")
Back to Journals » Research and Reports in Urology » Volume 15
Traumatic Kidney Injury: A 6-Year Retrospective Study in Childhood and Adolescence
Authors Palinrungi MA , Faruk M , Christeven R
Received 3 June 2023
Accepted for publication 12 August 2023
Published 20 September 2023 Volume 2023:15 Pages 415—424
DOI https://doi.org/10.2147/RRU.S424273
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Muhammad Asykar Palinrungi,1,2 Muhammad Faruk,3 Robert Christeven3
1Division of Urology, Department of Surgery, Faculty of Medicine, Universitas Hasanuddin, Makassar, Indonesia; 2Department of Urology, Universitas Hasanuddin Hospital, Makassar, Indonesia; 3Department of Surgery, Faculty of Medicine, Universitas Hasanuddin, Makassar, Indonesia
Correspondence: Muhammad Asykar Palinrungi, Division of Urology, Department of Surgery, Faculty of Medicine, Universitas Hasanuddin, Jalan Perintis Kemerdekaan KM 11, Makassar, 90245, Indonesia, Fax +62411587571, Email [email protected]
Background: Traumatic kidney injuries are the most common urinary tract injuries. Pediatric patients are more susceptible to renal injury from blunt trauma than adults because of anatomic factors. The aim of this publication was to provide a reference for traumatic kidney injury in the pediatric group based on the study in our center.
Methods: A retrospective study was conducted from January 2014 to December 2019 to review medical records of children admitted with renal trauma. Relevant findings including demographics, mechanisms and grades of injury, clinical parameters, interventions, and outcomes were recorded.
Results: Thirty-three pediatric patients were investigated. Males experienced traumatic kidney injury more often than the females with a ratio of 10:1. Most cases occurred during the adolescent (12– 18) years (81.82%). Left-side kidney injury (63.64%) was more frequent than right side (36.36%). Most cases (96.97%) were caused by blunt trauma, mainly traffic accidents (81.82%). Most patients (90.91%) had stable hemodynamics. Grade IV kidney injury was the most frequently found injury (39.39%). The cause of renal function disturbance was based on the blood urea nitrogen/creatinine (BUN/Cr) ratio with 21.87% of patients suffering from intra-renal causes and 12.5% from pre-renal causes. No significant association between different grades and BUN/creatinine ratio was found. Isolated renal injuries were found in 54.54% of patients. Most patients were treated conservatively (87.88%), and survival was 96.97%.
Conclusion: Non-operative management is safe and yields good outcomes in kidney trauma patients with stable hemodynamics. Renal trauma severity is not associated with the BUN/Cr ratio.
Keywords: pediatric, trauma injuries, kidney trauma, non-operative management
Background
Trauma injuries are a prominent cause of death among children and adolescents.1,2 Traumatic kidney injuries are the most common urinary tract injuries.3 Pediatric patients are more susceptible to renal injuries from blunt trauma than adults because of several pediatric anatomic factors, including less perirenal fat, weaker abdominal musculature, more immature pliable thoracic cage, and lower position of the kidney in the abdomen than in adult counterparts, which leads to less protection to the kidney.3–7 Furthermore, the kidneys are supported in their position in the body cavity by the vascular pedicle and the ureter (especially ureteropelvic junction) and are surrounded by capsule, Gerota’s fascia, and perirenal fat.6
In accordance with the National Trauma Data Bank, the review study from Grimsby et al8 concerning 2213 pediatric kidney injuries showed that the most renal trauma in children was found to be low grade (79%) and blunt (>90%). The average age at the time of injury was 13.7 years with 94% of the patients in the age range of 5 to 18 years old. About 79% of injuries were low-grade injuries (grade I, II, or III). Penetrating injury was accounted for less than 10% of all patients. Nephrectomy was performed in 122 (5.5%) cases.8
The kidney injuries are graded according to the severity assessment, which was classified by the American Association for the Surgery of Trauma (AAST) Organ Injury Scale.9 The contemporary guidelines of pediatric kidney trauma management are based on these limited references.8 Additional studies to support the establishment of evidence-based recommendations are imperative. The aim of this publication was to provide a reference for traumatic kidney injury in the pediatric group based on the study in our center, including the incidence, patient’s characteristics, etiology, mechanism of injury, clinical features, associated injuries, management, and outcomes.
Methods
A retrospective study was conducted in our tertiary referral center hospitals of East Indonesia (Wahidin Sudirohusodo and Universitas Hasanuddin Hospitals) to identify and review data from medical records of the children admitted with renal trauma from January 2014 to December 2019. Relevant findings, including demography, mechanism of injury, clinical parameters, kidney injury grade, laboratory parameters, interventions, and outcomes, were recorded. The hospital care included observation with close monitoring of vital signs and relevant medications, such as analgesics and intravenous antibiotics. After discharge from the hospital, the children were followed in our outpatient clinics.
The severity of renal injury was graded according to American Association for the Surgery of Trauma (AAST) classification by assessment from computed tomography (CT) and operative findings. For clinical purposes, grades I–III were classified as low grade, and grades IV and V were classified as high grade.9–11
Gross hematuria was determined by documentation of the visible color of the urine, while microscopic hematuria was defined as four or more red blood cells per high-power field (RBCs/HPF) based on the clinical laboratory report.12 Hemodynamic stability was assessed using several parameters, including blood pressure, heart and peripheral pulse rates, capillary refill time, and urine output.13
Blunt trauma can be defined as an injury to the body caused by forceful impact/injury, or physical attack with a dull object or surface.11,14 On the other hand, penetrating trauma is an injury in which an object or surface pierces the body, causing an open wound.15–17
The complete blood counts were determined using a Sysmex XP-300™ (Sysmex; Kobe, Japan) according to the manufacturer’s instructions. Renal function was measured using the Cobas® 8000 modular analyzer series (Roche Diagnostics, Indianapolis, IN, USA) according to the manufacturer’s instructions.
The typical range for hemoglobin is 11.0 to 14.5 g/dl.18 The cut-off value of normal blood urea nitrogen in pediatric patients was determined as ≤18 mg/dl.19 The cause of renal function impairment was determined from the blood urea nitrogen/creatinine ratio (BUN/Cr) ratio and divided into several categories: (1) prerenal (>20:1), (2) normal/postrenal (12–20:1), and (3) intrarenal (<12:1). The hypothesis in this study stated that the severity of renal trauma may affect the BUN/Cr ratio.
Kidney injury was managed by either non-operative management (NOM), nephrorrhaphy, or nephrectomy. The data were provided with the assistance of IBM Statistical Package for the Social Sciences version 25 (IBM Corp., Armonk, NY, USA) and Microsoft Excel applications 2013 (Microsoft, USA). An analysis of the association between kidney injury grade and BUN/Cr ratio was conducted using the Mann–Whitney U-test.
Results
A total of 33 pediatric patients with traumatic kidney injury from January 2014 to December 2019 were admitted (Table 1) (Figure 1). The most frequent cases were found in 2018 with 11 cases (33.33%). Males underwent traumatic kidney injury more often than the females with a ratio of 10:1. Most cases were found during the adolescence years (12–18 years) with 27 cases (81.82%). The mean age was 14 years old, while the oldest and youngest ages were 18 and 5 years, respectively. Left-side kidney injury (63.64%) was more frequent than the right side (36.36%). Most cases (96.97%) were caused by blunt trauma. Traffic accidents were the main cause of traumatic kidney injuries with 27 cases (81.82%). Most patients experienced flank pain (90.91%) and gross hematuria (72.73%). Most of the patients were admitted to the emergency room with stable hemodynamics (90.91%). Grade IV kidney injury was the most frequently found injury (39.39%). Isolated renal injuries were found in 18 patients (54.54%).
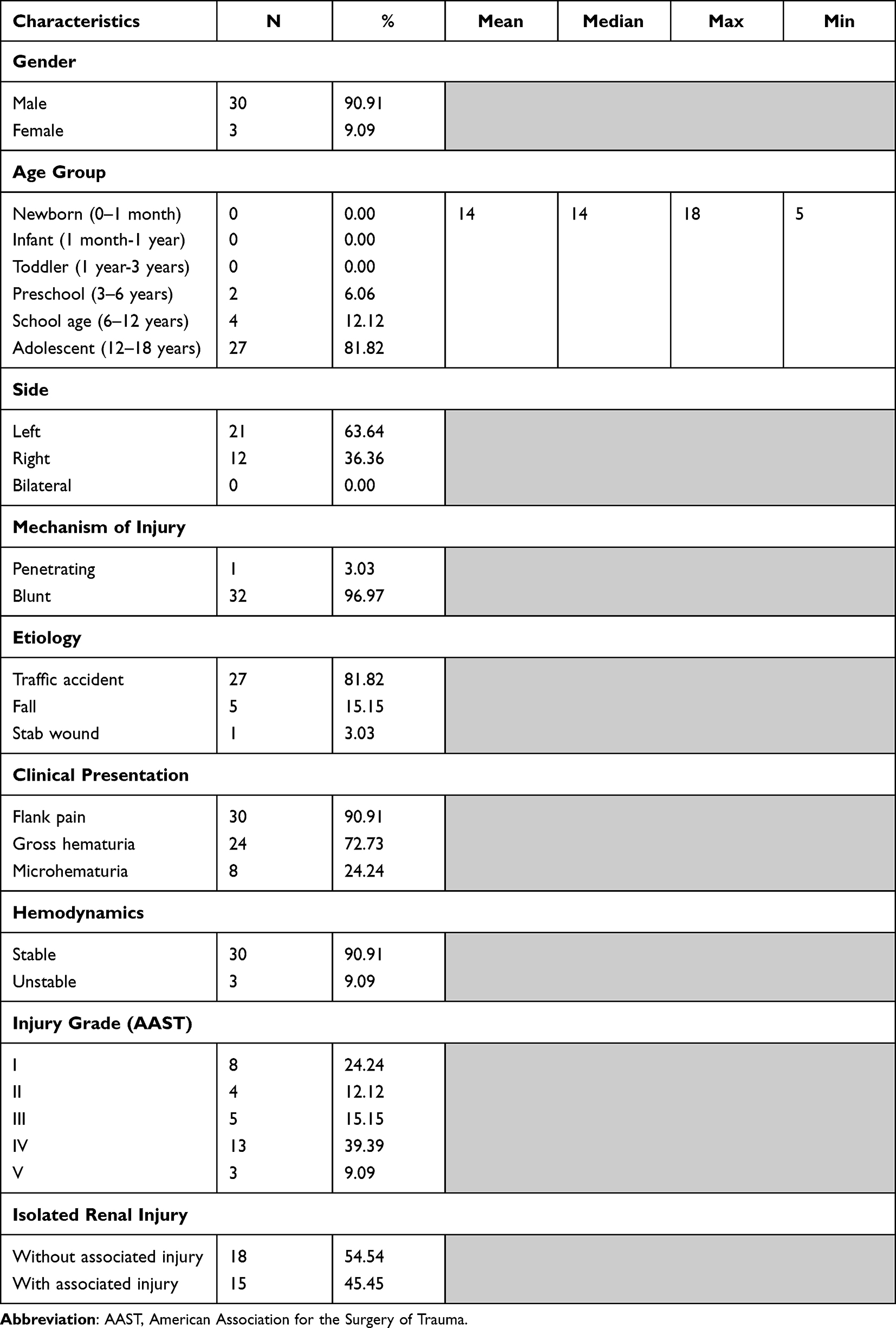 |
Table 1 General Characteristics of Traumatic Kidney Injury |
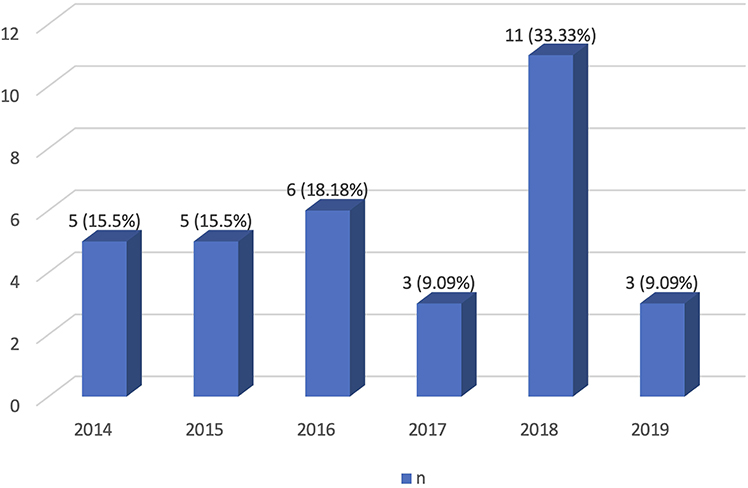 |
Figure 1 The description of case number per year. |
According to the laboratory findings (Table 2), most patients (68.75%) were admitted with normal BUN levels (≤18 mg/dl). The mean value of BUN was 15.9 mg/dl, and the highest and the lowest BUN levels were 43.5 mg/dl and 7.5 mg/dl, respectively. Most patients (62.5%) still maintained the normal limit of plasma creatinine levels (≤1.06 mg/dl). The cause of renal function disturbance was determined from BUN/Cr ratio with 21.87% of patients suffering from intra-renal causes and 12.5% of patients suffering from pre-renal causes. No significant association between the different grades and BUN/Cr ratio (p=0.77) was found (Table 3). Most patients (63.6%) were admitted with anemia (hemoglobin level < 11 g/dl), and those patients received blood transfusions when the hemoglobin (Hb) level was <9 g/dl.
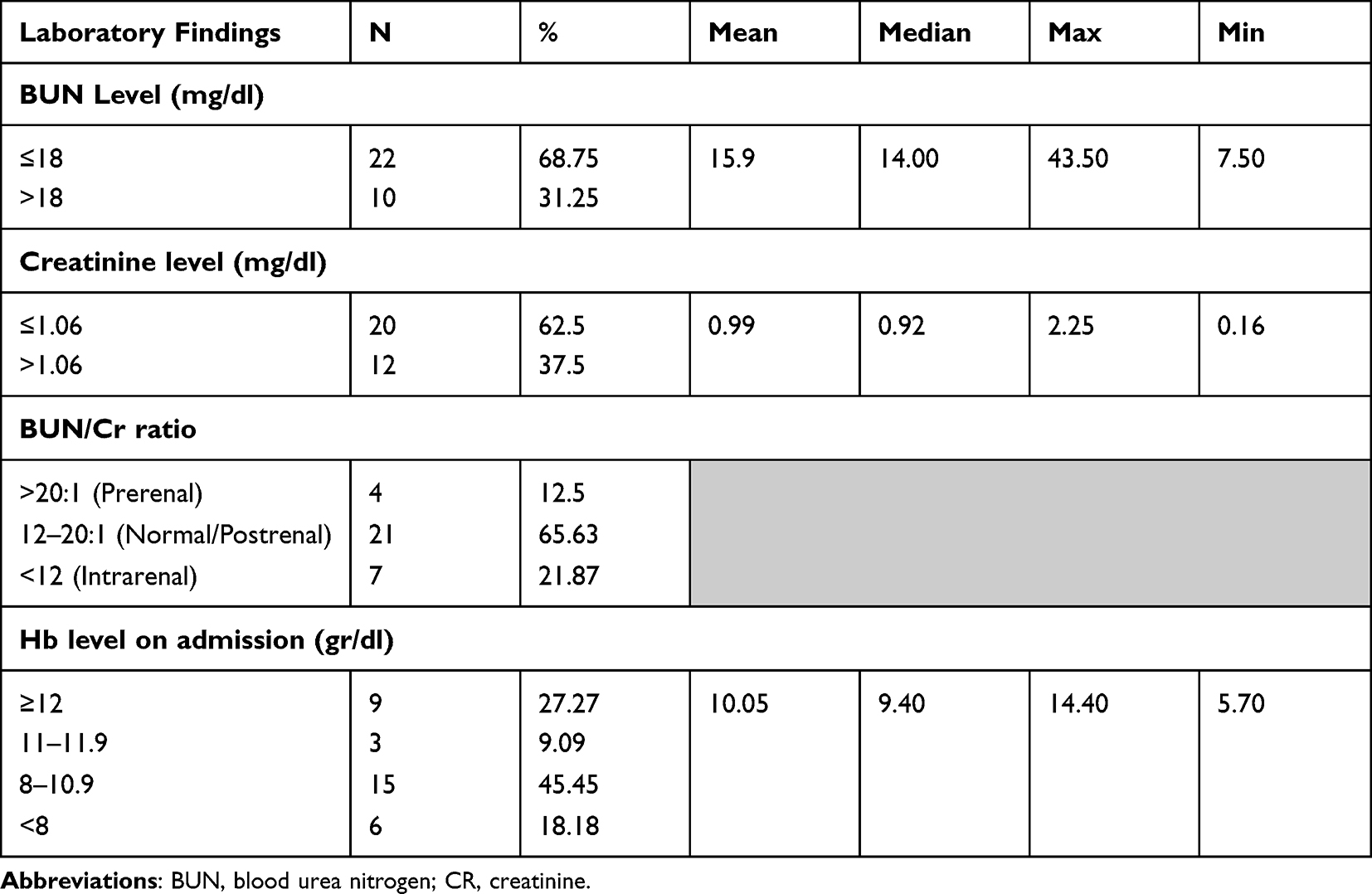 |
Table 2 The Laboratory Value of Traumatic Kidney Injury |
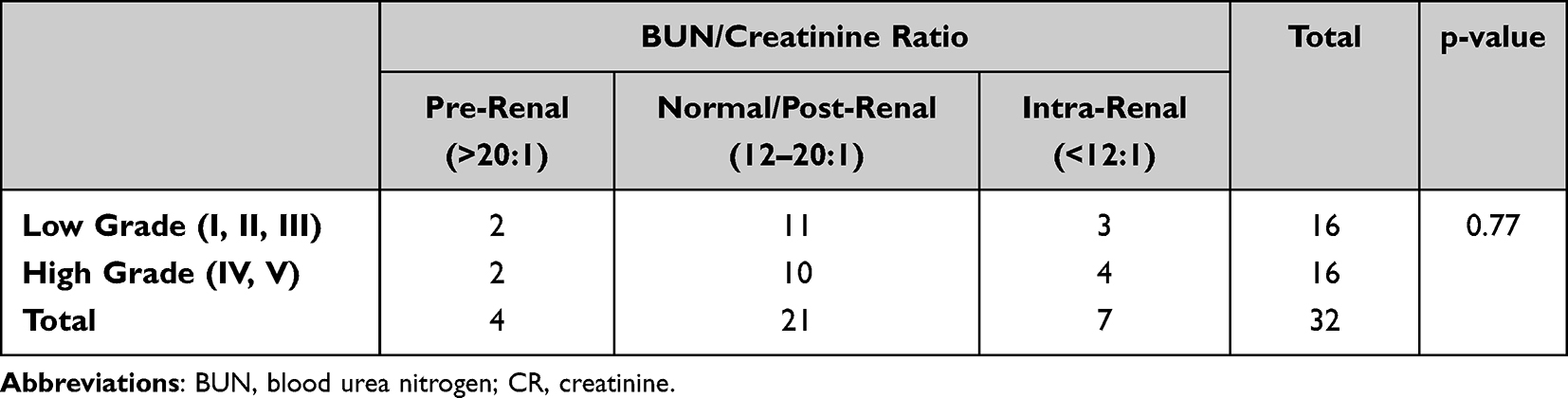 |
Table 3 Association Between the Severity of Kidney Trauma and Underlying Cause of Kidney Disease According to BUN/Cr Ratio |
Most patients (42.42%) were treated in the hospital for a duration of 8 to 14 days (Table 4). The mean length of stay (LOS) was 12 days, the longest and the shortest LOSs were 43 and one day, respectively. Traumatic brain and spleen injuries were frequently found as the associated injury with percentages of 15.15% and 12.12%, respectively. Most traumatic kidney injury patients were treated conservatively (87.88%). Most patients were survived (96.97%), and only 1 patient (3.03%) died.
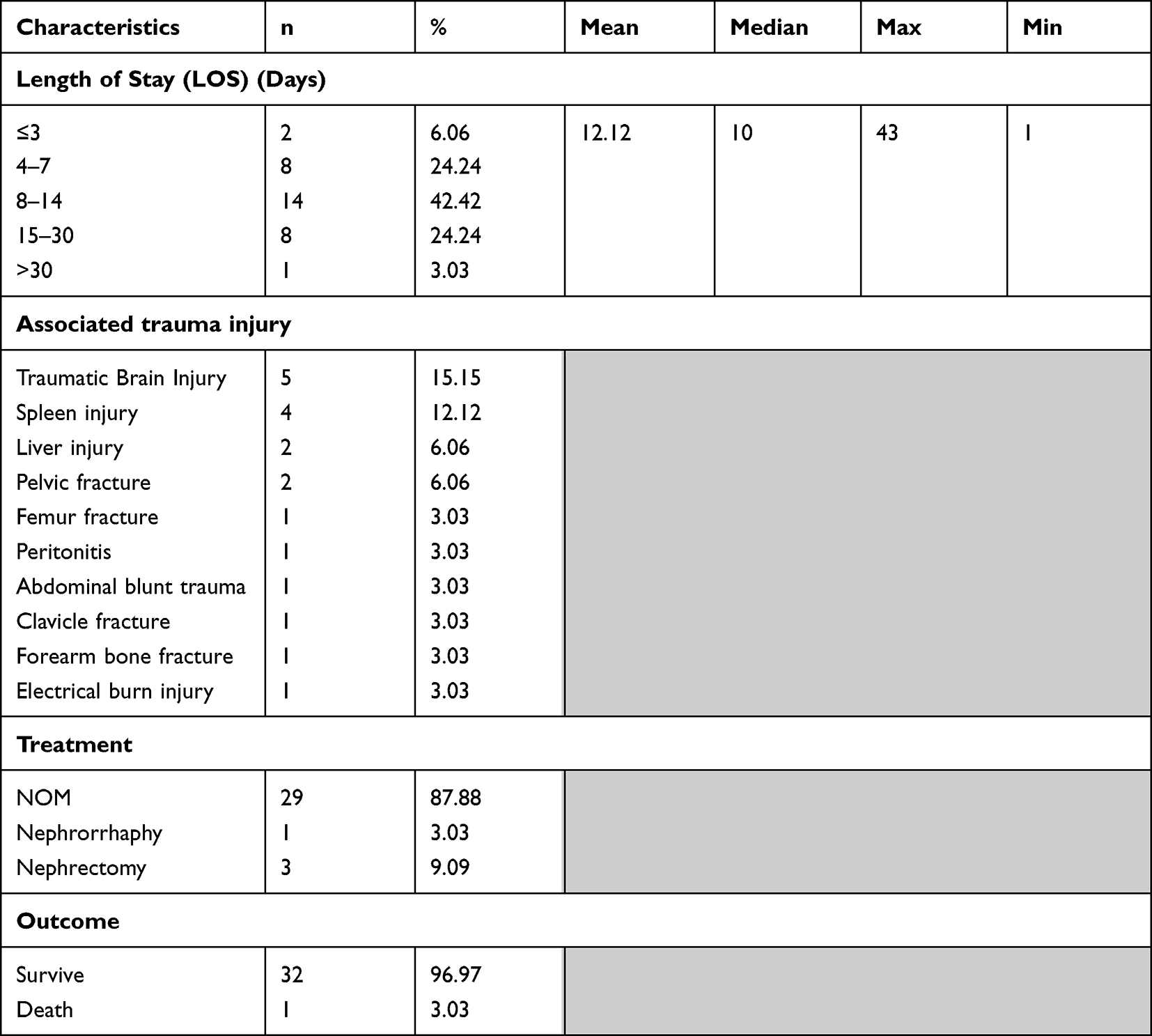 |
Table 4 Length of Stay, Associated Trauma Injury, Treatment, and Outcome |
Discussion
Genitourinary tract injury is a frequent phenomenon that occurs in children and adolescents. The kidneys are the most frequent site of damage in genitourinary tract injuries and represent 10–20% of blunt abdominal trauma cases.8,20 According to the study by Grimsby et al, the average age at time of injury was 13.7 years old with almost patients (94%) between the ages of 5 and 18.8 The result of this study agrees fairly well with our results for which it was shown that most cases were found at adolescent age with a mean age of 14 years old. The range of age was between 5 and 18 years old. The incidence of kidney trauma is most common in adolescence because the patients in this age group begin to undertake more activity and mobility, especially in terms of traffic and sports. Kidney trauma is rare in children under five years of age due to their limited mobility. Our study showed that males experience traumatic kidney injury more frequently than females. This result corresponded to results from a study by Ishida et al.21 This higher incidence in males was apparent because males are more frequently involved in motorcycle accidents than are females.22
When viewed from the lateral aspect, it was found that the left kidney was more susceptible to traumatic injury than the right side (63.64% versus 36.36%). This condition is not fully understood, but it might be due to the protective effect of the liver toward the right kidney. In addition, the right kidney is positioned just below the diaphragm, posterior to the liver, and relatively closer to the midline than the left kidney. The left kidney is also slightly larger than the right kidney.21
Most cases of kidney damage (96.97%) were found to be caused by blunt trauma. Traffic accidents were the main cause of traumatic kidney injury with 27 cases (81.82%). Grimsby et al,8 also found that more than 90% of kidney trauma patients in their study were caused by blunt trauma. According to Alonso et al,23 blunt renal trauma accounts for up to 80% to 90% of all cases with motor vehicle accidents being the most common cause. The other causes are direct impact to the flank or abdomen during an assault, a fight, sports activity, or fall from a height.
The diagnosis of traumatic kidney injury is made with high suspicion concerning the injury. Careful assessment of the mechanism of injury and clinical presentation must be conducted precisely. Prompt diagnosis is key as the injury may be life threatening.24
The most prominent clinical features of kidney trauma patients are flank pain and gross hematuria.3,8,21,25 Our study also found similar results. While hematuria is present in 95% of patients with renal trauma, its absence did not rule out the kidney injury.24 There was no clear association between the presence and the type of hematuria with the degree of kidney injury because 36–40% of renal injuries and more than 24% of renal artery occlusion did not show hematuria.6,26 However, macrohematuria seems to be more associated with major renal injuries. The general recommendation is to perform imaging investigations in blunt trauma patient with urinalysis findings >50 RBCs/HPF.26
The severity of traumatic kidney injury was classified using the well-known AAST Organ Injury Scale. This scale classifies traumatic kidney injury into five grades ranging from I to 5 regarding the severity of trauma complexity (Table 5).9,10
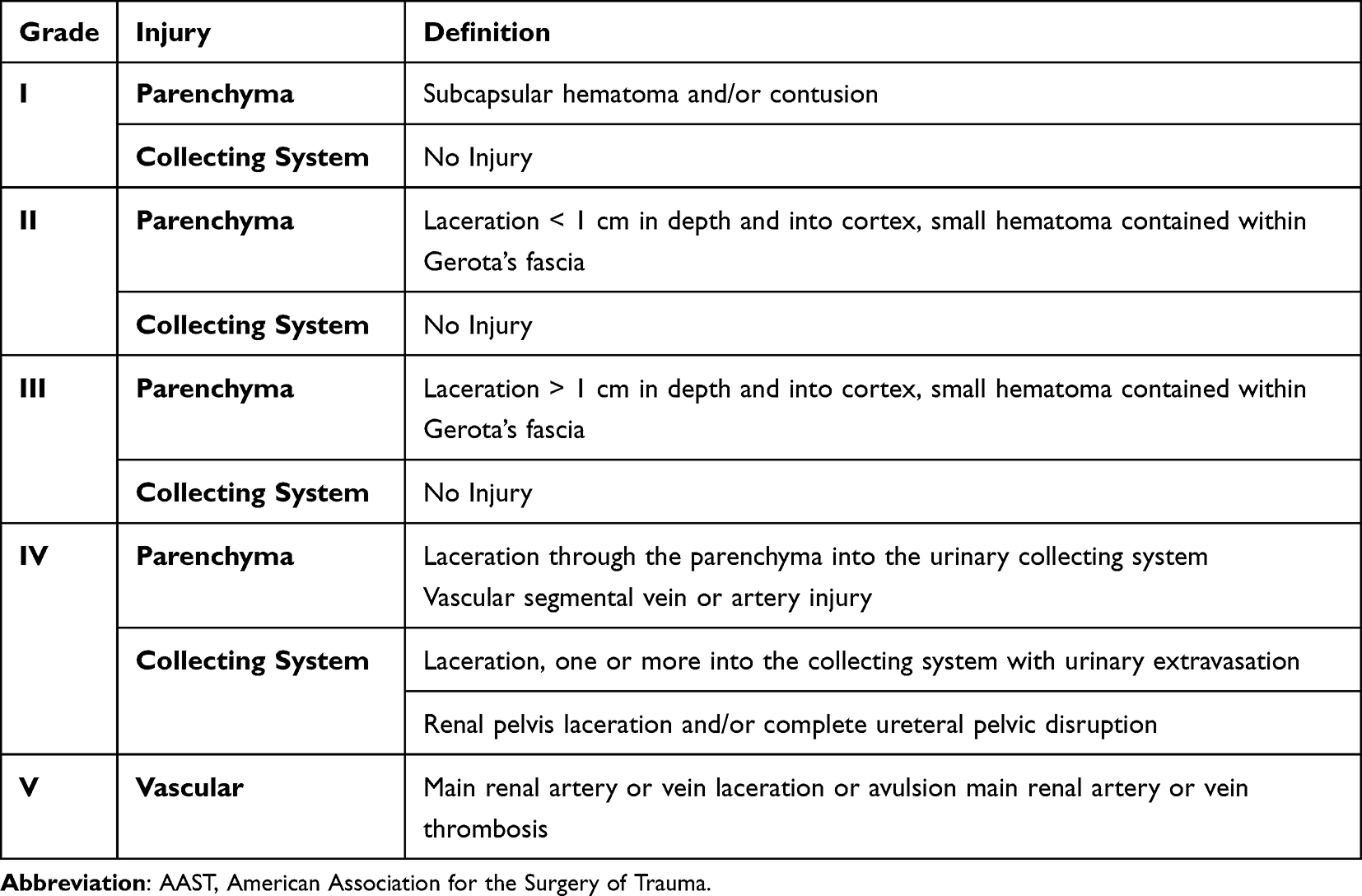 |
Table 5 Revised AAST Injury Staging Classification |
However, for clinical purposes, the degree of renal trauma is divided into low grade (I, II, and III) and high grade (IV and V).27
According to a study by Redmond et al based on their 10 years of experience, the distribution of AAST grade kidney injury in pediatric patients was 49% Grade IV, 37.8% Grade III, and 13.2% Grade V.7 This result was similar to our study in which it was also shown that the most frequent injury was grade IV (39.39%) followed by grade I (24.24%), grade III (15.15%), grade II (12.12%), and grade V (9.09%). On the other hand, the different results were apparent for distribution of traumatic kidney injury in all age groups including adult and pediatric patients. According to the meta-analysis study by Petrone et al, the most frequent injury was grade I (32%), followed by grade IV (25%), grade III (22%), grade II (16%), and grade V (5%).24 This difference occurs because children are more vulnerable to renal injuries because of the relatively increased renal size (beyond the rib cage) and the kidney mobility.6 The demographic differences in different areas may also be a factor. In a 5‑year retrospective review at single institution in Makassar, Syarif et al found that the most cases of renal trauma were grade IV (42.6%) followed by grade I (25%), grade II (14.7%), grade III (8.8%), and grade V (8.8%).28
Ten patients (31.25%) had increased BUN levels (>18 mg/dl). Plasma Cr levels were increased (>1.06 mg/dl) in 12 patients (37.5%). BUN and Cr levels may be related to acute trauma-induced kidney injury (AKI).29,30 Trauma patients are at risk of AKI induced by renal hypoperfusion (secondary to hemorrhagic shock), rhabdomyolysis, and direct renal injury.29
The cause of renal function disturbance was determined from BUN/Cr ratio with 21.87% of patients suffering from intra-renal causes and 12.5% of patients suffering from pre-renal causes. Most patients (65.63%) had BUN/Cr ratios of 12–20:1, which indicates normal or post-renal function impairment.31 Statistically, however, no significant association between the different grades and BUN/Cr ratio (p=0.77) was found. This result shows that although kidney trauma can cause damage to the intra-renal parenchyma, acute kidney function disorder can occur due to either pre-, intra-, or post-renal causes. No previous study that analyzes the association between the different grades and BUN/Cr ratio has been published.
In our study, most patients had anemia (hemoglobin level < 11 gr/dl). Anemia can occur from trauma-related acute blood loss and/or other chronic causes. Our patients were administered blood transfusion when the hemoglobin (Hb) level was <9 gr/dl. According to Chegondi et al, a hemoglobin threshold of ≤8 g/dl is recommended for transfusion if patients are symptomatic. However, patients with acute blood loss underwent blood transfusions at a hemoglobin threshold value of 7.83 ± 1.32 g/dl.32
The hemoglobin threshold for transfusion varies according to clinical conditions. Limited data from clinical trials comparing the outcomes of transfusion protocols in pediatric patients are available. The decision to perform a blood transfusion in our study was made with consideration of clinical conditions, anemia-related symptoms, hemodynamic instability, and trauma severity. Most patients were admitted to the emergency room with stable hemodynamics (90.91%). The results from our study agreed with those from a study by Syarif et al who found 89.7% of their patients came to the emergency department with stable hemodynamics.28 However, strict monitoring is generally needed for renal trauma in children because hypotension is a late manifestation of hypovolemia in children; blood pressure is not considered as a reliable parameter for early management in pediatric population.6 Isolated renal injuries were found in 54.54% of our patients. This finding was also consistent with the result of a retrospective study conducted by Syarif et al who found that the isolated renal injury percentage in their study was 58.8%.28
Most patients (42.42%) had been treated in the hospital for 8 to 14 days, and the mean of length of stay (LOS) was 12 days. The longest and the shortest LOS periods were 43 and 1 day, respectively. A study by Grimsby et al consisting of LOS evaluation of pediatric kidney trauma found that the LOS mean was 8.63 days.8 This difference was not far from our result, and the variation in LOS might have been caused by another associated injury. However, this finding indicates that treatment of renal trauma in children may require treatment duration of more than one week.
Blunt renal injuries in children are seldom isolated, and multiorgan injury (liver, spleen, closed head, orthopedic fractures) is the general rule.6 Several associated organ injuries that are commonly found in traumatic kidney injury are spleen and liver.25 This condition can occur due to the organs’ proximity to the kidney. The other injuries found in our study were traumatic brain injury, bone fracture, associated abdominal trauma injury, and burn injury.
Most pediatric kidney trauma patients in our study were treated conservatively (87.88%). This result was similar to the meta-analysis study by Hagedorn et al (with a total of 5561 children) in which it was found that only 10% of blunt renal trauma patients underwent surgical intervention, and 89.6% were managed nonoperatively. Another study by Grimsby et al also reported treating 94% of their pediatric kidney trauma patients conservatively.8 Current evidence suggests that conservative management in all hemodynamically stable traumatic pediatric blunt renal injuries is appropriate.3,4,6–8,10 This paradigm shift is probably derived from several considerations: (1) the accumulated evidence about the safety and outcome of the nonoperative approach in renal trauma and (2) the improvement in imaging modalities, such as computed tomography (CT) scanning, and in minimally invasive procedures. These procedures include angioembolization in cases of active bleeding and endourological stenting in managing urine extravasation.10 In hemodynamically stable children, further investigation should be conducted. Absolute indications for operative (or interventional radiology management) management include unresponsiveness to aggressive resuscitation (>3 concentrated transfusions) due to renal hemorrhage, hemodynamic instability, grade 5 vascular injury, and/or an expanding or pulsatile perirenal hematoma found during laparotomy performed for associated injuries. Relative indications are large lacerations of the renal pelvis, avulsion of the ureteropelvic junction, coexisting bowel or pancreatic injuries, persistent urinary leakage, post-injury urinoma, perinephric abscess, extensive (>20%) nonviable tissue, and incomplete staging.6
Non-operative management (NOM) consists of bed rest with vital signs and laboratory test monitoring, observation with supportive care, re-imaging when any deterioration occurs, the use of minimally invasive procedures (angioembolization or ureteral stenting) if indicated, and restriction of physical activity for six weeks.3,6,10,33, Currently, advance evidence that supports NOM for hemodynamically stable patients with penetrating renal trauma is available. Moolman et al successfully treated 65.3% of the 75 penetrating kidney trauma patients non-operatively with excellent outcomes and no conversion to surgical exploration.33
Operative management is performed for patients with indications. The most common approach is transperitoneal. Renal salvage by renorrhaphy or partial nephrectomy requires maximal exposure of the kidney, control of bleeding by sutures, debridement of nonviable tissue, closure of parenchymal injuries, and watertight closure of the collecting system. The omental flap of perirenal fat can be utilized to cover the large defects.10
In agreement with the meta-analysis conducted by Hagedorn et al addressing pediatric blunt renal trauma practice management guidelines, almost half (44.9%) of the children in the operative group had renal loss (nephrectomy) when compared with 1.5% in the non-operative group. About 2.4% of the patients in the operative group developed a urinoma versus 1.2% in the non-operative group.3
Most patients in our study survived (96.97%), and only one patient (3.03%) died due to severe brain injury. According to the literature, the mortality rate is 6%, but this value may be related to the presence of other concurrent organ injuries and not caused by renal trauma alone.
Our data were obtained from patient medical records at a referral center rather than a major trauma hospital. Therefore, the number of cases was limited, and the cases were often more severe than those in the general population. Furthermore, radioisotope renography (renogram) was not available in our center, making it difficult to assess follow-up renal function. Further investigation is required to observe late complications, including the formation of urinary tract stones, hypertension, chronic upper urinary tract infection, hydronephrosis, pseudo-aneurysms, and arteriovenous fistulae. In the future, we plan to conduct further studies at a multi-trauma center with renal function follow-up tests and long-term follow-up to observe any late complications.
Conclusion
Traumatic kidney injuries are more frequent in male adolescents due to more involvement in injury-risk activity. Hematuria is not an accurate parameter for assessing the severity of a kidney injury. Vital sign monitoring should be performed continuously because hypotension is a late manifestation of hypovolemia in children. The severity of a traumatic kidney injury was found not to be associated with the BUN/Cr ratio. Non-operative management may be performed safely with good outcomes in kidney trauma patients who have stable hemodynamics. Mortality is rare and may be related to concomitant injuries in other organ systems.
Abbreviations
BUN/Cr, blood urea nitrogen/creatinine; AAST, American Association for the Surgery of Trauma; CT, computed tomography; RBCs/HPF, red blood cells per high-power field; NOM, non-operative management; Hb, hemoglobin; LOS, length of stay; AKI, acute kidney injury; g, gram; mg, milligram; dl, deciliter.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The ethical approval was given by the medical research ethical committee of Faculty of Medicine Universitas Hasanuddin. No. 680/UN4.6.4.5.31/PP36/2023. All procedures involving human participants were performed in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all child’s parents or guardian participants included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Cunningham RM, Walton MA, Carter PM. The major causes of death in children and adolescents in the United States. N Engl J Med. 2018;379(25):2468–2475. doi:10.1056/NEJMsr1804754
2. Fraga AMA, Bustorff-Silva JM, Fernandez TM, et al. Children and adolescents deaths from trauma-related causes in a Brazilian City. World J Emerg Surg. 2013;8(1):52. doi:10.1186/1749-7922-8-52
3. Hagedorn JC, Fox N, Ellison JS, et al. Pediatric blunt renal trauma practice management guidelines: collaboration between the Eastern Association for the Surgery of Trauma and the Pediatric Trauma Society. J Trauma Acute Care Surg. 2019;86(5):916–925. doi:10.1097/TA.0000000000002209
4. Pirinççi N, Kaba M, Geçit İ, Güneş M, Tanik S, Ceylan K. Conservative approach in the treatment of renal trauma in children. Urol Int. 2014;92(2):215–218. doi:10.1159/000350753
5. Deepak J, Khanday ZS, Bagdi RK, et al. Three cases of blunt renal trauma in children. Sri Ramachandra J Med; 2007:62:1–74.
6. Fernández-Ibieta M. Renal trauma in pediatrics: a current review. Urology. 2018;113:171–178. doi:10.1016/j.urology.2017.09.030
7. Redmond EJ, Kiddoo DA, Metcalfe PD. Contemporary management of pediatric high grade renal trauma: 10 year experience at a level 1 trauma centre. J Pediatr Urol. 2020;16(5):656.e1–656.e5. doi:10.1016/j.jpurol.2020.06.033
8. Grimsby GM, Voelzke B, Hotaling J, Sorensen MD, Koyle M, Jacobs MA. Demographics of pediatric renal trauma. J Urol. 2014;192(5):1498–1502. doi:10.1016/j.juro.2014.05.103
9. Buckley JC, McAninch JW. Revision of current American association for the surgery of trauma renal injury grading system. J Trauma. 2011;70(1):35–37. doi:10.1097/TA.0b013e318207ad5a
10. Erlich T, Kitrey ND. Renal trauma: the current best practice. Ther Adv Urol. 2018;10(10):295–303. doi:10.1177/1756287218785828
11. Kozar R A, Crandall M, Shanmuganathan K et al. Organ injury scaling 2018 update: Spleen, liver, and kidney. J Trauma Acute Care Surg. 2018;85(6):1119–1122. doi 10.1097/TA.0000000000002058
12. Bolenz C, Schröppel B, Eisenhardt A, Schmitz-Dräger BJ, Grimm M. The Investigation of Hematuria. Dtsch Arztebl Int.2018;115(48):801–807. doi: 10.3238/arztebl.2018.0801
13. Sevransky J. Clinical assessment of hemodynamically unstable patients. Curr Opin Crit Care. 2009;15(3):234–238. doi: 10.1097/MCC.0b013e32832b70e5
14. Simon LV, Lopez RA, King KC. Blunt Force Trauma. In: StatPearls. Treasure Island (FL): StatPearls Publishing;2023.
15. Burton-Williams KM. Resuscitation of the Traumatically Injured Patient. Critical Care Nursing Clinics of North America. 2021;33(3):245–261. doi: 10.1016/j.cnc.2021.05.002
16. Lotfollahzadeh S, Burns B. Penetrating Abdominal Trauma. [Updated 2023 Jun 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
17. Asensio, JA, Verde, JM (). Penetrating Wounds. In: Vincent, JL, Hall, JB (eds) Encyclopedia of Intensive Care Medicine. Springer, Berlin, Heidelberg. 2012:
18. Wang M. Iron Deficiency and Other Types of Anemia in Infants and Children. Am Fam Physician. 2016;93(4):270–278.
19. Hruschak J. Mosby’s diagnostic and laboratory test reference. AORN J. 1995;62(5):823. doi:10.1016/s0001-2092(06)63542-4
20. Alsaywid B, Alkhashan MY, Alrimawi M, Abu-Alsaud N, Al-Rimawi H. Blunt renal trauma in pediatric population. Urol Ann. 2019;11(3):241–246. doi:10.4103/UA.UA_149_18
21. Ishida Y, Tyroch A, Emami N, McLean S. Characteristics and management of blunt renal injury in children. J Emerg Trauma Shock. 2017;10(3):140–145. doi:10.4103/JETS.JETS_93_16
22. Romero DL, de Barros DM, Belizario GO, De Pádua Serafim A, Useche SA. Personality traits and risky behavior among motorcyclists: an exploratory study. PLoS One. 2019;14(12):e0225949. doi:10.1371/journal.pone.0225949
23. Alonso RC, Nacenta SB, Martinez PD, Guerrero AS, Fuentes CG. Kidney in danger: CT findings of blunt and penetrating renal trauma. Radiographics. 2009;29(7):2033–2053. doi:10.1148/rg.297095071
24. Petrone P, Perez-Calvo J, Brathwaite CEM, Islam S, Joseph DK. Traumatic kidney injuries: a systematic review and meta-analysis. Int J Surg. 2020;74(December 2019):13–21. doi:10.1016/j.ijsu.2019.12.013
25. Govindarajan KK, Utagi M, Naredi BK, Jindal B, Sambandan K, Subramaniam D. High grade renal trauma due to blunt injury in children: do all require intervention? J Bras Nefrol. 2019;41(2):172–175. doi:10.1590/2175-8239-JBN-2018-0186
26. Coccolini F, Moore EE, Kluger Y, et al. Kidney and uro-trauma: WSES-AAST guidelines. World J Emerg Surg. 2019;14(1):54. doi:10.1186/s13017-019-0274-x
27. Reis LO, Kim FJ, Moore EE, et al. Atualização da classificação e tratamento das lesões renais complexas. Rev Col Bras Cir. 2013;40(4):347–350. doi:10.1590/S0100-69912013000400016
28. Syarif S, Palinrungi AM, Kholis K et al. Renal trauma: a 5-year retrospective review in single institution. Afr J Urol. 2020;26(1):61. doi:10.1186/s12301-020-00073-2
29. Perkins ZB, Captur G, Bird R, et al. Trauma induced acute kidney injury. PLoS One. 2019;14(1):e0211001. doi:10.1371/journal.pone.0211001
30. Lai W-H, Rau C-S, S-C W, et al. Post-traumatic acute kidney injury: a cross-sectional study of trauma patients. Scand J Trauma Resusc Emerg Med. 2016;24(1):136. doi:10.1186/s13049-016-0330-4
31. Brown D, Edwards H. Lewis’s Medical-Surgical Nursing: Assessment and Management of Clinical Problems. Elsevier Australia; 2012.
32. Chegondi M, Sasaki J, Raszynski A, Totapally BR. Hemoglobin threshold for blood transfusion in a pediatric intensive care unit. Transfus Med Hemother. 2016;43(4):297–301. doi:10.1159/000446253
33. Moolman C, Navsaria PH, Lazarus J, Pontin A, Nicol AJ. Nonoperative management of penetrating kidney injuries: a prospective audit. J Urol. 2012;188(1):169–173. doi:10.1016/j.juro.2012.03.009
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.