")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 16
The Older Adults’ Intention to Use Silver Diamine Fluoride for Dental Caries Treatment
Authors Nakphu R , Urwannachotima N, Pisarnturakit PP
Received 18 December 2023
Accepted for publication 19 March 2024
Published 3 April 2024 Volume 2024:16 Pages 61—73
DOI https://doi.org/10.2147/CCIDE.S445454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Ratchawipa Nakphu,1 Nipaporn Urwannachotima,2 Pagaporn Pantuwadee Pisarnturakit2
1Geriatric Dentistry and Special Patients Care Program, Faculty of Dentistry, Chulalongkorn University, Bangkok, Thailand; 2Department of Community Dentistry, Faculty of Dentistry, Chulalongkorn University, Bangkok, Thailand
Correspondence: Pagaporn Pantuwadee Pisarnturakit, Department of Community Dentistry, Faculty of Dentistry, Chulalongkorn University, 34 Henry Dunant Road, Patumwan, Bangkok, 10330, Thailand, Tel/Fax +662 218 8545, Email [email protected]
Purpose: This study aimed to determine the intention of older adults to use silver diamine fluoride (SDF) for treating tooth decay.
Patients and Methods: A group of Thai-speaking individuals between the ages of 60 and 90 were asked to participate in the study. They were provided with information about SDF and then asked to complete a questionnaire based on the Theory of Reason Action (TRA). The questionnaire consisted of 23 questions divided into seven constructs aimed at determining the determinants of the intention to use SDF. These constructs were behavioral belief, evaluation of behavioral outcome, normative belief, motivation to comply, attitude towards behavior, subjective norm, and intention. The responses were rated on a 4-point Likert scale ranging from 1 (Strongly disagree) to 4 (Strongly agree). The characteristics and TRA scores of the participants were analyzed and compared based on their intention to use SDF, using the Chi-square test and t-test. Multiple logistic regression was employed to determine the determinants of the intention to use SDF.
Results: The study involved 588 participants, with an average age of 65.3 years (SD= 5.53). Of the participants, 52.7% were women, 58.1% were unemployed or retired, 80.8% lived with family, 63.4% had less than sixth-grade education, 62.9% had a monthly family income of less than 10,000 baht, and 63.6% had underlying diseases. The study found that 82.7% of the participants intended to use SDF for dental caries treatment, with an average score of 2.86 out of 4. The study also found that age, family income, underlying diseases, dental health problems, and fear of the dentist significantly affected their intention. Behavioral beliefs and evaluations of behavioral outcomes significantly affected the intention to use SDF treatment.
Conclusion: Most older adults in the study intended to use SDF for dental caries treatment.
Keywords: dental caries, older adults, intention, oral health literacy, silver diamine fluoride, Theory of Reason Action
Introduction
Older adults will likely develop oral health problems in the next few years. Systemic diseases in older adult patients can also complicate their general and oral health.1,2 Tooth decay is a leading cause of tooth loss among older adults. Tooth loss is the most significant negative impact on older adults’ oral health-related quality of life.1–3
Fluoride is an effective tooth decay-preventing substance. Various fluoride applications, such as fluoride varnish or different forms of sodium fluoride, have a topical effect on the tooth surface. Besides invasive procedures, non-invasive treatments such as silver diamine fluoride (SDF), Atraumatic Restorative Treatment (ART), and fluoride varnish are available for caries treatment.3 The primary mechanism of fluoride to prevent tooth decay is promoting remineralization and preventing demineralization of the tooth structure.4,5 SDF is an alternative form of topical fluoride that can arrest the progression of dental caries.
SDF has been proven effective for caries prevention and arrest among children and older adults.6,7 One disadvantage of the SDF treatment is the black staining on the decayed area after SDF treatment. Many studies revealed the acceptance of the staining of SDF treatment in children. The primary and the posterior teeth were more accepted than the permanent and the anterior teeth.7,8 Studies reported that the child’s caregivers admitted the black stain after SDF treatment.8 The parents accepted the staining after SDF treatment in primary and posterior teeth rather than the stain in permanent and anterior teeth because they are less visible and beneficial for uncooperative children.8,9 Many parents prefer SDF treatment to other alternative treatments under general anesthesia.8,9 Indications for SDF application include patients with high caries risk who have active cavitated caries lesions present with behavioral challenges or medical management, patients with multiple cavitated caries lesions that may not all be treated in one visit and have no signs of pulp inflammation or spontaneous pain.5,7,10 The patients should be informed and consent to the SDF treatment before the treatment, emphasizing the expected staining of treated lesions, potential staining on the skin, and clothing.7,11
The Theory of Reason Action (TRA) aims to describe the relationship between attitudes and human behaviors. It predicts how a person will behave based on their attitude and intention. The decision to participate in a specific behavior depends on the individual’s expected outcomes, as derived from previous research in social psychology.12–14 The TRA constructs included behavioral beliefs, evaluations of behavioral outcomes, normative beliefs, motivation to comply, attitude, and subjective norms.12–14 This TRA is suitable to explain the factors related to the intention of a specific behavior.
However, in Thailand, SDF is one method for treating tooth decay among older adults,11,15,16 but it needs to be better known. Recognizing this importance, the researcher aims to fill the knowledge gap. Unfortunately, there are very few studies on SDF treatment among older adults. The black staining on the carious teeth is noticeable, so older adults might have different perceptions of SDF treatment. Thus, this study applied the TRA to explore the decision on SDF treatment among older Thai adults. This study aimed to identify factors associated with the intention to use SDF for dental caries treatment among older adults, including behavioral belief, evaluation of the behavioral outcome, normative beliefs, motivation to comply, attitude, subjective norms, and intention to use SDF treatment.
Materials and Methods
Study Design and Participants
This study is a cross-sectional survey. Patients 60 years or older who could care of themselves and read Thai, attending the Faculty of Dentistry Hospital, Chulalongkorn University, and elders in Nakhon Pathom nursing home community were invited to participate in the study. They were excluded if they are unwilling to participate in the study. Data were collected from January 2022 to June 2022.
The calculated sample size, by G Power 3.1.9.617 was 469 and compensating for estimated 20% incomplete information, the minimum required sample size was 563 participants. The t-test for calculating means: difference from constant (one sample case) were calculated with effect size = 0.15; α = 0.05; and power = 0.90.
Data Collection
Data was collected from January 2022 to June 2022. Information about SDF was provided through electronic posters on the following topics: 1) What is SDF? SDF is a dental treatment used to stop tooth decay. 2) What is the chemical reaction of SDF? The silver ions in SDF stop demineralization, prevent collagen degradation, and have a bactericidal effect. 3) What is the method of use? The steps for SDF application are explained. 4) What is the price? The application charge is covered under Thailand’s Universal Coverage Scheme. 5) What are the advantages and disadvantages of SDF treatment? SDF is easy to use, painless, and inexpensive, but it may leave a black stain. The research team prepared an electronic questionnaire in simple language and with pictures to help older adults understand it better. The researchers accompanied the older adults during the survey to answer any questions they had. Participants were then asked to independently complete the questionnaire, designed based on the Theory of Reasoned Action (TRA), to measure their intention to use SDF treatment. The questionnaire consisted of 23 questions covering seven constructs related to the intention to use SDF treatment. The questionnaire used a 4-point Likert scale, with scores ranging from 1 to 4 (1 = Strongly Disagree, 2 = Disagree, 3 = Agree, and 4 = Strongly Agree). Participants who answered “Strongly disagree” or “Disagree” to the intention question were categorized as “Not intending to use SDF”.
The newly developed questionnaire was evaluated for its construct validity and reliability through exploratory factor analysis (EFA) and Cronbach’s alpha coefficient. The results of EFA revealed that the final factors explained 77.82% of the variance, and the factor loadings of the statements ranged from 0.571 to 1.131 after rotation. The internal consistency of each factor, as indicated by Cronbach’s coefficient, ranged between 0.87 and 0.95.18 Before participating in the study, research participants signed a consent form and were informed about the research study, its aims, methods, data use and storage, voluntary identification, participation, and the right to withdraw from the study.
The study analyzed socio-demographic characteristics such as gender, occupation, highest education level, family income, diseases, daily activity, and pain experience, as well as the TRA construct which includes behavioral belief (BB), evaluation of behavioral outcome (EO), normative belief (NB), motivation to comply (MC), attitudes (AT), subjective norms (SN) and intention to use (I). Additionally, reasons for not intending to use SDF were examined. Descriptive statistics, IBM SPSS Statistics (Version 29, IBM), were used for the analysis. The Chi-square test was used to compare the participants’ characteristics with different intentions, and the score distribution of each TRA question according to different intentions to use SDF was analyzed using the Chi-square test and t-test. Multiple logistic regression was employed to determine the effect of variables on the intention to use SDF.
Results
A total of 588 participants were recruited for the study. They are 60–90 years of age with average 65.3 (5.53) years of age. Most participants (86.1%) were 60–70 years old. The socio-demographic characteristics of participants are shown in Table 1. Half of the participants (52.7%) were female. Most participants (58.1%) were unemployed/retired, most (80.3%) stayed in house-with-family, 63.4% had a Grade 6 education or lower, and 14.1% had a bachelor’s degree or higher. 62.9% of participants had a monthly family income of less than 10,000 Baht (300 US$), 63.6% had underlying diseases, and hypertension is the most frequent underlying disease. Moreover, 80.6% of the participants reported having had dental problems, and 79.9% indicated they feared seeing a dentist (Table 1).
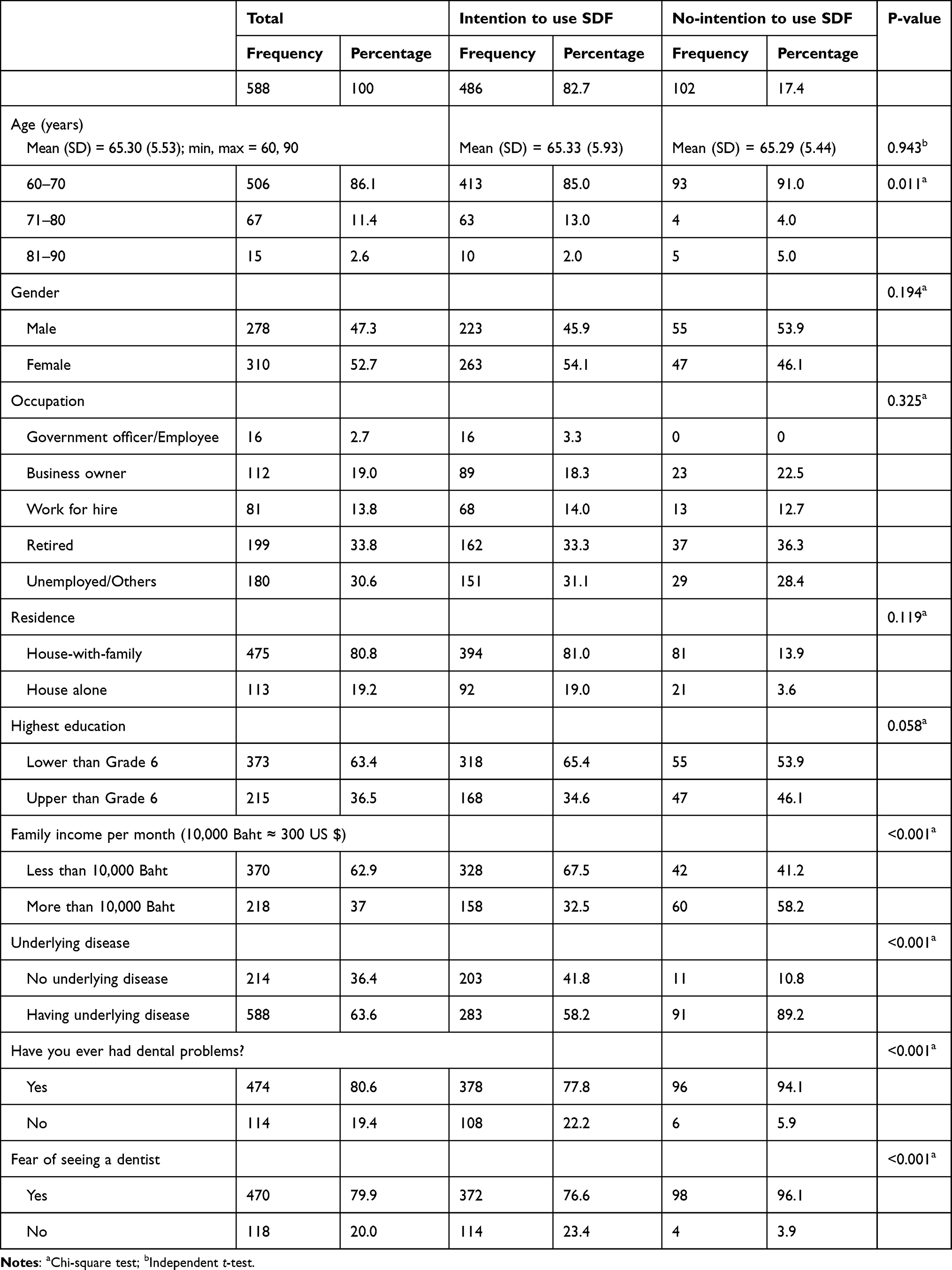 |
Table 1 Sociodemographic Characteristics and Comparisons of Different Intentions to Use SDF Among Different Characteristics |
Four hundred eighty-six participants, which is 82.7% of the total, indicated their intention to use SDF for treating dental caries. The average age of participants who intended to use SDF (65.33 (5.93)) and who did not intend to use SDF (65.29 (5.44)) was not significantly different (t-test, P=0.943). However, a significant difference (P=0.11) was observed in the proportion of participants with different intention to use SDF. Almost all participants (91.0%) who stated no intention to use SDF were 60–70 years of age. The study revealed that age (P=0.011), family income (P<0.001), underlying disease (P<0.001), dental problem (P<0.001), and a fear of seeing a dentist (P<0.001) were the factors associated with the intention to use SDF. Participants who had a monthly family income of less than 10,000 Baht, had an underlying disease, dental problems, and feared seeing a dentist indicated an intention to use SDF.
The average mean (SD) score of the statement number 23, intention to use (I), is 2.86 (0.539) indicating the intention to use SDF. The average mean scores of each TRA variable ranged from 2.20 to 3.02. Most participants (52.7% to 76.7%) indicated they agreed with every statement except for the motivation to comply (MC) statements (statements 15 and 16). The majority of participants (51.9% to 52.6%) disagreed with statements 15 and 16. (Tables 2 and 3).
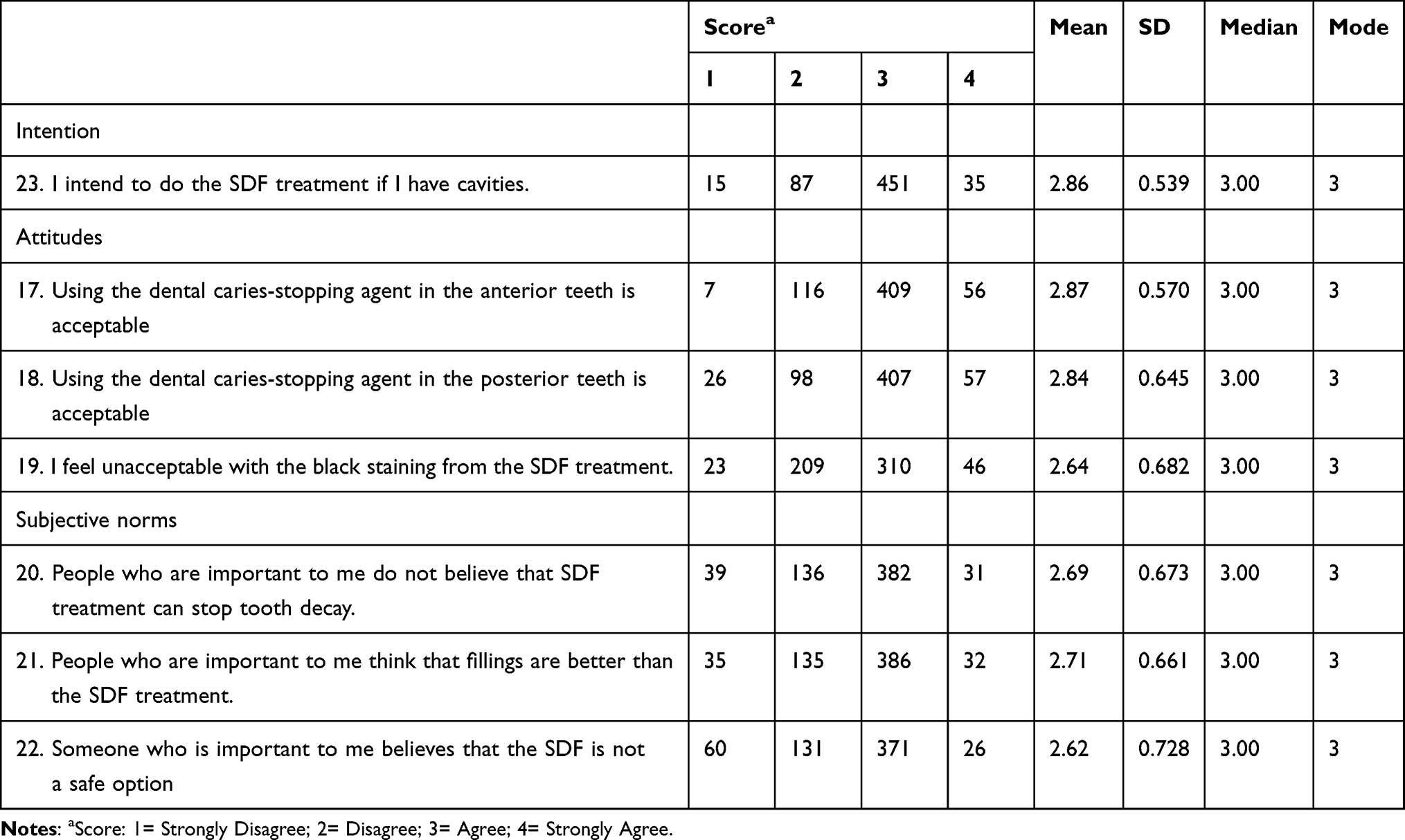 |
Table 2 Score Distribution and Descriptive Statistics of Each TRA Question (Direct Measurement) |
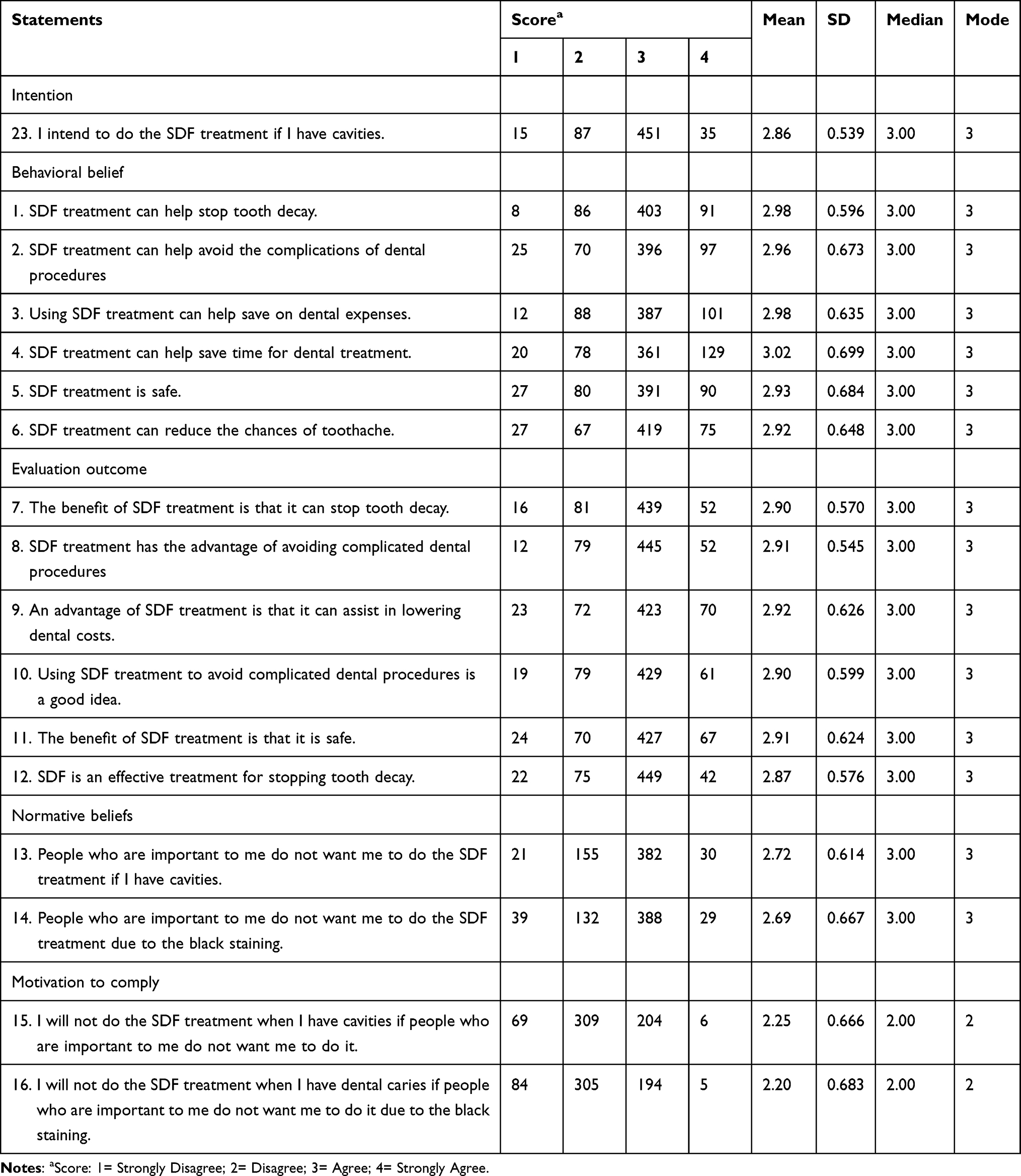 |
Table 3 Score Distribution and Descriptive Statistics of Each TRA Question (Indirect Measurement) |
The average mean scores of each TRA statement among different intention to use SDF were statistically significant different (P<0.001). The difference ranged from 0.37 to 1.32 (data not shown). The MC statements revealed the least different scores (0.37 (Statement 16) and 0.46 (Statement 15)). The distribution of TRA variable scores according to different intentions to use SDF were statistically significantly different (P<0.001) in all statements of TRA variables except motivation to comply, both direct and indirect intention measurements. (Figures 1 and 2) Most participants who intended to use SDF agreed (strongly agree or agree) with TRA statements, while those who did not intend to use SDF disagreed (strongly disagree or disagree) with TRA statements.
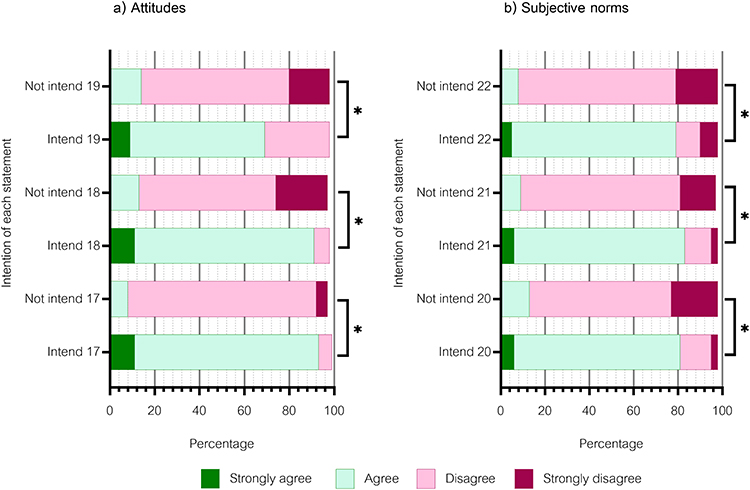 |
Figure 1 The proportion of responses to each statement among participants with different intentions for SDF treatment (Direct measurement); (a) Statements about attitudes towards SDF treatment; (b) Statements about subjective norms related to SDF treatment; *Chi-square test; p-value<0.05. |
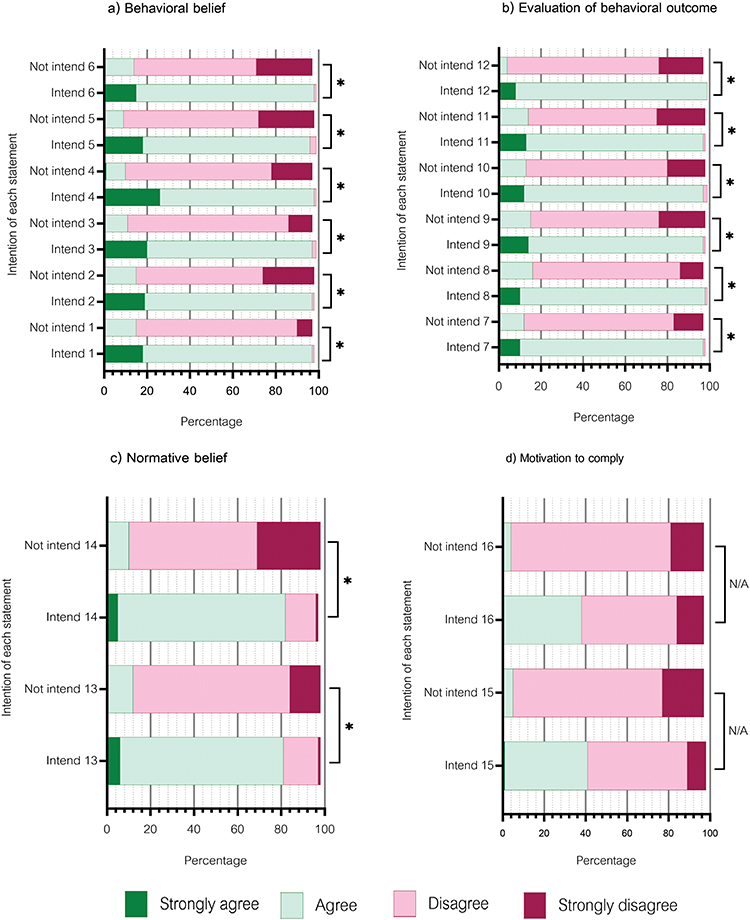 |
Figure 2 The proportion of responses to each statement among participants with varying intentions towards SDF treatment (Indirect measurement); (a) Statements about behavioral beliefs related to SDF treatment; (b) Statements about evaluation of the behavioral outcome of SDF treatment; (c) Statements of normative beliefs related to SDF treatment; (d) Statements about the motivation to comply with SDF treatment; *Chi-square test; p-value<0.05. |
It is noteworthy that despite having different intentions to use SDF, most of the participants disagreed (strongly disagree and disagree) with the MC statements. The study also found that some participants who intend to use SDF disagreed with TRA statements, while some participants who do not intend to use SDF agreed with TRA statements. It is interesting to note that over half of the participants disagreed with the MC statements.
Multivariate Analysis
Table 4 displays the adjusted multivariate models for the intention of older adults to use SDF treatment. When adjusting for the sociodemographic variables only (Model 1), age, income, lack of fear of seeing a dentist, having no dental problem, and having an underlying disease were found to have significant effects on the intention to use SDF treatment. Model 1 is capable of predicting correctly 84.4% with −2 Log likelihood© (−2LL) 430.67, Nagelkerke R Square 0.288. Older adults aged 71–80 years intend to use SDF treatment 3.33 times more often than those aged 60–70 years. Older adults with lower incomes intended to use SDF treatment 4.30 times more often than those with higher incomes. Older adults with no fear of seeing a dentist intended to use SDF treatment 5.23 times more often than those with a fear of seeing a dentist. It was found that older adults with no dental problems were 3.95 times more likely to use SDF treatment than those with dental problems. Similarly, older adults without any underlying disease were 5.12 times more likely to use SDF treatment compare to those with an underlying disease.
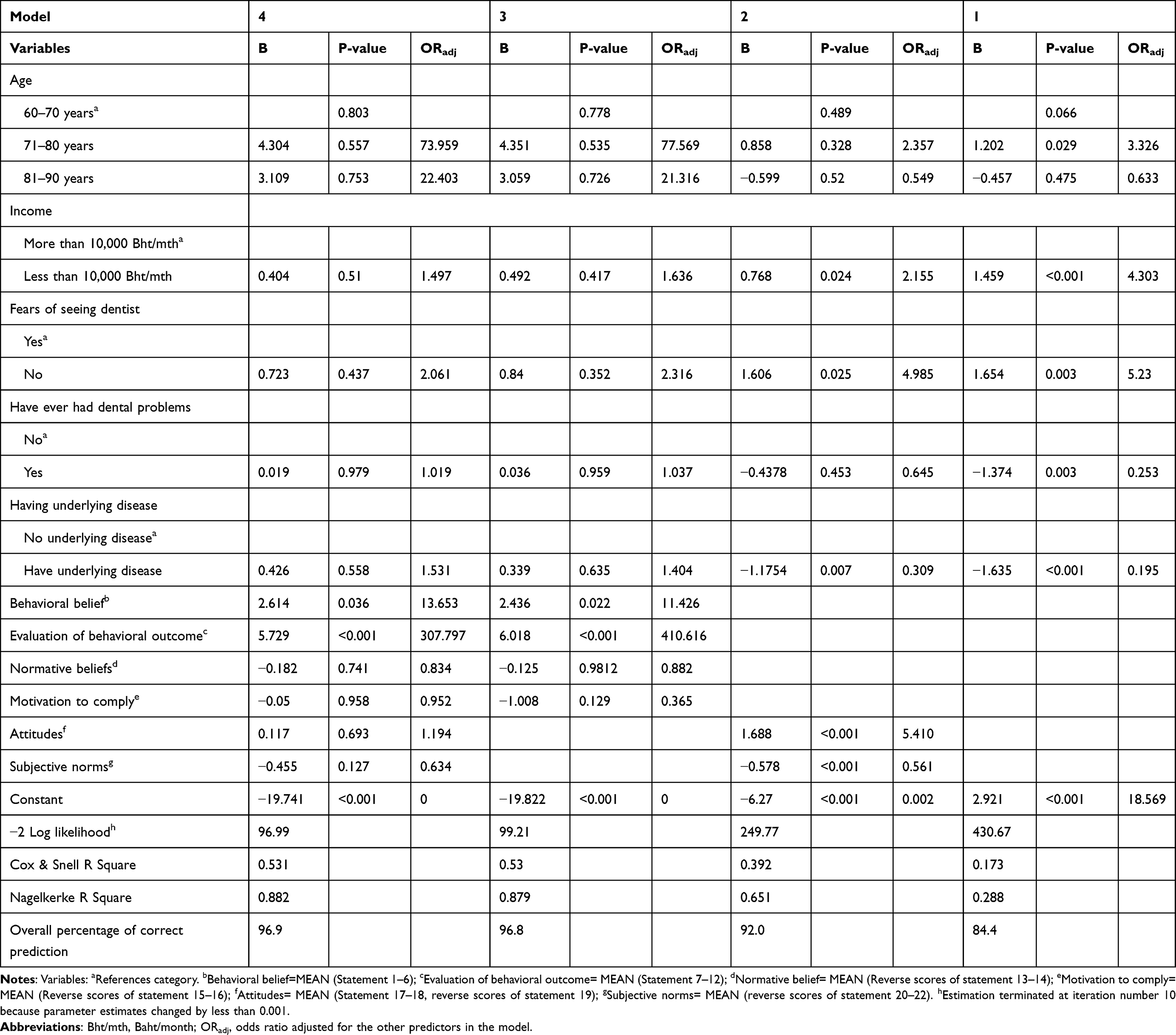 |
Table 4 Multiple Logistic Regression Models of Intention to Use SDF for Dental Caries Treatment by Sociodemographic and TRA Variables |
Adjusting for the direct measurement of TRA variables (AT and SN) and sociodemographic variables (Model 2), it was concluded that income, lack of fear of seeing a dentist, absence of underlying disease, attitudes, and subjective norms were the crucial factors that influenced intention to use SDF treatment. Model 2 was able to predict with 92.0% accuracy with −2LL 249.77, Nagelkerke R Square 0.651. The older adult with a positive attitude toward SDF intended to use SDF treatment 5.410 times more than those with a negative attitude. Interestingly, all the sociodemographic variables become non-significant in the model which was adjusted with indirect measurement of TRA variables (BB, EO, MC, and NB) in Model 3. Model 3 was able to predict with 96.8% accuracy with −2LL 99.21, Nagelkerke R Square 0.879. The significant variables in this model were the behavioral belief and evaluation of behavioral outcome. The evaluation of SDF outcome had a very high impact on the intention to do SDF treatment (Adjusted OR = 410.6). Model 4, which was adjusted with sociodemographic variables, and all TRA variables, indicated only two variables, behavioral belief and evaluation of behavioral outcome, had significant effects on the intention to use SDF treatment. Model 4 was able to predict with 96.9% accuracy, with −2LL 96.99, Nagelkerke R Square 0.882. In conclusion, older adults who have a positive belief towards SDF and a more positive evaluation of SDF treatment are highly likely to use the SDF treatment.
According to the study, out of 102 participants who had no intention of using SDF treatment, the reasons for their reluctance were as follows: SDF is not aesthetically pleasing (16.7%); lack of knowledge about SDF (37.3%); concerns about the safety of SDF (39.2%), belief that SDF cannot effectively stop tooth decay (53.9%); and other reasons (19.6%). (Table 5).
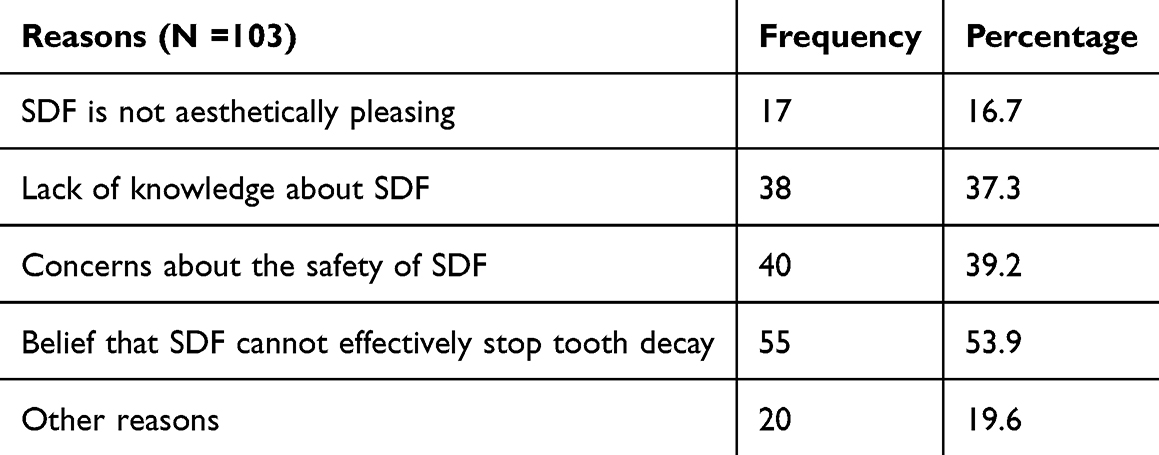 |
Table 5 Reasons for Not Intending to Use SDF. (Only Participants Who Did Not Intend to Use SDF) |
Discussion
According to the results, older adults have varying intentions when it comes to using SDF. Most of them plan to use SDF for dental caries treatment. Interestingly, the average age of participants with different intentions was similar. However, almost all (91%) of the participants who stated no intention to use SDF for dental caries treatment were aged 60–70 years old. This could be due to younger older adults being more active and independent, which allows them to receive extended periods of dental treatments without being hindered by travel constraints. Figures 1 and 2 indicate some participants who intended to use SDF treatment agreed with the negative statements, especially in MC statements. The study participants expressed their determination to use SDF treatment even though they faced opposition from those around them. Despite finding the black staining caused by SDF treatment unacceptable, they still intended to use it. Other factors might affect their intention, such as their socio-economic status, having an underlying disease or fear of seeing a dentist. They might have made this decision because they believed the treatment’s benefits outweighed its drawbacks.
The study highlighted that the participant’s beliefs about the treatment and their evaluation of its outcomes were the most important factors influencing their decision to use SDF. The study’s findings suggest that the participants made informed decisions based on their evaluation of the treatment’s benefits and their beliefs about it.
The analysis of the relationship between sociodemographic variables and the intention to use SDF treatment showed that several factors influence this intention, including age, income, presence of underlying diseases, fear of seeing a dentist, and dental problems. On the other hand, the analysis of the relationship between TRA variables and the intention to use SDF treatment revealed that all TRA variables, except MC statements, play a significant role in shaping this intention. However, the multivariate analysis of the intention to use SDF treatment identified only two determining factors: the BB and EO statements. After taking into account the socio-demographics and all TRA variables, it was found that the evaluation of SDF treatment outcomes (EO) had a greater impact on the intention to use SDF treatment compared to other TRA variables. Participants who scored higher in positive BB and EO statements were more likely to have the intention to use SDF treatment. The best model for predicting the intention to use SDF treatment was model 3 due to its high overall percentage of correct prediction and low −2LL. Therefore, the BB and EO statements are the determinants of intention to use SDF treatment. Increasing awareness of the benefits of SDF for treating dental caries can improve its usage.
According to the study, the use of SDF among older adults is not very common. However, the results indicated that the majority of older adults (76.7%) agreed or strongly agreed (6%) with the statement “I intend to use SDF when I have cavities”, with a mean score of 2.86 (0.54). Only 16% of older adults showed no intention of using SDF to treat dental caries, as they either disagreed (14.8%) or strongly disagreed (2.6%) with the statement. Despite being a relatively new alternative procedure for dental caries treatment, almost all older adults (76.7%) had a positive attitude towards SDF treatment, as evidenced by their intention to use it.
Adhering to regulatory guidelines for treating dental caries is important. Silver diamine fluoride (SDF) treatment has shown to be highly effective, and it is included in the Thai Universal Coverage program’s list for all cases. The intention of patients to undergo SDF treatment depends on their evaluation of the positive outcomes of the treatment. SDF treatment is cost-effective and can save a lot of money compared to more complex treatments. This treatment can greatly benefit older Thai adults because 52.6% of 60–74-year-olds have dental caries, with an average of 1.8 teeth affected per person.19 By choosing SDF treatment, patients can save time and enable dental personnel to provide other necessary treatments to patients in need.
It has been observed that using SDF can be highly beneficial in stopping tooth decay quickly. This treatment not only decrease the time and cost involved in treating dental caries but also be helpful for older adults who would otherwise need to bear the expenses of traveling and out-of-pocket expenses for the same. Additionally, the shortage of dental personnel could be lessened, allowing dental health personnel to provide other necessary dental health services.15 Furthermore, 82% of participants who intended to undergo the SDF treatment considered the benefits of SDF over the black staining of SDF treatment. This consideration of the benefits of SDF is also indicated in the multivariate analysis. Evaluating behavioral outcomes became the most critical factor in deciding to use SDF treatment.
The use of SDF has been established as a highly effective solution for treating dental decay in older adults.20 A study conducted on children has further confirmed the success of this treatment.21 The research revealed that the acceptability of SDF treatment increased as the child required more advanced methods of behavior guidance.21 Parents were also found to accept the pigmentation caused by SDF,21 a common side effect of the treatment. Based on the comparison of the results with another study, it was found that older adults also had similar positive and negative views regarding the SDF treatment. The discoloration caused by SDF was observed to be less of a concern when it was applied to less visible areas. Furthermore, the participants preferred it as it helped them avoid pain or complicated dental procedures, and its discoloration was overcome with the advantage.22 That study also indicated that older adults found SDF treatment to be valuable for people who are immobile or in need of care.22 SDF treatment is a non-invasive and easy-to-perform dental procedure that requires minimal time and budget, making it an excellent option for reducing barriers to dental health services.23,24 Thailand’s universal health coverage covers SDF treatment, but it’s not widely used in the country. Therefore, it’s important to raise awareness about the benefits of SDF treatment. A study shows that people still need to be convinced of its effectiveness, even after receiving additional information about it. Encouraging SDF treatment among older adults will improve their quality of life by reducing tooth loss and saving the time and cost of dental caries treatment.
Limitation
This study is focused on the intention to use SDF treatment, which may not necessarily reflect the actual rates of SDF treatment. However, the results of the study can be used to promote the benefits and safety of SDF and encourage its use for dental caries treatment. A further study that examines short-term and long-term SDF treatment satisfaction would be beneficial to dental health professionals and the elderly, making it more widely used in routine practice. It is also important to acknowledge the potential for unconscious bias when analyzing statements, as there is a trend of most people who agree to use SDF also agree with all the other statements, including negative ones.
Conclusion
After receiving the essential information about the SDF treatment, most Thai older adults indicated an intention to use SDF treatment. Factors influencing different intentions were the belief and evaluation of SDF treatment’s outcomes.
Abbreviations
SDF, Silver diamine fluoride; DMFT, average number of decayed, missing, filled teeth; SD, Standard deviation; TRA, Theory of Reason Action; BB, Behavioral belief; EO, Evaluation of behavioral outcome; NB, Normative belief; MC, Motivation to comply; AB, Attitude towards behaviors; SN, Subjective norm; I, intention.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The research has been conducted following the guidelines in the Declaration of Helsinki. The Faculty of Dentistry’s Committee on Human Research at Chulalongkorn University approved the study (HREC_DCU 2017-084) in accordance with ethical standards. The participants gave written informed consent. Notifying participants of the study’s details before data collection begins is crucial. Participation in the research is voluntary, and the participants were informed that they could withdraw from the study or complete the questionnaire at any time. By filling out the self-administered questionnaire, the participants agreed to participate in the study.
Acknowledgments
The authors would like to gratitude all participants who participated in this study. We also appreciated the support from patients of the faculty of dentistry, Chulalongkorn University and their families, the staff of Geriatric Dentistry and Special Patients Care, friends, family who helped this study achieve its goal successfully.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Grants for research from the Faculty of Dentistry, Chulalongkorn University. The study protocol has undergone peer-review by this funding body. They had no role in the design of this study and will not have any role during its execution, data analyses/interpretation, or decision to submit results.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yi BG, Tao H, Xue DZ, et al. How root caries differs between middle-aged people and the elderly: findings from the 4th National Oral Health Survey of China. Chin J Dent Res. 2018;21(3):221–229. doi:10.3290/j.cjdr.a41078
2. Heasman PA, Ritchie M, Asuni A, et al. Gingival recession and root caries in the ageing population: a critical evaluation of treatments. J Clin Periodontol. 2017;44(18):S178–S193. doi:10.1111/jcpe.12676
3. Hendrik M-L, Vita M, Rodrigo AG. How to Intervene in the root caries process? Systematic review and meta-analyses. Caries Res. 2019;53(6):599–608. doi:10.1159/000501588
4. Marília ARB, Juliano PP, Heitor MH, et al. Mechanisms of action of fluoride for caries control. Monogr Oral Sci. 2011;22:97–114.
5. Fejerskov O, Nyvad B, Kidd E. Dental Caries the Disease and Its Clinical Management. Oxford: Blackwell Munksgaard; 2008:209–231.
6. Nassar S, Mark R, Jeanette M, et al. The use of silver diamine fluoride (SDF) in dental practice. Br Dent J. 2022;228(2):75–81.
7. Jaana G. Silver diamine fluoride may prevent and arrest root caries in older adults. J Evid Based Den Pract. 2019;19(2):186–188. doi:10.1016/j.jebdp.2019.05.009
8. Sara MB, Heba JS, Samer MA, et al. Parental acceptance of the utilization of silver diamine fluoride on their child’s primary and permanent teeth. Patient Preference Adherence. 2019;13:1431–1432.
9. Yasmi OC, Malvin NJ, Dylan SH, et al. Parental perceptions and acceptance of silver diamine fluoride staining. J Am Dent Assoc. 2017;148(7):510–518. doi:10.1016/j.adaj.2017.03.013
10. Buzalaf MAR. Fluoride and the oral environment. Monogr Oral Sci. 2011;22:97–114.
11. Jeremy AH, Hellene E, Peter MM. UCSF protocol for caries arrest using silver diamine fluoride: rationale, indications, and consent. J Calif Dent Assoc. 2016;44(1):16–28. doi:10.1159/000380887
12. Sutton S. Health behaviour: psychosocial theories. In: Smelser NJ, Baltes B, editors. International Encyclopedia of Social and Behavioural Sciences. Oxford: Elsevier; 2001:6499–6506.
13. Joanna H. Introduction to Health Behavior Theory.
14. Glanz K, Rimer BK, Viswanath K. Health Behavior and Health Education: Theory, Research, and Practice.
15. Banloo SLD, Suntaree P. Situation of the Thai Elderly. Foundation of Thai Gerontology Research and Development Institute (TGRI); 2014.
16. Department of Provincial Administration, Ministry of Interior, Department of Older Persons. Elderly statistics; 2019. Available from: http://statbbi.nso.go.th/staticreport/page/sector/en/01.aspx.
17. Franz F, Edgar E, Albert GL, Axel B. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
18. Nakphu R. Intention to Obtain Silver Diamine Fluoride Treatment for Dental Caries Among Elderly [MSD thesis]. Thailand: Faculty of Dentistry, Chulalongkorn University; 2023.
19. Bureau of Dental Public Health Department of Health, Ministry of Public Health. The 8th National Oral Health Survey. Vol. 8. Bangkok: Ministry of Public Health; 2018:39–52.
20. Alice KYC, Manisha T, Chloe MJ, et al. Clinical evidence for professionally applied fluoride therapy to prevent and arrest dental caries in older adults: a systematic review. J Dent. 2022;125:104273. doi:10.1016/j.jdent.2022.104273
21. Marcela BM, Luciana PS, Daniele MF, et al. Aesthetic perception, acceptability and satisfaction in the treatment of caries lesions with silver diamine fluoride: a scoping review. Int J Paediatr Dent. 2019;29(3):257–266. doi:10.1111/ipd.12465
22. Wiebke S, Paul G, Anne M, et al. Older patients’ perception of treating root caries with silver diamine fluoride – a qualitative study based on the Theoretical Domains Framework. J Dent. 2023;130:104408. doi:10.1016/j.jdent.2022.104408
23. Nadia H, Neamit E, Heba NAE, et al. Barriers affecting the utilization of dental health services among community dwelling older adults. Alexandria Sci Nurs J. 2018;20(1):103–118. doi:10.21608/asalexu.2018.207750
24. Shanahan O, Neill D. Barriers to dental attendance in older patients. Irish Med J. 2017;4:548.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.