")
Back to Journals » Clinical Ophthalmology » Volume 14
Trends in Glaucoma Filtration Procedures: A Retrospective Administrative Health Records Analysis Over a 13-Year Period in Canada
Authors Kansal V , Armstrong JJ , Hutnik CML
Received 29 September 2019
Accepted for publication 10 January 2020
Published 20 February 2020 Volume 2020:14 Pages 501—508
DOI https://doi.org/10.2147/OPTH.S232873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Vinay Kansal,1 James J Armstrong,2,3 Cindy ML Hutnik2– 4
1University of Saskatchewan, Department of Ophthalmology, Saskatoon, SK, Canada; 2Western University Canada, Schulich School of Medicine, Department of Pathology and Laboratory Medicine, London, ON, Canada; 3Western University Canada, Schulich School of Medicine, Department of Ophthalmology, London, ON, Canada; 4Ivey Eye Institute, St. Joseph’s Hospital, London, ON, Canada
Correspondence: Cindy ML Hutnik
Ivey Eye Institute, St. Joseph’s Hospital, 268 Grosvenor Street, London, ON N6A 4V2, Canada
Tel +1 519-646-6100 Ext 66272
Fax +1 519-646-6410
Email [email protected]
Background: Glaucoma surgical management has evolved significantly with the introduction of minimally invasive glaucoma surgery. Our aim was to evaluate trends in Canadian glaucoma surgery billing code usage as a surrogate index of the current impact of this new technology in Canada’s publicly funded health-care system.
Methods: Retrospective administrative health records analysis of all patients who underwent a publicly funded glaucoma filtration procedure from January 2003 to December 2016 in the 6 largest Canadian provinces. The frequency of glaucoma-related procedures was adjusted against primary open-angle glaucoma prevalence data. Frequency of all glaucoma filtration procedures with and without implantation of a drainage device in each province per year is reported.
Results: Nationwide, glaucoma filtration procedures per 1000 primary open-angle glaucoma patients per year remained constant, with increased drainage device implantation over time (P< 0.0001). Ontario and Nova Scotia mirrored the overall population. British Columbia and Saskatchewan showed increased rates of glaucoma filtration surgery, with increased drainage device implantations. In Quebec, overall filtration surgery decreased, while the rate of device implantation increased (p< 0.0001). Alberta showed a decline in filtration surgery and device implantations from 2003 to 2008, and then increased thereafter.
Conclusion: Over the study period, there was a distinct trend towards billing code usage for implanted devices. Challenges encountered during this investigation highlight the need for identifiers in provincial health databases to accommodate the introduction of novel technologies. The absence of specific billing codes for newer technologies prevents accurate analyses of impact, utilization, efficacy and cost implications in contemporary patient management.
Keywords: glaucoma, minimally invasive glaucoma surgery, MIGS, glaucoma filtration surgery, population analysis
Introduction
Novel, advanced minimally invasive therapies have been increasingly adopted as the standard of care across most surgical fields, often reducing risks and allowing for faster recovery. Unfortunately, while practice patterns evolve to employ new technologies, the systems in place to track and remunerate the provision of these services may not. The evolution of the management of elevated intraocular pressure in glaucoma is a model example of this paradigm shift. Trabeculectomy surgery is the gold standard, used to filter aqueous humor out of the eye and lower intraocular pressure1,2 Historically, primarily due to risk, it has been indicated later in the treatment paradigm, following the use of medication and laser-based therapies.3–5 Novel surgical techniques, collectively termed minimally invasive glaucoma surgeries have emerged purporting improved safety profiles and faster recovery times.6–8 The ability to lower intraocular pressure while reducing dependency on topical anti-hypertensive medication has created significant interest in minimally invasive glaucoma surgery, with current utilization of these surgical procedures earlier in glaucoma management.
Despite the great interest, guidance regarding the use of minimally invasive glaucoma surgery is not yet widely outlined in the most recently published international clinical practice guidelines.9 A systematic review of 11 glaucoma clinical practice guidelines reports that only 3 mentioned minimally invasive glaucoma surgery with little guidance regarding recommendations for their use.9 In the absence of up-to-date clinical practice guidelines and procedure-specific billing codes, data to track utilization are non-existent. Following the federal approval of a newer surgical device, there is often a delay in the update of clinical practice guidelines, introduction of billing codes and public funding. Health policy makers depend upon evidence from reliable clinical trials and population-level data for decision-making. The lack of specific billing codes for novel technologies hampers the collection of robust data for these investigations. In Canada where the government serves as a single payer, where patients are not permitted to directly pay for medically necessary procedures, it is impossible to determine the exact utilization and demand for newer technologies on a population level using provincial datasets. The total number of glaucoma procedures performed can be determined; however, it is often not possible to differentiate between the types of surgical procedures performed. In Canada, access to medically necessary, novel technologies is often made possible by physician selection of semi-equivalent, existing billing codes as surrogates. The purpose of this study was to evaluate the trends in Canadian glaucoma surgery billing code usage over a period of time coinciding with the availability of several new minimally invasive glaucoma surgery procedures and devices.
Methods
Study Design and Data Sources
This was a retrospective administrative health records analysis of data from centralized databases of six Canadian provincial health ministries. These jurisdictions combined comprise 92.2% of the Canadian population. Data on the number of glaucoma-related procedures billed for from January 2003 to December 2016 were obtained from databases maintained by the Ministries of Health of British Columbia, Alberta, Saskatchewan, Ontario, Quebec, and Nova Scotia. These databases have been previously validated for many outcomes, exposures and diagnoses.10 Specifically, data were obtained on the number of glaucoma filtration procedures performed, with and without implanted drainage device during each calendar year. The term “glaucoma filtration procedures” in general refers to trabeculectomy and tube shunt implantation. With the advent of minimally invasive glaucoma surgery, many of these procedures are being classified as glaucoma filtration procedures as well. This study used only aggregate data, obtained at a population level, with no personal patient or surgeon identifying information. Specific procedural billing codes obtained from each province are outlined in Appendix A.
Four provinces were excluded from analysis: (1) Prince Edward Island – glaucoma filtering procedures are not performed, (2) Manitoba and New Brunswick – Schedules of Benefits do not list separate codes for drainage device implantation during glaucoma filtration surgery, and (3) Newfoundland and Labrador’s Schedule of Benefits – a separate code for drainage device implantation has only existed since 2013, precluding comparative analyses between provincial datasets. Ethics approval waiver was received from both Western University Canada and the University of Saskatchewan for this research.
Statistical Methods
Population data were obtained from Statistics Canada and were cross-referenced with data on the age distribution of primary open-angle glaucoma11 to estimate the number of glaucoma patients in each province. This allowed standardization of the number of glaucoma surgeries within each province relative to the number of estimated patients at risk within that same province, as done previously.12 This allowed the data to be expressed as the number of billings of each code, per 1000 patients, and facilitated comparison of trends across multiple provinces with varying numbers of glaucoma patients. The specific calculations performed to arrive at these adjusted estimates are outlined in Appendix B. The frequency of glaucoma filtration procedures was reported, per 1000 patients, per year, for (1) all glaucoma filtration procedures, (2) filtration procedures without implantation of a drainage device, and (3) filtration procedures with implantation of a filtration device. Data points were regressed to the line of best fit using simple linear regression. The slopes of the trend lines were compared using analysis of covariance to (1) assess whether a significant trend existed over time, and (2) to determine whether a significant difference existed between the slopes of the frequency trend lines for the IDD and no-IDD groups – ie that the trend line slopes are non-parallel.13,14 All statistical analysis was performed using Prism 7 (Version 7.03, GraphPad Software Inc.).
Results
During the 14-year study period, the number of glaucoma filtration procedures remained relatively constant, at approximately 35 per 1000 patients. Rate of drainage device implantation steadily increased (slope: 0.80, confidence interval (CI) 0.71,0.88, p<0.001). The rate of procedures performed without drainage device implantation correspondingly decreased (Slope: −0.80, CI −0.94,-0.66, p<0.001). These trends differed significantly (p<0.0001; Figure 1, Table 1 and Appendix C)
 |
Table 1 Analysis of Covariance and Linear Regression Outcomes. Slope of Trendlines, and Comparison Between Procedures with and Without an Implanted Drainage Device |
 |
Figure 1 Frequencies of glaucoma filtration procedures per 1000 primary open-angle glaucoma patients in Canada over the study period. Abbreviations: GFS, glaucoma filtration procedures; IDD, implanted drainage device; POAG, primary open-angle glaucoma. |
Analysis was stratified by each of the included provinces and results of this are reported in Table 1, Appendix C, and Figure 2 (British Columbia), Figure 3 (Alberta), Figure 4 (Saskatchewan), Figure 5 (Ontario), Figure 6 (Quebec), and Figure 7 (Nova Scotia). Reported are the rates of filtration surgery overall, filtration surgery with implanted drainage device, and filtration surgery without implanted drainage device.
 |
Figure 2 Frequencies of glaucoma filtration procedures per 1000 primary open-angle glaucoma patients in British Columbia over the study period. Abbreviations: GFS, glaucoma filtration procedures; IDD, implanted drainage device; POAG, primary open-angle glaucoma. |
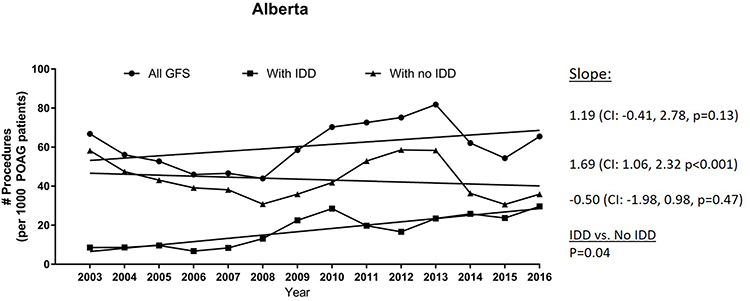 |
Figure 3 Frequencies of glaucoma filtration procedures per 1000 primary open-angle glaucoma patients in Alberta over the study period. Abbreviations: GFS, glaucoma filtration procedures; IDD, implanted drainage device; POAG, primary open-angle glaucoma. |
 |
Figure 4 Frequencies of glaucoma filtration procedures per 1000 primary open-angle glaucoma patients in Saskatchewan over the study period. Abbreviations: GFS, glaucoma filtration procedures; IDD, implanted drainage device; POAG, primary open-angle glaucoma. |
 |
Figure 5 Frequencies of glaucoma filtration procedures per 1000 primary open-angle glaucoma patients in Ontario over the study period. Abbreviations: GFS, glaucoma filtration procedures; IDD, implanted drainage device; POAG, primary open-angle glaucoma. |
 |
Figure 6 Frequencies of glaucoma filtration procedures per 1000 primary open-angle glaucoma patients in Quebec over the study period. Abbreviations: GFS, glaucoma filtration procedures; IDD, implanted drainage device; POAG, primary open-angle glaucoma. |
 |
Figure 7 Frequencies of glaucoma filtration procedures per 1000 primary open-angle glaucoma patients in Nova Scotia over the study period. Abbreviations: GFS, glaucoma filtration procedures; IDD, implanted drainage device; POAG, primary open-angle glaucoma. |
Discussion
Main Findings
Trends in glaucoma filtration procedures from 2003 to 2016 demonstrate that while the overall frequency of glaucoma filtration surgery has remained relatively stable, the proportion of cases performed with an implanted drainage device significantly increased over the study period. This time period straddles the Health Canada approval of minimally invasive glaucoma surgery, such as the iStent (Glaukos Corporation) in 2009. Our cohort allowed evaluation of trends in glaucoma filtration surgery billing code frequencies spanning the period before the introduction of minimally invasive glaucoma surgery, during the early adoption of these techniques, through to more widespread use.
The results supported the study rationale by highlighting the challenges caused by infrequently updated surgical billing code schedules. It was not possible to reliably differentiate between the novel minimally invasive glaucoma surgery procedures and the traditional, more invasive, glaucoma tube-shunts. In the absence of updated specific procedure codes, surgeons must select an existing code, or submit claims under an “independent consideration” category, creating inherent variability in the process. The use of a single code applied to a combination of older and newer procedures makes it nearly impossible to determine accurate practice patterns and cost-effectiveness.
In most provinces, it is impossible to differentiate between ab interno (from inside the eye) and ab externo (from outside the eye) surgical approaches. The traditional trabeculectomy is an ab externo approach which is generally more time-consuming and associated with greater risk due to increased tissue dissection. Alberta and Quebec have both introduced minimally invasive glaucoma surgery-specific billing codes (ie ab interno vs ab externo). In Alberta, glaucoma filtration surgery declined from 2003 to 2008, and then rose until 2014, potentially corresponding to the adoption of minimally invasive glaucoma surgery in 2009 and the use of existing glaucoma surgical codes at the time. The subsequently observed decrease after 2014 may correspond to the introduction of more specific codes and likely reflects an appropriate reclassification of some of these procedures. In Quebec, similar trends were not seen after the introduction of a minimally invasive glaucoma surgery code in 2015, although records of drainage device implantation did steadily increase over the 13-year study period.
The inability to study the use of specific implanted devices at a population level hinders their inclusion in clinical practice guidelines, leaving minimal guidance for novel technologies.9 The significant delay between the advent of new technologies and updates to the physician billing schedules is reflected across several surgical specialties and hamstrings the relatively broad and rapid retrospective analysis that could be performed on these datasets. Due to these unintended blind spots in provincial data collection, the opportunity to assess the true impact of novel technologies, and ultimately, optimal patient treatment strategies, is lost.
These system-level limitations also hinder the ability to study the overall economic impact of these interventions. The use of inaccurate existing billing codes prevents tracking the real costs of these surgeries to the system, including physician payment, cost of devices, operating room time, admission and hospital stay. Certain procedures may require increased frequency of follow up or repeat intervention due to complications or lack of efficacy. Under the current system, it is difficult to determine which type of procedure or patient incurs these costs. The issues of efficacy and cost are intrinsically intertwined. Limited access due to funding restricts broad utilization which is an impediment to understanding which patients would most benefit. This, in turn, prevents the optimization of health-care expenditures.
This investigation also highlights the striking differences in physician billing code schedules between provinces. Only 6 of 10 provincial databases had codes for glaucoma filtration surgery specifying concurrent implantation of a drainage device. Specific terminology of glaucoma filtering procedures varied widely. In the absence of billing codes that accurately describe contemporary treatments, physicians select codes that they feel best represent the procedure performed, inevitably leading to inconsistencies. A noteworthy observation is that each province has its own specific Schedule of Benefits, all with different procedural values and processes by which they are created and updated.
Comparison with Other Studies
This limitation has also been identified by the Canadian Agency for Drugs and Technologies in Health, in their report on the topic “Optimal Use of MIGS: A Health Technology Assessment”15 They identify several concerns facing the adoption of minimally invasive glaucoma surgery into the glaucoma therapy paradigm: (1) insufficient evidence for the comparative clinical effectiveness and safety of minimally invasive glaucoma surgery versus pharmacotherapy, laser therapy, different minimally invasive glaucoma surgery (one vs the other), or filtration surgery, (2) cost-effectiveness of minimally invasive glaucoma surgery is uncertain, and (3) concerns about equal access and informed consent in the context of surgical innovation.
Future Directions
Based on the findings and challenges of the present investigation, a number of recommendations are suggested to improve future population-based studies of novel technologies, such as microinvasive and traditional glaucoma filtration surgeries. First, harmonization of billing code terminology would facilitate tracking of health-care utilization at a national level. Code specificity, such as between ab interno and ab externo glaucoma procedures, would reduce variability and increase database accuracy. An analysis of the impact of more specific types of codes introduced in Alberta and Quebec would also be informative regarding wider adoption. Removal of antiquated and redundant codes would also serve to reduce variability and prevent erroneous use. Mechanisms can be considered to allow newer technologies within a class, with sufficient evidence for safety and efficacy, to have a facilitated path to a “trial” billing code assignment. To these, a specific descriptor could be added to identify the specific procedure performed. Data derived from this can inform decision-making to either create a permanent code, or to allow the temporary code to expire. The ultimate driver of any such process should be equal access for all Canadians to innovative technologies that are considered medically necessary and which offer health-related quality of life benefits.
Limitations
The primary challenge with the currently available data is the lack of a coding strategy that reconciles the multitude of available glaucoma procedures with appropriate billing codes for tracking them. At the very least, codes differentiating between minimally invasive glaucoma surgery and trabeculectomy are absolutely necessary for meaningful analysis. A second limitation was that data were not included from all Canadian provinces and territories. This limitation, however, is mitigated by the fact that excluded regions represent only 7.8% of Canadian population, and these patients are typically referred to alternate jurisdictions for surgical glaucoma management and therefore would likely be captured in our datasets.
In order to provide context to the filtration surgery rates, data were adjusted against the population of primary open-angle glaucoma patients, the largest subgroup of glaucoma patients undergoing surgery,16 estimated to be living in each province. These methods have been used successfully previously,11,12 however, are subject to geographic and demographic variations over time. Furthermore, the prevalence estimates derived by Tuck and Crick used may not directly match our study population. Other estimates of glaucoma prevalence in Ontario are available from self-report surveys, such as the National Population Health Survey and the Canadian Community Health Survey. Self-report data, however, depend on patient’s accurate knowledge regarding their glaucoma status. Further, these surveys do not differentiate between glaucoma subtypes. Finally, these data do not cover the study period and, therefore, were of little use.
Conclusions
Over the study period, there was a significant increase in the rate of glaucoma drainage device implantation in the majority of Canadian provinces. Challenges encountered during this investigation highlight the need for identifiers in provincial health databases to better delineate between ab interno and ab externo procedures, as well as between traditional filtration surgery and minimally invasive glaucoma surgery to allow more robust understanding of the efficacy of new and emerging therapies.
Ethics Approval and Informed Consent
Exemption for ethics approval was obtained from the research ethics boards of the University of Saskatchewan and Western University Canada for this work.
Data Sharing Statement
Data are available upon request.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Beckers HJM, Kinders KC, Webers CAB. Five-year results of trabeculectomy with mitomycin C. Graefes Arch Clin Exp Ophthalmol. 2003;241:106–110. doi:10.1007/s00417-002-0621-5
2. Watson PG, Grierson I. The place of trabeculectomy in the treatment of glaucoma. Ophthalmology. 1981;88:175–196. doi:10.1016/S0161-6420(81)35051-9
3. Canadian Ophthalmological Society Glaucoma Clinical Practice Guideline Expert Committee, Canadian Ophthalmological Society. Canadian Ophthalmological Society evidence-based clinical practice guidelines for the management of glaucoma in the adult eye. Can J Ophthalmol. 2009;44(Suppl 1):S7–S93. doi:10.3129/i09.080
4. Anon. European Glaucoma Society Terminology and Guidelines for Glaucoma, 4th Edition - Chapter 3: treatment principles and options supported by the EGS foundation: part 1: foreword; Introduction; Glossary; Chapter 3 Treatment principles and options. Br J Ophthalmol. 2017;101:130–195.
5. Prum BE, Lim MC, Mansberger SL, et al. Primary open-angle glaucoma suspect preferred practice pattern® guidelines. Ophthalmology. 2016;123:P112–P151. doi:10.1016/j.ophtha.2015.10.055
6. Conlon R, Saheb H, Ahmed IIK. Glaucoma treatment trends: a review. Can J Ophthalmol. 2017;52:114–124. doi:10.1016/j.jcjo.2016.07.013
7. Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311:1901–1911. doi:10.1001/jama.2014.3192
8. Kerr NM, Wang J, Barton K. Minimally invasive glaucoma surgery as primary stand-alone surgery for glaucoma: minimally invasive glaucoma surgery. Clin Experiment Ophthalmol. 2017;45:393–400. doi:10.1111/ceo.2017.45.issue-4
9. Michaelov E, Armstrong JJ, Nguyen M, et al. Assessing the methodological quality of glaucoma clinical practice guidelines and their recommendations on microinvasive glaucoma surgery: a systematic review. J Glaucoma. 2017;27:1.
10. Williams JI, Young W. A summary of studies on the quality of health care administrative databases in Canada. Patterns Health Care Ont ICES Pract Atlas 2nd Ed Ottawa. Can Med Assoc. 1996;339:45.
11. Tuck MW, Crick RP. The age distribution of primary open angle glaucoma. Ophthalmic Epidemiol. 1998;5:173–183. doi:10.1076/opep.5.4.173.4192
12. Szigiato AA, Trope GE, Jin Y, Buys YM. Trends in glaucoma surgical procedures in Ontario: 1992–2012. Can J Ophthalmol. 2015;50:338–344. doi:10.1016/j.jcjo.2015.07.005
13. Zar JH. Biostatistical Analysis. Prentice Hall; 2010.
14. Zar JH. Biostatistical Analysis. Englewood Cliffs; Prentice Hall, 1984.
15. Canadian Agency for Drugs and Technologies in Health. Optimal Use of Minimally Invasive Glaucoma Surgery: A Health Technology Assessment; 2019;62.
16. Cook C, Foster P. Epidemiology of glaucoma: what’s new? Can J Ophthalmol. 2012;47:223–226. doi:10.1016/j.jcjo.2012.02.003
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.