")
Back to Journals » Patient Related Outcome Measures » Volume 13
The Use of Patient Engagement to Gather Perceptions on the Cost of Infant Feeding
Authors Blackmore A , Etchegary H, Allwood-Newhook LA, Gao Z , Nguyen HV, Parsons-Mercer K, Twells L
Received 18 March 2022
Accepted for publication 7 July 2022
Published 23 November 2022 Volume 2022:13 Pages 239—247
DOI https://doi.org/10.2147/PROM.S366721
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
Alicia Blackmore,1 Holly Etchegary,1,2 Leigh Anne Allwood-Newhook,3 Zhiwei Gao,1 Hai Van Nguyen,4 Kaylah Parsons-Mercer,5 Laurie Twells1
1Faculty of Medicine, Memorial University of Newfoundland, St. John’s, Newfoundland and Labrador, Canada; 2Scientific Patient Engagement Lead of NL SUPPORT Unit, St. John’s, Newfoundland and Labrador, Canada; 3Department of Pediatrics, Faculty of Medicine, Memorial University of Newfoundland, St. John’s, Newfoundland and Labrador, Canada; 4School of Pharmacy, Memorial University of Newfoundland, St. John’s, Newfoundland and Labrador, Canada; 5Patient Partner, St. John’s, Newfoundland and Labrador, Canada
Correspondence: Alicia Blackmore, Faculty of Medicine, Memorial University of Newfoundland, St. John’s, Newfoundland and Labrador, Canada, Email [email protected]
Purpose: Patient-oriented research (POR) and patient engagement (PE) has highlighted the value of incorporating patients’ ideas and priorities in health research. Using the guiding principles of POR and PE, the current study conducted PE sessions to gain insight on the perceptions of mothers regarding the costs of infant feeding.
Methods: Four patient engagement sessions were held with mothers residing in Newfoundland and Labrador between November 2019 and January 2020. Mothers were targeted through the Brighter Futures Coalition of St. John’s, a not-for-profit community organization. PE sessions were designed in a two-hour format, allowing the research team to engage mothers and identify costs of infant feeding from a mothers’ perspective.
Results: Through the guiding principles of patient-oriented research and patient engagement, our research team successful engaged with mothers in discussions surrounding the costs of infant feeding. The sessions allowed for an in-depth discussion surrounding monetary costs (eg, incidentals of breast or formula feeding), the associated costs of infant feeding and the workplace (eg, perceived productivity) and environment impacts (eg, single use plastics). During each session, evaluations were provided to solicit feedback on whether the goals and expectations of mothers had been met, and whether they felt their opinions were heard and understood.
Conclusion: By conducting patient engagement sessions, informed by patient-oriented research guiding principles, we were able to successfully recruit and engage mothers in discussions that led to a better understanding of their perspectives on the costs of infant feeding.
Keywords: patient engagement, infant feeding, patient-oriented research
Introduction
Recently, there has been a move toward involving both the patients and the public in health research, called patient-oriented research. Patient-oriented research highlights the value of incorporating patients’ ideas and priorities, improving the overall relevance and quality of research outcomes. It is defined as:
Research that engages patients, their caregivers, and families as partners in the research process. Where patients are defined as an overarching term and includes those with personal experience, their caregivers, family members and friends. This engagement helps to ensure that studies focus on patient-identified priorities, which ultimately leads to better patient outcomes….1
There are various ways of addressing and incorporating patient ideas and priorities into research designs, with varying levels of patient engagement as defined by the International Association for Public Participation (IAP2) spectrum.2 The IAP2 identifies five levels of engagement: inform, consult, involve, collaborate, and empower, where the depth of patient involvement deepens with the progression across the spectrum of these levels.2,3 These levels allow for involvement to vary based on the input and decision-making patients provide.3 Patient engagement sessions allow for “meaningful collaboration”, where patients have the ability to become actively engaged throughout various project stages including: governance, priority setting, research question development, and research performance.4 While there is no gold standard for patient engagement, there are several key principles that allow patients to thrive in patient-oriented research. Meaningful patient engagement is guided by: inclusiveness, support, mutual respect, flexibility, responsiveness, and accountability.3
An area of research that would provide invaluable insight to its research outcomes using patient-oriented research would be in cost analyses, specifically those examining the costs associated with breast and formula feeding. Over the last number of decades researchers have examined the value of breastfeeding and its association with lower rates of infant illness, and subsequently health-care service use, including number and duration of hospital admissions, emergency room and physician visits.5,6 Studies have found that based on the protective effect of breastfeeding on a number of acute infections in infancy, and chronic illnesses in childhood, low breastfeeding rates impact the costs to the health-care system.7,8 Researchers have also examined the indirect costs that are associated with infant feeding. This includes costs that are incurred by patients or families because of their infections or illness.9 Taking all costs into consideration, researchers in the US have examined the economic impact to the health-care system, society and the costs related to premature death, demonstrating how suboptimal breastfeeding rates cost the US economy $14billion annually.10 By demonstrating the economic benefits of increasing breastfeeding rates, policymakers can make informed decisions around the development of policies and programs to invest in breastfeeding support.
While cost analyses have examined a wide scope of outcomes associated with the costs of infant feeding, there is still a gap when considering the cost of infant feeding to mothers and families, largely, the opportunity costs associated with a mothers’ time and caregiving, especially that spent breastfeeding.11 With a gap in costs related to mothers, we sought to engage mothers using the principles of patient-oriented research, to obtain their perceptions on the associated costs of infant feeding. By engaging with those with lived experience, we sought to obtain their perspectives on additional costs and outcomes that could be considered in future cost analyses.
The overarching goal of patient-oriented research and the development of patient engagement is to ensure research is relevant, valuable and a priority to those it impacts directly. In this paper we provide an example of using patient-oriented research, specifically patient engagement methods to explore costs of infant feeding from mothers’ perspectives. Using the guiding principles of patient-oriented research and patient engagement, our aim was to engage with mothers, to gather their perceptions on the costs of infant feeding. By identifying and prioritizing costing outcomes of importance to mothers’, our study hopes to guide future research around the costs of infant feeding, from a mother's perspective.
Materials and Methods
Aim
The purpose of this study was to use the principles of patient-oriented research and patient engagement, and conduct sessions to engage with mothers and gather their perceptions on the costs of infant feeding. Engaging with mothers provides an opportunity to identify additional costing outcomes that may not have been previously considered in cost analyses. By engaging with those with lived experience, our aim was to gain insight on the cost of infant feeding from a mother's perspective.
Design
Patient engagement sessions were developed to engage mothers in a discussion surrounding the costs of infant feeding. Based on the International Association for Public Participation spectrum, the sessions allowed mothers to be engaged at an informed and collaborative level.2 The GRIPP2 Reporting Checklist – Short Form was used and is further described in the Supplemental Material, (Table S1).12 The patient engagement sessions were designed in a two-hour format, which allowed for introductions, background information on infant feeding and studies examining the economic impact of infant feeding. A 20-min presentation was developed which covered the introductions of the team, background information related to patient-oriented research, and an overview of the research being conducted at the Memorial University of Newfoundland. In order to facilitate discussion and ensure consistency across sessions, questions were developed prior to the sessions. Questions prompted the discussion of various feeding modes, and from their perspectives what outcomes should be considered in future cost analyses. This then led to a discussion centred around a mothers’ perceptions on the costs of infant feeding during their infants first year of life. Since infant feeding journeys are individual in their experiences, these sessions provided a safe avenue for discussing different views and opinions. The session facilitator (AB) kept the discussion on track and promoted an open platform for each mother to bring forth all experiences. This allowed all mothers to take part in the discussion and ensured those with similar or differing perspectives were highlighted.
Setting
Four sessions were held with mothers residing in Newfoundland and Labrador between November 2019 and January 2020. Mothers were targeted through the Brighter Futures Coalition of St. John’s, a not-for-profit organization made up of parents, community members, and professionals from the area. Members of the research team attended family resource centres, to provide a baby-friendly environment where patient engagement sessions could be conducted. Lunch was provided to those in attendance as a thank you for their time.
Data Collection
The recruitment process involved connecting with mothers and asking if they would be interested in attending a patient engagement session and partake in discussions surrounding the costs of infant feeding. By connecting with a community organization, this study recruited a convenience sample of individuals who attend the family resource center, who were currently pregnant, or had given birth within the last year. By attending the PE sessions, mothers provided their consent to partake in this study and provide their experiences and perspectives in identifying future research outcomes. Following written consent for audio recording, a digital recorder was placed in the centre of the room to capture the sessions. Qualitative data collection was used, where detailed notes were taken by both team members, while audio recorders were replayed at a later date to capture any additional information from the sessions. Following each session, notes were compiled regarding emerging topics. At the end of the sessions, a printed survey was circulated to mothers to collect demographic information and an evaluation of the usefulness of the session. Mothers were encouraged to complete all survey questions and make note of any comments, questions or concerns moving forward. This provided the team with an opportunity to have the session critiqued for completeness, detail, information provided, and discussion upheld.
Data Analysis
Written notes from the sessions and audio recordings comprise the data for analysis. Information was collected on the emerging topics based on mothers’ discussions from prompted questions. Information was written and presented as a comprehensive summary of the mothers’ ideas. AB and RS discussed the written notes and comprehensive summary with the other team members to ensure they were the key themes.
Ethical Approval
Ethical Approval for the current study was deemed unnecessary by The Newfoundland and Labrador Health Research Ethics Authority (personal communication) as the objective of the sessions was to engage with patient partners to help inform future research questions and methodology. Their provided guidelines are informed by both Involve (a government-funded entity supporting public involvement in the National Health Service in the UK) and the Canadian Institutes of Health Research Ethics Guidance.
Results
By following the guiding principles and best practices for patient-oriented research and developing patient engagement sessions, we were able to actively engage with community groups (eg, Brighter Futures Coalition) who shared information on the engagement sessions through various means (eg, Facebook). This organization schedules weekly gatherings for mothers to attend within their community, and members of the research team were able to put off the patient engagement sessions in these settings. During the sessions, the research team along with mothers, explored and discussed the costs associated with infant feeding.
Four sessions were held, with 26 mothers and 18 babies (16 singletons, 1 set of twins) in community settings. On average, sessions lasted two hours each. Demographic information was captured for all but two mothers. The majority of mothers were Caucasian (n = 22), married or common law (n = 20), between 26 and 34 years of age (n = 15), and with a university degree or diploma (n = 15). All mothers were accessing care in the Eastern Health Region of Newfoundland and Labrador (n = 26). The majority of mothers were primiparous (n = 20), and 46% exclusively breastfed (n = 12) (breast milk only, no other food or water) and exclusively formula fed (n = 12) (defined as only formula), while 8% used a mixed feeding method (n = 6). Demographic information is outlined in Table 1.
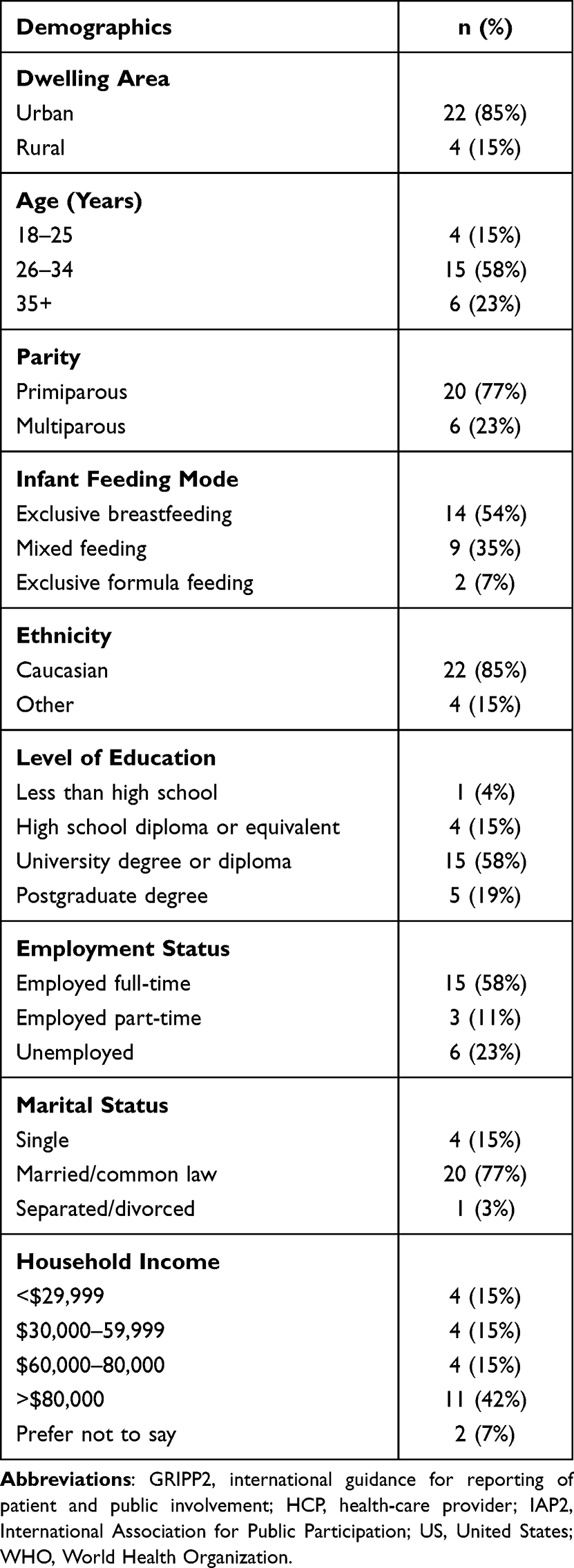 |
Table 1 Sample Characteristics |
There were a number of topics that arose from the patient engagement sessions, in terms of what outcomes should be considered when examining the costs incurred to mothers and families related to infant feeding. Based on the literature review around the gaps associated with the costs of infant feeding, we developed open-ended questions prior to the sessions to cover topics related to general costs of feeding, workplace productivity, and environmental impacts associated with infant feeding. A summary of information collected, and outcomes discussed based on prompted questions are outlined in Table 2.
 |
Table 2 Outcomes of Interest Identified by Mother’s |
Printed evaluation forms were circulated at the end of each session. Scales were provided as a method of ranking their satisfaction with the session, as well as open-ended responses regarding their experiences and how the session could be improved. Mothers felt that the session was detailed, complete, and easy to understand. They felt that they had enough information to actively engage in the discussions, and felt their opinions were heard and understood. Notably, there was a higher uptake in responses for scaled questions in comparison to questions that required a written response. Detailed responses to their evaluation can be found in the Supplementary Materials (Table S2).
Discussion
One of the valuable components of patient-oriented research is that through patient engagement, individuals with lived experience have the opportunity to help inform the development of future research questions. Patient engagement provides an avenue for exploring patient perspectives on a particular health-care issue that is relevant to them. Engaging those with lived experience can provide meaningful input to the research agenda. It can be argued, that having a better understanding of their perspectives is a critical component in developing future areas of research. Due to limited research on the costs of infant feeding from a mothers’ perspective, we conducted patient engagement sessions to explore the perceptions of mothers on this topic.
Using the guiding principles of patient-oriented research, patient engagement sessions were planned and successfully conducted to explore and better understand the costs of infant feeding from a mothers’ perspective. The key principles of patient engagement played an important role in the success of our sessions. Our patient engagement sessions included a range of perspectives and experiences (ie, inclusiveness), and mothers that felt sufficiently supported to meaningfully contribute to the discussion (ie, support). The structure of the sessions allowed for various levels of involvement (ie, flexibility), where mothers felt acknowledged and valued and were able to engage and provide input at the level of their comfort (ie, mutual respect). During each session, evaluations were provided to solicit feedback on whether the goals and expectations of mothers had been met, and whether they felt their opinions were heard and understood (ie, responsive).
For our research on infant feeding, engaging mothers with lived experience brought to our attention constructs that captured a more holistic view of the costs of infant feeding than may typically be considered or measured in cost analysis studies. The outcomes identified by mothers illustrate the value of using patient-oriented research in engaging those with lived experience. Overall, three broad categories were discussed, costs of infant feeding, impact on workplace productivity and environmental impact. The patient engagement sessions allowed us to explore in-depth how women perceived these categories of costs, further elucidating the types of costs that would fall under these categories. For example, the costs on infant feeding included discussions on the incidentals of breast or formula feeding (eg, nipple creams, bottles, bottle warmers), discussions around workplace productivity (eg, perceived productivity, needing additional breaks related to feeding, time off), and discussions around environmental impacts (eg, single use plastics, breast pads, ready-made formula). Interestingly, in the sessions there were conversations among mothers around the opportunity costs associated with infant feeding (eg, cost of mothers’ time (time spent feeding, cleaning/preparing bottles, outsourcing guidance, and support), the cost of inaccessibility of health-care providers and support when establishing infant feeding mode). In all patient engagement sessions, independent of discussions around costs, all mothers reported the need for more information, knowledge and support related to infant feeding, whether infants were breast or formula fed. Due to limited support around infant feeding, mothers discussed the additional time, effort, and costs spent looking for information and support while establishing breast or formula feeding (eg, information on breast-pumping or preparing formula, paying for private lactation consultants). Referencing the critical role that health-care providers can play during the stages of mothers establishing infant feeding (ie, lactation consultants, public health nurses, general practitioners, and specialists).
Topics identified by mothers that have been previously examined in cost analyses included the cost of incidentals for either feeding method, where researchers have attempted to outline the potential costs incurred by families related to breast or formula feeding,13 as well as the timing spent feeding their babies, which has been examined, but is yet to be considered in a larger global scale cost analysis.14 Mothers felt that understanding the costs that may be incurred to families during their infant's first year of life related to infant feeding, may allow them to better prepare financially. Other researchers have also considered the importance of the time required by families during that first year of life to promote and support their infant feeding journeys, relating to paid maternity leave.15 Researchers have examined the impact of paid parental leave on the ability to enhance population health, by providing families a greater opportunity to achieve breastfeeding initiation and longer breastfeeding durations.15
Additional emerging topics that may not have been previously identified by mothers in this context include the importance of the workplace. Mothers outlined their concerns with perceived productivity in the workplace when returning from maternity leave, requiring time and resources for breast pumping milk, or the necessity for their own personal sick or vacation days now being used for purposes related to their infant. Mothers mentioned the impact of their career on infant feeding, and how for some it is not feasible to have planned breaks throughout their workday, or how being self-employed or a business owner can impact infant feeding journeys. These emerging topics highlighted the importance of having a work environment conducive to mothers’ infant feeding journeys. This highlights the importance of workplace policies and legislation and better understanding the needs of mothers during this time.16 Policies which include access to breastfeeding friendly spaces (eg, a clean and comfortable space if breast pumping, somewhere to store pumped milk, or to clean equipment), and if feasible, the ability to spend a scheduled work break feeding their infant (ie, by breast pumping, or by having sufficient time to return home). Another topic that has been emerging in infant feeding research includes examining the environmental impact of formula feeding companies.17 Mothers brought to our attention the environmental impact of either feeding method. Their concerns were with their use of single-use plastics (eg, breast pads, storage bags for breast milk, premade liquid formula) and the waste associated with both feeding methods, which has not been considered. Conducting patient engagement sessions, as an element of patient-oriented research, allowed for much more in-depth discussion on the costs of infant feeding not reported elsewhere. This information may help to inform future cost analyses related to the economic impact of infant feeding.
We have several recommendations for future patient-oriented researchers, from our lessons learned throughout the creation, planning, and implementation phases of our patient engagement sessions. These lessons are those learned from our engagement sessions, but would be applicable to other researchers engaging in patient-oriented research. First, linking up our research team with a community organization, was a key component to our successful patient engagement. Inserting ourselves as researchers in a community setting led to active engagement and collaboration in a setting that was welcoming to those we wanted to engage with. We recommend that by engaging community organizations, researchers can more easily connect with and engage with those with lived experience. Second, throughout each session information on the topics discussed was compiled in various formats (audio recording, written notes, evaluation forms). This allowed the team members to better understand ideas of mothers and identify any additional outcomes to be further discussed or discussed at the following patient engagement sessions. Third, having an understanding of the needs of those you are engaging with is paramount for optimal engagement. Our sessions allowed mothers to attend with their infants, so upon the completion of a session when printed surveys were circulated, it was not as feasible for mothers to spend time completing evaluations. Specifically, the time required to fill out free-text questions, therefore in future we would consider altering the format of these surveys to better fit those in attendance (eg, verbal discussions vs paper format). Fourth, patient engagement requires time and resources to uphold these sessions and contact between those that have been engaged. By preparing for the time and resources required, it ensured mothers remained informed, involved, and updated at several project stages.
This study identifies costs and outcomes to be included in a broader approach to measurement in a cost analysis from a mother’s perspective. Moving forward, we hope that the use of patient-oriented research, specifically patient engagement, can inform future research questions and further expand on cost analyses on infant feeding. Future research should consider including additional outcomes in cost analyses examining the economic impact of infant feeding. In addition, future research should examine the effectiveness of infant feeding supports, prior to examining the cost effectiveness of interventions.
Limitations
Patient engagement has its limitations, based on funding, timing and recruitment. Due to the small numbers engaged throughout these sessions, there is a possible underrepresentation of individuals falling in different sociodemographics, as well as a bias that may present itself in smaller group sessions. Notably, with additional sessions there is potential for additional emerging topics and key priorities for future studies to arise. At the end of each session printed evaluations were circulated to mothers. We found additional incentives were needed regarding obtaining session feedback in this format. In future sessions we would ensure that the evaluation is in a format that is more easily completed (eg, verbal discussion vs printed survey).
To our knowledge this is the first study using patient engagement as a method of engaging mothers to identify costing factors related to infant feeding. These sessions allowed for a rich discussion regarding mothers’ perspectives, information that would not necessarily be captured in standard surveys or cost analysis measures. It allowed for a group collaboration in describing their experiences, which then allowed us to draw emerging topics which can inform future research questions associated with the costs of infant feeding.
Conclusion
Patient-oriented research has highlighted the value of incorporating patients’ ideas, priorities, and experiences in health research. By conducting PE sessions, informed by patient-oriented research guiding principles, we were able to successfully recruit and engage mothers in discussions that led to a better understanding of their perspectives on the costs of infant feeding.
Acknowledgments
We would like to thank the NL SUPPORT Unit for their guidance and support in organizing the patient engagement sessions (Kate Lambert, Kathleen Maher, Chelsey McPhee), as well as masters student, Rosie Stanoev, for attending sessions and recording minutes of the sessions. We would also like to thank the organizations that welcomed our team to engage with mothers in a community setting – and to all of those that attended and provided their time, perspectives, and experiences.
Disclosure
The authors report no conflicts of interest in this work. Funding for the patient engagement sessions were provided by the NL SUPPORT Unit through a patient engagement grant. NL Support also provides the educational funding for the lead author. The funding body had no role in the design of the study, data collection, analysis, and interpretation or in the writing of the manuscript.
References
1. CIHR. Strategy for patient oriented research. Available from: https://cihr-irsc.gc.ca/e/41204.html.
2. IAP2 Spectrum of public participation. Available from: https://patientvoicesbc.ca/resources/iap2-spectrum-public-participation/.
3. Parfrey PS, Barrett B. Chapter 29, changing health-related behaviours 1: patient-oriented research and patient engagement in health research. In: Clinical Epidemiology: Practice and Methods in Molecular Biology. Springer Nature; 2021.
4. CIHR. Patient Engagement. Available from: https://cihr-irsc.gc.ca/e/45851.html.
5. Ip S, Chung M, Raman G, et al. Breastfeeding and maternal and infant health outcomes in developed countries. In: Evidence Report/Technology Assessment Number 153. Rockville, MD: Agency for Healthcare Research and Quality; 2007.
6. Duijts L, Jaddoe VW, Hofman A, Moll HA. Prolonged and exclusive breastfeeding reduces the risk of infectious diseases in infancy. Pediatrics. 2010;126:e18–e25. doi:10.1542/peds.2008-3256
7. Dieterich CM, Felice JP, O’sullivan E, Rasmussen KM. Breastfeeding and health outcomes for the mother-infant dyad. Pediatr Clin North Am. 2013;60(1):31–48. doi:10.1016/j.pcl.2012.09.010
8. Shiva F, Ghotbi F, Padyab M. Infant feeding and hospitalization during the first six months of life. JPMA. 2007;57(12):599–603.
9. Bartick MC, Stuebe AM, Schwarz EB, Luongo C, Reinhold AG, Foster EM. Cost analysis of maternal disease associated with suboptimal breastfeeding. Obstet Gynecol. 2013;122(1):111–119. doi:10.1097/AOG.0b013e318297a047
10. Bartick MC, Schwarz EB, Green BD, et al. Suboptimal breastfeeding in the United States: maternal and pediatric health outcomes and costs. Matern Child Nutr. 2017;13(1):e12366. doi:10.1111/mcn.12366
11. Smith JP. Counting the cost of not breastfeeding is now easier, but women’s unpaid health care work remains invisible. Health Policy Plan. 2019;34(6):479–481. doi:10.1093/heapol/czz064
12. Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. Res Involv Engagem. 2017;3(1):13. doi:10.1186/s40900-017-0062-2
13. Bartick M. Breastfeeding and the US economy. Breastfeed Med. 2011;6(5):313–318. doi:10.1089/bfm.2011.0057
14. Smith JP, Forrester R. Who pays for the health benefits of exclusive breastfeeding? An analysis of maternal time costs. J Hum Lact. 2013;29(4):547–555. doi:10.1177/0890334413495450
15. Burtle A, Bezruchka S. Population health and paid parental leave: what the United States can learn from two decades of research. InHealthcare. 2016;4(2):30. doi:10.3390/healthcare4020030
16. Strang L, Broeks M. Maternity leave policies: trade-offs between labour market demands and health benefits for children. Rand Health Q. 2017;6(4):9.
17. Perdue RT, Sbicca J, Holcomb J. A life cycle approach to food justice: the case of breastfeeding. Environ Justice. 2012;5(3):168–172. doi:10.1089/env.2011.0040
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.