")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
The Frequency and Predictors of Sexual Dysfunction Among People Living with HIV/AIDS
Authors Abdu Z , Dule A , Habib S
Received 28 September 2023
Accepted for publication 18 December 2023
Published 21 December 2023 Volume 2023:15 Pages 729—737
DOI https://doi.org/10.2147/HIV.S436966
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Zakir Abdu,1 Aman Dule,1 Sadik Habib2
1Department of Psychiatry, Mattu University, Mattu, Oromia, Ethiopia; 2Department of Family Health, Mattu Health Science College, Mattu, Oromia, Ethiopia
Correspondence: Zakir Abdu, Tel +251913845371, Email [email protected]
Background: The frequency of sexual dysfunctions reported by HIV/AIDS patients is significantly higher than that of their peers. Sexual dysfunction and its predictors may result in increased viral loads, worsening HIV infection, and infectivity. To mitigate its consequences, appropriate evaluation and intervention are required.
Methods: A cross-sectional study design was conducted among 336 HIV/AIDS-positive individuals at one hospital in southwest Ethiopia. To assess sexual dysfunctions, a tool called the Changes in Sexual Functioning Questionnaire (CSFQ-14) was used. Data analysis was done with SPSS version 20. Bivariate and multivariable logistic regressions were used to identify independent predictor variables, and statistical significance was declared at a p-value of < 0.05.
Results: 98.53% of the sample completed the questionnaire accordingly. The frequency of SD was 72.0% (95% CI = 67.4– 77.0). The frequency of SD was reported to be more prevalent among males (76.8% (95% CI = 70.6– 81.6)) than that of females (66.2% (95% CI = 59.5– 73.5)). Among the domains of sexual dysfunction, sexual pleasure problems (96.70%, (95% CI: 94.60– 98.50)) were the higher figure of SD, and sexual desire problems (82.40%, (95% CI: 78.60– 86.60)); were the least prevalent sexual dysfunctions. Predictors of the SD were age, social anxiety, nicotine use, poor sleep quality, and time of resuming ART medication.
Conclusion: The frequency of SD was 72.0%. Predictors of the SD were age, social anxiety, nicotine use, poor sleep quality, and time of resuming ART medication.
Keywords: SD, PLWH, Ethiopia
Background
Sexual dysfunctions (SDs) have a negative impact on the individual’s quality of life, self-esteem, and interpersonal relationships.1–3 Often, it is the cause of psychopathological disorders.3 Currently, SDs are a highly prevalent public health problem.3,4 Globally, SDs are more common among human immunodeficiency virus/acquired immunodeficiency syndrome-positive (HIV/AIDS-positive) individuals than age-matched HIV-negative individuals.5 The five categories of SDs include orgasmic, desire, arousal, sexual pain, and pleasure disorders.6 Sexual desire issues, orgasmic dysfunction, and sexual pain disorders are all commonly recognized.7,8
People living with HIV/AIDS (PLWH) face barriers to sexual exercise due to stigma.9 Also, there might be a lack of compliance with medication and a rise in risky sexual behavior in those groups.10 In addition, it is accountable for psychopathological disturbances and a lower quality of life,3 unsafe sexual practices that predict SDs can result in a higher HIV viral load in their body and increased viral load in the seminal fluid, increasing their risk of HIV transmission.5 The severity of HIV infection and infectivity is worsened by this increased viral load.11
SD is a result of multiple factors, which include hormonal changes, psychological disturbances, and factors associated with organ diseases such as vascular diseases, chronic diseases, and substance use.5 In addition, common predictors of SDs among PLWH include individual general lifestyle factors such as substance misuse, medical-related factors such as having a history of anxiety symptoms, duration of HIV medication, and socio-demographic conditions such as age, sex, and marital status.1,3,4,12 The prediction of erectile dysfunction was found in seven European HIV treatment centers to be older age, use of psychotropic medication, and long-term ARV treatment. There was a significant increase in risk of dysfunction in the quadrant with the longest exposure.2,3 A report confirms that the risk of SDs was inversely correlated with the educational level.3
SDs in HIV-positive patients may be due to metabolic complications, including hyperlipidemia or dyslipidemia, psychological, cognitive, and endocrine disorders, among other factors.5,13,14 According to the participants, they experienced depression, anger, and anxiety after knowing that they had HIV, not after starting antiretroviral therapy. SD was reported by the participants after experiencing these symptoms.6 Another complication of HIV/AIDS is dementia related to HIV/AIDS15 and results in sexual behavior that is inappropriate. Psychosocial therapy may be of benefit to individuals with HIV.16
There is still a lack of research and management of related issues pertaining to SD in African countries,11 despite the many studies on SDs in PLWH that have been conducted in developed countries.7,8 There are no SDs in PLWH data in the study area. In order to address the numerous detrimental effects of SDs and enhance the health of the impacted populations, it is crucial that the current study provide key recommendations. This study’s goal was to evaluate the frequency and predictors of sexual dysfunction in HIV/AIDS patients at a single hospital in southwest Ethiopia.
Methodology
Study Area
In a single hospital in southwest Ethiopia, the study was conducted. Currently, the hospital serves as a referral facility for a few areas of Gembela, the Southwest region, and the Oromia region. The ART clinic at this hospital is currently providing care to 1600 people in total. About 25 to 35 people typically make a daily visit to the clinic.
Study Period and Design
The design was cross-sectional, and the data were gathered between May 1 and May 30, 2020.
Study population
Every HIV/AIDS-positive person receiving treatment during the time of data collection.
Sample Size Determination
A 50% proportion was chosen because, as far as we could tell while reviewing the literature, there was no national research article on SDs among PLWH that had been published. The sample size was 341 using the single population proportion formula, 95% CI, a 5% marginal error, and an addition of 10%.
Sampling Procedure
This study used systematic sampling as its methodology. The participants were chosen for inclusion based on predetermined criteria, and in the event that an individual declined to participate, other participants were assigned in their place. The division of the entire population (1600) by the sample (341), yielded the sampling interval (≈ 5).
Data Collection Tools
A face-to-face interview and a structured questionnaire were used to gather data. Other psychosocial variables as well as sociodemographic data (age, sex, marital status, religion, level of education, employment status, and living arrangement) were included in the questionnaire. SDs were evaluated using the Change in Sexual Functioning Questionnaire (CSFQ-14), which has separate forms for men and women (CSFQ-Male Clinical Version and CSFQ-Female Clinical Version). The purpose of the 14-item CSFQ is to determine whether study participants have any sexual problems. Using a 5-point Likert scale, the CSFQ-14 gives the patient the chance to assess their own sexual behaviors and issues in a number of areas. Higher scores correspond to higher sexual functioning for all items.17 The female version of the CSFQ-14 has a Cronbach’s α of 0.897 and the male version has an α of 0.910 in the current study. To determine if low quality of sleep was present or not, the Pittsburgh Sleep Quality Index (PSQI) was utilized. Evaluating the presence or absence of poor sleep quality is legitimate and trustworthy.18 Adults’ sleep patterns and quality can be measured with the PSQI, an efficient tool. Seven domains are measured in order to distinguish between “good” and “poor” sleep: subjective sleep quality, sleep latency, duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and dysfunction during the previous month’s daytime hours. Each of these seven categories of sleep is self-rated by the respondent. The responses are scored on a 0–3 scale, where 3 represents the Likert scale’s negative extreme. A “poor” sleeper is indicated by a global sum of “5” or higher.18 The PSQI is the most extensively utilised validated tool in clinical and research contexts for evaluating the overall quality of sleep that HIV-positive individuals get.19 To measure social anxiety, the Social Phobia Inventory (SPIN) was employed. Based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria, a clinical confirmation of the diagnosis of social anxiety disorder is suggested if the total score is greater than 19, and there is associated dysfunction in work, home, or social settings.20 Nigeria was the location of SPIN’s validation. The SPIN’s sensitivity was 82.2%, and its specificity was 77.6%. Each of the predictive values, positive and negative, was 80%.21 Tobacco dependence was measured using the Fagerstrom Test for Nicotine Dependence (FTND). The FTND is a structured questionnaire with six items that is given by an interviewer and has a total score that ranges from 0 to 10. It is used to measure nicotine dependence.22 At a cut-off score of ≥ 5, which was considered to indicate tobacco dependence, the FTND has good sensitivity and specificity (0.75 and 0.80, respectively).23
The Dependency Scale (DS) severity was utilized to evaluate the condition of Khat use disorder. It is a screening tool for Khat use disorder, which is classified as such in the DSM-5.24 A quick and easy screening tool called DS was validated in Ethiopia to identify people with high rates of negative consequences associated with their use of Khat and who fit the description of a person with a Khat use disorder syndrome. A 4-point rating system (0–3) is used for each of the five items. The 5-item ratings are added together to determine the final score.25,26
Using the four-item CAGE questionnaire (Cut down, Annoyed, Guilty, Eye-opener), alcohol use disorders (AUDs) were evaluated. CAGE is brief and simple to use in medical settings. At a cut-off score of less than 2, CAGE’s sensitivity and specificity were 0.91 and 0.90, respectively.27–29 For the purposes of this study, an alcohol use disorder will be identified in males and females with a total CAGE score of ≥ 2 and ≥ 1, respectively.
The questionnaire in the English language was translated into Amharic and Afan Oromo and back to English by an independent person to check for consistency and understandability of the tool.
Analysis of Data
Following the acquisition of all required data, the data were examined for accuracy. After being modified, cleared, and coded, the data were added to EpiData version 3.1. Version 20.0 of SPSS was used to analyze the data that were gathered. Basic descriptive statistics were employed for the data analysis. A bivariate analysis was performed to assess the association’s significance. In order to account for confounders, variables exhibiting strong associations in bivariate analysis were added to multivariate logistic regressions. The adjusted odds ratio, with a p-value of 0.05, was used to indicate the significance of the association.
Ethics Approval and Consent to Participate
The Helsinki Declaration was followed in the conduct of this investigation. The Mattu University Institutional Research Ethics Review Committee granted ethics approval. Next, the College of Health Sciences provided the authorization letter. The chosen subjects were invited to participate after being made aware of the nature, objectives, advantages, and drawbacks of the research. All pertinent issues were brought up, and privacy was guaranteed. Every participant signed a written informed consent form indicating that their participation was completely voluntary and had no financial or other motivation. Participants’ absolute right to withdraw or refuse to continue at any time was duly observed.
Results
Participants’ Characteristics
336 of the 341 samples finished every task. Most of them were married, male, living in cities, and practicing orthodox religion (Table 1). 185 (55.1%) of them had been HIV positive for more than 7.8 years. Of the participants, 51.8% had started ART for less than 6.8 years (Table 2).
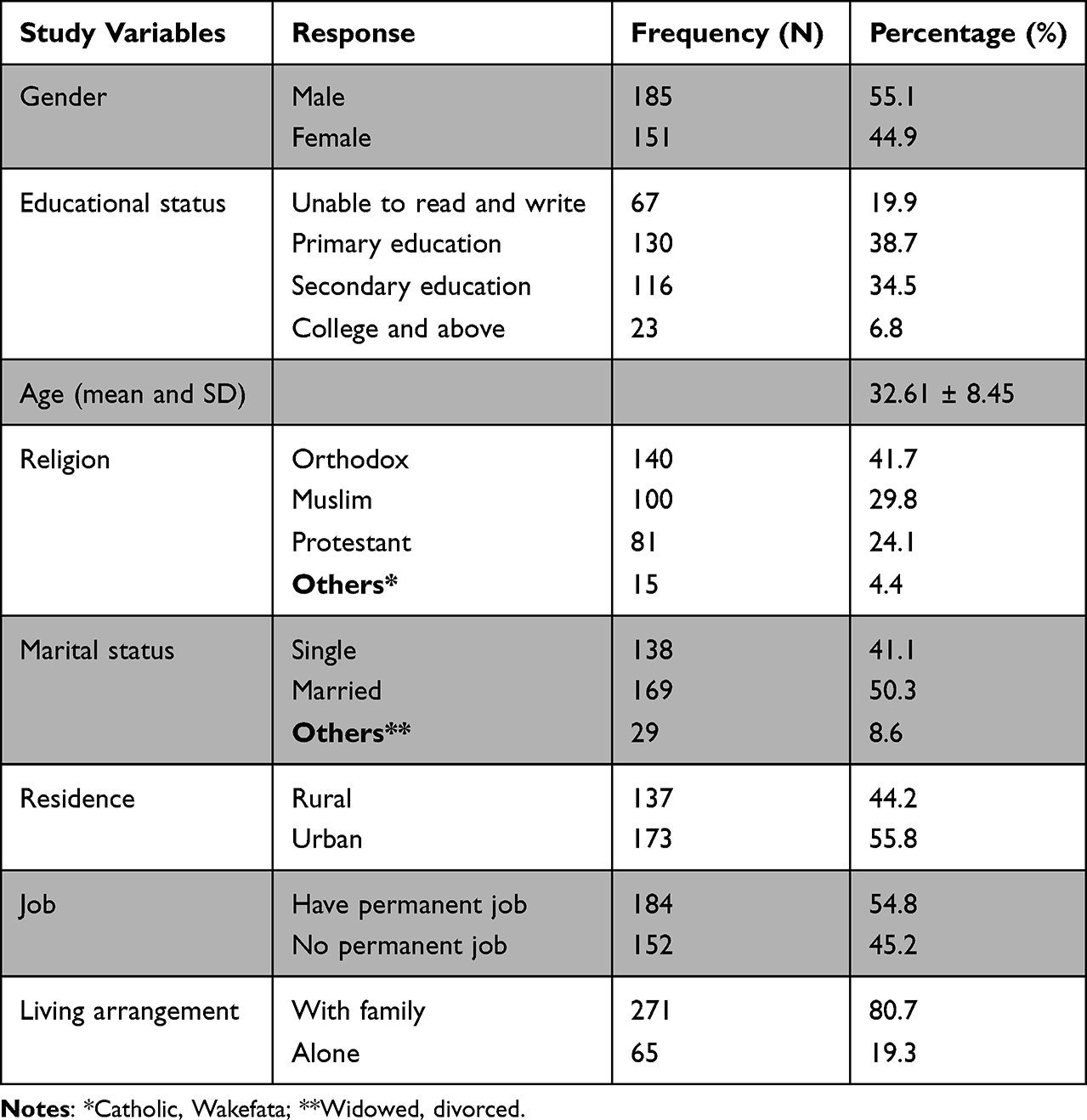 |
Table 1 Background Characteristics of Study Participants Among PLWH, South West Ethiopia, May 2020 (N=336) |
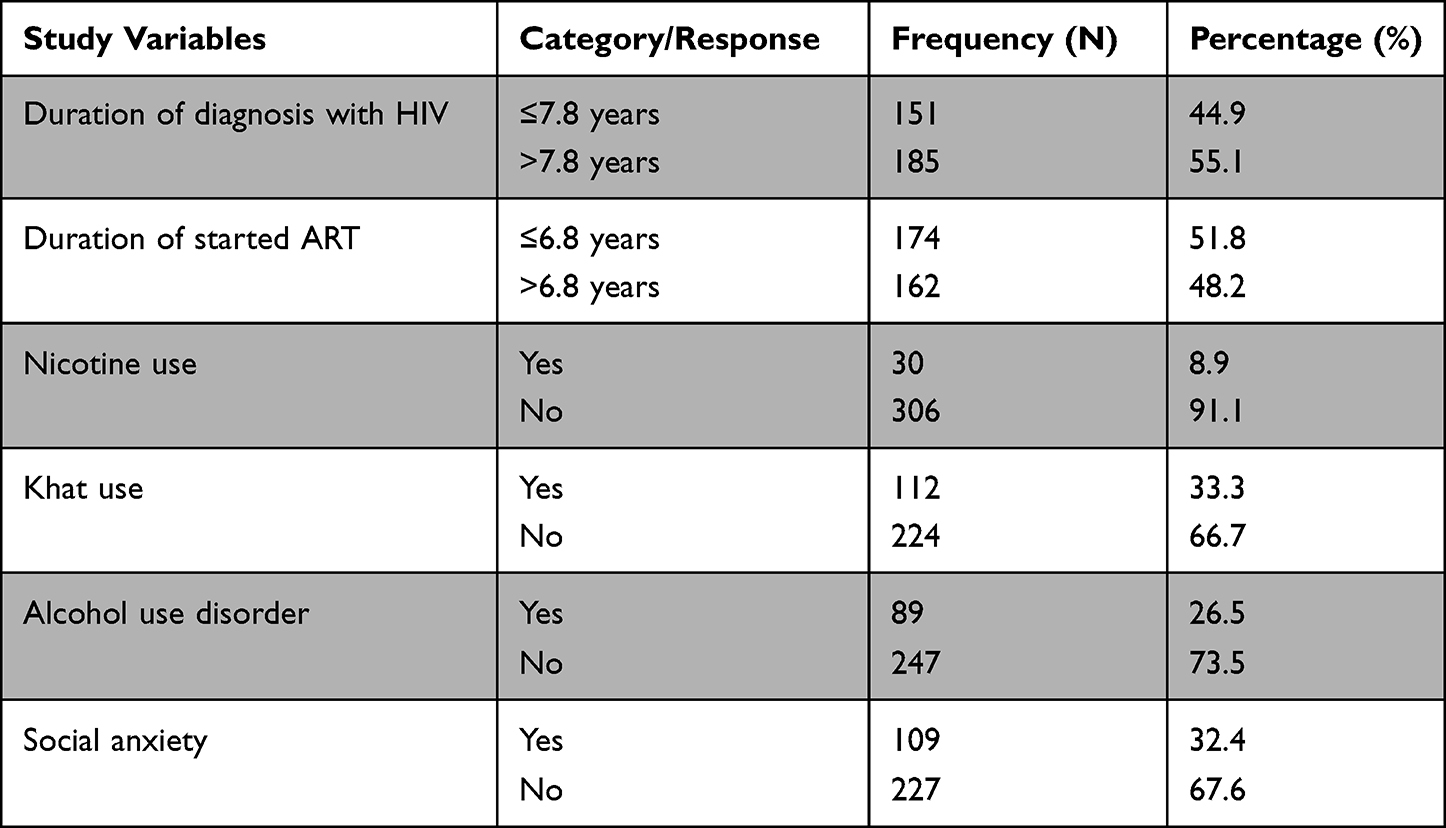 |
Table 2 HIV-Related Clinical Characteristics of Study Participants Among PLWH, South West Ethiopia, May 2020 (N=336) |
Frequency of SD in Individuals Having HIV/AIDS
In people living with HIV/AIDS, the frequency of SD was 72.0% (95% CI = 67.4–77.0). Males have a higher prevalence of it (76.8%, 95% CI = 70.6–81.6) than females do (66.2%, 95% CI = 59.5–73.5).
Frequency of Each Domain of Sexual Dysfunction
Compared to other domains, PLWH have a higher frequency of sexual pleasure problems (96.70%, 95% CI: 94.60–98.50) and a lower frequency of sexual desire problems (82.40%, 95% CI: 78.60–86.60) in each domain.
Frequency of Domains of Sexual Dysfunction by Sex
In terms of sexual dysfunction in both sex categories, the sexual pleasure problem is the most common and highest: 96.2% (95% CI; 93.3, 98.6) for men and 97.4% (95% CI; 94.7, 100) for women. The sexual desire problem is the least common: 80.0% (95% CI; 74.1, 85.9) for men and 85.4% (95% CI; 80.7, 92.1) for women (Figure 1).
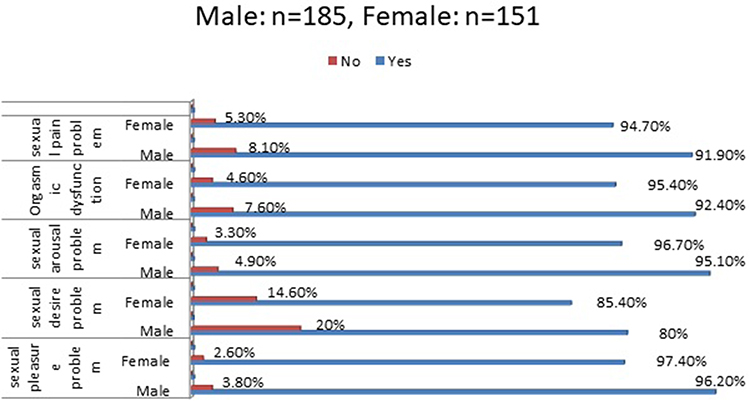 |
Figure 1 Frequency of sexual dysfunction in each domain by sex among PLWH at one hospital in southwest Ethiopia. |
Predictors of SD in Persons Who Have HIV/AIDS
A permanent job, place of residence, marital status, level of education, type of housing, time after HIV/AIDS diagnosis, and alcohol consumption have not been found to be significantly correlated with SD in the binary regression. Nevertheless, the multivariable regression does not reveal any correlation between khat use and sexual dysfunction; rather, it only serves as a predictor for the former in the binary analysis.
Sexual dysfunction was found to be predicted by age, social anxiety, nicotine use, poor sleep quality, and the length of time since ART initiation, according to multivariable logistic regression analysis. Age was found to have a statistically significant correlation with SD, according to the study. Participants aged 27–29 years had odds of SD approximately 66% lower than those aged 18–26 years (AOR = 0.34, 95% CI: 0.15–0.78). The results of the study indicated a statistically significant correlation between SD and social anxiety. In this instance, individuals with social anxiety had 2.54 times higher odds of SD [AOR=2.54 (1.32, 4.91)] than those without it. According to the study, participants with a history of nicotine use had 4.07 times higher odds of having SD [AOR=4.07 (1.10, 15.02)] (Table 3).
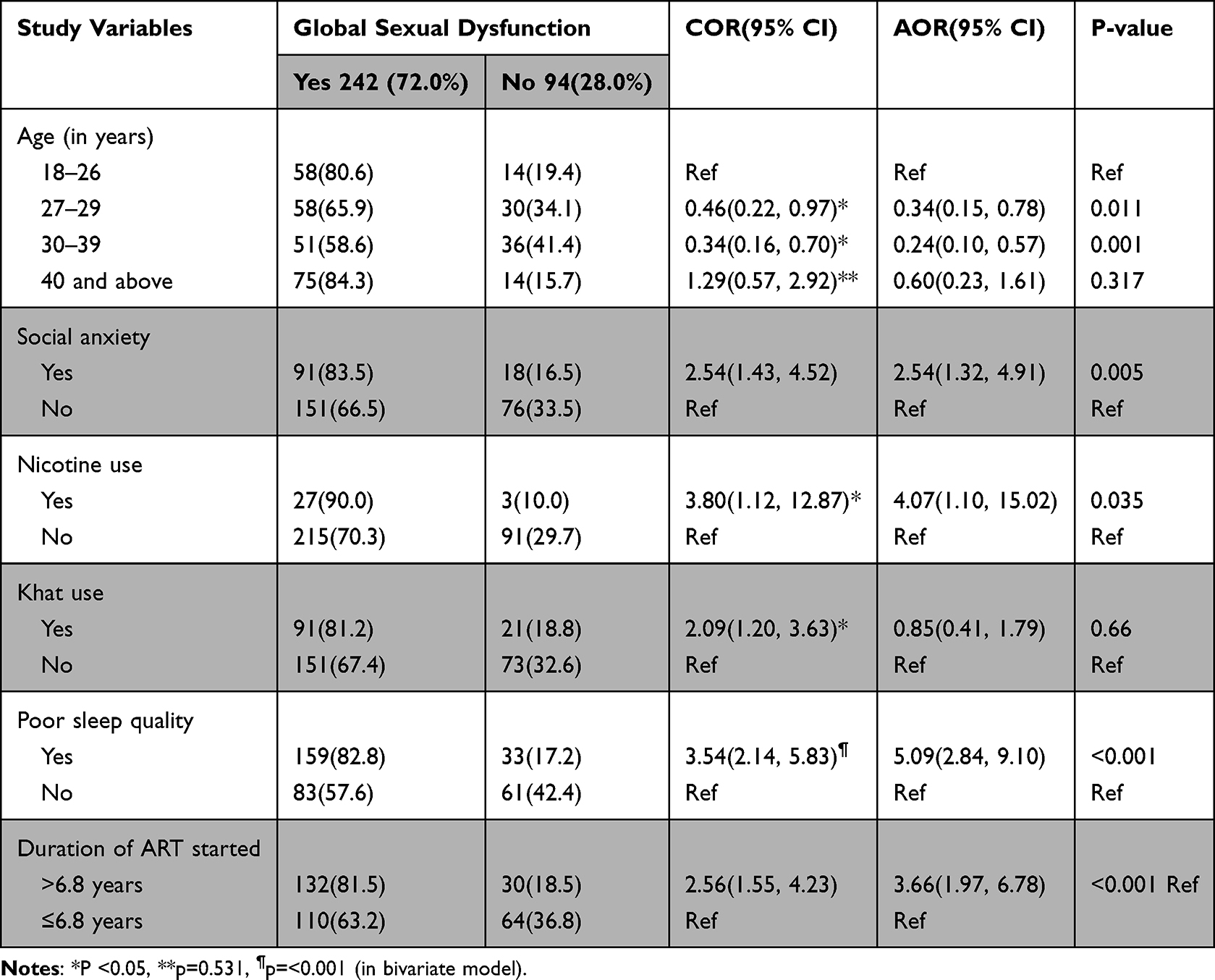 |
Table 3 Predictors of Sexual Dysfunction by Bivariate and Multivariate Logistic Regression Among PLWH, South West Ethiopia, May 2020 (N=336) |
Discussion
When we compare it with the previous study conducted in Iran (46.2%)3 and Italy (58%),5 our finding is higher. The disparity between the study populations’ socioeconomic profiles and Ethiopia’s limited access to healthcare services could be the cause.
Compared to other SD domains, sexual pleasure and sexual desire problems exhibited higher and lower figures, respectively.
The percentage of sexual pleasure issues in this study was significantly higher than in previous investigations when we compared the results. In Spain, 67.1% of people had erectile dysfunction (ED),30 in Mexico, 65.1%,31 in Brazil, 21.6%,32 and in the UK, 33%.2 The high percentage in this report may be attributed to participant differences in socioeconomic status and culture. According to the study,33 it is likely the case that those with higher socioeconomic status have greater sexual pleasure than their counterparts, as demonstrated by the comparison of these findings. Another explanation for the discrepancy in the results could be that earlier research was done in nations with more access to clinical services than Ethiopia. These disparities may be caused by service-related problems, such as the accessibility and availability of high-quality services like sophisticated pharmaceuticals and associated counseling support.
In the earlier research,9 HIV-positive women reported having 64.5% of their problems with desire. Our outcome surpasses that of the preceding report. The sociocultural backgrounds of the research participants may account for the variation in the results. Due to Ethiopian cultural taboos against sexual desire, women may conceal their willingness to engage in sexual activity.34
Our current findings show that, in comparison to participants under the age of 26, study participants aged 27–39 had higher risks for SD. The same results were previously reported.12,35 This could be because the majority of people start using drugs at this age, and it’s also when various mental illnesses start to manifest.24 In other words, there was no significant correlation found in this study between having an SD and being older than 40. It deviates from the earlier outcome.2 The fact that our study participants’ mean age was lower than the results of previous publications could be one explanation. The earlier study, which found that age is not a predictor of SD, supports this.32
Our findings supported the notion that individuals with social anxiety had greater odds of having SD than those without it. Premature ejaculation was found to be predicted by anxiety, and research has linked mental illnesses like anxiety to issues with sex.36 Those who contract HIV through anxiety may experience SD because anxiety impedes sexual function. However, anxiety that follows arguments with partners after a diagnosis may be associated with a higher risk of developing SD. Compared to individuals who do not use nicotine, those who use nicotine have a higher chance of developing SDs. The results of the earlier studies corroborate the present finding.12 The SD of those who smoked cigarettes was more advanced. It has been established through previously published research that using nicotine aggravates SD. This could be because nicotine depletes nitric oxide, either directly or indirectly through the vascular system.37
According to the current findings, participants who had lower quality of sleep reported a higher number of SDs than those who had better sleep patterns. Participants’ propensity for poor-quality sleep, which alters the hormonal balance in the bloodstream, may be the cause of this. In the event that normal testosterone levels are not circulating, the reproductive organs may not receive enough blood, which could result in ED. Unsatisfactory sleep is a marker for SD.38,39
The contribution of stigma and discrimination to problems related to sexuality among PLWH is unavoidable, even though it was not considered in our assessment. It is well known that psychological distress in this population is predicted by the stigma40,41 and lower self-esteem.42,43 These are the two primary psychological conditions that have a significant impact on sexuality among PLWH, according to the evidence.44 Accordingly, the discrimination and stigma experienced by PLWH may have an impact on their sexuality, either directly through direct fear of the stigma or indirectly through distress and low self-esteem.
Limitations
One limitation of this study is that it did not evaluate serum testosterone and hypogonadism, or potential risk factors such as antidepressants, psychotropic medications, Body Mass Index (BMI), sexual orientation, past sexual history, co-morbidities, men who sex with men (MSM), and sexual abuse.
Conclusion
PLWH experienced SD at a high frequency. In men, the frequency is higher. Sexual pleasure problems and sexual desire problems were the most and least common domains of SD, respectively. SDs were significantly correlated with variables such as age, social anxiety, use of nicotine, poor quality of sleep, and length of time since starting ART. It poses a serious challenge to PLWH. It is advised that in order to comprehend and address the mechanisms and their connection to the underlying factors, a longitudinal study may be necessary. Future researchers should consider evaluating the potential impact of HIV stigma, anxiety, and fear of disease mechanisms on sexuality in these populations. Another suggestion is that the best way to eliminate SD-related factors is through early detection, and that populations should be educated so they can maintain healthy sexual health. In order to do this, it is essential to acquaint the accountable clinicians with talking to patients about sexual issues during routine follow-up visits and evaluating potential drug side effects. Future studies should also evaluate serum testosterone and hypogonadism levels, a history of hormone imbalances, heart disease, diabetes, psychosocial factors, and nerve disorders. In general, a better understanding of the frequency of SD is crucial to planning more effective treatment and prevention strategies. Future researchers should evaluate potential factors like antidepressants, psychotropic medication, BMI, sexual orientation, history of sexual activity, and the presence of other co-morbidities. Future research and longitudinal studies should also take these factors into consideration.
Abbreviations
ART, Antiretroviral Therapy; CAGE, Cut Down, Annoyed, Guilty, Eye Open; CSFQ-14, Change Sexual Functioning Questionnaire Short-Form; DS, Dependency Scale; DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; ED, Erectile Dysfunction; HIV/AIDS, Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome; PLWH, People Living With HIV/AIDS; SD, Sexual Dysfunction.
Data Sharing Statement
All reasonable individuals can assess the data used for this research from Dereje Tsegaye [email protected], and Zakir Abdu [email protected].
Acknowledgments
We acknowledged Mattu University, the hospitals, data collectors, and study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No specific funding for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Moreira ED, Helena C, Abdo N, et al. Prevalence and correlates of erectile dysfunction: results of the Brazilian study of sexual behavior. Elsevier Adult Urol. 2001;58:583–588.
2. Asboe D, Catalan J, Mandalia S, et al. Sexual dysfunction in HIV-positive men is multi-factorial: a study of prevalence and associated factors. AIDS Care. 2007;19(8):955–965. doi:10.1080/09540120701209847
3. Jaafarpour M, Ali K, Javaher khaJavikhan ZS. Female sexual dysfunction: prevalence and risk factors. J Clin Diagn Res. 2013;7(12):2877–2880.
4. Nicolosi A, Moreira ED, Shirai M, Ismail M, Mohd BIN, Glasser DB. Epidemiology of erectile dysfunction in four countries: cross-national study of the prevalence and correlates of erectile dysfunction. Elsevier. 2003;61(1):201–206.
5. Pinzone MR, Gussio M, Bellissimo F, et al. Self-reported sexual dysfunction in HIV-positive subjects: a cross-sectional study. Infect Dis Trop Med. 2015;1(2):1–5.
6. Florence E, Authors O, Florence E, Schrooten W, Dreezen C, Gordillo V. Prevalence and factors associated with sexual dysfunction among HIV-positive women in Europe. AIDS Care. 2004;16(5):550–557. doi:10.1080/09540120410001716333
7. Mrcpi LH, Mrcp RN, Kell P. Medical management of sexual difficulties in HIV-positive individuals. Int J STD AIDS. 2002;13(9):587–592. doi:10.1258/09564620260216272
8. Luzi K, Guaraldi G, Murri R. Body image is a major determinant of sexual dysfunction in stable HIV-infected women. Int Med Press. 2009;14:85–92.
9. Araujo AD, Regina P, Barbosa M, Brignol S, Villela W, Souza S. Drivers of sexual inactivity among women living with HIV and AIDS: findings of the GENIH study in São Paulo, Brazil. Arch Sex Behav. 2018;47:1983–1993.
10. Scanavino MDT. Sexual Dysfunctions of HIV-Positive Men: Associated Factors, Pathophysiology Issues, and Clinical Management. Hindawi Publ Corp Advances Urol; 2011.
11. Lema VM. Sexual dysfunction among HIV patients: three case reports and review of literature. Afr J Reprod Heal. 2013;17(4):161–170.
12. Lewis RW, Fugl-Meyer KS, Bosch ARF-M R, Laumann EO, Lizza A-M-M. Epidemiology/risk factors of sexual dysfunction. J Sex Med. 2004;1(1):35–39. doi:10.1111/j.1743-6109.2004.10106.x
13. Mohamed Ali Ismail A. Is there a role for exercise in men suffering from HIV-induced erectile dysfunction. Aging Male. 2023;26(1):2174512. doi:10.1080/13685538.2023.2174512
14. Mcarthur JC, Brew BJ, Nath A. Neurological complications of HIV infection. The Lancet. Neurology. 2005;4(9):543–555. doi:10.1016/S1474-4422(05)70165-4
15. Shuman E. Complications of HIV Infection. Saint-Chopra guide to inpatient med; 2019. 305–C55.P30.
16. Shacham E, Lo JD, Souza P, Overton ET. Examining sexual function among individuals with HIV in a Midwestern US urban outpatient clinic setting. J Int Assoc Provid AIDS Care. 2017;16(5):481–486. doi:10.1177/2325957417724205
17. Keller A, McGarvey EL, Clayton AH. Reliability and construct validity of the changes in sexual functioning questionnaire short-form (CSFQ-14). J Sex Marital Ther. 2006;32(1):43–52. doi:10.1080/00926230500232909
18. Daniel JB, Reynolds III CF, Timoth HM, Berman DJK. SR. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Elsevier Psychiatry Res. 1988;28:193–213.
19. Wu J, Wu H, Lu C, Guo L, Li P. Self-reported sleep disturbances in HIV-infected people: a meta-analysis of prevalence and moderators. Sleep Med Elsevier B V. 2015;16(8):901–907.
20. Davidson J. Social Phobia Inventory (SPIN). Br J Psychiatry. 1995. 176(4):379.
21. Dc C, Eo O. Validation of the Social Phobia Inventory (SPIN) in Nigeria. J Psychiatry Psychiatr Disord. 2018;02(02):49–54. doi:10.26502/jppd.2572-519X0040
22. Kozlowski LT, Frecker RC, Frecker RC, Fagerstrom K-O. The fagerstrom test for nicotine dependence: a revision of the fagerstrom tolerance questionnaire. Br J Addict. 1991;86(9):1119–1127. doi:10.1111/j.1360-0443.1991.tb01879.x
23. Klinsophon T, Prawit Janwantanakul PT. Reliability of the Thai version of the Fagerstrom Test for Nicotine Dependence (FTND). J Med Assoc Thai. 2017;100(101):1130–1134.
24. Benjamin BJ. Sadock VAS. Kaplan & Sadock’s Synopsis of Psychiatry Behavioral Sciences/Clinical Psychiatry.
25. Manzar MD, Alamri M, Mohammed S, Khan MA, Chattu VK. Psychometric properties of the severity of the dependence scale for khat (SDS-khat) in polysubstance users. BMC Psychiatry. 2018;18(343). doi:10.1186/s12888-018-1917-2
26. Martin G, Copeland J, Gates P, Gilmore S. The Severity of Dependence Scale (SDS) in an adolescent population of cannabis users: reliability, validity and diagnostic cut-off. Drug Alcohol Depend. 2006;83(1):90–93. doi:10.1016/j.drugalcdep.2005.10.014
27. Williams N. The CAGE Questionnaire. Occupational Medicine. Oxford University Press; 2014:473–474.
28. Institute University of Washington. Canadian guideline for safe and effective use of opioids for cncp — part b. alcohol and drug abuse; Institute University of Washington.
29. CAGE Substance Abuse Screening Tool. Johns Hopkins health care; 1984.
30. Moreno T, Navarro F, Santos J, Palacios R. Prevalence and factors associated with erectile dysfunction in a cohort of HIV-infected patients. Int J STD AIDS. 2015;24(9):712–715.
31. Romero-velez G, Lisker-cervantes A, Villeda-sandoval CI. Erectile dysfunction among HIV patients undergoing highly active antiretroviral therapy: dyslipidemia as a main risk factor. Sex Med. 2014;2(1):24–30. doi:10.1002/sm2.25
32. Veras T, Brites C. Prevalence and risk factors for erectile dysfunction in HIV-infected patients in Salvador, Brazil. Braz J Infect Dis. 2019;23(6):464–467.
33. Higgins JA, Lands M, Ufot M, McClelland SI. Socioeconomics and erotic inequity: a theoretical overview and narrative review of associations between poverty, socioeconomic conditions, and sexual wellbeing. J Sex Res. 2022;00(00):1–17. doi:10.1080/00224499.2022.2044990
34. Zegeye B, Woldeamanuel GG, Negash W, Shibre G. Sexual satisfaction and its associated factors among married women in northern Ethiopia. Ethiop J Health Sci. 2020;30(2):169–178. doi:10.4314/ejhs.v30i2.4
35. Collazos J. Sexual dysfunction in the highly active antiretroviral therapy era. AIDS Rev. 2007;9(4):237–245.
36. Dunn KM, Croft PR, Hackett GVI. Association of sexual problems with social, psychological, and physical problems in men and women: a cross sectional population survey. J Epidemiol Community Heal. 1999;53(3):144–148. doi:10.1136/jech.53.3.144
37. Kovac JR, Labbate C, Ramasamy R, Tang D, Lipshultz LI. Effects of cigarette smoking on erectile dysfunction. Andrologia. 2016;47(10):1087–1092. doi:10.1111/and.12393
38. Cho JW, Duffy JF. Sleep, sleep disorders, and sexual dysfunction. World J Mens Health. 2018;37(3):261–275. doi:10.5534/wjmh.180045
39. Mohammadi SZ, Shahparian M, Esmaeili HA. Relationship between sleep disorders and erectile dysfunction, depression and quality of life in male patients with systolic heart failure. J Nurs Midwifery Sci. 2016;3(1):15–22. doi:10.18869/acadpub.jnms.3.1.15
40. Kulkarni G, Hoffman S, Melaku Z, Elul B, Nash D. Among individuals initiating ART in Ethiopia. AIDS Behav. 2019;22(12):3815–3825.
41. Basha EA, Derseh BT, Haile YGE, Tafere G. Factors affecting psychological distress among people living with HIV/AIDS at selected hospitals of North Shewa Zone, Amhara region, Ethiopia. AIDS Res Treat. 2019;2019:1–8. doi:10.1155/2019/8329483
42. Adimora DE, Aye EN, Akaneme IN, Nwokenna EN, Akubuilo FE. Stigmatization and discrimination as predictors of self-esteem of people living with HIV and AIDS in Nigeria. Afr Health Sci. 2019;19(4):3160–3171. doi:10.4314/ahs.v19i4.39
43. Yator O, Mathai M, Albert T, Kumar M. Burden of HIV-related stigma and post-partum depression: a cross-sectional study of patients attending prevention of mother-to-child transmission clinic at Kenyatta national hospital in Nairobi. Front Psychiatry. 2021;11(February):1–12. doi:10.3389/fpsyt.2020.532557
44. De VS, Tartaro G, Rochira V, Santi D. HIV and sexual dysfunction in men. J Clin Med. 2021;10(5):1–25.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.