")
Back to Journals » Research and Reports in Urology » Volume 15
Unilateral Testicular Infarction a Very Rare Complication of Genital Tuberculosis: A Case Report and Literature Review
Authors Issack FH , Bogale NT , Hassen SM, Ibrahim AI, Abdi AM, Bore TM, Answar IO
Received 5 August 2023
Accepted for publication 28 October 2023
Published 31 October 2023 Volume 2023:15 Pages 479—484
DOI https://doi.org/10.2147/RRU.S434046
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Guglielmo Mantica
Feysel Hassen Issack,1 Nahom Tadesse Bogale,1 Samater Mohammed Hassen,1 Abdulhafiz Idris Ibrahim,2 Abdurehman Mohamed Abdi,1 Tariku Mulatu Bore,3 Isak Omer Answar4
1Urology Unit, Department of Surgery, Jigjiga University Sheik Hassen Yabare Comprehensive Specialized Hospital, Jigjiga, Ethiopia; 2Department of Radiology, Jigjiga University Sheik Hassen Yabare Comprehensive Specialized Hospital, Jigjiga, Ethiopia; 3Department of Pathology, Jigjiga University Sheik Hassen Yabare Comprehensive Specialized Hospital, Jigjiga, Ethiopia; 4Department of Pathology, University of Gondar, College of Medicine and Health Sciences, Gondar, Ethiopia
Correspondence: Feysel Hassen Issack; Nahom Tadesse Bogale, Urology Unit, Department of Surgery, Jigjiga University Sheik Hassen Yabare Comprehensive Specialized Hospital, PO Box:1020, Jigjiga, Ethiopia, Tel +251932511145, Email [email protected]; [email protected]
Background: Genitourinary tuberculosis is the second most common form of extrapulmonary tuberculosis in developing countries. Isolated genital TB is rare, but testicular infarction is an unusual complication of delayed management, in which surgical intervention is warranted.
Case Presentation: A 29-year-old male non-smoker presents with painful left scrotal pain of 21 days. Initially managed with intravenous antibiotics, the disease progressed and resulted in testicular infarction. Left orchiectomy was performed, and the specimen was sent for histopathological examination, which revealed features consistent with a testicular tuberculous abscess.
Conclusion: Tuberculous epididymo-orchitis (TBEO) with testicular infarction was unusual. It is prudent to consider this in patients presenting with long-standing urinary symptoms, particularly in those unresponsive to the initial antibiotic therapy. It requires a high index of suspicion, especially in TB endemic areas.
Keywords: tuberculosis, acute scrotum, epididymo-orchitis, genitourinary tuberculosis, testicular infarction, orchiectomy
Introduction
Tuberculosis (TB) is a common cause of morbidity and mortality, worldwide. It is the most common cause of death owing to a single infectious agent.1 It is estimated that approximately 25% of the world’s population has contracted tuberculosis. The most affected individuals live in developing countries. Ethiopia has a high burden.2
Extra-pulmonary tuberculosis is a clinical presentation of tuberculosis involving organs other than the lungs. It is also a huge public health concern accounting for 15–20% of cases.2,3 In Ethiopia, it accounts for 30% of TB cases the lymph nodes, pleura, bone, and central nervous system being the common extra-pulmonary sites.2,4 Genitourinary TB accounts for 20–40% of EPTB. It is the second and third most common extrapulmonary site in developing and developed countries, respectively.5,6 Both urinary and genital organs will be involved in half of the cases, but isolated diseases of the genital organs are rare.5 The kidney is the most common site of GUTB with devastating morbidity, whereas male genital TB is a unique subset, with the epididymis and prostate being the most commonly affected genital organs.7 Genital TB other than TB epididymitis is rare, and few reports are available to guide its diagnosis and suggest its management.8
Here, we present a case of isolated unilateral left-sided TB epididymo-orchitis leading to testicular abscess and infarction after the patient presented with scrotal pain and swelling for 03 weeks duration which was refractory to initial antibiotics and later progressed to testicular abscess and infarction, for whom left-sided orchiectomy was performed, and the patient was discharged with Anti- TB chemotherapy.
Case Presentation
A 29-year-old male patient presented to a tertiary hospital with complicated epididymo-orchitis and testicular abscess from a private clinic. He initially presented with a three-day history of left testicular pain and swelling. The pain is vague and dull aching in type which is relieved with scrotal elevation and support. For which reason, he visited a private clinic and given intravenous antibiotics for five days with a diagnosis of acute epididymo-orchitis. Despite the antibiotic treatment the patient’s initial complaints worsened and later he visited our hospital. Otherwise, he had no fever, chills, or rigor. The patient had no history of urethral discharge or urinary complaints. He was married and had a monogamous sexual relationship with his wife. The patient had no trauma to the pelvis or genitalia. He had no recent or chronic cough, or contact with a chronic cough, anorexia, infertility, or significant weight loss. The patient had no past medical history of diabetes mellitus or hypertension. The patient was neither an alcoholic nor a smoker. Physical examination revealed a mildly tender left scrotum with normal-appearing scrotal skin and an enlarged, indurated left testicle. The Prehn’s sign was positive; otherwise, the cremasteric reflex remained intact. Initial laboratory test results (CBC and urine analysis, culture, serology, and AFB) were unremarkable. The patient was initially administered intravenous antibiotics (ceftriaxone, 1 g IV BID, for 02 weeks together with NSAIDs analgesics (Diclofenac) and scrotal elevation. Despite medical management, the patient’s complaints worsened and evolved into an abscess. Initial scrotal Doppler ultrasound showed post-infectious testicular infarction with a heterogeneous left testicle with hypoechoic and hyperechoic areas and no flow on color Doppler detected over the testicular parenchyma. The left testis was diffusely enlarged measuring 4.7×3.2 cm in size. Otherwise, no hydrocele, spermatic chord, or epididymal enlargement was noted, and the overlying skin has normal contour. The contralateral testis showed normal studies. (Figure 1).
 |
Figure 1 Scrotal Doppler ultrasound showing left testicular infarction with heterogeneous parenchyma and areas of hypoechoic and hyper-echoic changes with no color Doppler flow detected over testicular parenchyma. Diffusely enlarged testicle measuring 4.7×3.2 cm in size. Otherwise, no hydrocele, epididymal, or spermatic chord enlargement noted with normal studies on contralateral testicle. |
On subsequent physical examination, skin changes with induration small subcutaneous fluctuant mass were noted but no ulceration on left hemiscrotum and for these incision and drainage of the left testicular abscess was performed. The Intra-operative finding was adhesion between the left testicle and the overlying scrotal skin and approximately 05 mL of thick non-offensive pus was drained, with focal necrotic areas on the anterior surface of the left testicle (Figure 2A). The spermatic cord was normal, with no evidence of torsion. The wound was left open with a saline-soaked dressing to observe further changes in the testes. We followed up the patient in our inpatient urology ward with wound care on a twice-daily basis, scrotal elevation, and antibiotics for 72 hours. However, necrotic changes and discoloration of the left testis had progressed (Figure 2B). Repeat Doppler ultrasonography revealed testicular parenchymal infarction. For this reason, we performed left-sided orchiectomy after obtaining informed consent, and the sample was sent for pathological examination. The patient was admitted to the outpatient department with an uneventful clinical course. The pathology report revealed a testicular tuberculous abscess (Figure 3A and B), where the patient was linked to the TB clinic and administered anti-TB medications according to national guidelines. Chest radiography, which was unremarkable, was performed subsequently. The patient is currently taking anti-TB chemotherapy and on follow up without any further complaint from his initial presentation.
 |
Figure 2 Intraoperative pictures. (A) Doubtful viability of left testis on the first incision and drainage with purulent fluid on the kidney dish. (B) Progressive testicular gangrene after three days of conservative management. |
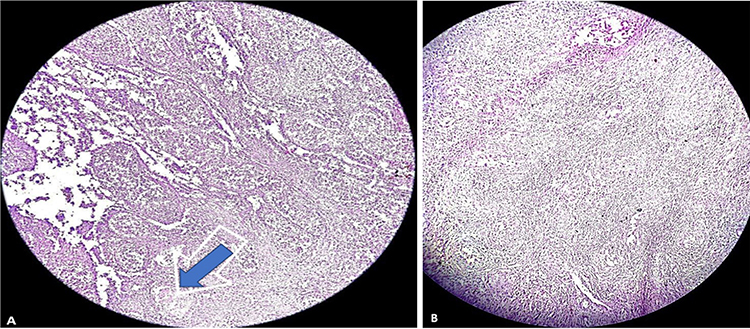 |
Figure 3 Pictures of the histopathology specimen slides. (A) Low power view showing nodular aggregates of epithelioid histiocytes (granuloma) with focus of necrosis at the center (indicated by the blue arrow). (B) Mononuclear inflammatory cells rimming the histiocytic aggregates. |
Discussion
Genitourinary system involvement is the second most common site of EPTB in developing countries.5 A study conducted in a single teaching hospital in Ethiopia reported GUTB as the fourth most common form of EPTB, following lymph node, abdominal, and pleural involvement.9 It attributes for 8–15% of all EPTB cases.7,10 Concomitant active PTB or history of previous PTB might be evident in approximately 56–87% of patients.10 Mutual involvement of both urinary and genital organs is reported in more than 50% of GUTB and isolated genital involvement is counted in 5–30% of cases, even though the number of organs involved in the disease process is dependent on the duration of the illness and the time it is diagnosed after acquisition of the bacterium.5–7
Kidney is most commonly affected by GUTB (80%), with pronounced frequency in immunodeficient and patients with other comorbidities.11
Isolated genital TB without evidence of kidney involvement is a rare condition that poses a challenge to diagnosis. The epididymis, prostate, seminal vesicles, testes, vas deferens, and penis have rarely been described under the umbrella of male genital TB. The epididymis and prostate are the most frequently affected organs.5,6,12,13
Implantation of the bacillus into genital organs mainly occurs through hematogenous deposition during early miliary spread (primary infection) or through lymphatic pathways. Sexual transmission has also been reported in rare cases of penile TB.5,6,12,14 The dissemination of the tubercle is again evident secondarily via local, direct spread from contagious infected organs through either the antegrade or retrograde route.14 Reactivation of latent tubercular infection in the genital organs occurs when the immune status of the patient wanes, with a latency period of 22 years, ranging from to 1–46 years.11
Isolated reactivation in genital organs results in isolated genital TB. Epididymis, due to its myriad of blood supply, is the most favorable site for genital TB, accounting for 27% of isolated genital TB cases. Single-focus reactivation in the epididymis is attributable to the majority of unilateral clinical cases, although multifocal and bilateral reactivation are also possible.5
Tuberculosis affecting testes is extremely rare, accounting for only 3% of male genital TB.7,13,15 Testicular involvement is typically secondary to TB epididymitis.6 Since there is a tight non-permeable blood-test barrier, metastatic blood-borne inoculation of the tubercle is uncommon and spreads directly from the infected contagious epididymis.5 Therefore, it is unusual to identify isolated testicular TB. It is common in areas where tuberculosis is epidemic and mostly attacks middle-aged males in their third and fourth decades of life.10
Patients have a wide variety of presentations, making the diagnosis difficult. The majority of cases present with painless or painful scrotal masses, bilateral involvement one-third of the time, and in more advanced disease, abscess and sinus formation is noted.5 The presence of an abscess or sinus might indicate progression to a severe form of epididymo-orchitis.16 There may also be irritative lower urinary tract symptoms, such as dysuria, frequency, or urgency.7,12 The presence of constitutional symptoms of pulmonary TB or a history suggestive of active or chronic TB is important, although uncommon, in consideration of possible genital TB. In the absence of such history, consideration of possible tuberculous epididymo-orchitis requires a high index of suspicion.
Clinical examination of patients with genital TB requires examination of the kidneys and lungs to rule out synchronous infections of these organs.6 Chest radiographic findings were remarkable in half of the patients. Abnormal urine analysis is evident in 77–90% of cases with urogenital TB.6,12 Hematuria and pyuria were detected in 79.7% and 67.1% of patients, respectively.12 Due to paucity of the bacilli in the urine, the yield from urine smears is less than 40%.17 Likewise, the yield from urine AFB culture is low, although it was previously considered the gold standard, and the absence of growth of bacilli on culture medium does not rule out tuberculosis.6,12 However, rapid microbiological diagnostic tests such as Gene X-pert have a relatively higher sensitivity than urine microscopy and culture.5,12
Ultrasound is the best initial modality for the diagnosis of scrotal pathologies. It differentiates possible differentials such as malignancy, testicular torsion, and epididymitis. Ultrasound also has the ability to detect complications, such as abscesses and infarctions, especially with Doppler studies. Ultrasound findings of TB epididymo-orchitis depend on the pathological stage of disease progression and are classified as follows: 1) diffusely enlarged, heterogeneously hypoechoic, 2) diffusely enlarged, homogenously hypoechoic, 3) nodular enlargement, heterogeneously hypoechoic, and 4) miliary.18 Other features, such as smooth peripheral calcifications, scrotal wall thickening, and hydrocele have also been reported to suggest tuberculosis. However, Ultrasound is non-specific, and cross-sectional studies using MRI are recommended in some equivocal scenarios. MRI has an added benefit of better definition of anatomy, soft tissue enhancement and ruling out other potential differential diagnoses.
Pathological examination and culture with isolation of mycobacteria are the gold standard confirmatory tests for TB diagnosis. The specimen to be tested was acquired either through fine-needle aspiration or biopsy (FNAC/B), or through surgical biopsy.7 FNAC can provide a histological diagnosis when a clinical and radiological suspicion of malignancy is unlikely. The presence of epithelioid cell granuloma with multinucleate giant cells and caseation is diagnostic,5 even though there is no consensus on its use since others are arguing against the probability of increasing the risk of needle site inoculation and fistula formation.12,17
The medical management is similar to that of pulmonary TB. It involves anti-tuberculosis chemotherapy for a total of six months.2,3 Medical treatment is sufficient if an early diagnosis is made and may prevent unnecessary orchiectomy.
In a retrospective study of 81 cases, it was reported that anti-TB chemotherapy alone could not effectively control scrotal lesions, and complications, including hydrocele, abscess, and sinus, were observed in 13 patients (16%) requiring radical surgery.12 In some equivocal cases, surgery is unavoidable when it is difficult to diagnose or unresponsive to antibiotic treatment. They also recommended triple therapy with sandwich radical surgery and pre- and postoperative anti-tuberculosis pharmacotherapy as effective management methods. Abscesses that do not respond to chemotherapy and a firm swelling that has remained unchanged or has slowly increased in size despite the use of antibiotics and anti-tuberculous chemotherapy are general indications for surgical management.19 Epididymectomy, orchiectomy, and epididymo-orchiectomy are surgical options that can be performed for advanced TB epididymo-orchitis, and the latter is the best option to completely eradicate lesions because TB orchitis is usually secondary to epididymitis.12
Our patient presented with painful swelling of the left testis, which was unresponsive to empirical antibiotic therapy, and progressed to develop testicular abscess, scrotal skin induration, and later testicular infarction, which is the natural course of the delayed severe form of TB epididymo-orchitis. The absence of concomitant pulmonary symptoms, normal laboratory examinations, and chest imaging with an initial ultrasound suggestive of infectious epididymo-orchitis necessitates antibiotic therapy considering the usual etiologies of bacterial epididymo-orchitis. We diagnosed Tuberculous Epididymo-orchitis (TBEO) based on histopathological examination of the orchiectomy specimen. Surgical treatment was inevitable in our patient because the disease progressed to abscess formation and infarction.
Conclusion
TBEO with testicular infarction is an unusual presentation. It is prudent to consider this in patients presenting with long-standing urinary symptoms, particularly in those unresponsive to the initial antibiotic therapy. This requires a high index of suspicion, particularly in highly endemic areas. Early diagnosis and medical management can help to avoid unnecessary surgical intervention. Since the diagnosis is often delayed due to non-specific symptoms and late patient presentation with complications such as abscess, sinus tracts with scrotal skin involvement and ulceration, and rarely with testicular infarction and necrosis, surgical intervention is unavoidable.
Abbreviations
EPTB, Extra-pulmonary Tuberculosis; FNAC, Fine Needle Aspiration Cytology; GUTB, Genito-Urinary Tuberculosis; HIV, Human Immunodeficiency Virus; MRI, Magnetic Resonance Imaging; PTB, Pulmonary Tuberculosis; TB, Tuberculosis; TBEO, Tuberculous Epididymo-orchitis.
Data Sharing Statement
All the generated data are included in this article.
Ethics Approval and Consent to Participate
No institutional review board approval was required.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent form is available for review by the Editor-in-Chief of this journal upon request.
Funding
The authors received no funding for this work.
Disclosure
The authors have no competing interests in this work.
References
1. World Health Organization. Global Tuberculosis Report. Geneva: World Health Organization; 2021.
2. Federal Ministry of Health, Ethiopia. Guidelines for Clinical and Programmatic Management of TB, TB/ HIV, DR-TB and Leprosy in Ethiopia. Addis Ababa, Ethiopia; 2021.
3. Assefa GT, Girum, Asfaw TZ, Isolated epididymal tuberculosis: case report and review of literature. Int J Sci Rep. 2022;8:231–235. doi:10.18203/issn.2454-2156.IntJSciRep20221837
4. Alehegn E, Gebreyohanns A, Berhane B, et al. Burden of Mycobacterium tuberculosis and Associated Factors among Presumptive Extra pulmonary Tuberculosis Patients from Selected Health Facilities, Addis Ababa, Ethiopia. IJID Regions. 2023;1(7):199–205. doi:10.1016/j.ijregi.2023.03.007
5. Yadav S, Singh P, Hemal A, Kumar R. Genital tuberculosis: current status of diagnosis and management. Transl Androl Urol. 2017;6(2):222. doi:10.21037/tau.2016.12.04
6. Kulchavenya E, Kim CS, Bulanova O, Zhukova I. Male genital tuberculosis: epidemiology and diagnostic. World J Urol. 2012;30:15–21. doi:10.1007/s00345-011-0695-y
7. Mehboob K, Madani TA. Isolated tuberculous orchitis presented as epididymo-orchitis: an unusual presentation of tuberculosis. Urol Ann. 2022;14(2):189. doi:10.4103/ua.ua_12_21
8. Mohamed Alı A, Doğan A, Ali MA, Çakmak BS. Testicular Tuberculosis: two Rare Case Report. Int Med Case Rep J. 2023;16:339–343. doi:10.2147/IMCRJ.S408874
9. Arega B, Mersha A, Minda A, et al. Epidemiology and the diagnostic challenge of extra-pulmonary tuberculosis in a teaching hospital in Ethiopia. PLoS One. 2020;15(12):e0243945. doi:10.1371/journal.pone.0243945
10. Das A, Batabyal S, Bhattacharjee S, Sengupta A. A rare case of isolated testicular tuberculosis and review of literature. J Family Med Primary Care. 2016;5(2):468. doi:10.4103/2249-4863.192334
11. Figueiredo AA, Lucon AM, Gomes CM, Srougi M. Urogenital tuberculosis: patient classification in seven different groups according to clinical and radiological presentation. Int Braz J Urol. 2008;34(4):422–432. doi:10.1590/S1677-55382008000400004
12. Huang Y, Chen B, Cao D, Chen Z, Wei Q. Surgical management of tuberculous epididymo-orchitis: a retrospective study of 81 cases with long-term follow-up. Infect Dis. 2021;21:1–8.
13. Mohamed Alı A, Doğan A, Ali MA, Çakmak BS. Testicular tuberculosis: two rare case reports. Int Med Case Rep. 2023;31:339–343. doi:10.2147/IMCRJ.S408874
14. Duchek M, Winblad B. Experimental male genital tuberculosis: the possibility of lymphatic spread. Urol Res. 1973;1:170–176. doi:10.1007/BF00256619
15. Tahaineh S, Mughli RA, Seetan K. Tuberculous peritonitis post orchiectomy for testicular tuberculosis: a case report and literature review. Radiol Case Reports. 2023;18(3):1084–1087. doi:10.1016/j.radcr.2022.12.011
16. Garbyal RS, Gupta P, Kumar S, et al. Diagnosis of isolated tuberculous orchitis using fine-needle aspiration cytology. Diagn Cytopathol. 2006;34(10):698–700. doi:10.1002/dc.20538
17. Kharbach Y, Retal Y, Khallouk A. Is orchiectomy avoidable in testicular tuberculosis mimicking malignancy? A case report. Af J Urol. 2021;27(1):1–5. doi:10.1186/s12301-021-00244-9
18. Muttarak M, Peh WC, Lojanapiwat B, Chaiwun B. Tuberculous epididymitis and epididymo-orchitis: sonographic appearances. Am J Roentgenol. 2001;176(6):1459–1466. doi:10.2214/ajr.176.6.1761459
19. Cek M, Lenk S, Naber KG, Grabe M. EAU guidelines for the management of genitourinary tuberculosis. Eur Urol. 2005;48(3):353–362. doi:10.1016/j.eururo.2005.03.008
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.