")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 20
The Use of Preoperative Video Distraction on Emergence Delirium in Preschool Children Undergoing Strabismus Surgery Under Anesthesia with Sevoflurane: A Randomized Controlled Trial
Authors Wang Y, Chu L, Li H, Du Y, Wang S, Liu Y, Wang G
Received 15 November 2023
Accepted for publication 10 March 2024
Published 22 March 2024 Volume 2024:20 Pages 217—225
DOI https://doi.org/10.2147/TCRM.S447419
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Yue Wang,* Liyan Chu,* He Li, Yingjie Du, Shanshan Wang, Ying Liu, Guyan Wang
Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, Beijing, 100730, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guyan Wang, Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, No. 1 Dongjiaominxiang, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86-13910985139, Email [email protected]
Purpose: The aim of this study was to determine whether preoperative video distraction reduces the incidence of emergence delirium in preschool children under general anesthesia with sevoflurane.
Patients and Methods: In this prospective randomized controlled study, children aged 3– 6 years were randomized to receive either video distraction (Group V) or common clinical practice (Group C) from arrival at the holding area to induction of anesthesia. The primary outcome was the incidence of emergence delirium. Preoperative anxiety scores, assessed by the simple modified Yale Perioperative Anxiety Scale, were also collected.
Results: A total of 160 patients were included in our study. The children in Group V (n=80) exhibited a significantly lower incidence of emergence delirium than did those in Group C (n=80) (12.5% vs 35.0%; RR 0.36, 95% CI 0.19, 0.69; P =0.0008). The maximum Pediatric Anesthesia Emergence Delirium score in Group V was significantly lower than that in Group C (3.0 vs 5.0; mean difference − 2.64, 95% CI: − 4.12, − 1.16; P=0.0003). The simple modified Yale Perioperative Anxiety Scale scores at separation from parents and the onset of inhalation induction in Group V were significantly lower than those in Group C (36.4 ± 9.9 vs 48.2 ± 16.7; mean difference 11.92, 95% CI 7.25, 16.59; P< 0.0001 and 41.5 ± 15.9 vs 59.7 ± 21.5; mean difference 18.11, 95% CI 11.76, 24.47; P< 0.0001).
Conclusion: Preoperative video distraction reduces the incidence of emergence delirium in preschool children who undergo strabismus surgery under general anesthesia with sevoflurane.
Keywords: emergence delirium, anxiety, children, preschool
Introduction
Sevoflurane is commonly used for the induction and maintenance of anesthesia in pediatric strabismus surgery to preserve spontaneous respiration and ensure quick turnover; its advantages include rapid induction and recovery, nonirritating smell and ability to maintain a stable breathing cycle. However, emergence delirium (ED) is a common behavioral disturbance during early recovery from sevoflurane anesthesia in children.1 ED can cause falling or venous cannula dislodgement, affect wound healing, prolong hospitalization, increase medical expenses, and cause dissatisfaction among parents and children. In addition, ED may increase the risk of negative postoperative behavioral changes (NPOBCs).2,3
Eye surgery is also an important risk factor for ED.4,5 Furthermore, preoperative conditions such as anxiety and confusion are risk factors for the development of ED and NPOBCs in children.6–8 Preschool children undergoing surgery are particularly vulnerable to preoperative anxiety and ED.9,10 Other risk factors that contribute to the development of ED include sevoflurane inhalation anesthesia, otorhinolaryngology procedures, parental anxiety, preexisting behaviors of children and negative interactions with health-care providers.11
Video distraction is a nonpharmacological intervention that has been proven to provide control of preoperative anxiety comparable to that of parental presence and premedication with midazolam in pediatric patients.10,12 Preschool children generally like watching cartoons and tend to be immersed in animated videos. Furthermore, multimedia devices are readily available at low cost and are easily accepted by children and parents. However, there are few relevant studies confirming that video distraction can reduce the occurrence of ED.
We conducted this randomized study to determine whether preoperative video distraction reduces the incidence of ED in preschool children who receive general anesthesia with sevoflurane.
Methods
Ethical approval for this study (No. TRECKY2019-072) was provided by the Ethics Committee of Beijing Tongren Hospital, Beijing, China, on 3 June 2019. This trial was registered before patient enrollment at the Chinese Clinical Trial Registry on 24/11/2020 (No. ChiCTR2000040187). This prospective randomized controlled clinical study was conducted from December 2020 to June 2021 at Beijing Tongren Hospital. The research protocol complied with the Consolidated Standards of Reporting Trials (CONSORT) statement and the Helsinki Declaration.
Participants
Children aged 3 to 6 years with an American Society of Anesthesiologists (ASA) physical status score of 1 or 2 scheduled for elective strabismus surgery were enrolled in this clinical study. Written consent was obtained from parents or authorized guardians during preoperative visits. The exclusion criteria were as follows: neuropsychiatric disorders, including mental retardation, attention deficit disorder, autism, and emotional handicap; important organ comorbidities; developmental delay; preoperative use of sedative drugs; and respiratory system infection.
Randomization and Blinding
Enrolled patients were randomly assigned to the control group (Group C) or video distraction group (Group V) according to a computer-generated random assignment scheme. The group allocation was concealed in sealed opaque envelopes. A nurse who was not involved in the study opened a sealed envelope once an enrolled patient arrived at the holding area on the day of surgery. The anesthesiologists and surgeons were not blinded to the allocation because they could see whether a child watched a video. The researchers in charge of evaluating the Pediatric Anesthesia Emergence Delirium (PAED) score, recording the recovery conditions, and attending the follow-up visits one day, one week and one month after surgery were blinded to the allocation.
Intervention
On the day before surgery, a trained anesthesiologist performed the preoperative visit for the inpatient children in the ward, collected general information, and explained the procedures related to anesthesia and surgery to the children and their parents. Afterward, the children were instructed to adapt to the breathing mask and breathe deeply. On the day of surgery, the children were taken to the preoperative holding area approximately 30 minutes before entering the operating room (OR). Ten immensely popular clips among preschool children, including Peppa Pig, Super Wings, Pleasant Goat, Katuri, PAW Patrol, The Octonauts, Boonie Bears, Pig Man, Hey Duggee, and Masha and The Bear, were used to distract the children. Children in Group V chose one of the 10 clips after randomization. They watched the self-selected cartoons with their parents in the holding area using portable tablet personal computers and on the way to the OR after leaving their parents until loss of consciousness after induction with sevoflurane. The children were supervised by the researcher in the holding area and were encouraged to choose another clip if they lost interest in the chosen video. The parents of the children in Group C accompanied them in the holding area while waiting for the operation. During the period from separation from their parents to induction with sevoflurane, storytelling, nonprocedural talk, or humor was used by well-trained pediatric anesthesiologists to distract the children. Three experienced pediatric anesthesiologists were responsible for anesthesia and communication with patients to ensure good standardization of the anesthetic techniques.
Anesthesia
Children in both groups were fasted for at least 6 h for solid food and 2 h for clear liquid. In the OR, both groups were induced with 8% sevoflurane plus 5 L/min oxygen inhalation via the tidal breathing technique. Then, venous access was established, and the laryngeal mask airway (LMA) was inserted after attaining a sufficient depth of anesthesia. Anesthesia was maintained with an inspired sevoflurane concentration of 2–3%. Subsequently, 0.01 mg/kg atropine, 0.15 mg/kg dexamethasone, and 0.1 mg/kg ondansetron were injected intravenously, and 0.1 µg/kg sufentanil was slowly administered. Electrocardiography, pulse oxygen saturation, noninvasive blood pressure, and end-tidal carbon dioxide were monitored throughout the process of anesthesia and surgery. During spontaneous breathing, end-expiratory CO2 was confined to 35–50 mmHg, and synchronized intermittent mandatory ventilation (SIMV) was used to assist ventilation in cases of apnea or end-expiratory CO2 pressure > 55 mmHg. Surgeons routinely administered topical anesthesia and subconjunctival infiltration anesthesia with 2% lidocaine to all patients at the completion of surgery to prevent postoperative pain. After the operation, sevoflurane inhalation was stopped, the LMA was removed under anesthesia, and the children were transferred to the postanesthesia care unit (PACU) for recovery.
Data Collection
Before surgery, the children’s level of anxiety was evaluated by a specially trained anesthesia resident who was not aware of the study purpose and outcomes at 3 time points, that is, upon arrival at the holding area prior to intervention (T1), upon separation from parents (T2), and at the onset of inhalation induction (T3), using the simple modified Yale Perioperative Anxiety Scale (mYPAS-SF). The mYPAS-SF was proposed by Jenkins et al and is an observational measure of preoperative anxiety in young children in the absence of their parents in the OR.13 The score ranges from 22.9 to 100, with a score >30 indicating the presence of anxiety and higher values indicating greater anxiety. During mask induction, the anesthesia resident evaluated the performance of the children using the induction compliance checklist (ICC), which is an objective scale containing 10 negative behavioral groupings. The ICC score represents the sum of the groupings occurring during mask induction, and a higher score indicates worse cooperation. For the purposes of analysis, the ICC scores were stratified into three categories: perfect (ICC score= 0), moderate (ICC score =1-3), and poor (ICC score > 4).14
In the PACU, ED was assessed using the PAED scale every 10 minutes by a well-trained researcher blinded to the study allocation until the children were awake and reached the threshold for leaving the PACU (modified Aldrete score ≥9). The PAED scale consists of 5 psychometric items describing emergence behavior. The scores of each item are summed to obtain a total PAED score ranging from 0 to 20.15 During the recovery of consciousness, the recorded maximum PAED score at any time reflected the severity of the children’s delirium. A maximum PAED score ≥ 10 indicated the occurrence of ED, and a maximum PAED score ≥15 was considered severe ED, which was treated with an intravenous bolus of 1 mg/kg propofol. The length of PACU stay and adverse reactions, including nausea, vomiting, laryngospasm, and hypoxemia (SPO2 <90%), were also recorded.
An investigator who was unaware of the group assignments followed up with the children and their parents one day after surgery and recorded postoperative adverse reactions, including pain, dizziness, nausea, vomiting, and drowsiness, by inquiring about and checking the medical records. The parents were asked to score their satisfaction with their child’s anesthesia-related treatment from waiting in the holding area to being transported out of the PACU on a scale of 0–10, where 0 means very dissatisfied and 10 means very satisfied, and complete the Post Hospitalization Behavior Questionnaire (PHBQ). The PHBQ contains 27 items belonging to six categories of anxiety, including general anxiety, separation anxiety, sleep anxiety, eating disturbances, aggression against authority and apathy/withdrawal.16 For each item, parents assess the extent to which the behavior changed in frequency compared with baseline before surgery. NPOBCs were defined as those with PHBQ scores > 0. The patients’ NPOBCs at one week and one month after surgery were obtained by telephone follow-up.
Outcomes
The primary outcome was the incidence of ED, which was defined as a maximum PAED score ≥ 10 during the recovery stage in the PACU.
The secondary outcomes included the incidence of a maximum PAED score ≥12, severe ED defined as a maximum PAED score ≥ 15, preoperative anxiety level reflected by the mYPAS-SF score, incidence of children who showed anxiety defined as an mYPAS-SF score >30 at T2 and T3, incidence of NPOBCs at one day, one week and one month after surgery, induction compliance, length of PACU stay, incidence of postoperative adverse reactions, parents’ satisfaction, and correlation between preoperative anxiety level and PAED score.
Statistical Analysis
A pilot study revealed that the incidence of ED in Group C was approximately 40%. A 50% reduction in the incidence of ED in Group V was considered clinically significant. A sample size of at least 80 participants per group was required considering an α risk of 0.05 and a power of 80%.
The data were analyzed with SAS 9.4 (SAS Institute Inc., Cary, NC, USA). Normally distributed data are expressed as the mean ± standard deviation (SD), and a t-test was used to compare normally distributed continuous variables. Nonnormally distributed data are expressed as the median (quartiles) (M (Q1, Q3)), and the Mann–Whitney test was used for comparisons between groups. The categorical variables were compared using the chi-square test or Fisher’s exact probability method, and differences were considered statistically significant at P<0.05.
Results
A total of 186 children were assessed for eligibility from December 2020 to June 2021. Twelve children declined to participate, and 14 did not meet the inclusion criteria. A total of 160 patients were included in our study and randomized into one of two groups (Group C, n=80; Group V, n=80; Figure 1).
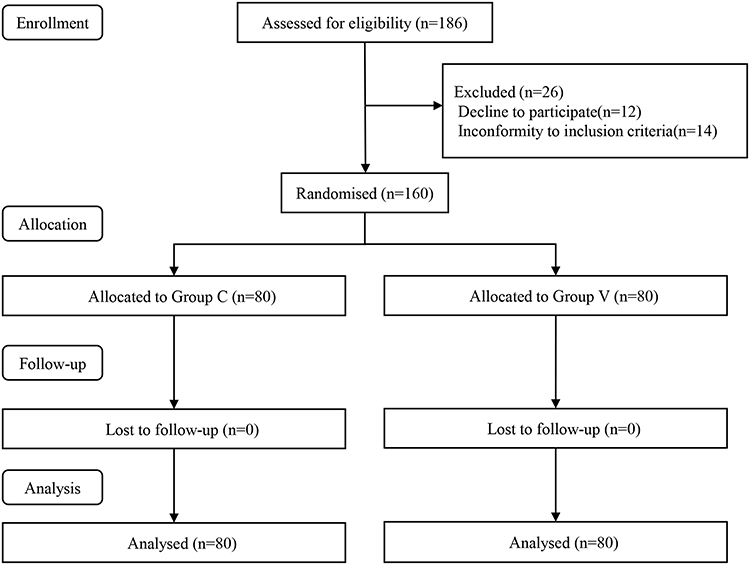 |
Figure 1 CONSORT trial flow diagram. Abbreviations: CONSORT, Consolidated Standards of Reporting Trials, Group C, control group, Group V, video distraction group. Notes: CONSORT figure adapted from Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3): e1000251. Copyright: © 2010 Schulz et al. Creative Commons Attribution License.17 |
There were no statistically significant differences in patient characteristics between the groups (Table 1).
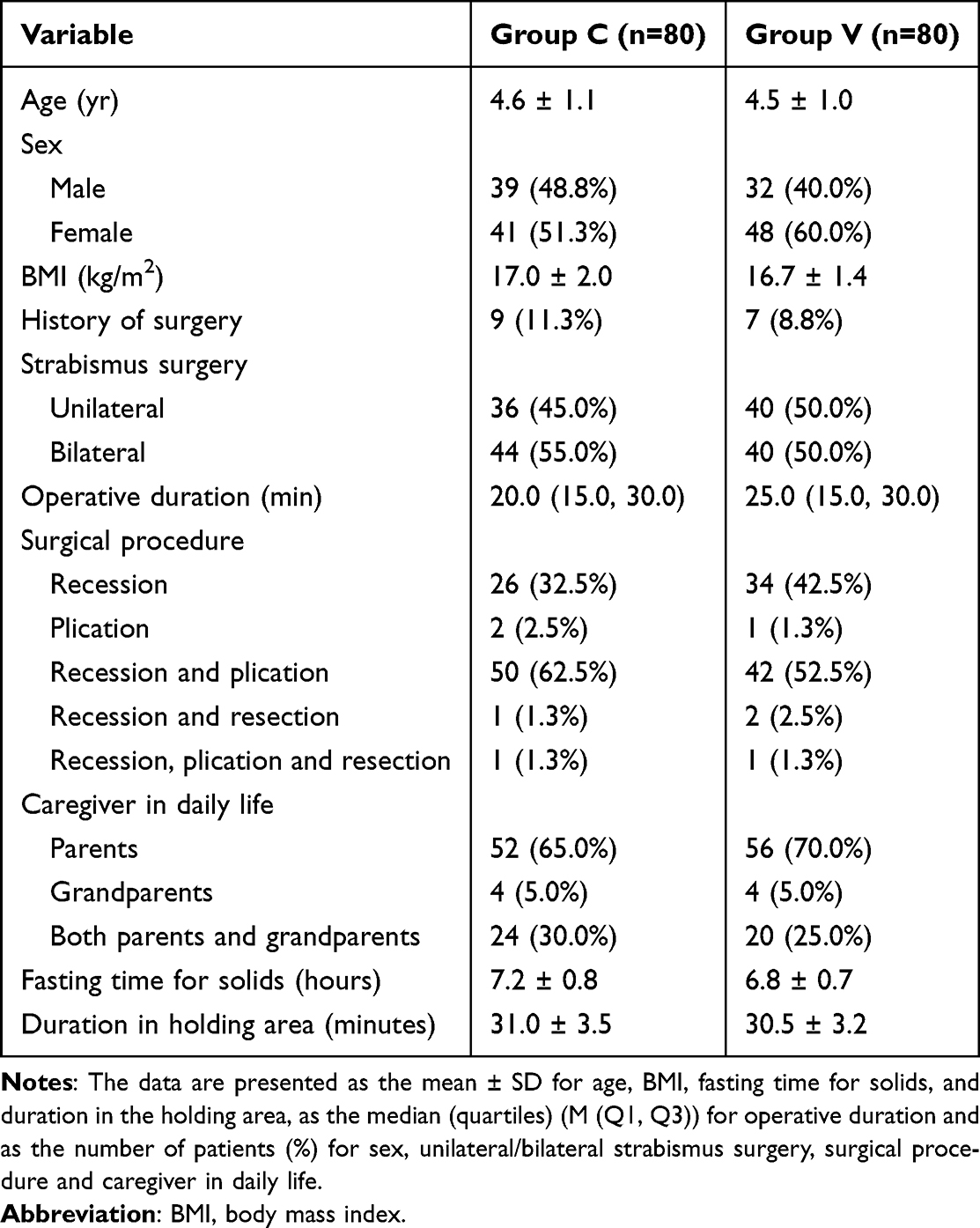 |
Table 1 Demographic and Baseline Characteristics |
Table 2 shows the ED-related outcomes and incidences of NPOBCs after surgery. The incidence of ED in Group V was significantly lower than that in Group C (12.5% vs 35.0%; RR 0.36, 95% CI 0.19, 0.69; P =0.0008). The incidence of a maximum PAED score ≥12 in Group V was significantly lower than that in Group C (8.8% vs 23.8%; RR 0.37, 95% CI 0.16, 0.83; P =0.0101). The maximum PAED score in Group V was also significantly lower than that in Group C (3.0 vs 5.0; mean difference −2.64, 95% CI: −4.12, −1.16; P=0.0003). There were no statistically significant differences in the incidence of severe ED (Table 2). The incidence of NPOBCs in Group V was significantly lower than that in Group C at one day (33.8% vs 66.3%; RR 0.51, 95% CI 0.36, 0.72; P<0.0001) and one week (10.0% vs 22.5%; RR 0.44, 95% CI 0.21, 0.96; P=0.0321) after surgery.
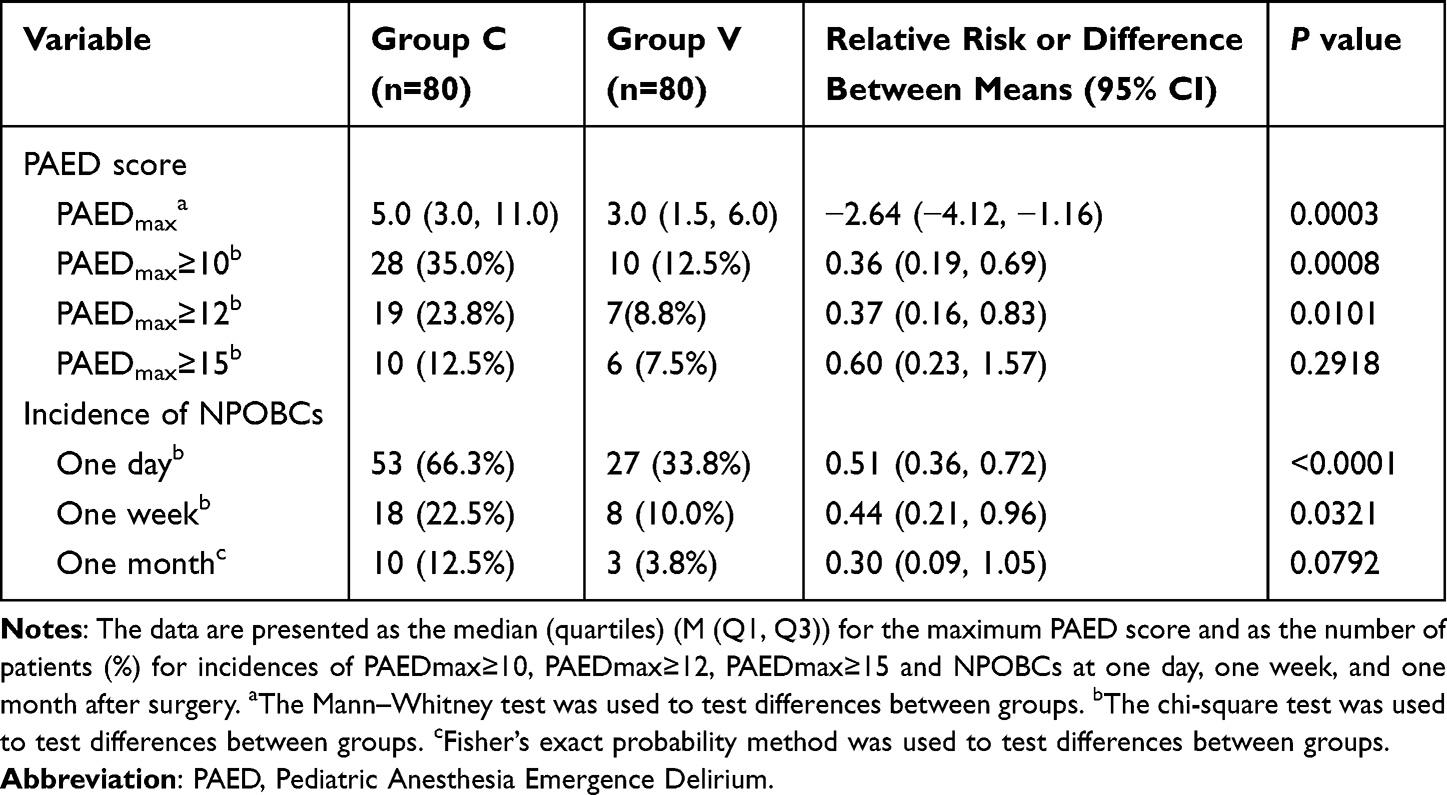 |
Table 2 Emergence Delirium (ED)-Related Outcomes and Incidences of Negative Postoperative Behavioral Changes (NPOBCs) After Surgery |
The mYPAS-SF score at T1 and the proportion of children who exhibited basic anxiety were not significantly different between the two groups (Table 3). The mYPAS-SF scores at T2 and T3 in Group V were significantly lower than those in Group C (36.4 ± 9.9 vs 48.2 ± 16.7; mean difference 11.92, 95% CI 7.25, 16.59; P<0.0001 and 41.5 ± 15.9 vs 59.7 ± 21.5; mean difference 18.11, 95% CI 11.76, 24.47; P<0.0001; Table 3). The proportion of children with mYPAS-SF scores >30 at T2 and T3 in Group V was significantly lower than that in Group C. T2: 60% vs 87.5%; RR 0.69, 95% CI 0.56, 0.84; P<0.0001; T3: 63.8% vs 92.5%; RR 0.69, 95% CI 0.58, 0.82; P<0.0001; Table 3) Compared with the children in Group C, those in Group V had significantly lower ICC scores (1.3 ± 2.1 vs 3.3 ± 3.2; mean difference 2.08, 95% CI 1.24, 2.91; P<0.0001; Table 3), and there were statistically significant differences in the proportions of children with perfect induction compliance (ICC=0) and poor induction compliance (ICC≥4) between the two groups (P=0.0001; Table 3).
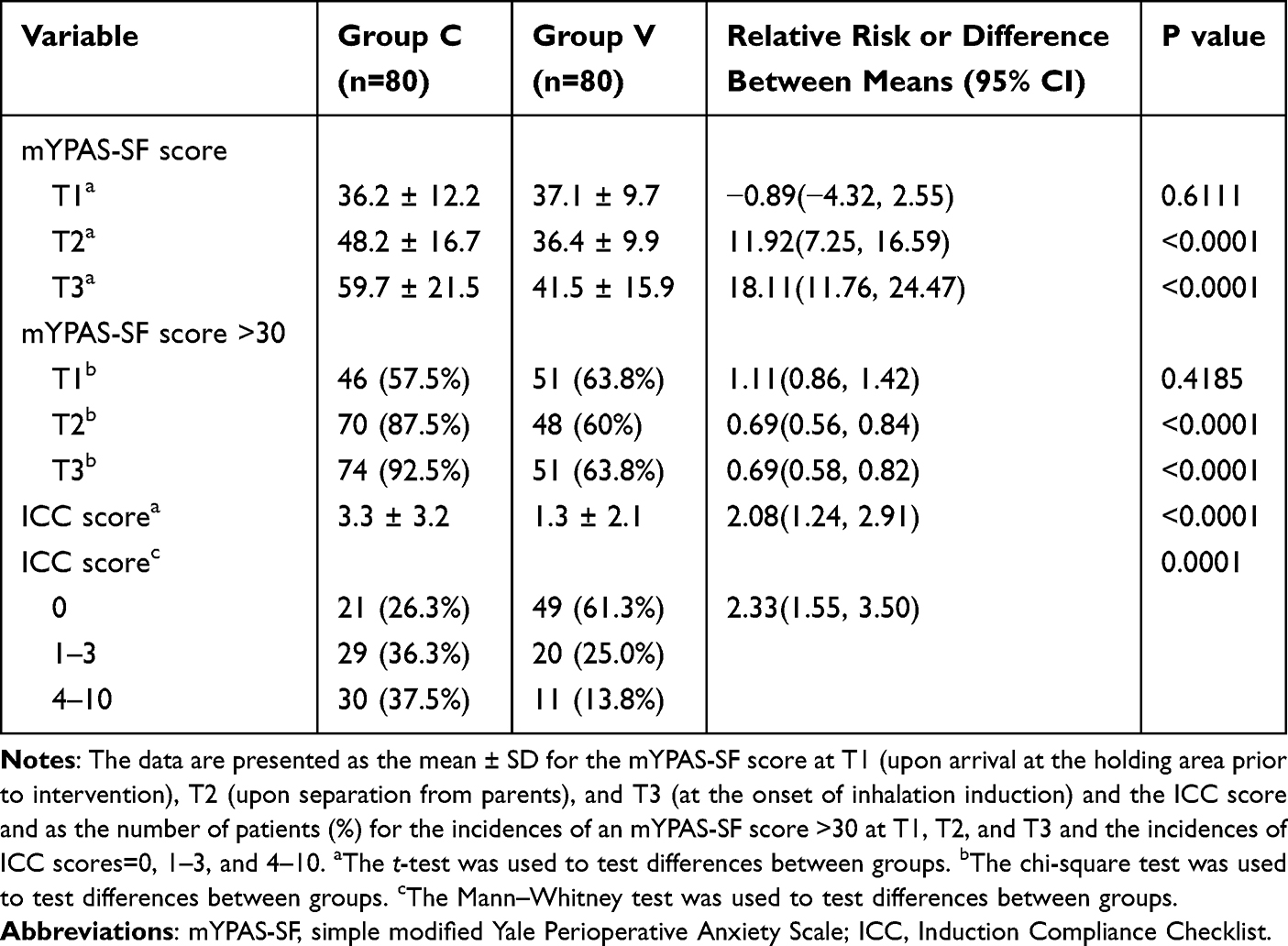 |
Table 3 Patients’ Preoperative Anxiety and Induction Compliance Checklist (ICC) Scores |
There was no statistically significant difference in the length of PACU stay (Table 4). Notably, in the PACU, 2 children in Group C experienced hypoxemia—one due to increased secretion-related hypoxemia and one due to tongue drop-related upper respiratory tract obstruction. Additionally, one patient in Group V experienced severe cough-related hypoxemia. The incidence of adverse reactions that occurred in the ward was low and not significantly different between the two groups (Table 4). Parents’ satisfaction was significantly greater in Group V than in Group C (Table 4).
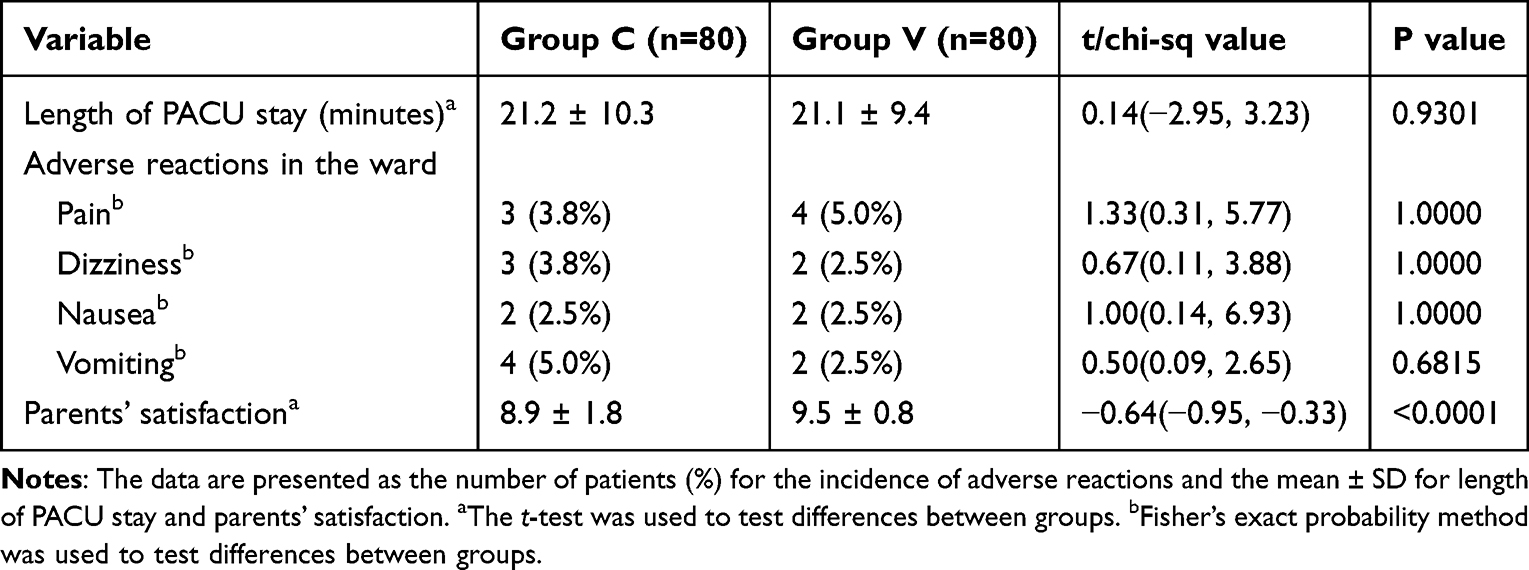 |
Table 4 Length of PACU Stay, Adverse Reactions in the Ward and Parental Satisfaction |
Correlation analysis between preoperative anxiety and ED showed that the mYPAS-SF scores at T2 and T3 were moderately correlated with the maximum PAED score (r=0.3243; P<0.0001 and r=0.4008; P<0.0001).
Discussion
Our study revealed that preoperative video distraction reduced the incidence of ED in preschool children, which may be related to improvements in preoperative anxiety.
ED is commonly observed during early recovery from sevoflurane anesthesia in children.1,18 Medical methods, such as dexmedetomidine, have been verified to effectively reduce the incidence of ED but are accompanied by problems, including noncooperation with medication, prolonged emergence time and hemodynamic changes,19–21 so we do not routinely perform pharmacological premedication. Video distraction, a simple nonpharmacological intervention, was proven to be effective in reducing the incidence of ED while ensuring quick turnover and recovery from strabismus surgery under general anesthesia with sevoflurane in our present study.
Because of differences in the recommended cutoff values in the literature,7,22,23 we further compared the incidence of patients with maximum PAED scores ≥12, and comparison of the two groups showed the same trend as that of patients with maximum PAED scores ≥10. Video distraction failed to decrease the occurrence of severe ED. This may be because the endpoint we set was the incidence of ED; thus, the sample size based on that endpoint was not large enough to verify the difference in the incidence of severe ED. Children experiencing severe ED were restless, inconsolable and not aware of their surroundings during the emergence period in the PACU. Common signs were nonpurposeful resistive movements such as kicking, pulling, and flailing, which put children at risk of self-injury, falling, and venous cannula dislodgement. We used intravenous propofol sedation to relieve severe ED, which has also been reported to be effective.7,24,25 In our study, 10 children in Group C and 6 children in Group V received propofol intravenously because of severe ED, and their conditions obviously improved.
Preschool children have an increased risk of developing preoperative anxiety.10,26 In addition, factors such as negative anticipation of surgical procedures, separation from parents, unfamiliar people and the environment in the OR further distress children in the preoperative stage.27 Children’s preoperative anxiety peaked upon mask introduction. In public hospitals in mainland China, parental accompaniment is not practical or routine during induction due to the relatively limited operating rooms and the large number of surgeries. In addition, it has been reported that parental accompaniment is not reliable for alleviating children’s preoperative anxiety.28,29 Therefore, accompaniment by parents was not allowed once the children went to the OR. We found that most of the children in the two groups experienced anxiety at separating from their parents and mask induction. The level of preoperative anxiety in children with video intervention was reduced, as was the proportion of children with preoperative anxiety. This finding proves that video distraction is an effective behavioral intervention for reducing the preoperative anxiety of preschool children. During inhalation induction of anesthesia, the acceptance of masks is an important factor affecting children’s induction compliance. The day before surgery, the anesthesiologist performing the preoperative visit taught the children to adapt to the breathing mask. Therefore, most children can cooperate with mask induction. Video distraction could reduce children’s anxiety during induction and further improve induction compliance, and these results are consistent with the findings of Lee et al30 and Kim et al12
Preoperative anxiety is an important risk factor for ED in children.6,7 In the correlation analysis, our study also revealed that the level of ED was moderately correlated with the levels of anxiety exhibited at separation from parents and anesthesia induction. In addition, we found decreased NPOBCs in children with video distraction in the relatively short term (one week). However, conclusions cannot be drawn from this finding because the PHBQ has not been properly validated.
There were several limitations to be noted regarding this study. First, observer bias could not be avoided in evaluations of preoperative anxiety and induction compliance because video watching was visible to the evaluator and participants. However, the researchers in charge of evaluating the PAED score, recording the recovery conditions and attending the follow-up visit at one day, one week, and one month after surgery were blinded to the allocation. Second, there was no postoperative pain assessment in the study protocol because we found that the incidence of pain after strabismus surgery under sevoflurane anesthesia and local anesthesia was low, and the degree was slight based on clinical observations and pilot studies. Third, this was a single-center prospective randomized controlled study with a relatively small sample size, and the data need to be assessed in a multicenter clinical study with a larger sample size.
Conclusions
In conclusion, as a simple, economical and safe intervention, preoperative video distraction may effectively reduce the occurrence of ED in preschool children who are undergoing strabismus surgery under general anesthesia with sevoflurane.
Data Sharing Statement
The data are not available to the general public due to the regulations of our institution, but they are available to researchers upon reasonable request by emailing Yue Wang ([email protected]).
Acknowledgments
Assistance with the study: The authors acknowledge the statistical assistance from Dr. Shaofei Su, PhD (Central Laboratory, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Chaoyang).
Funding
Financial support was provided by the Beijing Hospitals Authority Clinical Medicine Development of Special Funding Support (ZYLX202103) and the Beijing Hospitals Authority’s Ascent Plan (DFL20220203).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aono J, Ueda W, Mamiya K, Takimoto E, Manabe M. Greater incidence of delirium during recovery from sevoflurane anesthesia in preschool boys. Anesthesiology. 1997;87(6):1298–1300. doi:10.1097/00000542-199712000-00006
2. Kain ZN, Caldwell-Andrews AA, Weinberg ME, et al. Sevoflurane versus halothane: postoperative maladaptive behavioral changes: a randomized, controlled trial. Anesthesiology. 2005;102(4):720–726. doi:10.1097/00000542-200504000-00005
3. Stargatt R, Davidson AJ, Huang GH, et al. A cohort study of the incidence and risk factors for negative behavior changes in children after general anesthesia. Paediatr Anaesth. 2006;16(8):846–859. doi:10.1111/j.1460-9592.2006.01869.x
4. Cho EJ, Yoon SZ, Cho JE, Lee HW. Comparison of the effects of 0.03 and 0.05 mg/kg midazolam with placebo on prevention of emergence agitation in children having strabismus surgery. Anesthesiology. 2014;120(6):1354–1361. doi:10.1097/aln.0000000000000181
5. Frederick HJ, Wofford K, de Lisle Dear G, Schulman SR. A randomized controlled trial to determine the effect of depth of anesthesia on emergence agitation in children. Anesth Analg. 2016;122(4):1141–1146. doi:10.1213/ane.0000000000001145
6. Kain ZN, Caldwell-Andrews AA, Maranets I, et al. Preoperative anxiety and emergence delirium and postoperative maladaptive behaviors. Anesth Analg. 2004;99(6):1648–1654. doi:10.1213/01.ane.0000136471.36680.97
7. Lin Y, Shen W, Liu Y, et al. Visual preconditioning reduces emergence delirium in children undergoing ophthalmic surgery: a randomised controlled trial. Br J Anaesth. 2018;121(2):476–482. doi:10.1016/j.bja.2018.03.033
8. Urits I, Peck J, Giacomazzi S, et al. Emergence delirium in perioperative pediatric care: a review of current evidence and new directions. Adv Ther. 2020;37(5):1897–1909. doi:10.1007/S12325-020-01317-X
9. Kain ZN, Mayes LC, Weisman SJ, Hofstadter MB. Social adaptability, cognitive abilities, and other predictors for children’s reactions to surgery. J Clin Anesth. 2000;12(7):549–554. doi:10.1016/s0952-8180(00)00214-2
10. Sola C, Lefauconnier A, Bringuier S, Raux O, Capdevila X, Dadure C. Childhood preoperative anxiolysis: is sedation and distraction better than either alone? A prospective randomized study. Paediatr Anaesth. 2017;27(8):827–834. doi:10.1111/pan.13180
11. Mason KP. Paediatric emergence delirium: a comprehensive review and interpretation of the literature. Br J Anaesth. 2017;118(3):335–343. doi:10.1093/BJA/AEW477
12. Kim H, Jung SM, Yu H, Park SJ. Video distraction and parental presence for the management of preoperative anxiety and postoperative behavioral disturbance in children: a randomized controlled trial. Anesth Analg. 2015;121(3):778–784. doi:10.1213/ane.0000000000000839
13. Jenkins BN, Fortier MA, Kaplan SH, Mayes LC, Kain ZN. Development of a short version of the modified yale preoperative anxiety scale. Anesth Analg. 2014;119(3):643–650. doi:10.1213/ane.0000000000000350
14. Varughese AM, Nick TG, Gunter J, Wang Y, Kurth CD. Factors predictive of poor behavioral compliance during inhaled induction in children. Anesth Analg. 2008;107(2):413–421. doi:10.1213/ane.0b013e31817e616b
15. Sikich N, Lerman J. Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale. Anesthesiology. 2004;100(5):1138–1145. doi:10.1097/00000542-200405000-00015
16. Vernon DTA, Schulman JL, Foley JM. Changes in children’s behavior after hospitalization. Some dimensions of response and their correlates. Am J Dis Child. 1966;111(6):581–593. doi:10.1001/ARCHPEDI.1966.02090090053003
17. Schulz KF, Altman DG, Moher D and. (2010). CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. PLoS Med, 7(3), e1000251 10.1371/journal.pmed.100025110.1371/journal.pmed.1000251.g00110.1371/journal.pmed.1000251.t00110.1371/journal.pmed.1000251.s00110.1371/journal.pmed.1000251.s002
18. Goa KL, Noble S, Spencer CM. Sevoflurane in paediatric anaesthesia: a review. Paediatr Drugs. 1999;1(2):127–153. doi:10.2165/00128072-199901020-00005
19. Hauber JA, Davis PJ, Bendel LP, et al. Dexmedetomidine as a rapid bolus for treatment and prophylactic prevention of emergence agitation in anesthetized children. Anesth Analg. 2015;121(5):1308–1315. doi:10.1213/ane.0000000000000931
20. Makkar JK, Bhatia N, Bala I, Dwivedi D, Singh PM. A comparison of single dose dexmedetomidine with propofol for the prevention of emergence delirium after desflurane anaesthesia in children. Anaesthesia. 2016;71(1):50–57. doi:10.1111/anae.13230
21. Chu L, Wang Y, Wang S, Su S, Guo Z, Wang G. Intranasal dexmedetomidine accompanied by cartoon video preoperation for reducing emergence delirium in children undergoing strabismus surgery: a prospective randomized trial. Front Surg. 2021;8:754591. doi:10.3389/fsurg.2021.754591
22. Byun S, Song S, Kim JH, Ryu T, Jeong MY, Kim E. Mother’s recorded voice on emergence can decrease postoperative emergence delirium from general anaesthesia in paediatric patients: a prospective randomised controlled trial. Br J Anaesth. 2018;121(2):483–489. doi:10.1016/J.BJA.2018.01.042
23. Bajwa SA, Costi D, Cyna AM. A comparison of emergence delirium scales following general anesthesia in children. Paediatr Anaesth. 2010;20(8). doi:10.1111/j.1460-9592.2010.03328.x
24. Rosen HD, Mervitz D, Cravero JP. Pediatric emergence delirium: Canadian pediatric anesthesiologists experience. Paediatr Anaesth. 2016;26(2):207–212. doi:10.1111/PAN.12812
25. Hallén J, Rawal N, Gupta A. Postoperative recovery following outpatient pediatric myringotomy: a comparison between sevoflurane and halothane. J Clin Anesth. 2001;13(3):161–166. doi:10.1016/S0952-8180(01)00236-7
26. Vetter TR. The epidemiology and selective identification of children at risk for preoperative anxiety reactions. Anesth Analg. 1993;77(1):96–99. doi:10.1213/00000539-199307000-00019
27. Kain ZN, Mayes LC, Caramico LA, et al. Parental presence during induction of anesthesia. A randomized controlled trial. Anesthesiology. 1996;84(5):1060–1067. doi:10.1097/00000542-199605000-00007
28. Kain ZN, Mayes LC, O’Connor TZ, Cicchetti DV. Preoperative anxiety in children. Predictors and outcomes. Arch Pediatr Adolesc Med. 1996;150(12):1238–1245. doi:10.1001/ARCHPEDI.1996.02170370016002
29. Fortier MA, Del Rosario AM, Martin SR, Kain ZN. Perioperative anxiety in children. Paediatr Anaesth. 2010;20(4):318–322. doi:10.1111/j.1460-9592.2010.03263.x
30. Lee J, Lee J, Lim H, et al. Cartoon distraction alleviates anxiety in children during induction of anesthesia. Anesth Analg. 2012;115(5):1168–1173. doi:10.1213/ANE.0b013e31824fb469
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.