")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
The Impact of COVID-19 Pandemic Lockdown on Emergency Department Visits in a Tertiary Hospital
Authors Shen B, Chen B, Li K, Cheng W, Mofatteh M , Regenhardt RW , Wellington J, Liang Z, Tang Q, Chen J, Chen Y
Received 4 April 2023
Accepted for publication 21 June 2023
Published 19 July 2023 Volume 2023:16 Pages 1309—1316
DOI https://doi.org/10.2147/RMHP.S415704
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Bisheng Shen,1 Baoxin Chen,2 Kuangyi Li,1 Weiyin Cheng,3 Mohammad Mofatteh,4 Robert W Regenhardt,5 Jack Wellington,6 Zhangrong Liang,1 Qi Tang,1 Jingli Chen,1 Yimin Chen7
1Department of Emergency Medicine, Foshan Hospital of Traditional Chinese Medicine, Foshan City, Guangdong Province, People’s Republic of China; 2Faculty of Humanities and Social Sciences, Macao Polytechnic University, Macao, People’s Republic of China; 3Department of Clinical Nutrition, Foshan Hospital of Traditional Chinese Medicine, Foshan City, People’s Republic of China; 4School of Medicine, Dentistry and Biomedical Sciences, Queen’s University Belfast, Belfast, UK; 5Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA; 6School of Medicine, Cardiff University, Cardiff, Wales, UK; 7Department of Neurology and Advanced National Stroke Center, Foshan Sanshui District People’s Hospital, Foshan, People’s Republic of China
Correspondence: Baoxin Chen, Faculty of Humanities and Social Sciences, Macao Polytechnic University, Macao, People’s Republic of China, Email [email protected] Kuangyi Li, Department of Emergency Medicine, Foshan Hospital of Traditional Chinese Medicine, Foshan City, Guangdong Province, People’s Republic of China, Email [email protected]
Purpose: This study aimed to highlight the impact of the COVID-19 pandemic lockdown on emergency department (ED) visits of non-COVID-19 patients in a tertiary hospital and evaluate protocol development during this period.
Patients and Methods: Clinical data of patients who visited the ED of Foshan Hospital of Traditional Chinese Medicine during the first-level response in Foshan, Guangdong province in 2020 (from January 23 to February 24) and the same period in 2019 and 2021 were collected. A retrospective cross-sectional analysis was performed to understand the characteristics of critically ill patients and compare the proportion of hospitalizations, deaths, and emergency ambulance calls (EACs).
Results: The number of patients presenting to the ED was significantly decreased, with a 37.75% reduction in 2020 (6196) compared to the same period in 2019 (9954). A rise in patient ED presentations was observed in the same period in 2021 (10,503). This decline was mostly in the 15– 45 age group. In 2019, 2020, and 2021, critically ill patients treated by the ED totaled 568 (5.706%), 339 (5.495%), and 590 (5.617%), respectively. Compared to the same period in 2019 and 2021, the proportion of critically ill patients with respiratory system involvement, severe trauma, and poisoning decreased most significantly in 2020 (P< 0.05). In contrast, the rates of EACs, hospitalizations, and deaths increased significantly (P< 0.05).
Conclusion: The number of ED visits to hospitals was decreased during the 2020 lockdown, while the rates of EACs, hospitalizations, and deaths increased significantly though there were no documented COVID-19 cases. Optimizing emergency medical resources and ensuring the safety of healthcare providers and patients were essential to provide efficient emergency diagnosis and treatment during the lockdown.
Keywords: COVID-19 pandemic, emergency medicine, coping strategies, emergency visit, non-COVID-19 patients
Introduction
COVID-19 has been globally disseminated throughout China and the world since 2019.1–4 The World Health Organization (WHO) declared the outbreak a public health emergency of international concern on January 30, 2020.5,6 Subsequently, the WHO named infectious pneumonia caused by this virus COVID-19 on February 11, 2020,7 and declared pandemic status on March 11, 2020.8 Highly contagious COVID-19 results in systemic multi-organ dysfunction,9,10 and is transmitted between humans through droplets and close contact.11 Public health emergencies caused by COVID-19 have had a serious negative global impact. China implemented unprecedented public health measures to control the rapid spread of COVID-19, including suspending public transportation, closing public spaces, closely monitoring communities affected by the pathogen, and isolating infected and exposed individuals.12 Foshan officially entered a state of lockdown from January 23 to February 24, 2020, when Guangdong launched a first-level response to this major public health emergency. The number of patients in the ED decreased significantly due to strict prevention and control measures alongside public concern about contracting COVID-19 during this response period. As a comprehensive tertiary hospital located in the prefecture-level city of Guangdong Province, the Foshan Hospital of Traditional Chinese Medicine was considered the major anti-COVID-19 hospital in Foshan. Most outpatient and inpatient hospital departments significantly reduced their routine medical services while the ED provided 24-hour healthcare services. The staff worked diligently to provide patients with timely and appropriate care while protecting themselves and others from the risk of infection. They also played a major role in providing guidance and support to the community during the pandemic. The hospital, fortunately, maintained a zero positive case count for COVID-19 during this period.
Recent studies suggested that COVID-19 diagnosis was associated with higher stroke mortality.13 Life-threatening consequences can occur if such diseases are not treated in time.
Research suggests preservation in stroke care of higher severity of disease through the first pandemic year.14 A study pointed out that the focus is not only on interventionist support in the ED, but also on workflow optimization and improving patient outcomes by assessing the emergency systems and response times in hospitals.15 Multidisciplinary collaboration and continuous workflow optimization may maintain stroke care during the COVID-19 pandemic lockdown.16 Our study aimed to explore changes in patient characteristics in the ED of our hospital during the first-level response to the COVID-19 pandemic when the city was under strict lockdown by comparing the patient characteristics to similar periods in the previous and subsequent years. We analyze changes in patient characteristics and propose protocols for the optimization of emergency treatment processes as well as resource allocation. These demonstrate the role of emergency medicine in responding to public health emergencies and provide strategies for the prevention and control of potential emerging infectious diseases.
Materials and Methods
This study was a retrospective cross-sectional study. Daily patient’s data were collected and analyzed. General patient information, including name, gender, age, and visit areas (eg, medical emergency room, trauma center emergency room, intensive care unit), was recorded for all patients in emergency pre-triage. In addition, we also recorded the time of arrival, route of admission, emergency ambulance calls (EACs), diagnosis, category of illness, and patient mortality.
Data Collection
Basic clinical information of ED patients was collected from January 23 to February 24 for the same period from 2019 to 2021, including gender, age, the number of critically ill patients, and the disease classification system. Computer systems enable data collection, and diseases diagnosis more effectively and accurately.17 These were analyzed using the emergency workstation system, emergency pre-examination triage system, and EXCEL registration reports of patients from different areas of the ED. The emergency pre-examination triage system based on RETTS18 classifies all patients in the ED according to the severity of their illness by categorizing them into grades I (Red, emergency), II (Orange, urgent), III (Yellow, less urgent), and IV (Green, not urgent). To avoid incorrect classification of critically ill patients who were not admitted to the intensive care unit (ICU) or did not accept emergency treatment, healthcare professionals reviewed the patient data from different ICU units separately. Inclusion criteria for critically ill patients were: 1. Grade I/II patients assessed by professionally trained medical staff; 2. Grade III patients were admitted to the emergency ICU after being examined by professionally trained medical staff. Exclusion criteria were: 1. Patients younger than 14 years old; 2. Grade IV patients who were assessed by professionally trained medical staff; 3. Grade III patients who did not qualify to be admitted to the emergency ICU or referred to fever clinic after assessment by professional trained medical staff; 4. Critically ill patients who did not enter the emergency ICU for treatment or did not accept the emergency ICU treatment process provided. Written informed consent was not required to participate in this study per the national legislation and institutional requirements.
Statistical Analysis
The present study’s data are descriptive of the gender, age, number of critically ill patients, and the disease classification system. Study data were expressed by percentage, and a Chi-square test was used to detect any significant difference between the categorical variables. Then pairwise comparisons were performed to further analyze the disease classifications for critically ill patients presenting via the ED from different periods. SPSS22.0 software was performed to analyze the data. P<0.05 was considered statistically significant.
Results
The number of patients presenting to the ED significantly decreased by 37.75% in 2020 (6196) compared to the same period in 2019 (9954) and increased in 2021 (10,503) (Table 1 and Figure 1).
 |
Table 1 Comparison of Gender and Age of Emergency Patients from January 23 to February 24, 2019, 2020 and 2021 |
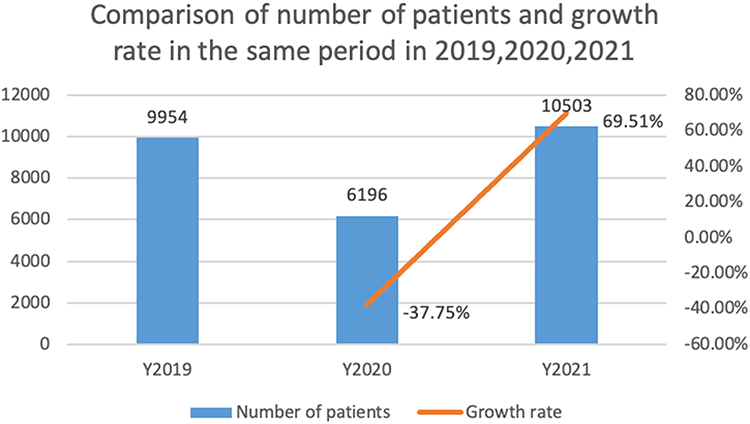 |
Figure 1 Comparison of the number of patients and growth rate presenting to the ED in the same period in 2019, 2020, and 2021. |
Across all three years, there were slightly more male patients than females (53.96%, 52.13%, and 53.02%), with no statistically significant differences in the gender composition for any year (χ2=5.246, P=0.073). Comparing different age groups, 15–45-year-old patients (2019: 44.32%, 2020: 41.81%, and 2021: 44.94%) were more prevalent, with the proportion decreasing as the age increased (Table 1). There were statistically significant differences in the proportions of the 15–45 age group in the three stages (χ2=16.239, P<0.001). Further analysis showed that there were a significant difference between 2020 with the same period in 2019 (χ2=9.833, P=0.002) or 2021 (χ2=17.415, P<0.001), while there were no differences between 2019 and 2021 (χ2=0.784, P=0.376).
In 2019, 2020, and 2021, the number of critically ill patients treated by the ED was 568 (5.706%), 339 (5.495%), and 590 (5.617%), respectively (Figure 2). The absolute number of critically ill patients in 2020 was less compared with the same period in 2019 and 2021. However, there was no statistically significant difference in the proportion of critically ill patients presenting via the ED in the same period across years (χ2=0.3204, P>0.05).
 |
Figure 2 The number of critically ill patients managed by the ED across the three years. |
Comparing the three years, the number of patients with respiratory diseases, severe trauma, and poisoning decreased significantly in 2020 compared with the same period in 2019 and 2021 (Table 2). Patients with diseases of the respiratory system accounted for 10.03% in 2020, 14.96% in 2019, and 15.08% in 2021, while severe trauma 3.24%, 7.57%, 8.14%, and poisoning 1.77%, 8.63%, 7.97%, respectively. There were no significant differences in endocrinological diseases between 2019, 2020, and 2021 (χ2=1.151, P=0.563). However, the proportion in 2020 was significantly higher than that in 2021, accounting for 10.03% and 6.10% (P=0.038). Finally, there was no statistically significant difference in the proportion of other disease classification systems (P>0.05). The information in Table 2 is summarized in Figure 3.
 |
Table 2 Comparison of Disease Classifications for Critically Ill Patients Presenting via the ED from January 23 to February 24, 2019, 2020, and 2021 |
 |
Figure 3 Comparison of disease classifications for critically ill patients presenting via the ED from January 23 to February 24, 2019, 2020, and 2021. |
We compared the number of EACs, hospitalizations, and deaths from January 23 to February 24 across three years (Table 3). Analyzing the number of EACs, hospitalizations, and deaths in 2020 compared with the same period in 2019 and 2021, the proportion of EACs, hospitalizations, and deaths in 2020 increased significantly (P<0.05 for each comparison). There were no statistically significant differences in the proportion of EACs, hospitalizations, and deaths comparing 2019 and 2021 (all P >0.05).
 |
Table 3 Comparison of the Number of EACs, Hospitalizations, and Deaths from January 23 to February 24, 2019, 2020, and 2021 |
Discussion
COVID-19 has evolved to become a pathogen of international public health concerns and a pandemic.7,8,19,20 Emergency medical services are facing unprecedented challenges during the COVID-19 pandemic,21 and the number of acutely ill patients, such as those with stroke and myocardial infarction, have demonstrated a significant decline.22–24 At present, the COVID-19 prevention and control situation in China continues to improve, but the fight against the epidemic continues.
In this study, we showed that the total number of patients in the ED of our hospital from January 23 to February 24 in 2019, 2020, and 2021 was 9954, 6169, and 10,503, respectively. There were no statistically significant differences in the gender of ED patients across the three years (P>0.05). Patients aged 15–45 years accounted for the largest proportion. There were differences in the proportions of age groups comparing the three years, with the most significant decrease in the number of patients aged 15–45 in 2020. There are several possible explanations for these observations. First, patients in the 15–45 age group are typically healthier, and most grade IV patients without underlying health conditions could utilize self-treatment or telemedicine approaches to their care. In addition, compared with the elderly, people in this age group are more likely to be informed, which may increase caution and fear, thus reducing ED visits.
Since COVID-19 began, some experts have raised concerns about the decline in ED visits, stating that the reduction in ED visits may threaten global health, causing delayed diagnoses and management leading to unnecessary worsened prognoses and death.25 Our study demonstrated that the overall number of emergency visits decreased from January 23 to February 24, 2020. However, no statistically significant difference in the proportion of critically ill patients (P>0.05). In terms of disease classification among critically ill patients, those with nervous system and cardiovascular system disorders accounted for the highest proportion across the three years, with no statistical significance comparing years (P>0.05). This can be attributed to the establishment of our stroke and chest pain centers as leading units of prefecture-level city hospitals. Such patients were transferred by ambulance to our hospital and were also referred by other community hospitals in the city.
In addition, from January 23 to February 24, 2020, the number of critical patients with respiratory diseases, severe trauma, and poisoning in the ED of our hospital were only 34 cases, 11 cases, and 6 cases, respectively, far fewer than in the same period in 2019 and 2021. Compared with the proportion in the same period in 2019 and 2021, such differences were statistically significant (P <0.05). Strict pandemic regulations likely reduced the number of patients suffering from respiratory diseases and traumatic diseases such as falls, traffic accidents, mechanical injuries, as well as poisoning.26,27 However, for patients with severe endocrinological diseases, the proportion in 2020 increased significantly compared with the same period in 2021 (P<0.05). This observation may be related to the suspension of outpatient services in our hospital during that period. Such patients with diabetes mellitus who could not monitor their blood glucose properly and were not adherent to medications faced diabetic complications and required ED treatment. It is possible that at the same time, lack of physical activity and staying at home could have been contributory, leading to blood sugar fluctuations.
Based on this analysis, the public health emergency caused by COVID-19 did not alter the proportion of critically ill patients seeking emergency medical attention during the first-level response phase, while the overall number of emergency visits decreased significantly. This is closely related to the significant increase in the number of EACs, hospitalizations, and deaths in our hospital in 2020 compared with the same period during 2019 and 2021 (all P < 0.05). There is an inseparable relationship between the number of critically ill patients, EACs, admissions, and deaths. Ambulance services are most often utilized for critically ill patients, thus increasing relatively the proportion of admissions, ED deaths, and pre-hospital deaths.
Hospitals can manage patients more effectively through multidisciplinary collaboration and workflow optimization.28 Given the data presented above, we propose the following protocols and coping strategies to optimize emergency medical resources, improve emergency provider retention, and ensure the safety of healthcare providers and patients.
Proposed protocols and coping strategies include: 1) Implementation of emergency pre-examination and triage system: Previous studies showed that a reasonable emergency pre-examination triage system could effectively reduce the waste of medical resources during COVID-19.29 2) Strengthening public information dissemination and education. 3) Construction of a fever clinic: Suspected COVID-19 patients were treated separately in the fever clinic, which reduced the risk of infection in ED.30 4) Medical staff training and health management. 5) Emergency department prevention and control layout: The ICU space was expanded in our hospital, and the bed capacity was increased by 200% to improve the crowding caused by the epidemic. Second, we temporarily converted some of the general inpatient wards into observation rooms and converted transitional isolation single rooms for patients with suspected COVID-19 infection. Third, given the significant decrease in severe trauma and acute poisoning, the emergency trauma room debridement area was temporarily transformed into an operating room for patients with suspected major COVID-19 trauma. 6) Custodial services staff regularly disinfected air, ground, and other equipment throughout the ED. 7) Simplification of the outpatient treatment process and emergency hospitalization process.
Limitations and Expectations
There are limitations to our study. First, the data were only from the ED of one hospital, and the sample size was small. Second, the retrospective study of electronic medical records has certain subjectivity to the results, which may increase the error information.
Conclusion
In conclusion, while the WHO has declared that COVID-19 no longer constitutes an “international public health emergency”, potential pandemics in the future would require the government to implement healthcare measures, including lockdowns. Our study suggests that inadequate awareness training in critically ill patients leads to an increase in the number of deaths associated with increased access barriers. People in critical condition should be encouraged to receive medical attention. In addition, the government’s deficiencies in the health management of chronic diseases should be addressed, and chronically ill patients should have channels to access medications. Multi-disciplinary collaboration based on the lessons learned from the current pandemic can prepare us for future global health disasters.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Foshan Hospital of Traditional Chinese Medicine institutional review board. Written informed consent was not required to participate in this study per the national legislation and institutional requirements. All patient information remains anonymous in compliance with patient confidentiality regulations. The study was conducted in accordance with the 1964 Helsinki Declaration or comparable standards. All authors are consent and approved for manuscript publication.
Acknowledgments
We would like to thank our patients for their contributions. In addition, we would like to extend our gratitude to reviewers and editors for their comments to help improve our manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the High-Level Medical Key Specialty Project in the 14th Five-Year Plan of Foshan City (FSGSPZD145098).
Disclosure
Dr Robert W Regenhardt reports personal fees from Rapid Medical, grants from National Institutes of Health, grants from Society of Vascular and Interventional Neurology, grants from Heitman Foundation for Stroke, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/s0140-6736(20)30183-5
2. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/s0140-6736(20)30211-7
3. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with Pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa2001017
4. Mohapatra RK, Pintilie L, Kandi V, et al. The recent challenges of highly contagious COVID-19, causing respiratory infections: symptoms, diagnosis, transmission, possible vaccines, animal models, and immunotherapy. Chem Biol Drug Des. 2020;96(5):1187–1208. doi:10.1111/cbdd.13761
5. World Health Organization. Clinical management of severe acute respiratory infection when novel coronavirus (2019-nCoV) infection is suspected: interim guidance; 2020. Available from: https://apps.who.int/iris/handle/10665/330893.
6. World Health Organization. 2019-nCoV outbreak is an emergency of international concern; 2020. Available from: http://www.euro.who.int/en/health-topics/emergencies/pages/news/news/2020/01/2019-ncov-outbreak-is-an-emergency-of-international-concern.
7. World Health Organization. Coronavirus Disease 2019 (COVID-19) pandemic; 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
8. Göktuğ A, Güngör A, Öz FN, et al. Evaluation of epidemiological, demographic, clinical characteristics and laboratory findings of COVID-19 in the pediatric emergency department. J Trop Pediatr. 2021;67(4). doi:10.1093/tropej/fmab066
9. Renu K, Prasanna PL, Valsala Gopalakrishnan A. Coronaviruses pathogenesis, comorbidities and multi-organ damage - a review. Life Sci. 2020;255:117839. doi:10.1016/j.lfs.2020.117839
10. Bajgain KT, Badal S, Bajgain BB, Santana MJ. Prevalence of comorbidities among individuals with COVID-19: a rapid review of current literature. Am J Infect Control. 2021;49(2):238–246. doi:10.1016/j.ajic.2020.06.213
11. Bao L, Gao H, Deng W, et al. Transmission of severe acute respiratory syndrome coronavirus 2 via close contact and respiratory droplets among human angiotensin-converting enzyme 2 mice. J Infect Dis. 2020;222(4):551–555. doi:10.1093/infdis/jiaa281
12. Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
13. Nguyen TN, Qureshi M, Klein P, et al. Global impact of the COVID-19 pandemic on cerebral venous thrombosis and mortality. J Stroke. 2022;24(2):256–265. doi:10.5853/jos.2022.00752
14. Nguyen TN, Qureshi MM, Klein P, et al. Global impact of the COVID-19 pandemic on stroke volumes and cerebrovascular events: a 1-year follow-up. Neurology. 2023;100(4):e408–e421. doi:10.1212/WNL.0000000000201426
15. Yang S, Yao W, Siegler JE, et al. Shortening door-to-puncture time and improving patient outcome with workflow optimization in patients with acute ischemic stroke associated with large vessel occlusion. BMC Emerg Med. 2022;22(1):136. doi:10.1186/s12873-022-00692-8
16. Chen Y, Nguyen TN, Siegler JE, et al. The impact of COVID-19 pandemic on ischemic stroke patients in a comprehensive hospital. Risk Manag Healthc Policy. 2022;15:1741–1749. doi:10.2147/RMHP.S380691
17. Bord S, Tur-Sinai A, Basis F. High non-COVID-19 in-hospital deaths during the first lockdown in Israel compared with the second and third lockdowns. Int J Environ Res Public Health. 2022;19(20):13134. doi:10.3390/ijerph192013134
18. Nissen L, Kirkegaard H, Perez N, Hørlyck U, Pape L. Inter-rater agreement of the triagesystem RETTS-HEV. Scand J Trauma Resusc Emerg Med. 2013;21(2):A32. doi:10.1186/1757-7241-21-S2-A32
19. Mishra S. Designing of cytotoxic and helper T cell epitope map provides insights into the highly contagious nature of the pandemic novel coronavirus SARS-CoV-2. Royal Soc Open Sci. 2020;7(9):201141. doi:10.1098/rsos.201141
20. Wang Q, Zhang T, Zhu H, et al. Characteristics of and public health emergency responses to COVID-19 and H1N1 outbreaks: a case-comparison study. Int J Environ Res Public Health. 2020;17(12). doi:10.3390/ijerph17124409
21. Albrecht R, Knapp J, Theiler L, Eder M, Pietsch U. Transport of COVID-19 and other highly contagious patients by helicopter and fixed-wing air ambulance: a narrative review and experience of the Swiss air rescue Rega. Scand J Trauma Resusc Emerg Med. 2020;28(1):40. doi:10.1186/s13049-020-00734-9
22. Nogueira RG, Qureshi MM, Abdalkader M, et al. Global impact of COVID-19 on stroke care and IV thrombolysis. Neurology. 2021;96(23):e2824. doi:10.1212/WNL.0000000000011885
23. Nogueira RG, Abdalkader M, Qureshi MM, et al. Global impact of COVID-19 on stroke care. Int J Stroke. 2021;16(5):573–584. doi:10.1177/1747493021991652
24. Nguyen TN, Haussen DC, Qureshi MM, et al. Decline in subarachnoid haemorrhage volumes associated with the first wave of the COVID-19 pandemic. Stroke Vasc Neurol. 2021;6(4):542–552. doi:10.1136/svn-2020-000695
25. Boserup B, McKenney M, Elkbuli A. The impact of the COVID-19 pandemic on emergency department visits and patient safety in the United States. Am J Emerg Med. 2020;38(9):1732–1736. doi:10.1016/j.ajem.2020.06.007
26. Descamps AK, Vandijck DM, Buylaert WA, Mostin MA, Paepe P. Characteristics and costs in adults with acute poisoning admitted to the emergency department of a university hospital in Belgium. PLoS One. 2019;14(10):e0223479. doi:10.1371/journal.pone.0223479
27. Mbarouk GS, Sawe HR, Mfinanga JA, et al. Patients with acute poisoning presenting to an urban emergency department of a tertiary hospital in Tanzania. BMC Res Notes. 2017;10(1):482. doi:10.1186/s13104-017-2807-2
28. Chen Y, Nguyen TN, Wellington J, et al. Shortening door-to-needle time by multidisciplinary collaboration and workflow optimization during the COVID-19 pandemic. J Stroke Cerebrovasc Dis. 2022;31(1):106179. doi:10.1016/j.jstrokecerebrovasdis.2021.106179
29. Ledvina A, Otero R, Hamilton J, et al. Preliminary report of drive-through screening COVID-19 screening process in a large suburban community. Int J Emerg Med. 2021;14(1):17. doi:10.1186/s12245-021-00340-1
30. Chen SC, Chang K, Kuo CH. Emergency department infection control strategies in response to COVID-19. Kaohsiung J Med Sci. 2020;36(7):568–569. doi:10.1002/kjm2.12243
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.