")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 14
The Interrelations of Family Relationship, Illness Cognition of Helplessness and Perceived Barriers to Medication Adherence: A Study of Adolescent and Emerging Adult Kidney Recipients and Their Parents
Authors Hamama-Raz Y , Frishberg Y, Ben-Ezra M, Levin Y
Received 13 June 2023
Accepted for publication 23 September 2023
Published 30 October 2023 Volume 2023:14 Pages 205—215
DOI https://doi.org/10.2147/AHMT.S423355
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yaira Hamama-Raz,1 Yaacov Frishberg,2 Menachem Ben-Ezra,1 Yafit Levin1
1School of Social Work, Ariel University, Ariel, Israel; 2Division of Pediatric Nephrology, Shaare Zedek Medical Center, Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel
Correspondence: Yaira Hamama-Raz, Email [email protected]
Background: Medication adherence among adolescents and emerging adults following kidney transplantation was found to be lower with harmful consequences. The current study aimed to examine associations between illness cognition of helplessness, family relationships, and perceived barriers to medication adherence among post-kidney transplant adolescent and emerging adult recipients and their parents by applying a dyadic perspective.
Methods: Fifty-nine dyads of adolescents and emerging adults aged 11– 26 years and their parents, were recruited from a pediatric nephrology department in a medical center in Israel. Both adolescents and emerging adults and parents completed self-report questionnaires addressing illness cognition of helplessness (subscale of Illness Cognition Questionnaire), family relationships related to conflict and cohesion (Brief Family Relationship Scale), and the adolescents’ perceived barriers (Adolescent Medication Barriers Scale) to taking their prescribed medications.
Results: Adolescents’ and emerging adults’ perceptions of family conflicts moderated the link between illness cognition of helplessness among parents and barriers to medication adherence via the illness cognition of helplessness among adolescents and emerging adults. However, only the adolescents’ and emerging adults’ perceptions of family cohesion had a direct association with barriers to medication adherence. Parents’ perceived family conflict and cohesion did not directly associate with barriers to medication adherence. Findings highlight the complex interplay between family dynamics, illness cognition, and barriers to medication adherence in adolescents and emerging adults.
Conclusion: Parents’, adolescents’ and emerging adults’ perceptions of family conflicts and cohesion, as well as their illness cognitions, can play important roles in understanding and addressing barriers to medication adherence in this population. The study reveals findings that highlight the dyadic transference process of illness cognition of helplessness among both adolescent and emerging adult kidney recipients and their parents in assessing barriers to medical treatment.
Keywords: illness cognition of helplessness, family relationships, barriers to medication adherence, adolescents, parents, kidney transplantation
Introduction
Chronic kidney disease (CKD) was found to be associated with poor long-term outcomes and decreased quality of life among adolescents and emerging adults.1 In addition, systematic reviews and meta-analyses in CKD demonstrated a high prevalence of anxiety disorders and elevated anxiety symptoms2 as well as the presence of depression, particularly in the dialysis setting.3 Unfortunately, a large number of chronically ill kidney patients with organ failure and end-stage disease require organ transplantation.4 This procedure necessitates lifelong adherence to complex medical regimens.4 In a recent systematic review conducted by Hoegy et al,5 medication adherence in pediatric and adolescent transplantation (kidney, liver, and other organs) was found to vary from 22% to 97%. Notably, among pre-dialysis CKD patients, medication adherence rate was found to be 67.4%,6 while the proportion of patients remaining adherent to medications - varied from 65% to 92% among dialysis patients.7
Given the high rates of non adherence and associated consequences (such as acute rejection, graft loss, and mortality),8 Reed-Knight et al9 noted that the patient’s journey through adolescence and into adulthood can pose specific challenges for medication adherence. Thus, developmentally appropriate levels of parental involvement and patient responsibility are critical for optimal treatment compliance. Overall, recognizing and addressing these barriers through tailored support and effective psycho-social interventions can help improve medication adherence and facilitate a successful transition into adult healthcare management.
The current study focused on a dyadic perspective in which individual and familial variables were examined among adolescents and emerging adults (hereafter adolescents) and their parents following kidney transplantation, to predict barriers to medication adherence for post-kidney transplantation treatment.
To begin with, two basic theories guided this research; the first relates to Lazarus and Folkman’s10 transactional theory of stress and coping, which argues that cognitive appraisal plays a significant role in coping with stress and may influence physical and psychological health status.10 In line with this notion, Evers et al11 proposed three generic illness cognitions that reflect different ways of reevaluating the inherently aversive character of a chronic condition namely, acceptance, perceived benefits and helplessness. Acceptance is a way to diminish the aversive meaning. Perceived benefits as a way of adding a positive meaning to the disease. Helplessness is a way of emphasizing the aversive meaning of the disease. Indeed, illness cognition of helplessness has been found to have a significant negative association with medical treatment adherence, as opposed to illness cognitions of acceptance and perceived benefits.12
The second theoretical base that guided the current research refers to Olson’s Circumplex Model12,13 and Moos and Moos’14 family environment mode. These theories suggest that family relationships, namely conflict, and cohesion, are central components for the individual’s wellbeing. Specifically, cohesion focuses on a balance between family member togetherness and family member separateness, and conflict relates to the amount of openly expressed anger, aggression, and conflict among family members.14,15 Regarding adherence to medical treatments, a study conducted by Simons & Blount,16 indicated that less family cohesion and greater conflict among family members were associated with barriers to medication adherence in pediatric populations. Moreover, studies conducted among kidney transplant patients showed that family interactions concerning low familial efficacy and low flexibility were related to increased barriers to medication adherence, while increased parental involvement promoted medication adherence.17,18 In line with this notion, Kraenbring et al19 revealed that perception of family relationships (based on the McMaster Model of Family Functioning)20 among mothers of adolescents aged 12–19 years who had kidney transplantation, was found to be a statistically significant predictor of missed doses of immunosuppressant medication after controlling for the child’s age, income, and caregiver involvement in medication management.
Given the above, and the paucity of research with dyadic data on barriers to medication adherence among adolescent transplantation recipients and their parents in reference to illness cognitions and family relationships, the current study sought to assess the association of illness cognition of helplessness of the parent and the adolescent to barriers to medication adherence post kidney transplant, as a possible path affected by family conflict and cohesion. Understanding these interrelations can inform healthcare providers and researchers in developing interventions and strategies to improve medication adherence. Specifically, the purpose for this research was twofold:
1. To examine whether adolescents’ perceived family relationships (namely, cohesion and conflict interaction) moderate the indirect association between parents’ illness cognition of helplessness and adolescents’ barriers to medication adherence via the adolescents’ illness perceptions of helplessness.
2. To examine whether parents’ perceived family relationships (namely, cohesion and conflict interaction) moderate the indirect association between parents’ illness cognition of helplessness and adolescents’ barriers to medication adherence via the adolescents’ illness perceptions of helplessness.
Based on the above theories, we expected to find a significant indirect effect, in which higher levels of helplessness illness cognition in parents would be associated with higher helplessness illness cognition in adolescents that would be associated with higher levels of barriers to medication adherence. We also expected that under conditions of low levels of family conflict and high levels of family cohesion of both the parent and the adolescent, the indirect effect would not be significant. In contrast, under conditions of high levels of family conflict and low levels of family cohesion of both the parent and adolescent, the indirect effect would be positive and significant.
Methods
Study Design
The study was cross-sectional and was conducted according to the STROBE guidelines for observational studies.
Data Collection Procedure
Participants were recruited from the Division of Pediatric Nephrology of Shaare Zedek Medical Center in Israel. Potential respondents were informed that participation was voluntary, and that data obtained from the survey would be analyzed in an anonymous format. Patients over the age of 18 years provided signed informed consent for participation in the study (according to Israeli law, parents lose guardianship when their child reaches the age of 18, and as such adolescents over the age of 18 need to give their consent). Parents who gave written informed consent for themselves and for their adolescents to participate in the study were asked to complete self-report questionnaires that were distributed by research assistants during a medical follow-up visit. In addition to the parents’ formal consent, the adolescent was also informed by the research assistants that participation was not mandatory and that confidentiality was assured. Inclusion criteria for the study were that the adolescent had received a kidney transplant, was at least 11 years of age, lived with at least one parent, spoke fluent Hebrew or Arabic, and was transplanted at least 12 months prior to participation. Data collection took place between September 2018 and February 2020.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by Shaare Zedek Medical Center Institutional Review Board and Ethics Committee (No. 0068–18-SZMC). All kidneys were donated voluntarily with written informed consent, and this was conducted in accordance with the Declaration of Istanbul.
Measures
Parents and adolescents completed three self-report questionnaires:
Illness cognition of helplessness was examined by the relevant sub-scale of the Illness Cognition Questionnaire (Evers et al, 2001),11 which consists of 6 items examining helplessness of one’s condition (eg, “My illness limits me in everything that is important to me”) on a scale ranging from 1 (“not at all”) to 4 (“completely”). Higher scores in the helplessness domain reflect poorer cognition. In the present study, we used a translated Hebrew version that was previously used in the Israeli population.21 Cronbach’s alpha value in the original study was 0.88 and in the current study was 0.81 for parents and 0.85 for adolescents.
Family relationships were examined using the Brief Family Relationship Scale (BFRS)22 (completed by both groups). We addressed only the conflict and cohesion subscales due to the weaker reliability of the expressiveness subscale as noted by Fok et al.16 The study then focused on cohesion (7 items, eg, “in our family, we really help and support each other”) and conflict (6- items; “in our family, we argue a lot”) subscales. The scale ranges from 1 (“almost not at all”) to 5 (“almost completely”). In the present study, we used translated Hebrew and Arabic versions. The translation was done by a bilingual translator who translated the BFRS from the original language to Hebrew/Arabic while a second bilingual translator independently back-translated the instrument from Hebrew/ Arabic to English. Cronbach’s alpha for total scale BFRS was 0.8822 and in the present study, it was 0.80, and 0.85 for the adolescent’s cohesion and conflict perceived family interactions, and 0.82 and 0.84 for the parent’s cohesion and conflict perceived family interactions.
Barriers to medication adherence - were assessed using the Simons and Blount’s16 scale which addressed the adolescent-perceived barriers to their taking prescribed medication (AMBS). The AMBS consists of 17 items rated on a 5-point Likert-like scale from “strongly disagree” to “strongly agree” with a maximum score of 85. According to Simons and Blount11 there are three factor-analytically derived subscales: disease frustration/adolescent issues with eight items (α = 0.84) (ie, “I do not want other people to notice me taking the medicine”), ingestion issues with five items (α = 0.70) (ie, “I believe the medicine has too many side-effects”), and regimen adaptation/cognitive with four items (α = 0.76) (ie, I find it hard to stick to a fixed medication schedule”). In the present study, we used translated Hebrew and Arabic versions. The translation was done by a bilingual translator who translated the AMBS from the original language to Hebrew/Arabic while a second bilingual translator independently back-translated the instrument from Hebrew/ Arabic to English. The Cronbach’s alpha of the total scale was 0.86 in the original study and 0.83 in the present study.
Data Analysis
Bivariate correlations between the study variables were conducted using SPSS v. 26. The proposed moderated mediation model was examined using the Process Macro for SPSS,23 applying Model 10 with 2000 bias-corrected bootstrap samples. A power analysis using the G*Power 3 software,24 assuming normal and non-dyadic data, a = 0.05, N = 59, and a low-medium effect size of 0.25 with 4 predictors (0.30 correlations within individuals) for analyses of regression indicated high power of 0.81. Assuming dyadic data using the actor-partner’s interdependence (https://robert-a-ackerman.shinyapps.io/APIMPowerRdis/) model with 4 variables and 2 interactions, a = 0.05, N = 59, and a low-medium effect size of 0.15 for effects between adolescent and parent, and 0.25 for the association between variables within the same person, the model has 0.80 power. These power indicators of 0.80–0.81 point that we may be underpowered and miss significant effects, due to type β error. Therefore, our analyses were cross-validated with sensitivity univariate examinations and yielded similar patterns of results. Therefore, we conducted two sets of hierarchical regression analyses to examine the relationships between the investigated measures. Barriers to medication adherence total scores were entered as the dependent variable, and helplessness illness cognition in parents scores were entered as independent. The helplessness illness cognition in adolescents scores was entered as a mediator. Then, two two-way interactions were examined to extend the results of the analyses. Parents’ and adolescents’ conflict and cohesion in family relationships were entered as moderators in the indirect effect via helplessness illness cognition in adolescents, as well as on the direct association between helplessness illness cognition in parents and adolescents’ barriers to medication adherence. Separate regression models were conducted for the parents’ family cohesion and conflict, and for the adolescents’ family cohesion and conflict. A p-value of 0.05 was set as the critical level for statistical significance (for the analysis of indirect effects, if the 95% confidence interval includes 0 then the indirect effect is not significant at the 0.05 level, if 0 is not in the interval then the indirect effect is statistically significant at the 0.05 level; see Hayes.23 The data used is dyadic and constructed as raw data to ensure controlling for the dependence between dyads.
Results
Participants
Seventy-six adolescent and emerging adult kidney recipients and their parents were approached. Of them 59 adolescents and emerging adults aged 11–26 years (M = 19.38; SD = 4.82) and a parent that was -identified as an informal caregiver (71.4% mothers, 28.6% fathers) provided written informed consent to participate and were recruited to the study. Owing to patient confidentiality we had no access to the medical files of the 17 kidney recipients who did not consent to participate, thus there was no information available regarding differences between those recruited and those who declined. Among the 59 participants, the average number of years post-kidney transplantation was 6.49 +5.29 (range 1–14 years), 55.9% (n=33) of them had a living organ transplant, 47 (79.7%) were treated with dialysis before transplantation range 1–77 months (M= 25.01, SD= 21.57).
Bivariate Correlations Between Study Variables
Table 1 presents the bivariate correlations between the study variables. As can be seen in Table 1, illness cognition of helplessness among parents positively correlated with illness cognition of helplessness among adolescents and with barriers to medication adherence. Illness cognition of helplessness among parents positively correlated with parents’ perceived family relationship (ie, cohesion and conflict). It was not correlated with the adolescents’ perceived family relationships (ie, cohesion and conflict).
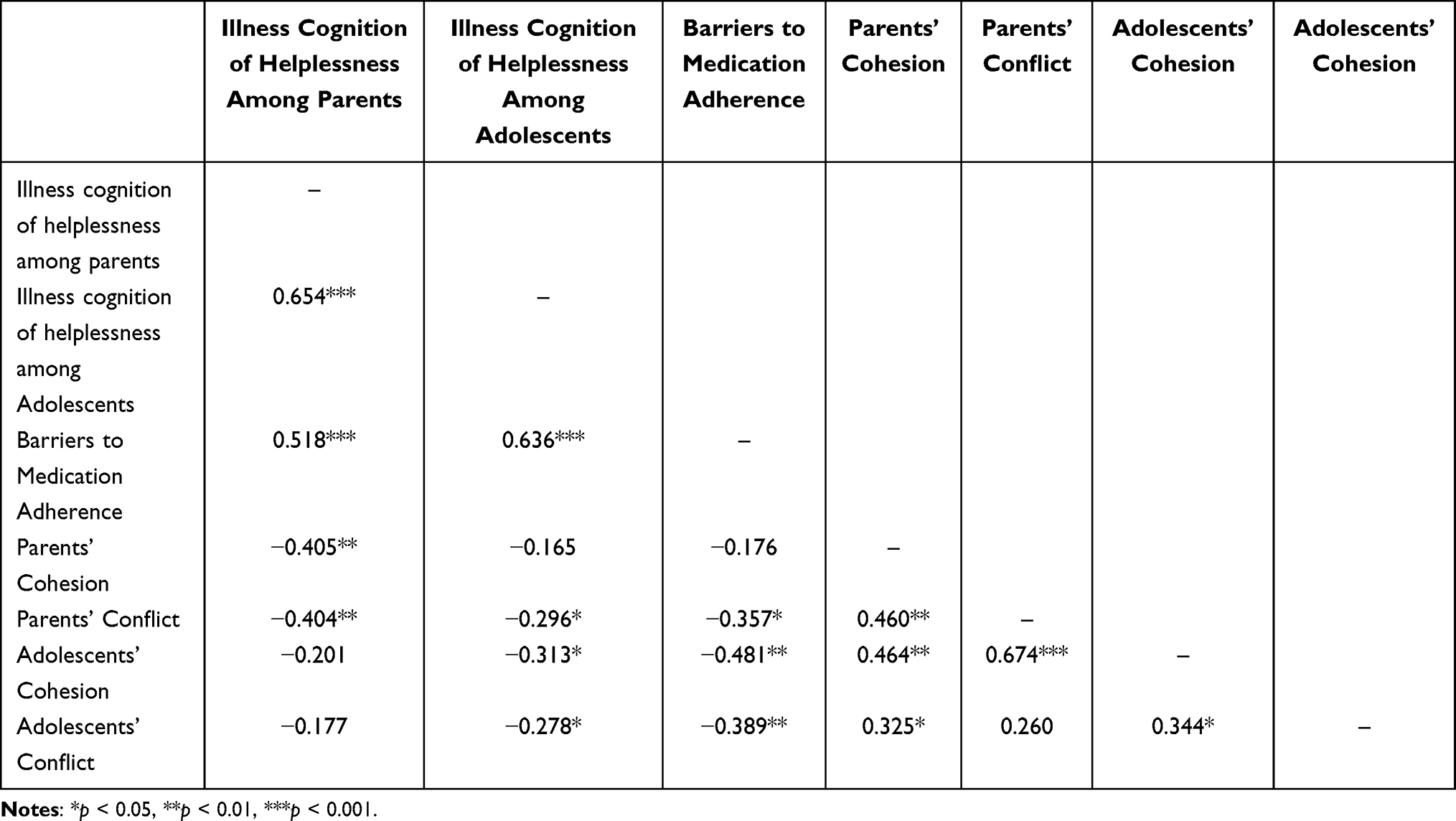 |
Table 1 Bivariate Correlations Between Study’s Variables |
Illness cognition of helplessness among adolescents positively correlated with barriers to medication adherence, and negatively with parents’ perceived family relationship (ie, conflict only) and with both adolescent’s perceived family relationship (ie, cohesion and conflict). Barriers to medication adherence negatively related to parents’ perceived family relationship (ie, conflict only).
The Moderated Mediation Model: From the Perspective of the Adolescent
The overall model for predicting illness cognition of helplessness among adolescents was significant (F (5, 32) = 5.89 p < 0.001 R²= 47.92%). The unstandardized coefficients are depicted in Figure 1. The main association of illness cognition of helplessness among parents (b = 0.68 SE = 0.14 t = 5.00 p < 0.001) was significant. Higher illness cognition of helplessness reported by the parent was associated with higher illness cognition of helplessness of the adolescent. The overall model with adolescents’ barriers to medication adherence as a dependent variable was significant (F (6, 31) = 17.63 p < 0.001) and reached 55% of the variance. Illness cognition of helplessness among adolescents was associated with higher levels of barriers to medication adherence (b = 2.29 SE= 0.40 t = 5.73 p <0.001). However, illness cognition of helplessness among parents was not associated with barriers to medication adherence (b = −0.14 SE= 0.41 t = −0.34 p =0.739). Regarding family relationships, higher levels of family cohesion were associated with lower levels of barriers to medication adherence (b = −1.45 SE = 0.46 t = −3.14 p = 0.004). However, adolescents’ perception of family conflict was not significantly associated with barriers to medication adherence (b = −0.43 SE = 0.41 t = −0.17 p = 0.123).
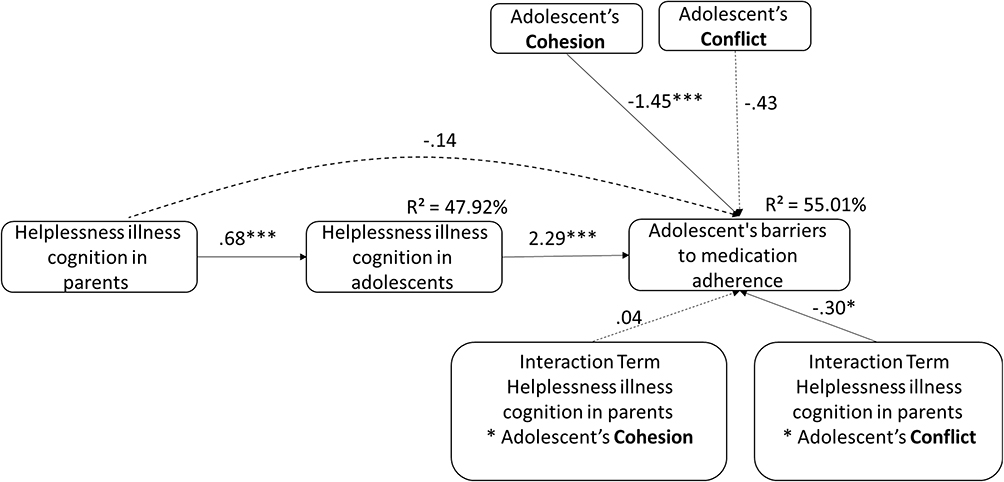 |
Figure 1 The moderating role of Adolescent’s family cohesion and conflict in the indirect effect between illness cognition of helplessness among parents and adolescents’ barriers to medication adherence via illness cognition of helplessness among adolescents. Notes: Solid lines represent significant paths. Dashed lines represent non-significant paths. The sub-factors of cohesion and conflict are bolded to ease reading of the figures. Asterisks in the squares represent the two components of the interaction terms. Asterisk on arrows represent significance levels as follows: *p < 0.05, **p < 0.001. |
The interaction between illness cognition of helplessness among parents and the adolescents’ perception of family conflict was significant (b = −0.30 SE = 0.12 t = −2.47 p = 0.019). However, the interaction between illness cognition of helplessness among parents and the adolescents’ perception of family cohesion, was not significant (b =0.04 SE = 0.05 t = 0.79 p = 0.435). Probing of the adolescents’ perceptions of family conflict and illness cognition of helplessness among parents showed that in higher levels of adolescents’ perceptions of family conflict, the indirect effect between illness cognition of helplessness among parents and the adolescents’ barriers to medication adherence via the illness cognition of helplessness among adolescents was significant (indirect effect b = 1.87 SE = 0.83 CI 95% 0.4745, 3.6955). Higher levels of illness cognition of helplessness among parents were associated with higher levels of illness cognition of helplessness among adolescents which were related with the adolescents’ higher levels of barriers to medication adherence. However, among lower levels of adolescents’ perceptions of family conflict, this indirect association was not significant (indirect effect b = 1.08 SE = 0.64 CI 95% −0.0233, 2.5885).
The Moderated Mediation Model: From the Perspective of the Parent
The overall model for prediction of illness cognition of helplessness among adolescents was significant (F (5, 29) = 8.39 p < 0.001 R²= 59.13%). The unstandardized coefficients are depicted in Figure 2. The main effect of illness cognition of helplessness was significant (b = 0.72 SE = 0.14 t = 5.14 p < 0.001). Higher illness cognition of helplessness among parents was significantly associated with higher illness cognition of helplessness among adolescents. In predicting the adolescents’ barriers to medication adherence, the model was significant (F (6, 28) = 7.99 p < 0.001 R²= 63.13%). The main effect of illness cognition of helplessness among adolescents (b = 2.33 SE = 0.60 t = 3.87 p < 0.001) was significant. However, the illness cognition of helplessness among parents was not associated with barriers to medication adherence (b = 0.17 SE= 0.63 t = 0.27 p =0.792). The main effect of family cohesion (b = 0.21 SE = 0.50 t = 0.43 p = 0.671) and family conflict (b = −0.71 SE = 0.78 t = −0.91 p = 0.373) was also not significant. Notably, the interactions between illness cognition of helplessness among parents and adolescents’ perception of family cohesion (b = −0.07 SE = 0.13 t = −0.53 p = 0.599), and between illness cognition of helplessness among parents and the adolescents’ perception of family conflict (b = −0.03 SE = 0.23 t = −0.15 p = 0.885) were not significant.
 |
Figure 2 The moderating role of Parent’s family cohesion and conflict in the indirect effect between helplessness illness cognition in parents and adolescent’s barriers to medication adherence via helplessness illness cognition in adolescents. Notes: Solid lines represent significant paths. Dashed lines represent non-significant paths. The sub-factors of cohesion and conflict are bolded to ease reading of the figures. Asterisks in the squares represent the two components of the interaction terms. Asterisk on arrows represent significance levels as follows: ***p < 0.001. |
Discussion
The present research focused on adolescents and emerging adults who underwent kidney transplants and on their parents. It examined the moderating role of perceived family relationships (ie, cohesion and conflict) in the indirect association between illness cognition of helplessness among parents and barriers to medication adherence via illness cognition of helplessness among adolescents. Our results showed that adolescents’ barriers to medication adherence were predicted by their illness cognition of helplessness and their perception of family cohesion. This finding supports a previous systematic review regarding barriers to medication adherence among chronically ill adolescents25 that showed that conflicts between adolescents and their parents seemed to be a major reason for non adherence to their medical treatment. In addition, this result highlights the importance of helplessness illness cognition, as a central factor that needs to be assessed in order to reduce barriers to medication adherence. Indeed, according to Leventhal’s common-sense model of illness representations26 the association between illness perception and health outcomes (namely medical adherence) could be related to engagement in self-care practices that involve complex decision making which depends on the patients’ representation of the illness. Thus, it is possible that post kidney transplant, there are parents and adolescents whose illness cognition is perceived as helpless, as they focus mostly on the aversive meaning of their medical situation (ie, commitment to medical follow-up, monitoring of serum creatinine, long-term nutritional management etc.). As such, higher barriers to medication adherence might emerge. Thus, the assessment of patients’ illness cognition of helplessness may provide valuable insights into their attitudes, beliefs, and emotional states, which may impact their ability to adhere to medication regimens.
Another important and novel finding that emerged from the data analysis relates to the dyadic effect that was revealed through the moderated mediation model. Specifically, adolescents’ perceived family conflict moderated the indirect effect between illness cognition of helplessness among parents and barriers to medication adherence via illness cognition of helplessness among adolescents. In higher levels of adolescents’ perceived family conflict, the effect of illness cognition in parents on adolescents’ barriers to medication adherence was not direct but occurred through the intermediary role of illness cognition among adolescents. Nevertheless, under low levels of adolescents’ perceived family conflict, this indirect association was not significant. This may point to the complex interplay between family dynamics, illness cognition and barriers to medication adherence. Interestingly, parents’ perceived family conflict and cohesion did not have a direct association with barriers to medication adherence, nor did they moderate the indirect association between illness cognition of helplessness among parents and barriers to medication adherence via illness cognition of helplessness among adolescents. A possible explanation for these results might be related to changes in the parent-child relations that are recognized during the phase of adolescence. That is, issues such as the quest for independence, experimental behaviors and emotional arousal might raise conflict with parents that can be regarded as normal for family relationships.27 However, numerous conflicts with parents might lead to lower psychosocial adjustment in adolescents and their adjustment problems might trigger more conflict with parents.28 These fluctuations may be salient during chronic illness and the experience of the burden of disease. Previous studies have found that parents and adolescent transplant recipients who report healthier family functioning also report barriers to medication adherence, such as forgetting medications, scheduling issues, and resistance towards medication.16,17 Given the aforementioned, it may be important to address these conflicts because when conflict relations are reported, adolescents’ barriers to medication adherence are more vulnerable to transmission of illness cognition of helplessness from parents to adolescents. This may involve interventions aimed at improving communication within the family, enhancing adolescents’ ability for managing their illness, and providing support and resources to promote optimal medication behaviors.
In reference to the indirect association between illness cognition of helplessness among parents and adolescents’ barriers to medication adherence via illness cognition of helplessness among adolescents, Berg and Upchurch29 claimed that family involvement in chronic disease management is actually a “shared” entity where family members perceive the illness as their own (ie, shared illness ownership), rather than perceiving the illness as the child’s own issue. Thus, it might be that when the parent is preoccupied with the adverse effects of kidney transplantation such as adhering to a strict treatment plan, he or she transmits this perception to their adolescent, which in turn gives rise to the illness cognition of helplessness among adolescents and it is thus associated with higher barriers to medication adherence.
Notably, regardless of the impact of illness cognition of helplessness among parents on the illness cognition of helplessness among adolescents and indirectly on adolescents’ barriers to medication adherence, parents’ perception of family conflict and cohesion did not have a direct association with barriers to medication adherence, nor did they moderate the indirect association between illness cognition of helplessness among parents and barriers to medication adherence via illness cognition of helplessness among adolescents. These results were quite surprising as they are not in line with Minuchin’s view,30 which claims that the family is a social structure with a variety of subsystems and interrelationships. Minuchin30 posited that when the family unit encounters pressures from internal sources or external sources, adaptations need to be applied which may create dysfunction within the family interrelationships. As such, future studies are warranted to replicate these findings. Notwithstanding, our findings highlight the need to assess the adolescents’ perceptions of their family relationships post-kidney transplant because they were found to be significant in comparison to their parents’ perceptions in reference to medical treatment barriers.
Implications
Based on the study’s findings, healthcare providers should prioritize monitoring illness cognition of helplessness among adolescent post kidney-transplant recipients and their parents. This monitoring can be facilitated by the post-transplant unit’s social worker or psychologist using a multidisciplinary approach.31 Additionally, psycho-social personnel in the post-transplant clinic can offer interventions aimed at reducing illness cognition of helplessness for both adolescents and their parents, ultimately reducing barriers to medication adherence. Cognitive-behavioral therapy (CBT) can be employed as an effective intervention, delivered through various formats such as face-to-face sessions, internet-based platforms, or individual and group therapy.32 Accessible platforms outside the hospital setting, such as public Health Management Organizations in Israel, can also be utilized for CBT interventions. These interventions focus on transforming unhelpful illness-related cognitions into helpful ones among children and adolescents with chronic diseases.33,34 In line with this notion, clinics for adolescents with peer support may also be another platform to address adolescents’ needs post-transplantation. This type of setting might foster communication among group members on how to transform illness cognitions of helplessness to helpful cognitions and provide valuable education regarding medication adherence.35
Furthermore, considering the association between family relationships, adolescents’ barriers to medication adherence, and the transmission of illness cognition of helplessness from parents to adolescents, parental counseling is recommended. This type of intervention can be delivered through psycho-educational parents’ group interventions conducted by the psychosocial team of the hospital’s transplant unit or in community settings such as Israeli individual and family welfare care centers. Parental counseling aims to increase parental awareness of the impact of their behavior and illness cognitions on their adolescent and may indirectly influence cooperation with medical treatment post-kidney transplantation. Indeed, insufficient family support has been previously linked to noncompliance among adolescent kidney transplant recipients.36
Limitations
Despite the useful information provided by this preliminary study, it is not without limitations. First, due to the cross-sectional design caution should be applied in generalization of the findings. Second, participants included a relatively small number of dyads recruited from a single institution. Therefore, the analytic plan involved two separate analyses instead of a united model. In addition, perhaps effects were missed due to type β error, and therefore the results should be interpreted cautiously. Important to note that univariate sensitivity analyses were conducted with a single predictor every time to examine the reliability of the findings and results show that all parameters were similar to the main model. Thereby, findings should be reexamined in future studies with larger and multisite samples. Third, the responsibility for the medication regimen was not assessed in the current research which might be a factor in perceived barriers to medication adherence and likely differs depending on the particular family unit. Thus, it is recommended that future studies should include such assessments in order to clarify the role of medication regime responsibility in barriers to medication adherence among adolescent and emerging adult transplantation recipients and their parents. Fourth, the study assessed adolescent and emerging adult-parent relationships which may be rooted in culture.37 Thus, future replication studies should be conducted in various cultures. Lastly, given the susceptibility to reporter bias and the use of subjective measures of barriers to medication adherence in the present study, future research should include objective measures for assessing these barriers to medication adherence such as lab results or daily diaries.
Conclusion
This study highlights the important role of illness cognition of helplessness in assessing barriers to medication adherence post-kidney transplantation in both adolescent and emerging adult recipients and their parents. Overall, findings from the current study indicate that adolescent and emerging adult transplant recipients reported higher barriers to medication adherence in the presence of illness cognition of helplessness among their parents as well as the presence of their own such cognition. Moreover, the current study stresses the importance of monitoring the level of adolescents’ perceived family conflict; When adolescents perceive higher levels of family conflict, illness cognition of helplessness among parents impacts illness cognition of helplessness among adolescents and indirectly impacts adolescents’ barriers to medication adherence.
Data Sharing Statement
The data are available from the corresponding author, upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported via an internal research grant from Ariel University Research Authority (RA1700000290).
Disclosure
The authors report there are no competing interests to declare for this work.
References
1. Ferris ME, Miles JA, Seamon ML. Adolescents and young adults with chronic or end-stage kidney disease. Blood Purif. 2016;41(1–3):205–210. doi:10.1159/000441317
2. Huang CW, Wee PH, Low LL, et al. Prevalence and risk factors for elevated anxiety symptoms and anxiety disorders in chronic kidney disease: a systematic review and meta-analysis. Gen Hosp Psychiatry. 2021;69:27–40. doi:10.1016/j.genhosppsych.2020.12.003
3. Palmer S, Vecchio M, Craig JC, et al. Prevalence of depression in chronic kidney disease: systematic review and meta-analysis of observational studies. Kidney Int. 2013;84(1):179–191. doi:10.1038/ki.2013.77
4. Gutiérrez-Colina AM, Eaton CK, Lee JL, et al. Executive functioning, barriers to adherence, and nonadherence in adolescent and young adult transplant recipients. J Pediatr Psychol. 2016;41(7):759–767. doi:10.1093/jpepsy/jsv107
5. Hoegy D, Bleyzac N, Robinson P, Bertrand Y, Dussart C, Janoly-Dumenil A. Medication adherence in pediatric transplantation and assessment methods: a systematic review. Patient Prefer Adherence. 2019;13:705–719. doi:10.2147/PPA.S200209
6. Seng JJB, Tan JY, Yeam CT, et al. Factors affecting medication adherence among pre-dialysis chronic kidney disease patients: a systematic review and meta-analysis of literature. Int Urol Nephrol. 2020;52(5):903–916. doi:10.1007/s11255-020-02452-8
7. Murali KM, Mullan J, Chen JHC, et al. Medication adherence in randomized controlled trials evaluating cardiovascular or mortality outcomes in dialysis patients: a systematic review. BMC Nephrol. 2017;18(1):42. doi:10.1186/s12882-017-0449-1
8. Lee JL, Eaton C, Gutiérrez-Colina AM, et al. Longitudinal stability of specific barriers to medication adherence. J Pediatr Psychol. 2014;39(7):667–676. doi:10.1093/jpepsy/jsu026
9. Reed-Knight B, Blount RL, Gilleland J. The transition of health care responsibility from parents to youth diagnosed with chronic illness: a developmental systems perspective. Fam Syst Health. 2014;32(2):219–234. doi:10.1037/fsh0000039
10. Lazarus R, Folkman S, editors. Stress, Appraisal, and Coping. New York: Springer; 1984.
11. Evers AW, Kraaimaat FW, van Lankveld W, Jongen PJ, Jacobs JW, Bijlsma JW. Beyond unfavorable thinking: the illness cognition questionnaire for chronic diseases. J Consult Clin Psychol. 2001;69(6):1026–1036. doi:10.1037/0022-006X.69.6.1026
12. Hoekstra T, Cornelius LR, Sjobbema C, Wilming L, Brouwer S. Impact of coping, illness cognitions and perceived health on treatment adherence in disabled workers. Eur J Public. 2018;28(suppl_4):214. doi:10.1093/eurpub/cky214.101
13. Olson DH. Circumplex Model of marital and family systems: assessing family functioning. In: Walsh F, editor. Normal Family Processes.
14. Olson DH. Circumplex model of marital and family systems. J Fam Ther. 2000;22(2):144–167. doi:10.1111/1467-6427.00144
15. Moos R, Moos BS, editors. Family Environment Scale: Manual. Palo Alto: Consulting Psychologists Press; 1981.
16. Simons LE, Blount RL. Identifying barriers to medication adherence in adolescent transplant recipients. J Pediatr Psychol. 2007;32(7):831–844. doi:10.1093/jpepsy/jsm030
17. Guilfoyle SM, Goebel JW, Pai AL. Efficacy and flexibility impact perceived adherence barriers in pediatric kidney post-transplantation. Fam Syst Health. 2011;29(1):44–54. doi:10.1037/a0023024
18. Zelikovsky N, Schast AP, Palmer J, Meyers KE. Perceived barriers to adherence among adolescent renal transplant candidates. Pediatr Transplant. 2008;12(3):300–308. doi:10.1111/j.1399-3046.2007.00886.x
19. Kraenbring MM, Zelikovsky N, Meyers KEC. Medication adherence in pediatric renal transplant patients: the role of family functioning and parent health locus of control. Pediatr Transplant. 2019;23(2):e13346. doi:10.1111/petr.13346
20. Epstein N, Baldwin L, Bishop D. The McMaster family assessment device. J Marriage Fam. 1983;9(2):
21. Palgi Y, Ben-Ezra M, Hamama-Raz Y, Shacham Shmueli E, Shrira A. The effect of age on illness cognition, subjective well-being and psychological distress among gastric cancer patients. Stress Health. 2014;30(4):280–286. doi:10.1002/smi.2521
22. Fok CC, Allen J, Henry D; People Awakening Team. The brief family relationship scale: a brief measure of the relationship dimension in family functioning. Assessment. 2014;21(1):67–72. doi:10.1177/1073191111425856
23. Hayes AF, editor. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. Guilford Press; 2013.
24. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/bf03193146
25. Hanghøj S, Boisen KA. Self-reported barriers to medication adherence among chronically ill adolescents: a systematic review. J Adolesc Health. 2014;54(2):121–138. doi:10.1016/j.jadohealth.2013.08.009
26. Leventhal H, Meyer D, Nerenz DR, Rachman S, editors. The common sense representation of illness danger. In: Contributions to Medical Psychology. Vol. 2. Pergamon Press; 1980:17–30.
27. Branje S, Laursen B, Collins WA. Parent–child communication during adolescence. In: Vangelisti A, editor. Routledge Handbook of Family Communication.
28. Branje S. Development of parent–adolescent relationships: conflict interactions as a mechanism of change. Child Dev Perspect. 2018;12(3):171–176. doi:10.1111/cdep.12278
29. Berg CA, Upchurch R. A developmental-contextual model of couples coping with chronic illness across the adult life span. Psychol Bull. 2007;133(6):920–954. doi:10.1037/0033-2909.133.6.920
30. Minuchin S, editor. Families and Family Therapy. Cambridge, MA: Harvard University Press; 1974.
31. Rianthavorn P, Ettenger RB, Malekzadeh M, Marik JL, Struber M. Noncompliance with immunosuppressive medications in pediatric and adolescent patients receiving solid-organ transplants. Transplantation. 2004;77(5):778–782. doi:10.1097/01.tp.0000110410.11524.7b
32. Douma M, Scholten L, Maurice-Stam H, Grootenhuis MA. Online cognitive-behavioral based group interventions for adolescents with chronic illness and parents: study protocol of two multicenter randomized controlled trials. BMC Pediatr. 2018;18(1):235. doi:10.1186/s12887-018-1216-6
33. Ajasllari J. Cognitive behavioral therapy and treatment of pediatric patients with chronic renal disease. GJPR. 2016;6(2):53–62. doi:10.18844/gjpr.v6i2.560
34. Thompson RD, Delaney P, Flores I, Szigethy E. Cognitive-behavioral therapy for children with comorbid physical illness. Child Adolesc Psychiatr Clin N Am. 2011;20(2):329–348. doi:10.1016/j.chc.2011.01.013
35. Barker D, Enimil A, Galárraga O, et al. In-clinic adolescent peer group support for engagement in Sub-Saharan Africa: a feasibility and acceptability trial. J Int Assoc Provid AIDS Care. 2019;18:2325958219835786. doi:10.1177/2325958219835786
36. Feinstein S, Keich R, Becker-Cohen R, Rinat C, Schwartz SB, Frishberg Y. Is noncompliance among adolescent renal transplant recipients inevitable? Pediatrics. 2005;115(4):969–973. doi:10.1542/peds.2004-0211
37. Tamm A, Kasearu K, Tulviste T, Trommsdorff G. Links between adolescents’ relationships with peers, parents, and their values in three cultural contexts. J Early Adolesc. 2018;38(4):451–474. doi:10.1177/0272431616671827
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.