")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
The Influence of Age-Associated Comorbidities on Responses to Combination Antiretroviral Therapy Among People Living with HIV, at the ART Clinic of Jimma Medical Center, Ethiopia: A Hospital-Based Nested Case-Control Study
Received 8 June 2023
Accepted for publication 30 July 2023
Published 9 August 2023 Volume 2023:15 Pages 457—475
DOI https://doi.org/10.2147/HIV.S421523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Abebaw Abie,1 Mekonnen Damessa2
1Department of Pharmacy, College of Medicine and Health Science, Debre-Markos University, Debre-Markos, Ethiopia; 2Department of Pharmacy, Institute of Health, Jimma University, Jimma, Ethiopia
Correspondence: Mekonnen Damessa, P.O.box: 378, Tel +251924100153, Email [email protected]
Introduction: Despite the high prevalence of age-associated comorbidities in HIV patients in sub-Saharan Africa, there is a lack of data on their influence on treatment outcomes in HIV patients. Therefore, this study aimed to assess the impact of age-associated comorbidities on responses to antiretroviral therapy (ART) among people living with HIV.
Methods: A hospital-based nested case–control study was conducted among adult HIV-infected patients at the Jimma Medical Center from January 3 to June 2, 2022. Data were recorded by interviewing the patients and their medical chart and analyzed using The Statistical Package for Social Science (SPSS) v. 23, and at p < 0.05.
The Results: The overall immunological and virologic failure rates were 13.8% and 13.4%, respectively. Being male [AOR = 3.079,95% CI (1.139– 8.327)], having age-associated comorbidity [AOR:10.57,95% CI (2.810– 39.779)], age ≥ 50 years [AOR = 2.855, 95% CI (1.023– 7.9650)], alcohol intake [AOR = 3.648,95% CI (1.118– 11.897)], and having a baseline CD4+ count of < 200 cells/uL [AOR:3.862, 95% CI (1.109– 13.456) were an independent predictor of immunological failure; Whereas Being alcoholic [AOR:3.11, 95% CI (1.044– 9.271)], having a baseline CD4+ count of < 200 cells/uL [AOR:5.11, 95% CI (1.547– 16.892)], a low medication adherence [AOR:5.92, 95% CI (1.81– 19.36)], bedridden baseline functional status [AOR:3.902, 95% CI (1.237– 12.307)], and lack of cotrimoxazole prophylaxis [AOR:2.735,95% CI (1.084– 6.902)] were found to be an independent predictor of virologic treatment failure, but being younger (age < 50 years) was protective for virologic failure.
Conclusion: Out of the eight patients who were treated for HIV at least one patient had developed immunological and/or virological failure. Age-associated comorbid chronic non-communicable diseases highly influence immunological outcomes compared with virological outcomes. Health providers should pay attention to age-associated comorbidities, encourage lifestyle modifications, and counsel on medication adherence to improve clinical outcomes in patients with HIV.
Keywords: age-associated comorbidity, combination antiretroviral therapy, HIV, immunological failure, virological failure, sub-Saharan Africa
Introduction
Due to population aging brought on by longer lifespans and declining fertility rates, the World Health Assembly adopted the first Global Strategy and Plan of Action on Ageing and Health in 2016.1 Similar to this, there are more patients with HIV who are 50 years of age or older (PLHIV50+)2 Estimates from the Joint United Nations Programme on HIV/AIDS (UNAIDS) for 2013 indicated that around 3.6 million people aged 50 years and older were living with HIV and 6.7 million by 2017.3
In 2019, an estimated 2.2 million people were living with HIV in Western, Central Europe, and North America; about 88% of people living with HIV were aware of their status, and 92% of these people were accessing antiretroviral treatment (ART).4 In 2019, approximately 160,000 people died from AIDS-related illnesses in the region in 2019.5
Sub-Saharan Africa remains among the most severely affected regions, with nearly one in every 20 adults (4.9%) living with HIV, accounting for 69% of the total global HIV cases.6 According to the Ethiopian Public Health Institute (EPHI) HIV-Related estimates for Ethiopia, there are an estimated 13,488 newly infected people, of whom 61.5% are females; and the annual estimated AIDS-related death for was 13,556.7
With the introduction of highly active antiretroviral therapy (HAART), HIV has become a chronic condition,8 and the life expectancy and survival of people living with HIV (PLWHIV) have improved with time.9,10 However, this rise in HIV-positive people’s survival and life expectancy does not come without a price. The vast majority of older HIV-positive adults (PLWHIV) have one or more age-associated Non-AIDS-Related Comorbidities (NARC),11 which are the leading causes of death in people living with HIV, especially among those on long-term highly active antiretroviral therapy (HAART).12
According to estimates, by the year 2030, 84% of patients infected with HIV are expected to have at least one non-communicable disease (NCD), which is an increase from 29% observed in the year 2010. Furthermore, it is predicted that 28% of HIV-infected patients in 2030 will have three or more NCDs.13 Another study conducted at Botswana predicts, in the population not living with HIV (ages 15+), the prevalence of neoplasms/cancers, cardiovascular diseases, and diabetes mellitus increases by about one-quarter between 2015 and 2040, whereas this prevalence will be more than double among people living with HIV (PLWHIV) by 2040.14
Nowadays countries with HIV epidemics are now experiencing growing rates of NCDs, which contribute to poor health, poverty, and inequities and slow the development of countries. Every year, 15 million people die before the age of 70, with 86% of these premature deaths occurring in developing countries.15 The combination of ART with poly-pharmacy for the management of comorbidities significantly increases the chance of potentially serious DDIs, which can lead to drug toxicity, loss of efficacy, and treatment failures;16 and it was becoming an emerging challenge in decreasing life expectancy, increased health care burden, and costs among PLWHIV.17
Despite the increasing burden of HIV and age-associated non-communicable diseases in sub-Saharan African countries, including Ethiopia, limited studies are available regarding the burden of the disease, its management, and the clinical outcomes for the region. Thus, this study assessed the influence of age-associated comorbidities on responses to combination antiretroviral therapy (ART) and their association with people living with HIV infection.
Methods and Materials
Study Design and Clinical Setting
This hospital-based nested case–control study was conducted at Jimma University Medical Center (JUMC) in Ethiopia. The JUMC serves as a referral center for the southwestern part of the country (over 15 million catchment populations). It is 352 km away from the capital city of Addis Ababa. This medical department has oncology, surgery, orthopedics, ophthalmology, internal medicine, pediatrics, gynecology and obstetrics, dermatology, psychiatric, and ART clinic subunits. The ART clinic provides services for approximately 3108 patients and comprises ART pharmacy, TB clinic, voluntary counseling and testing (VCT), adult and pediatric follow-up clinic, data clerkship, laboratory, and cervical cancer screening. This study was conducted between January 3 and June 2, 2022.
Study Population
All adults living with HIV/AIDS (PLWHA) on cart and who were diagnosed with one or more age-associated chronic NCD (ie, CVDs, diabetes, asthma, mental illnesses) were grouped as a case, whereas those patients who were living with HIV/AIDS (PLWHA) on a cart, but not with age-associated NCD, were grouped as a control group. Patients who had regular follow-up and were on combination antiretroviral therapy (ART) for more than six months, who had a baseline CD4 + T cell count and at least two viral load measurements, and CD4+ T cell counts were included in this study.
Sample Size Determination and Sampling Techniques
The sample was determined using the single population proportion formula. Considering the prevalence of influence of age-associated comorbidities on responses to combination antiretroviral therapy in older people living with HIV 17%,18 level of confidence 95%, and margin of error 5%, by adding contingency rate of 10% then the final sample size was 224. A purposive sampling technique was used to collect the data.
Data Collection
The data collection tool was developed by reviewing the literature conducted in a different setting. The data collection tool included sociodemographic, behavioral, clinical, medication-related, age-associated comorbidities, laboratory parameters, and treatment outcomes (immunological and virological). A pre-test was conducted on 5% of the study population before commencing data collection, and appropriate modifications were made to the data-collection tool. Three healthcare professionals (one B. Farm, one BSc nurse, and one medical intern) working at the ART clinic of JUMC collected the data after receiving two days of training on the study purpose and data collection tool. Data collectors abstracted clinical information such as viral load, CD4 count, and WHO staging from the patient’s medical record, as well as from a computerized database and other factors by interviewing the patients when they came for their appointment.
Study Outcomes and Validating Tools
The primary endpoint of this study was to assess the influence of age-associated comorbidities, defined as virological and immunological outcomes, on the response to cART. In the current study, outcome ascertainment was based on the Ethiopian National Comprehensive HIV Prevention, Care and Treatment guideline19 and World Health Organization (WHO) guidelines.20
Operational Definition and Definitions of Terms
- Virological Failure was considered when there was a viral load above 1000 copies/meal based on two consecutive viral load measurements taken three months apart, with adherence support following the first viral load test.
- Immunological failure was defined as a CD4 count ≤ 250 cells/mm3 following clinical failure or Persistent CD4 levels < 100 cells/mm3 (persistent refers to at least two CD4 measurements below the threshold (100 cells/mm3)).
- Age-associated comorbidities: Diseases that emerge according to the patient’s age, such as hypertension, diabetes, dyslipidemia, and impaired renal function, are advanced.
- Comedication: Comedication was defined as a non-antiretroviral medication prescribed for use for ≥30 days total during the study period.
- Polypharmacy: The use of four or more non – HIV medications (excluding HAART), complimentary medications, or supplements within the period from the previous visit.
- Chronic Non-Communicable Disease: Diseases that cannot be transmitted to others through contact with the index person and are not caused by disease-causing microorganisms. Patients are on follow-up for care and treatment at health institutions for at least the last 30 days.21
Statistical Analysis
The collected data were checked for completeness, clarity, and accuracy and entered into Epidata version 4.4.1. The Statistical Package for Social Science (SPSS) version 23 (IBM, Armonk, NY, USA) was used for data analysis. Categorical variables are reported as frequency and percentage (%), and continuous variables are summarized as mean ± standard deviation. A multivariate logistic regression model was used to identify the independent predictors of immunological and virological failure. Variables with a p-value < 0.25 on univariate analysis were considered as candidates for multivariate logistic regression. Variables with a p-value < 0.05, were considered statistically significant.
Results
A total of 224 participants (112 cases and 112 controls) were included in this study.
Socio-Demographic Characteristic
The majority (57.1% vs 67.0% of cases and controls) of the study participants were females. Meaner ± SD age of the study participants was 49.29 ± 10.39 and 41.92 ± 8.74 years for the case and control groups, respectively. One hundred-seven (47.8%) of the patients (45.5% vs.50.0% case and control respectively) were married. The majority of the study participants (38.4% vs.47.3% case and control, respectively) had a primary educational background, and more than 80% of the participants from both cases were urban residents. Sixty-two (55.4%) and 45 (40.2%) controls had no regular incomes. Approximately 96% of cars and 94% of control participants disclosed their HIV status (Table 1).
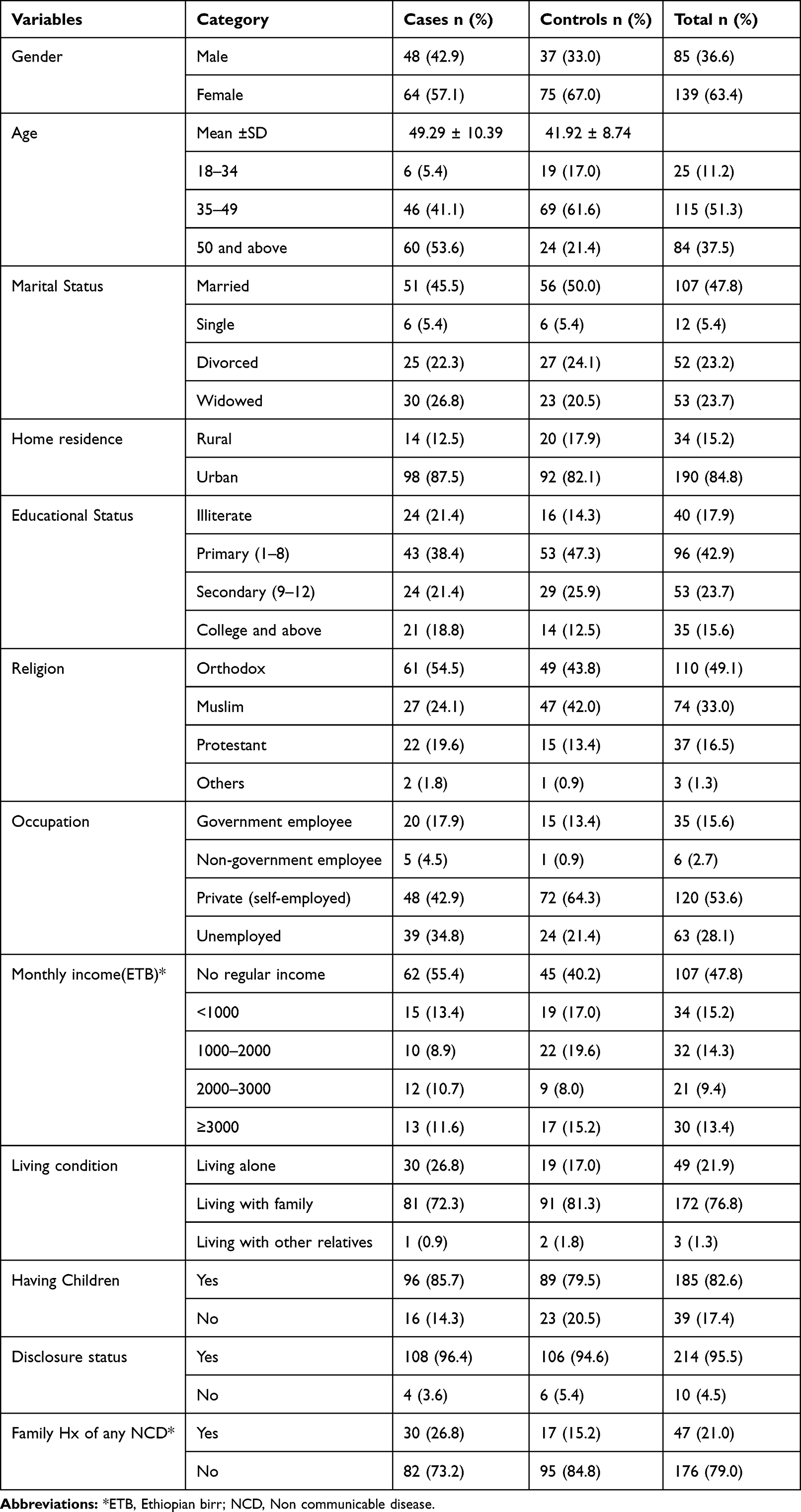 |
Table 1 Baseline Socio-Demographic of HIV Patients at ART Clinic of JMC, Ethiopia |
Patients’ Behavioral Characteristics
Sixty-eight (60.7%) participants in the case group and 69 (61.6%) controls had a history of alcohol consumption. Smoking history was assessed among the study participants (38.4% vs 33.9% of cases and controls). Forty-four (39.3%) participants in the case group and 39 (34.8%) participants in the control group practiced self-medication. Physical exercise (31.3% vs.41.1%), reduced daily salt consumption (83% vs 66.1%), and a sugar-containing diet (82.1% vs.73.2%) were initiated as lifestyle modifications for participants in the case and control groups (Table 2).
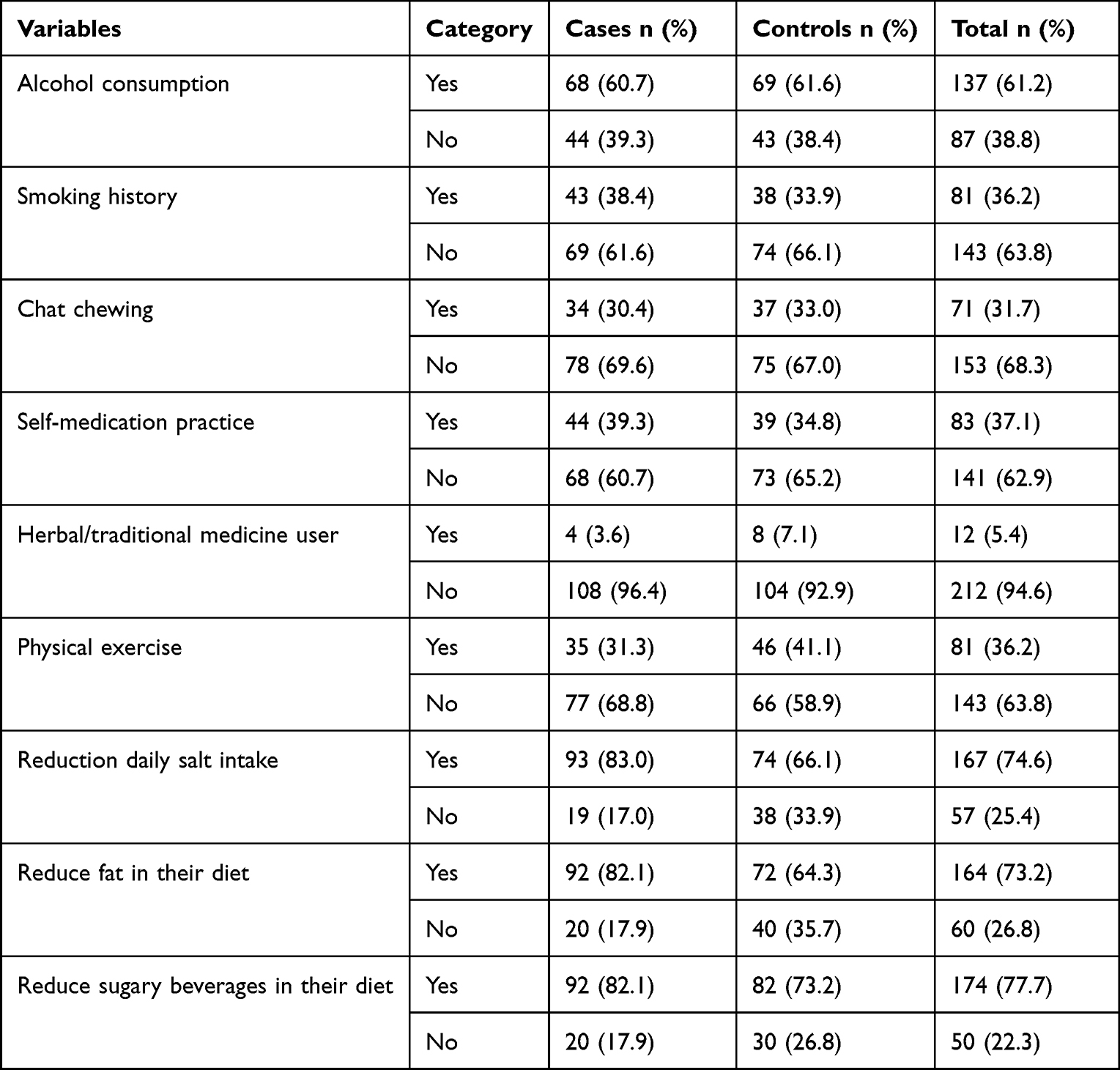 |
Table 2 Behavioral and Life Style Characteristics of HIV Patients at ART Clinic of JMC, Ethiopia |
Clinical Characteristics
Meaner ± SD baseline body mass index (BMI) was 20.15 ± 3.62 and 19.51 ± 2.79 kg/m2 for the case and control groups, respectively. Regarding baseline BMI, 44 (39.3%) patients and 42 (37.5%) controls had a low BMI or were underweight (BMI <18.5) (Table 3). On admission, the majority of the study subjects in both the case and control groups were WHO clinical stage III (34.8% vs 28.6%). Eighteen (16.1%) and 24 (21.4%) study participants in the case and control groups, respectively, started treatment at WHO clinical stage I. Seventy-two (64.3%) and 70 (62.5%) participants were in the case and control groups, respectively. Six (5.4%) and five (4.5%) patients in the control group had HBV co-infection. There were 33 (29.5%) and 39 (34.8%) patients were diagnosed and treated for TB in the case and control groups, respectively; Pulmonary TB was the most common type of TB in both groups. Fifty-four (48.2%) cases and 45 (40.2%) controls had a history of opportunistic infections, whereas 40 (35.7%) cases and 15 (13.4%) controls had a history of hospitalization. The median duration of HIV diagnosis was 167.44 and 141.72 months among cases and controls, respectively (Mann–Whitney U-test) (Table 3).
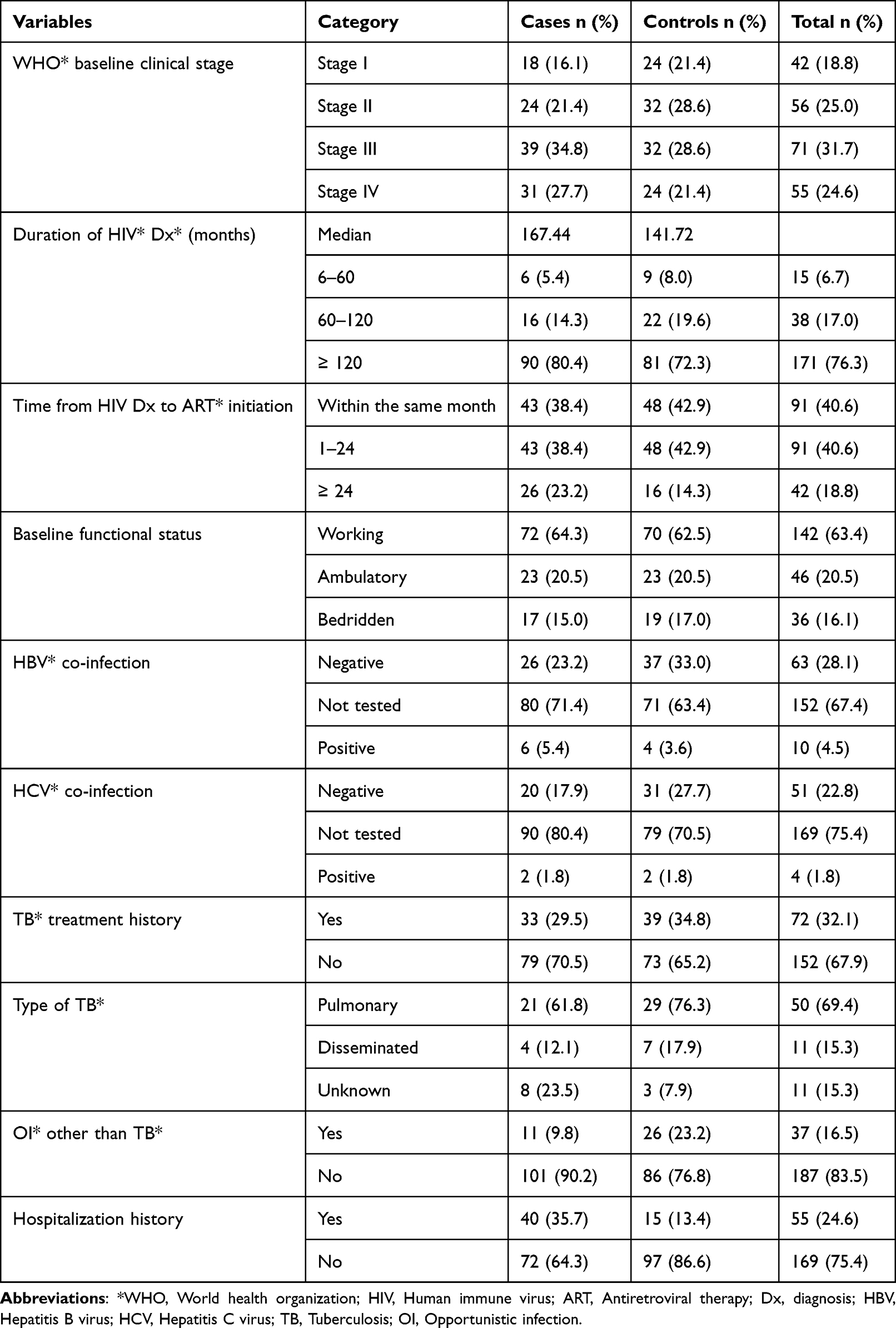 |
Table 3 Clinical Characteristics of HIV Patients at ART Clinic of JMC, Ethiopia |
Age-Associated Comorbidities
Among a total of 112 HIV infected patients who were grouped as case, 84 (75.1%) patients had one age-associated NCD whereas about 18 (24.9%) patients had multi-morbidities. The common age-associated NCD identified among case group were hypertension 32 (28.6%), asthma 17 (15.2%), and diabetes mellitus 15 (13.4) (Figure 1).
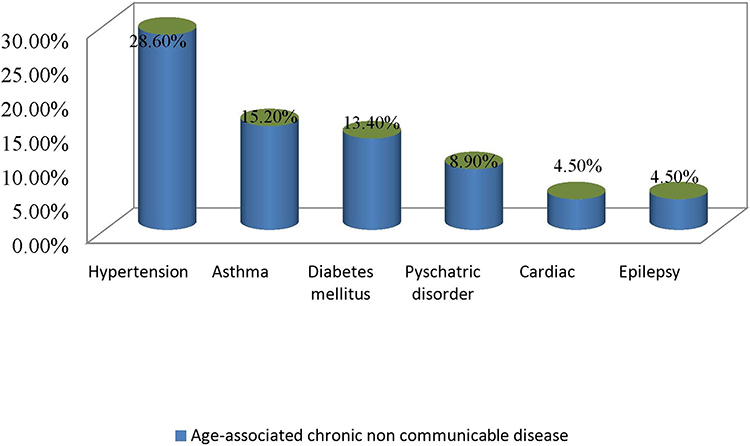 |
Figure 1 Types of age-associated non-communicable diseases among HIV patients at ART clinic of JMC, Ethiopia. |
Medication Related Characteristics
Eighty-eight (78.57%) patients and 96 (85.71%) controls were on the first-line ART regimen (TDF/3TC/DTG). Cotrimoxazole preventive therapy (71.4%) vs 67.9%) was initiated in the case and control groups, respectively, whereas isoniazid (INH) preventive therapy was considered in (86.6% and 85.7%) of the cases and control groups, respectively. TDF/3TC/DTG combination antiretroviral therapy was initiated as the first-line treatment in 80.35% and 85.71% of the case and control groups, respectively. All participants from the case group and 110 (98.2%) controls underwent regimen changes, and the majority (78.57% vs 85.71% cases and controls, respectively) were switched to the first-line chart. Forty-five (40.2%) and 38 (33.9%) patients experienced drug reactions. Twenty–six (23.2%) patients in the chase group were identified as polymedicated, whereas none of the patients in the control group was polymedicated (Table 4).
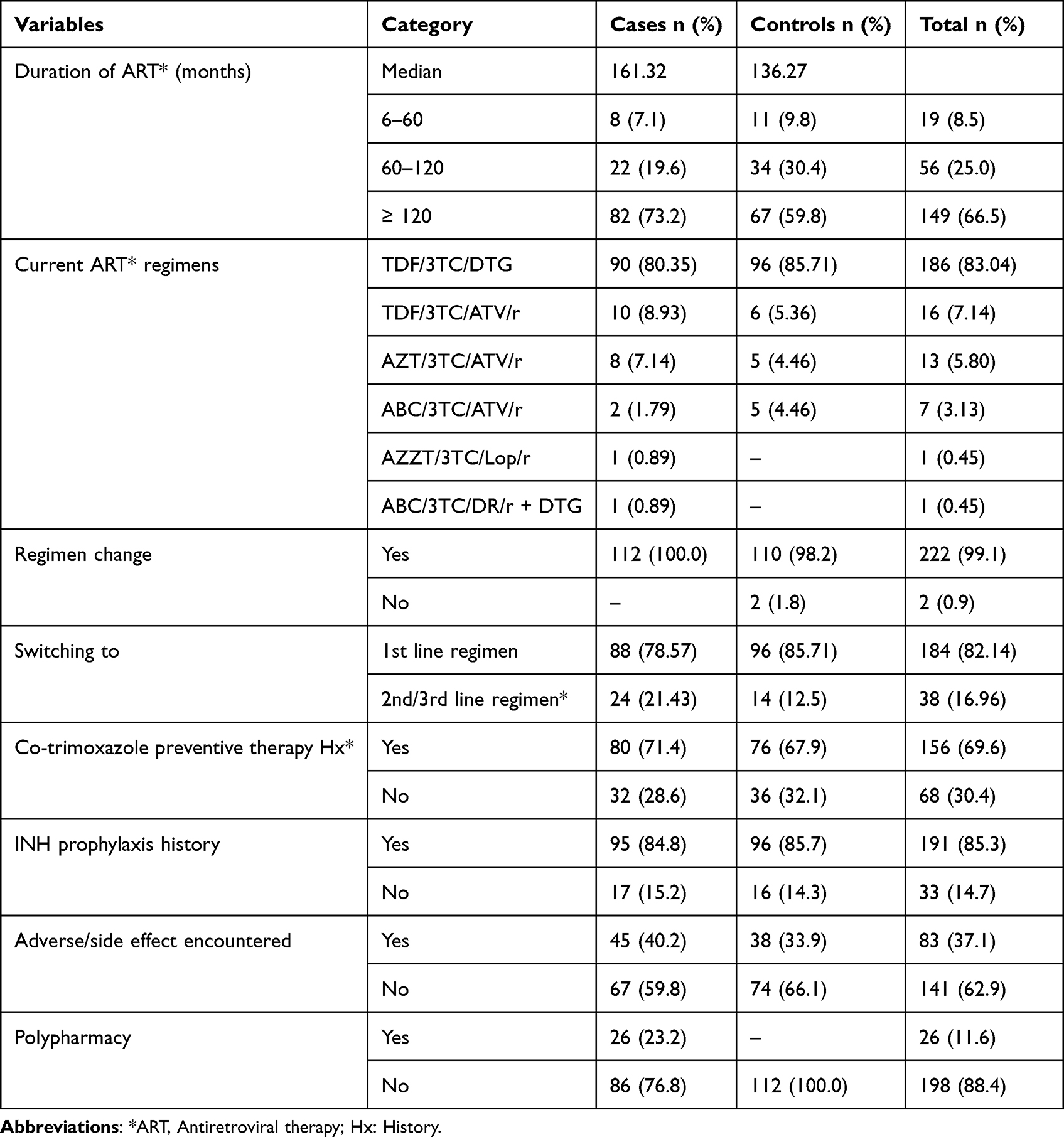 |
Table 4 Management-Related Factors of HIV Patients at ART Clinic of JMC, Ethiopia |
The Level of Medication Adherence Based on the Adherence in Chronic Disease Scale (ACDS)
In the study population, low adherence was found in 22.3% and 3.6% of cases and controls, respectively (Figure 2).
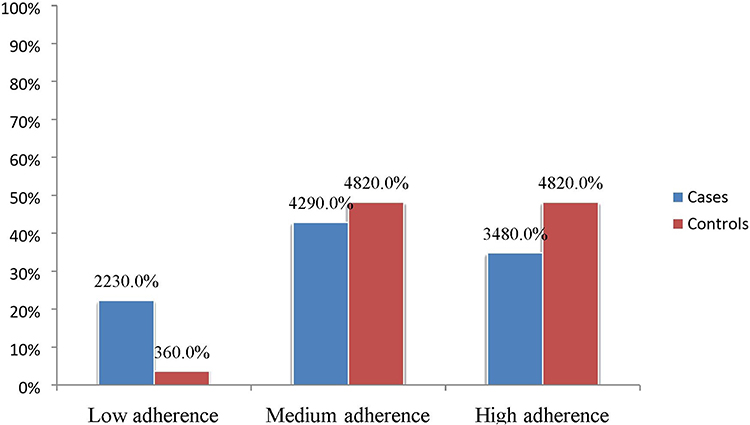 |
Figure 2 The level of medication adherence among HIV patients at ART clinic of JMC, Ethiopia. |
Immunological Characteristics
Seventy-two (64.3%) and 65 (58.0%) controls had a baseline CD4 count </UL. In the study, the median CD4 count of the patients was increased from 169.5 to 504 cells/ at the initiation of ART. A median change in CD4 count change of 334.50 cells/μL was observed after 161.32 months on ART. The median rate of CD4+ T cell increment was 2.07 cells/month among the case group. However, the median CD4 count increased from 183 to 540.50 cells/UL, at the most recent visit. A median CD4 count change of 357.50 cells/μL was observed after 136.27 months of ART treatment. The median rate of CD4+ T cell increase was 2.62 cells/month in the control group (Figure 3).
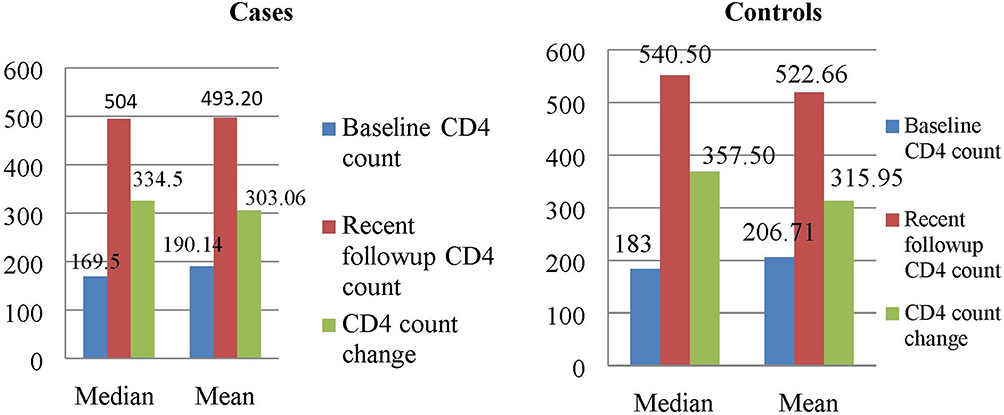 |
Figure 3 The median and mean CD4 count change among cases and controls at ART clinic of JMC, Ethiopia. |
Hematologic Factors
The baseline and recent visit mean white blood cell (WBC) counts in the case and control groups were (2.80±6.67×103 /μL vs 2.81±6.27×103 /μL) and (3.75 ±7.89 × 103/μL vs 3.95 ± 6.94×103/μL), respectively. The mean and standard deviation baseline platelet counts for the case and control groups were 121.91 ± 281.38×103 cells/μL and 114.89 ± 263.02×103 cells/μL, respectively. The recent one was 106.82 ± 272.42×103 cell/μL for cases and 111.42 ± 290.00×103 cells/μL for controls (Table 5).
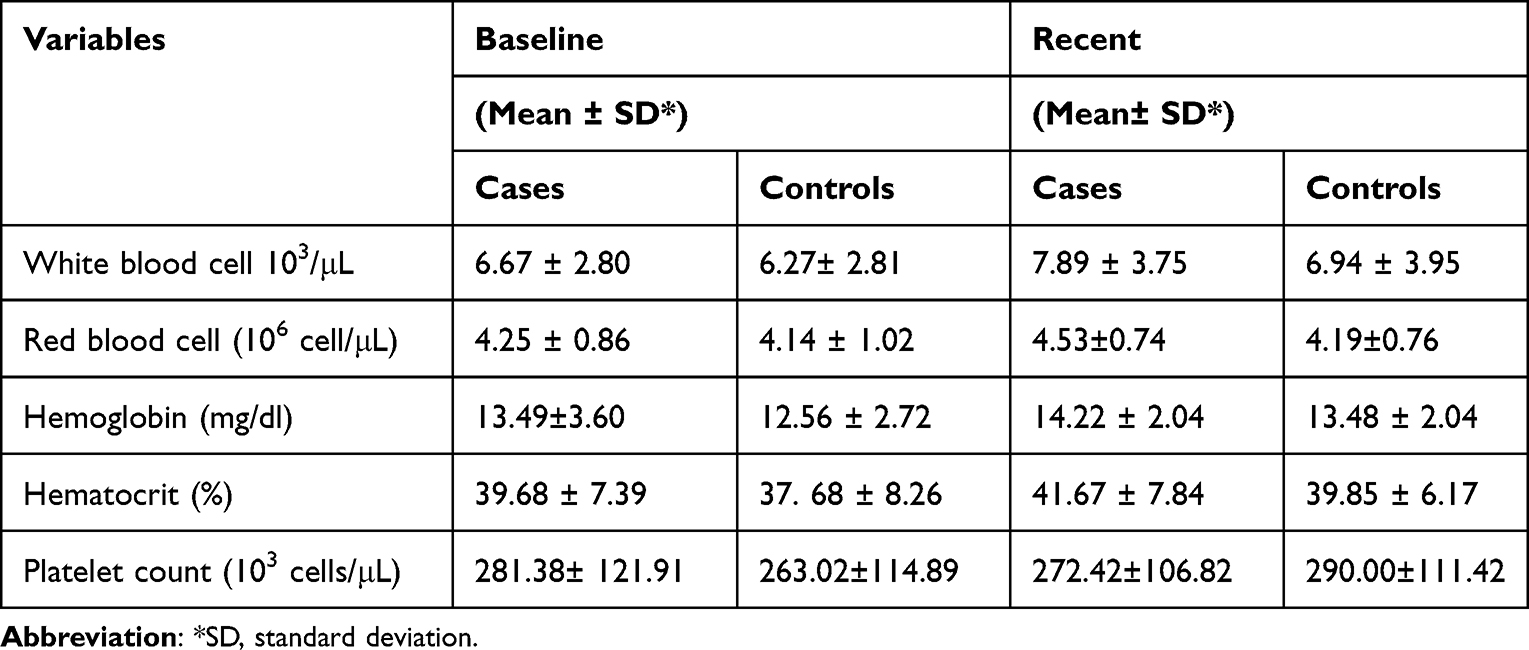 |
Table 5 Baseline Hematological Finding of HIV Patients at ART Clinic of JMC, Ethiopia |
Immunological and Virological Outcomes
Immunological failure was identified in 31 (13.8%), 26 (23.2%), and 5 (4.5%) patients in the case and control groups, respectively. Similarly, overall virological failure was identified among 13.39% of the study participants, which was (15.18% and 11.60%) of patients among the case and control groups, respectively.
Factors Associated with Immunological Failure
In multivariable logistic regression analysis, being male was associated with a three-fold increase in immunological failure Adjusted odds ratio (AOR = 3.079, 95% CI:1.139–8.327); similar patients who had age-associated comorbid conditions had a ten-fold increment in immunological failure (AOR:10.573, 95% CI:2.810–39.779). The other variable that had a statistically significant association with immunological failure was age ≥50 years, with an approximately three-fold increase (AOR:2.855, 95% CI; 1.023–7.965) and history of alcohol intake, which increased immunological failure by four-folds (AOR = 3.648,95% CI: 1.118–11.897). Finally, patients who had a baseline CD4+ count of < 200 cells/uL (AOR: 3.862, 95% CI: 1.109–13.456) had also an approximately four-fold increase in immunological failure (Table 6).
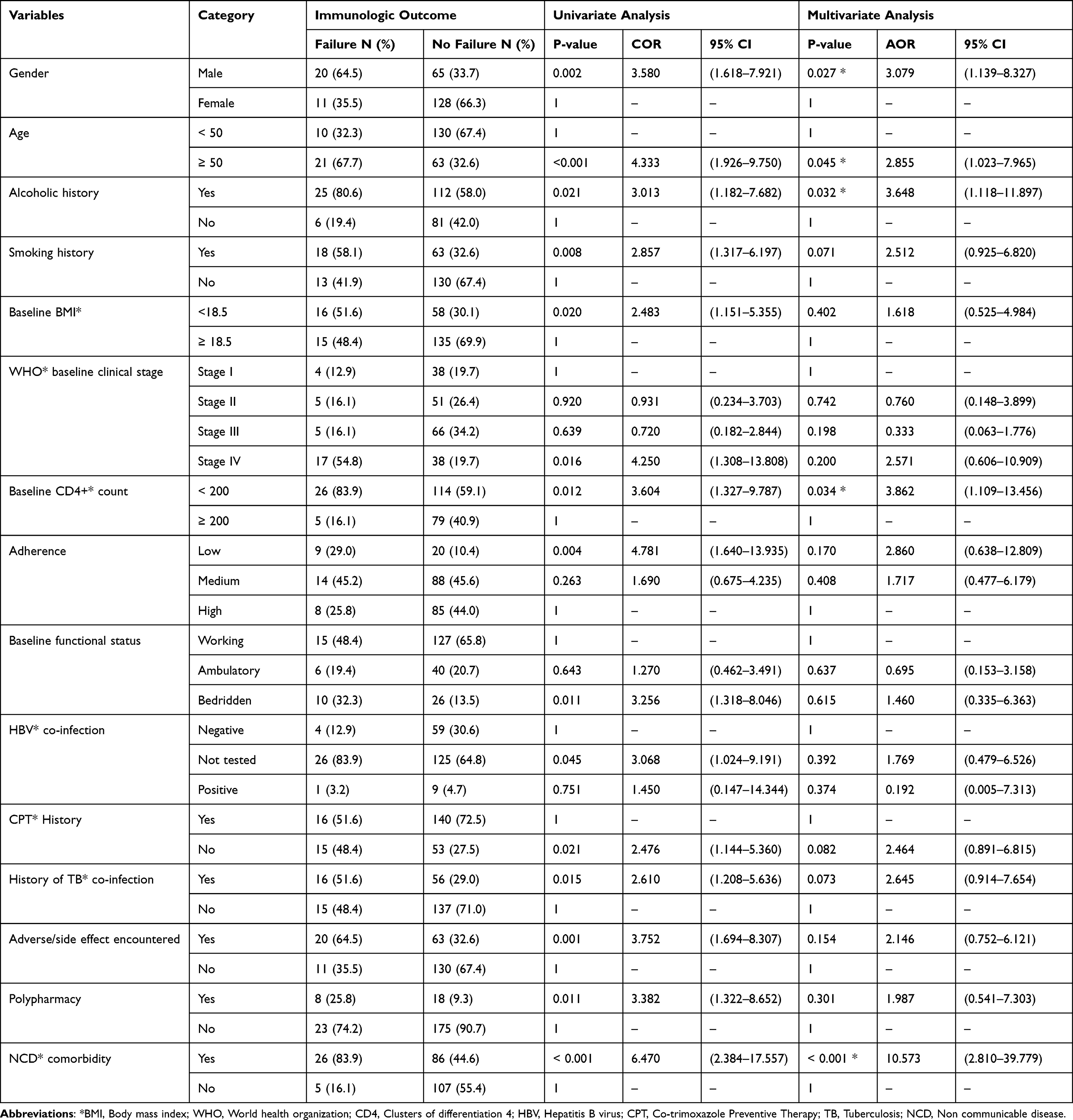 |
Table 6 Predictors of Immunological Failure Among of HIV Patients at ART Clinic of JMC, Ethiopia |
Factors Associated with Virological Failure
Patients who were alcoholic had an approximately three-fold increase in virological failure (AOR, 3.11; 95% CI: 1.044–9.271); whereas those who had a baseline CD4+ count of < 200 cells/uL had an approximately five-fold increase (AOR,5.11; 95% CI: 1.547–16.892). A low level of medication adherence also increased virological failure six-fold (AOR, 5.92; 95% CI: 1.810–19.362). Similarly, lack of cotrimoxazole preventive therapy (AOR: 2.73, 95% CI: 1.084–6.902), and having a baseline bedridden functional status (AOR:3.90, 95% CI: (1.237–12.307)) increased virological failure by approximately three and four-folds respectively. Older age (≥50 years) was the only variable identified as protective against virologic failure (AOR, 0.15; 95% CI:0.047–0.512) (Table 7).
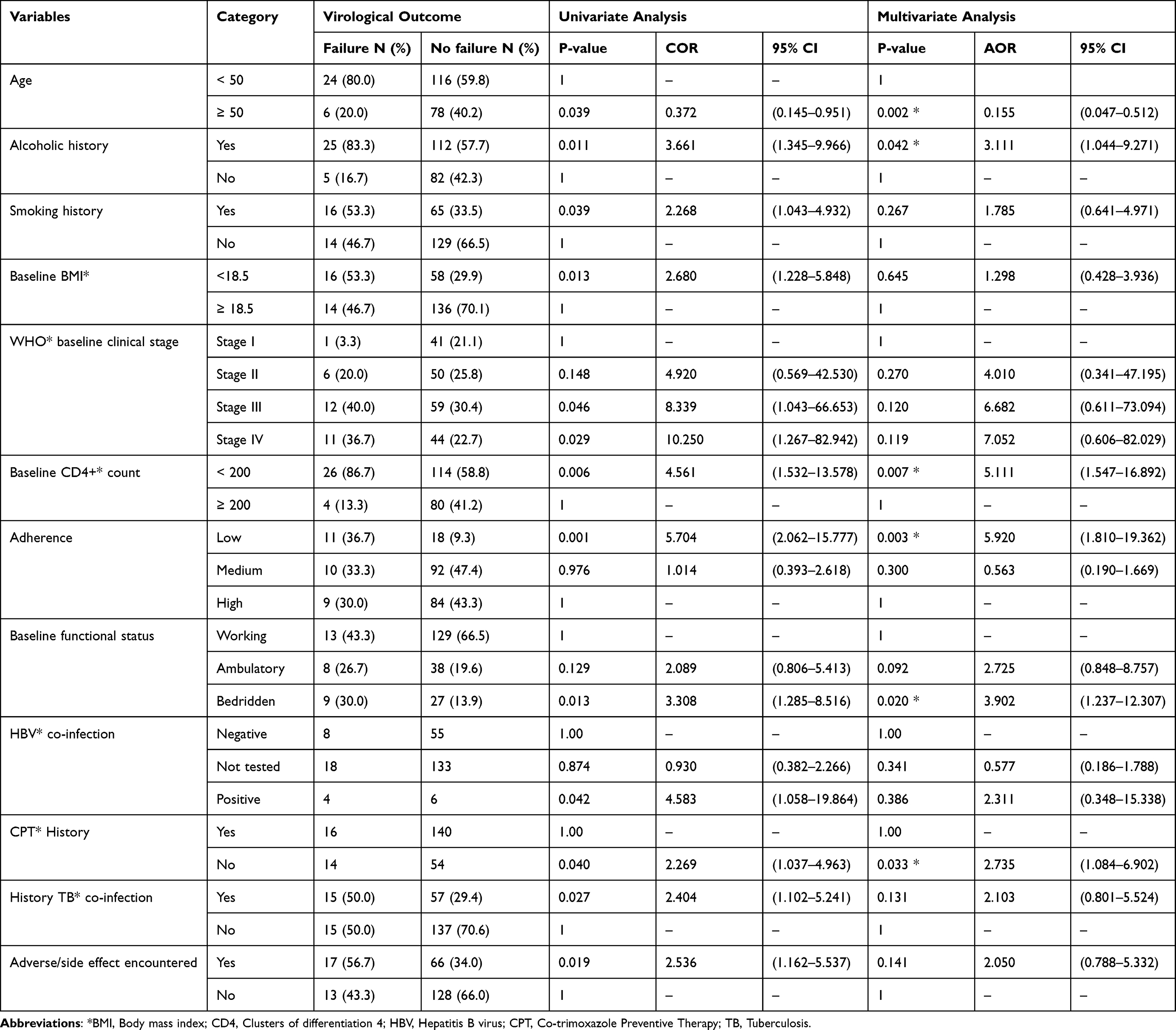 |
Table 7 Predictors of Virological Failure Among HIV Patients at ART Clinic of JMC, Ethiopia |
Discussion
This study assessed the influence of age-associated comorbidities on the therapeutic outcomes of combination antiretroviral therapy (carts). The current study reported that hypertension (28.6%) as an age-associated comorbidity was common among patients with HIV. This finding was lower than that reported in studies conducted in Asia (34%), the USA (40.4%), and Portugal (39.7%).11,18,22 The observed differences might be due to differences in the study populations (that is. In the current study, the majority of the population was younger than the older population in later studies).
The overall rate of immunological failure was 13.8% (23.2% vs.4.5%) in the case and control groups, respectively. This rate was higher than that reported in a study conducted in Asia (7%).18 The difference observed might be due to the age differences among the study participants included (ie, in our study, 37.5% of the study participants were ≥50 years vs later study, only 9.6% of the study participants were ≥50 years). However, this was lower than that reported in a study conducted in Dire Dawa, Ethiopia (19.3%).23 This difference might be due to sample size (eg, 224 vs 949).
In the current study, male sex, age ≥50 years, the presence of age-associated comorbid condition being alcoholic, and having a low baseline CD4 count (<200 cells/UL) were independent predictors of immunological failure. Male patients were three times more likely to develop immunological failure than female patients were. This finding is supported by previous studies conducted in Asia and Ethiopia.18,24
Similarly, patients aged ≥50 years were nearly three times more likely to develop immunological failure than those aged <50 years were. This was in line with studies conducted in Asia, Israel, and the USA18,25,26 which showed a slower increase in CD4 + cell counts in patients aged ≥50 years than in their younger counterparts. However, the current finding was contrary to those of studies conducted in Nigeria and Uganda27,28 which reported that CD4 recovery was not significantly associated with age differences. This discrepancy might be due to the study population differences; in the current study, the baseline CD4 count was (166.50 cells/mm3 Vs 179.50 cells/mm3) in participants aged ≥50 years and <50 years, respectively; the later studies included populations with baseline CD4 counts (306 cells/mm3 vs /mm3) in participants aged ≥50 years and <50 years, respectively.
In addition, this study reported that HIV-infected patients with age-associated comorbidities (cases) were 10 more likely to develop immunological failure than those infected with HIV alone (controls). This is consistent with a study conducted in Jimma.10
Patients with a history of alcohol consumption were also three times more likely to experience immunological failure than those with no history of alcohol consumption. This was contradictory to the results of a study conducted in French,29 which reported that patients with a history of low alcohol consumption had better CD4 counts.
Moreover, patients with low CD4 counts (<200 cells/µL) were more than three times more likely to have immunological failure than those with baseline CD4 counts ≥ 200 cells/uL. This finding was supported by studies conducted in Asia, China and Ethiopia.18,24,30,31 Nevertheless, a study conducted in southern Ethiopia reported a higher baseline CD4 cell count as a risk factor for immunological failure.32 This inconsistency might be due to the difference in CD4 cut-off points used to define immunological failure (WHO 2016 vs WHO 2010, which defines immunological failure when CD4 levels remain below 100 cells/mm3 and/or 50% fall from the on-treatment peak value).
The second treatment outcome measured was virological failure in HIV-infected patients. The overall magnitude of virological failure reported in this study was 13.39% (15.18% vs.11.60%) in cases and controls, respectively. This was comparable to studies conducted in Adigrat (12.5%), South Wollo (15.9%), and Ethiopia.32,33 However, it was higher than that reported in studies conducted at Mizan-Tepi University (2.3%), Southwest Ethiopia.31 The observed inconsistency might be due to methodological differences used to capture virological failure (that is. A previous study assessed only patients on first-line antiretroviral therapy, whereas the current study reported the virological outcomes of all patients, regardless of their regimen).
The current study reported that patients aged <50 years were more likely to experience virological failure than elderly patients. Our findings are consistent with those of studies conducted in Uganda, Canada and Ethiopia.34–37 In contrast, studies conducted in the Waghimra Zone, Northern Ethiopia reported that patients older than 35 years had a higher likelihood of virological failure than their younger counterparts.38 This variation may have been due to the difference in the number of younger patients included in the current study (62.5% vs 37.5%), which may have increased the magnitude of virological failure in this study.
Another variable that had a statistically significant association with virological failure was a low level of medication adherence; thus, patients who had a low level of medication adherence were nearly six times more likely to develop virological failure than those who adhered to their medications. Our findings are similar to those of studies conducted in Asia,18 Ethiopia (10,32,34,36) and Uganda.39
A lower baseline CD4 count (ie, </UL) was also a predictor of virological failure. Patients with a baseline CD4 count of < 200 cells/uL was five times more likely to have virological failure than those with a baseline CD4 count of ≥/UL. This has been confirmed by several studies conducted in Asia,18 South Africa,40 Ethiopia.19,31
Similarly, patients with a history of alcohol consumption were three times more likely to experience virological failure than those with no history of alcohol consumption. This finding was supported by a study conducted in Guatemala, central America.41
The baseline functional status was also an independent predictor of virological failure. Our findings showed that patients with a bedridden baseline functional status were nearly four times more likely to develop virological failure than those with working functional status. This is in line with the studies conducted in Ethiopia, Debre-Markos and Arba Minch.42,43
Finally, the use of cotrimoxazole prophylaxis was significantly associated with virological failure. In this study, patients who did not receive cotrimoxazole prophylaxis were more than twice as likely to develop virological failure as compared to those who did cotrimoxazole prophylaxis. This is consistent with the results of a study done in Uganda.28 A study conducted in China44 showed that patients using cotrimoxazole preventive therapy were approximately two times more likely to have a risk of virological failure. This discrepancy might be due to differences in the outcome ascertainment methods used to define virological failure (ie, in the current study, virological failure was defined as two consecutive viral loads greater than 1000 copies/mL within 3 months with enhanced adherence support, whereas the previous study defined virological failure as a viral load greater than 400 copies/mL for two or more consecutive times over 6 months on ART).
This study aimed to prospectively examine the behavioral characteristics, clinical characteristics, age-associated comorbidities, medication-related characteristics, and outcomes of patients in the study setting. However, the study has several limitations that should be considered when interpreting the findings. Firstly, due to resource constraints, the study was conducted on a small sample population, which may limit the generalizability of the results to other populations. Secondly, there was difficulty in pairing the participants, and the lack of adequate control groups for each case selected may have affected some results. Thirdly, the diagnoses of age-associated NCD were mostly based on patients’ self-reports, and early identification of these diseases was not routinely performed in the setting due to a lack of adequate human power and socioeconomic status of the patients.
Fourthly, CD4 tests and virological tests were not regularly performed for the patients due to a lack of regular follow-up at the same clinic and inadequate resources, which made it challenging to make decisions for some patients as per guideline recommendations. Lastly, other important outcomes such as economic cost, quality of life, and quality of care were not measured.
Conclusion
There was a high magnitude of both immunological and virological failure among the study participants. Age-associated chronic comorbidities were highly associated with immunological failure, whereas there was no significant association between virological outcomes and age-associated comorbidities. Male sex, age ≥50 years, and the presence of age-associated chronic medical conditions were independent predictors of immunologic treatment failure. On the other hand, a low level of patient medication adherence, lack of cotrimoxazole preventive therapy, and baseline bedridden functional status were found to be independent predictors of virologic treatment failure. History, alcohol consumption, and a baseline CD4+ count </UL were significantly associated with both immunological and virological failure. However, age ≥50 years was protective against virological failure. We recommend that health providers pay attention to the prevention of age-associated comorbidities, encourage lifestyle modifications, and initiate ART early to improve immunological and virological failures in HIV-infected patients.
Abbreviations
ART, Antiretroviral Therapy, ARV: Antiretroviral; cART, Combination Antiretroviral Therapy, CBC: Complete blood cell count; CD4, Cluster of Differentiation 4; CPT, Co-trimoxazole preventive therapy; HAART, Highly Active Antiretroviral Therapy; HIV/AIDS, Human Immune deficiency Virus/Acquired immune deficiency syndrome, LMIC: Low and Middle Income Country, NCDs: Non-communicable diseases, PLWHIV: People living with human immunodeficiency virus, SPSS: Statistical Package for Social Sciences, TDF/3TC / DTG: Tenofovir/Lamivudine/Deltugravir, WHO: World Health Organization.
Data Sharing Statement
The dataset used to support the findings of this study will be made available by the corresponding author (M.D) upon reasonable request.
Ethical Approval and Consent to Participate
The study protocol was approved by the Institutional Review Board (IRB) of Jimma University, Institute of Health (reference number IHRPGD/567/2020). The study participants were provided with information regarding the objectives of the study, as well as their full right to withdraw from the study and decline participation. Both written and verbal informed consent was obtained from all participants included in this study. All the study protocols were performed in accordance with the ethical principles of the Declaration of Helsinki.45 The privacy and confidentiality of personal information were also maintained and protected.
Acknowledgment
We would like to thank Jimma University for facilitating the study and covering stationery materials and data collection costs. We would also like to acknowledge all data collectors, supervisors, and respondents without whom this research would not have been realized. This paper was presented at the Jimma University master’s thesis as an abstract presentation with interim findings. The poster’s abstract was deposited in https://repository.ju.edu.et//handle/123456789/7826.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Jimma University Institute of Health (grant number [JUIH/567/2020]). The funder made no contribution to this study regarding the study design, data collection, data analysis, interpretation of data, or writing of the manuscript.
Disclosure
The authors declare that there are no conflicts of interest regarding this work.
References
1. Rudnicka E, Napierała P, Podfigurna A, Męczekalski B, Smolarczyk R, Grymowicz M. The World Health Organization (WHO) approach to healthy ageing. Maturitas. 2020;139:6–11. doi:10.1016/j.maturitas.2020.05.018
2. Autenrieth CS, Beck EJ, Stelzle D, Mallouris C, Mahy M, Ghys P. Global and regional trends of people living with HIV aged 50 and over: estimates and projections for 2000–2020. PLoS One. 2018;13:e0207005. doi:10.1371/journal.pone.0207005
3. Mugisha Okello J, Nash S, Kowal P, et al. Survival of people aged 50 years and older by HIV and HIV treatment status: findings from three waves of the SAGE-Wellbeing of Older People Study (SAGE-WOPS) in Uganda. AIDS Res Ther. 2020;17:1–8. doi:10.1186/s12981-020-00276-1
4. Nugraha AP, Mensana MP, Soebadi B, et al. Correlation of low CD4+ counts with high dental caries prevalence in children living with perinatal HIV/AIDS undergoing antiretroviral therapy. Pesqui Bras Em Odontopediatria E Clínica Integrada. 2020;13:19.
5. Odlum M, Moise N, Kronish IM, et al. Trends in poor health indicators among Black and Hispanic middle-aged and older adults in the United States, 1999-2018. JAMA Netw Open. 2020;3:e2025134. doi:10.1001/jamanetworkopen.2020.25134
6. Oputa R, Chinenye S. Diabetes mellitus: a global epidemic with potential solutions. Afr J Diabetes Med. 2012;20:33.
7. Mussie KM, Gradmann C, Manyazewal T. Bridging the gap between policy and practice: a qualitative analysis of providers’ field experiences tinkering with directly observed therapy in patients with drug-resistant tuberculosis in Addis Ababa, Ethiopia. BMJ Open. 2020;10:e035272. doi:10.1136/bmjopen-2019-035272
8. Maciel RA, Klück HM, Durand M, Sprinz E. Comorbidity is more common and occurs earlier in persons living with HIV than in HIV-uninfected matched controls, aged 50 years and older: a cross-sectional study. Int J Infect Dis. 2018;70:30–35. doi:10.1016/j.ijid.2018.02.009
9. Teeraananchai S, Kerr S, Amin J, Ruxrungtham K, Law M. Life expectancy of HIV‐positive people after starting combination antiretroviral therapy: a meta‐analysis. HIV Med. 2017;18:256–266. doi:10.1111/hiv.12421
10. Trickey A, May MT, Vehreschild JJ, et al. Survival of HIV-positive patients starting antiretroviral therapy between 1996 and 2013: a collaborative analysis of cohort studies. Lancet HIV. 2017;4:e349–56. doi:10.1016/S2352-3018(17)30066-8
11. Serrão R, Piñero C, Velez J, et al. Non-AIDS-related comorbidities in people living with HIV-1 aged 50 years and older: the AGING POSITIVE study. Int J Infect Dis. 2019;79:94–100. doi:10.1016/j.ijid.2018.10.011
12. Croxford S, Kitching A, Desai S, et al. Mortality and causes of death in people diagnosed with HIV in the era of highly active antiretroviral therapy compared with the general population: an analysis of a national observational cohort. Lancet Public Health. 2017;2:e35–46. doi:10.1016/S2468-2667(16)30020-2
13. Smit M, Brinkman K, Geerlings S, et al. Future challenges for clinical care of an ageing population infected with HIV: a modelling study. Lancet Infect Dis. 2015;15:810–818. doi:10.1016/S1473-3099(15)00056-0
14. Haacker M, Bärnighausen T, Atun R. HIV and the growing health burden from noncommunicable diseases in Botswana: modelling study. J Glob Health. 2019;9. doi:10.7189/jogh.09.010428
15. Adeyemi O, Lyons M, Njim T, et al. Integration of non-communicable disease and HIV/AIDS management: a review of healthcare policies and plans in East Africa. BMJ Glob Health. 2021;6:e004669. doi:10.1136/bmjgh-2020-004669
16. Ojagbemi A. Contributions of chronic diseases to measured disability in older adults living in Low/middle income countries: a systematic review with syntheses. Afr J Med Med Sci. 2017;46:19–29.
17. Nachega JB, Hsu AJ, Uthman OA, Spinewine A, Pham PA. Antiretroviral therapy adherence and drug–drug interactions in the aging HIV population. Aids. 2012;26:S39–53. doi:10.1097/QAD.0b013e32835584ea
18. Ahn MY, Jiamsakul A, Khusuwan S, et al. The influence of age‐associated comorbidities on responses to combination antiretroviral therapy in older people living with HIV. J Int AIDS Soc. 2019;22:e25228. doi:10.1002/jia2.25228
19. Abdu M, Ali Y, Anteneh S, et al. Determinant factors for the occurrence of tuberculosis after initiation of antiretroviral treatment among adult patients living with HIV at Dessie Referral Hospital, South Wollo, Northeast Ethiopia, 2020. A case-control study. PLoS One. 2021;16:e0248490. doi:10.1371/journal.pone.0248490
20. World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: Recommendations for a public health approach. World Health Organization; 2016.
21. Melaku T, Mamo G, Chelkeba L, Chanie T. Immunologic restoration of people living with human immunodeficiency virus on highly active anti-retroviral therapy in Ethiopia: the focus of chronic non-communicable disease Co-morbidities. Open AIDS J. 2019;1:13.
22. Palella FJ, Hart R, Armon C, et al. Non-AIDS comorbidity burden differs by sex, race, and insurance type in aging adults in HIV care. Aids. 2019;33:2327–2335. doi:10.1097/QAD.0000000000002349
23. Lenjiso GA, Endale BS, Bacha YD. Clinical and immunological failure among HIV-positive adults taking first-line antiretroviral therapy in Dire Dawa, eastern Ethiopia. BMC Public Health. 2019;19:1–10. doi:10.1186/s12889-019-7078-5
24. Weldemhret L, Aregay A, Bekurtsion H, Gebreegziabher G, Asmelash T, Hagos DG . Pattern of CD4+ T cell recovery and determinants of HIV infected individuals receiving highly active antiretroviral treatment in Mekelle Hospital, Tigray Northern Ethiopia; Retrospective study. 2023. doi:10.21203/rs.3.rs-2470790/v1
25. Asher I, Guri KM, Elbirt D, et al. Characteristics and outcome of patients diagnosed with HIV at older age. Medicine. 2016;95(1):e2327. doi:10.1097/MD.0000000000002327
26. Ocheretyaner E, Yusuff J, Park T. Immunologic and virologic responses to antiretroviral therapy in treatment-naive, HIV-infected elderly patients. Int J STD AIDS. 2019;30:1304–1310. doi:10.1177/0956462419872857
27. Akinyemi JO, Ogunbosi BO, Fayemiwo AS, et al. Demographic and epidemiological characteristics of HIV opportunistic infections among older adults in Nigeria. Afr Health Sci. 2017;17:315–321. doi:10.4314/ahs.v17i2.4
28. Mermin J, Lule J, Ekwaru JP, et al. Effect of co-trimoxazole prophylaxis on morbidity, mortality, CD4-cell count, and viral load in HIV infection in rural Uganda. The Lancet. 2004;364:1428–1434. doi:10.1016/S0140-6736(04)17225-5
29. Bhatta DN, Adhikari R, Karki S, Koirala AK, Wasti SP. Life expectancy and disparities in survival among HIV-infected people receiving antiretroviral therapy: an observational cohort study in Kathmandu, Nepal. BMJ Glob Health. 2019;4:e001319. doi:10.1136/bmjgh-2018-001319
30. Zhang F, Sun M, Sun J, Guan L, Wang J, Lu H. The risk factors for suboptimal CD4 recovery in HIV infected population: an observational and retrospective study in Shanghai, China. Biosci Trends. 2015;9:335–341. doi:10.5582/bst.2015.01107
31. Siraj J, Feyissa D, Mamo Y, et al. Antiretroviral treatment failure and associated factors among HIV patients on the first-line antiretroviral therapy at Mizan-Tepi University teaching hospital, Southwest Ethiopia: a cross-sectional study. Medicine. 2021;100.
32. Yirdaw KD, Hattingh S. Prevalence and predictors of immunological failure among HIV patients on HAART in Southern Ethiopia. PLoS One. 2015;10:e0125826. doi:10.1371/journal.pone.0125826
33. Negash H, Welay M, Legese H, et al. Increased virological failure and determinants among HIV patients on highly active retroviral therapy in Adigrat General Hospital, Northern Ethiopia, 2019: hospital-based cross-sectional study. Infect Drug Resist;2020. 1863–1872. doi:10.2147/IDR.S251619
34. Bulage L, Ssewanyana I, Nankabirwa V, et al. Factors associated with virological non-suppression among HIV-positive patients on antiretroviral therapy in Uganda, August 2014–July 2015. BMC Infect Dis. 2017;17:1–11. doi:10.1186/s12879-017-2428-3
35. Cescon A, Cooper C, Chan K, et al. Factors associated with virological suppression among HIV‐positive individuals on highly active antiretroviral therapy in a multi‐site Canadian cohort. HIV Med. 2011;12:352–360. doi:10.1111/j.1468-1293.2010.00890.x
36. Bayu B, Tariku A, Bulti AB, Habitu YA, Derso T, Teshome DF. Determinants of virological failure among patients on highly active antiretroviral therapy in University of Gondar Referral Hospital, Northwest Ethiopia: a case–control study. HIVAIDS-Res Palliat Care. 2017;153–159. doi:10.2147/HIV.S139516
37. Meshesha HM, Nigussie ZM, Asrat A, Mulatu K. Determinants of virological failure among adults on first-line highly active antiretroviral therapy at public health facilities in Kombolcha town, Northeast, Ethiopia: a case–control study. BMJ Open. 2020;10:e036223. doi:10.1136/bmjopen-2019-036223
38. Emagnu A, Abay Z, Bulti AB, Animut Y. Determinants of virologic failure among adult HIV patients on first-line antiretroviral therapy at waghimra zone, northern Ethiopia: a case-control study. Adv Public Health. 2020;2020:1–8. doi:10.1155/2020/1929436
39. Kazooba P, Mayanja BN, Levin J, Masiira B, Kaleebu P. Virological failure on first-line antiretroviral therapy; associated factors and a pragmatic approach for switching to second line therapy–evidence from a prospective cohort study in rural South-Western Uganda, 2004-2011. Pan Afr Med J. 2018;29:1–16. doi:10.11604/pamj.2018.29.191.11940
40. George S, McGrath N, Oni T. The association between a detectable HIV viral load and non-communicable diseases comorbidity in HIV positive adults on antiretroviral therapy in Western Cape, South Africa. BMC Infect Dis. 2019;19:1–11. doi:10.1186/s12879-019-3956-9
41. Al-Sadi AM, Al-Oweisi FA, Edwards SG, Al-Nadabi H, Al-Fahdi AM. Genetic analysis reveals diversity and genetic relationship among Trichoderma isolates from potting media, cultivated soil and uncultivated soil. BMC Microbiol. 2015;15:1–11. doi:10.1186/s12866-015-0483-8
42. Abebaw A, Taddele M, Alem G, Birlew T. Magnitude of virologic failure and associated factors among adult patients on antiretroviral therapy at Debre Markos Referral Hospital, Northwest Ethiopia, 2018; 2020.
43. Enderis BO, Hebo SH, Debir MK, Sidamo NB, Shimber MS. Predictors of time to first line antiretroviral treatment failure among adult patients living with HIV in public health facilities of Arba Minch Town, Southern Ethiopia. Ethiop J Health Sci. 2019;29:175–186. doi:10.4314/ejhs.v29i2.4
44. Qin S, Lai J, Zhang H, et al. Predictive factors of viral load high-risk events for virological failure in HIV/AIDS patients receiving long-term antiviral therapy. BMC Infect Dis. 2021;21:1–11. doi:10.1186/s12879-021-06162-z
45. Shrestha B, Dunn L. The declaration of Helsinki on medical research involving human subjects: a review of seventh revision. J Nepal Health Res Counc. 2019;17:548–552. doi:10.33314/jnhrc.v17i4.1042
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.