")
Back to Journals » Clinical Optometry » Volume 15
The Patients’ Perspective for the Impact of Late Detection of Ocular Diseases on Quality of Life: A Cross-Sectional Study
Authors Almazroa A , Almatar H , Alduhayan R , Albalawi M, Alghamdi M , Alhoshan S, Alamri S, Alkanhal N, Alsiwat YJ, Alrabiah S, Aldrgham M, AlSaleh AA, Alsanad HA, Alsomaie B
Received 22 May 2023
Accepted for publication 1 September 2023
Published 11 September 2023 Volume 2023:15 Pages 191—204
DOI https://doi.org/10.2147/OPTO.S422451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Ahmed Almazroa,1,2 Hessa Almatar,1,2 Reema Alduhayan,1,2 Maram Albalawi,2,3 Mansour Alghamdi,4 Saja Alhoshan,5 Suhailah Alamri,1,2 Norah Alkanhal,1,2 Yara J Alsiwat,1,2 Saad Alrabiah,6 Mohammed Aldrgham,7 Ahmed A AlSaleh,8 Hessa Abdulrahman Alsanad,9 Barrak Alsomaie1,2
1Department of Imaging Research, King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 2King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 3Department of Biostatistics and Bioinformatics, King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 4Department of Optometry and Vision Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia; 5Department of Ophthalmology, King Abdulaziz Medical City, Ministry of National Guard-Health Affairs, Riyadh, Saudi Arabia; 6Department of Ophthalmology, King Fahad Medical City, Riyadh, Saudi Arabia; 7Department of Ophthalmology, King Abdullah bin Abdulaziz University Hospital, Princess Nourah Bint AbdulRahman University, Riyadh, Saudi Arabia; 8AL-Hokama Eye Specialist Center, Riyadh, Saudi Arabia; 9Department of Social Planning, College of Social Work, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia
Correspondence: Ahmed Almazroa, Email [email protected]
Background: Late detection of ocular diseases negatively affects patients’ quality of life (QoL), encompassing health status, psychological, financial, and social aspects. However, the early detection of eye conditions leads to rapid intervention and avoiding complications, thus preserving the QoL. This study assessed the impact of ocular diseases late detection on patients’ QoL at multi-eye clinics based on questionnaire responses.
Methods: We developed an original Arabic-English questionnaire to assess the QoL of patients with ocular diseases referred from primary and secondary healthcare centers to tertiary hospitals. It covered preliminary data, patient perspectives on having lately detected ocular disease and treatment costs, and the impact of late detection on finances, social life, psychology, health status, and awareness of current initiatives. Logistic regression analysis was used to explore the associations between patient perspectives on having ocular diseases detected at a late stage and its impact on different domains. Multivariate logistic regression was applied with impact types of health status, psychological, financial, and social (dependent variables) and age, income levels, and hospital type (independent variables).
Results: Three hundred and eighty-eight responded, with 50% experiencing psychological effects, 27% health issues, 23% social impacts, and 23% financial burdens. Two hundred seventeen patients (56%) reported having ocular condition detected in late stage. Logistic regression analysis showed positive association with health status, social well-being, and financial effects (p < 0.05). Multivariate analysis revealed pronounced effects in patients ≤ 50 years, with income \< 5000 SAR, and those visiting private clinics (p < 0.05). The social impact was greater in patients visiting private hospitals. Ninety percent of all patients emphasized the importance of increasing awareness for better QoL.
Conclusion: Significant associations were found between the late detection of eye diseases and their impact on QoL. Therefore, early detection and increasing patients’ awareness of ocular diseases and treatment are essential.
Keywords: irreversible vision, physiological effects, financial effects, social effects, ocular diseases
Introduction
Quality of life (QoL) encompasses various elements that contribute to individuals’ life satisfaction, including physical and psychological health, life contentment, and social well-being.1–3 According to the World Health Organization (WHO), QoL is defined as individuals’ perceptions of their position in life within their cultural and value contexts, involving their aspirations, expectations, standards, and concerns.4 The consequence of losing normal visual function is a vision impairment (VI), which poses a significant impediment to many eye diseases and negatively affects the QoL of patients and their families.5,6 Approximately, 1.1 billion people globally have VI, and this number is projected to rise to approximately 1.8 billion by 2050.7 Furthermore, VI and ocular diseases cause a significant economic burden on medical care.8 In US, treating VI diseases, including medical, nursing care, and supportive services, reached $98.7 billion in 2017.9 Moreover, sever visually impaired open-angle glaucoma patients have medical healthcare expenditures higher than those with mild and moderate cases.10
VI can be either reversible or irreversible, often due to delayed detection of ocular diseases that result in permanent damage.11–13 Irreversible VI has the most profound impact on patients’ QoL, affecting their functioning, emotional well-being, mobility, and independence.5,14 Numerous studies have evaluated the impact of early and late stages of irreversible ocular diseases on QoL,3,5,15 including vision-threatening diabetic retinopathy (DR) and age-related macular degeneration (AMD). A late-stage of DR and AMD have a greater impact on QoL, while, in the early stages, there were no impact on QoL. On the other hand, few studies have comprehensively assessed the effect of the late detection of ocular diseases on QoL. Most studies have focused on a specific aspect of QoL in relation to a particular disease; for instance, Chai et al observed increased physiological symptoms of anxiety and depression in children with strabismus.16 Moreover, other studies have found that patients with vision loss due to AMD exhibit similarities to individuals with other serious chronic illnesses in terms of depression and psychological distress.17 Some studies have investigated QoL in the context of social influence; for instance, Devenney et al reported that DR had various effects on QoL, including social isolation and loss of social roles.18 Additionally, cases of poor face recognition associated with VI have been found to impact social life and activities, and increase the risk of isolation.19 Regarding health effects, vision significantly influences an individual’s health status, mobility, and ability to perform daily activities.20,21 Older adults with visual impairment face a heightened risk of mobility limitations.20 Moreover, VI is associated with an increased risk of falls.21
Several studies have highlighted the financial ramifications for the increasing prevalence of VI. For instance, Marques et al examined the global reduction in employment and annual productivity due to VI, revealing a productivity loss of $410.7 billion and 30.2% decrease in employment due to VI.22 Another study emphasized that individual costs, including income reduction and career burdens resulting from VI, surpass those of the medical and healthcare systems.23 Consequently, understanding the distinct impacts (health, psychological, financial, and social) of eye diseases on QoL is essential for providing tailored solutions to patients. The early detection and utilization of ophthalmic interventions play a pivotal role in clinical management to safeguard and enhance QoL.24,25
Furthermore, a crucial factor for the optimal clinical management and preservation of QoL is awareness and educational level among patients with ocular diseases. Prior research has explored patient awareness regarding the early diagnosis of ocular diseases.26–29 Scholars from various countries have assessed awareness levels concerning eye diseases in patients26,27 or parents of children with ocular diseases.28,29 These findings consistently indicated limited awareness levels. Therefore, promoting guidelines for late-detected ocular diseases among patients is crucial for enhancing knowledge and mitigating the risk of vision-threatening complications. This is especially significant as healthcare transitions toward a more holistic and value-based care approach. In this study, we aimed to investigate the impact of late detection of ocular diseases on QoL among patients visiting retinal and glaucoma clinics at tertiary hospitals within the Saudi population. We used questionnaires to assess health status, physiological effects, financial implications, and social consequences. In addition, we evaluated the level of awareness regarding ongoing educational initiatives for the early diagnosis of ocular diseases. Such insights have the potential to enhance interactions between healthcare providers and patients and support the decision-making processes, and contribute to improved healthcare services and QoL.
Methods
Study Population and Design
This cross-sectional questionnaire study was conducted between January 2020 and September 2022. The patients were recruited from ophthalmology at governmental tertiary hospitals in Riyadh (King Abdulaziz Medical City (KAMC) at the Ministry of National Guard; King Fahad Medical City at the Ministry of Health; and King Abdullah bin Abdulaziz University Hospital), and a private eye center (Alhokama Eye Specialist Center) in Riyadh, Saudi Arabia.
This study included random male or female patients aged 18 years or older, visiting retina and glaucoma clinics at tertiary hospitals to provide sub specialty eye care for advanced ocular diseases’ (vision loss) cases. Patients with advanced eye conditions due to trauma were excluded from the study.
The study was approved by the ethical committee of the King Abdullah International Medical Research Center. Furthermore, authorized by Institutional Review Board (IRB) number RC20/007/R. The study was adhered to the rules of the Declaration of Helsinki for research involving human participants. A consent form was introduced to the patients, with a full explanation of the study aims and the contents of the questionnaire. Then, an optometrist interviewed the patients and their attendants (if required) to answer the questionnaire for 15–20 minutes.
Clinical Assessment of Eye Diseases
The patients were referred from primary healthcare centers, where only a Visual Acuity (VA) test was conducted by nurses (except for KAMC, the VA test and refraction were conducted by optometrists), with no further ocular screening examinations, and secondary healthcare centers, where further slit lamp examinations were conducted by non-specialized ophthalmologists. Thus, all referred patients had no follow-up for their cases at these centers (1st visit). Therefore, they were referred for urgent ophthalmic intervention due to vision loss (not trauma). On the other hand, patients visiting a private clinic were not required to pre-visit a primary healthcare centers for the referral. All patients were recorded with advanced ocular diseases such as glaucoma, diabetic retinopathy and its associated complications, and AMD with consideration of not early detection. Therefore, no clinical assessment was conducted in this study.
Questionnaire Validity and Resource
A consultation was held with faculty members from the Social planning department at the Social Work College in Princess Nourah bint Abdulrahman University to develop an original Arabic- English questionnaire comprising 79 questions. Thereafter, the questionnaire was introduced to pilot patients (25 patients) at KAMC to check whether it was appropriate and had no issues. Seventeen questions were removed due to their difficulty and misunderstanding, whereas 62 questions remained.
Questionnaire Components
The questionnaire conveys four domains: patients primary data, late detection and treatment costs, the impact of vision loss, and level of awareness of current initiatives and future suggestions. See Figure 1.
- Patients’ primary data in multiple-choice questions included age, education, educational level, marital status, employment status, children, family monthly income, place of residence, type of residence, owner of the residence, type of home, and who is responsible for paying for medical care (government, insurance, or self-paid).
- Patients’ perspective on having advance ocular disease detected in late stage and its treatment costs in yes/no questions, including two main questions: “Do you have advanced ocular disease? Detected at a late stage” and “do you know that the charges are costly when ocular diseases are detected in an late stage?”. If they answered “yes” to both questions, eight detailed yes/no questions were probed to address the costs of eye disease cases.
- The impact of vision loss on one’s health status, psychological, financial, and social well-being in yes/no questions included four main questions: “Does your eye condition affect your health status?” “did you have any negative or psychological feelings because of your eye condition?”, “was your income affected by your eye condition?”, “Were your social or family relationships affected by your eye condition?”. If the patient responded with a “yes”, then 4–8 specific yes/no type questions were further asked for each main question.
- The level of awareness of present educational initiatives for the early diagnosis of ocular diseases was assessed through yes/no questions, along with the patients’ initiatives and suggestions to identify cases earlier.
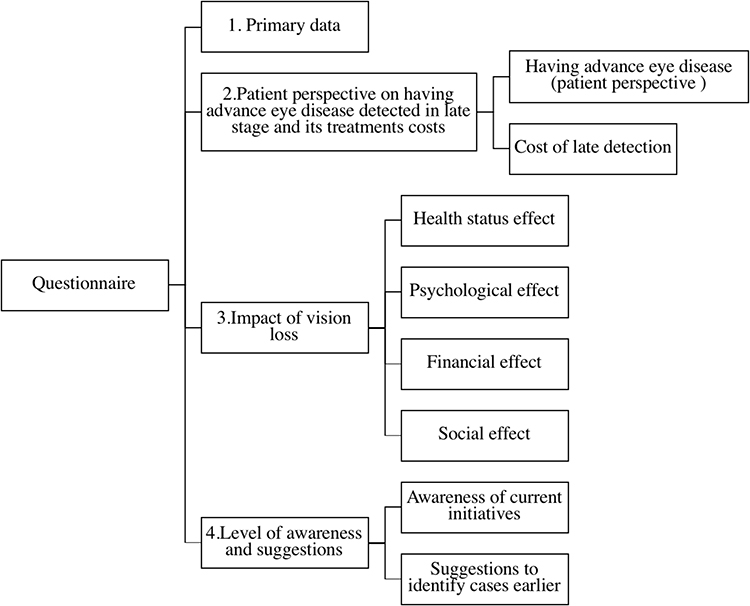 |
Figure 1 Questionnaire Components. |
Statistical Analysis
All data analyses were conducted using SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA) to evaluate primary outcome measures. Data were presented as frequencies and percentages. In the results tables, (n) represents the number of patients, excluding missing values. Logistic regression analysis was performed to test the relationship between the types of impact (health status, psychological, financial, and social) and patient perspective on having ocular eye diseases. Moreover, multivariate logistic regression was used to assess the association of the type of impact (health status, psychological, financial, and social) as dependent variables and age, educational status, income levels, and type of hospital as independent variables. The significance level was set at P < 0.05.
Results
Table 1 presents the demographics and characteristics of the 388 patients (Questioner components section [#1 in Figure 1]). The majority of the patients were 50 years old or older, which was expected because of their eye-related pathological conditions. Furthermore 30% were from outside Riyadh.
 |
Table 1 Patients Demographic Characteristics |
The patients’ characteristics were collected to be associated with the rest of the questioner for the logistic regression and the multivariate logistic regression analysis. However, few variables were excluded from the analysis due to missing responses such as the gender and level of education. While other variables were excluded due to the lack of compatibility such as having children or not and the type of the residency location. The instances of missing data were attributed to the patients choosing to avoid the question for personal reasons. However, data related to gender (54%), where the question was not visible (located at the top of the questionnaire page) to the optometrists administering the questionnaire.
Table 2 presents the patients’ responses (Questioner components section [#2 in Figure 1]) regarding their awareness of late detection and the associated treatment costs. Despite all patients seeking care at tertiary hospitals for subspecialty treatment, 43% reported not having advanced eye conditions detected in the late stage. Moreover, nearly 30% were uninformed about the treatment costs associated with eye diseases detected in the late stages.
 |
Table 2 Participants’ Awareness of the Disease’s Late Detection and Treatment Costs |
Health status, psychological, financial, and social effects questions are listed in Table 3. The primary effect was the psychological effects for all the patients with stress and fear due to vision condition being the primary concern, followed by health status effects, then social and financial impacts.
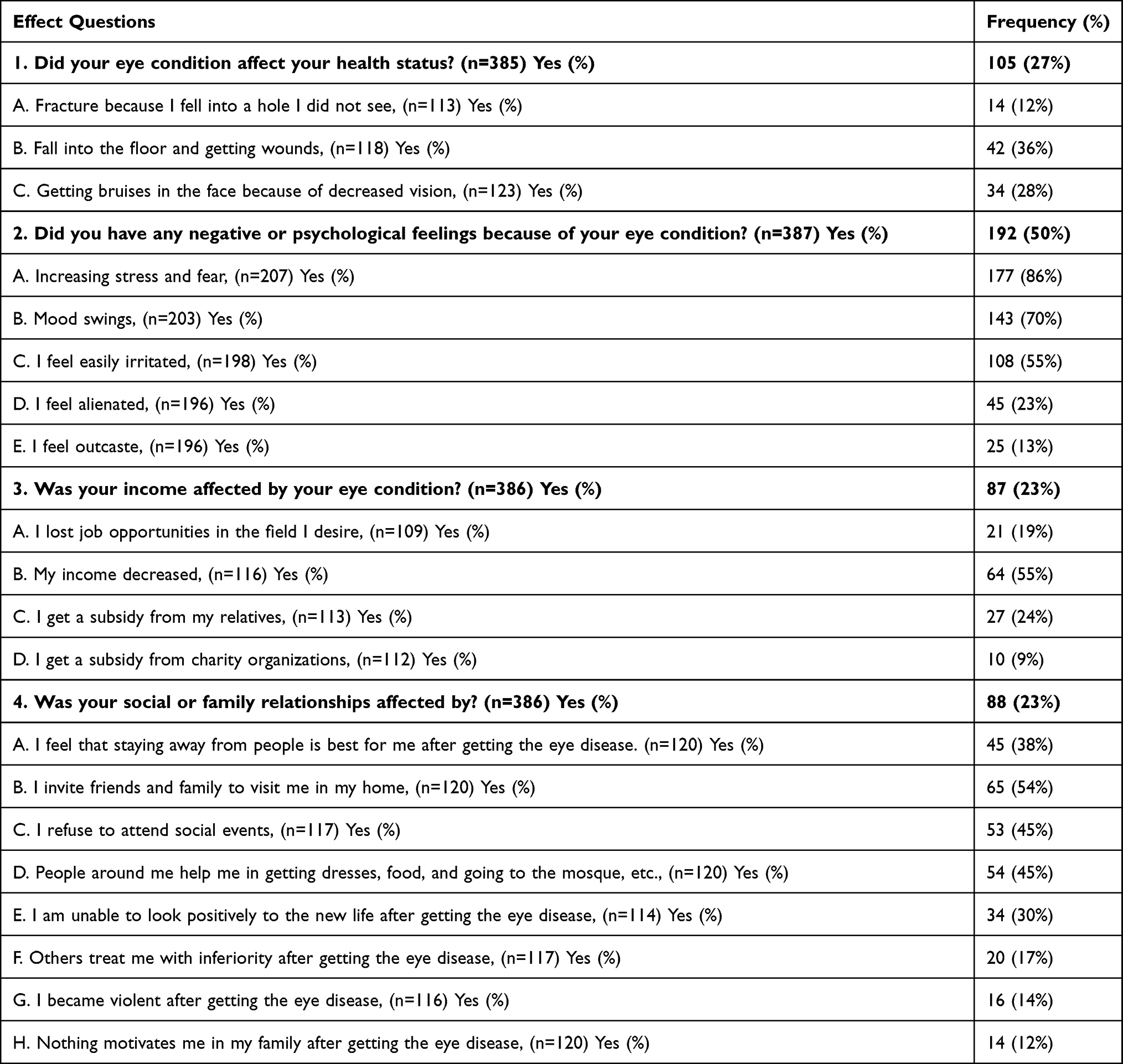 |
Table 3 Health Status, Psychological, Financial, and Social Effects |
Table 4 displays the awareness and suggestions of patients regarding late detection of eye conditions highlighting the patients perspectives concerning awareness of the current initiatives and recommendations for identifying cases earlier to mitigate the associated effects (Question [#4 in Figure 1]).
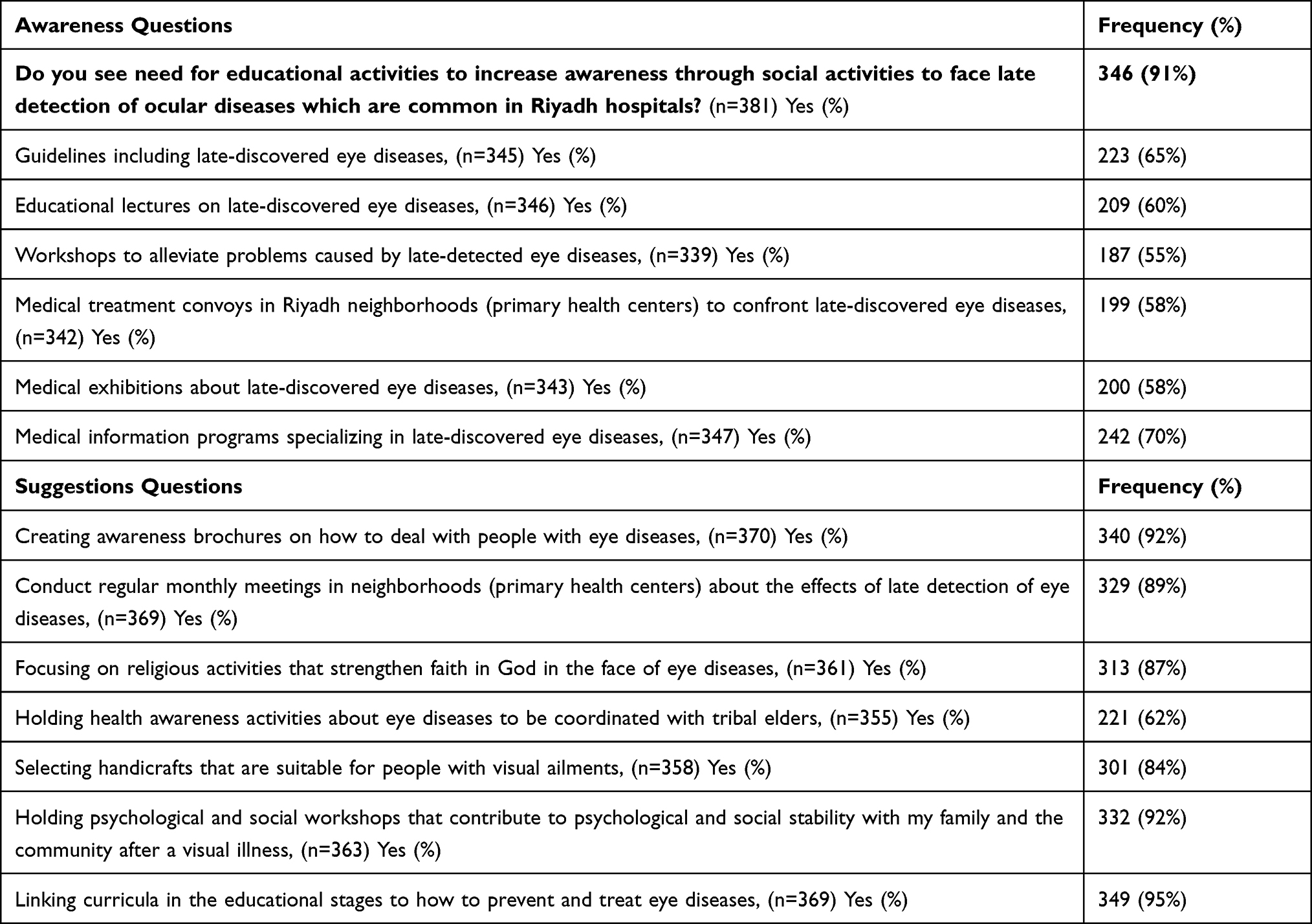 |
Table 4 Awareness and Suggestions Responses |
Logistic regression analysis (Table 5) was conducted to investigate the relationship between the psychological, financial, social and health status effects and the patient’s perspective on having ocular disease detected in late stage. The results revealed that patients who had felt having an advanced condition due to the late detection were influenced by their health, financial, and social status (p < 0.05). However, the psychological feelings were on the borderline (p=0.0544) because the two groups were influenced almost equally (54% and 46%) as depicted in Figure 2.
 |
Table 5 Logistic Regression Analysis to Investigate the Relationship Between the Psychological, Financial, Social and Health Status Effects and the Patient’s Perspectives on Having Ocular Disease Detected in Late Stage |
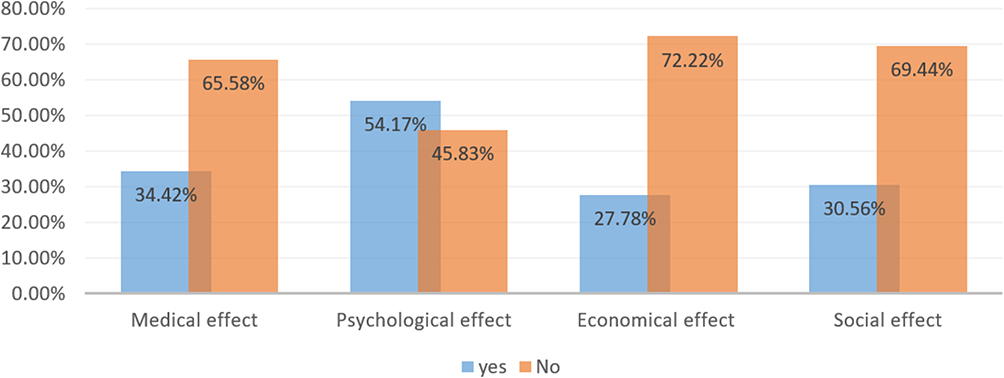 |
Figure 2 A comparison of the health status, psychological, financial, and social impacts of individuals with patients perspective of having advanced eye disease (who answered “Yes” to the question, “Do you have an advanced eye disease? Detected in an advanced stage?”) and those without eye disease (who answered “No”). |
Finally, the multivariate logistic regression analysis between education, age, income, and health care provider (hospital) with health status, psychological, financial, and social effects are shown in Table 6. The results revealed a strong age correlation with health status effect and physiological impact. Patients aged ≤ 50 years were more likely to be affected than those aged > 50 years were (reference set in multivariate logistic regression analysis test as (> 50 years)). The individual income level was significantly associated with the health status, psychological, and financial affected individuals, whereas patients with incomes of more than 10,000 SAR (1 SAR = 0.266 USD) were less likely to be affected (reference set in multivariate logistic regression analysis test as (< 5000 SAR)). Additionally, we found that patients who visited private hospitals were more likely to experience health status, psychological, financial, and social effects (p < 0.05) (reference set in multivariate logistic regression analysis test as (patients who visited governmental hospitals)).
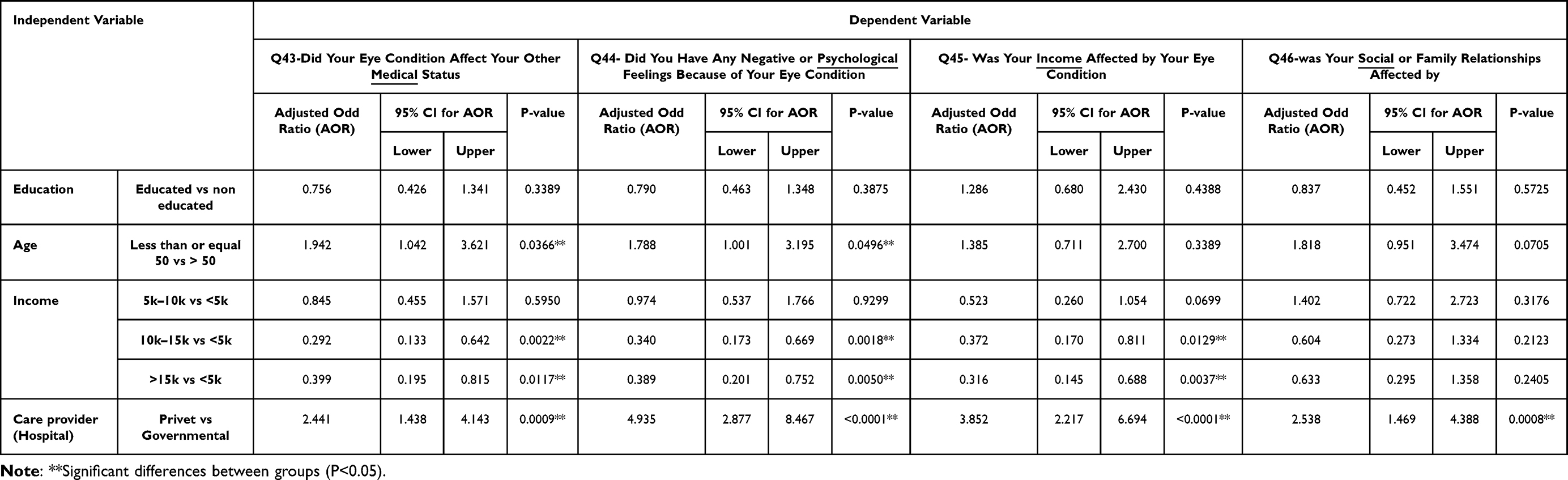 |
Table 6 Multivariate Logistic Regression Analysis Between Education, Age, Income and Health Care Provider (Hospital) with Medical, Psychological, Financial and Social Effects |
Discussion
This study presents the QoL of patients detected with late-onset ocular diseases. Earlier research has often explored the relationship between VI and a single risk factor, such as psychological effects, focusing on specific aspects of patients’ general QoL. However, only a limited number of studies have delved into the broader impact of the late detection of irreversible ocular diseases on QoL. Such insights hold promise for future decision making, leading to improved healthcare and patient experiences by fostering effective communication between patients and healthcare professionals. Furthermore, our results point to the demand for more comprehensive rehabilitative interventions and educational activities. These could encompass initiatives such as awareness brochures, psychological and social workshops, and integrating ocular disease prevention and treatment content into the educational curricula.
Once an eye disease becomes visually impaired, significant disability is associated with direct (medical care) and indirect (productivity loss) financial costs to individuals and society. Notably, the most pronounced impact in our study was the psychological toll, characterized by stress and fear, followed by mood swings, which emerged as a primary concern. These findings align with those of previous research.30,31 Patients with VI exhibit twice the rates of depression and anxiety than do non-VI patients, as studied in the context of depressive and anxiety symptoms among older adults with vision impairment.30 Additionally, psychological distress is notably higher among adults with VI than among those with normal vision.31 Such outcomes could be attributed to the challenges they encounter when performing visual tasks,32 which gradually intensifies their psychological distress and apprehension about vision loss. These findings interpret the notable responses in our study for the psychological effect for the patients’ responses to not having the advance condition due to the late detection.
Another dimension explored in this study pertains to the effect of health status. Our results underscore that falls and injuries due to reduced vision were the major concerns among our patients. This could be attributed to the fact that our participants were patients who visited glaucoma and retinal clinics. Consequently, most patients exhibited reduced visual acuity and/or impaired visual fields owing to conditions such as glaucoma, AMD, and DR. Wood et al33,34 found associations between impaired visual fields, reduced visual acuity, poor contrast sensitivity, and an increased risk of falls. Moreover, adults with impaired vision are twice as likely to experience falls and resultant injuries as individuals without vision loss.35
While the social and economic impacts reported in our study were less pronounced than the preceding effects, prior research has indicated that individuals with VI are more likely to be at greater risk of social isolation.36 In addition, they have lower educational attainment and employment opportunities than individuals without disabilities.37 Köberlein et al38 found that the time spent by family members or assistants caring for persons who have lost their vision increases substantially as vision decreases. Hassell et al39, found a statistically significant restriction in leisure and work, social and consumer interaction, and household and personal care difficulties in patients with moderate and severe visual impairment. A correlational and intervention study indicated that family members could influence how both adults and children manage their social lives amidst diseases and illnesses.40 In Saudi Arabia, the family plays a pivotal role; society is deeply rooted in a culture of mutual assistance and familial support.41 Additionally, in 2016, the establishment of a Family Affairs Council42 in Saudi Arabia aligned with the ambitious goals of Vision 2030. The council’s purpose is to enhance services that contribute to family stability. These contextual factors account for the discrepancies in our findings of diminished social effects among patients with advanced ocular diseases in comparison to prior research.
Regarding the economic aspect, the observed reduced impact was anticipated, considering that 80% of the healthcare system in Saudi Arabia is publicly funded, with only 20% of the healthcare services provided by the private sector.43,44 Moreover, the majority of patients receiving treatment at governmental hospitals where they were not subject to any health service fees. However, financial costs caused by VI, the estimated global annual cost of productivity losses due to VI were 410.7$ billion in 2018.22 Gordois et al45 estimated the 2010 global total cost of VI at 3$ trillion, of which 2.3$ trillion were direct costs. The estimated United States population’s financial burden of VI was 134.2$ billion (direct costs were 98.7$ billion, and indirect costs were 35.5$ billion) in 2017. Rein DB et al found that the annual VI cost per patient in the United States was 16,838$.46 Hence, these costs exert an impact on national healthcare expenditures, the associated financial burdens, and the financial resources of individuals and their families, particularly those with lower incomes. Our findings indicate that patients with lower incomes are more vulnerable to these effects than those with higher incomes.
Another noteworthy discovery from our study was the pronounced response emphasizing the necessity for educational initiatives aimed at increasing awareness through social engagement in addressing the advanced detection of eye diseases. This indicates a diminished level of awareness among the population, consistent with the findings of other studies.47,48 Consequently, education campaigns that enhance knowledge, awareness, and early detection can mitigate the progression of VI and safeguard QoL.
Limitations and Future Work
The data were collected at the beginning of COVID-19. Therefore, the consequent COVID-19 quarantine and restrictions led to a delay of 7–8 months as a result of the hospital’s refusal to allow any patient contact for research and data collection purposes. Even after permission to resume data collection was granted, the number of patients visiting the retina and glaucoma clinics was minimal. The questionnaire was the final step for patients visiting glaucoma and retina clinics; therefore, they were typically tired from lengthy waits, numerous examinations, and intervention procedures such as lasers, injections, and dilation. The examination times are much longer in government hospitals than in other sectors because patients are attended to by interns and residents. The patients’ level of understanding and information delivery was prolonged because the majority were above the age of 50. As a result, the explanation of the questionnaire and answering the questions take at least 15 minutes.
To extend the study outcomes, a questionnaire can be distributed in the future for the patients visiting the eye clinics at primary and secondary healthcare centers, then the findings for both questionnaires are analyzed to emphasize the late detection impact. Moreover, clinical examinations such as visual acuity and slit lamp tests can be incorporated in the analysis for further findings.
Conclusion
The study was conducted in Riyadh particularly within three governmental tertiary hospitals and one private eye clinic, to ensure a diverse range of patients’ feedback. Patients were drawn from various regions encompassing both urban and non-urban areas. This study focused on patients attending subspecialty eye clinics for specialized eye care. A questionnaire, designed by a social planning professor and eye healthcare professionals, was distributed to our participating patients to facilitate self-reporting. The study’s findings indicated that 27% and 50% of patients experienced health status and psychological effects, respectively. Additionally, a significant relationship emerged between financial, social, and health status effects among patients felt having ocular diseases detected in late stages. The study’s conclusion underscored that over 90% of the patients expressed a strong desire to enhance their awareness of the early detection of ocular diseases at late stage.
Anticipating an increase in such cases over time, hence the financial implications of late detection ripple into governmental expenses aimed at covering treatment and care for these patients. It is important to note that Saudi Arabia lacks approved screening program protocols endorsed by the Ministry of Health, the regulator organization. However, manpower is not a constraint considering the presence of trained technicians, nurses, optometrists, and ophthalmologists.49
Consequently, primary healthcare centers situated in villages, small towns, and larger cities across various neighborhoods present accessible avenues for improving eye care services in Saudi Arabia and preventing the late detection of eye diseases. Additionally, optical shops constitute another essential channel, given that trained optometrists play a pivotal role in providing primary eye care in developed countries such as the USA and the UK.50–52 Moreover, advanced technologies such as artificial intelligence approaches based on ocular images offer further potential solutions.
Abbreviations
AMD, Age Related Macular Degeneration; DR, Diabetic Retinopathy IRB, Institutional Review Board; KAMC, King Abdulaziz Medical City; QoL, Quality of Life; VI, Visual Impermanent.
Ethics Approval and Consent to Participate
This study was approved by the ethical committee of the King Abdullah International Medical Research Center and authorized by Institutional Review Board (IRB) number RC20/007/R. The study was adhered to the rules of the Declaration of Helsinki for research involving human participants. A consent form was introduced to the patients, with a full explanation of the study aims and the contents of the questionnaire.
Consent for Publication
The manuscript is approved by all authors for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no financial relationship relevant to this submitted work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Felce D, Perry J. Quality of life: its definition and measurement. Res Dev Disabil. 1995;16(1):51–74. doi:10.1016/0891-4222(94)00028-8
2. Kaplan RM, Ries AL. Quality of life: concept and definition. COPD. J Chronic Obstr Pulm Dis. 2007;4(3):263–271. doi:10.1080/15412550701480356
3. Kamelska AM, Mazurek K. The assessment of the quality of life in visually impaired people with different level of physical activity. Phys Cult Sport. 2015;67(1):31–41. doi:10.1515/pcssr-2015-0001
4. World Health Organization. WHOQOL: Measuring quality of life. Available from: https://www.who.int/tools/whoqol.
5. Gupta P, Fenwick EK, Man RE, et al. Different impact of early and late stages irreversible eye diseases on vision-specific quality of life domains. Sci Rep. 2022;12(1):1–11. doi:10.1038/s41598-022-12425-9
6. Schwartz R, Loewenstein A. Early detection of age related macular degeneration: current status. International. J Retin Vitr. 2015;1(1):1–8.
7. World Health Organization. Blindness and vision impairment; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment#:~:text=Globally%2C%20at%20least%202.2%20billion,has%20yet%20to%20be%20addressed.
8. Wittenborn JS, Zhang X, Feagan CW, Crouse WL, Shrestha S, Kemper AR, Vision Cost-Effectiveness Study Group. The economic burden of vision loss and eye disorders among the United States population younger than 40 years. Ophthalmology. 2013;120(9):1728–1735. doi:10.1016/j.ophtha.2013.01.068
9. Vision Health Initiative (VHI). Economic studies. Available from: https://www.cdc.gov/visionhealth/projects/economic_studies.htm.
10. Shih V, Parekh M, Multani JK, et al. Clinical and economic burden of glaucoma by disease severity: a United States claims-based analysis. Ophthalmol Glaucoma. 2021;4(5):490–503. doi:10.1016/j.ogla.2020.12.007
11. Lan YW, Henson DB, Kwartz AJ. The correlation between optic nerve head topographic measurements, peripapillary nerve fibre layer thickness, and visual field indices in glaucoma. Br J Ophthalmol. 2003;87(9):1135–1141. doi:10.1136/bjo.87.9.1135
12. Flores R, Carneiro Â, Vieira M, Tenreiro S, Seabra MC. Age-related macular degeneration: pathophysiology, management, and future perspectives. Ophthalmologica. 2021;244(6):495–511. doi:10.1159/000517520
13. Endo H, Kase S, Tanaka H, et al. Factors based on optical coherence tomography correlated with vision impairment in diabetic patients. Sci Rep. 2021;11(1):3004. doi:10.1038/s41598-021-82334-w
14. Burton MJ, Ramke J, Marques AP, et al. The Lancet global health commission on global eye health: vision beyond 2020. Lancet Glob Health. 2021;9(4):e489–551. doi:10.1016/S2214-109X(20)30488-5
15. Cheng HC, Guo CY, Chen MJ, Ko YC, Huang N, Liu CJ. Patient-reported vision-related quality of life differences between superior and inferior hemifield visual field defects in primary open-angle glaucoma. JAMA Ophthalmol. 2015;133(3):269–275. doi:10.1001/jamaophthalmol.2014.4908
16. Chai Y, Shao Y, Lin Y, et al. Vision-related quality of life and emotional impact in children with strabismus: a prospective study. Journal of International Medical Research. 2009;37(4):1108–1114. doi:10.1177/147323000903700415
17. Rovner BW, Casten RJ, Tasman WS. Effect of depression on vision function in age-related macular degeneration. Arch Ophthalmol. 2002;120(8):1041–1044. doi:10.1001/archopht.120.8.1041
18. Devenney R, O’Neill S. The experience of diabetic retinopathy: a qualitative. Stud Br J Health Psychol. 2011;16(4):707–721. doi:10.1111/j.2044-8287.2010.02008.x
19. Klauke S, Sondocie C, Fine I. The impact of low vision on social function: the potential importance of lost visual social cues. J Optom. 2023;16(1):3–11. doi:10.1016/j.optom.2022.03.003
20. Swenor BK, Simonsick EM, Ferrucci L, Newman AB, Rubin S, Wilson V. Health, aging and body composition study. Visual impairment and incident mobility limitations: the health, aging and body composition study. J Am Geriatr Soc. 2015;63(1):46–54. doi:10.1111/jgs.13183
21. Lopez D, McCaul KA, Hankey GJ, et al. Falls, injuries from falls, health related quality of life and mortality in older adults with vision and hearing impairment—is there a gender difference? Maturitas. 2011;9(4):359–364. doi:10.1016/j.maturitas.2011.05.006
22. Marques AP, Ramke J, Cairns J, et al. Global economic productivity losses from vision impairment and blindness. EClinicalMedicine. 2021;35:100852. doi:10.1016/j.eclinm.2021.100852
23. Lafuma A, Brézin A, Lopatriello S, et al. Evaluation of non-medical costs associated with visual impairment in four European countries, France, Italy, Germany and the UK. Pharmacoeconomics. 2006;24:193–205.
24. Riva I, Legramandi L, Rulli E, et al. Vision-related quality of life and symptom perception change over time in newly-diagnosed primary open angle glaucoma patients. Sci Rep. 2019;9(1):6735. doi:10.1038/s41598-019-43203-9
25. Assi L, Chamseddine F, Ibrahim P, et al. A global assessment of eye health and quality of life: a systematic review of systematic reviews. JAMA Ophthalmol. 2021;139(5):526–541. doi:10.1001/jamaophthalmol.2021.0146
26. Haddad MF, Bakkar MM, Abdo N. Public awareness of common eye diseases in Jordan. BMC Ophthalmol. 2017;17(1):1–7. doi:10.1186/s12886-017-0575-3
27. Bressler NM, Varma R, Doan QV, et al. Underuse of the health care system by persons with diabetes mellitus and diabetic macular edema in the United States. JAMA Ophthalmol. 2014;132(2):168–173. doi:10.1001/jamaophthalmol.2013.6426
28. Surrati AM, Almuwarraee SM, Mohammad RA, et al. Parents’ awareness and perception of children’s eye diseases in Madinah, Saudi Arabia: a cross-sectional study. Cureus. 2022;14(2):e22604. doi:10.7759/cureus.22604
29. Ebeigbe JA, Emedike CM. Parents’ awareness and perception of children’s eye diseases in Nigeria. J Optom. 2017;10(2):104–110. doi:10.1016/j.optom.2016.06.001
30. Heesterbeek TJ, van der Aa HP, van Rens GH, et al. The incidence and predictors of depressive and anxiety symptoms in older adults with vision impairment: a longitudinal prospective cohort study. Ophthalmic Physiol Opt. 2017;37(4):385–398. doi:10.1111/opo.12388
31. Munaw MB, Tegegn MT, Wang J. Visual impairment and psychological distress among adults attending the University of Gondar tertiary eye care and training center, Northwest Ethiopia: a comparative cross-sectional study. PLoS One. 2022;17(2):e0264113. doi:10.1371/journal.pone.0264113
32. Janz NK, Wren PA, Guire KE, et al. Fear of blindness in the collaborative initial glaucoma treatment study: patterns and correlates over time. Ophthalmology. 2007;114(12):2213–2220. doi:10.1016/j.ophtha.2007.02.014
33. Wood JM, Lacherez P, Black AA, Cole MH, Boon MY, Kerr GK. Risk of falls, injurious falls, and other injuries resulting from visual impairment among older adults with age-related macular degeneration. Invest Ophthalmol Vis Sci. 2011;52(8):5088–5092. doi:10.1167/iovs.10-6644
34. Black AA, Wood JM, Lovie-Kitchin JE. Inferior field loss increases rate of falls in older adults with glaucoma. Optom Vis Sci. 2011;88(11):1275–1282.
35. Jian-Yu E, Mihailovic A, Schrack JA, et al. Characterizing longitudinal changes in physical activity and fear of falling after falls in glaucoma. J Am Geriatr Soc. 2021;69(5):1249–1256. doi:10.1111/jgs.17014
36. Brunes A, Hansen B, M HT. Loneliness among adults with visual impairment: prevalence, associated factors, and relationship to life satisfaction. Health Qual Life Outcomes. 2019;17(1):1–7. doi:10.1186/s12955-019-1096-y
37. McDonnall MC, Tatch A. Educational attainment and employment for individuals with visual impairments. J Vis Impair Blind. 2021;115(2):152–159. doi:10.1177/0145482X211000963
38. Köberlein J, Beifus K, Schaffert C, Finger RP. The economic burden of visual impairment and blindness: a systematic review. BMJ Open. 2013;3(11):e003471. doi:10.1136/bmjopen-2013-003471
39. Hassell J B. (2006). Impact of age related macular degeneration on quality of life. British Journal of Ophthalmology, 90(5), 593–596. 10.1136/bjo.2005.086595
40. Martire LM, Helgeson VS. Close relationships and the management of chronic illness. Assoc Interv Am Psychol. 2017;72(6):601–612. doi:10.1037/amp0000066
41. Saudi Arabian Culture. Family structure, culture alatlas; 2022. Available from: https://culturalatlas.sbs.com.au/saudi-arabian-culture/saudi-arabian-culture-family.
42. Family Affair Council. Unified national platform. Available from: https://www.my.gov.sa/wps/portal/snp/agencies/agencyDetails/AC600/!ut/p/z0/04_Sj9CPykssy0xPLMnMz0vMAfIjo8zivQIsTAwdDQz9LQwNzQwCnS0tXPwMvYwNDAz0g1Pz9L30o_ArAppiVOTr7JuuH1WQWJKhm5mXlq8f4ehsBpQryHYPBwBL-O7t/.
43. Khattab E, Sabbagh A, Aljerian N, et al. Emergency medicine in Saudi Arabia: a century of progress and a bright vision for the future. International. J Emer Med. 2019;12:1–8.
44. Health Care In The Kingdom of Saud Arabia. Unified national platform. Available from: https://www.my.gov.sa/wps/portal/snp/aboutksa/HealthCareInKSA/?lang=en.
45. Gordois A, Cutler H, Pezzullo L, et al. An estimation of the worldwide economic and health burden of visual impairment. Glob Public Health. 2012;7(5):465–481. doi:10.1080/17441692.2011.634815
46. Rein DB, Wittenborn JS, Zhang P, et al. The economic burden of vision loss and blindness in the United States. Ophthalmology. 2022;129(4):369–378. doi:10.1016/j.ophtha.2021.09.010
47. Pan CW, Wang S, Qian DJ, Xu C, Song E. Prevalence, awareness, and risk factors of diabetic retinopathy among adults with known type 2 diabetes mellitus in an urban community in China. Ophthalmic Epidemiol. 2017;24(3):188–194. doi:10.1080/09286586.2016.1264612
48. Al-Lahim WA, Al-Ghofaili RS, Mirghani H, ALBalawi H. Evaluation of awareness and attitudes towards common eye diseases among the general population of Northwestern Saudi Arabia. Egypt J Hosp Med. 2018;70(11):1983–1989. doi:10.21608/ejhm.2018.9403
49. Alotaibi A. Optometry services in Saudi Arabia. Glob J Health Sci. 2017;9(8):91–98. doi:10.5539/gjhs.v9n8p91
50. Optometrist. Health careers. Available from: https://www.healthcareers.nhs.uk/explore-roles/wider-healthcare-team/roles-wider-healthcare-team/clinical-support-staff/optometrist/optometrist.
51. Baker H, Ratnarajan G, Harper RA, Edgar DF, Lawrenson JG. Effectiveness of UK optometric enhanced eye care services: a realist review of the literature. Ophthalmic Physiol Opt. 2016;36(5):545–557. doi:10.1111/opo.12312
52. AOA. What’s a doctor of optometry? Available from: https://www.aoa.org/healthy-eyes/whats-a-doctor-of-optometry.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.