")
Back to Journals » Open Access Surgery » Volume 16
Treatment Outcomes of Non-Traumatic Acute Abdomen and Its Associated Factors in Adult Patients at Tibebe Ghion Specialized Hospital, Bahir Dar, Ethiopia: Cross-Sectional Study
Authors Yesuf M, Taye M, Bogale EK
Received 24 October 2023
Accepted for publication 15 December 2023
Published 20 December 2023 Volume 2023:16 Pages 105—113
DOI https://doi.org/10.2147/OAS.S443457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Luigi Bonavina
Mohammed Yesuf,1,* Mequanint Taye,1 Eyob Ketema Bogale2,*
1Department of Surgery, Bahir Dar University, Bahir Dar, Ethiopia; 2Health Promotion and Behavioral Sciences Department, Bahir Dar University, Bahir Dar, Ethiopia
*These authors contributed equally to this work
Correspondence: Eyob Ketema Bogale, Email [email protected]
Objective: To assess the treatment outcomes of non-traumatic acute abdomen and its associated factors among adult patients in Bahir Dar city, Ethiopia.
Methods: A retrospective hospital-based cross-sectional study was done, and a random sampling technique was used. A total of 303 records were examined, and a pre-tested data extraction checklist was used to collect the data, which was entered into the Kobo toolbox. The data was then exported and analysed using SPSS version 26, a binary logistic regression model was used, and finally, an adjusted odds ratio with a 95% CI and a p-value less than 0.05 was considered statistically significant factors associated with the treatment outcomes of non-traumatic acute abdomen.
Results: The magnitude of unfavorable treatment outcomes for non-traumatic acute abdomen was found to be 11.9% with 95% CI: (8.6– 15.5). Those patients with guarding (AOR = 2.98, 95% CI = 1.05, 8.47), having postoperative complications (AOR = 1.65, 95% CI = (1.07, 3.53)), and having temperature ≥ 37.5 (AOR = 3.21, 95% CI = (1.78, 19.5)) were significantly associated with the treatment outcome of non-traumatic acute abdomen.
Conclusion: The findings of this study showed that the magnitude of unfavorable treatment outcomes for non-traumatic acute abdomen was found to be high. Presence of postoperative complications, having temperature ≥ 37.5°C, and having abdominal guarding were statistically significant factors associated with unfavourable treatment outcome of non-traumatic acute abdomen. Hence, all level medical workers should give more attention to infection prevention in the ward and in the operating room.
Keywords: acute abdomen, non-traumatic, outcome, Tibebe Ghion Specialized Hospital
Introduction
Acute abdomen is the acute onset of abdominal disease entities that, in the majority of cases, necessitate immediate surgical intervention.1 Non-traumatic acute abdomen is a component of acute abdomen and a significant public health issue. It is a common emergency with little chance of being prevented that costs a lot to treat surgically. In several Asian and some African nations, it accounts for up to 54% of general surgical admissions and up to 88.2% of all emergency procedures. Despite the widespread use of contemporary surgery, non-traumatic acute abdominal surgical emergencies nevertheless have a high death rate, with the highest rates occurring at the oldest and youngest ages.2–4
Due to socioeconomic, demographic, and dietary differences, the magnitude of non-traumatic surgical acute abdomen varies by region. Additionally, different settings and geographies have varied incidences of post-operative problems.5,6 Mortality rates from acute abdominal surgery emergencies remain very high. Patients over 60 had a significantly greater death rate than the general 4.2% rate.7,8
Vomiting and stomach pain are the most typical symptoms, although soreness and guarding are the most typical clinical findings. It is a frequent surgical emergency that, if improperly handled, carries a substantial risk of morbidity and mortality.5,9–12
While biliary disease, bowel obstruction, intestinal ischemia and infarction, and diverticulitis are more common in elderly patients, appendicitis is more common in young people.13 In tropical nations, typhoid ileal perforation is still a highly serious disorder. Its occurrence might be anywhere from 0.9% to 39%, yet its fatality rate is still very high.3,14 Early (in-hospital) postoperative problems occurred in about 26.6% of operating patients,15 and 15.3% was the overall mortality rate.16
Increased morbidity and mortality are frequently caused by inadequate health education, subpar medical facilities, and tardy presentations. Age (>55 years) and sickness duration (more than 2 days) were significantly linked to postoperative complications.16,17
The studies’ finding in Ethiopia showed that the mortality rate of the surgically treated acute abdomen was 3% in Nekemte Referral Hospital,18 and 22% in Wolaita Referral Hospital.19 Only a few studies have been conducted in Ethiopia about the treatment outcome of non-traumatic acute abdomen and its associated factors,3,18,19 but especially in our study area, Bahir Dar, there has been no research paper done on this subject matter. Periodical investigations are required because the extent of non-traumatic acute surgical abdomen varies globally as well as regionally, and changes in the disease pattern over time are well reported in the literature.4,6,20,21
Hence, the importance of accurate data regarding treatment outcomes and its associated factors in the non-traumatic acute abdomen is indisputable. Therefore, the objective of this study was to assess the treatment outcomes of non-traumatic acute abdomen and its associated factors among adult patients in Bahir Dar city, Ethiopia to fill the aforementioned gap.
Materials and Methods
Study Design and Settings
An institution-based cross-sectional study design was conducted among adult patients who had been diagnosed with non-traumatic acute abdomen at Tibebe Ghion Specialized Hospital (TGSH) from August 1, 2020, to July 31, 2021.
This study was conducted at TGSH, which is a specialized teaching hospital under the Bahir Dar University College of Health Science and Medicine in Bahir Dar, Ethiopia. Bahir Dar, the city, is located at a distance of 505 kilometers in the north-west direction from Addis Ababa (the capital city of Ethiopia). TGSH is a tertiary-level hospital established in 2011 E.C. and serving about 5 million people. The hospital has 493 beds, and the surgery wards have 107 beds. It has seven functional operating rooms. Currently, the hospital has 706 clinical staff. The emergency OPD has 25 beds, and since 2011, nearly 25,000 patients have been seen.
Participants and Sampling
All adult patient charts or cards diagnosed with non-traumatic acute abdomen by history, physical examination, or other investigation modalities at TGSH and older than 18 years old were included in the study, whereas all patient charts or cards discharged against medical advice, patients with diagnoses of non-traumatic surgical acute abdomen who were operated outside of TGSH and admitted after operation in the hospital, and patients with diagnoses of non-traumatic surgical acute abdomen were excluded from the study.
The sample size was calculated using a single population proportion formula. Based on the single population proportion assumptions, there was a 95% confidence level (Z), a 5% margin of error (E), and a proportion of NTAA patients who had favorable outcomes of 0.75 from the study done at Wolaita.21 The final sample size was 303 after adding 10% non-respondents.
Systematic random sampling was applied to select study participants. The total number of admitted NTAA patients at Tibebe Ghion Specialized Hospital was obtained from the log books. The sampling interval (kth unit) was obtained by dividing the entire admitted NTAA patients in TGSH from August 1, 2020, to July 31, 2021 (682) by the desired sample size (303), and it was approximately 2.
The first participant was randomly chosen for the survey by the lottery method from the first two participants, and then every two participants were recruited for the study to identify a total of 303 samples.
Data Collection
Structured data extraction checklists were prepared by reviewing the literature.2 The first part of the questionnaire consists of issues related to personal information, including age, sex, and place of residence. The second part is concerned with causes of non-traumatic acute abdomen, hospital stay, treatment given, procedures applied, complications, and outcomes of non-traumatic acute abdomen (Supplementary File 1). The target study populations were first identified from the registration books of surgical units and operation theatres. Then, the patient’s medical records were retrieved, and data was collected using a pre-prepared standard checklist from the chart.
Operational Definition
Non-Traumatic Acute Abdomen Outcomes are Operationalized as
- Favourable: when either operatively managed or conservative treatment with supportive management of the patient’s charts was documented with a clinical diagnosis of stable vital signs and/or documented as improved on the discharge summary sheet and discharged from the hospital.22
- Non-favourable: patients with a clinical diagnosis who were operatively or conservatively managed for acute abdomen but did not improve on discharge (including death, referral, or worsening).22
Non operative management (conservative): This means the management of patients with appendiceal masses, partial bowel obstruction, recurrent adhesive obstruction, or during the early postoperative period with NGT suction, IV fluids, and frequent clinical reassessment to rule out bowel strangulation, which may need operative management.21
Operative management means surgical exploration of the abdomen.21
Data Quality Assurance
The structured data extraction checklists prepared in the English version were assessed. The training was given to data collectors about the data collection tool and how to collect data before data collection to have a common understanding. Before data analysis, we checked the completeness and consistency of each checklist with close supervision. All the collected data were checked and rechecked, and the necessary corrections were made each day.
Data Management and Analysis
After data was collected by the Kobo toolbox, it was coded, entered, and cleaned in SPSS version 26 computer software for descriptive and logistic regression analysis of the data. Binary and multivariate logistic regression analyses were used. On binary logistic regression analysis, a p-value of <0.25 was used as a candidate for multivariate logistic regression analysis. The data were presented in terms of frequency, tables, and figures. The association between dependent and independent variables was checked by using a logistic regression model. Crude and adjusted odds ratio was used to know and ascertain any association between the independent and dependent variables. The adjusted odds ratio (AOR) with a 95% CI and a P-value less than 0.05 was considered statistically significant in this study.
Results
Socio-Demographic Characteristics of Respondents
A total of 303 cards were chosen for the study over the course of the one-year study period. The study’s participants ranged in age from 16 to 83, with a mean age of 37.58 years and a standard deviation (SD) of 16.42 years. The mean duration of illness before admission was 2.46 days, and the length of hospital stay was 4.14 days (Table 1).
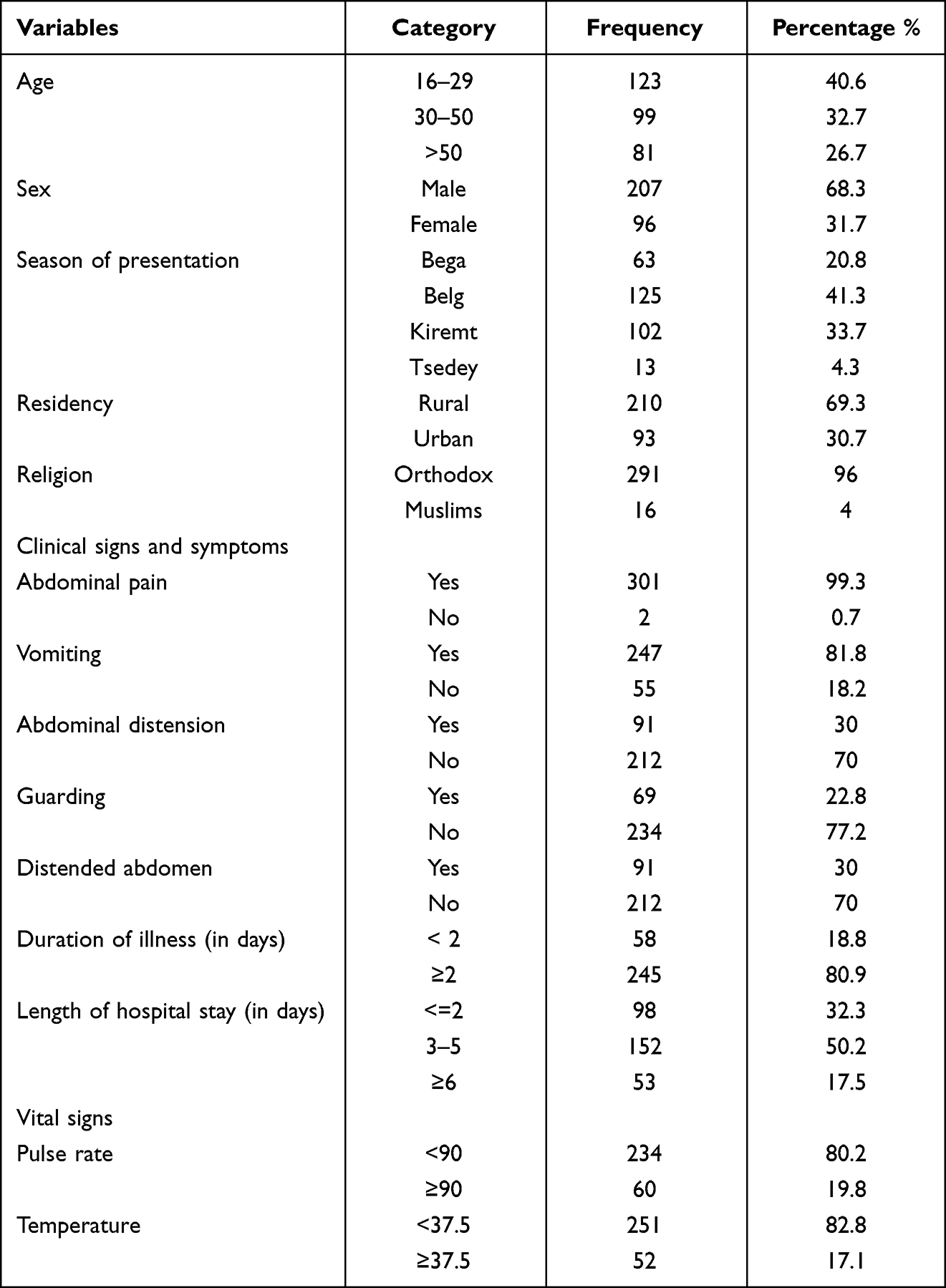 |
Table 1 Socio Demographic Characteristics and Clinical Features of Patients with Non-Traumatic Acute Abdomen in TGSH from August 2020 to July 2021 |
Patterns of Non-Traumatic Acute Abdomen Among Study Participants
Abdominal discomfort (99%), nausea (98.3%), abdominal soreness (92.1%), and abdominal distension (30%) were the most prevalent clinical characteristics (Table 1). About 80.9% of the non-traumatic acute abdominal cases showed up after two days of illness. In this study, the most common cause of non-traumatic acute abdomen was appendicitis which accounts 48.8% followed by intestinal obstruction (20.1%), and peritonitis (18.5%), and cholecystitis and pancreatitis (12.6%) (Table 2).
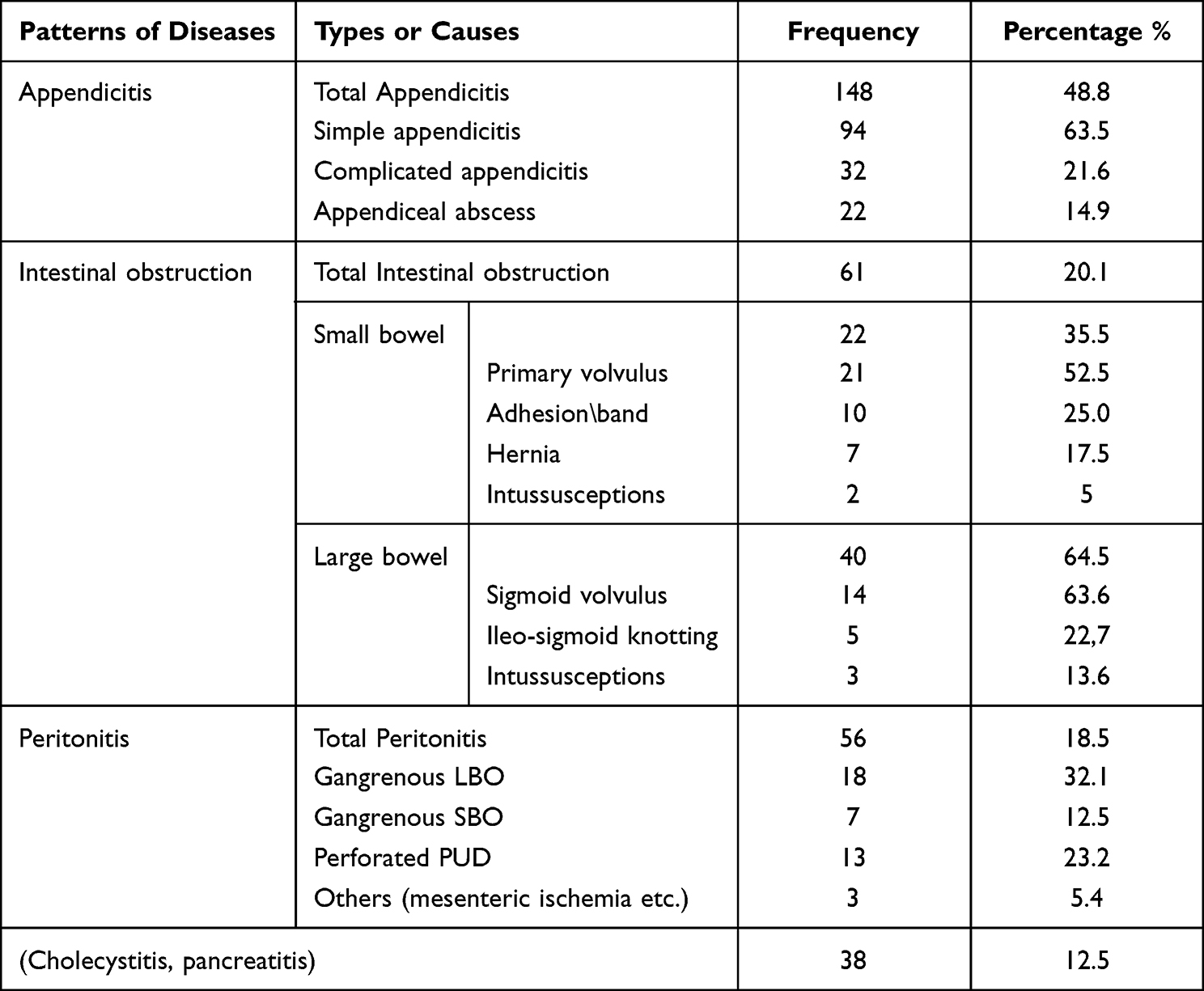 |
Table 2 Common Patterns and Causes of Non-Traumatic Acute Abdomen in TGSH from August 2020 to July 2021 |
Treatment Modality and Complications of Patients Admitted with Non-Traumatic Acute Abdomen
About 90% of the participants received surgical treatment, with the remaining participants receiving conservative care. In this study, the overall postoperative complication rate was 11.6% and overall mortality rate was 1%. The most common postoperative complication among non-traumatic acute abdomen was a wound infection, which accounts 5.9%, followed by pneumonia (3%) and sepsis (0.7%) (Table 3).
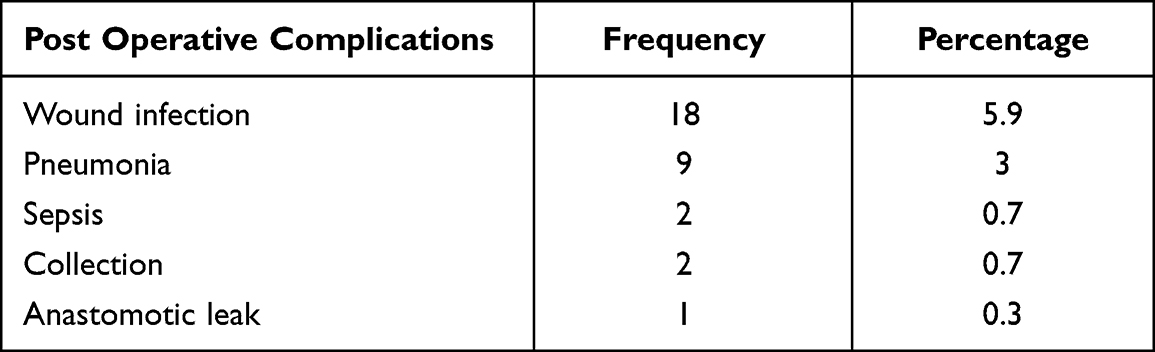 |
Table 3 Post Operative Complication Frequencies of NTAA Participants |
Magnitude of Treatment Outcome of Patients Admitted with Non- Traumatic Acute Abdomen
The study revealed that the magnitude of unfavorable treatment outcomes for non-traumatic acute abdomen was found to be 11.9% with 95% CI: (8.6–15.5). The majority of the participants who had appendicitis (94%) and intestinal obstruction (84%) were managed and discharged with a good outcome, whereas 66% of the participants with peritonitis had a favourable outcome.
Factors Associated with the Treatment Outcome of Non-Traumatic Acute Abdomen
In bivariable analysis, age, abdominal distension, guarding, temperature ≥37.5, distended abdomen, and postoperative complications were found candidate variable for multivariable analysis at p value less than 0.25.
In multivariable analysis, patients who had sign and symptoms of guarding, having postoperative complications and having temperature ≥37.5°C were significantly associated with favourable treatment outcome of non traumatic acute abdomen at p value less than 0.05.
The odds of unfavorable treatment outcome among non-traumatic acute abdomen patients who had guarding was 2.98 times more likely than the counterparts (AOR = 2.98, 95% CI = 1.05, 8.47).
The odds of unfavorable treatment outcome among non-traumatic acute abdomen patients who had body temperature ≥37.5°C were 3.21 times more likely than those who had normal body temperature (AOR = 3.21, 95% CI = 1.78, 19.45).
The odds of unfavorable treatment outcome among non-traumatic acute abdomen patients who had postoperative complications were 1.65 times more likely than the counterparts (AOR = 1.65, 95% CI = (1.07, 3.53)) (Table 4).
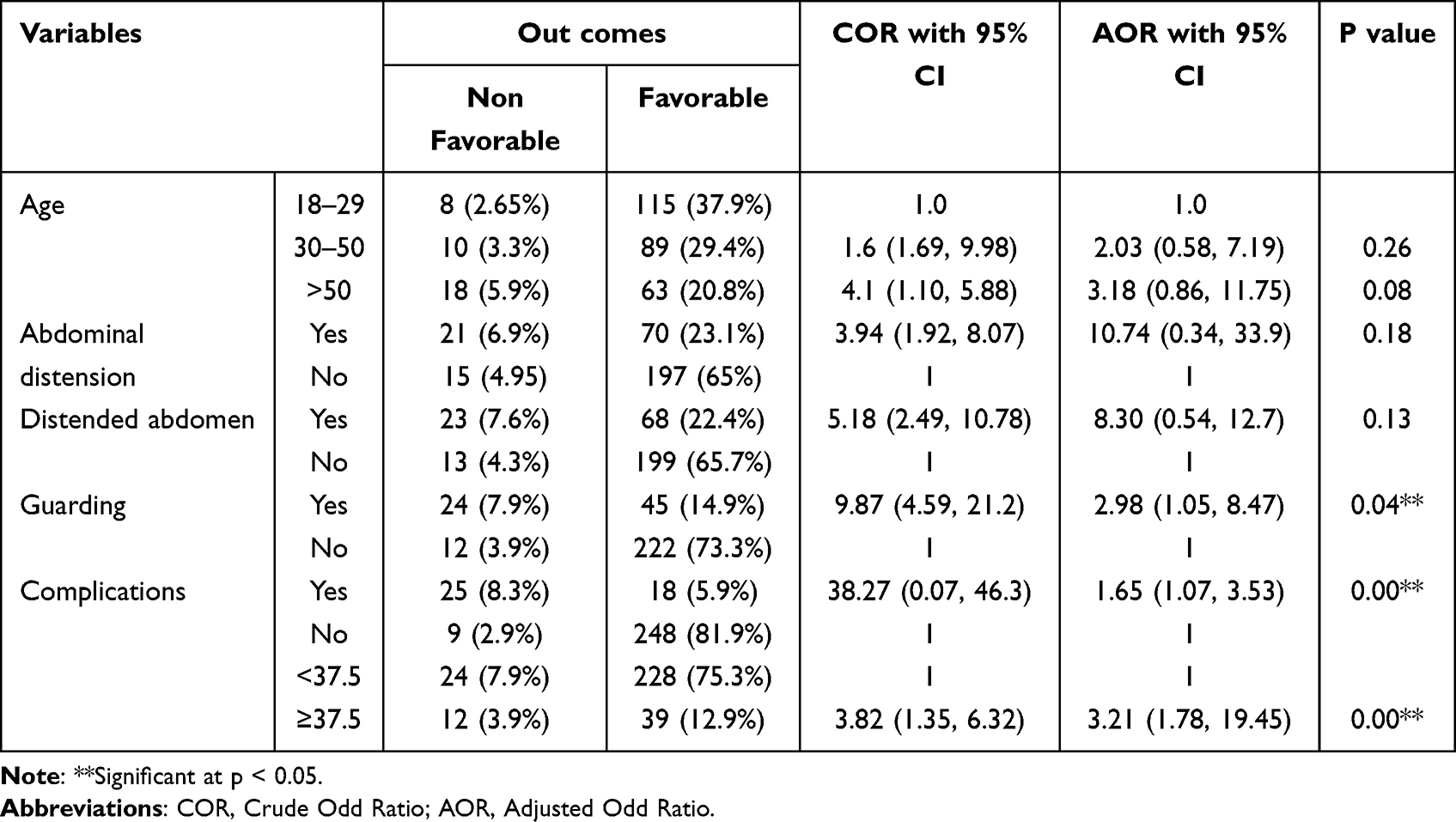 |
Table 4 Multivariate Analysis Showing Independent Predictors of Management Outcomes of Non-Traumatic Acute Abdomen in TGSH from August 2020 to July 2021 |
Discussion
Acute appendicitis (48.8%), intestinal obstruction (20.1%), and peritonitis (20.1%) were the most frequent causes of non-traumatic acute abdomen in our hospital. Similar findings were found in Nekemte20 and Attat.22 This may be because the majority of participants were in the young age group in the second and third decades.14 Contrary to our findings, research conducted at the Gondar University Hospital15 found that the most common operational diagnoses were SBO (43.4%), appendicitis (34.6%), and LBO (11.5%). The participants’ diets and socioeconomic backgrounds may be connected to this. Acute abdominal patients who underwent surgery were mostly from rural locations (58.2%).
The overall postoperative complication rate was 11.6%, which is nearly lower than the 17% reported in Mekelle research.2 The most frequent early postoperative complications were wound infection and pneumonia. This could be because abdominal surgery is an emergency procedure that may be contaminated or filthy, post-operative problems are one of the most frequent complications after abdominal surgery and consequently increase mortality and morbidity in patients who come with an acute abdomen.14
Our hospital’s overall mortality rate was 1%, which is lower than the rates at Malawi23 Tikur Anbessa Teaching Hospital (15.3%), Nekemte Referral Hospital (3.05%), and Mekelle Referral Hospital (2.4%). This could be a result of the inadequate treatment and recording of fatalities.22,24
The overall non-favourable treatment outcome was 11.9% (95% CI: 8.6–15.5). The majority of the participants who had appendicitis (94%) and intestinal obstruction (84%) were managed and discharged with a good outcome, whereas 66% of the participants with peritonitis had a favourable outcome.
The results of this study showed that those who experienced post-operative complications had significant association with unfavourable treatment outcome. This finding is supported by research conducted at Gondar Hospital (3), Tikur Anbessa Hospital,4 and Attat Hospital22 in which post-operative complications had a significant impact on patients’ outcomes.
Patients who had a record of body temperatures over 37.5 had significant association with unfavourable treatment outcome. This finding is similar with a study conducted at Tikur Anbessa Hospital,25 which revealed that patients with records of high body temperatures had a lower chance of improving than those with normal body temperatures. This might be due to fever being characterized by a temperature of 37.5°C or higher and is accompanied by alterations in the immunological and metabolic systems. It significantly affects the clinical presentation and prognosis of the illness.14
Participants who had guarding on physical examination had significant association with unfavourable treatment outcome. Similar findings were observed at Black Lion Hospital,25 and Goba Hospital.26 This is owing to the patient’s aversion to have their abdomen handled due to peritoneal inflammation and irritation, a condition known as guarding. It is one of the physical sign of patients with local or generalized peritonitis.
Strengths and Limitations of the Study
This study will have an advantage by providing baseline information about non-traumatic acute abdomen magnitude, patterns, and treatment outcomes. The limitation of the study is that it will not represent the whole study since it is an institution-based study and does not show long-term complications. Besides to this, using the retrospective design is one of the main limitation of this study, as it is difficult to extrapolate the results.
Conclusions
The findings of this study showed that the magnitude of unfavorable treatment outcomes for non-traumatic acute abdomen was found to be high. The majority of patients who encountered post-operative problems had acceptable treatment outcomes, and most were connected to developing peritonitis and complex appendicitis. Presence of postoperative complications, having temperature ≥37.5°C, and having abdominal guarding were statistically significant factors associated with treatment outcome of non-traumatic acute abdomen. Hence, all level medical workers should give more attention on infection prevention in the ward and in the operating room, since wound infection and pneumonia were frequent post-operative complications linked to management results.
Abbreviation
AOR, Adjusted Odds Ratio; BDU, Bahir Dar University; COR, Crude Odds Ratio; CI, Confidence Interval; CMHS, College of Medicine and Health Sciences; GSBV, Gangrenous Small Bowel Volvulus; GSV, Gangrenous Sigmoid Volvulus; ETB, Ethiopian birr; IO, Intestinal Obstruction; IV, Intravascular; LBO, Large Bowel Obstruction; MRN, Medical Record Number; NG, Nasogastric; PPUD, Perforated peptic ulcer disease; SBO, Small Bowel Obstruction; SD, Standard Deviation; SPSS, Statistical Package for Social Science; SSI, Surgical Site Infection; SSV, Simple Sigmoid Volvulus; TGSH, Tibebe Ghion Specialized Hospital; WHO, World Health Organization.
Data Sharing Statement
All relevant data are within the manuscript and its Supporting Information files.
Ethical Consideration
Ethical approval was obtained from the Institutional Review Board (IRB) of Bahir Dar University, College of Medicine and Health Sciences with reference number 558/2022. The IRB of Bahir Dar University allowed us to collect the data from medical records without collecting personal identifiers including name and they waived the requirement for informed consent. The authors had no access to information that could identify individual participants after data collection. A formal letter was written by the medical director that allowed us to collect the data and conduct this study. The data was obtained using a structured questionnaire checklist filled from the medical record of the patient. The patient chart was kept secured or confidential and the personal identifiers such as name not be extracted. Data obtained in the course of study was only handled by the research team. Information was used as aggregated after analysis of whole data.
Acknowledgment
We would like to thank the staff of Tibebe Ghion Specialized Hospital for giving valuable information and permission. We want to give our special thanks to the data collectors, and supervisors. Finally, it is our pleasure to give our deepest thanks to our family for their contributions and patience throughout this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Faiz O, Banerjee S, Tekkis P, et al. We still need to operate at night. World J Emerg Surg. 2008;2(1):29. doi:10.1186/1749-7922-2-29
2. Berhane Y, Girmay K, Gebresilassie A. Outcome of emergency surgical operations performed for non-traumatic acute abdomen among adults in Mekelle hospital, Tigray, Ethiopia, 2013. Eur J Pharm Med Res. 2016;Vol. 3:106–111.
3. Mohammed K. Treatment of sigmoid volvulus: experience in Gondar, North west Ethiopia. EMJ. 1998;36(1):47–52.
4. Nyundo M, Rugwizangoga E, Ntakiyiruta G, Kakande I. Outcome of emergency abdominal surgery at Kigali University teaching hospital: a review of 229 cases. East Central Afr J Surg. 2013;18:1.
5. Hosbey M. An approach to the acute abdomen. In: Faruk H, editor. Pathways in Surgical Management.
6. Daniel E, Melaku G, Yoo MC, Agezew Y, Gebre W. Analysis of surgical admission to the Ethio-Swedish Children’s Hospital in A/Ababa. EMJ. 1990;28(1):15–22.
7. Tsegaye S, Osman M, Bekele A. Surgically treated acute abdomen at Gondar University hospital, Ethiopia. East Cent Afr J Surg. 2006;12:53–57.
8. Deneke A, Tadesse B. Incidence, patterns and clinical presentation of acute appendicitis in adults at (ZMH). Ethiop J Health Sci. 2003;13:122–130.
9. Awori MN, Jani PG. Surgical implications of abdominal pain in patients presenting to the Kenyatta national hospital casualty department with abdominal pain. East Afr Med J. 2005;82(6):307–310. doi:10.4314/eamj.v82i6.9302
10. Ohene-Yeboah M. Acute surgical admissions for abdominal pain in adults in Kumasi, Ghana. ANZ J Surg. 2006;76(10):898–903. doi:10.1111/j.1445-2197.2006.03905.x
11. McConkey MB. Case series of acute abdominal surgery in rural Sierra Leone. World J Surg. 2002;26(4):509–513. doi:10.1007/s00268-001-0258-2
12. Soressa U, Mamo A, Hiko D, Fentahun N. Prevalence, causes and management outcome of intestinal obstruction in Adama Hospital, Ethiopia. BMC Surg. 2016;16(1):38. doi:10.1186/s12893-016-0150-5
13. Postier RG, Squires RA. Acute abdomen. In: Sabiston Textbook of Surgery.
14. Sharma AK, Sharma RK, Sharma SK, Sharma A, Soni D. Typhoid intestinal perforation: 24 perforations in one patient. Ann Med Health Sci Res. 2013;3(5):112–115. doi:10.4103/2141-9248.121220
15. Zelalem A. Pattern of acute abdomen in Yirgalem Hospital, southernEthiopia. Ethiop Med J. 2000;38(4):227–235.
16. Kotiso Y, Abdurahman Z. Pattern of acute abdomen in adult patients in Tikur Anbessa teaching hospital, Addis Ababa, Ethiopia. East Central Afr J Surg. 2007;12:47–52.
17. Johnson LP. Recent experience with sigmoid volvulus in Ethiopia: its incidence and management by primary resection. EMJ. 1966;4:197–201.
18. Ayenew Z, Gizaw AT, Workneh D, Fentahun N. Outcome of non-traumatic surgical acute abdomen in nekemte referral hospital, Southwest, Ethiopia: a retrospective cross-sectional study. Surgery Curr Res. 2016;7:282.
19. Mekuanint N. Assessment of non traumatic acute abdominal cases treated operatively at Wolaita Sodo teaching hospital, Southern Ethiopia; 2017. Int Peer Rev J. 2017;1:22.
20. Ray S, Patel M, Parmar H. Management of acute abdomen: study of 110 cases. IAIM. 2016;3:18–24.
21. Adesunkanmi AR, Agbakwuru EA. Changing pattern of acute intestinal obstruction in a tropical African Population. East Afr Med J. 2006;73:727–731.
22. Gebrie TA, Handiso TB, Hagisso SN. Management outcome and associated factors of surgically treated non-traumatic acute abdomen at Attat hospital, Gurage zone, Ethiopia. Int J. 2019;6:99.
23. Samuel JC, Qureshi JS, Mulima G, et al. An observational study of the etiology, clinical presentation and outcomes associated with peritonitis in Lilongwe, Malawi. World J Emerg Surg. 2011;6(1):2–5. doi:10.1186/1749-7922-6-37
24. Muhammad TA, Asma H, Waqar SH, Shah SF, Zafar IM, Zahid MA. Presentation and outcome of acute abdomen in a tertiary care unit. AnnPak Inst Med Sci. 2011;7:137.
25. Msrujan K, Magrini S, Tacconi L. The non-traumatic acute abdomen and its clinical spectrum, Andhra Pradesh, India. Inter Surg J. 2019;5(2):e42–e45. doi:10.1055/s-0039-1693082
26. Tassew B, Haile MT, Tefera TB, et al. Presentation and outcome of acute abdomen in Goba referral hospital, Goba, Southeast Ethiopia: retrospective Study. SM J Fam Med. 2017;1:1003.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.