")
Back to Journals » Lung Cancer: Targets and Therapy » Volume 14
Tiragolumab (Anti-TIGIT) in SCLC: Skyscraper-02, a Towering Inferno
Authors Brazel D, Ou SI , Nagasaka M
Received 21 June 2022
Accepted for publication 22 December 2022
Published 5 January 2023 Volume 2023:14 Pages 1—9
DOI https://doi.org/10.2147/LCTT.S379389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Fengying Wu
Danielle Brazel,1 Sai-Hong Ignatius Ou,1,2 Misako Nagasaka1– 3
1Department of Medicine, University of California Irvine School of Medicine, Orange, CA, USA; 2Chao Family Comprehensive Cancer Center, Orange, CA, USA; 3St. Marianna University School of Medicine, Kawasaki, Japan
Correspondence: Misako Nagasaka, Department of Medicine, University of California Irvine School of Medicine, 101 the City Drive, Orange, CA, USA, Email [email protected]
Abstract: Small cell lung cancer (SCLC) is characterized by rapid progression and poor prognosis. Although the phase II CITYSCAPE-02 trial found objective response rate (ORR) and progression-free survival (PFS) of non-small cell lung cancer (NSCLC) patients improved when tiragolumab was added to atezolizumab and chemotherapy, the phase III SKYSCRAPER-02 failed to find PFS or OS benefit in patients with SCLC. Atezolizumab was the first immunotherapy to show survival benefit in extensive SCLC based on the phase III IMpower133 study. Given that immunotherapy has become the standard of care for SCLC patients, further research is needed into ways to augment the immune system to better treat these patients.
Keywords: tiragolumab, TIGIT, immunotherapy, small cell lung cancer
Introduction
Small cell lung cancer (SCLC) is characterized by rapid progression and poor prognosis. It is typically associated with tobacco smoking. SCLC management depends on whether the disease is classified as limited or extensive stage, with 56.6% of patients presenting with extensive stage disease at diagnosis.1 Extensive-stage small cell lung carcinoma remains difficult to treat. Current standard of care is chemotherapy plus immunotherapy.
Immunotherapy with monoclonal antibodies against programmed cell death 1 (PD-1), programmed death-ligand 1 (PD-L1), and cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) are now standard of care for a number of cancers. Atezolizumab was the first immunotherapy to show survival benefit in extensive SCLC based on the phase III IMpower133 study.2 Additionally, the CASPIAN study utilizing chemotherapy and durvalumab, another PDL1 inhibitor, also showed comparable results to those of the IMpower133 study.3
Cluster of differentiation 155 (CD155) is involved in the cellular adhesion, migration, differentiation, proliferation, survival, and metastases of tumor cells4,5 as well as immune regulation.6 The role of CD155 in immune regulation of the tumor microenvironment is not well understood but has been shown to interact with T cell receptor and TIGIT domains to inhibit lymphocyte cytotoxicity and proliferation. Previous studies found CD155/T-cell immunoreceptor with Ig and ITIM domains (TIGIT) and PD-L1/PD-1 are highly expressed in SCLC tumors and that elevated expression of PD-L1 or CD155 portends worse overall survival.7 The receptors of CD155 and PD-L1 were constitutively expressed on both CD8 tumor infiltrating lymphocytes and on SCLC cells. These findings suggest that tumor cells may upregulate CD155 and PD-L1 to evade immune detection.
Tiragolumab (Genentech) is an anti-TIGIT antibody that was given breakthrough therapy designation by the US Food and Drug Administration (FDA) in February 2021 for treatment of PD-L1-high metastatic NSCLC. This was based off of the promising phase II CITYSCAPE study. In this review, we discuss the role of TIGIT inhibition in solid tumors, early clinical trials, and recently released results of tiragolumab in SCLC.
Structural Characteristics and Mechanism of Action
TIGIT is a transmembrane glycoprotein composed of an immunoglobulin variable domain, a transmembrane domain, and a cytoplasmic tail.8–10 TIGIT initiates an inhibitory signaling cascade via the cytoplasmic tail. When ligand binds, the tail is phosphorylated, ultimately inhibiting the phosphoinositide 3 kinase (PI3K)/mitogen-activated protein kinase (MAPK) signaling cascades.11 Additionally, though recruitment of Src-containing inositolphosphate-1 (SHIP-1) to inhibit tumor necrosis factor (TNF) and nuclear factor kappa B (NF-kB) activation.11,12 TIGIT has multiple ligands but seems to have a greater affinity for PVR (Necl-5 or CD155) which is upregulated in several types of cancer13,14 and is associated with poor prognosis.15,16
TIGIT is found on T cells and natural killer (NK) cells. TIGIT expression is known to strongly correlate with PD-1 expression.17
Pharmacodynamics/Kinetics
Exposure of tiragolumab increased with increasing dose followed by nonlinear pharmacokinetics at doses greater than or equal to 100 mg every 3 weeks.18 Pharmacokinetics were unchanged when administered in combination with atezolizumab. Peripheral TIGIT receptors on cluster of differentiation 8 (CD8) cells were completely occupied for sustained periods at tiragolumab doses at least 30 mg every 3 weeks. Clinical activity was observed at 400 mg to 600 mg doses every 3 weeks.
Preclinical Studies
In mouse tumor models, decreased TIGIT delays growth of both B16F10 cells, MC38 cells, and lung metastases of B16 cells.19,20 Further, anti-TIGIT antibodies inhibit mouse T cell proliferation and cytokine production without antigen presenting cells.21,22
Anti-TIGIT antibodies appear to work synergistically with anti-PD-1 antibodies through CD8+ responses.23 Within ex vivo cell cultures of CD3+ TILS and Mel-624 cells, anti-TIGIT antibodies promote interferon gamma and interleukin-2 production.24 These findings were seen in a variety of solid tumor types.
Based on the biochemical mechanism and preclinical studies, investigators sought to utilize TIGIT-mediated immune regulation to enhance T and NK cell activity.
Clinical Trials
Approximately 10 human anti-TIGIT monoclonal antibodies with varying isotypes or forms have entered clinical trials. Tiragolumab is being studied alone or in combination with atezolizumab in phase I to III trials of solid tumors such as cervical cancer, SCLC, and blood cancers (Table 1).
 |  |  |  |
Table 1 Ongoing Studies Utilizing Tiragolumab |
Phase I Solid Tumors
In a phase Ia/Ib trial of tiragolumab in 73 patients with solid tumors were treated in dose-escalation.18 Only 4% of patients experienced grade 3 or higher treatment-related adverse events, with the most commonly reported adverse events including fatigue (38%) and anemia (31%). No dose-limiting toxicities were observed. Within the metastatic NSCLC expansion cohort 9 (n=14), ORR was 50% with DCR 79%. Based on maximum receptor occupancy and clinical activity observed in the phase 1 results, the recommended dose of tiragolumab was determined to be 600 mg every 3 weeks.
Phase II NSCLC
The phase II CITYSCAPE (NCT03563716) studied tiragolumab in combination with atezolizumab in PD-L1 positive advanced/metastatic NSCLC without epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) mutations.25 A total of 135 patients were randomized to the combination tiragolumab 600 mg plus atezolizumab 1200 mg IV every 3 weeks or atezolizumab plus placebo. At a median follow-up of 10.5 months, the trial showed significant improvement in ORR (37% vs 21%) and PFS (5.6 vs 3.9 months; hazard ratio (HR) 0.59). When further stratified by high PD-L1 status, defined as PD-L1 expression at least 50%, the ORR increased to 66% in the combination vs 24% with atezolizumab alone.17 A 21% of patients in the combination group and 18% in the atezolizumab alone cohort had serious treatment-related adverse events. The most common grade 3 or higher adverse event was lipase increase (9% combination, 3% atezolizumab). Two treatment-related deaths (pyrexia and infection) occurred in the combination cohort. As a result of these findings, the phase III SKYSCRAPER-01 study was launched.
Phase III NSCLC
The phase III SKYSCRAPER-01 trial (NCT04294810) studied combination tiragolumab and atezolizumab in newly diagnosed metastatic NSCLC with PD-L1 expression of at least 50%. A total of 534 patients were randomized to this study. At interim analysis, the study did not meet its co-primary end point of improvement in PFS. At the time of analysis, data for overall survival (OS) was immature.26 The study will continue until the next planned data analysis.
Phase III SCLC
In the SCLC space, the phase III SKYSCRAPER-02 (NCT04256421) is ongoing. In this study of newly diagnosed extensive-stage small cell lung cancer, 490 patients are randomized to atezolizumab 1200 mg IV every 3 weeks plus carboplatin and etoposide either with (n=243) or without (n=247) tiragolumab 600 mg IV every 3 weeks.27 At a median follow-up of 14.3 months, 397 patients were analyzed for interim analysis. This study failed to meet its co-primary endpoint of PFS improvement. Median PFS was 5.4 months (95% CI 4.7–5.5) with tiragolumab vs 5.6 months without this agent.28 The other co-primary endpoint of OS was unlikely to reach statistical significance by planned final analysis. The median OS was 13.6 months for both cohorts (95% CI 0.10.8–14.9). There was no significant difference in OS based on stratifying for factors including Eastern Cooperative Oncology Group (ECOG) performance status (PS), brain metastases or lactate dehydrogenase levels. Additionally, ORRs were similar between cohorts (70.8% (95% CI 64.6–76.3) with tiragolumab vs 65.6 (95% CI 59.3–71.4) with placebo). Duration of response (DOR) was also similar at 4.2 months (95% CI 4.1–4.4) with tiragolumab compared to 5.1 (95% CI 4.4–5.8) without. The study will continue until planned final OS analysis.
Adverse events were common in SKYSCRAPER-02, with 99.6% of patients in both cohorts reporting side effects. Grade 3 or higher adverse events occurred in 69.4% of patients receiving tiragolumab compared to 70.3% of patients receiving placebo. Toxicity resulted in withdrawal in 5.0% and 5.3% of patients receiving tiragolumab and placebo, respectively. The most common adverse events were anemia, neutropenia, and alopecia, though pruritus was more common in the tiragolumab group.
Discussion
Although studies have shown that patients with NSCLC and SCLC have better outcomes when immunotherapy is added to chemotherapy, it is unclear which patients will benefit the most or develop serious immune-related adverse effects. More research is needed and there is an unmet need for additional immune system targets/complementary pathways.
The IMpower133 trial showed a significant improvement in OS (12.3 months vs 10.3 months; HR death 0.70; 95% CI 0.54–0.91) with atezolizumab in extensive stage SCLC.2 Median PFS was 5.2 months vs 4.3 months (HR 0.77; 95% CI 0.62–0.96). These findings showed the potential for immune regulation to alter clinical outcomes in extensive SCLC and received FDA approval in March 2019. Additionally, results from the CASPIAN study further backed up the synergistic effects of immunotherapy added onto chemotherapy in extensive stage SCLC patients and thus these two regimens became the standard of care. Table 2 compares these studies side by side in addition to the Skyscraper-02 study. Of note, KEYNOTE-604 studied pembrolizumab or placebo combined with platinum and etoposide in the first-line setting of extensive stage SCLC. Results showed improved PFS (HR 0.75; 95% CI 0.61–0.91) as well as 12-month PFS of 13.6% vs 3.1%.29 OS was longer with the addition of pembrolizumab but did not reach statistical significance. The ORR was 70.6% vs 61.8% with similar rates of adverse events.
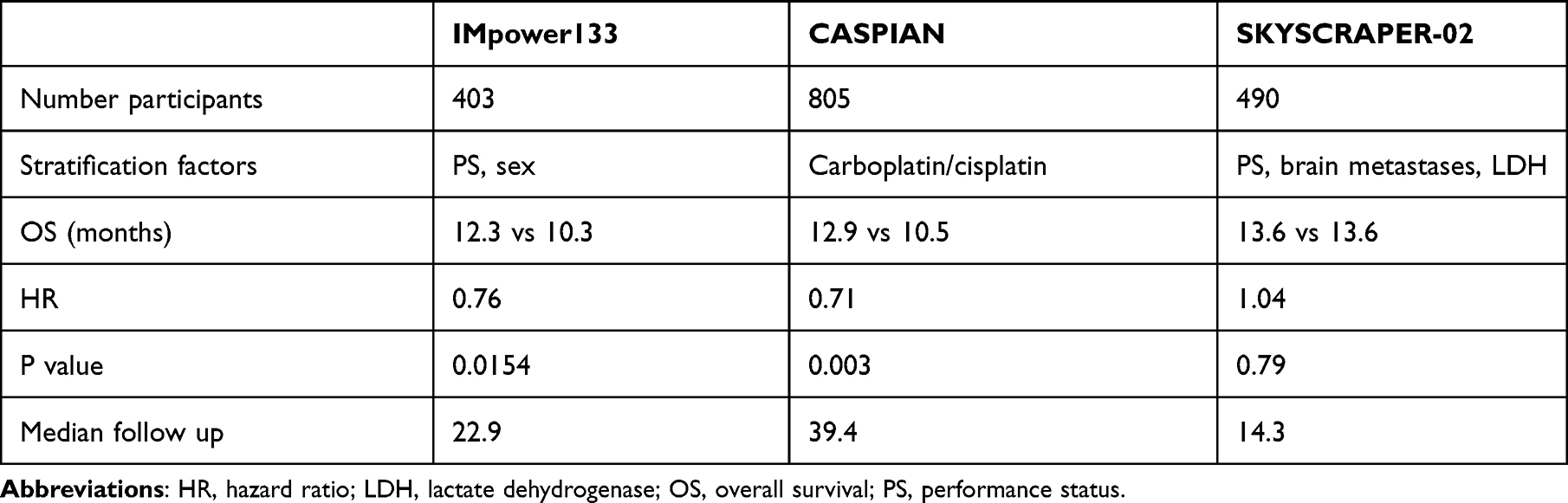 |
Table 2 Comparison of IMpower133, CASPIAN and SKYSCRAPER-02 Endpoints |
Nevertheless, extensive stage SCLC remains a difficult diagnosis to treat due to disease progression being ultimately inevitable with oftentimes limited therapeutic options. Unfortunately, the addition of tiragolumab to atezolizumab did not provide clinical benefit at interim analysis for either PFS or OS based on Skyscraper-02. But why?
Comparing IMpower133 and Skyscraper-02, the control arm outperformed expectations in the Skyscraper-02 study, which is likely the cause of negative endpoints, at least partially, in addition to the fact that enhanced benefit in the tiragolumab arm was not seen. However, the reason for this is unclear. Stratification factors in Skyscraper-02 included ECOG performance status, brain metastasis and LDH, whereas in IMpower133, patients were stratified based on ECOG performance status and sex. The distribution of both ECOG performance status and sex were largely similar in IMpower133 and Skyscraper-02. If anything, Skyscraper-02 study had a larger percentage of patients with brain metastasis at baseline (19.3% in the tiragolumab arm and 18.6% in the placebo arm), whereas IMpower133 had only 8.5% and 8.9% of patients in the investigational arm and placebo arm, respectively. While this observation was surprising, perhaps we are missing a more important factor in SCLC, which could be related to the molecular subtypes of SCLC.
Indeed, Gay et al reported differential survival benefits to the IMpower133 regimen based on the molecular subtypes of SCLC.30 SCLC-I, or SCLC-inflamed subtype, had the best survival benefit when compared to other subtypes such as SCLC-A (SCLC-ASCL1), SCLC-N (SCLC-NEUROD1) and SCLC-P (SCLC-POU2F3). Characterized by the increased absolute number of immune cells including T-cells, NK cells and macrophages, the SCLC-I subtype had significant OS benefit relative to all other subtypes with an HR of 0.566 (95% CI: 0.321–0.998) with the chemotherapy and atezolizumab arm but not with the chemotherapy and placebo arm, which suggests that SCLC-I subtype may be predictive of benefit to immune checkpoint blockade.
Future Directions
Further research is needed on the association of cluster of differentiation 226 (CD226) activation with the efficacy of anti-TIGIT antibodies. Despite the lack of success in phase III trials, the preclinical and phase II data shows that PD-L1 complementary immune regulatory pathways may merit further investigation in lung cancer. In SCLC, more focus should be given on the molecular subtypes and perhaps utilization of anti-TIGIT combinations should be evaluated in cohorts enriched with the SCLC-inflamed subtype. For NSCLC, in addition to the SKYSCRAPER-01 study, phase II/III trials of tiragolumab are still ongoing including SKYSCRAPER-03 for unresectable stage 3 NSCLC and SKYSCRAPER-06 for treatment naïve nonsquamous NSCLC (Table 1).
Conclusion
Extensive stage SCLC remains difficult to treat. Although initial results of tiragolumab as a complement to PD-L1 inhibition were promising, the drug has failed to meet its endpoint in the phase III SKYSCRAPER-02 trial for SCLC. Phase III trials of this drug are still ongoing in NSCLC and other tumor types such as esophageal cancer. Given the positive results of IMpower133 and CASPIAN, there appears to be synergistic effects of chemotherapy and immunotherapy in SCLC. More research to understand ways to improve the immune regulation in SCLC patients is needed. Not all SCLC are created equal. Perhaps, it is time to look at the subtypes of SCLC and treat accordingly.
Abbreviations
ALK, anaplastic lymphoma kinase; CD8, cluster of differentiation 8; CD155, cluster of differentiation 155; CD226, cluster of differentiation 226; CTLA-2, cytotoxic T lymphocyte-associated antigen 4; DOR, duration of response; ECOG, Eastern Cooperative Oncology Group; EGFR, epidermal growth factor receptor; FDA, Federal Drug Administration; HR, hazard ratio; MAPK, mitogen-activated protein kinase; NF-kB, nuclear factor kappa beta; NK, natural killer; NSCLC, non-small cell lung cancer; ORR, objective response rate; OS, overall survival; PD-1, programmed cell death 1; PD-L1, programmed death-ligand 1; PFS, progression-free survival; PI3K, phosphoinositide 3 kinase; SCLC, small cell lung cancer; TIGIT, T-cell immunoglobulin and ITIM domain; TNF, tumor necrosis factor.
Funding
No funding was secured for this report.
Disclosure
SIO has stock ownership and was on the scientific advisory board of Turning Point Therapeutics Inc (until Feb 28, 2019); is a member of the SAB of Elevation Oncology and has stock ownership; honoraria from AstraZeneca, Caris Life Science, Daiichi Sankyo, DAVA Oncology LLP, Janssen/JNJ, Merck, Pfizer, Roche/Genentech, Takeda/ARIAD, BeiGene. MN reports honorarium/consulting from/for AstraZeneca, Daiichi Sankyo, Takeda, Novartis, EMD Serono, Janssen, Pfizer, Eli Lilly, Genentech, Mirati, Caris Life Sciences, Blueprint Medicines; travel support from AnHeart Therapeutics. The authors report no other conflicts of interest in this work.
References
1. Govindan R, Page N, Morgensztern D, et al. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol. 2006;24(28):4539–4544. doi:10.1200/JCO.2005.04.4859
2. Horn L, Mansfield AS, Szczęsna A, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018;379(23):2220–2229. doi:10.1056/NEJMoa1809064
3. Goldman JW, Dvorkin M, Chen Y, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): updated results from a randomised, controlled, open-label, Phase 3 trial. Lancet Oncol. 2021;22(1):51–65. doi:10.1016/S1470-2045(20)30539-8
4. Rikitake Y, Mandai K, Takai Y. The role of nectins in different types of cell-cell adhesion. J Cell Sci. 2012;125(Pt 16):3713–3722. doi:10.1242/jcs.099572
5. Sloan KE, Eustace BK, Stewart JK, et al. CD155/PVR plays a key role in cell motility during tumor cell invasion and migration. BMC Cancer. 2004;4(1):73. doi:10.1186/1471-2407-4-73
6. Kamran N, Takai Y, Miyoshi J, et al. Toll-like receptor ligands induce expression of the costimulatory molecule CD155 on antigen-presenting cells. PLoS One. 2013;8(1):e54406. doi:10.1371/journal.pone.0054406
7. Xu Y, Cui G, Jiang Z, et al. Survival analysis with regard to PD-L1 and CD155 expression in human small cell lung cancer and a comparison with associated receptors. Oncol Lett. 2019;17(3):2960–2968. doi:10.3892/ol.2019.9910
8. Yu X, Harden K, Gonzalez LC, et al. The surface protein TIGIT suppresses T cell activation by promoting the generation of mature immunoregulatory dendritic cells. Nat Immunol. 2009;10(1):48–57. doi:10.1038/ni.1674
9. Boles KS, Vermi W, Facchetti F, et al. A novel molecular interaction for the adhesion of follicular CD4 T cells to follicular DC. Eur J Immunol. 2009;39(3):695–703. doi:10.1002/eji.200839116
10. Stanietsky N, Simic H, Arapovic J, et al. The interaction of TIGIT with PVR and PVRL2 inhibits human NK cell cytotoxicity. Proc Natl Acad Sci USA. 2009;106(42):17858–17863. doi:10.1073/pnas.0903474106
11. Liu S, Zhang H, Li M, et al. Recruitment of Grb2 and SHIP1 by the ITT-like motif of TIGIT suppresses granule polarization and cytotoxicity of NK cells. Cell Death Differ. 2013;20(3):456–464. doi:10.1038/cdd.2012.141
12. Li M, Xia P, Du Y, et al. T-cell immunoglobulin and ITIM domain (TIGIT) receptor/poliovirus receptor (PVR) ligand engagement suppresses interferon-γ production of natural killer cells via β-arrestin 2-mediated negative signaling. J Biol Chem. 2014;289(25):17647–17657. doi:10.1074/jbc.M114.572420
13. Li BT, Shen R, Buonocore D, et al. Ado-trastuzumab emtansine for patients with HER2 -mutant lung cancers: results from a phase II basket trial. J Clin Oncol. 2018;36(24):2532–2537. doi:10.1200/JCO.2018.77.9777
14. Kučan Brlić P, Lenac Roviš T, Cinamon G, et al. Targeting PVR (CD155) and its receptors in anti-tumor therapy. Cell Mol Immunol. 2019;16(1):40–52. doi:10.1038/s41423-018-0168-y
15. Nishiwada S, Sho M, Yasuda S, et al. Clinical significance of CD155 expression in human pancreatic cancer. Anticancer Res. 2015;35(4):2287–2297.
16. Triki H, Charfi S, Bouzidi L, et al. CD155 expression in human breast cancer: clinical significance and relevance to natural killer cell infiltration. Life Sci. 2019;231:116543. doi:10.1016/j.lfs.2019.116543
17. American Association for Cancer Research. Tiragolumab Impresses in Multiple Trials, in Cancer Discov. United States: ©2020 American Association for Cancer Research; 2020:1086–1087.
18. Bendell JC, Bedard P, Bang Y-J, et al. Abstract CT302: phase Ia/Ib dose-escalation study of the anti-TIGIT antibody tiragolumab as a single agent and in combination with atezolizumab in patients with advanced solid tumors. Cancer Res. 2020;80(16_Supplement):CT302. doi:10.1158/1538-7445.AM2020-CT302
19. Kurtulus S, Sakuishi K, Ngiow S-F, et al. TIGIT predominantly regulates the immune response via regulatory T cells. J Clin Invest. 2015;125(11):4053–4062. doi:10.1172/JCI81187
20. Zhang Q, Bi J, Zheng X, et al. Blockade of the checkpoint receptor TIGIT prevents NK cell exhaustion and elicits potent anti-tumor immunity. Nat Immunol. 2018;19(7):723–732. doi:10.1038/s41590-018-0132-0
21. Joller N, Hafler JP, Brynedal B, et al. Cutting edge: TIGIT has T cell-intrinsic inhibitory functions. J Immunol. 2011;186(3):1338–1342. doi:10.4049/jimmunol.1003081
22. Lozano E, Dominguez-Villar M, Kuchroo V, et al. The TIGIT/CD226 axis regulates human T cell function. J Immunol. 2012;188(8):3869–3875. doi:10.4049/jimmunol.1103627
23. Grapin M, Richard C, Limagne E, et al. Optimized fractionated radiotherapy with anti-PD-L1 and anti-TIGIT: a promising new combination. J ImmunoTher Cancer. 2019;7(1):160. doi:10.1186/s40425-019-0634-9
24. Whelan S, Ophir E, Kotturi MF, et al. PVRIG and PVRL2 are induced in cancer and inhibit CD8+ T-cell function. Cancer Immunol Res. 2019;7(2):257–268. doi:10.1158/2326-6066.CIR-18-0442
25. Cho BC, Abreu DR, Hussein M, et al. Tiragolumab plus atezolizumab versus placebo plus atezolizumab as a first-line treatment for PD-L1-selected non-small-cell lung cancer (CITYSCAPE): primary and follow-up analyses of a randomised, double-blind, Phase 2 study. Lancet Oncol. 2022;23(6):781–792. doi:10.1016/S1470-2045(22)00226-1
26. Genentech reports interim results for phase III SKYSCRAPER-01 study in PD-L1 high metastatic non-small cell lung cancer; 2022. Available from: https://www.gene.com/media/press-releases/14951/2022-05-10/genentech-reports-interim-results-for-ph.
27. Rudin CM, Liu SV, Lu S. SKYSCRAPER-02: primary results of a Phase III, randomized, double-blind, placebo-controlled study of atezolizumab (atezo) + carboplatin + etoposide (CE) with or without tiragolumab (tira) in patients (pts) with untreated extensive-stage small cell lung cancer (ES-SCLC). J Clin Oncol. 2022;40(17_suppl):LBA8507.
28. Genentech provides update on phase III SKYSCRAPER-02 study in extensive-stage small cell lung cancer; 2022. Available from: https://www.gene.com/media/press-releases/14947/2022-03-29/genentech-provides-update-on-phase-iii-s.
29. Rudin CM, Awad MM, Navarro A, et al. Pembrolizumab or placebo plus etoposide and platinum as first-line therapy for extensive-stage small-cell lung cancer: randomized, double-blind, phase III KEYNOTE-604 study. J Clin Oncol. 2020;38(21):2369–2379. doi:10.1200/JCO.20.00793
30. Gay CM, Stewart CA, Park EM, et al. Patterns of transcription factor programs and immune pathway activation define four major subtypes of SCLC with distinct therapeutic vulnerabilities. Cancer Cell. 2021;39(3):346–360.e7. doi:10.1016/j.ccell.2020.12.014
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.