")
Back to Journals » Research and Reports in Urology » Volume 15
Treatment Landscape for Metastatic Castrate-Sensitive Prostate Cancer: A Review
Authors Meagher MF, Salmasi A, Stewart TF
Received 11 July 2023
Accepted for publication 3 November 2023
Published 13 November 2023 Volume 2023:15 Pages 509—517
DOI https://doi.org/10.2147/RRU.S398129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Panagiotis J Vlachostergios
Margaret F Meagher,1 Amirali Salmasi,1 Tyler F Stewart2
1Department of Urology, University of California San Diego, La Jolla, CA, USA; 2Division of Hematology-Oncology and BMT, University of California San Diego, La Jolla, CA, USA
Correspondence: Tyler F Stewart, Tel +1 (866) 773-2703, Email [email protected]
Abstract: With the advent of new therapeutic modalities, management of metastatic castrate-sensitive prostate cancer (mCSPC) has been in flux. From androgen-deprivation therapy to docetaxel to androgen receptor–signaling inhibitors, each agent has heralded a new treatment paradigm. As such, the optimal first-line therapy for mCSPC remains incompletely defined. This review provides a narrative of recent advances to systemic therapy within the mCSPC treatment space, particularly with regard to expansion to triplet therapy.
Keywords: metastatic, castrate-sensitive prostate cancer, darolutamide
Introduction
Treatment of metastatic castrate-sensitive prostate cancer (mCSPC) has evolved dramatically over the past 20 years. In the early 21st century, treatment of advanced prostate cancer relied upon androgen ablation via either surgical castration or neutralization through estrogen administration.1,2 Increased understanding of the androgen pathways led to the development of new means of androgen-deprivation therapy (ADT) by manipulating various aspects of testosterone production.3,4 Continuous administration of luteinizing hormone-releasing hormone (LHRH) agonists along with an induction course of antiandrogen therapy or continuous treatment with LHRH antagonists are the contemporary backbones of ADT for locally advanced and metastatic disease.5,6 In select cases, intermittent ADT may also be employed.
Despite initial response to ADT, patients with initial castrate-sensitive disease will progress to castrate-resistant prostate cancer (CRPC).7 CRPC portends poor outcomes with a mean survival time of about 30 months in the metastatic setting.8 As new agents demonstrated therapeutic benefit for patients with CRPC, multiple studies investigated these agents in the CSPC space (Table 1).
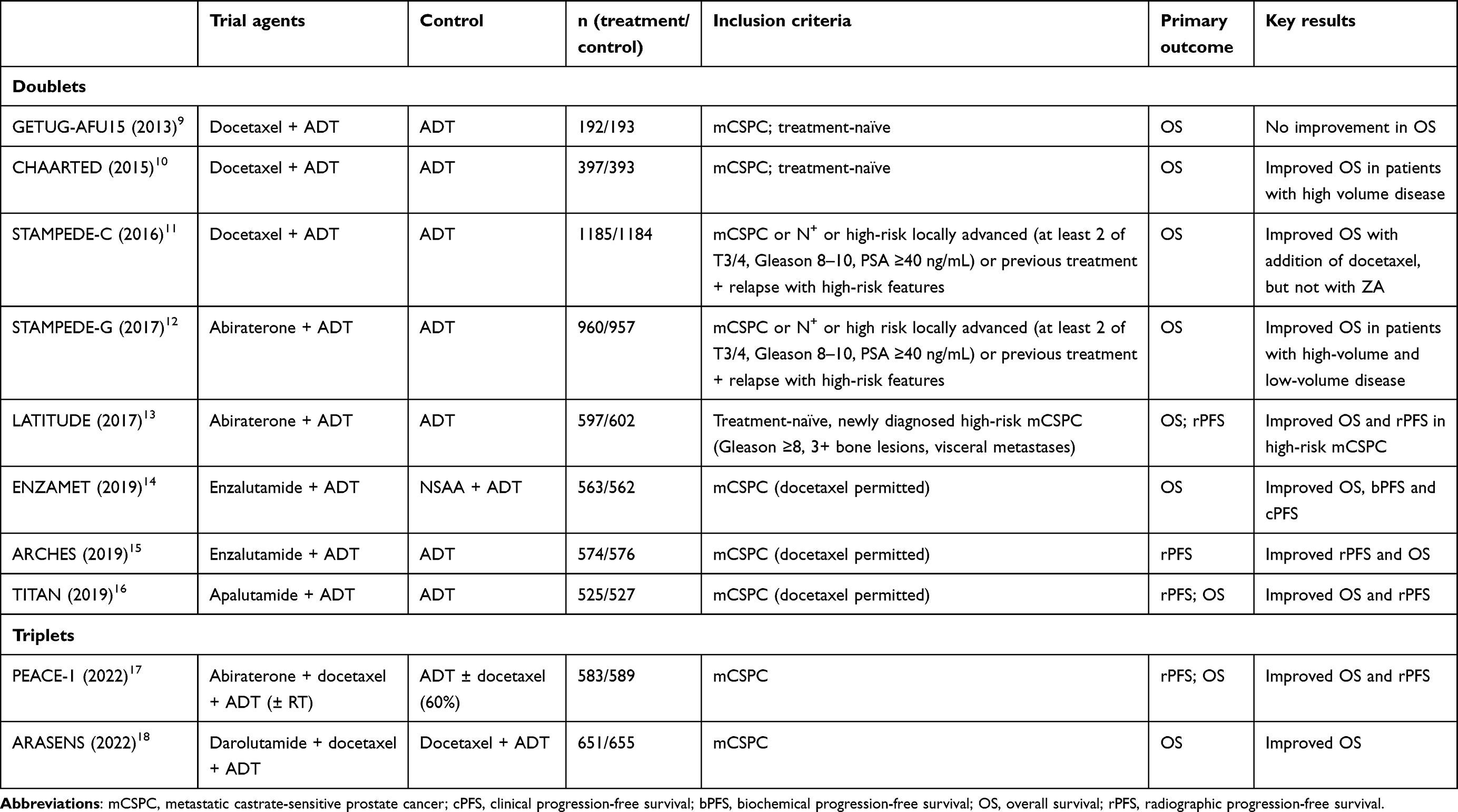 |
Table 1 Completed clinical trials in mCSPC |
ADT Plus Docetaxel for mCSPC
In 2004, the FDA approved the chemotherapeutic agent docetaxel for treatment of CRPC.19,20 The survival benefits of docetaxel inspired multiple studies investigating the addition of docetaxel in the treatment of mCSPC. The GETUG-AFU15 study included 385 patients, enrolled from 2004 to 2008, and compared the combination of ADT plus docetaxel versus ADT alone.9 This trial did not demonstrate a significant increase in overall survival (OS; HR 1.01, p=0.955). However, on the heels of the CHAARTED data (see below), a post hoc analysis was performed using the CHAARTED definition of low- and high-volume disease burden. Based on this, there was a non–statistically significant 20% reduction in mortality (HR 0.78, 95% CI 0.56–1.09; p=0.14). No benefit was observed for patients with low-volume disease.21
CHAARTED was a randomized trial investigating 790 patients with mCSPC that evaluated addition of docetaxel to ADT vs ADT alone.10 This study stratified patients according to extent of disease: high volume (defined as the presence of visceral metastases or four or more bone lesions with one or more beyond the vertebral bodies and pelvis) vs low volume. CHAARTED demonstrated an improvement in OS (HR 0.61, 95% CI 0.47–0.80; p<0.001). With more mature follow-up, the benefit was more apparent for patients with high-volume disease (HR 0.63, 95% CI 0.50–0.79; p<0.001) rather than low-volume disease (HR 1.04, 95% CI 0.70–1.55; p=0.86).22
Similarly, STAMPEDE investigated the use of up-front docetaxel for CSPC. The trial enrolled patients with metastatic and nonmetastatic disease and compared the addition of both docetaxel and zoledronic acid in a 2×2 design. Docetaxel was associated with an improvement in OS.11 Interestingly, in a post hoc analysis of patients with metastatic disease only and classifying patients by CHAARTED volume criteria, the benefit of docetaxel appeared to be similar for patients with high-volume disease (OS HR 0.81, 95% CI 0.64–1.02; p=0.064) and low-volume disease (OS HR 0.76, 95% 0.54–1.07; p=0.107).12 Together, these trials heralded in a new era of ADT + docetaxel as the new standard of care for early mCSPC, particularly for patients with high-volume disease.23,24
ADT Plus Novel Hormonal Agents for mCSPC
Similarly to the benefits of docetaxel in the CRPC space, novel androgen receptor–signaling inhibitors (ARSIs) were also demonstrated to improve OS for patients with CRPC. Abiraterone, which inhibits CYP17 and halts the production of androgens, was shown to prolong survival in the setting of CPRC.25,26 In light of this, both STAMPEDE and LATITUDE investigated the role of abiraterone in combination with ADT for patients with mCSPC. STAMPEDE demonstrated a benefit in OS in patients with metastatic disease (HR 0.61, 95% CI 0.49–0.75).27 In 2020, an updated analysis using the CHAARTED criteria for stratification demonstrated improved OS for both high-volume (HR 0.59,95% CI 0.47–0.74; p<0.001) and low-volume disease (HR 0.59, 95% CI 0.47–0.74; p<0.001).27 These results were affirmed by the LATITUTE trial, which evaluated 1199 patients with “high-risk” mCSPC (defined as having at least two of three criteria: Gleason score ≥8, three or more bone lesions, and/or visceral metastases) and evaluated ADT plus abiraterone vs ADT plus placebo. OS was significantly improved with abiraterone (HR 0.62, 95% CI 0.51–0.76; p<0.001).13 In a post hoc analysis of the STAMPEDE trial using the LATITUDE risk criteria, the combination of abiraterone plus ADT appeared to benefit both groups of patients (high-volume and low-volume disease).28
Three secondary ARSIs have shown benefit for CRPC, leading to investigating their role for patients with mCSPC: enzalutamide, apalutamide, and darolutamide.8,29–35 Enzalutamide was investigated in the hormone-sensitive setting in the ENZAMET and ARCHES trials. ENZAMET randomized 1125 patients to enzalutamide plus ADT vs a nonsteroidal antiandrogen drug (bicalutamide, nilutamide, flutamide) plus ADT, and found improvement in OS (HR 0.67, p=0.002), progression-free survival (PFS; HR 0.39, p<0.001), and clinical PFS (HR 0.40, p<0.001) with enzalutamide.14 Importantly, this trial included patients who may also have been receiving early docetaxel therapy (45%). For patients who received early docetaxel, the OS HR was 0.90 (95% CI 0.62–1.31), suggesting that for patients who are planned for docetaxel, the addition of enzalutamide may not be beneficial. The addition of enzalutamide, however, also increased the frequency of serious toxic effects (68.4% vs 41.8%), which was potentiated by the addition of early docetaxel treatment. The beneficial effect of enzalutamide was also demonstrated in the ARCHES trial, where the combination was associated with improved OS (HR 0.66, 95% CI 0.53–0.81).15 On subgroup analysis, those who had received prior docetaxel (18%) had improved radiographic PFS and there was a suggestion of improved OS (HR OS 0.74, 95% CI 0.46–1.20).36
Apalutamide is mechanistically similar to enzalutamide and was investigated in the setting of concomitant ADT for mCSPC in the TITAN trial.16 Radiographic PFS at 2 years was 68.2% in the apalutamide group versus 47.5% in the placebo group (HR 0.48, p<0.001). Similarly to the ARCHES trial, this beneficial effect was favorable across all subgroups including previous docetaxel (11%) exposure along with both CHAARTED and LATITUDE disease criteria. In the updated survival analysis with a median follow-up for the entire cohort of 44 months, the addition of apalutamide reduced the risk of death by 35% (OS HR 0.65, 95% CI 0.53–0.79; p<0.0001). In the subgroup of patients that received prior docetaxel, there did not appear to be a benefit from adding enzalutamide (OS HR 1.12, 95% CI 0.59–2.12); however, the authors noted that limited conclusions should be made for the combination of apalutamide and docetaxel, given the small number of patients for this analysis.37
Together, these data have demonstrated overwhelming evidence of the beneficial effect of the addition of an ARSI agent to ADT for both low-volume and high-volume mCSPC. To this end, the NCCN guidelines now recommend each of these combinations for patients with mCSPC while discouraging single-agent ADT, unless there are clear contraindications for combination therapy.38
ADT Plus Docetaxel and Novel Hormonal Agents for mCSPC
In 2022, PEACE-1 heralded a new investigation era of triplet therapy. PEACE-1 was a multicenter randomized trial with a 2×2 factorial design investigating the addition of abiraterone and/or radiotherapy for primary lesions in men with de novo mCSPC compared to SOC.17 During accrual, the study was amended to allow for prior use of docetaxel, and subsequently docetaxel was required so that the study could investigate if the addition of abiraterone improved outcomes compared to ADT plus docetaxel alone. In total, 1173 were enrolled, with 60% receiving ADT plus docetaxel. PEACE-1 demonstrated improved radiographic PFS (HR 0.54, p<0.0001) and OS (HR 0.82, p=0.030) with the addition of abiraterone. Specifically, in the subgroup receiving ADT plus docetaxel, abiraterone demonstrated improved rPFS (HR 0.50, 95% CI 0.34-0.71; p≤0.0001) and OS (HR 0.75, 95% CI 0.59–0.95; p=0.017). Toxicity rates between the treatment and control arms were similar, except for increased rates of hypertension with abiraterone (22% vs 13%). This trial led to changes in guidelines and practice, as patients who were planned to receive docetaxel could also be considered for escalation with the addition of abiraterone.
The most recent ARASENS trial investigated triplet therapy with darolutamide, ADT, and docetaxel vs doublet therapy with ADT and docetaxel.18 The study included 1306 patients with mCSPC. ARASENS demonstrated an improvement in OS with the addition of darolutamide to ADT plus docetaxel (HR 0.68, p≤0.001) and delay in the time to castrate-resistant disease. In a post hoc subgroup analysis based on both CHAARTED and LATITUDE risk stratification, the addition of darolutamide improved OS in patients at high and low risk, as well as high-volume disease. For patients with low-volume disease, there was a suggestion of OS benefit; however, data remain immature.
Doublet versus Triplet
Data from PEACE-1 and ARASENS demonstrate that men with mCSPC should all receive escalation of therapy with a secondary hormonal agent unless there is a clinically compelling reason to avoid this. However, the additional benefit of docetaxel in the up-front treatment for mCSPC remains uncertain. A recent network meta-analysis by Riaz et al aimed to analyze the benefit of enhanced therapy.39 Their work demonstrated that triplet combinations with ADT, docetaxel, and either abiraterone or darolutamide were associated with improved OS compared to ADT and docetaxel, but the triplet did not improve OS compared to ADT + ARSI. When this was broken down by volume of disease, the triplet (data only including abiraterone) improved OS compared to ADT plus docetaxel, but not compared to ADT plus ARSI alone. For patients with low-volume disease, the triplet was not associated with improvements compared to the doublet, raising some doubt about the benefit of docetaxel in addition to ARSI in the frontline space.
Clinically, it may be reasoned that those with high-risk features may benefit from triplet therapy, but no clinical trial has prospectively demonstrated this. In a recent meta-analysis by the STOPCAP Collaboration of the GETUG AFU15, STAMPEDE, and CHAARTED trials performed, all of which investigated docetaxel plus ADT vs ADT alone for patients with mCSPC, Vale et al highlighted characteristics of patients who gain the most significant benefit from docetaxel, including clinical T stage, higher volume of metastases, and to a lesser extent synchronous metastases (vs metachronous).40 The group plans to use these data to analyze which patients are most likely to benefit from the addition of docetaxel, which may provide further clarity.
Optimal First-Line Therapy in a Changing Landscape
The optimal first-line choice of therapy must be taken into the context of a rapidly evolving field, with newer technologies and treatment. For instance, application of CHAARTED or LATITUDE disease stratification requires a CT scan and bone imaging with a nuclear medicine bone scan. However, PSMA PET/CTs are increasingly standard approaches for staging. PSMA PET/CTs significantly change staging for prostate cancer, identifying metastatic disease in patients who would otherwise be deemed nonmetastatic and identifying higher disease burden than previously identified by CT and bone scans. Patients undoubtedly deemed “high-volume” based on PSMA PET/CTs have “low-volume” disease based on CT and bone scan imaging. Clinicians using PSMA PET/CTs predominantly may need to consider CT scans and nuclear medicine bone scans for borderline cases to identify patients most likely (and least likely) to benefit from the addition of docetaxel. The addition of docetaxel without clear clinical benefit should not be taken lightly, as docetaxel is associated with toxicity. In PEACE-1, docetaxel was associated with neutropenia in 10% of patients and febrile neutropenia in 5%.17 Although the magnitude of benefit for up-front docetaxel in addition to ARSI remains a relevant question, it is not clear if there is an appetite in the prostate cancer community to perform a large study to evaluate this in the context of newer technologies.
Currently, for patients with metastatic hormone-sensitive prostate cancer, a combination of ADT and ARSI is the standard of care (Figure 1). Although single-agent ADT may be considered in some, based on the abundant evidence of combination therapy, there usually has to be a compelling reason not to offer an ARSI. No specific ARSI has been shown to be superior to the others, so often the specific ARSI is determined by availability, comorbidities, and drug–drug interactions. For patients with high-volume disease and particularly those with de novo high-volume disease, the addition of up-front docetaxel is very reasonable; however, the absolute benefit of the addition of docetaxel remains unknown. In addition to systemic therapy, for patients with de novo low-volume disease as per CHAARTED criteria, radiation to the prostate should strongly be considered, as this has been shown to improve OS.41
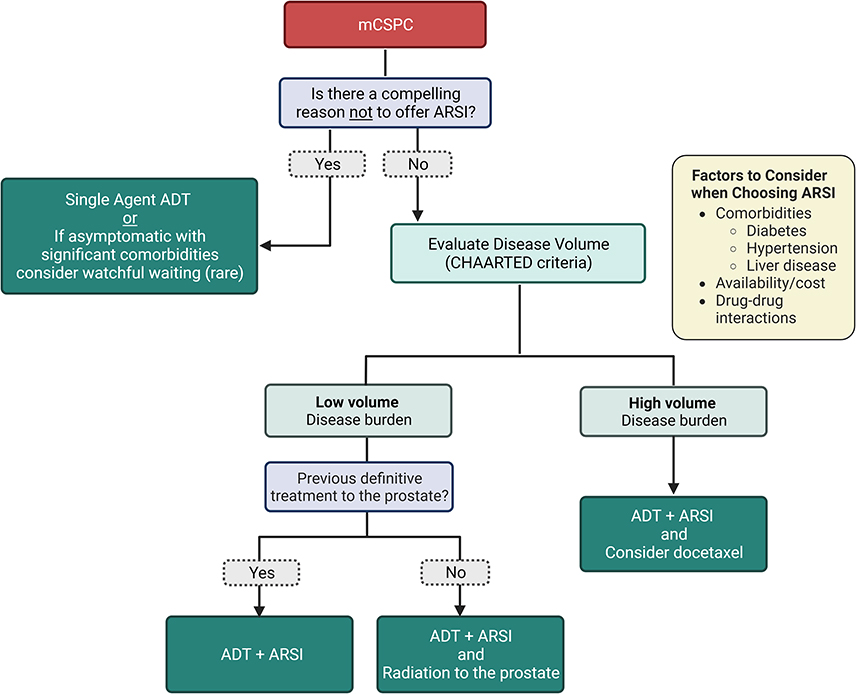 |
Figure 1 Treatment algorithm for mCSPC. |
The Future Landscape for mCSPC
The landscape for mCSPC will evolve over the next few years. Agents that are now approved for mCRPC are currently in clinical trials in the hormone-sensitive space, while novel combinations are under investigation (Table 2).42–47
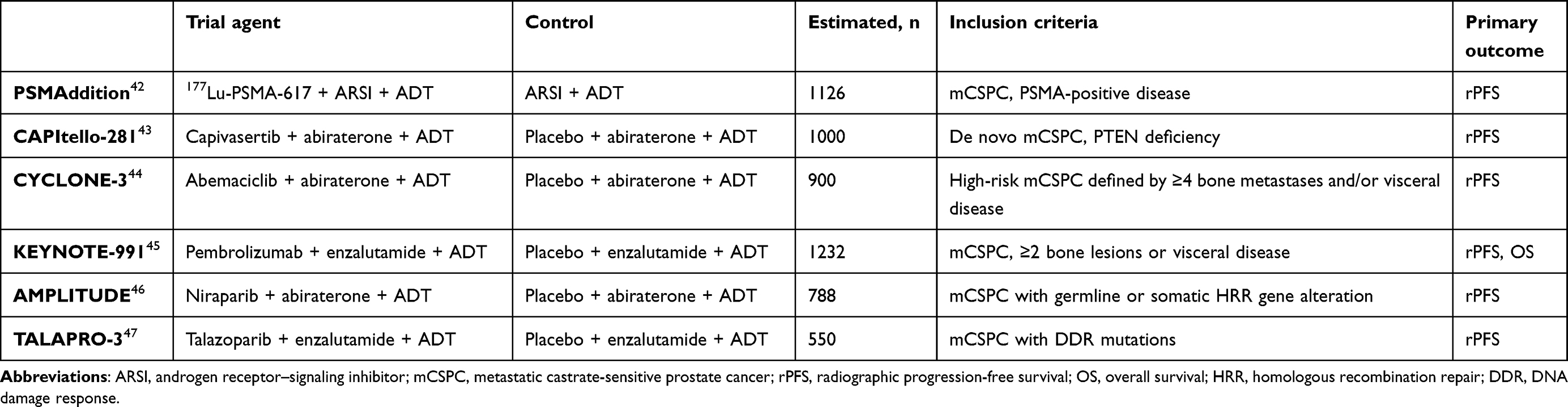 |
Table 2 Selected ongoing phase III clinical trials in the mCSPC setting |
Poly(ADP-ribose) polymerase inhibitors (PARPIs) prevent repair of single-stranded DNA breaks promoting conversion to double-stranded breaks. PARPIs have demonstrated significant clinical benefit for patients with mCRPC that harbors homologous recombination repair mutations, either somatic or germline.48–52 More recently, combinations of ARSI with PARPIs have demonstrated OS benefit compared to ARSI patients.53–55 Although there remains controversy as to whether this benefit is limited to patients who harbor BRCA1/2 mutations, any homologous recombination repair mutation, or if this benefit is seen in all patients with mCRPC, combination ARSIs plus PARPIs certainly benefit some patients. Based on this, frontline trials are now exploring the combination of PARPIs with ARSIs for patients with mCSPC.
Possibly the most exciting advance for mCRPC has been radiotheranostics. Radioligand therapies deliver radiation therapy to the cell that contains the target while sparing normal cells. This is often delivered with either α or β particles, with α particles being larger and able to inflict more damage than β particles. In 2013, radium 223 was approved for patients with mCRPC without visceral disease after demonstrating improvement in OS and decreased time to symptomatic skeletal event compared to placebo.56 Lutetium 177–PSMA-617 (Lu-PSMA) is a radioligand therapy that delivers β-particle radiation to cells that express PSMA. In the Vision trial, Lu-PSMA demonstrated improvement in PFS and OS compared to an alternative ARSI agent for patients with mCRPC, leading to its FDA approval. Additionally, the TheraP trial demonstrated improvement in response rate, decreased adverse events, and similar OS compared to cabazitaxel.57,58 While novel radiotheranostics are currently in trial for patients with mCRPC, the field is eagerly awaiting the results of the PSMAddition study, which is investigating the role of up-front LuPSMA in addition to ADT plus ARSI for patients with mCSPC.
Additional novel methods to improve long-term outcomes for patients with mCSPC are currently in development or already in clinical trials. These include novel therapeutic combinations, including those investigating alternative compelling molecular pathways (PTEN, CDK4/6). More studies will be evaluating the role of radiation-directed therapy to oligometastatic sites. Finally, there will be studies looking at de-escalation of therapy, including the use of intermittent therapy for patients with excellent response to systemic therapy. If (or when) multiple studies in the frontline space are positive, cross-trial comparison will be even more difficult and selecting the optimal treatment plan will become more nuanced, with treatment determined by genomics, volume of disease, and individualized based on patients’ goals.
Conclusion
The treatment landscape for mCSPC has significantly evolved, offering patients and providers a range of options to consider. Therapy with ADT plus ARSIs has become the established frontline setting unless there is a significant competing reason to avoid ARSIs. The benefit of adding docetaxel to ADT and ARSIs is not yet proven, but should be considered in the context of various factors, including patient characteristics, disease burden, and individual treatment goals. Future research and ongoing clinical trials will continue to refine our understanding of optimal treatment strategies, ultimately improving outcomes and quality of life for patients with metastatic hormone-sensitive prostate cancer.
Acknowledgments
We would like to thank Dr Kit Yuen for assisting in the creation of Figure 1.
Disclosure
Dr Tyler F Stewart reports an MCC Cancer Center Support Grant (CCSG) as an Early-Stage Clinical Investigator during the conduct of the study, grants from GRAIL, and personal fees from Seattle Genetics, Astellas, and AstraZeneca outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Denmeade SR, Isaacs JT. A history of prostate cancer treatment. Nat Rev Cancer. 2002;2(5):389–396. PMID: 12044015; PMCID: PMC4124639. doi:10.1038/nrc801
2. Veurink M, Koster M, Berg LT. The history of DES, lessons to be learned. Pharm World Sci. 2005;27(3):139–143. doi:10.1007/s11096-005-3663-z
3. Labrie F, Dupont A, Belanger A, et al. New hormonal therapy in prostatic carcinoma: combined treatment with an LHRH agonist and an antiandrogen. Clin Invest Med. 1982;5(4):267–275. PMID: 6819101.
4. Conn PM, Rogers DC, Seay SG. Biphasic regulation of the gonadotropin-releasing hormone receptor by receptor microaggregation and intracellular Ca2+ levels. Mol Pharmacol. 1984;25(1):51–55.
5. Crawford ED, Hou AH. The role of LHRH antagonists in the treatment of prostate cancer. Oncology. 2009;23(7):626–630. PMID: 19626830.
6. Clinton TN, Woldu SL, Raj GV. Degarelix versus luteinizing hormone-releasing hormone agonists for the treatment of prostate cancer. Expert Opin Pharmacother. 2017;18(8):825–832. PMID: 28480768; PMCID: PMC7171911. doi:10.1080/14656566.2017.1328056
7. Eisenbergerg M, Blymenstein B, Crawford E, et al. Bilateral orchiectomy with or without flutamide for metastatic prostate cancer. N Engl J Med. 1998;339:1036–1042. doi:10.1056/NEJM199810083391504
8. Beer T, Armstrong A, Rathkopf D, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014;371:424–433. doi:10.1056/NEJMoa1405095
9. Gravis G, Fizazi K, Joly F, et al. Androgen-deprivation therapy alone or with docetaxel in non-castrate metastatic prostate cancer (GETUG-AFU 15): a randomised, open-label, Phase 3 trial. Lancet Oncol. 2013;14(2):149–158. doi:10.1016/S1470-2045(12)70560-0
10. Sweeney C, Chen Y-H, Carducci M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med. 2015;373:737–746. doi:10.1056/NEJMoa1503747
11. James ND, Sydes MR, Clarke NW. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage platform randomized controlled trial. Lancet. 2016;387(10024):1163–1177. doi:10.1016/S0140-6736(15)01037-5
12. Clarke NW, Ali A, Ingleby FC, et al. Addition of docetaxel to hormonal therapy in low- and high-burden metastatic hormone sensitive prostate cancer: long-term survival results from the STAMPEDE trial. Anna Oncol. 2019;30(12):1992–2003. doi:10.1093/annonc/mdz396
13. Fizazi K, Tran N, Fein L. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med. 2017;377:352–360. doi:10.1056/NEJMoa1704174
14. Davis ID, Martin AJ, Stockler MR. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med. 2019;381:121–131. doi:10.1056/NEJMoa1903835
15. Armstrong AJ, Szmulewitz RZ, Petrylak DP, et al. ARCHES: a randomized, phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2019;37(32):2974–2986. PMID: 31329516; PMCID: PMC6839905. doi:10.1200/JCO.19.00799
16. Chi KN, Agarwal N, Bjartell A, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med. 2019;381:13–24. doi:10.1056/NEJMoa1903307
17. Fizazi K, Foulon S, Carles J. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomized, phase 3 student with a 2x2 factorial design. Lancet. 2022;399(10336):1695–1707. doi:10.1016/S0140-6736(22)00367-1
18. Smith MR, Hussain M, Saad F. Darolutamide and survival in metastatic, hormone-sensitive prostate cancer. N Engl J Med. 2022;386:1132–1142. doi:10.1056/NEJMoa2119115
19. Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351:1502–1512. doi:10.1056/NEJMoa040720
20. Petrylak DP, Tangen CM, Hussain MH, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351:1513–1520. doi:10.1056/NEJMoa041318
21. Gravis G, Boher JM, Joly F, et al. Androgen deprivation therapy (ADT) plus docetaxel versus ADT alone in metastatic non castrate prostate cancer: impact of metastatic burden and long-term survival analysis of the randomized phase 3 GETUG-AFU15 trial. Eur Urol. 2016;70(2):256–262. doi:10.1016/j.eururo.2015.11.005
22. Kyriakopoulos C, Chen YH, Carducci M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer: long-term survival analysis of the randomized phase III E3805 CHAARTED trial. J Clin Oncol. 2018;36(11):1080–1087. doi:10.1200/JCO.2017.75.3657
23. Puente J, Grande E, Medina A, Maroto P, Lainez N, Arranz JA. Docetaxel in prostate cancer: a familiar face as the new standard in a hormone-sensitive setting. Ther Adv Med Oncol. 2017;9(5):307–318. PMID: 28529548; PMCID: PMC5424862. doi:10.1177/1758834017692779
24. Mottet N, van den Bergh RCN, Briers E, et al.: EAU Guidelines. Presented at the EAU Annual Congress Copenhagen, Denmark. Arnhem, The Netherlands: EAU Guidelines Office; 2018. Available from: https://uroweb.org/wp-content/uploads/EAU-ESUR-ESTRO-SIOG-Guidelines-on-Prostate-Cancer-large-text-V2.pdf.
25. Ryan CJ, Smith MR, Fizazi K, et al. Abiraterone acetate plus prednisone versus placebo plus prednisone in chemotherapy-naive men with metastatic castration-resistant prostate cancer (COU-AA-302): final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2015;16:152–160. doi:10.1016/S1470-2045(14)71205-7
26. de Bono JS, Logothetis CJ, Molina A, et al. Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med. 2011;364:1995–2005. doi:10.1056/NEJMoa1014618
27. James ND, de Bono JS, Spears MR. Abiraterone for prostate cancer not previously treated with hormone therapy. N Engl J Med. 2017;377:338–351. doi:10.1056/NEJMoa1702900
28. Hoyle AP, Ali A, James ND, et al. Abiraterone in “high-” and “low-risk” metastatic hormone-sensitive prostate cancer. Eur Urol. 2019;76(6):719–728. doi:10.1016/j.eururo.2019.08.006
29. Scher HI, Fizazi K, Saad F, et al.; AFFIRM Investigators. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med. 2012;367(13):1187–1197. doi:10.1056/NEJMoa1207506
30. Hussain M, Fizazi K, Saad F, et al. Enzalutamide in men with nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2018;378(26):2465–2474. doi:10.1056/NEJMoa1800536
31. Sternberg CN, Fizazi K, Saad F, et al. Enzalutamide and survival in nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2020;382(23):2197–2206. doi:10.1056/NEJMoa2003892
32. Smith MR, Saad F, Chowdhury S, et al. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med. 2018;378(15):1408–1418. doi:10.1056/NEJMoa1715546
33. Smith MR, Saad F, Chowdhury SO, et al. Apalutamide and overall survival in prostate cancer. Eur Urol. 2021;79(1):150–158. doi:10.1016/j.eururo.2020.08.011
34. Fizazi K, Shore N, Tammela TL, et al. Darolutamide in nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2019;380(13):1235–1246. doi:10.1056/NEJMoa1815671
35. Fizazi K, Shore N, Tammela TL, et al. Nonmetastatic, castration-resistant prostate cancer and survival with darolutamide. N Engl J Med. 2020;383(11):1040–1049. doi:10.1056/NEJMoa2001342
36. Amstrong A, Azad A, Iguchi T. Improved survival with enzalutamide in patients with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2022;40(15):1616–1622. doi:10.1200/JCO.22.00193
37. Chi KN, Chowdhury S, Bjartell A, et al. Apalutamide in patients with metastatic castration-sensitive prostate cancer: final survival analysis of the randomized, double-blind, phase III TITAN study. J Clin Oncol. 2021;39(20):2294–2303. doi:10.1200/JCO.20.03488
38. Schaeffer EM, Srinivas S, Adra N, et al. NCCN guidelines® insights: prostate cancer, version 1.2023. J Natl Compr Canc Netw. 2022;20(12):1288–1298. doi:10.6004/jnccn.2022.0063
39. Riaz I, Naqvi S, He H, et al. First-line systemic treatment options for metastatic castration-sensitive prostate cancer: a living systematic review and network meta-analysis. JAMA Oncol. 2023;9(5):635–645. doi:10.1001/jamaoncol.2022.7762
40. Vale C, Fisher D, Godolphin P, et al. Which patients with metastatic hormone-sensitive prostate cancer benefit from docetaxel: a systematic review and meta-analysis of individual participant data from randomized trials. Lancet. 2021;24(7):783–797. doi:10.1016/S1470-2045(23)00230-9
41. Burdett S, Boevé L, Ingleby F, et al. Prostate radiotherapy for metastatic hormone-sensitive prostate cancer: a STOPCAP systematic review and meta-analysis. Eur Urol. 2019;1(76):115–124. doi:10.1016/j.eururo.2019.02.003
42. Sartor A, Tagawa S, Saad F, et al. PSMAddition: a Phase 3 trial to compare treatment with 177Lu-PSMA-617 plus standard of care (SOC) versus SOC alone in patients with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2022;40(6_suppl):TPS210–TPS210. doi:10.1200/JCO.2022.40.6_suppl.TPS210
43. Fizazi K, George D, Santis M, et al. A phase III trial of capivasertib and Abiraterone versus placebo and Abiraterone in patients with de novo metastatic hormone-sensitive prostate cancer characterized by PTEN deficiency (CAPItello-281). J Clin Oncol. 2021;39:TPS178–TPS178. doi:10.1200/JCO.2021.39.6_suppl.TPS178
44. Smith MR, Nobuaki N, McKay R, et al. CYCLONE 3: a phase 3, randomized, double-blind, placebo-controlled study of abemaciclib in combination with Abiraterone plus prednisone in men with high-risk, metastatic, hormone-sensitive prostate cancer (mHSPC). J Clin Oncol. 2023;41:TPS289–TPS289. doi:10.1200/JCO.2023.41.6_suppl.TPS289
45. Gratzke C, Kwiatkowski M, De Giorgi U, et al. KEYNOTE-991: pembrolizumab plus enzalutamide and androgen deprivation for metastatic hormone-sensitive prostate cancer. Future Oncol. 2023. PMID: 36705526. doi:10.2217/fon-2022-0776
46. Rathkopf D, Chi K, Olmos D. AMPLITIDE: a study of niraparib in combination with Abiraterone acetate plus prednisone (AAP) versus AAP for the treatment of patients with deleterious germline or somatic homologous recombination repair (HRR) gene-altered metastatic castration-sensitive prostate cancer (mCSPC). J Clin Oncol. 2021;39:TPS176–TPS176.
47. Agarwal N, Azad A, Fizazi K, et al. TALAPRO-3: a phase 3, double-blind, randomized study of enzalutamide (ENZA) plus talazoparib (TALA) versus placebo plus enza in patients with DDR gene mutated metastatic castration-sensitive prostate cancer (mCSPC). J Clin Oncol. 2022;40(6_suppl):3301–3309. doi:10.1200/JCO.2022.40.6_suppl.TPS221
48. Johann de Bono MB, Mateo J, Fizazi K, et al. Olaparib for metastatic castration-resistant prostate cancer. N Eng J Med. 2020;382:2091–2102. doi:10.1056/NEJMoa1911440
49. Fizazi K, Piulats J, Reaume N. Rucaparib or physician’s choice in metastatic prostate cancer. N Eng J Med. 2023;388:719–732. doi:10.1056/NEJMoa2214676
50. Abida W, Campbell D, Patnaik A, et al. Rucaparib for the treatment of metastatic castration-resistant prostate cancer associated with a DNA damage repair gene alteration: final results from the phase 2 TRITON2 study. Eur Urol. 2023;84(3):321–330. doi:10.1016/j.eururo.2023.05.021
51. Smith M, Scher H, Sandhu S, et al. Niraparib in patients with metastatic castration-resistant prostate cancer and DNA repair gene defects (GALAHAD): a multicentre, open-label, phase 2 trial. Lancet Oncol. 2022;23(3):362–373. doi:10.1016/S1470-2045(21)00757-9
52. de Bono J, Mehra N, Scagliotti G, et al. Talazoparib monotherapy in metastatic castration-resistant prostate cancer with DNA repair alterations (TALAPRO-1): an open-label, phase 2 trial. Lancet Oncol. 2021;22(9):1250–1264. doi:10.1016/S1470-2045(21)00376-4
53. Clarke N, Armstrong A, Thiery-Vuillemin A, et al. Abiraterone and Olaparib for metastatic castration-resistant prostate cancer. NEJM Evid. 2022;1(9). doi:10.1056/EVIDoa2200043
54. Chi K, Rathkopf D, Smith M, et al. Niraparib and Abiraterone acetate for metastatic castration-resistant prostate cancer. J Clin Oncol. 2023;41(18):3339–3351. doi:10.1200/JCO.22.01649
55. Agarwal N, Azad A, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): a randomised, placebo-controlled, phase 3 trial. Lancet. 2023;402(10398):291–303. doi:10.1016/S0140-6736(23)01055-3
56. Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival and metastatic prostate cancer. N Engl J Med. 2013;369:213–223. doi:10.1056/NEJMoa1213755
57. Hofman M, Emmett L, Sandhu S, et al. [177Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): a randomized, open-label, phase 2 trial. Lancet. 2021;397(10276):797–804.
58. Hofman M, Emmet L, Sandhu S, et al. TheraP: 177 Lu-PSMA-617 (LuPSMA) versus cabazitaxel in metastatic castration-resistant prostate cancer (mCRPC) progressing after docetaxel—Overall survival after median follow-up of 3 years (ANZUP 1603). J Clin Oncol. 2022;40:5000. doi:10.1200/JCO.2022.40.16_suppl.5000
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.