")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Tribute to the Flute: A Literature Review of Playing-Related Problems in Flautists
Authors Winkler S , Lohs A, Zinn-Kirchner ZM , Alotaibi M , Caffier PP
Received 5 November 2023
Accepted for publication 1 February 2024
Published 14 February 2024 Volume 2024:17 Pages 649—671
DOI https://doi.org/10.2147/JMDH.S448301
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Silvia Winkler,1,2 Anne Lohs,2 Zahavah M Zinn-Kirchner,1,2 Moonef Alotaibi,2,3 Philipp P Caffier1,2
1Berlin Center for Musicians Medicine (BCMM), Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, D-10117, Germany; 2Department of Audiology and Phoniatrics; Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, D-10117, Germany; 3King Fahad Medical City, Department of Otorhinolaryngology, Head and Neck Surgery, Riyadh, Kingdom of Saudi Arabia
Correspondence: Philipp P Caffier, Department of Audiology and Phoniatrics, Berlin Center for Musicians Medicine, Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Campus Charité Mitte, Charitéplatz 1, Berlin, D-10117, Germany, Tel +4930 450 655 097, Fax +4930 450 555 931, Email [email protected]
Abstract: Playing musical instruments places unusually high demands on specific parts of the human body. Relative to the instruments they play, musicians may experience instrument-related symptoms, as recorded in flute players. The objective was to provide an overview of the study findings addressing medical problems in flautists to better understand their complaints and pave the way for more personalized healthcare. Several electronic databases (PubMed, Embase, Cochrane Library) were systematically searched in July 2022. Furthermore, the references of all included articles were reviewed for additionally relevant sources. The resulting set of studies was summarized in a table, with quality assessment according to the SIGN grading system. From an initial 433 hits, the search yielded 95 studies with a total of 32,600 musicians, including at least 2134 flautists. Among the latter, evidence was found for musculoskeletal, neurological, dermatological, temporomandibular, and hearing complaints, overuse and reflux symptoms, velopharyngeal insufficiency, as well as upper and lower airway impairment. Other specialists may be consulted equally often and should be sensitive to the particular medical problems in flautists. Future studies would ideally contain specific outcome analyses on an international scale and consider flautists as an individual subgroup within a larger number of total participants.
Keywords: flautists health, instrument-associated disease, music pathology, occupational medicine, playing-related injuries, musico-medical care, performing arts medicine
Introduction
Playing music, whether it be at a recreational or professional level, requires complex sequences of sensorimotor precision, especially within the auditory system.1 Pathologies that occur here may lead to considerable discomfort in musicians and in severe cases endanger their professional careers. Musicians of all instrumental groups may be afflicted, though there are certain pathologies that occur more commonly among certain instrument-players.2
As instrument lessons often begin in early childhood, students as young as 5 years of age may be at risk of developing instrument-related complaints.3 Whilst musculoskeletal issues are the most prevalent, pathologies may require treatment from a plethora of specialties.4 These may not only affect the ability of the musician to perform, by reducing playing time or causing missed performance opportunities, but may also have a significant impact on the personal lives of those affected, resulting in both a loss of identity and jeopardizing livelihoods.5,6
The path toward developing physical, pain-related disorders in musicians is multifactorial. Postural misalignment, improper technique, intensity and type of practice, discrepancies between instrument size and player body size, stress, lack of conditioning, and lifestyle changes may contribute.7,8 The strain a specific instrument exerts on the body is largely related to the place of greatest muscular effort, as reflected in the prevalence and localization of the pathologies we observed while conducting this review.9–12 In woodwind musicians, such as flautists, this is frequently caused by static strain as well as repetitive finger movements.13,14 The instrument-related complaints in this paper refer to the various medical problems associated with flute playing. Within this review, ‘flautists’ will be used to describe transverse flute, piccolo, and recorder players.
When practicing and playing the flute, there is constant contact between the instrument and the musician’s skin, albeit with variable intensities. Apart from the aggravation of predisposed skin diseases, certain dermatological symptoms may develop directly as a result of playing a musical instrument.15 Flautists may further complain of neurological deficits such as nerve compression syndromes,16–19 and musicians’ dystonias,20–29 among others. Musicians may be equally predisposed to larger- and smaller-scale pathologies. Mild symptoms may be perceived with heightened sensitivity, as a result of digital and auditory acuity. Wind instrument players specifically may belong to a class susceptible to orofacial changes, due to the intense demands on facial and jaw muscle activity.9,23,30
The hearing ability of musicians is a crucial element of their professional lives and performing capacity.31 The volume produced by the player’s own instrument contributes significantly to sound exposure, which places musicians at a variable risk of hearing damage, depending on their primary instrument.1 Furthermore, musicians often fail to acknowledge pain that occurs during or after playing.11,13,30,32,33 Affected individuals habitually attempt to continue performing everyday activities despite injuries or overuse syndromes and feel seeking medical support would be a sign of an inability to cope with the associated difficulties of professional musicianship. Overuse syndromes of the upper limbs are particularly common in musicians.34 In flautists, overuse injuries and syndromes can occur in various areas of the body involved in flute playing, though they may be most prevalent in the musculoskeletal and respiratory systems. Denial and trivialization of early symptoms may predispose the affected individuals to chronification.35,36
The flute is a member of the woodwind family. This literature review will focus mainly on the transverse flute. The structure of transverse flutes can be seen in Figure 1.
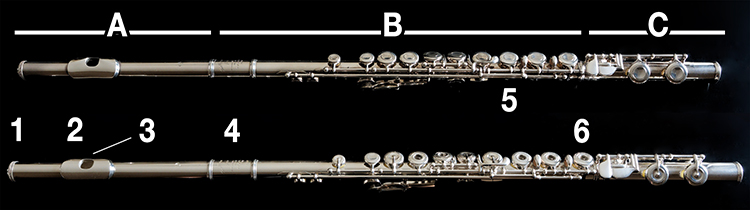 |
Figure 1 Structure and components of transverse flutes: A, head joint; B, body; C, foot joint; 1, crown; 2, lip plate; 3, embouchure hole; 4, barrel; 5, closed key; 6, ring key. Above: Muramatsu GX with full silver head and body, silver-plated closed keys, and Reform Embouchure. Below: Muramatsu DS full silver flute with ring keys and traditional mouthpiece. |
The transverse flute, as the name implies, is held across the body and is positioned dominantly over the right side. Both of the musician’s hands are used to operate the holes and to support and position the flute against the mouth. This inherently requires an asymmetrical posture with extreme angulation of the wrist and fingers. The center of mass is not in line with the central axis of the flute, which the fingers must artificially hold in alignment. At the same time, repetitive movements of the fingers are performed at high speeds and with extreme demands on precision and timing.37 When playing the flute, the player changes the amount of air blown into the headjoint of the flute by varying the mouth opening and by contracting their abdominal and respiratory muscles, resulting in approximately five liters of airflow through the instrument per second.38 Figure 2 shows the position of the transverse flute and the body posture while playing.
 |
Figure 2 Position of the transverse flute and typical posture of the upper body, arms, fingers, head and lips while playing. The person in this figure has provided written informed consent for the image to be published. |
The aim of this narrative literature review is to provide an overview of the health problems associated with flute playing as recorded in the current literature in order to better understand common complaints and pave the way for more personalized healthcare. It attempts to answer the following questions: what long-term effects may arise from playing the flute, and which health problems are prevalent among flautists.
Materials and Methods
To identify primary studies, the databases MEDLINE (via PubMed), EMBASE (via Ovid), and Cochrane Library were systematically examined (author SW and AL) between July 17th and 20th, 2022. A structured search strategy was developed that included free-text terms. Using these search terms, all similar and synonymous terms were automatically included. The databases were searched for the occurrence of the following keywords anywhere in the text:
(“flute” OR “flutes” OR “flautist*” OR “flutist*” OR “woodwind*” OR “wood-wind*” OR “wood wind” OR “wood winds”) AND (“injur*” OR “pain*” OR “damage*” OR “disorder*” OR “trauma*” OR “problem*” OR “distress” OR “overuse*” OR “discomfort” or “condition*” OR “disab*”)
All entries published before July 20th, 2022 were considered. No limits for publication date, language, study type or other criteria were applied. All study types, except systematic reviews and dissertations, were included. The studies in which the number of participating flautists was not explicitly stated were included if it could be reasonably assumed that the flautists participated in the study. For this reason, studies had to include the words “flute” or “flutist” or “flautist” or “recorder” or “piccolo” somewhere in the text to be included. The word “woodwind” or “wood-wind” was not sufficient. There were no age restrictions. English-, German-, Slovak- and Czech-language articles were included. Articles about health problems of flautists that did not occur in conjunction with their flute-playing (ie, accidents during other activities, congenital maladies) were not included.
An Excel spreadsheet was prepared with pre-filled fields for author, study design (Level of Evidence), number of participants, number of flautists, instrument-related complaints and type of flute played as mentioned by the authors. The articles were read through, and the fields in the table were completed to the extent possible. After the initial data collections, the articles were read a second time, and the table was checked for completeness and accuracy. To clarify the significance of the studies regarding flautists’ complaints, the number of flautists was also reported as a percentage of total participants whenever possible. Because only a few studies reported exclusively on flautists, the table indicated to which participants the complaints referred. The SIGN grading system’s levels of evidence (LoE) were used to assess the quality of the included studies.39 The levels rank studies according to the likelihood of bias.
This study is a review of published articles, not including any personal information such as patient names, social security numbers, addresses, or phone numbers. Because there are no ethical issues, this study did not require an institutional review board review. The information published in this manuscript is in compliance with the Charité Ethics Committee’s regulations.
Results
Altogether 433 studies were compiled through the initial database search:
- MEDLINE (via PubMed): 214 hits (48 potentially relevant, 25 included)
- EMBASE (via Ovid): 166 hits (47 potentially relevant, none included)
- Cochrane Library: 53 hits (2 potentially relevant, none included).
Ninety-seven of these studies were considered to be potentially relevant based on the title or abstract. Full-text articles were obtained and evaluated for meeting the inclusion criteria. Duplicates were filtered out. The bibliographies of the 25 included publications were reviewed for any further studies. Articles obtained in this manner were subjected to the same inclusion and exclusion criteria as the ones from the database search. This process was repeated until no additional studies could be identified. As a result, 70 further studies could be added to our compendium. A flowchart of the steps in our search with the number of publications found and included in this review is shown in Figure 3.
 |
Figure 3 Flowchart of the search strategy showing the number of publications found and included in the literature review. |
Our findings included 95 papers, with over 32,600 participants, of whom at least 2134 were flautists. The exact number could not be determined, as not all of the papers contained this information. Table 1 summarizes the main characteristics of the studies and their participants, including the LoE classification. Because of the small number of flautists in the study groups, the number of flautists was also reported as the percentage of total participants. The specialty-dependent complaints and pathologies are briefly summarized below.
 |
Table 1 Overview of Included Studies |
Musculoskeletal Complaints
Complaints of the musculoskeletal system, particularly the upper extremity and hand, have been found to be of importance in numerous epidemiological studies. There were six authors who addressed musculoskeletal complaints specifically in flautists.7,40–44 Ackermann, Fortune and Kenny were able to demonstrate that in a group of 20 flautists, 95% of the respondents suffered from issues connected to the musculoskeletal system.40,41 Most of the complaints (63%) persisted for more than three months.
Lonsdale et al showed that close to half (49.7%) of the participants experienced flute-playing-related musculoskeletal issues affecting their performance, and over a quarter (25.8%) were forced to take an “extended break” from playing (not further specified).7
Some studies suggest that playing with an asymmetrical and/or elevated position of the arms may lead to upper body musculoskeletal symptoms.7,13,32,43,45
Five studies addressed joint hypermobility.43,44,46–48 Larsson et al showed that joint hypermobility can either limit the impact of musculoskeletal issues or conversely exacerbate them, depending on whether the hypermobility occurs in joints directly involved in intense repetitive movements or in the supporting apparatus.46 Flautists tend to be hypermobile in the joints directly involved in playing the instrument, when applying the Beighton scale, though no large differences could be detected in the static joints as compared to the general population.43
With regard to musculoskeletal complaints, existing studies suggest a point prevalence of at least 60% among flautists.5,11,33,35,49,50 Figure 4 shows postural deformity with shoulder misalignment and symptomatic muscular imbalances in an amateur flautist presenting at our Berlin Center for Musicians Medicine.
 |
Figure 4 Postural deformity with shoulder asymmetry, recurrent tightness and pulling in the playing-associated higher left shoulder in a 63-year-old amateur flautist. History of 54 years of transverse flute playing and >30,000 cumulative practice hours (max. 2h/day). |
Overuse
Overuse syndrome/repetitive strain injury was reported by 5 studies.13,37,70–72 Overuse is a collective term for symptoms associated with activities that exceed the biological limits of the affected tissue. Newmark and Lederman established a link between the significantly increased playing time and overuse, resulting in newly acquired playing-related problems.71 Seventy-two percent of the musicians participating in the study reported overuse, the majority of whom had more than doubled their playing time over a four-week period.
Fry and Rowley conducted a case–control study among 7–19-year-old students.70 The proportion of music school students that experienced pain was significantly higher than in the non-music school, 71% as compared to 50%. Pain in the music school was primarily reported in conjunction with playing, whereas the other mentioned complaints after playing sports and writing. While music students reported long hours of practice, intensity appears to be more important than the duration of practice in the severity of pain experienced. A total of 11 flautists participated in the study, 82% of which were found to have playing-related pain due to overuse syndromes. In another cross-sectional study of 485 orchestral musicians, including 93 woodwind players, a painful overuse syndrome appeared in 64% of players.13
Neurological Complaints
Orofacial dystonia is one of the activity-specific dystonias that affects the muscles controlling airflow into the mouthpiece of a wind instrument. This review presents 6 case studies that described embouchure dystonia in flautists.20,22,23,27–29
There were also 6 studies about focal dystonia/occupational cramp.20,21,24–26,29 Altenmüller et al came to the conclusion that the left upper limb is affected most severely in flautists.26
Lederman conducted a case study of 17 participants, including 2 flautists, on thoracic outlet syndrome that presented with symptoms of pain and paresthesia, predominantly present in the forearm, wrist, and fingers, that worsened in certain positions and movements performed while playing.19
In their study, Wainapel and Cole presented 2 cases of entrapment of the distal ulnar nerve at the wrist in Guyon’s canal in flautists.16 In both cases, the left hand was affected, and the left wrist was held in dorsal flexion and radial deviation that resulted in nerval impingement.
Dermatological Complaints
Dermatological problems are addressed by 4 case studies.15,75–77 Inoue et al were able to show that eczema can develop as a result of playing a metallic flute due to the contents of its alloys – specifically nickel – in areas where the flute is in contact with the body and saliva is present.76 Another case of nickel-induced issues was documented by Freeman and Stephens and classified as cheilitis.77
A similar case of an acne-like rash in the chin area was presented by Dahl et al, though the type and composition of the flute was not specified.75 This condition receded after several weeks of rest from practice.
Hausen and Beinhauer reported of a 69-year-old music teacher who developed an allergy to cocobolo after playing a new “decorative” recorder.15
Reflux Symptoms
A cross-sectional study by Cammarota et al tallied gastro-oesophageal symptoms that occurred during a one-year period in 1083 orchestral musicians, including 414 woodwind players.38 Reflux symptoms were observed significantly more frequently among wind instrumentalists than in the control group consisting of musicians of other specialties. Significantly adjusted Prevalent Rate Ratio (PRR) for heartburn (PRR 1.69, 95% CI 1.30–2.20) and belching (PRR 1.64, 95% CI 1.29–2.09) were found in flautists, in reference to the controls.
Temporomandibular Complaints
Temporomandibular complaints affect the masticatory muscles and temporomandibular joints, or structures associated with them. Four cross-sectional publications with these endpoints were included in this review.2,9,10,30 A total of 2657 participants were involved, including 371 woodwind players and 87 flautists.
Steinmetz et al found orofacial pain to be significantly more frequent in flautists specifically, compared to other types of musicians used as a baseline.2
Similar conclusions were also reached by van Selms et al.9 Jang et al,10 and Gloria et al,30 who reported that wind players may be prone to orofacial changes, due to the intense demands on facial and jaw muscle activity.
Hearing Complaints
Hearing problems were investigated in 20 cross-sectional studies, including a total of at least 5326 participants, 237 of whom were flautists.1,31,78–95 All of the participants were orchestral musicians, save for 2 studies in which professionals were distinguished from players in other capacities.85,86 These studies suggested that exposure thresholds are strongly dependent on the instrument played and the position in the orchestra. To varying degrees, other studies showed flautists experiencing hearing damage.1,31,78–84,87–95 Exposure levels for flautists ranged from 78.1 to 98 dB(A) and from 85.0 to 112 dB(A) for woodwind players. The studies posited that flautists were exposed to noise levels in excess of the “upper exposure action level” of 85 dB(A) and thus at risk of hearing damage.
In contrast, two studies showed different results with regard to hearing function. Lee et al could not prove an elevated risk for hearing damage, calculating Lex values at 81.8 dB(A), which describe the normalized yearly noise exposure level (equivalent to a daily work period of 8 hours). These values were below the danger zone, although the noise exposure for flautists (87.4–92.1 dB(A)) exceeded the upper exposure limit of 85 dB(A).80 Kähäri et al could not attribute severe hearing losses to exposure to musical noise.90 However, percussion and woodwind players displayed slightly worse hearing thresholds than did other musicians.
Figure 5 shows inner ear hearing loss on the right side in a flautist presenting at our Berlin Center for Musicians Medicine.
 |
Figure 5 Sensorineural hearing loss in the right inner ear with chronic tinnitus aurium in a 53-year old professional flautist. History of 42 years of transverse flute-playing and > 60,000 cumulative practice hours (average 4h/day). Above: Pure-tone audiometry with right-sided noise induced c5-dip (ie, 4 kHz loss) caused by asymmetric long-term postural exposure to higher loudness levels of own instrument. Below: Transitory evoked otoacoustic emissions (TEOAE) with evidence of damage to the outer hair cells. |
Velopharyngeal Insufficiency (VPI)
Schwab and Schultze-Florey studied the connection between intraoral pressures developed while playing and the development of velopharyngeal insufficiency and its triggering factors (ie, colds and stress).96 Of the 148 brass and woodwind musicians included in the study, 24 showed symptoms of VPI. The pressure that is normally produced when playing in comfortable ranges was low for flute and piccolo players (1 to 6 mmHg and 2 to 9 mmHg respectively), compared to other groups, which may explain why they were not as heavily affected.
Malick et al conducted a cross-sectional study on brass and woodwind musicians using questionnaires.97 They concluded that nearly 34% of the musicians had experienced nasal air leaks and/or nasal sounds, defined by the authors as symptoms of stress velopharyngeal incompetence (SVPI). It is unclear if the 23 responding flautists were affected. Malick et al suggested a connection between SVPI and elevated oral pressure while playing, similarly to Schwab and Schultze-Florey in VPI.
Upper Airway Function
Laryngopharyngeal diverticula are the result of constant elevation of pressure while playing and can be classified as an “occupational overuse syndrome”. Costa and Alvite examined 22 professional wind instrumentalists by videofluroscope.98 They discovered that all of the study participants, including 2 flautists, had asymptomatic lateral laryngopharyngeal diverticula in areas less able to withstand high pressures.
In a questionnaire-based cross-sectional study by Capellaro and Beber, symptoms of vocal tract discomfort affecting the players’ quality of life were investigated.99 The most common complaints were dryness, ache, and irritability. Nearly one-fourth of the participants were flautists, but the overall incidence and individual frequency of discomfort were not specified in this group.
Lower Airway Function
Plamenac et al examined the sputum of 30 participants and posited that chronic strain on the respiratory tract can cause various changes in bronchial epithelial tissues.101 Of the four flautists that participated, there were 3 cases of squamous metaplasia and one case of irritation of ciliated columnar epithelium, despite being asymptomatic.
Deniz et al compared the spirometric measurements of 34 wind instrument players, including 2 flautists, and 44 non-musicians.102 Surprisingly, all spirometric values measured in wind players were significantly diminished relatively to the control. To explain these findings, the authors hypothesized that a history of bronchial asthma or the presence of barotrauma while playing could be a causative agent. Instrument-specific measurements were not included in the results.
Discussion
The aim of this literature review was to provide an overview of existing publications on the medical problems and instrument-specific complaints in flautists. No restrictions regarding demographic data were used. Several studies showed that musculoskeletal,3–5,7,11,32,33,35,40–69 neurological,16–29,73,74 dermatological,15,75–77 and temporomandibular complaints,2,9,10,30 as well as reflux symptoms,38 may occur as a result of playing the flute. The literature also revealed evidence of hearing problems due to exceeding the exposure limit of 85 dB(A)1,31,78–95 and overuse as a result of small and precise, repetitive movements.13,37,70–72 Other common handicaps included upper and lower airway impairment.98–102 Studies examining VPI showed an increased incidence among woodwind players with higher intraoral pressure, though flautists were found to have comparatively lower pressures in this cohort.96,97 Due to the lack of specific instrument analysis in the original work, the prevalence of VPI in flautists could not be conclusively assessed. There are certainly further areas of expertise that could be relevant but have not yet been adequately researched. This review was only able to consider the information published in the studies included, using the in-/and exclusion criteria. Despite efforts to use the most sensitive search strategy possible, it cannot be guaranteed that all relevant publications on the topic were detected. Most of the articles included in this review were found in the bibliographies of other publications, as much of the literature on this topic was so old that a keyword search did not reveal it until further investigation. Other (non-medical) databases could be additionally searched to herald a wider swath of results.
During our search, the terms for instrument-related symptoms were neither well defined nor consistently used by publications. Symptoms were often the result of activities unrelated to playing the flute, which we attempted to exclude here. It is evident that there were differences among populations (eg, age, playing level), methods of data collection (questionnaires, interviews, retrospective review of patient charts), response rates (questionnaires), and even in the willingness to participate. This wide array of players, combined with the limited number of flautists specified in the studies, made it difficult to compare populations at times and could be improved upon in study designs by highlighting the unique nature of pathologies as they arise specifically in flautists.
Only a few authors provided in-depth documentation about flautists’ playing background and experience.17,18,23,24,27,53,54,58,74 The type of flute was explicitly mentioned in only a couple of investigations, e.g.,7,15,45,54,84,87,89,99,100 and otherwise had to be deduced from the context of the publication or study population. The inclusion of case studies allows for the possibility of individual, albeit rare issues, to be analyzed in addition to more commonly occurring pathologies.15–25,27–29,44,75–77,98,100,101 Other investigations involved a significant number of musicians but only a small number of flautists. It should also be noted that in some cohorts, musicians played multiple instruments, meaning that playing-associated complaints cannot be attributed to the flute alone. Another limitation is the grouping of instruments as a woodwind for example, as each category includes several types of instruments, with differences in playing posture and technique, and therefore different kinds of stresses on the musculoskeletal apparatus and other body systems.
Similar considerations apply to the study design. Comparative studies depend on observations and comparisons where correlations may not equal causation. The majority of investigations collected data using questionnaires. Selection bias is possible, as musicians may fear suffering consequences for sharing their physical complaints or comments about their experiences at work.103 In addition, one’s own experiences, management and coping with musculoskeletal or other symptoms may influence the decision to participate. Flautists who have previously experienced playing-related illness may be more willing to participate because they recognize the importance of taking their pathologies seriously. Differences in response and participation rates between studies (eg, 8.6% in Gasenzer et al35 vs 100% in the study by Fry and Rowley70) have implications for the representativeness and comparability of the results. All of these considerations must be made when interpreting the data in Table 1. Most listed studies were classified as LoE 3 (non-analytic studies, eg, case reports, case series) and LoE 2– (case control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causal) according to the SIGN grading system.39 Nevertheless, for several of the issues discussed, “low” levels of evidence are quite tolerable, eg, for cross-sectional prevalence surveys. Case reports, too, have low incidence rates by nature, while still maintaining their specificity.
One of the strengths of our literature review as compared to previous flute-related reviews is our multidisciplinary and comprehensive approach toward tallying health problems associated with flute playing. Our extensive table clearly presents the prevalent health problems among flautists, as a result of long-term playing. Although this review has helped to recognize the complexity of playing-related pathologies, much remains to be desired in terms of solution-based research.
In 2008, the Federal Ministry of Labor and Social Affairs in Germany released a statement listing the professions that may result in hearing loss, including professional musicians, stating that high-intensity frequencies produced during performances have the potential to cause long-term hearing deficits.104 This “Königstein Recommendation” concerns the assessment of occupational noise-induced hearing loss (occupational disease No. 2301) and was updated in 2020.105 Recognizing work-related illness among musicians, as in any other professional group, is a crucial step toward tracking epidemiological trends so as to be able to further preventative measures in the future.106 Delving into the specific pathologies that may arise, attempts have been made at outlining treatment options. In hearing loss specifically, some form of in- or over-ear protection may be useful, assuming it reduces the intensity of the sound waves, rather than the frequency of the tone while playing, to allow normal playing to continue.107–110
Musculoskeletal discomfort may be alleviated by implementing a thumb rest for the right hand that attaches to the instrument and reduces strain on the fingers, wrist, and muscles of the forearm by preventing longitudinal rotation of the flute.111 Other researchers have examined the efficacy of yogic breathing and flexibility exercises in relieving muscular tension and overall relaxation.112 In velopharyngeal insufficiency, an inferior-based pharyngeal flap may show promise, as it has in other patients with a cleft palate.113 Temporomandibular disjunction may be prevented by expanding diagnostic measures, such as implementing infrared thermograms or measuring the embouchure force.114
There are myriad other complaints individual musicians may experience, not all of which we were able to fully explore within the realms of this review. Kenny et al investigated music performance anxiety (MPA) in 20 skilled flute players.115 This study identified a robust predictive model of MPA that supports previous theories. Multiple, partially independent factors contributed to the experience of MPA during a skilled musical performance, including anxiety measures (trait anxiety, situational anxiety, fear of negative evaluation), the level of accomplishment achieved on one’s flute, the amount of practice time for the performance, and physiological measures (eg, EMG, heart rate). Recognizing not just physical but further mental obstacles while working in such a high-intensity environment are a decisive factor in providing comprehensive patient care.
Conclusion
To conclude, flute players can be affected by numerous pathologies as a result of their playing habits and performing environment. Regarding their treatment, performing arts medicine covers a wide field of medical maladies that may require differing degrees of specialist attention. Based on the research found in the studies reviewed, altering the playing and practice routine in flautists can prevent chronification of injuries that may arise from playing this instrument.
Several questions remain to be answered, one of which being whether or not it is possible to predict if a flautist will develop a pathology over time. Given the data compiled here, more cross-sectional and comparative studies in different populations would be needed, particularly taking into account nuances in gender, age, playing time and general health, in order to make appropriate assessments. Future, larger-scale investigations of pathologies in flautists, specifically, would aid researchers in compiling more relevant data, so as to be able to successfully treat a wider range of players.
Disclosure
The authors have no conflicts of interest, no financial relationships or any sources of funding to disclose for this work.
References
1. O’Brien I, Wilson W, Bradley A. Nature of orchestral noise. J Acoust Soc Am. 2008;124(2):926–939. doi:10.1121/1.2940589
2. Steinmetz A, Zeh A, Delank KS, Peroz I. Symptoms of craniomandibular dysfunction in professional orchestra musicians. Occup Med. 2014;64(1):17–22. doi:10.1093/occmed/kqt148
3. Burkholder KR, Brandfonbrener AG. Performance-related injuries among student musicians at a specialty clinic. Med Probl Perform Art. 2004;19(3):116–122. doi:10.21091/mppa.2004.3020
4. Fishbein M, Middlestadt S, Ottati V, Straus S, Ellis A. Medical problems among ICSOM musicians: overview of a national survey. Med Probl Perform Art. 1988;3:1–8.
5. Stanhope J, Milanese S, Grimmer K. University woodwind students experiences with playing-related injuries and their management: a pilot study. J Pain Res. 2014;7:133–148. doi:10.2147/JPR.S49620
6. Guptill C. The lived experience of working as a musician with an injury. Work. 2011;40(3):269–280. doi:10.3233/WOR-2011-1230
7. Lonsdale K, Laakso EL, Tomlinson V. Contributing factors, prevention, and management of playing-related musculoskeletal disorders among flute players internationally. Med Probl Perform Art. 2014;29(3):155–162. doi:10.21091/mppa.2014.3032
8. Cruder C, Soldini E, Gleeson N, Barbero M. Factors associated with increased risk of playing-related disorders among classical music students within the risk of music students (RISMUS) longitudinal study. Sci Rep. 2023;13(1):22939. doi:10.1038/s41598-023-49965-7
9. van Selms MKA, Wiegers JW, Meer HA, Ahlberg J, Lobbezoo F, Visscher CM. Temporomandibular disorders, pain in the neck and shoulder area, and headache among musicians. J Oral Rehabil. 2020;47(2):132–142. doi:10.1111/joor.12886
10. Jang JY, Kwon JS, Lee DH, Bae JH, Kim ST. Clinical signs and subjective symptoms of temporomandibular disorders in instrumentalists. Yonsei Med J. 2016;57(6):1500. doi:10.3349/ymj.2016.57.6.1500
11. Roset-Llobet J, Rosinés-Cubells D, Saló-Orfila JM. Identification of risk factors for musicians in Catalonia (Spain). Med Probl Perform Art. 2000;15(4):167–174. doi:10.21091/mppa.2000.4032
12. Rodríguez-Gude C, Taboada-Iglesias Y, Pino-Juste M. Musculoskeletal pain in musicians: prevalence and risk factors – a systematic review. Int J Occup Saf Ergon. 2023;29(2):883–901. doi:10.1080/10803548.2022.2086742
13. Fry HJ. Incidence of overuse syndrome in the symphony orchestra. Med Probl Perform Art. 1986;1(2):51–55.
14. Yang N, Fufa DT, Wolff AL. A musician-centered approach to management of performance-related upper musculoskeletal injuries. J Hand Ther. 2021;34(2):208–216. doi:10.1016/j.jht.2021.04.006
15. Hausen B, Beinhauer A. Cocobolo-Holzallergie bei einer Flötenlehrerin. Akt Dermatol. 2004;30(11):489–492. doi:10.1055/s-2004-825987
16. Wainapel S, Cole J. The not-so-magic flute: two cases of distal ulnar nerve entrapment. Med Probl Perform Art. 1988;3(2):63–65.
17. Cynamon KB. Flutist’s neuropathy. N Engl J Med. 1981;305(16):961.
18. Charness ME, Parry GJ, Markison RE, Rosegay H, Barbaro NM. Entrapment neuropathies in musicians. Neurology. 1985;35(4 Suppl 1):1.
19. Lederman RJ. Thoracic outlet syndromes. Med Probl Perform Art. 1987;2(3):87–91.
20. Brandfonbrener AG. Musicians with focal dystonia: a report of 58 cases seen during a ten-year period at a performing arts medicine clinic. Med Probl Perform Art. 1995;10:121–127.
21. Lederman RJ. Occupational cramp in instrumental musicians. Med Probl Perform Art. 1988;3:45–51.
22. Brandfonbrener AG, Robson C. A review of 111 musicians with focal dystonia seen at a performing artist’s clinic 1985–2002. Mov Disord. 2002;17(5):1135. doi:10.1002/mds.10319
23. Frucht SJ. Embouchure dystonia: a video guide to diagnosis and evaluation. J Clin Mov Disord. 2016;3(1):10. doi:10.1186/s40734-016-0035-x
24. Wilson FR, Wagner C, Hömberg V. Biomechanical abnormalities in musicians with occupational cramp/focal dystonia. J Hand Ther. 1993;6(4):298–307. doi:10.1016/S0894-1130(12)80331-0
25. Charness ME, Ross MH, Shefner JM. Ulnar neuropathy and dystonic flexion of the fourth and fifth digits: clinical correlation in musicians. Muscle Nerve. 1996;19(4):431–437. doi:10.1002/mus.880190403
26. Altenmüller E, Baur V, Hofmann A, Lim VK, Jabusch HC. Musician’s cramp as manifestation of maladaptive brain plasticity: arguments from instrumental differences. Ann N Y Acad Sci. 2012;1252(1):259–265. doi:10.1111/j.1749-6632.2012.06456.x
27. Frucht SJ, Fahn S, Greene PE, et al. The natural history of embouchure Dystonia. Mov Disord. 2001;16(5):899–906. doi:10.1002/mds.1167
28. Frucht SJ. Embouchure dystonia: portrait of a task-specific cranial dystonia. Mov Disord. 2009;24(12):1752–1762. doi:10.1002/mds.22550
29. Lederman RJ. Focal dystonia in instrumentalists: clinical features. Med Probl Perform Art. 1991;6:132–136.
30. Glória JC, Balestra AA, Iasbik NS, Douglas-de-Oliveira DW, Flecha OD, Gonçalves PF. Prevalence of orofacial changes in wind instrumentalists: a cross-sectional pilot study in Brazil. Med Probl Perform Art. 2018;33(1):1–5. doi:10.21091/mppa.2018.1002
31. Rodrigues M, Freitas M, Neves M, Silva M. Evaluation of the noise exposure of symphonic orchestra musicians. Noise Health. 2014;16(68):40. doi:10.4103/1463-1741.127854
32. Wahlström Edling C W, Fjellman-Wiklund A. Musculoskeletal Disorders and asymmetric playing postures of the upper extremity and back in music teachers: a pilot study. Med Probl Perform Art. 2009;24(3):113–118. doi:10.21091/mppa.2009.3025
33. Guptill C, Zaza C, Paul S. An occupational study of physical playing-related injuries in college music students. Med Probl Perform Art. 2000;15(2):86–90. doi:10.21091/mppa.2000.2018
34. Bird HA. Overuse syndrome in musicians. Clin Rheumatol. 2013;32(4):475–479. doi:10.1007/s10067-013-2198-2
35. Gasenzer E, Klumpp M, Pieper D, Neugebauer E. The prevalence of chronic pain in orchestra musicians. Ger Med Sci. 2017;15:Doc01.
36. Stanhope J, Weinstein P. Should musicians play in pain? Br J Pain. 2021;15(1):82–90. doi:10.1177/2049463720911399
37. Fry HJH. Patterns of over-use seen in 658 affected instrumental musicians. Int J Music Educ. 1988;os-11(1):3–16. doi:10.1177/025576148801100101
38. Cammarota G, Masala G, Cianci R, et al. Reflux symptoms in wind instrument players. Aliment Pharmacol Ther. 2010;31(5):593–600. doi:10.1111/j.1365-2036.2009.04208.x
39. SIGN grading system 1999–2012 Edinburgh: Scottish intercollegiate guidelines network; 2023. Available from: https://www.sign.ac.uk/assets/sign_grading_system_1999_2012.pdf.
40. Ackermann BJ, Kenny DT, Fortune J. Incidence of injury and attitudes to injury management in skilled flute players. Work. 2011;40(3):255–259. doi:10.3233/WOR-2011-1227
41. Fortune J, Kenny DT, Ackermann BJ. Performance-related musculoskeletal disorders in tertiary-level flute players and relationships with muscle tension and music performance anxiety. Med Probl Perform Art. 2007;22:175–176.
42. Spence C S. Prevalence rates for medical problems among flautists: a comparison of the UNT-musician health survey and the flute health survey. Med Probl Perform Art. 2001;16(3):99–101. doi:10.21091/mppa.2001.3017
43. Artigues-Cano I, Bird H. Hypermobility and proprioception in the finger joints of flautists. J Clin Rheumatol. 2014;20(4):203–208. doi:10.1097/RHU.0000000000000109
44. Patrone NA, Hoppmann RA, Whaley J, Chauncey B. Benign hypermobility in a flutist. Med Probl Perform Art. 1988;3:158–161.
45. Ramella M, Fronte F, Converti R. Postural disorders in conservatory students: the diesis project. Med Probl Perform Art. 2014;29(1):19–22. doi:10.21091/mppa.2014.1005
46. Larsson L, Baum J, Mudholkar G, Kollia G. Benefits and disadvantages of joint hypermobility among musicians. N Engl J Med. 1993;329(15):1079–1082. doi:10.1056/NEJM199310073291504
47. Dawson WJ. Upper-extremity Problems Caused by Playing Specific Instruments. Med Probl Perform Art. 2002;17(3):135–140. doi:10.21091/mppa.2002.3022
48. Shoup D. Survey of performance-related problems among high school and junior high school musicians. Med Probl Perform Art. 1995;10:100–105.
49. Kok LM, Groenewegen KA, Huisstede BMA, Nelissen RJ, Rietveld ABM, Haitjema S. The high prevalence of playing-related musculoskeletal disorders (PRMDs) and its associated factors in amateur musicians playing in student orchestras: a cross-sectional study. PLoS One. 2018;13(2):e0191772. doi:10.1371/journal.pone.0191772
50. Kok LM, Vlieland TPV, Fiocco M, Nelissen RG. A comparative study on the prevalence of musculoskeletal complaints among musicians and non-musicians. BMC Musculoskelet Disord. 2013;14(1):9. doi:10.1186/1471-2474-14-9
51. Manchester RA. The incidence of hand problems in music students. Med Probl Perform Art. 1988;3:15–18.
52. Bengtson KA, Schutt AH. Upper extremity musculoskeletal problems in musicians: a follow up survey. Med Probl Perform Art. 1992;7:44–47.
53. Knishkowy B, Lederman RJ. Instrumental musicians with upper extremity disorders: a follow-up study. Med Probl Perform Art. 1986;1:85–89.
54. Hochberg FH, Leffert RD, Heller MD, Merriman L. Hand difficulties among musicians. JAMA. 1983;249(14):1869–1872. doi:10.1001/jama.1983.03330380057027
55. Cayea D, Manchester RA. Instrument-specific rates of upper-extremity injuries in music students. Med Probl Perform Art. 1998;13:19–25.
56. Manchester RA, Flieder D. Further observations on the epidemiology of hand injuries in music students. Med Probl Perform Art. 1991;6:11–14.
57. Wolff AL, Ling DI, Casey EK, Toresdahl BG, Gellhorn AC. Feasibility and impact of a musculoskeletal health for musicians (MHM) program for musician students: a randomized controlled pilot study. J Hand Ther. 2021;34(2):159–165. doi:10.1016/j.jht.2021.04.001
58. Brandfonbrener AG. Joint laxity and arm pain in a large clinical sample of musicians. Med Probl Perform Art. 2002;17(3):113–115. doi:10.21091/mppa.2002.3017
59. Britsch L. Investigating performance-related problems of young musicians. Med Probl Perform Art. 2005;20(1):40–47. doi:10.21091/mppa.2005.1007
60. Steinmetz A, Möller H, Seidel W, Rigotti T. Playing-related musculoskeletal disorders in music students-associated musculoskeletal signs. Eur J Phys Rehabil Med. 2012;48(4):625–633.
61. Sousa CM, Machado JP, Greten HJ, Coimbra D. Occupational diseases of professional orchestra musicians from northern Portugal: a descriptive study. Med Probl Perform Art. 2016;31(1):8–12. doi:10.21091/mppa.2016.1002
62. Ackermann B, Driscoll T, Kenny DT. Musculoskeletal pain and injury in professional orchestral musicians in Australia. Med Probl Perform Art. 2012;27(4):181–187. doi:10.21091/mppa.2012.4034
63. Steinmetz A, Seidel W, Muche B. Impairment of postural stabilization systems in musicians with playing-related musculoskeletal disorders. J Manipulative Physiol Ther. 2010;33(8):603–611. doi:10.1016/j.jmpt.2010.08.006
64. Nemoto K, Arino H. Hand and upper extremity problems in wind instrument players in military bands. Med Probl Perform Art. 2007;22(2):67–69. doi:10.21091/mppa.2007.2014
65. Nyman T, Wiktorin C, Mulder M, Johansson YL. Work postures and neck–shoulder pain among orchestra musicians. Am J Ind Med. 2007;50(5):370–376. doi:10.1002/ajim.20454
66. Stanek JL, Komes KD, Murdock FA. A cross-sectional study of pain among U.S. college music students and faculty. Med Probl Perform Art. 2017;32(1):20–26. doi:10.21091/mppa.2017.1005
67. Ranelli S, Straker L, Smith A. Playing-related musculoskeletal problems in children learning instrumental music: the association between problem location and gender, age, and music exposure factors. Med Probl Perform Art. 2011;26(3):123–139. doi:10.21091/mppa.2011.3021
68. Paarup HM, Baelum J, Holm JW, Manniche C, Wedderkopp N. Prevalence and consequences of musculoskeletal symptoms in symphony orchestra musicians vary by gender: a cross-sectional study. BMC Musculoskelet Disord. 2011;12(1):223. doi:10.1186/1471-2474-12-223
69. Kok LM, Haitjema S, Groenewegen KA, Rietveld ABM. The influence of a sudden increase in playing time on playing-related musculoskeletal complaints in high-level amateur musicians in a longitudinal cohort study. PLoS One. 2016;11(9):e0163472. doi:10.1371/journal.pone.0163472
70. Fry HJ, Rowley GL. Music related upper limb pain in schoolchildren. Ann Rheum Dis. 1989;48(12):998–1002. doi:10.1136/ard.48.12.998
71. Newmark J, Lederman RJ. Practice doesn’t necessarily make perfect: incidence of overuse syndromes in amateur instrumentalists. Med Probl Perform Art. 1987;2(4):142–144.
72. Hartsell HD, Tata GE. A retrospective survey of music-related musculoskeletal problems occurring in undergraduate music students. Physiother Can. 1991;43(1):13–18.
73. Newmark J, Hochberg FH. Isolated painless manual incoordination in 57 musicians. J Neurol Neurosurg Psychiatry. 1987;50(3):291–295. doi:10.1136/jnnp.50.3.291
74. Lederman RJ. Tremor in instrumentalists: influence of tremor type on performance. Med Probl Perform Art. 2007;22(2):70–73. doi:10.21091/mppa.2007.2105
75. Dahl MG. Flautist’s chin: a companion to fiddler’s neck. BMJ. 1978;2(6143):1023. doi:10.1136/bmj.2.6143.1023
76. Inoue A, Shoji A, Fujita T. Flautist’s chin. Br J Dermatol. 1997;136:147. doi:10.1111/j.1365-2133.1997.tb08778.x
77. Freeman S, Stephens R. Cheilitis: analysis of 75 cases referred to a contact dermatitis clinic. Am J Contact Dermat. 1999;10(4):198–200.
78. Jansen EJM, Helleman HW, Dreschler WA, de Laat JAPM. Noise induced hearing loss and other hearing complaints among musicians of symphony orchestras. Int Arch Occup Environ Health. 2009;82(2):153–164. doi:10.1007/s00420-008-0317-1
79. Laitinen HM, Toppila EM, Olkinuora PS, Kuisma K. Sound exposure among the Finnish national opera personnel. Appl Occup Environ Hyg. 2003;18(3):177–182. doi:10.1080/10473220301356
80. Lee J, Behar A, Kunov H, Wong W. Musicians’ noise exposure in orchestra pit. Appl Acoust. 2005;66(8):919–931. doi:10.1016/j.apacoust.2004.11.009
81. Qian C, Behar A, Wong W. Noise exposure of musicians of a ballet orchestra. Noise Health. 2011;13(50):51. doi:10.4103/1463-1741.74000
82. Schmidt JH, Pedersen ER, Juhl PM, et al. Sound exposure of symphony orchestra musicians. Ann Occup Hyg. 2011;55(8):893–905. doi:10.1093/annhyg/mer055
83. Royster DJ, Royster LH, Killion MC. Sound exposure and hearing thresholds of symphony orchestra musicians. J Acoust Soc Am. 1991;89(6):2793–2803. doi:10.1121/1.400719
84. Sabesky IJ, Korczynski RE. Noise exposure of symphony orchestra musicians. Appl Occup Environ Hyg. 1995;10(2):131–135. doi:10.1080/1047322X.1995.10389295
85. Axelsson A, Lindgren F. Hearing in classical musicians. Acta Otolaryngol. 1981;91(sup377):1–100. doi:10.3109/00016488109108191
86. Chesky K, Henoch MA. Instrument-specific reports of hearing loss: differences between classical and nonclassical musicians. Med Probl Perform Art. 2000;15(1):35–38. doi:10.21091/mppa.2000.1007
87. Emmerich E, Rudel L, Richter F. Is the audiologic status of professional musicians a reflection of the noise exposure in classical orchestral music? Eur Arch Otorhinolaryngol. 2008;265(7):753–758. doi:10.1007/s00405-007-0538-z
88. Ostri B, Eller N, Dahlin E, Skylv G. Hearing impairment in orchestral musicians. Scand Audiol. 1989;18(4):243–249. doi:10.3109/01050398909042202
89. McBride D, Gill F, Proops D, Harrington M, Gardiner K, Attwell C. Noise and the classical musician. BMJ. 1992;305(6868):1561–1563. doi:10.1136/bmj.305.6868.1561
90. Kähäri KR, Axelsson A, Hellström PA, Zachau G. Hearing assessment of classical orchestral musicians. Scand Audiol. 2001;30(1):13–23. doi:10.1080/010503901750069536
91. Toppila E, Koskinen H, Pyykkö I. Hearing loss among classical-orchestra musicians. Noise Health. 2011;13(50):45. doi:10.4103/1463-1741.74001
92. Cramp JE, Horstman SW. Musician sound exposure during performance of wagner’s ring cycle. Med Probl Perform Art. 1992;7:37–39.
93. Folprechtová A, Mikšovská O. Akustické podmínky v symfonickém orchestru. Prac Lék. 1976;28(1–2):1.
94. Jahto K, Hellmann H. Zur Frage des Lärm- und Klangtraumas des Orchestermusikers. HNO. 1972;20(1):21–29.
95. Flach M, Aschoff E. Zur Frage berufsbedingter Schwerhörigkeit beim Musiker. Laryngologie. 1966;43:595–605.
96. Schwab B, Schultze-Florey A. Velopharyngeal insufficiency in woodwind and brass players. Med Probl Perform Art. 2004;19(1):21–25. doi:10.21091/mppa.2004.1004
97. Malick D, Moon J, Canady J. Stress velopharyngeal incompetence: prevalence, treatment, and management practices. Cleft Palate Craniofac J. 2007;44(4):424–433. doi:10.1597/06-176.1
98. Costa MMB, Alvite FL. Lateral laryngopharyngeal diverticula: a videofluoroscopic study of laryngopharyngeal wall in wind instrumentalists. Arq Gastroenterol. 2012;49(2):99–106. doi:10.1590/S0004-28032012000200002
99. Cappellaro J, Beber BC. Vocal tract discomfort and voice-related quality of life in wind instrumentalists. J Voice. 2018;32(3):314–318. doi:10.1016/j.jvoice.2017.05.011
100. Trollinger V, Alnouri G, Sataloff RT. LEMG findings of vocal fold paresis in voice patients who play or played wind instruments. J Voice. 2021;S0892–1997(21):356–358. doi:10.1016/j.jvoice.2021.10.018
101. Plamenac P, Nikulin A. Atypia of the bronchial epithelium in wind instrument players and in singers: a cyto pathologic study. Acta Cytol. 1969;13(5):274–278.
102. Deniz O, Savci S, Tozkoparan E, Ince DI, Ucar M, Ciftci F. Reduced pulmonary function in wind instrument players. Arch Med Res. 2006;37(4):506–510. doi:10.1016/j.arcmed.2005.09.015
103. Bourne D, Hallaran A, Mackie J. The lived experience of orchestral string musicians with playing related pain. Med Probl Perform Art. 2019;34(4):198–204. doi:10.21091/mppa.2019.4031
104. Merkblatt zu der Berufskrankheit Nr. 2301 der Anlage zur Berufskrankheiten-Verordnung: lärmschwerhörigkeit [Fact sheet on occupational disease No. 2301 of the Annex to the Regulation on Occupational Diseases: Noise-induced hearing loss]; 2008. Available from: https://www.baua.de/DE/Themen/Praevention/Koerperliche-Gesundheit/Berufskrankheiten/pdf/Merkblatt-2301.pdf.
105. Empfehlung für die Begutachtung der Lärmschwerhörigkeit (BK-Nr. 2301) – königsteiner Empfehlung [Recommendation for the assessment of noise-induced hearing loss (occupational disease no. 2301) - Königstein recommendation]; 2020. Available from: https://publikationen.dguv.de/widgets/pdf/download/article/2559.
106. Notified and recognized occupational diseases in the field of the Berufsgenossenschaften. Classification: years, region, sex, type of occupational disease. Available from: https://www.gbe-bund.de/gbe/pkg_isgbe5.prc_menu_olap?p_uid=gast&p_aid=9921866&p_sprache=E&p_help=0&p_indnr=842&p_indsp=&p_ityp=H&p_fid=.
107. Bächinger D, Jecker R, Hannig JC, et al. The professional ear user-implications for the prevention, diagnosis, and treatment of ear diseases. HNO. 2022;70(12):891–902. doi:10.1007/s00106-022-01235-0
108. Tikka C, Verbeek JH, Kateman E, Morata TC, Dreschler WA, Ferrite S. Interventions to prevent occupational noise-induced hearing loss. Cochrane Database Syst Rev. 2017;7(7):CD006396. doi:10.1002/14651858.CD006396.pub4
109. Richter B, Zander M, Hohmann B, Spahn C. Hearing protectors in musicians. HNO. 2011;59(6):538–546. doi:10.1007/s00106-011-2306-z
110. Teie PU. Noise-induced hearing loss and symphony orchestra musicians: risk factors, effects, and management. Md Med J. 1998;47(1):13–18.
111. Koppejan S, Snijders CJ, Kooiman T, Van Bemmel B. Hand and arm problems in flautists and a design for prevention. Ergonomics. 2006;49(3):316–322. doi:10.1080/00140130500436213
112. Lee SH, Carey S, Dubey R, Matz R. Intervention program in college instrumental musicians, with kinematics analysis of cello and flute playing: a combined program of yogic breathing and muscle strengthening-flexibility exercises. Med Probl Perform Art. 2012;27(2):85–94. doi:10.21091/mppa.2012.2016
113. Visser A, Van Der Biezen JJ. Inferior-based pharyngeal flap for correction of stress velopharyngeal incompetence in musicians: case reports and review of the literature. J Plast Reconstr Aesthet Surg. 2012;65(7):960–962. doi:10.1016/j.bjps.2011.11.049
114. Clemente M, Mendes J, Moreira A, Vardasca R, Ferreira A, Amarante J. Wind Instrumentalists and temporomandibular disorder: from diagnosis to treatment. Dent J. 2018;6(3):41. doi:10.3390/dj6030041
115. Kenny DT, Fortune JM, Ackermann B. Predictors of music performance anxiety during skilled performance in tertiary flute players. Psychol Music. 2013;41(3):306–328. doi:10.1177/0305735611425904
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.