F, Rinonapoli G, Nardi A, Antinolfi P, Caraffa A, Fatal Sepsis A. Caused by hyaluronate knee injection: how much the medical history and the informed consent might be important? Case Rep Orthop. 2017;2017:1518401. doi:10.1155/2017/1518401
14. Daftary AR, Karnik AS. Perspectives in ultrasound-guided musculoskeletal interventions. Indian J Radiol Imaging. 2015;25:246–260. doi:10.4103/0971-3026.161445
15. Dodre E, Lefebvre G, Cockenpot E, Chastanet P, Cotten A. Interventional MSK procedures: the Hip. Br J Radiol. 2016;89:20150408. doi:10.1259/bjr.20150408
16. Lalam RK, Winn N, Cassar-Pullicino VN. Interventional articular and para-articular knee procedures. Br J Radiol. 2016;89:20150413. doi:10.1259/bjr.20150413
17. Holland C, Jaeger L, Smentkowski U, Weber B, Otto C. Septic and aseptic complications of corticosteroid injections: an assessment of 278 cases reviewed by expert commissions and mediation boards from 2005 to 2009. Dtsch Arztebl Int. 2012;109:425–430. doi:10.3238/arztebl.2012.0425
18. Aydin M, Arikan M, Togral G, Varis O, Aydin G. Viscosupplementation of the knee: three cases of acute Pseudoseptic Arthritis with painful and irritating complications and a literature review. Eur J Rheumatol. 2017;4:59–62. doi:10.5152/eurjrheum.2016.15075
19. Sinha MK, Mishra P, Mishra TS, Barman A. Aspiration and steroid injection in ganglion cysts: an ultrasound guided evaluation of the response. J Clin Orthop Trauma. 2019;10:S252–S257. doi:10.1016/j.jcot.2019.03.004
20. Kim JY, Chung SW, Kim JH, et al. Among compression plus nonsteroidal antiinflammatory drugs, aspiration, and aspiration with steroid injection for nonseptic olecranon bursitis. Clin Orthop Relat Res. 2016;474:776–783. doi:10.1007/s11999-015-4579-0
21. Liang T, Panu A, Crowther S, Low G, Lambert R. Ultrasound-guided aspiration and injection of an intraneural ganglion cyst of the common peroneal nerve. HSS J. 2013;9:270–274. doi:10.1007/s11420-013-9345-9
22. Kozar S, Jeromel M. Minimally invasive CT guided treatment of intraspinal synovial cyst. Radiol Oncol. 2014;48:35–39. doi:10.2478/raon-2013-0024
23. Kostanian VJ, Mathews MS, Guided CT. Aspiration of a cervical synovial cyst. Case report and technical note. Interv Neuroradiol. 2007;13:295–298. doi:10.1177/159101990701300310
24. Henrotin Y, Chevalier X, Raman R, et al. EUROVISCO guidelines for the design and conduct of clinical trials assessing the disease-modifying effect of knee viscosupplementation. Cartilage. 2020;11:60–70. doi:10.1177/1947603518783521
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.