")
Back to Journals » Clinical Ophthalmology » Volume 18
The Underutilization of Mental Health Care Services in the Lives of People with Blindness or Visual Impairment: A Literature Review on Rehabilitation Factors Toward Provision
Authors Richardson CG
Received 28 September 2023
Accepted for publication 21 March 2024
Published 29 March 2024 Volume 2024:18 Pages 953—980
DOI https://doi.org/10.2147/OPTH.S442430
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Richardson.
Views: 55
Clairissa G Richardson
School of Social Work, Simmons University, Boston, MA, USA
Correspondence: Clairissa G Richardson, School of Social Work, Simmons University, 300 the Fenway, Boston, MA, 02115, USA, Tel +1 401 206 0458, Email [email protected]
Purpose: Roughly 3 million adult Americans have a visual impairment or blindness, and over 4 million adults aged 40 and older. Despite data demonstrating an elevated prevalence of mental health symptoms in people with BVI, this population remains largely untreated. Given that people with BVI often interface with multiple systems of rehabilitative care that are designed to improve quality of life, the relatively low rates of initiation of mental health care services are particularly alarming. In this review, the systematic processes of mental health care services across pertinent rehabilitation groups are identified and critically examined.
Patients and Methods: A comprehensive literature review was conducted. The literature review utilized a critical systems typology, whereby relevant literature was selected, reviewed, and analyzed intra and extra organizationally. In addition, a thorough discussion of disability-related factors was provided, lending a socio-political lens to the problem.
Results: Considerable data indicates that short-term mental health care services for people with BVI are ineffective treatment methods, albeit primarily employed in health-rehabilitative processes. Multiple studies offered data indicating the presence of diverse and entangled mental health issues relative to vocational rehabilitation services, mobility tool utility, and emotional reactions to vision loss. Many studies suggested that disability identity work be integrated into health-rehabilitative processes for people with BVI.
Conclusion: To improve the utility of mental health care services for people with BVI, a reenergization of the mental health care needs of this population must occur. A critical podcast or forum focused on educating listeners about the health-rehabilitation factors that influence the provision of mental health care services can aid to improve future mental health policy and practice for people with BVI. Disability scholars need to advance research on integrating critical theories in work with people with BVI and accelerate qualitative, community-based methods to enhance understanding of this population and their unique mental health needs.
Keywords: blindness, visual impairment, critical theories, vocational rehabilitation, mental health, orientation and mobility, rehabilitation, vision loss
Introduction
According to the World Health Organization (WHO),1 as many as 2.2 billion people have impaired vision worldwide. Of these individuals, 39 million are blind, and an estimated 246 million have visual impairments.1 In the United States, almost one-third of people with blindness or visual impairment (BVI) experience subclinical depression and anxiety, while around 5% to 7% have a major depressive disorder and 7% have an anxiety disorder, with a significantly higher percentage compared with those having a healthy vision.2 Numerous other studies have demonstrated a link between vision impairment and depression specifically (eg,3–5). People with BVI experience a range of mental health issues, including reduced quality of life,6 accidental injuries,7 mental fatigue,8 and poor social contact,9 which can induce feelings of loneliness.10 With age-related eye diseases being the leading cause of disability among aging adults in the United States (eg,11,12), these findings are a personal and national issue.13
Most research and subsequent treatment interventions operate dichotomously in the conceptualization of causality regarding mental health among people with BVI, advancing the conclusion that such problems are either related to physical impairment (eg,5,14) or social structure (eg,15,16). However, a recent literature review performed by Demmin and Silverstein13 indicated that despite a high prevalence of clinically significant anxiety and depression reported by individuals with age-related eye diseases, up to 91% are not receiving treatment for these mental health issues (see also17–19). In this same study, findings were mixed regarding the prevalence, rates, and origins of mental health issues, suggesting that improved assessment of the mechanisms that contribute to the onset and maintenance of mental health issues among people with BVI is a better predictor.13 Despite these results, Demmin and Silverstein13 acknowledged the tendency for vision loss to be most commonly conceptualized as a medical problem, reducing the condition of visual impairment to lacking psychological recognition; this is a common conclusion of many disability scholars (eg,20–23). To better understand the current state of mental health utility in the lives of people with BVI, an examination of disability as a social-political category and narrative must first occur. The following section consolidates what is known regarding the prevalence and predictors of mental health issues for people with BVI, separated by context, disability, and definition. Past and current trends related to mental health issues for people with BVI are also discussed.
History and Background
Disability Attachment: Past and Current Trends
The primary efforts of rehabilitation following the aftermath of World War I was concerned with integrating people with disabilities (PwD) into ordinary life and work.22,24 Despite this moral obligation to occupy discourse surrounding rights for PwD, institutional welfare arrangements were born, shifting from notions of rights to privilege.22,24 The evolution of rehabilitation as a medical and paramedical expertise, finding root in the struggle for professional control over injured bodies of the First World War, piloted the formation of disability as a concern of the state.20,22,25 This new definition of health rehabilitation insinuated the general notions of replacement, substitution, and compensation, which progressively were applied to all impairments, including congenital and acquired conditions.20,25 The spread of health rehabilitation and intervention by the state has been assisted by welfare institutions, legislation, business interests, professional specializations, and medical diagnoses.22,26 Such endorsements encompassed political interests relative to the redistribution of support for PwD.22,26 Medical professionals selected by the state were burdened with dictating who is entitled to the rights of financial support and relative services.22,26 This practice of dividing the deserving from the undeserving is both a historical and current problem.
Over the years, research in this area has documented a mixed report of work-related disability27 among US adults.28 Going as far back as 1962, Oi29 reported that work-related disability had increased from 7% in 1962 to 11% in 1973, then declined to 9% in 1984. Between the years of 1981 and 1988, there was no significant trend; however, the fluctuation across time suggests the difficulty of defining and measuring the population of PwD. More recently, The United States Department of Labor30 (DOL) conducted an annual labor survey of 60,000 households, to which 31,000 adults were categorized as having data indicative of a disability.31 Results showed that from 2021 to 2022, the unemployment rate for PwD decreased from 10% to 7%, roughly, with inconsistent trends reported from prior years; however, results from this data also indicated that employed PwD was more likely to be self-employed, and when compared with those people without a disability, the rate of unemployment for PwD were twice as high.31 This review of the history and evolution of disability bears implications to the prevalence of mental health issues among people with BVI. For instance, as people with BVI interact with specific work-related legislation,32 including programs that focus on vocational rehabilitation (eg, see33), it can be suggested that reliability in work-related disability and thus security affects mental health symptomology. It is difficult to conclude that the definition of health rehabilitation pertaining to disability and its associated measures are reliable amidst the fluctuating estimations of work-related disability.
Definitions and Interactions with Mental Health
Thomas Szazs,34 a Hungarian American scholar and psychiatrist, was the first to propose the dilemma of mental health being interspersed with medical conditions. With the publication of his first book, The Myth of Mental Illness: Foundations of a Theory of Personal Conduct, Szasz34 called for the amelioration of medicine from mental health study, critically exposing the interplay between categorizing matters of the mind as medical diagnoses and social-political power. Szasz34 believed the role of medication should not be privileged intervention over the complexity of normal human life. Rather, his theory of personal conduct suggested people only behave according to the effects of their social and relational lives, attributing individual circumstances of life predictive of personal conduct.34 Thus, for Szasz,34 “mental illness” as a disease, is a myth as it pertains to matters of thought and cognition, not the physical body. Szasz34 defined illnesses with respect to deviation from a norm, and in the case of physical illness, the norm refers to the structural or functional integrity of the body or some aspect of it. Illnesses, then, can be characterized as physical diseases, such as Lyme disease or rheumatoid arthritis. His definition excluded mental illnesses as diseases because they lacked relevancy to the physicalist framework of traditional medicine.34
Szasz’s34 theory of mental illness contains components that have since been accepted, rejected, and combined to elucidate working definitions of mental illness by many other theorists and scholars akin to the social and behavioral sciences. Like Szasz,34 mental illness is a myth that inappropriately pathologizes “problems of living” such as relational distress, poor financial situations, and job-related stress,35 which can be improperly applied to behavioral and intellectual disabilities.36 Alternatively, and more recently, mental illness is a disease with both medical and social causes such as genetic vulnerability, peer influence, and level of social skills37,38 that should not be distinguished from medicine, yet included to consider a more nuanced view of disease. Unlike the traditional physicalist framework (eg,39), the latter definition provides a more holistic perspective of mental illness, which helped to expand both the definition and concept of disability through an anti-reductionist lens, impacted social institutional reform,35,36,40 and the assessment of mental illness in the United States.
Despite the definition of mental illness taking many forms across decades, the origins of its interest lie within the medical model of disability, to which the social model of disability countered. The social model of disability, a concept that
breaks the causal link between impairment and disability…the reality of impairment is not denied but is not the cause of disabled people’s economic and social disadvantage
is valued in most social and behavioral professions over the medical model, which is a more prominent value in mainstream US health care, particularly rehabilitation.41 The social model points to how, and to what extent, society restricts opportunities resulting in dependency.42 The emergence of the social model of disability and the renewed perspective of mental illness helped to orchestrate global social reform by introducing frameworks and strategies that include multifactorial approaches to disability (eg,43–45). The WHO46 was the harbinger behind this effort, responding with a tool and framework that has since been utilized by researchers to improve understanding of disability and propose welltargeted solutions. The International Classification of Functioning, Disability, and Health (ICF)46 is a non-traditional health indicator that measures the livelihood of PwD in consideration of relationships between health conditions and environments, including mental health functioning. The ICF46 framework positions itself multidimensionally to determine health-related inequities for PwD. As such, it holds value for medical practice, law, and social policy to improve the overall treatment of PwD.46
Community-Based Rehabilitation and the World Health Organization’s (WHO) Definition of Mental Illness
Community-based rehabilitation (CBR) matrix47 is a framework that was developed and supported by the WHO47 to input a comprehensive lens to health rehabilitation for PwD; the ICF is the tool, while the CBR matrix is the framework. The ICF46 has been shown to provide construct validity across various medical conditions, such as osteoarthritis,48 lymphedema,49 and even serious mental illnesses.50 Relating specifically to people with BVI, a single study51 was found that assessed the content validity of the ICF.46 In this same study, results reported that it had high content validity, as part of a quantitative, cross-sectional survey; however, this study occurred in Brazil. To date, there are no research studies that were conducted in the United States relative to the validity of the ICF46 for people with BVI. The aggregation of disability bears implications to the maintenance of mental health issues among people with BVI.
Throughout this review, the definition of mental illness utilized by the WHO is adopted:
A mental disorder is characterized by a clinically significant disturbance in an individual’s cognition, emotional regulation, or behavior. It is usually associated with distress or impairment in important areas of functioning. There are many different types of mental disorders.52
It is important to note, while there exist many definitions of “mental illness”, the WHO’s52 definition is one of the few that is inclusive of broader conditions to which mental illness may be affixed. For instance, according to the WHO,52 psychosocial disability and mental states associated with significant distress, impairment in functioning, or risk of self-harm are inclusive of mental illness.52 Given that most research surrounding mental illness and BVI varies in professional and organizational interpretation (eg,13,53), this definition is best suited for this review. During this review, the term mental health is utilized to refer to subject matter that encompasses the WHO’s52 definition of mental illness, or otherwise, mental disorder. To increase understanding of how disability eclipses mental health issues for people with BVI, it must also be appropriately framed within the contexts to which it is most often addressed.
The Role of Vocational Rehabilitation (VR), Orientation and Mobility (O&M), and Care Practitioners
The state-federal vocational rehabilitation (VR) system serves PwD preparing for and securing employment, as well as attempting to retain their jobs or advance in their careers.32 It is one of the most integral statues in the United States and supports vocational development and competition for PwD (for a review, see54), operating in partnership with the DOL,30 Department of Education (DOE),55 and Health and Human Services (HHS).56 Formally established in 1920, the VR system evolved with the changing needs of people injured following the aftermath of World War I and beyond. The Rehabilitation Act of 197357 was the most influential piece of legislation for PwD, as it provided a legal basis for opposing discrimination due to disability, including work-related discrimination. Calls for equality within disability helped to pass the Americans with Disabilities Act of 1990, which defines disability as
a person who has a physical or mental impairment that substantially limits one or more major life activity.58
Today, the WIOA,32 initially passed in 2014, is designed to provide work-related services to eligible PwD with the goal of job security and retention.
Despite the importance of facilitating work-related services for PwD, some research has questioned the credibility and effectiveness of the VR program. One study seeking to assess the construct validity of VR-related services specific to mental health found variations in return across client characteristics,59 suggesting that clients with specific mental health-related needs have negative long-run rates of work-related returns. Specific to people with BVI, a more recent study asserted that people with BVI have unique stressors that are lacking critical examination, thereby impacting work-related security and retention.60 Numerous research argues similarly (eg,61–63). Considering the history of social-political interests pertaining to disability, VR efforts appear to prioritize reintegration and economic sustainability, and thus may not necessarily consider the emergence of mental illness as cause for concern indiscriminately. According to data from the Annual Disability Statistics Compendium,64 sourced by the DOL,30 DOE,55 and the HHS,56 the VR system served 4013 people with BVI in 2016, with 1431 of those cases closed without employment (see also65). Due to changes in the reporting and data collection of state VR agencies, such data is not readily available, with the most recent data provided to the public in 2016.64 It is suggested that people with BVI are underserved as prospects for mental health services under the VR system.
Orientation and mobility (O&M) training is provided to people with BVI to assist with maintaining travel competency and independence.66 It teaches people with BVI new orientation and mobility skills to compensate for reduced visual information66 and is a typical provision by state VR agencies. O&M specialists are professionals (eg,67) with training and certification (eg,68) who provide rehabilitation services to people with BVI across the life span.66 A recent study performed by Keay et al69 seeking to assess the cost-benefit of O&M training for people with BVI concluded that the services offer substantial benefits toward objective functioning and thus are worth the cost of providing. However, according to the National Federation of the Blind,70 only an estimated 2% to 8% of people with BVI utilize mobility tools (eg, cane, guide dog). While this percentage does not appear significant, when considering the overall benefit of O&M training, it is difficult to conclude that another variable does not exist. For instance, an older study71 questioned the lack of subjective outcome measures to assess the effects of O&M training for people with BVI, such as quality of life. It is suggested that mental health issues for people with BVI may include components of O&M.
Research on the relationships between care practitioners intimately involved in the lives of people with BVI is lacking in the current literature (eg,13). In Demmin and Silverstein’s13 recent literature review, 15 studies were identified that included experimental mental health interventions conducted with people with BVI. However, none of the treatment approaches within these studies identified mechanisms of change, such as increased hope for the future or recovery of self-esteem; such mechanisms are indicative of long-term outcomes.13 In the absence of a theoretical or conceptual frame that centers people with BVI, it is difficult to conclude that mental health issues are being appropriately targeted. Research indicating relationships with care practitioners are often interspersed in aggregate with other health professionals, such as rehabilitation psychologists and social workers. Therefore, for this reason, I adopt the term “care practitioner” to refer to all proposed professionals within the current literature with specific training in mental illness and have past or present involvement in the lives of people with BVI. To maintain a focus on the circularity of care for people with BVI, it is important to solely examine those care practitioners who are most involved in the related systematic processes (eg,72). The following section will examine the contrasting and related terms specific to mental health between the VR system and those generally utilized.
Mental Disability and Mental Illness: Implications for Mental Health Care Services
While WIOA32 federally mandates the provision of VR-related services, including mental health-related services, states have separate regulatory privileges pertaining to these services. Therefore, the definition of mental illness varies across states and agencies (eg,73). For this review, the state of Florida VR program and its agencies will be utilized to elucidate the defining terms. Although terminology in the field is not standardized, mental illness generally refers to clinically significant dysregulation of a person’s cognition, emotion, or behavior, whereas mental disability generally refers to a state or condition of mental impairment (eg,21,52). The Florida VR program utilizes the latter term to assess mental impairment and provide mental health services.74 Additionally, the term restoration services are utilized to describe the following association:
Physical and mental restoration services are provided to correct or substantially modify a physical or mental condition that is stable or slowly progressive.74
While this term can include physical as well as mental impairments, it should be noted that both psychological services and mental health services are considered part of restoration services and are often utilized interchangeably within the literature. The Florida VR program utilizes these interchangeable terms to describe the following association:
In cases where psychological treatment (including psychotherapy) has been recommended by a psychologist, psychiatrist or other physician, a counselor may authorize the psychologist to provide the treatment. In any case in which a physician is providing medical treatment and a psychologist is providing psychological treatment concurrently, both should be kept informed of any changes in the individual’s therapeutic regime, which would affect the treatment process. The local community mental health center should be considered as a comparable service for long-term psychotherapy, or when an individual no longer requires services from VR to achieve an employment outcome.74
The term “counselor” in this legal definition refers to “vocational rehabilitation counselor” and can be interpreted as a case manager for people engaged in VR-related services. The terms assessment and evaluation are also services that refer to a person’s eligibility for VR-related services and should not be interpreted as strictly relating to mental health services. The Florida VR program utilizes these terms to describe the following association:
Diagnosis of mental health disabilities shall be made by a psychiatrist and/or a licensed psychologist. Diagnosis by a professional staff with less than an M.D. or Ph.D. credential is acceptable only if such individual(s) are employed by a licensed/certified facility with M.D. or Ph.D. oversight.74
This distinction between mental disability and mental illness is critical to understand as it distinguishes two terms that allude to differences in professional treatment. As aforementioned, traditional health rehabilitation categorizes mental health conditions and/or symptoms as “mental disabilities”, thereby requiring a dominant medical lens to treat or restore, which is generally considered short-term (eg,22,75). Therefore, “mental illness” is arguably not considered a disability because it can be manipulated and improved, albeit often requiring long-term care. It is suggested that the prevalence of the medical model corresponds to the determination of mental health services within the Florida VR program. It is important to note that despite the variability of services across states, many of the VR-related services are similar in nature (eg, concept and definition) and should be interpreted with such similarity for the purpose of this review (for a review of federal similarity, see76).
The major purpose of the present discussion was to examine what is known about the prevalence and predictors of mental health issues for people with BVI, separated by context, disability, and definition. While most of the research discussed identified connections within VR, O&M, and care practitioner relationships relative to the conceptualization of mental health issues for people with BVI, there is a dearth of research about how all these services systematically influence the provision of mental health services for people with BVI. Therefore, the aim of this review is two-fold. First, utilizing a critical systems framework, I provide a comprehensive analysis among the interconnected systems to identify human activity and interdependencies affecting processes of mental health utility within the lives of people with BVI. Second, I identify the variables that exist across the care systems that offer the most influence on the provision of mental health for people with BVI.
Fixsen et al’s72 research on relational dynamics within organizations suggests that systems thinking (eg,77) must include a critical element, inclusive of the emergence and interrelatedness of social influences, both intra and extra organizationally. This review seeks to utilize a critical systems theoretical framework72 to identify and analyze such influences on the nature of mental health utility and provision for people with BVI. Slusser et al78 and Stringfellow79 maintain that the dynamics of a system unveils the unique character of interactivity that translates to output.80 The analysis of system dynamics, then, can provide a deep understanding of the social and biological influences that accumulate systematic activity.79 The outcome of this critical literature review will assist people with BVI and relevant stakeholders in better understanding how these systems of care influence and reinforce each other in the presence of mental health issues. All literature will originate from research conducted within the United States.
Methodology
A literature search was conducted utilizing the databases Complementary Index, Academic Search Ultimate, CINAHL Complete, SocINDEX with Full Text, Business Source Premier, MEDLINE, APA PsycInfo, APA PsycArticles, Social Sciences Citation Index, and ERIC. Searches included a combination of the following keywords: “blindness” “visual impairment” “low vision” “mental health” “orientation and mobility” “vocational rehabilitation” and “mental health practitioners.” Literature was further identified utilizing the subject identifiers “depression” “anxiety” “psychology” “quality of life” “social support” “rehabilitation” “psychosocial stress” “social stigma” “disability” and “mental health treatment.” Studies that combined data from adults with BVI and children with BVI in analyses were excluded from this review. Studies that focused on the medical consequences of blindness or visual impairment negate of a critical lens or those studies that focused on employment mechanisms solely were also excluded. For the purposes of this review, the term “blindness” and “visual impairment” correspond to objective visual acuities of 20/70 to 20/200 or worse, with the latter acuity indicative of legal blindness (for a review of the current classification system, see81). Data retrieved and analyzed from studies in this review utilize either the current classification system ratified by the WHO81 or the code of federal regulations82 when establishing blindness or visual impairment and corresponding objective assessment.
This review primarily focuses on people with BVI in the United States; however, data from people with BVI from other countries are also presented throughout the article for comparison purposes. Twenty-four studies were identified as meeting criteria. All 24 studies had been published since 2010, and thus were further excluded based on date of publishing; however, two studies that were first published in 2011 were included due to their seminal distinctions (eg,11,83). The additional exclusion was to improve the credibility of included sources. As such, sources, records, and reports published prior to 2013 were excluded from this review. Seventeen out of the 24 studies were examined and included in the final review based on the above criteria. Table 1 shows the representation of the selected studies in a summary format, with Table 2 showing the excluded studies and rationale.
 |
Table 1 Studies Examining Interfacing Components of VR, O&M, and/or Care Practitioners and the Presence of Mental Health Issues Among People with BVI in the United States |
 |
Table 2 Excluded Studies |
Types of Mental Health Issues and Interventions
Although only one study13 was very specific about the nature of mental illness and diagnoses were stated (eg, major depressive disorder, generalized anxiety disorder), a moderate number of research stated that the participants had a high risk of developing a mental illness (eg,92,93,100). Still, most stated that the participants’ prevalence rates were high relative to subclinical depression, anxiety, and affective disorders, attributing psychological factors such as distress,13,92 identity conflict,13,93 low life-satisfaction,11,13,83,89–92 vision-specific stress,11,13 low self-worth,93 and negative social support.11,13,83,88 Accountability relative to the predictors of mental health issues largely focused on VR and employer characteristics (eg,60,87), with a fair number of research that focused on disability and professional development (eg,84,85). Recent therapeutic interventions were specifically described in a single study13 with targeted therapeutic recommendations provided in different research (eg,84). Although few research included O&M implications in their conclusionary findings (eg,91), there was no recent research that examined O&M comprehensively as a training resource.
Types of Qualitative Methodologies
One study employed a modified type of grounded theory, and two studies used a form of content analysis. Anderson et al84 combined both inductive and deductive approaches to their grounded theoretical methodology to encourage the theoretical constructs of VR personnel involved in their study. It is important to note that although Anderson et al’s84 study integrated community-based research approaches, people with BVI were not explicitly mentioned as part of the participant pool in this study. Therefore, it is difficult to conclude that the relative findings can be generalized to this population; findings should be interpreted within the broader context of VR solely and with caution. Bourgeois et al85 deployed a survey to which 83 rehabilitation counselors were asked to describe both rates and sources of moral distress, taking a conceptual approach to understanding patterns and the prevalence of ethical dilemmas involving people with disabilities engaged in health rehabilitation and/or VR-related services. Like Anderson et al’s84 study, people with BVI are not explicitly mentioned as a constituent demographic in Bourgeois et al’s85 study, and as such findings should be interpreted with caution. Crudden and Steverson60 described their methodology as an iterative process, whereby data collected through semi-structured interviews with people with BVI was repeatedly reviewed, recorded, and summarized. The purpose of Crudden and Steverson’s60 study was to better understand the experiences of people with BVI who had prior engagement with VR. It is important to note that Crudden and Steverson’s60 study was the sole study in which participants were explicitly identified as having blindness or visual impairment, and a qualitative methodological approach was utilized.
Types of Quantitative Methodologies
One study employed a quasi-experimental method, and nine studies pursued a correlational predictive method. Two studies examined data using only descriptive methods. Guerette and Smedema83 used a combination of bivariate and hierarchical regression analysis to explore the relationship between perceived social support and well-being in adults with BVI. Brennan et al11 deployed a longitudinal design to examine cause and effect relationships across time for people with a specific age-related eye disease. Giesen and Hierholzer86 described their methodology as multilevel, and purposed to evaluate service patterns and the impact of VR on employment outcomes for people with BVI receiving social security benefits. Concentrated in the service structure of VR for people with BVI and an identified mental illness, Dean et al59 formulated a multivariate model to capture service provision choices and corresponding service receipts. Clapp et al87 added to the literature by providing a descriptive analysis of a longitudinal data set consisting of cross-state variations of VR-related services and labor market outcomes for people with BVI. McDonnall and Lund’s88 study tested the theory of planned behavior (TPB, see101) relative to employer attitudes toward people with BVI using confirmatory factor analysis (CFA). Zapata’s89 earliest study used multiple logistic regression to analyze cross-sectional data to examine correlations between general self-efficacy and employment in people with a specific age-related eye disease. In the next study,90 stepwise logistic regression was used to explore the correlation between PDI and employment status to advance psychosocial correlates of employment for people with BVI. The following year,91 multiple linear regression was used to examine the association between impairment-related factors and personal disability identity (PDI) and group disability identity (GDI). Zapata’s92 most recent work utilized hierarchical linear regression to analyze the association GDI attitudes and mental health indicators. In the same year, Zapata and Pearlstein93 conceptualized PDI with disability identity theoretical constructs, utilizing hierarchical regression analysis to analyze the association between PDI and disability-related factors. McDonnall et al94 utilized hierarchical linear modeling to investigate job quality as well as predictors of job quality for people with BVI engaged in VR. Two literature reviews were conducted; one focused on current mental health treatment and outcomes for people with BVI (see13), and the other, a systematic literature review, focused on factors related to employment in people with BVI and who are engaged in VR-related services (see95).
Results
Theme 1: Education and Intervention: The Impact of Educating Across Long-Term Expectations
Two studies in this review identified the importance of health-related education that is inclusive of long-term mental health outcomes and strategic therapeutic interventions that involve the complex lives of people with BVI. In a quasi-experimental study with a longitudinal design, participants with age-related macular degeneration (AMD) were interviewed for objective and subjective severity of visual impairment between the years of 1998 and 2004,11 with an assessment of corresponding levels of social support (eg, instrumental, and affective) across time. Out of the participants included in the analysis sample (n = 242), results indicated that 40% had daily contact with their children and more than half saw their children at least once a week. Ninety-one percent of participants reported having other relatives (eg, siblings and grandchildren) with stable weekly contact at 36%. In this same study,11 a repeated-measures multivariate analysis of variance (MANOVA) found no significant change in the level of family instrumental (ranging from an average of 15.6 at the baseline to 16.0 at Time 4) nor family affective support (ranging from an average of 7.8 at the baseline to 7.2 at Time 4).
A literature review by Demmin and Silverstein13 indicated several experimental studies that were effective at reducing psychological distress and improving self-efficacy and functioning in people with AMD. In introducing self-management interventions (eg, managing disease progression and related psychological issues), people with AMD were found to sustain effective results for up to 12 weeks, 6 months in some studies. However, the replication of self-management interventions across less specific eye-related diseases has not been done. It was suggested13 that the families of prospective clients (ie, patients) require education specific to the development of eye-related diseases to facilitate support across time, including self-supportive strategies to manage future mental health issues. Perhaps the most notable finding within Brennan et al’s11 study was that there was no significant main effect for objective visual impairment, but there was a significant main effect for subjective visual impairment overall (p < 0.001) at each time of measurement and for the objective and subjective interaction overall (p = 0.009). That is, the greater severity of subjective visual impairment equated to greater levels of instrumental support from families; however, those with poorer visual acuities (eg, 20/70 to 20/199) equated to no change in levels of assistance. Brennan et al11 suggested that the use of social support resources may be more motivated by an older person’s self-perceptions of the need for help than by objective criteria of visual function (eg, acuity). Demmin and Silverstein13 note this same discrepancy, reporting that some studies seeking an association between objective evaluations of visual function and depressive symptoms were unable to correlate such scores. Rather, higher levels of depressive symptoms were found when assessing vision-specific distress (ie, emotional reactions to vision loss) or vision-related tasks (eg, navigation). Demmin and Silverstein13 explicitly reported the sizable amount of qualitative data indicating the rate to which people with BVI develop negative self-perceptions due to societal stigma and experience feelings of loss, like bereavement. Demmin and Silverstein concluded that
even the perceived loss of vision may generate significant distress and result in mental health problems.13
The study by Brennan et al11 suggested that VR counselors and care practitioners exploit the stability of family and friend social support in the planning of rehabilitative needs; however, the authors emphasized the connections between self-perception and levels of distress by way of family and friends, encouraging these issues be addressed through education. While Demmin and Silverstein13 did not speak to the sequencing of self-perceptions by way of family and friends, it was suggested that education and including families is an important step to better address the long-term impact of mental health issues in the lives of people with BVI. Although the study by Brennan et al11 is considerably older, it is the only study that utilized a longitudinal design to measure how the severity of objective and subjective visual impairment affects levels of social support with a large population size (N = 384). It is also the first study to identify the discrepancy between objective and subjective visual impairment and its implications for mental health outcomes. To date, no studies have longitudinally assessed levels of social support in correspondence to objective and subjective evaluations of visual impairment in the United States. Still, the study conducted by Brennan et al11 did not operate using randomized clinical trials (RCT), making it difficult to conclude generalizability to its effects.
Theme 2: Employer Attitudes and Social Support: Differential Outcomes Between the Quality and Level of Social Support
The study of social support and its influence on the lives of people with BVI was expanded in two other studies. A quantitative study by Guerette and Smedema83 explored the relationship between perceived social support and well-being in adults with BVI; however, the use of multiple indicators of well-being in adults with BVI (N = 199) was investigated (eg, physical well-being, psychological well-being, financial well-being, family and social well-being, and medical well-being), in which the entire population size was sampled. The participants in this study reported visual acuities from 20/80 to total blindness. Results of the regression analysis performed with the five subscales (Sense of Well-Being Inventory [SWBI], see102) were all significant (p < 0.001) for physical, psychological, economic, and family and social well-being. With respect to psychological well-being, F(6, 192) = 7.14, p < 0.001, age was significantly positively associated with psychological well-being (β = 0.16, t(198) = 2.26, p < 0.05), and social support was significantly positively associated with psychological well-being (β = 0.38, t(198) = 5.62, p < 0.001), controlling for demographic and disability characteristics. These results are contradictory to findings found in Brennan et al’s11 study, which indicated that older adults who reported more levels of social support had higher negative perceptions of their visual impairment and thus more susceptible to distress. However, like Brennan et al,11 Guerette and Smedema83 emphasized the negative influence of “overprotection” upon people with BVI stemming from a lack of education and impacting self-perceptions.
Most notably, no significant correlations were found in the sense of medical well-being, F(8, 192) = 0.2.85, p < 0.05, in Guerette and Smedema’s83 study (p = 0.019). It was suggested that the degree of severity or the age of onset of a disability may not affect the well-being of people with BVI. Unlike Brennan et al’s11 quasi-experimental study with similar variables, the control of confounding variables such as demographic characteristics (eg, age and employment) and more flexibility with measuring disability (eg, age of onset of disability and subjective feelings on disability) were unmeasured. Thus, the SWBI is a reasonably valid substitute for measuring subjective visual impairment. Despite the age of this study, Guerette and Smedema’s83 work was the first in the field of BVI to incorporate a subjective instrument (SWBI) that was specifically designed for people with disabilities. Additionally, this study was a partial replication of another study conducted by Cimarolli and Boerner,103 to which perceived quality of social support was not measured. Rather, Cimarolli and Boerner103 measured perceived levels of social support on a continuum; Guerette and Smedema’s83 study is considered seminal.
The other study took a different approach to analyzing social support, incorporating the workplace context. In a quantitative study focused on the explanatory utility of the theory of planned behavior (TPB, see101), McDonnall and Lund88 deployed an online survey to hiring managers (n = 388) to examine the construct validity of a TPB structural model (N = 25,843). The aim of the study was to uncover employers’ hiring intentions of people with BVI. Originally grounded in psychology, TPB101 posits that behaviors are influenced by intentions, which are determined by three factors: attitudes, subjective norms, and perceived behavioral control. It is also possible for external factors to directly coerce or intercept behaviors,101 regardless of the intention, depending on the extent to which a behavior is controlled by the individual, and the extent to which perceived behavioral control is a valid measure of actual behavioral control (see also104,105).
Research in this area aims to uncover these hidden values and ideas that influence decision-making using meta-analyses. An extensive body of literature has supported the utility of the TPB model of behavior intention (for a review, see106). However, this is the first study88 that has applied and tested the TPB in relation to employer hiring intentions regarding PwD, specifically, people with BVI. Developing four unique constructs (eg, subjective norms, perceived behavioral control, attitudes-productive, attitudes-challenges, and intent to hire), the researchers reached a significant correlation among them (r = 0.35-0.75). A confirmatory factor analysis (CFA) was conducted to ensure factorial structure of the TPB-related items, improving model fit (r = 0.37-0.90). Results indicated that paths between intent to hire and subjective norms (β = 0.32), perceived behavioral control (β = 0.19), and attitudes-productivity (β = 0.39) were all significant (p < 0.001). However, the path between attitudes-challenges and intent to hire (β = 0.07, p = 0.31) was the only insignificant path. Cronbach’s alpha was lower for total scores in this domain of items (r = 0.39-0.66). McDonnall and Lund88 suggested that the insignificance of this factor may relate to ambiguity, as some aspects of subjective norms and perceived behavioral control may have accounted for the variance, resulting in participants not answering correctly and conflating the items. Both Guerette and Smedema78 and Brennan et al11 found that the discrepancy between subjective and objective evaluation of visual impairment can impact mental health, social support resources, and the use of rehabilitation services. Guerette and Smedema83 explicitly mention that while objective measures of quality of life are most often utilized for PwD, it typically includes criteria such as employment status, marital status, and physical and material indicators, which have been found to be deficit of the disability community (eg, see22,50), thereby resulting in lower levels of quality of life. Given these findings, it is difficult to conclude that the items from the attitudes-challenges domain in McDonnall and Lund’s88 study can be answered indiscriminately to these perspectives. McDonnall and Lund elucidated,
although prejudice toward people who are blind in general is typically not seen as socially permissible, negative attitudes toward potential employees or job applicants who are blind may be more common and viewed as more permissible.88
A similar perspective is illustrated in Demmin and Silverstein’s13 recent literature review of therapeutic interventions, to which they found that many of the current interventions for people with BVI are focused almost exclusively on improving functionality through skills training and less on vision-specific distress. This study’s structural model of TPB accounted for over 61% of variance in intent to hire people with BVI. The strongest predictors of intent to hire were attitudes toward productivity (β = 0.39) followed by attitudes toward subjective norms (β = 0.32). McDonnall and Lund88 suggested that VR counselors and care practitioners focus efforts on educating employers about how people with BVI can effectively manage their jobs as well as assess the subjective norms of the prospective employers.
Theme 3: Identity: The Relationship Between Disability and the Self-Concept of Blindness
Five studies emphasized the role of disability identity on mental health in people with BVI. All five studies were conducted by the same researcher, although one was co-authored. The first study89 in chronological sequence was intended to explore the associations between general self-efficacy (GSE) and employment status in working-age adults with retinitis pigmentosa (RP). Demmin and Silverstein’s13 most recent literature review found several therapeutic interventions that measured self-efficacy as an outcome; however, as noted previously, these experiments lacked orientation to the mechanisms to which such change occurred, affecting longevity of treatment outcomes. In comparison, Zapata’s89 earliest study concerning disability identity intended to correlate GSE to employment status in people with BVI, specifically people with RP; in other words, employment was examined as a mechanism by which GSE may be manipulated. In a large sample size of (n = 183) participants, multiple logistic regression was conducted to analyze cross-sectional data. Findings indicated that individuals with RP who have a bachelor’s degree or higher had significantly higher odds of being employed (p < 0.01), at 158% higher likelihood, and that individuals with RP who use a cane or guide dog had significantly lower odds of being employed (p < 0.01). Most notably, participants who used a cane or guide dog had an estimated 64% lower odds of having full- or part-time employment, compared to participants who did not use a cane or guide dog, after accounting for the other variables in the model.
These findings lend to findings from a later study by Zapata,91 to which results indicated that the use of a mobility tool (eg, cane, guide dog) reported higher disability affirmation (eg, personal disability identity [PDI]) in participants (p = 0.001), with younger participants displaying higher reports of connectedness with the disability community (eg, group disability identity [GDI], p = 0.001). However, in this same study, disability acceptance, an item such as “I regret that I am a person with a disability”, was not significantly associated with any of the variables, such as age, gender, or impairment-related factors, accounting for only 12% of variance. Clinical application was suggested by Zapata91 relative to O&M to address the social issues inhibiting mobility tool use. Earlier critiques by Virgili and Rubin71 stated the same, recommending O&M providers apply a subjective measure of quality of life in the assessment of mobility for people with BVI. Assertiveness training and disability-affirmative case conceptualization was suggested by Zapata;91 however, Demmin and Silverstein’s13 recent literature review indicated that no such intervention exists.
Retreating to the earliest study, Zapata89 controlled for factors previously linked to employment outcomes for people with BVI (eg, age, gender, education level, mobility tool use, ability to drive, and age at diagnosis), to which age, gender, and age at RP diagnosis were not found to be associated with employment status. GSE was measured on a 10-item unidimensional scale. For every 1-point increase in GSE, participants had 8% higher odds of having full or part-time employment, with the odds ration approaching statistical significance (z = 1.82, p = 0.07). Using Bandura’s107 theory of self-efficacy, Zapata89 suggested that employment and psychological well-being were connected, with self-perception in ability connected with self-efficacy levels, an item such as “I can usually handle whatever comes my way”.
The suggestion that self-perceptions are an alterable cognitive construct and may be the target of interventions to increase employment outcomes for adults with RP or other eye conditions is supported by Brennan et al,11 who found that the greater severity of subjective visual impairment equated to greater levels of instrumental support from families, thereby affecting self-perception. Zapata89 suggested that self-efficacy expectations are influenced by social persuasion, such as someone else suggesting that another can cope successfully in a specific, formerly stressful situation (see also107). Self-efficacy was an outcome target in many of the experimental studies reviewed by Demmin and Silverstein,13 and rates of self-efficacy did improve; however, employment was not linked as a mechanism to which change occurred. Considering what was found by Zapata89 on associations of self-efficacy and employment, it is suggested that therapeutic interventions may not be linking self-efficacy as a social construct, but in terms of functional mastery. As is elucidated by Zapata,
the effect of this information [social persuasion] on people’s self-efficacy is determined by how they cognitively appraise the information.89
Going beyond a mere reference to the concept, Zapata and Pearlstein93 incorporated recent theories from earlier studies (eg, see108,109) to assess PDI and its psychological impact on people with BVI. Using two novel attitudinal subconstructs of PDI (eg, self-worth and personal meaning and disability-related factors), with corresponding general anxiety and depression measures (Patient Health Questionnaire [PHQ-4], see110), lower disability self-worth was significantly associated with increased depression and anxiety (β = −0.40, p < 0.001). Additionally, this study controlled for demographic and disability-related factors, allowing for more variance to disability as a mechanism for change in mental health and clinical settings for people with BVI. Most notably, findings from this study indicated that the effects of self-worth (r = −0.47) were greater than personal meaning (r = −0.23) in the prevalence of anxiety and depression; in other words, it was the strongest predictor of symptoms of depression and anxiety for people with BVI in this study. Demmin and Silverstein13 also reported many other predictive–correlational studies that found associations between anxiety and depression and people with BVI; however, predictors identified in this study included vision adjustment, age at onset of vision loss, low vision acceptance, and vision-specific distress. Age and gender were also variables in Zapata and Pearlstein’s93 study, to which age (β = −0.18, p < 0.001) and gender (β = −0.15, p < 0.001) were also significantly correlated; males and older adults with BVI who have high self-worth, predicted less anxiety and depression. Given what was found in Brennan et al11 and Guerette and Smedema’s83 studies regarding the discrepancies between subjective and objective visual function, and Zapata89 and Zapata and Pearlstein’s93 studies regarding connections of self-worth and self-efficacy, it is difficult to conclude that such predictions found in Demmin and Silverstein’s13 literature review are not inclusive of these and are simply lacking appropriate measures.
A notable strength to this study93 is the use of a novel PDI instrument to measure disability self-worth and personal meaning, such that both items encompass aspects of disability from a subjective perspective rather than objectively. For instance, for disability self-worth, one item was “I have as much to offer the world as people without a disability”, and a personal meaning item was “my disability gives me perspective on what mattes in life”. Again, Guerette and Smedema83 and Brennan et al11 found that discrepancies exist between subjective and objective evaluations of visual impairment, leading to skewed results, echoing historical measurements of disability discussed earlier (eg,28,29).
The final study by Zapata92 explicitly focused on the association of lower anxiety and depression in people with BVI relative to GDI. In contrast to earlier studies,89,90 this most recent study withdrew correlations to employment specifically, although implications were indicated. Interested in furthering the concept of GDI and its association with mental health outcomes, Zapata92 utilized a cross-sectional design to examine the associations between two GDI attitudes (disability integration and disability isolation) and three mental health-related indicators (life satisfaction, anxiety, and depression) in a large sample of US adult members (n = 187) of BVI community groups. In controlling for demographic and impairment-related variables, results indicated that participants who reported a higher sense of connection to the disability community (ie, disability integration) also reported overall higher life satisfaction (β = 0.25, p = 0.001). Participants who reported higher sense of isolation from both the disabled and nondisabled community (ie, disability isolation) also reported overall lower life satisfaction (β = −0.45, p < 0.001) as well as higher anxiety (ß = 0.26, p < 0.001) and depression (ß = 0.40, p < 0.001). The negative association between depression and being employed approached significance (ß = −0.23, p = 0.004), which correlates to earlier studies regarding connections between self-efficacy89 and self-worth93 and employment. Notably, for integrators, the association between anxiety and gender approached significance (ß = −0.19, p = 0.009), and for isolators, gender (ß = −0.21; p = 0.003) were significantly associated with anxiety. Apart from any demographic or impairment factors, GDI attitudes (integration and isolation) were the only variables that reached statistical significance in predicting life satisfaction in this study. Specifically, disability isolation, but not disability integration, was a significant predictor of anxiety and depression. Zapata92 suggested that care practitioners consider supporting clients’ (ie, people with BVI) mental health and related outcomes by facilitating their exploration of disability identity attitudes including feelings of connection to the disability community.
Theme 4: VR Classification and Service Patterns: The Concept of Risk
Five studies quantitatively explored the factors that predict employment outcomes for people with BVI, including the assessment of VR service patterns and classification. The earliest study to investigate was a multilevel analysis by Giesen and Hierholzer,86 who explored VR service patterns and evaluated the potential employment outcomes for people with BVI using FY 2011 rehabilitation services administration (RSA-911) data on consumers (N = 3610) who also received social security disability income (SSDI). Results indicated that services are delivered in clusters, such that the higher correlations of services within clusters inform services within factors that tend to be received together. Regarding evaluation services (ie, factor), which are inclusive of mental health services, only two of the four services in this factor group were related to employment outcomes: VR counseling and guidance and assessment.86 Results from this study indicated that people receiving VR counseling and guidance have 32% higher odds of competitive employment, whereas assessment services indicated 34% lower odds of competitive employment. Information and referral services and technical assistance services were not significantly related to outcome.
Dean et al’s59 study examined the types of services provided to people with BVI who have an identified mental illness. Results showed that when combining the employment and earnings effects together, apart from diagnosis and evaluation, all service types had positive long-run effects. Similarly, Clapp et al’s87 analysis of VR-related services indicated persistent earnings benefits; however, there was substantial cross-state heterogeneity relative to types of services offered. Further, in their cost-return analysis, results indicated that diagnosis and evaluation had a mean service cost of $408 per client and restoration at $2,576; in order of magnitude, both were less expensive than all the other services. In any case, it was suggested that such services are considered a “risk” to employment outcomes.86
Similarly, Lund and Cmar’s95 recent systematic literature review postulated the potential “risk” for VR consumers with BVI to have unsuccessful closures due to poorly targeted supports and interventions, particularly those receiving SSDI. McDonnall et al94 also postulated this same risk, stating that people with BVI who are also receiving SSDI may be at risk for poorer employment quality. Still, this study86 found that there exists a holistic, multilevel assessment process that operates systematically depending on service needs. However, these needs are considered a “risk” if not associated with employment outcomes. Despite its age, this is the first study that offered a systematic lens to VR services for people with BVI. Giesen and Hierholzer stated,
the negative link between receipt of assessment services and competitive employment may involve a more complicated situation in which the needs of the individuals are not readily apparent.86
The necessity of long-term studies for improved treatment outcomes was echoed in Demmin and Silverstein’s13 literature review, and clinically emphasized by the findings in Zapata’s89,90 studies relative to the role of psychosocial factors in employment outcomes.
While some studies in this theme did utilize RSA-911 data to explore characteristics of VR,86,94 many studies highlighted its limitations.59,86,87,95 In McDonnall et al’s86 study, results indicated that job quality indicators were higher for consumers who were employed at application than for those not employed at application. Most notably, in terms of VR-related services, receipt of a certificate, receipt of an associate degree, and receipt of bachelor’s or higher degree were positively associated with job quality at VR case closure; however, receipt of job readiness training and on-The-job supports–supported employment were negatively associated with job quality. Lund and Cmar’s95 systematic literature review highlighted this same weakness in RSA-911 data, finding it limiting to what is contained within the data set (eg, demographic vs consumer rating of services). Based on findings from Giesen and Hierholzer’s86 study on the systematic patterns of VR services and their connections to employment outcomes, it is suggested that employment outcomes are multidimensional; therefore, it is difficult to conclude that job quality outcomes are indicative of objective evaluations solely. Dean et al59 and Clapp et al87 were the sole researchers who did not utilize RSA-911 data for their studies. Clapp et al87 asserted that while employment earnings were constant across states, the varied services are misleading accounts to VR long-term effectiveness for people with BVI. All studies in this theme operated under the most current legislation of WIOA,32 which emphasizes job retention, not simply job attainment, adding to the strengths of all findings.
Theme 5: VR Counselor Relationships and Community Involvement: The Role of Persistence, Morality, and Social Aggravators Amidst Employment Challenges
Two studies sought to explore the impact of VR-related services from a qualitative perspective, and one used a mixed-methods approach. The aim of all the studies in this theme was to examine the personal experiences of people with BVI, VR counselors, and the impact of their communities and organizations. Crudden and Steverson60 conducted semi-structured interviews with people with BVI who had a history of navigating the VR system (n = 11) to better understand how jobs are retained. Results were organized under two broad areas: generalizable skills and issues associated with retention. Generalizable skills included technology, networking, and persistence. Issues associated with job retention included VR support, personal factors, and workplace efficiency. These results correspond with McDonnall & Lund’s88 study which found that employer’s strongest predictor of intent to hire was attitudes toward the productivity of people with BVI. Participants described the psychosocial stressors (eg, anxiety) associated with job retention; however, reported benefiting from persistence and support networks. Notably, the theme of “persistence” emerged as both a generalizable skill and an issue associated with retention. Specifically, six participants reported persistence as a skill that assisted them in being successful in their jobs, and three mentioned persistence was a personal factor that assisted them in retaining their jobs.60 Regarding VR-related services specifically, five participants expressed concerns with the timeliness of VR-related services and three stated that VR-related services are not equipped to provide long-term support. This finding contradicts findings from Lund and Cmar’s95 most recent systematic literature review which indicated that job-related services were the stronger predictor of employment. Job-related services can be defined as services that prepare people with BVI to obtain and retain positions. In McDonnall et al’s86 study job-related services were not correlated with job quality, or had a small, negative correlation. These findings are consistent with other studies in which a negative relationship between job-related services and job quality was found.111–113 McDonnall et al asserted,
consumers who require assistance from VR with preparing for or locating employment, rather than being able to prepare for and find it on their own, are more likely to obtain lower quality jobs.86
Crudden and Steverson’s60 study utilized an iterative approach to data analysis, improving the overall credibility of the data. However, the sample size was incredibly small, affecting generalizability of the data.
Work-related stressors were also experienced by VR counselors. A recent mixed-method study explored the concept of moral distress from the perspective of VR counselors. Using a randomized sampling method of (N = 1000) VR counselors, Bourgeois et al85 explored the prevalence and impact of moral distress within the context of professional work. Moral distress can be defined as
when one knows the right thing to do but institutional constraints make it nearly impossible to pursue the right course of action.114
It is important to note that in this specific study, Bourgeois et al85 distinguishes between moral distress and ethical dilemma, in that the latter constitutes difficulty in decision-making whereas the former’s effects are relative to external constraints to a decision. For participants who completed the survey (n = 83), results indicated that the average rating of moral distress was 4.32 (uncomfortable) out of 10, with 43% reporting a distress rating of 5 (uncomfortable/distressing) or higher. A notable finding within this study85 was the theme of “compromised service delivery”, which emerged as a common source of moral distress for VR counselors. Specifically, it was found that there was an inability to provide optimal services to clients due to the following: large caseloads, time constraints, lack of qualified counselors, a shared finding from Demmin and Silverstein’s13 literature review, and lack of training and focus on outcomes and cost control. One participant (#29), as cited in Bourgeois et al stated,
I am concerned that my clients are not getting the good quality care that they need to recover from mental health or substance abuse problems.85
Cost control was also a theme in Clapp et al’s87 analysis to which they found that diagnosis and evaluation services were among the lowest in terms of mean service cost, while restoration services were much higher; nonetheless, both services were indicated to have the lowest probability of service receipt. Lund and Cmar’s95 systematic literature review spoke to VR focus on employment outcomes, suggesting that people with BVI who have secondary disabilities or may need additional support are at “risk” for unsuccessful closures.
The strength of Bourgeois et al’s85 study lies in their methodology, as they used a consensual qualitative research (CQR) approach, an inductive approach to describe phenomenon, adding reliability to this study’s findings. The same approach was utilized by Anderson et al,84 to which they examined the intersection of race and poverty in the engagement of VR-related services. Results indicated that trauma-sensitive and culturally responsive care are needed to meet the demands of the social-political realities of VR consumers. In Lund and Cmar’s95 systematic literature review, they found that African American race was a significant negative predictor in two (OR = 0.67–0.70) of eight analyses of competitive employment. McDonnall et al86 found that job quality was negatively associated with African American race, female gender, disability, and SSDI. Anderson et al84 suggested that VR programs identify and address ongoing racial stressors associated with depression and related mental health considerations, emphasizing that engagement in VR is impacted by these ongoing stressors. Demmin and Silverstein’s13 most recent literature review on therapeutic interventions indicated no such clinical approaches or assessments.
Discussion
Little is known about the multifactorial influence of mental health utilization in the lives of people with BVI. To address this gap, this review aimed to provide a comprehensive analysis and synthesis of current literature utilizing a critical systems framework to examine the social and biological relationships between the systems most involved in the lives of people with BVI. There are marked contrasts between VR and people with BVI on what predicts job quality and subsequent competitive employment for people with BVI, which consequently transcends into the clinical environment; most interventions fixate on improving occupational functionality through skills-training, a short-term issue when considering the multidimensional needs, identities, and experiences of people with BVI. Intersectionality is greater than the sum of any singular identity, and thus must be considered as part of solutions and affected by social problems.115
Most employers rely on the subjective norms on people with BVI and their productivity levels when considering hiring potential. Consequently, these attitudes are a factor in the emergence of mental health symptoms, such as anxiety, depression, and feelings relative to self-efficacy and wellbeing. Furthermore, it is difficult to conclude that among these challenges, people with BVI would seek independent mental health intervention, through employer benefits or otherwise, as much of the reviewed literature found service delivery congruent with objective evaluations of visual function rather than subjective evaluations. Moreover, the discrepancy identified between objective and subjective reports of visual function, such that self-perceptions of visual impairment can overrule objective criteria of visual function, only serves to widen this gap. Without appropriate theoretical and conceptual frameworks that offer choice, people with BVI may not be provided welltargeted care. The Diversity, Equity, and Inclusion (DEI) (eg,116) tenet of equity emerges here as a reminder of the importance of fulfilling opportunity through congruent approaches that are intended to mobilize the most marginalized and not simply fill a need (see also115). Other research has documented the work of interventions that offer choice and incorporate peer power for people with BVI. Koolaee et al’s99 experimental study utilized choice theory117 and a combination of group training and action strategies to investigate its impact on quality of life and hope in people with BVI (n = 30). Utilizing the Quality-of-Life Questionnaire (WHOQOL, see118) to measure multiple effects (eg, physical, psychological) of the training and therapeutic sessions, results indicated that the training of choice theory concepts affected the quality of life (F = 22.5, p < 0.001) and hope (F = 35.17, p < 0.001) of people with BVI. Considering the prior research indicating barriers to the comprehension of mental health concepts for people with BVI, it seems safe to conclude that the training of choice theory concepts may improve the quality of life and hope for people with BVI, thereby improving ecological validity. However, this study was conducted outside of the United States, and thus more research is needed.
In contrast to the mainstream population, the classification of disability arguably does not interfere with the conceptualization and utilization of mental health services. It is inequitable for people with BVI, and their emerging mental health needs to be conceptualized as more or less complex than the average person without a disability. Concerning VR, the long-standing impact of disability attachment and its social-political history may be part of the problem with how VR is managing mental health, its establishment as a condition, and related services. Clinicians, specifically, may believe that outreach concerning this population is not necessary because VR is providing appropriate services, including assessing the need for mental health services; however, this is inconclusive.
The Power of a Podcast: Building Collective Equity
A critical forum in the medium of a podcast or otherwise collaborative online discourse may aid in exposing and addressing the underutilization of mental health in the lives of people with BVI. There exist multiple strengths associated with this proposal. New digital technologies, such as podcasts, provide socially marginalized people around the world with a mechanism through which they can make their voices heard.119 Despite traditional media’s (eg, television media) social task to represent the interests of all members of society, marginalized people’s injustices and needs are often devalued, with content primarily focused on and designed for dominant or popular groups.120 Members of the privileged class have received criticism for appropriating traditional media to reinforce their interests and dismissing or misreporting perspectives that go against their interests.121
In addition to underrepresentation in traditional media outlets, marginalized groups often face exclusion from government bodies. In considering societal issues, members from the dominant culture tend to launch communication, and their recommendations have more power.122 A podcast that focuses on collaborating to fuel reparations and reenergize the concept of mental health for people with BVI does not seek expertise from centuries-old rudimentary processes; it seeks a renewed understanding and reexamined process. People with BVI have access to education pertinent to their mental health experiences and issues that are accessible (ie, they can listen and share for free). In addition, there exists no academic bias to membership to this podcast or its content; such is the case for most privileged information in scholarly journals.
Rehabilitation professionals can receive contextually relevant education without a cost; and that is informed by research, testing theory to story, and practice.123 In addition, busy professionals can listen quickly and easily without scheduling a conference or taking time off.124,125
There exist limitations to this capstone project that should also be acknowledged. In many academic circles, podcasts, despite being well researched and supported, lack credibility because they are not affiliated with an institution, lab, or research facility (eg,123). As such, there is a possibility that replication of scholarly suggestions does not occur because they lack peer-review processes. As is elucidated by Kiernan et al,
the listener must rely on their own assessment of the weight they should give to the supplied content.123
There exist four theories that have been conceived to inform the need for a critical forum or podcast: (1) critical disability theory (eg, see126), (2) choice theory (eg, see117), (3) theory of self-efficacy (eg, see107), and (4) liberation health theory/framework (eg, see127).
Critical Disability Theory
First, critical disability theory can be framed and understood by examining the earliest works by Max Horkheimer126 relative to his critique of traditional social inquiry and order. In his 1937 essay titled, “Traditional and Critical Theory”, Horkheimer126 states that critical theory is a social theory oriented toward critiquing and changing society, in contrast to traditional theory oriented only toward understanding or explaining it. Critical disability theory, then, can be defined as a methodology of inquiry that
involves scrutinizing not bodily or mental impairments but the social norms that define particular attributes as impairments, as well as the social conditions that concentrate stigmatized attributes in particular populations.23
Similar definitions have also been ascribed to the theory (eg,128,129). When considering findings from current research, there exist no utility of critical frameworks nor approaches that examine the mental health issues of people with BVI; while current research exists surrounding the mental health effects of social and impairment-related issues relative to this population (eg, see89–92), none of these findings have been replicated since first identified in 2011 (eg, see11,83), with current practice primarily focused on vision-related mental health issues (eg, see13), such as visual function (eg, acuity). A critical forum or podcast can work to intentionally critique and challenge traditional approaches to understanding the mental health issues of people with BVI with the goal of producing new methods of problem-solving, particularly within the centralized and interconnected relationships between VR, O&M, care practitioners, and people with BVI.
Choice Theory
Second, choice theory, as aforementioned within the discussion section of the literature review, was developed with a proceeding therapeutic approach targeted toward the education of clients with control-based psychological deficits.117 According to Glasser,117 choice theory explains that we are motivated by the pleasure we experience when we satisfy our five basic needs for survival (ie, love and belonging, power, freedom, fun, and survival). Thus, all behavior is an individual choice, not necessarily a product, or outcome, of someone or something else. However, when we seek external control (eg, via coercion or threats) to satisfy any one of these five needs, we experience unpleasant emotions and mental states simply since we are unable to control others, only ourselves.117 Reality therapy, the established therapeutic approach consistent with choice theory, utilizes cognitive behavioral therapy principles to aid clients in gaining new perspectives and techniques that will help them to manage challenges on their own.117 As William Glasser pragmatically explained in a published interview by Onedera and Greenwalt:
That’s the definition of mental health; it is healthy relationships and especially relationships that are so healthy that you don’t try to change people around you…you eliminate the use of what I call ‘external control psychology’ from the relationship…and so it’s a triple metaphor, mental health equals happiness equals choice theory.130
When considering the current research indicating the concentration of mental health resources for people with BVI a consequence of VR-related assessment and evaluation (eg, see86,87), the relationship between VR (ie, case managers, counselors) and people with BVI is one that requires a re-establishment of the notion of locus of control (eg, see131). Oppressive and structural systems challenge social influence thereby impacting social constructions, leading to recursive effects.22,132–135 That is, what a person can receive from society and structures may shape their activity, yet this same activity is voluntary and continues to shape and affect their social lives.131 A critical forum or podcast can provide a means of educative introspection that aids people with BVI to recognize power that is given, not necessarily power held. Reality therapy, then, can be an organized effort to incorporate into clinical settings to which people with BVI are cognizant of, and may specifically request, during assessment or evaluative procedures. Further, concepts learned through this podcast project may assist people with BVI in making sound choices related to seeking privatized mental health care, disconnected from VR entirely. When considering what was found in the research by60 related to the overall discontent with VR-related services by people with BVI (eg, timeliness, appropriateness), concepts from reality therapy may be beneficial to reducing the proclivity to “persist” in such situations, and rather “abandon” attempting to single-handedly control such a complex structural system; indeed, healthy relationships begin when individuals can notice the nature and benefit of relationships and their unique role and needs within it,117 adjusting as necessary (see also130).
Theory of Self-Efficacy
Third, the theory of self-efficacy is defined by Albert Bandura as
beliefs in one’s capabilities to organize and execute the courses of action required to produce given attainments.107
Bandura107 asserted that a person’s belief in their capabilities affects their initiation and persistence on a given task; this mention of “persistence” was noted in the current literature as both a “personal factor” and “skill” that assisted in job retention.60 When an individual believes that they can successfully perform a task that will produce a desired outcome, they will exert more effort in their performance of that task. Expectations relative to self-efficacy stores rely on a combination of four sources: performance accomplishments, vicarious experiences, physiological states, and verbal persuasion.105 When we consider the current research by Zapata89 indicating the associations between self-efficacy and employment outcomes, and how self-efficacy was primarily utilized as a “skills-based” outcome target in Demmin and Silverstein’s13 recent literature review, it can be suggested that the role of self-efficacy as a cognitive construct is effective at mitigating the emergence of mental health symptoms for people with BVI. However, based on the current research data regarding the prevalence of mental health symptomology for people with BVI (eg, see92,93,100), and long-term mental health ineffectiveness (eg, see13), self-efficacy may not be a target of mental health treatment outcomes associated with social aggravators (eg, prejudice). A critical forum or podcast may aid in the development of clinical treatment approaches, including measures, to appropriately identify sources of self-efficacy to which deficits may be targeted. Additionally, the education and collaboration intent of this podcast project may help current and prospective employers challenge the subjective norms placed on people with BVI (eg, see88) such that “performance” and “productivity” are not considered the primary “quality” measures to which people with BVI are categorized.
Liberation Health Theory
Fourth, liberation health theory, a combination of radical social work (eg, see136), liberation psychology (eg, see137), and Paulo Freire (eg, see138) and popular education, focuses on expanding “traditional case work” into actionable practices that serve to disrupt the interplay of dominant socio-political forces.127 In a participatory sense, clients become “subjects”, developing a new “consciousness” that rejects the “passive sense of self”, allowing for meaningful progress to occur in the context of their problem.127 Historical trends (eg, see20,22,25) relative to the role of disability as a classification measure have been utilized to conceptualize problems for people with BVI for decades, including the emergence of mental health issues (eg, see5,14), which in turn, impact how mental health symptoms are managed by VR, O&M, and care practitioners with mental health expertise. The category of disability arrives with predetermined outcomes that are socialized and subsequently reinforced by professionalization,139–141 eg, deficit, personal tragedy; similarly, PwD assume this identity, centering their impairment causal to their “suffering”.22,142–146 This causal sequencing affects problem-solving and perceived action efficacy for PwD, particularly as it pertains to social or economic need.140,141 Within many health organizations, the medical model is dominant, as it aligns with the pedagogical truths inherent to most health-rehabilitation professionals. The presence of the two models inhibits holistic understanding based on discipline specific training and promotes conjectures of need for PwD.139–141
When considering the historical trends denoting the dichotomous processes that occur when related professionals behave consistent with the medical or social models of disability (eg, see22,26), and current research identifying discrepancies in the objective and subjective evaluations of vision impairment (eg, visual function, visual acuity) and correlations to depressive and anxious symptoms (eg, see13), two points are suggested: (1) related professionals are choosing one of the two models of disability, without attempting to learn about the validity of the other, and (2) people with BVI are lacking subjectivity to the clinical processes that hypothesize the direction of causality regarding mental health issues. A critical forum or podcast can work to utilize liberation health theory as a framework for exposing the dominant discourse (eg, see147) and relevant training that helped shape professional knowledge, specifically the knowledge of VR, O&M professionals, and care practitioners with expertise in mental health philosophy. By leveling power as neutral and referring to guests and podcast listeners as “learners”, they can reflect critically on their experiences and foundational knowledge to enhance their understanding of roles; this work challenges prior assumptions and critiques the idealism (eg, see148) behind subconscious behavior (eg, ableism and disability diversity), evoking new consciousness.127 DEI (eg, see116) reinforces this work, asking for the transition of knowledge to evolve, embracing complex intersectionalites with the goal of disrupting dominant knowledge (see also115). Finally, by including people with BVI in such discourse (ie, talking about but not with people), we are rejecting the traditional processes in which change, and reform occur relative to ameliorating problems of marginalized populations (eg, see149).
Recommendations for Future Work
Future work relative to an educational podcast or forum should focus on the goal of disengaging the traditional milieu by which mental health as a health-related resource is conceptualized and, thus, remedied for people with BVI. The concentration of rehabilitation in the lives of people with BVI generates a culture-specific framework of professional intervention that disrupts the significance of mental health symptomology. A podcast’s educative and collaborative resources must aim to penetrate professional development whereby behavior change in this area may occur. It is through such learning that anticipates that new knowledge is integrated into current knowledge, maintaining and improving skills.
Such a goal will require restructuring the learning methodology to meet the needs of VR counselors, O&M professionals, and care practitioners through knowledge transition (KT) activities (eg, see150,151). Knowledge transition can be defined as
the exchange, synthesis, and ethically sound application of knowledge within a complex system of interactions among researchers and users.151
The development of a continuing education course (CEC) is an excellent option to improve the reliability and sustainability of podcast-based education, increasing the likelihood of penetration in rehabilitation and clinical practice.
Rather than relying on information from a combination of varied research to inform clinical decisions, health-rehabilitation professionals can receive evidence-based, multicomponent educative strategies that parallel their respective disciplines (eg, see151–153). For instance, three teaching sessions spread over a 12-week period that incorporate a combination of interactive and didactic learning activities aimed at developing strategies to gather mental health information from people with BVI, developing and implementing a plan that integrates vocational information into clinical information, analyzing and measuring the effectiveness of knowledge relative to the plan intersubjectively, thereby improving KT.151 Although evidence shows that CECs can enhance knowledge,154,155 it is less clear that traditional CECs alone are effective at manipulating professional behavior or enhancing patient outcomes (eg, see156,157). As critiqued by Schreiber et al,
a traditional CEC delivered at a single point in time employs a lecture-based format and counts hours of learning (i.e., continuing education units) rather than improved knowledge, competence, and performance.151
A CEC course that integrates knowledge transition activities can also lead to improved assessment tools. Taking into consideration the current research by Zapata,89 indicating the associations between self-efficacy and employment outcomes and how self-efficacy was primarily utilized as a “skills-based” outcome target in Demmin and Silverstein’s13 recent literature review, it can be suggested that the role of self-efficacy as a cognitive construct is effective at mitigating the emergence of mental-health symptoms for people with BVI. However, based on current research regarding the high prevalence of mental health symptomology for people with BVI (eg, see92,93,100) and current treatment interventions lacking long-term effectiveness (eg, see13), self-efficacy may not be a target of mental health treatment outcomes associated with social aggravators (eg, prejudice, employer discrimination, disability isolation). Learnings from an educative podcast or forum may aid in the development of assessment tools that appropriately identify sources of self-efficacy to which deficits may be targeted. To better demonstrate this, a novel assessment tool is proposed that utilizes the theory of self-efficacy (eg, see107) and its psychological constructs to capture multiple dimensions of self-efficacy across VR, O&M, and care practitioner contexts. Most salient, the proposed measure is informed by research pertinent to the limitations of mental health as a health-related resource for people with BVI (eg, see13,60,71,88). The title of the assessment tool is Blindness, Visual Impairment Self-Efficacy Scale and is informed by Bandura’s158 guide for constructing self-efficacy scales. The measure is intended to be self-administered and completed on a recurring basis, as self-efficacy stores are malleable.107,158 As such, Web Content Accessibility Guidelines159 should also be followed to promote respondent equity. It is important to note that the Blindness, Visual Impairment Self-Efficacy Scale has not been tested and, thus, lacks empirical evidence. Rather, it is intended to promote scholarly attention and movement toward an improved design to which multiple self-efficacy dimensions may be captured for people with BVI, thereby improving experimental study designs and clinical care targeting for this population.
For instance, the Blindness, Visual Impairment Self-Efficacy Scale may be used as a tool to cultivate structural competency (eg, see160) in clinical practitioners working with people with BVI. For a graphical illustration of the Blindness, Visual Impairment Self-Efficacy Scale, see Figure 1.
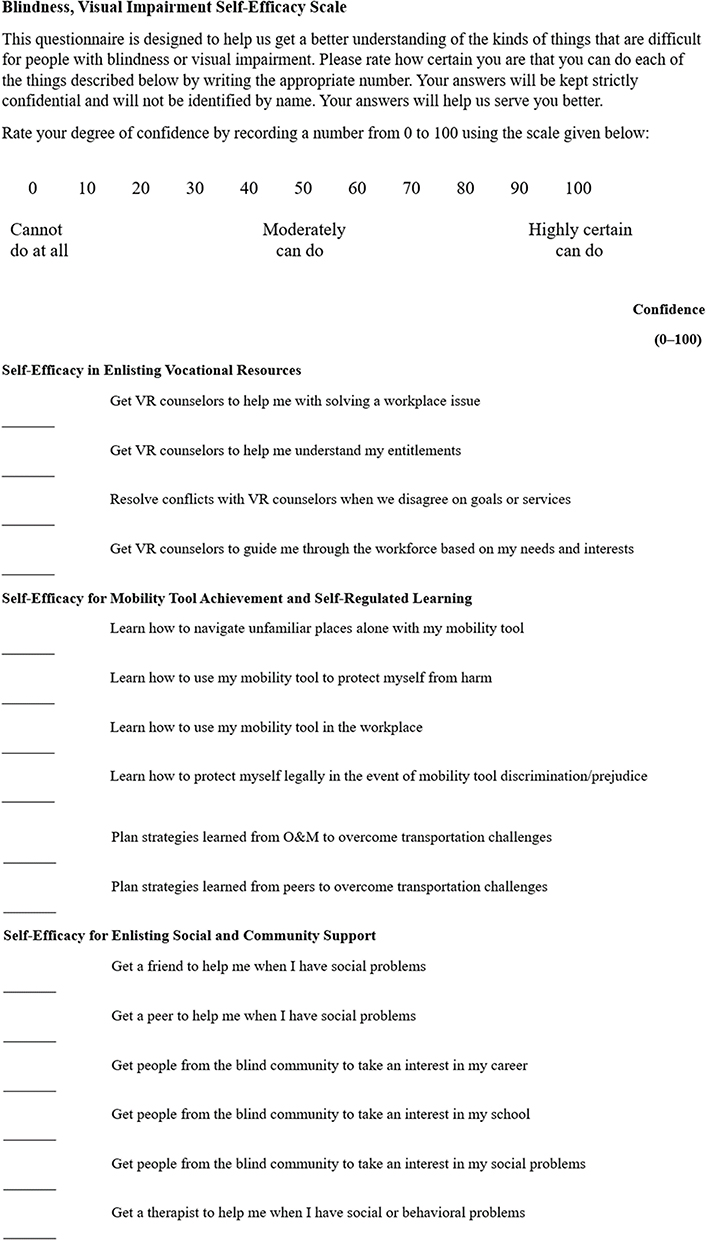 |
Figure 1 This figure displays the blindness and visual impairment self-efficacy scale. The blindness, visual impairment self-efficacy scale is a proposed scale and has no empirical strength. Notes: Used with permission of Information Age Publishing, from Bandura A. Guide for constructing self-efficacy scales. In: Pajares F, Urdan T, eds. Self-Efficacy Beliefs of Adolescents. 2006;5:307–337; permission conveyed through Copyright Clearance Center, Inc.158 |
A CEC course that integrates knowledge transition activities (eg, see151) can also lead to the development of teaching methods relative to the theory of self-efficacy (eg, see107). Such methods can be constructed as questions to which VR, O&M, and care practitioners may query their clients (ie, people with BVI) relative to self-efficacy dimensions. The purpose of the questions is to gain a more concentrated understanding of the disincentives to outcome expectations unique to clients. This can be better understood when examining Bandura’s158 distinction between perceived self-efficacy as a judgment of capability and perceived self-efficacy as a judgement of outcome expectations, specifically as it relates to performance accomplishments. According to Bandura:
Perceived self-efficacy is a judgment of capability to execute given types of performances; outcome expectations are judgments about the outcomes that are likely to flow from such performances. Outcome expectations take three different forms…. they include the positive and negative physical, social, and self-evaluative outcomes…. the positive expectations serve as incentives, the negative ones as disincentives. The outcomes people anticipate depend largely on their judgments of how well they will be able to perform in given situations.158
This explicative emphasizes that what an individual can do may present vastly different relative to the outcome depending on the situation and their judgment of it. When considering earlier research by Virgili and Rubin71 to which the authors questioned the lack of subjective outcome measures to assess the effects of O&M training for people with BVI, such as hope or quality of life, and current research by Zapata89 indicating that people with BVI who utilize mobility tools have 64% greater odds of unemployment, this distinction between perceived self-efficacy as a judgment of capability and perceived self-efficacy as a judgment of outcome expectations is imperative for health-rehabilitation professionals working with people with BVI. In other words, and for instance, people with BVI who participate in O&M training may feel self-efficacious following such training, in terms of navigation and mobility skills; however, such skill performance may become more ambiguous and, thus, less efficacious in the presence of specific social situations or unforeseen physiological problems. With respect to an appropriately framed question, the following question is proposed: “Are there any places, circumstances, or people in particular of which you believe that your O&M skills would be more difficult to use or employ?”
Conclusion
In summary, interdependencies related to the provision of mental health services as a resource exist between VR, O&M, and care practitioners involved in the health rehabilitation of people with BVI (see Figure 2). Multiple studies indicated long-term support for people with BVI was needed to adequately capture the diverse and entangled mental health issues experienced relative to VR-initiated services, mobility tool utility, and emotional reactions to vision loss and associated prejudice. Disability identity discourse and support was also a recurring theme within the literature, correlating psychological variables of well-being, self-efficacy, and self-worth. Such goals require the development of enhanced and appropriately targeted evaluative measures and approaches that center the multidimensional lives of people with BVI. VR’s short-term foci on competitive employment arguably frames mental health issues as a co-occurring detriment, which in turn reinforces the subjective norms placed on people with BVI and related employment potential. Relevant studies indicated that such behavior simply transcends into the clinical arena, building upon this notion that people with BVI have short-term problems which require short-term solutions; people with BVI must effectively choose between mental health or vocational stability.
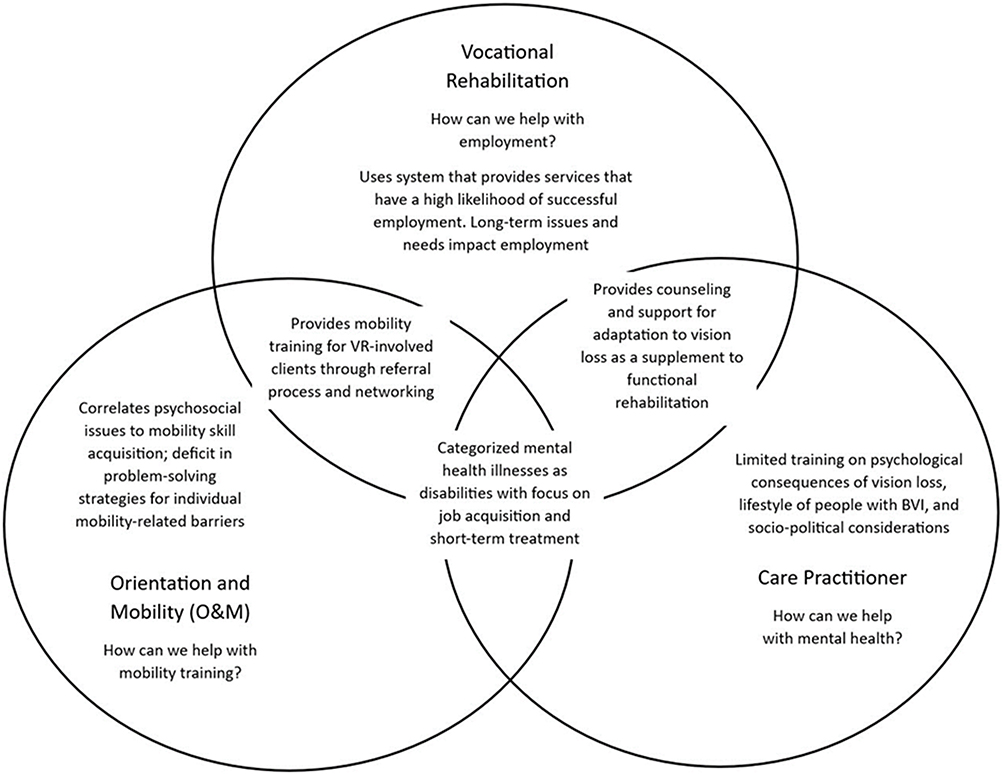 |
Figure 2 This figure illustrates the interdependent nature of VR, O&M, and care practitioners when considering mental health symptoms and subsequent provision of services for people with BVI. Notes: Adapted from Demmin DL, Silverstein SM. Visual impairment and mental health: unmet needs and treatment options. Clin Ophthalmol. 2020; 14:4229–4251. Creative Commons.13 |
This literature review demonstrates that integrating critical systems theory will illustrate the gap in mental health utility, address areas of social and biological influence, and promote future innovation in mental health policy and practice for people with BVI. The proposed dimensions to be explored through critical discourse to illustrate the current limitations in mental health policy and practice for people with BVI are as follows: (1) decenter disability as incontestable truths relative to the concept of mental health as a health-related resource for people with BVI, including mental health treatment and outcomes; (2) recenter ableism as a perpetuating social reality and, thus, psychological influence in the lives of people with BVI; (3) liberate the traditional methodology of psychological assessment for people with BVI engaged in health-rehabilitation processes, evoking new consciousness and improved relationships with health-rehabilitation professionals; (4) alter the self-perceptions of listeners, their roles and beliefs and the self-concept of people with BVI; and (5) engage in critical discourse through honest conversation and restructure disability as having subjective power and, thus, diversity.
The research findings revealed significant deficiencies in the traditional health-rehabilitation model for people with BVI, particularly as it relates to mental health resources and services. The limitation of the findings indicated that disability scholars need to advance research on integrating critical theories in work with people with BVI and accelerate qualitative, community-based methods to enhance understanding of this population and their unique mental health needs.
An educational podcast or forum may benefit to help spread awareness and facilitate education on the mental health gap in the lives of people with BVI. A podcast will help to expand accountability to the underutilization of mental health for people with BVI by way of establishing a common goal and vision. Much of the literature has examined mental health issues for people with BVI in organizational isolation. Observing an organization in its “wholeness” would simply constitute an overabundance of energy on a non-linear natured system; this is general systems thinking, not critical systems thinking. Thinking of an organization as a conversation rather than a machine encourages a collective equity that is accessible, collaborative, and designed to evolve knowledge to create new pathways to problem solving. DEI (eg, see115,116) encourages the sharing and exposure of new knowledge to create new pathways to problem solving, impacting collective equity.
Disclosure
The author reports no conflicts of interest in this work.
References
1. World Health Organization. Blindness and visual impairment; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment.
2. Lundeen EA, Saydah S, Ehrlich JR, Saaddine J. Self-Reported vision impairment and psychological distress in U.S. adults. Ophthal Epidemiol. 2022;29(2):171–181. doi:10.1080/09286586.2021.1918177
3. Choi HG, Lee MJ, Lee SM. Visual impairment and risk of depression: a longitudinal follow-up study using a national sample cohort. Sci Rep. 2018;8(1):2083. doi:10.1038/s41598-018-20374-5
4. Mayro EL, Murchison AP, Hark LA, et al. Prevalence of depressive symptoms and associated factors in an urban, ophthalmic population. Eur J Ophthalmol. 2021;31(2):740–747. doi:10.1177/1120672120901701
5. Zhang X, Bullard KM, Cotch MF, et al. Association between depression and functional vision loss in persons 20 years of age or older in the United States, national health, and nutrition examination survey 2005–2008. JAMA Ophthalmol. 2013;131(5):573–581. doi:10.1001/jamaophthalmol.2013.2597
6. Khorrami-Nejad M, Sarabandi A, Akbari MR, Askarizadeh F. The impact of visual impairment on quality of life. Med Hypothesis Discov Innov Ophthalmol. 2016;5(3):96–103.
7. Dhital A, Pey T, Stanford MR. Visual loss and falls: a review. Eye. 2010;24(9):1437–1446. doi:10.1038/eye.2010.60
8. Mojon-Azzi SM, Sousa-Poza A, Mojon DS. Impact of low vision on well-being in 10 European countries. Ophthalmologica. 2008;222(3):205–212. doi:10.1159/000126085
9. Kempen GI, Ballemans J, Ranchor AV, van Rens GH, Zijlstra GA. The impact of low vision on activities of daily living, symptoms of depression, feelings of anxiety and social support in community-living older adults seeking vision rehabilitation services. Qual Life Res. 2012;21(8):1405–1411. doi:10.1007/s11136-011-0061-y
10. Brunes A, B Hansen M, Heir T. Loneliness among adults with visual impairment: prevalence, associated factors, and relationship to life satisfaction. Health Qual Life Outcomes. 2019;17(1):24. doi:10.1186/s12955-019-1096-y
11. Brennan M, Horowitz A, Reinhardt JP, Stuen C, Rubio R, Oestreicher N. The societal impact of age-related macular degeneration: use of social support resources differs by the severity of the impairment. J Vis Impairment Blindness. 2011;105(1):5–19. doi:10.1177/0145482X1110500102
12. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–e116. doi:10.1016/S2214-109X(13)70145-1
13. Demmin DL, Silverstein SM. Visual impairment and mental health: unmet needs and treatment options. Clin Ophthalmol. 2020;14:4229–4251. doi:10.2147/OPTH.S258783
14. Rees G, Tee HW, Marella M, Fenwick E, Dirani M, Lamoureux EL. Vision-Specific distress and depressive symptoms in people with vision impairment. Invest Ophthalmol Vis Sci. 2010;51(6):2891–2896. doi:10.1167/iovs.09-5080
15. Chou C-F, Beckles GLA, Zhang X, Saaddine JB. Association of socioeconomic position with sensory impairment among us working-aged adults. Am J Public Health. 2015;105(6):1262–1268. doi:10.2105/AJPH.2014.302475
16. Carrière I, Delcourt C, Daien V, et al. A prospective study of the bi-directional association between vision loss and depression in the elderly. J Affect Disord. 2013;151(1):164–170. doi:10.1016/j.jad.2013.05.071
17. Holloway EE, Sturrock BA, Lamoureux EL, Keeffe JE, Rees G. Depression screening among older adults attending low-vision rehabilitation and eye-care services: characteristics of those who screen positive and client acceptability of screening. Australas J Ageing. 2015;34(4):229–234. doi:10.1111/ajag.12159
18. Nyman SR, Gosney MA, Victor CR. Psychosocial impact of visual impairment in working-age adults. Br J Ophthalmol. 2010;94(11):1427–1431. doi:10.1136/bjo.2009.164814
19. Senra H, Balaskas K, Mahmoodi N, Aslam T. Experience of anti-vascular endothelial growth factor therapy treatment and clinical levels of depression and anxiety in patients with wet age-related macular degeneration. Am J Ophthalmol. 2017;177:213–224. doi:10.1016/j.ajo.2017.03.005
20. Arluke A, Gritzer G. The Making of Rehabilitation: A Political Economy of Medical Specialization, 1890–1980 (Comparative Studies of Health Systems and Medical Care). University of California Press; 1985.
21. Donaldson E. Literatures of Madness: Disability Studies and Mental Health. Palgrave Macmillan; 2018.
22. Hiranandani V. Towards a critical theory of disability in social work. Crit Soc Work. 2019;6(1). doi:10.22329/csw.v6i1.5712
23. Minich JA. Enabling whom? Critical disability studies now. Lateral. 2016;5(1). doi:10.25158/L5.1.9
24. Stiker H-J. A History of Disability. University of Michigan Press; 1982.
25. Jürgen H. The Theory of Communicative Action. A Critique of Functionalist Reason. Beacon Press; 1987.
26. Ingstad B, Whyte SR. Disability and Culture. University of California Press; 1995.
27. Basic definition of disability, 20 C.F.R § 404.1505; 1980. Available from: https://www.ecfr.gov/current/title-20/chapter-III/part-404/subpart-P/subject-group-ECFRd3e28073a44a293/section-404.1505.
28. Bonaccio S, Connelly CE, Gellatly IR, Jetha A, Martin Ginis KA. The participation of people with disabilities in the workplace across the employment cycle: employer concerns and research evidence. J Bus Psychol. 2020;35(2):135–158. doi:10.1007/s10869-018-9602-5
29. Oi WY. Work for Americans with disabilities. Ann Am Acad Pol Soc Sci. 1992;523(1):159–174. doi:10.1177/0002716292523001014
30. United States Department of Labor. Disability resources; 2023. Available from: https://www.dol.gov/general/topic/disability.
31. Bureau of Labor Statistics. Persons with a disability [Data set]. Labor Force Characteristics. United States Department of Labor; 2023. Available from: https://www.bls.gov/news.release/pdf/disabl.pdf.
32. Workforce Innovation And Opportunity Act of. U.S.C. § 3101 et seq; 2014. Available from: https://uscode.house.gov/view.xhtml?path=/prelim@title29/chapter32&edition=prelim.
33. Division of Blind Services. Program Manual. Voc Rehab. Available from: https://dbs.fldoe.org/Voc-Rehab/Manual/.
34. Szasz TS. The Myth of Mental Illness. HarperPerennial; 1961.
35. Albee GW. To thine own self be true. Am Psychol. 1975;30(12):1156–1158. doi:10.1037/0003-066X.30.12.1156
36. Goffman E. Asylums: Essays on the Social Situation of Mental Patients and Other Inmates. Anchor Books; 1961.
37. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–136. doi:10.1126/science.847460
38. Crow L. Including all of our lives: renewing the social model of disability. In: Barnes C, Mercer G, editors. Exploring the Divide: Illness and Disability. Disability Press; 1996:5–9.
39. Benning TB. No such thing as mental illness? Critical reflections on the major ideas and legacy of Thomas Szasz. BJPsych Bull. 2016;40(6):292–295. doi:10.1192/pb.bp.115.053249
40. Wolfensberger W. The Principle of Normalization in Human Services. National Institute on Mental Retardation; 1972.
41. Oliver M, Barnes C. The New Politics of Disablement. Palgrave Macmillan; 2012.
42. Oliver M. The Politics of Disablement. Macmillan; 1990.
43. Bhattarai J, Bentley J, Morean W, Wegener ST, Pollack Porter KM. Promoting equity at the population level: putting the foundational principles into practice through disability advocacy. Rehabil Psychol. 2020;65(2):87–100. doi:10.1037/rep0000321
44. Herrman D, Papadimitriou C, Green B, LeFlore A, Magasi S. Relationships at work: integrating the perspectives of disability partners to enhance a peer navigation intervention. Front Rehabil Sci. 2022;3(1):876636. doi:10.3389/fresc.2022.876636
45. Iáñez Domínguez A, González Luna B. Disability in the Spanish press: from the paradigm of rehabilitation to the paradigm of personal autonomy. Commun Soc. 2019;32(1):77–90. doi:10.15581/003.32.1.77-90
46. World Health Organization. International classification of functioning, disability, and health. IMB Community Foundation; 2001. Available from: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health.
47. World Health Organization. Community based rehabilitation guidelines: CBR: community based rehabilitation. NLM classification: WB 320; 2010. Available from: https://www.who.int/publications/i/item/9789241548052.
48. Kurtaiş Y, Oztuna D, Küçükdeveci AA, Kutlay S, Hafiz M, Tennant A. Reliability, construct validity and measurement potential of the international classification of functioning, disability, and health: ICF. A comprehensive core set for osteoarthritis. BMC Musculoskelet Disord. 2011;12(255):1–12. doi:10.1186/1471-2474-12-255
49. Devoogdt N, Van Kampen M, Geraerts I, Coremans T, Christiaens MR. Lymphoedema functioning, disability, and health questionnaire: reliability and validity. Phys Ther. 2011;91(6):944–957. doi:10.2522/ptj.20100087
50. Pinna F, Fiorillo A, Tusconi M, Guiso B, Carpiniello B. Assessment of functioning in patients with schizophrenia and schizoaffective disorder with the mini-international classification of functioning, disability, and health: ICF-Application: a validation study in Italy. Int J Ment Health Syst. 2015;9(37):1–10. doi:10.1186/s13033-015-0030-x
51. Silva MR, Nobre MI, Carvalho KM, de Montilha R. Visual impairment, rehabilitation and international classification of functioning, disability, and health: ICF. Rev Bras Oftalmol. 2014;73(5):291–301. doi:10.5935/0034-7280.20140063
52. World Health Organization. Mental disorders; 2022. Availabe from: https://www.who.int/news-room/fact-sheets/detail/mental-disorders.
53. Shakespeare T, Kleine I. Educating health professionals about disability: a review of interventions. Health Soc Care Educ. 2013;2(2):20–37. doi:10.11120/hsce.2013.00026
54. Mueller S, Weintraub L. The workforce innovation and opportunity act of 2014. Plain Language Series. Issue No. 4. University of Massachusetts – Boston, Institute for Community Inclusion; 2020. Available from: https://thinkcollege.net/sites/default/files/files/resources/PL4_WIOA_R.pdf.
55. United States Department of Education. Individuals with Disabilities Education Act; 2023. Available from: https://sites.ed.gov/idea/.
56. United States Department of Health and Human Services. Programs for people with disabilities; 2023. Available from: https://www.hhs.gov/programs/social-services/programs-for-people-with-disabilities/index.html.
57. Rehabilitation act of 1973, 29 U.S.C. § 794 et seq; 1973. Available from: https://www.govinfo.gov/content/pkg/USCODE-2010-title29/html/USCODE-2010-title29-chap16.htm.
58. Americans with Disabilities Act of 1990. U.S.C. § 12101 et seq;1990:42. Available from: https://www.ada.gov/pubs/adastatute08.htm.
59. Dean D, Pepper JV, Schmidt R, Stern S. The effects of vocational rehabilitation services for people with mental illness. J Hum Resour. 2017;52(3):826–858. doi:10.3368/jhr.52.3.0114-6111R1
60. Crudden A, Steverson A. Job retention: perspectives of individuals with blindness and low vision. J Vocat Rehabil. 2022;57(2):127–140. doi:10.3233/JVR-221204
61. Bruce I, Baker M. Segmenting and targeting employed and unemployed people with sight problems. Int Congr S. 2005;1282:1125–1129. doi:10.1016/j.ics.2005.05.054
62. Crudden A, Steverson AC. Job retention and career advancement: a survey of persons who are blind or have low vision. J Rehabil. 2021;87(2):28–35.
63. Papakonstantinou D. Person-Related factors of people with disabilities affecting employers’ attitudes toward their vocational integration: a literature review of the top list. J Rehabil. 2022;88(2):11–20.
64. Annual disability statistics compendium. Vocational rehabilitation—number of participants served, number of cases closed with and without employment by State Agency: 2016 [Data set]; 2021. Available from: https://disabilitycompendium.org/compendium/2021-annual-disability-statistics-compendium-A?page=19.
65. Paul S, Rafal M, Houtenville A. Annual Disability Statistics Compendium: 2021 (Table 14.1). University of New Hampshire, Institute on Disability; 2021.
66. Wiener WR, Welsh RL, Blasch BB. Foundations of Orientation and Mobility. AFB Press; 2010.
67. University of Alabama in Huntsville. Orientation and mobility concentration; 2023. Available from: https://www.uah.edu/education/departments/curriculum-and-instruction/graduate-programs/master-of-education/orientation-and-mobility-concentration.
68. Academy for Certification of Vision Rehabilitation and Education Professionals. Certifications; 2023. Available from: https://www.acvrep.org/certifications/landing.
69. Keay LJ, Chang KJ, Angell B, Rogers K, Jan S. Cost-benefit analysis of orientation and mobility programs for adults with vision disability: a contingent valuation study. Disabil Rehabil. 2022;45(5):857–865. doi:10.1080/09638288.2022.2044523
70. National Federation of the Blind. Blindness statistics; 2019. Available from: https://nfb.org/resources/blindness-statistics.
71. Virgili G, Rubin G. Orientation and mobility training for adults with low vision. Cochrane Database Syst Rev. 2010;2010(5):1–23. doi:10.1002/14651858.CD003925.pub3
72. Fixsen A, Seers H, Polley M, Robins J. Applying critical systems thinking to social prescribing: a relational model of stakeholder “buy-in. BMC Health Serv Res. 2020;20(1):580. doi:10.1186/s12913-020-05443-8
73. Cmar JL, McDonnall MC. Characteristics, services, and outcomes of vocational rehabilitation consumers who are deaf-blind. J Am Deafness Rehabil Assoc. 2019;52(2):12–23.
74. Division of Vocational Rehabilitation. Counselor policy manual. Rehab Works; 2018. Available from: https://www.rehabworks.org/_resources/docs/policies/manual/counselor-policy-manual.pdf.
75. Shakespeare T. Disability Rights and Wrongs Revisited. Routledge; 2013.
76. Social Security Administration. Vocational rehabilitation providers’ handbook. Social Security Administration; 2020. Available from: https://yourtickettowork.ssa.gov/Assets/yttw/docs/vocational-rehabilitation/VR-Providers-Handbook-2020.pdf.
77. Bertalanffy LV. General System Theory: Foundations, Development, Applications. George Braziller Inc; 1968.
78. Slusser MM, García Luis I, Reed C-R, McGinnis PQ. Foundations of Interprofessional Collaborative Practice in Health Care. Elsevier; 2019.
79. Stringfellow EJ. Applying structural systems thinking to frame perspectives on social work innovation. Res Soc Work Pract. 2017;27(2):154–162. doi:10.1177/1049731516660850
80. Gillies DA. Nursing Management: A Systems Approach. W B Saunders; 1982.
81. World Health Organization. List of official ICD-10 updates ratified. World Health Organization; 2006 [cited February 17, 2024]. Available from: https://www.who.int/publications/m/item/icd-10-updates-2006.
82. Meaning of blindness as defined in the law, 20 C.F.R. § 404.1581; 1980. Available from: https://www.ecfr.gov/current/title-20/section-404.1581.
83. Guerette AR, Smedema SM. The relationship of perceived social support with well-being in adults with visual impairments. J Vis Impairment Blindness. 2011;105(7):425–439. doi:10.1177/0145482X1110500705
84. Anderson CA, Hergenrather K, Jones WD. Empowering community voices: the influences of consumer race, disability, and poverty on public vocational rehabilitation service engagement. J Rehabil. 2021;87(1):40–47.
85. Bourgeois P, Green K, Hartley M, White M, Clarke B. Moral distress within rehabilitation counseling. Rehabil Res Policy Educ. 2021;35(2):117–128. doi:10.1891/RE-20-08
86. Giesen JM, Hierholzer A. Vocational rehabilitation services and employment for social security disability income beneficiaries with visual impairments. J Vocat Rehabil. 2016;44(2):175–189. doi:10.3233/JVR-150789
87. Clapp CM, Pepper JV, Schmidt R, Stern S. Overview of vocational rehabilitation data about people with visual impairments: demographics, services, and long-run labor market trends. J Vis Impairment Blindness. 2020;114(1):43–56. doi:10.1177/0145482X20901380
88. McDonnall MC, Lund EM. Employers’ intent to hire people who are blind or visually impaired: a test of the theory of planned behavior. Rehabil Couns Bull. 2019;63(4):206–215. doi:10.1177/0034355219893061
89. Zapata MA. An exploratory study of general self-efficacy and employment in adults with retinitis pigmentosa. J Vis Impairment Blindness. 2020a;114(1):18–30. doi:10.1177/0145482X19900715
90. Zapata MA. Disability affirmation predicts employment among adults with visual impairment and blindness. Rehabil Couns Bull. 2020b;65(2):120–128. doi:10.1177/0034355220957107
91. Zapata MA. Mobility tool use relates to disability affirmation among adults with visual impairments. J Vis Impairment Blindness. 2021;115(5):382–392. doi:10.1177/0145482X211046684
92. Zapata MA. Group identity in blindness groups predicts life satisfaction and lower anxiety and depression. Rehabil Psychol. 2022;67(1):42–52. doi:10.1037/rep0000432
93. Zapata MA, Pearlstein JG. Disability self‐worth relates to lower anxiety and depression in people with visual impairment. J Clin Psychol. 2022;78(7):1491–1499. doi:10.1002/jclp.23308
94. McDonnall MC, Cmar JL, McKnight Z. What predicts job quality of vocational rehabilitation consumers who are blind or have low vision? Rehabil Couns Bull. 2021;66(2):100–111. doi:10.1177/00343552211060012
95. Lund EM, Cmar JL. Factors related to employment outcomes for vocational rehabilitation consumers with visual impairments: a systematic review. J Vis Impairment Blindness. 2019;113(6):518–537. doi:10.1177/0145482X19885277
96. Papadopoulos K, Papakonstantinou D, Koutsoklenis A, Koustriava E, Kouderi V. Social support, social networks, and happiness of individuals with visual impairments. Rehabil Couns Bull. 2015;58(4):240–249. doi:10.1177/0034355214535471
97. McDonnall MC, Cmar JL, McKnight ZS. Beyond employment rates: self-employment and other categories of work among people with visual impairments. J Vis Impair Blind. 2022;116(5):729–735. doi:10.1177/0145482X221128831
98. Papakonstantinou D, Papadopoulos K. Forms of social support in the workplace for individuals with visual impairments. J Vis Impairment Blindness. 2010;104(3):183–187. doi:10.1177/0145482X1010400306
99. Khodabakhshi Koolaee A, Mosalanejad L, Mamaghanirad B. The effectiveness of group training of choice theory on quality of life and hope in blind people. Iran Rehabil J. 2017;15(3):199–206. doi:10.29252/nrip.irj.15.3.199
100. Haegele JA, Zhu X, Healy S. Behavioral correlates of depression among adults with visual impairments. J Vis Impairment Blindness. 2021;115(5):403–413. doi:10.1177/0145482X211046696
101. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Processes. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
102. Rubin SE, Chan F, Bishop M, Miller SM. Psychometric validation of the sense of well-being inventory for program evaluation in rehabilitation. Prof Rehabil. 2003;11(2):54–59.
103. Cimarolli VR, Boerner K. Social support and well-being in adults who are visually impaired. J Vis Impairment Blindness. 2005;99(9):521–534. doi:10.1177/0145482X0509900904
104. Bamberg S, Ajzen I, Schmidt P. Choice of travel mode in the theory of planned behavior: the roles of past behavior, habit, and reasoned action. Basic Appl Soc Psychol. 2003;25(3):175–187. doi:10.1207/S15324834BASP2503_01
105. Suntornsan S, Chudech S, Janmaimool P. The role of the theory of planned behavior in explaining the energy-saving behaviors of high school students with physical impairments. Behav Sci. 2022;12(9):334. doi:10.3390/bs12090334
106. Hagger MS, Hamilton K. Longitudinal tests of the theory of planned behaviour: a meta-analysis. Eur Rev Soc Psychol. 2023;1–57. doi:10.1080/10463283.2023.2225897
107. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037//0033-295x.84.2.191
108. Dunn DS, Burcaw S. Disability identity: exploring narrative accounts of disability. Rehabil Psychol. 2013;58(2):148–157. doi:10.1037/a0031691
109. Putnam M. Conceptualizing disability: developing a framework for political disability identity. J Disabil Policy Stud. 2005;16(3):188–198. doi:10.1177/10442073050160030601
110. Kroenke K, Spitzer RL, Williams JB, Löwe B. An ultra-brief screening scale for anxiety and depression: the patient health questionnaire-4. Psychosomatics. 2009;50(6):613–621. doi:10.1176/appi.psy.50.6.613
111. Chan F, Wang -C-C, Fitzgerald S, Muller V, Ditchman N, Menz F. Personal, environmental, and service-delivery determinants of employment quality for state vocational rehabilitation consumers: a multilevel analysis. J Vocat Rehabil. 2016;45(1):5–18. doi:10.3233/JVR-160806
112. McDonnall MC, Cmar J. Employment outcomes and job quality of vocational rehabilitation consumers with deaf-blindness. Rehabil Couns Bull. 2019;63(1):13–24. doi:10.1177/0034355218769461
113. McDonnall MC, Cmar JL, McKnight ZS. Service factors and personal characteristics associated with employment and job quality for vocational rehabilitation consumers with combined traumatic brain injury and visual impairment. J Vocat Rehabil. 2020;52(3):223–238. doi:10.3233/JVR-201073
114. Jameton A. Nursing Practice: The Ethical Issues. Prentice Hall; 1984.
115. Dyer J, Gushwa M. Going Diversity, Equity, Inclusion, Power, Antiracism DEIPAR Deeper: Developing and Incorporating a Social Justice Curricular Framework [Manuscript submitted for publication]. DSW Program, Simmons University; 2023.
116. Arsel Z, Crockett D, Scott ML. Diversity, equity, and inclusion (DEI) in the journal of consumer research: a curation and research agenda. J Con Res. 2022;48(5):920–933. doi:10.1093/jcr/ucab057
117. Glasser W. Choice Theory. HaperCollins Publishers; 1998.
118. The WHOQOL Group. The Development of the World Health Organization Quality of Life Assessment Instrument (the WHOQOL). In: Orley J, Kuyken W, editors. Quality of Life Assessment. International Perspectives. Springer; 1994. doi:10.1007/978-3-642-79123-9_4
119. Walsh T. A right to inclusion? Homelessness, human rights and social exclusion. Aust J Hum Rights. 2006;12(1):185–204. doi:10.1080/1323238X.2006.11910818
120. Lievrouw L. Alternative and Activist New Media. Polity Press; 2011.
121. Miranda SM, Young AG, Yetgin E. Are social media emancipatory or hegemonic? Societal effects of mass media digitization in the Case of the SOPA Discourse. MIS Q. 2016;40(2):303–329. doi:10.25300/MISQ/2016/40.2.02
122. Sunstein CR. The law of group polarization. J Pol Philos. 2002;10(2):175–195. doi:10.1111/1467-9760.00148
123. Kiernan MA, Mitchell BG, Russo PL. The power of podcasts: exploring the endless possibilities of audio education and information in medicine, healthcare epidemiology, and antimicrobial stewardship. Antimicrob Stewardship Healthc Epidemiol. 2023;3(1):e98, 1–3. doi:10.1017/ash.2023.178
124. Tobin SJ, Guadagno RE. Why people listen: motivations and outcomes of podcast listening. PLoS One. 2022;17(4):e0265806. doi:10.1371/journal.pone.0265806
125. Roland D, Thoma B, Tagg A, Woods J, Chan TM, Riddell J. What are the real-world podcast-listening habits of medical professionals? Cureus. 2021;13(7):e16240, 1–9. doi:10.7759/cureus.16240
126. Horkheimer M. Traditional and Critical Theory. Continuum; 1937.
127. Belkin-Martinez D. The liberation health model: theory and practice. In: Belkin Martinez D, Fleck-Henderson A, editors. Social Justice in Clinical Practice: A Liberation Health Framework for Social Work. Routledge; 2014:9–28.
128. Hall MC. Critical disability theory. Stanford Encycl Philos. Metaphysics Research Laboratory, Stanford University; 2019. Available from: https://plato.stanford.edu/archives/win2019/entries/disability-critical/.
129. Schalk S. Critical disability studies as methodology. Lateral. 2017;6(1):1–4. doi:10.25158/L6.1.13
130. Onedera JD, Greenwalt B. Choice theory: an interview with Dr. William Glasser. Fam J. 2007;15(1):79–86. doi:10.1177/1066480706294150
131. Kondrat ME. Actor-Centered social work: re-Visioning “person-in-environment” through a critical theory lens. Soc Work. 2002;47(4):435–448. doi:10.1093/sw/47.4.435
132. Adams M. Readings for Diversity and Social Justice [Introduction]. Castañeda C, Hackman H, Peters M, Zúñiga X, Blumenfeld W, editors. Routledge; 2010:1–5.
133. Adams M, Castañeda C, Hackman H, Peters M, Zúñiga X, Blumenfeld W. Readings for Diversity and Social Justice. Routledge; 2010.
134. Hardiman R, Jackson B, Griffin P. Conceptual foundations for social justice education. In: Adams M, Bell L, Griffin P, editors. Teaching for Diversity and Social Justice. Routledge; 2007:35–66.
135. Freire P. Pedagogy of the Oppressed. Continuum International Publishing Group Ltd; 1994.
136. Beresford P. Radical social work and service users: a crucial connection. In: Lavalette M, editor. Radical Social Work Today: Social Work at the Crossroads. Policy Press; 2011:95–114.
137. Burton M, Kagan C. Liberation social psychology: learning from Latin America. Community Appl Soc Psy. 2005;15(1):63–78. doi:10.1002/casp.786
138. Freire P. Education as the practice of freedom. In: Freire P, editor. Education for Critical Consciousness. Continuum; 1974:1–78.
139. Forber-Pratt AJ, Mueller CO, Andrews EE. Disability identity and allyship in rehabilitation psychology: sit, stand, sign, and show up. Rehabil Psychol. 2019;64(2):119–129. doi:10.1037/rep0000256
140. Kulnik ST, Nikoletou D. A qualitative study of views on disability and expectations from community rehabilitation service users. Health Soc Care Community. 2017;25(1):43–53. doi:10.1111/hsc.12180
141. Rebolledo-Sanhueza J, Besoain-Saldaña Á, Manríquez-Hizaut M, Huepe-Ortega G, Aliaga-Castillo V. Experiencias y percepciones sobre discapacidad y participación social en centros de rehabilitación comunitaria de Chile. Saúde Soc. 2021;30(2):1–10. doi:10.1590/s0104-12902021200858
142. Brooks NA. Self-empowerment among adults with severe physical disability: a case study. J Sociol Soc Welf. 1991;18(1):105–120. doi:10.15453/0191-5096.1971
143. Brzuzy S. Deconstructing disability. J Pover. 1997;1(1):81–91. doi:10.1300/J134v01n01_06
144. Quinn P. Social work education and disability. J Teach Soc Work. 1996;12(1–2):55–71. doi:10.1300/J067v12n01_05
145. Hahn H. Paternalism and public policy. Society. 1983;20(3):36–46. doi:10.1007/BF02700073
146. Mackelprang RW, Salsgiver RO. People with disabilities and social work: historical and contemporary issues. Soc Work. 1996;41(1):7–14. doi:10.1093/sw/41.1.7
147. Kant JD. Becoming a liberation health social worker. In: Martinez DB, editor. Social Justice in Clinical Practice: A Liberation Health Framework for Social Work. Routledge; 2014:29–43.
148. Moya P. What’s identity got to do with it? Mobilizing identities in the multicultural classroom. In: Alcoff LM, Hames-Garcia M, Mohanty SP, editors. Identity Politics Reconsidered. Palgrave Macmillan; 2006:96–117.
149. Charlton JI. Nothing About Us Without Us: Disability Oppression and Empowerment. University of California Press; 1998.
150. Davis D, Evans M, Jadad A, et al. The case for knowledge translation: shortening the journey from evidence to effect. BMJ. 2003;327(7405):33–35. doi:10.1136/bmj.327.7405.33
151. Schreiber J, Perry S, Downey P, Williamson A. Knowledge translation outcomes following innovative continuing education. J Phys Ther Educ. 2015;29(4):42–51. doi:10.1097/00001416-201529040-00007
152. Rappolt S, Tassone M. How rehabilitation therapists gather, evaluate, and implement new knowledge. J Contin Educ Health Prof. 2002;22(3):170–180. doi:10.1002/chp.1340220306
153. Ketelaar M, Russell DJ, Gorter JW. The challenge of moving evidence-based measures into clinical practice: lessons in knowledge translation. Phys Occup Ther Pediatr. 2008;28(2):191–206. doi:10.1080/01942630802192610
154. Taylor JM, Neimeyer GJ. The development of the professional competencies scale: foundational, functional, and continuing competencies. Train Educ Prof Psychol. 2022;16(2):112–120. doi:10.1037/tep0000383
155. Luhanga U, Chen W, Minor S, et al. Promoting transfer of learning to practice in online continuing professional development. J Contin Educ Health Prof. 2022;42(4):269–273. doi:10.1097/CEH.0000000000000393
156. Kucsera JV, Zimmaro DM. Comparing the effectiveness of intensive and traditional courses. Coll Technol. 2010;58(2):62–68. doi:10.1080/87567550903583769
157. McCluskey A, Lovarini M. Providing education on evidence-based practice improved knowledge but did not change behavior: a before and after study. BMC Med Educ. 2005;5:40. doi:10.1186/1472-6920-5-40
158. Bandura A. Guide for constructing self-efficacy scales. In: Pajares F, Urdan T, editors. Self-Efficacy Beliefs of Adolescents. Information Age Publishing; 2006:307–337.
159. Web accessibility initiative. Web content accessibility guidelines WCAG 2.2; 2023. Available rom: https://www.w3.org/TR/WCAG22/.
160. Bourgois P, Holmes SM, Sue K, Quesada J. Structural vulnerability: operationalizing the concept to address health disparities in clinical care. Acad Med. 2017;92(3):299–307. doi:10.1097/ACM.0000000000001294
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.