")
Back to Journals » Lung Cancer: Targets and Therapy » Volume 15
The Nail in the Coffin?: Examining the KEYNOTE-789 Clinical Trial’s Impact
Authors Arter ZL, Nagasaka M
Received 4 October 2023
Accepted for publication 11 January 2024
Published 25 January 2024 Volume 2024:15 Pages 1—8
DOI https://doi.org/10.2147/LCTT.S443099
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Fengying Wu
Zhaohui Liao Arter,1,2 Misako Nagasaka1– 3
1Department of Medicine, Division of Hematology-Oncology, University of California Irvine School of Medicine, Orange, CA, USA; 2Chao Family Comprehensive Cancer Center, Orange, CA, USA; 3Department of Medicine, St. Marianna University School of Medicine, Kawasaki, Japan
Correspondence: Misako Nagasaka, Department of Medicine, Division of Hematology-Oncology, University of California Irvine School of Medicine, Orange, CA, 92602, USA, Email [email protected]
Abstract: Targeted therapies, such as epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs), have revolutionized the treatment landscape for EGFR-mutant non-small cell lung cancer (NSCLC). However, the emergence of resistance to EGFR TKIs especially the third generation TKIs such as osimertinib remains a major clinical challenge. As a broader strategy for combating resistance, several clinical trials have explored the efficacy of immune checkpoint inhibitors (ICIs)+chemotherapy in EGFR-mutated NSCLC. Until now, the ORIENT-31 and IMpower150 trials suggested that ICIs+ chemotherapy may be more effective than chemotherapy alone after failure of EGFR-TKIs (although ORIENT-31 was negative for overall survival [OS] and IMpower150 was a subset analysis, so the study was not powered to detect a difference); however, the CheckMate-722 trial yielded disappointing results. Thus, the results of this global trial KEYNOTE-789 were highly anticipated.
Keywords: EGFR, post-osimertinib, chemo-immunotherapy, targeted therapy
Introduction
NSCLC is a heterogeneous disease with many genetic alterations. Mutations in the EGFR are observed frequently in a subset of NSCLC patients. EGFR exists at the cell surface as a monomer and must dimerize to activate tyrosine kinases (TK). Although the TK activity of EGFR is tightly regulated in normal cells, the genes encoding these receptors may have circumvented their intracellular inhibitory mechanisms in cancer cells. Approximately 15% of NSCLC adenocarcinomas diagnosed in the United States are thought to harbor EGFR TK mutations, which are more prevalent in females and non-smokers. Significantly higher rates of EGFR mutations are observed in Asian populations.1
NSCLCs with specific EGFR mutations, such as exon 19 deletions or exon 21 L858R mutations, are extremely sensitive to EGFR TKIs. NCCN guidelines recommend analyzing the presence or absence of a driver mutation in EGFR to determine whether an EGFR TKI should be used for the initial treatment of a patient with metastatic NSCLC.2
The FLAURA trial was a pivotal clinical trial that played a significant role in shaping the treatment landscape for EGFR-positive NSCLC. The trial focused on evaluating the efficacy and safety of osimertinib, a third-generation EGFR TKI, in comparison to standard first-generation EGFR TKIs (gefitinib or erlotinib) as first-line treatment for patients with advanced EGFR-mutated NSCLC. The trial demonstrated that osimertinib significantly improved progression-free survival (PFS)3 and OS4 when compared to standard EGFR TKIs in this setting. The FLAURA trial’s findings led to the approval of osimertinib as a first-line treatment option for patients with EGFR-mutated NSCLC in various countries around the world.
EGFR Resistance
Nearly all patients who initially respond to an EGFR TKI eventually develop disease progression. The causes of acquired resistance are not fully understood. Here are some of the common mechanisms of TKI resistance in EGFR mutated NSCLC.
A secondary mutation (such as T790M) in EGFR has been linked to acquired resistance to EGFR TKIs of earlier generations. However, osimertinib is now considered the first-line treatment for EGFR-mutant NSCLC in many parts of the world,3,4 which has largely addressed the T790M resistance issue.
Generally speaking, the mechanisms of resistance to osimertinib fall into two categories: a. those involving genetic alterations at the EGFR gene (on-target mechanisms, such as C797S),5 and b. those involving different genetic alterations and activation of other pathways (off-target mechanisms, such as MET amplification, HER2 amplification, PI3K pathway).6
The resistance mechanisms can be heterogeneous, and multiple mechanisms can coexist within the same tumor or even in different metastatic sites within a patient. Different strategies are being explored to overcome or delay resistance in EGFR-mutated NSCLC. Intensifying initial treatment, such as by combining a third-generation EGFR TKI with chemotherapy (FLAURA2)7 or an EGFR-MET bispecific (MARIPOSA),8 could potentially prevent or delay resistance. Another approach is to combat resistance mechanisms directly, which includes targeting any resistance they may develop (for example, if a patient develops a C797S mutation, which confers resistance to osimertinib, a 4th generation EGFR inhibitor might be an option) or by a broader approach, such as chemotherapy, antibody drug conjugates (ADC), or chemotherapy plus immunotherapy (± VEGF inhibitor).
Role for Immune Checkpoint Inhibitors in EGFR Mutated NSCLC
Although ICIs that target the programmed cell death protein-1 (PD-1)/programmed cell death ligand-1 (PD-L1) axis have substantially altered the treatment paradigm for advanced NSCLC, the clinical benefits of these agents are limited in patients with EGFR-mutated NSCLC. It failed to show improved benefit as monotherapy in both first line setting,9,10 or as second or subsequent line.11–13 The trial results of addition of the ICI to platinum-based doublet chemotherapy in nonsquamous NSCLC with EGFR mutation are conflicting (Table 1).
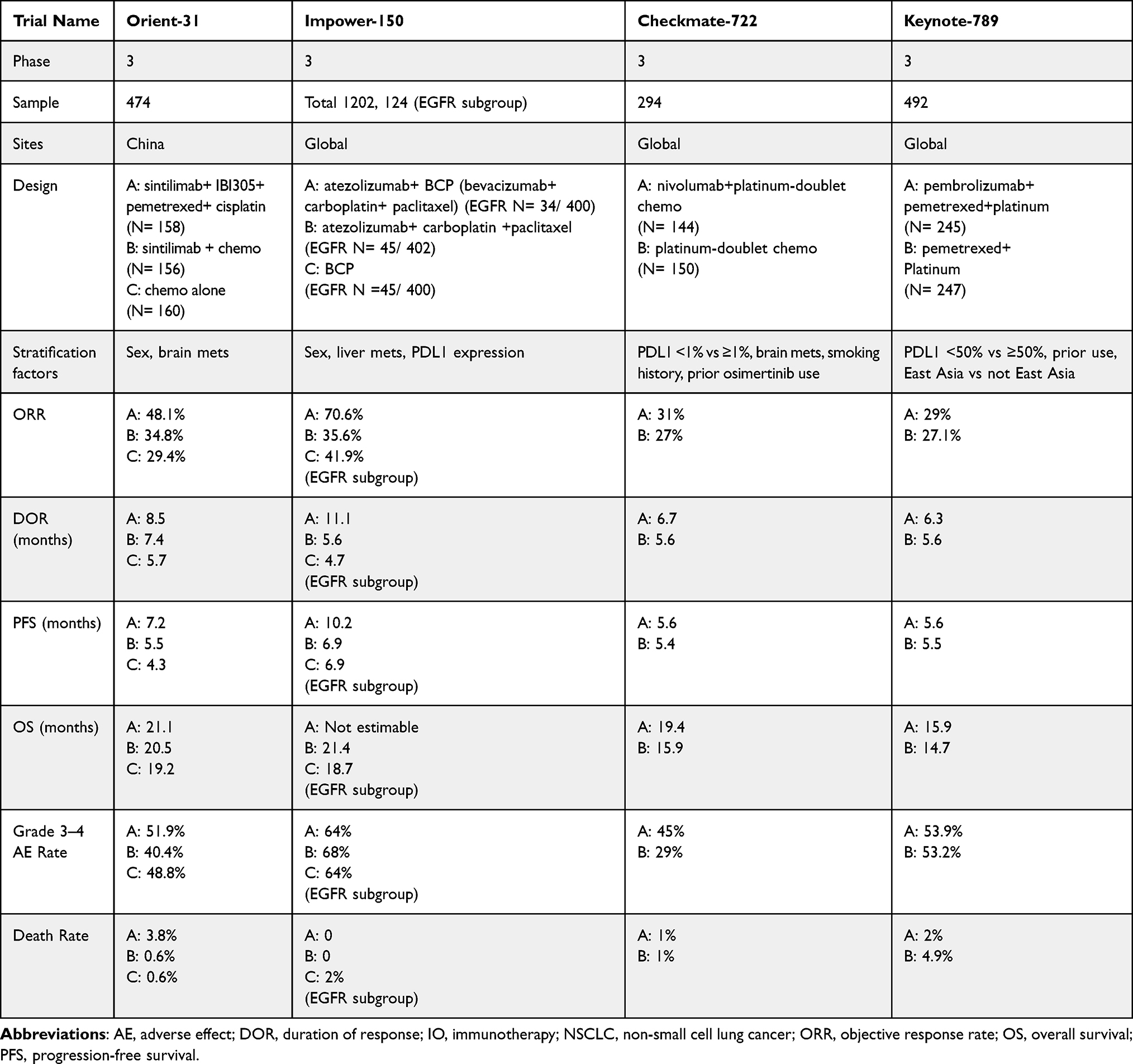 |
Table 1 Efficacy and Safety of IO + Chemotherapy for EGFR Mutated NSCLC in Clinical Trials |
In the IMpower 150 trial, 1202 patients with advanced NSCLC were enrolled.14 In EGFR-positive patients (124 of 1202), OS was not estimable (NE; 95% CI 17.0–NE) with atezolizumab + bevacizumab + carboplatin + paclitaxel (N=34) and 18.7 months (95% CI 13.4–NE) with bevacizumab+ carboplatin+ paclitaxel (N=45; hazard ratio [HR] 0.61 [95% CI 0.29–1.28]).15 However, the study was insufficiently powered to detect difference for the subsets. Similarly, positive results were reported in the ORIENT-31 Phase 3 trial,16 in which patients with EGFR-mutant NSCLC who had progressed on TKI therapy were randomized to sintilimab, an investigational PD1 inhibitor (which has gained certain approvals in China) with IBI305 (bevacizumab biosimilar) plus chemotherapy, to sintilimab plus chemotherapy, or to chemotherapy alone. Significant progression-free survival benefit was sustained with sintilimab plus IBI305 plus chemotherapy compared with chemotherapy alone (median 7.2 months [95% CI 6.6-9.3]; hazard ratio [HR]: 0.51 [0.39-0.67]; two-sided p<0.0001). The median overall survival was 21.1 months (95% CI 17.5-23.9) for sintilimab plus IBI305 plus chemotherapy (HR 0.98 [0.72-1.34]) and 20.5 months (15.8-25.3) for sintilimab plus chemotherapy group (HR 0.97 [0.71-1.32]) versus 19.2 months (15.8-22.4) for chemotherapy alone- and no statistical significance was reached. Also, as ORIENT-31 was conducted exclusively in China, this increased anticipation for the results of a global phase 3 trial devoted to the use of chemotherapy and ICIs in EGFR-mutant NSCLC.
Then, the global phase 3 trial CheckMate-722 was presented.17 The addition of nivolumab to chemotherapy did not demonstrate a substantial benefit, with a median PFS by blinded independent central review (BICR) of 5.6 months in the nivolumab + chemotherapy group versus 5.4 months in the chemotherapy group, with a HR of 0.72 (95% CI: 0.54–0.97), only marginally favoring the chemo-IO in the common sensitizing EGFR mutation group. However, the investigators of CheckMate-722 did note that due to a reduction in sample size in the setting of accrual difficulties with the COVID-19 pandemic, the resulting sample size of 270 left investigators with 83% power to detect a far more challenging HR of 0.692 at an alpha level of 0.05, whereas the initial plan was to study 500 patients providing 90% power to detect a HR of 0.735. With this context in mind, the results of this global trial KEYNOTE-789 were highly anticipated.
Keynote-789
KEYNOTE-789 was a randomized, double-blind phase 3 study.18 It was designed to evaluate the addition of pembrolizumab to platinum-based chemotherapy in patients with TKI-resistant EGFR-mutated nonsquamous NSCLC.
The trial enrolled patients with stage IV nonsquamous NSCLC with EGFR del 19 or L858R mutation who progressed on first- or second-generation EGFR TKI without a T790M mutation; or after a first- or second-generation EGFR TKI with T790M mutation and osimertinib failure as first line therapy regardless of T790M status. A total of 492 patients were randomized 1:1 to 35 cycles of pembrolizumab 200 mg every 3 weeks or placebo plus 4 cycles of pemetrexed and carboplatin or cisplatin every 3 weeks followed by maintenance pembrolizumab. The dual primary endpoint was PFS by BICR and overall survival (OS). The secondary endpoints include objective response rate (ORR), duration of response (DOR) and safety. Of note, with 492 patients, the study had up to 91% power to detect a HR of 0.7 for PFS and up to 86% power to detect a HR of 0.72 for OS.
After a median follow-up of 42.0 months, median PFS was 5.6 months with pembrolizumab plus chemotherapy and 5.5 months with placebo plus chemotherapy (HR 0.80, 95% CI [0.65, 0.97]; P = 0.0122). Median OS was 15.9 months and 14.7 months, respectively (HR 0.84, 95% CI [0.69, 1.02]; P = 0.0362). In both analyses, the p value did not meet the predefined efficacy boundary of P = 0.0117.
The investigators did observe a trend toward a greater benefit with pembrolizumab in the subset of patients with PD-L1 tumor proportion score 1%, but this was not statistically significant. Although the hope was to further investigate whether chemoimmunotherapy would be more beneficial for patients with higher PD-L1 expression, the HR for OS was similar in PD-L1 programmed cell death protein-1 (PD-1)/programmed cell death ligand-1 (PD-L1) tumor proportion score (TPS) ≥50% (HR, 0.84) and TPS <50% groups (HR, 0.85). The ORR was 29.0% with pembrolizumab plus chemotherapy and 27.1% with placebo plus chemotherapy.
As anticipated, immune-related adverse events (AEs) and infusion reactions occurred more frequently with pembrolizumab compared to placebo: Grade ≥3 treatment-related AEs occurred in 43.7% of patients in pembrolizumab + chemotherapy arm and 38.6% in placebo + chemotherapy arm. Grade ≥3 immune-mediated AEs and infusion reactions occurred in 4.5% of patients in the pembrolizumab + chemotherapy arm and 2.0% in the placebo +chemotherapy arm.
In the KEYNOTE-789 study, addition of pembrolizumab to chemotherapy in patients with TKI-resistant, EGFR-mutant, metastatic nonsquamous NSCLC did not significantly prolong PFS and OS in comparison to placebo + chemotherapy.
Discussion
Until now, we had two “positive” trials (IMpower150 and ORIENT-31) and one negative trial of CM-722 for EGFR mutation NSCLC patients who progressed on an EGFR TKI. That is why KN789 was highly anticipated and yet again, the combination of chemo+ immunotherapy (IO) did not produce significant benefit in this population. Why were there contradictory results? Is immunotherapy a complete no-go for EGFR-mutated NSCLC? Or is there a subset of EGFR-mutated NSCLC patients who may benefit from immunotherapy? If so, how do we identify this population?
The FLAURA trial represents a significant advancement in the treatment landscape for patients with advanced NSCLC harboring EGFR mutations. The trial demonstrated a PFS of 18.9 months among patients receiving osimertinib.3 This extended PFS duration signifies the effectiveness of osimertinib in delaying disease progression compared to earlier EGFR inhibitors. However, it is important to note that despite this promising outcome, a considerable number of patients eventually require subsequent therapy after osimertinib treatment due to the development of resistance mechanisms. This underlines the need for ongoing research into strategies to address resistance and optimize treatment sequencing in order to further improve the long-term outcomes for patients with EGFR-mutated NSCLC.
As discussed previously, there are two ways to overcome resistance to osimertinib and other third-generation TKIs. One approach is to enhance the initial treatment upfront by combining EGFR TKIs with other agents, as in the FLAURA2 and MARIPOSA trials. Indeed, FLAURA219 showed a median PFS improvement of 8.8 months (per investigator) and 9.5 months (per BICR) with the addition of chemotherapy to osimertinib vs osimertinib, although OS data was not mature at the time of presentation. Results of MARIPOSA are forthcoming and are highly anticipated given the positive press release. The other approach is to combat the resistance itself, by using 4th generation EGFR TKIs in those who have developed the resistant C797X mutations; or by a broad (or non-target) approach with chemotherapy, ADCs such as HER3-targeting ADC or IO+ chemotherapy as seen in ORIENT-31, IMpower 150, CheckMate-722 and KEYNOTE-789.
When considering the use of IO + chemotherapy as a broad strategy, we must remember that administering the KEYNOTE-189 (carboplatin, pemetrexed and pembrolizumab) and similar regimens to patients with sensitizing EGFR mutations after osimertinib is a no-go due to KEYNOTE-789 being completely negative. Also, as a general rule, the use of immunotherapy in the treatment of patients with EGFR mutant NSCLC must be approached with extreme caution. Clinical trials are currently evaluating a number of fourth-generation EGFR TKIs such as BLU-945, BDTX-1535, JIN-A02, H002, BBT-207 and THE-349. Exposure to immunotherapy prior to these 4th-generation EGFR TKIs may increase the risk of immune-related adverse events, as was the case with 3rd-generation EGFR TKIs,20 although the actual risk is uncertain.
The difference seen between the results of the CheckMate-722, KEYNOTE-789 trials and the more favorable results from the IMpower 150 and ORIENT-31 trials may suggest that the addition of VEGF-targeted therapies to immunotherapy in the treatment of TKI-refractory EGFR-mutant NSCLC is a reasonable approach; however, we must keep in mind that ORIENT 31 was negative for OS and IMpower 150 was a subset analysis not powered to determine differences in the EGFR/ALK subset.
Researchers are attempting to reveal the possible underlying mechanisms for the poor efficacy of anti–PD-1/PD-L1 treatment in EGFR-mutated NSCLC. Several studies21–24 have revealed that immunosuppressive tumor microenvironment (TME), tumor mutation burden (TMB), intrinsic immune escape mechanisms and coexistence of driver mutations were possible explanations for poor immunoresponse.
TME is a very complex system to support tumor growth that includes malignant cells, immune cells, stroma, fibroblast, cytokines, etc. EGFR-mutated NSCLC often exhibits an immunologically “cold” tumor microenvironment, characterized by limited T cell infiltration and immune cell activity. The tumor microenvironment can be influenced by several factors, including low levels of tumor-infiltrating lymphocytes, high immunosuppressive cell populations (eg, regulatory T cells and myeloid-derived suppressor cells), and an absence of pro-inflammatory cytokines. These conditions contribute to an immune-suppressed state, impeding the success of immunotherapy.21 Patients with EGFR-mutated NSCLC often have distinct clinical characteristics, including a higher frequency of never-smokers25 and a higher incidence in Asian populations.1 These factors might influence the tumor microenvironment and immune response. Qiao M et al22 integrated the seven parameter classes (human leukocyte antigen, interleukin-6, interleukin-8; myeloid-derived suppressor cell; natural killer; PD-L1; tumor-associated neutrophil; T cell receptor; transforming growth factor-b, vascular endothelial growth factor) with the features of TME in EGFR-mutated NSCLC to constitute a framework that could partly uncover the underlying mechanisms for poor immunotherapy response in such population.
Immunotherapy, particularly ICIs, relies on the recognition of tumor-specific neoantigens by activated T cells. TMB, representing the number of genetic mutations in a tumor, is often associated with higher response rates to immunotherapy. However, EGFR-mutated NSCLC typically exhibits a low TMB,23 resulting in fewer neoantigens available for immune recognition and activation, thereby reducing the potential for an immune-mediated response.
EGFR-mutated NSCLC cells can acquire intrinsic mechanisms to evade immune surveillance. Activation of EGFR signaling pathways can lead to the upregulation of immune checkpoint proteins (eg, PD-L1) or the downregulation of major histocompatibility complex molecules, which are crucial for T cell recognition. These alterations diminish the tumor’s visibility to the immune system, rendering it less susceptible to immune attack.
In EGFR-mutated NSCLC, additional oncogenic driver mutations can coexist with EGFR mutations. For instance, mutations in genes such as KRAS or BRAF24 may be present. These concurrent mutations can activate alternative oncogenic signaling pathways, further driving tumor growth and survival, and potentially rendering the tumor less responsive to immunotherapy.
While EGFR-mutated NSCLC generally exhibits poor response rates to immunotherapy, there are certain populations within this subset that may still derive benefit from these treatments. The following populations have shown potential for improved responses to immunotherapy: A, Patients with coexisting genetic alterations. EGFR-mutated NSCLC tumors may harbor additional genetic alterations, such as PD-L1 amplification, STK11/LKB1 mutations, or KEAP1/NRF2 mutations. Some studies have indicated that certain genetic alterations, such as PD-L1 amplification, may sensitize tumors to immunotherapy.26 Therefore, patients with EGFR mutations and specific coexisting alterations might have an enhanced likelihood of responding to immunotherapy. B: High TMB: Although EGFR-mutated NSCLC typically exhibits a low TMB, a subset of patients may have concomitant alterations or higher mutational loads. In cases where the TMB is increased, the likelihood of generating neoantigens that can elicit an immune response is higher. Consequently, patients with EGFR-mutated NSCLC and high TMB may have a better chance of responding to immunotherapy. C: Combination approaches. When comparing the designs of these four clinical trials, the addition of a VEGF inhibitor in IMpower150 and ORIENT-31 was the most notable difference. VEGF is mostly released by stromal or tumor cells, where it promotes angiogenesis and draws in immune-suppressive cells.27 Hypoxia-independent constitutive upregulation of hypoxia-inducible factor 1-alpha can result in VEGF gene expression upon EGFR activation.28,29 In addition, the cross-talk between VEGF and EGFR downstream pathways causes the increased VEGF level in EGFR-mutated lung cancer cells30 and EGFR TKI downregulates VEGF expression.31 The addition of a VEGF-targeted agent may have altered the TME in such a way that the immunotherapy and chemotherapy group may have had a bigger benefit than the chemotherapy group alone.
Conclusion
Despite the excellent efficacy of osimertinib, particularly in first-line settings, the majority of patients develop resistance. Consequently, the development of agents to combat resistance is of urgent need. While considering the use of chemo-immunotherapy in this setting was a reasonable “broad” approach, the dismal outcomes of the KEYNOTE-789 and CheckMate-722 trials have forced us to reconsider the utility of immunotherapy in EGFR-mutated NSCLC; and administering the KEYNOTE-189 regimen to those with EGFR mutations after osimertinib is a no-go in light of the KEYNOTE-789 trial’s negative outcome.
The selection of appropriate patients who are likely to benefit from immunotherapy remains an ongoing challenge. Understanding the complex interplay between EGFR mutations and the tumor microenvironment is crucial for optimizing immunotherapy outcomes in EGFR-mutated NSCLC. At this time, immunotherapy with anti VEGF and chemotherapy may be the only way forward in this population. However, caution is advised as increase in immune-related AE is a concern with the 4th generation TKIs coming into clinic through clinical trials. Preclinical research and ongoing studies aim to identify predictive biomarkers, molecular signatures, and novel therapeutic targets that can enhance the effectiveness of immunotherapy in this patient population.
Abbreviations
AE, adverse effect; ALK, anaplastic lymphoma kinase; BICR, Blinded Independent Central Review; DOR, duration of response; EGFR, epidermal growth factor receptor; ICIs, immune checkpoint inhibitors; IO, immunotherapy; NSCLC, non-small cell lung cancer; OS, overall survival; ORR, objective response rate; PD-L1, programmed cell death ligand-1; PD-1, programmed cell death protein-1; PFS, progression-free survival; TMB, tumor mutation burden; TME, immunosuppressive tumor microenvironment; TPS, tumor proportion score; TK, tyrosine kinase; TKI, tyrosine kinase inhibitors; VEGF, Vascular endothelial growth factor.
Ethics Statement
This work is a commentary utilizing published de-identified clinical trial results and is considered exempt from IRB approval.
Funding
No funding was received for this project.
Disclosure
There are no direct conflicts of interest to disclose. Dr Arter has no potential conflicts to disclose. Dr Nagasaka has received consulting fees from Caris Life Sciences, honoraria from AstraZeneca, Daiichi Sankyo, Novartis, Lilly, Pfizer, EMD Serono, Genentech, Mirati, Regeneron, Takeda, Janssen, Blueprint Medicine and travel support from AnHeart Therapeutics.
References
1. Shi Y, Au JS, Thongprasert S, et al. A prospective, molecular epidemiology study of EGFR mutations in Asian patients with advanced non-small-cell lung cancer of adenocarcinoma histology (PIONEER). J Thorac Oncol. 2014;9(2):154–162. doi:10.1097/JTO.0000000000000033
2. National Comprehensive Cancer Network. Non-small cell lung cancer (version 3.2023). Available from: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1450.
3. Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113–125. doi:10.1056/NEJMoa1713137
4. Ramalingam SS, Vansteenkiste J, Planchard D, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382(1):41–50. doi:10.1056/NEJMoa1913662
5. Akli A, Girard N, Fallet V, et al. Histomolecular resistance mechanisms to first-line osimertinib in EGFR-mutated advanced non-small cell lung cancer: a multicentric retrospective French study. Target Oncol. 2022;17(6):675–682. doi:10.1007/s11523-022-00915-9
6. Nie K, Jiang H, Zhang C, et al. Mutational profiling of non-small-cell lung cancer resistant to osimertinib using next-generation sequencing in Chinese patients. Biomed Res Int. 2018;2018:9010353. doi:10.1155/2018/9010353
7. Planchard D, Feng PH, Karaseva N, et al. Osimertinib plus platinum-pemetrexed in newly diagnosed epidermal growth factor receptor mutation-positive advanced/metastatic non-small-cell lung cancer: safety run-in results from the FLAURA2 study. ESMO Open. 2021;6(5):100271. doi:10.1016/j.esmoop.2021.100271
8. Cho BC, Felip E, Hayashi H, et al. MARIPOSA: phase 3 study of first-line amivantamab + lazertinib versus osimertinib in EGFR-mutant non-small-cell lung cancer. Future Oncol. 2022;18(6):639–647. doi:10.2217/fon-2021-0923
9. Lisberg A, Cummings A, Goldman JW, et al. A Phase II study of pembrolizumab in EGFR-mutant, PD-L1+, tyrosine kinase inhibitor naive patients with advanced NSCLC. J Thorac Oncol. 2018;13(8):1138–1145. doi:10.1016/j.jtho.2018.03.035
10. Gettinger S, Rizvi NA, Chow LQ, et al. Nivolumab monotherapy for first-line treatment of advanced non-small-cell lung cancer. J Clin Oncol. 2016;34(25):2980–2987. doi:10.1200/JCO.2016.66.9929
11. Herbst RS, Baas P, Kim DW, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet. 2016;387(10027):1540–1550. doi:10.1016/S0140-6736(15)01281-7
12. Fehrenbacher L, Spira A, Ballinger M, et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, Phase 2 randomised controlled trial. Lancet. 2016;387(10030):1837–1846. doi:10.1016/S0140-6736(16)00587-0
13. Rittmeyer A, Barlesi F, Waterkamp D, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet. 2017;389(10066):255–265. doi:10.1016/S0140-6736(16)32517-X
14. Socinski MA, Jotte RM, Cappuzzo F, et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med. 2018;378(24):2288–2301. doi:10.1056/NEJMoa1716948
15. Reck M, Mok TSK, Nishio M, et al. Atezolizumab plus bevacizumab and chemotherapy in non-small-cell lung cancer (IMpower150): key subgroup analyses of patients with EGFR mutations or baseline liver metastases in a randomised, open-label phase 3 trial. Lancet Respir Med. 2019;7(5):387–401. doi:10.1016/S2213-2600(19)30084-0
16. Lu S, Wu L, Jian H, et al. Sintilimab plus chemotherapy for patients with EGFR-mutated non-squamous non-small-cell lung cancer with disease progression after EGFR tyrosine-kinase inhibitor therapy (ORIENT-31): second interim analysis from a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Respir Med. 2023;11(7):624–636. doi:10.1016/S2213-2600(23)00135-2
17. Mok TS, Nakagawa K, Park K, et al. LBA8 Nivolumab (NIVO)+ chemotherapy (chemo) vs chemo in patients (pts) with EGFR-mutated metastatic non-small cell lung cancer (mNSCLC) with disease progression after EGFR tyrosine kinase inhibitors (TKIs) in CheckMate 722. Ann Oncol. 2022;33:S1561.
18. Yang JC, Lee DH, Lee JS, et al. Pemetrexed and platinum with or without pembrolizumab for tyrosine kinase inhibitor (TKI)-resistant, EGFR-mutant, metastatic nonsquamous NSCLC: phase 3 KEYNOTE-789 study. J Clin Oncol. 2023;41(17):1.
19. Planchard D, Janne P, Cheng Y, et al. Osimertinib with or without Chemotherapy in EGFR-Mutated Advanced NSCLC. N Engl J Med. 2023;389(21):1935–1948. doi:10.1056/NEJMoa2306434
20. Schoenfeld AJ, Arbour KC, Rizvi H, et al. Severe immune-related adverse events are common with sequential PD-(L)1 blockade and osimertinib. Ann Oncol. 2019;30(5):839–844. doi:10.1093/annonc/mdz077
21. Madeddu C, Donisi C, Liscia N, Lai E, Scartozzi M, Maccio A. EGFR-mutated non-small cell lung cancer and resistance to immunotherapy: role of the tumor microenvironment. Int J Mol Sci. 2022;23:12.
22. Qiao M, Jiang T, Liu X, et al. Immune checkpoint inhibitors in EGFR-mutated NSCLC: dusk or dawn? J Thorac Oncol. 2021;16(8):1267–1288. doi:10.1016/j.jtho.2021.04.003
23. Offin M, Rizvi H, Tenet M, et al. Tumor mutation burden and efficacy of EGFR-tyrosine kinase inhibitors in patients with EGFR-mutant lung cancers. Clin Cancer Res. 2019;25(3):1063–1069. doi:10.1158/1078-0432.CCR-18-1102
24. Chen J, Facchinetti F, Braye F, et al. Single-cell DNA-seq depicts clonal evolution of multiple driver alterations in osimertinib-resistant patients. Ann Oncol. 2022;33(4):434–444. doi:10.1016/j.annonc.2022.01.004
25. Chapman AM, Sun KY, Ruestow P, Cowan DM, Madl AK. Lung cancer mutation profile of EGFR, ALK, and KRAS: meta-analysis and comparison of never and ever smokers. Lung Cancer. 2016;102:122–134. doi:10.1016/j.lungcan.2016.10.010
26. Masuda K, Horinouchi H, Tanaka M, et al. Efficacy of anti-PD-1 antibodies in NSCLC patients with an EGFR mutation and high PD-L1 expression. J Cancer Res Clin Oncol. 2021;147(1):245–251. doi:10.1007/s00432-020-03329-0
27. Goel HL, Mercurio AM. VEGF targets the tumour cell. Nat Rev Cancer. 2013;13(12):871–882. doi:10.1038/nrc3627
28. Xu L, Nilsson MB, Saintigny P, et al. Epidermal growth factor receptor regulates MET levels and invasiveness through hypoxia-inducible factor-1 alpha in non-small cell lung cancer cells. Oncogene. 2010;29(18):2616–2627. doi:10.1038/onc.2010.16
29. Jackson AL, Zhou B, Kim WY. HIF, hypoxia and the role of angiogenesis in non-small cell lung cancer. Expert Opin Ther Targets. 2010;14(10):1047–1057. doi:10.1517/14728222.2010.511617
30. Le X, Nilsson M, Goldman J, et al. Dual EGFR-VEGF pathway inhibition: a promising strategy for patients with EGFR-mutant NSCLC. J Thorac Oncol. 2021;16(2):205–215. doi:10.1016/j.jtho.2020.10.006
31. Ciardiello F, Caputo R, Bianco R, et al. Inhibition of growth factor production and angiogenesis in human cancer cells by ZD1839 (Iressa), a selective epidermal growth factor receptor tyrosine kinase inhibitor. Clin Cancer Res. 2001;7(5):1459–1465.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.