")
Back to Journals » Psoriasis: Targets and Therapy » Volume 14
The Effects of Cardiometabolic Comorbidities on Biologic Treatment for Psoriasis with Respect to PASI Scores: A Qualitative Systematic Review
Authors Osman A, Nigro A, Taylor AC , Saal R, Ormaza Vera A, Enos C
Received 26 September 2023
Accepted for publication 23 December 2023
Published 10 January 2024 Volume 2024:14 Pages 1—10
DOI https://doi.org/10.2147/PTT.S441642
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Uwe Wollina
Alim Osman, Alexandra Nigro, Amanda Chen Taylor, Ryan Saal, Ana Ormaza Vera, Clinton Enos
Department of Dermatology, Eastern Virginia Medical School, Norfolk, VA, USA
Correspondence: Alim Osman, Department of Dermatology, Eastern Virginia Medical School, Norfolk, VA, USA, Email [email protected]
Objective: Cardiometabolic risk factors have been shown to decrease biologic efficacy in patients treated for inflammatory conditions. The purpose of this systematic review is to provide a qualitative evaluation of studies investigating biologic response among psoriasis patients with cardiometabolic comorbidities.
Methods: A comprehensive review was conducted according to the Preferred Reporting Guidelines for Systematic Reviews and Meta-Analysis guidelines to screen for studies including patients with cardiometabolic risk factors receiving biologic therapy for psoriasis. Studies not including a Psoriasis Area and Severity Index (PASI) score to evaluate treatment outcomes were not included. All studies underwent quality/bias analysis using the Methodological Index for Non-Randomized Studies (MINORS) scale.
Results: Obesity and Body Mass Index (BMI) were the most studied cardiometabolic risk factors. The majority of the studies reported a lower frequency of achieving PASI75 and PASI90 response with increasing BMI/obesity rates. Diabetes and hypertension showed similar findings but were not studied as frequently. Hyperlipidemia and other lipid disorders were less frequently studied.
Conclusion: Relationships between cardiometabolic risk factors and lower frequencies of achieving PASI75/90 exist in current literature. This qualitative systematic review reports evidence of lower PASI75 and PASI90 response rates in the presence of cardiometabolic risk factors.
Keywords: psoriasis, cardiometabolic, obesity, PASI, hypertension, biologic
Introduction
Psoriasis is a chronic, immune-mediated, inflammatory disease of the skin and joints. Psoriatic disease commonly involves systemic inflammation, dysmetabolism, and increased comorbid disease burden.1–5 The management of moderate to severe psoriasis has undergone significant advancements with the availability of biologic therapies,6 which include tumor necrosis factor-inhibitors (TNFi) [etanercept, infliximab, adalimumab, certolizumab], interleukin (IL) 12/23 inhibitors (IL-12/23i) [ustekinumab], IL-17 inhibitors (IL-17i) [secukinumab, ixekizumab, brodalumab], and IL-23 inhibitors (IL-23i) [guselkumab, tildrakizumab, risankizumab].1 In Phase III clinical trials, approximately 65% of patients treated with IL-17i7 have demonstrated 90% improvement in Psoriasis Area and Severity Index (PASI90) after 12 weeks of therapy, and approximately 74% of individuals treated with IL-23i achieved PASI90 after 16 weeks.8 Despite the effectiveness of these therapies in clinical trials, response to biologics is not universal in a real-world setting.9 Reasons for these variations in response to biologic therapies are not fully understood.
Treatment algorithms for managing moderate-to-severe psoriasis with biologics often are dependent on characteristics from specific patient populations (eg, pregnancy) and the presence or risk of exacerbation of comorbid diseases (eg psoriatic arthritis, chronic infections, inflammatory bowel disease, demyelinating disease, or heart failure).10,11 Psoriasis is often accompanied by cardiometabolic-risk factor-type diseases that are similarly associated with chronic, systemic inflammation, such as type 2 diabetes mellitus, hypertension, hyperlipidemia, obesity.12 Aside from contributing to poorer health, cardiometabolic risk factors have been shown to decrease biologic efficacy for various conditions.13,14 Subanalyses of randomized controlled clinical trials indicate reduced efficacy of fixed-dose TNFi in the treatment of psoriasis among overweight and obese patients.15–17 In contrast, randomized controlled clinical trials for IL-17i, IL-23i, and IL-12/23i have demonstrated equal effectiveness irrespective of body weight.18–20 Although these trials offer valuable insights for clinicians, it is crucial to acknowledge that the observed favorable responses in the referenced studies may not be universal for everyone.
While biologic therapies may decrease incidence of myocardial infarctions21 and onset of diabetes mellitus,22 little research has been focused on how the presence of cardiometabolic comorbidities might be associated with response to biologic therapies. The purpose of this systematic review is to provide a qualitative evaluation of studies that have assessed PASI scores in patients with cardiometabolic comorbidities treated with biologic therapies.
Materials and Methods
This systematic review was conducted according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.23 A comprehensive literature search was performed for all studies evaluating psoriasis treatment with respect to cardiometabolic factors. All studies published from inception until January 2023 were identified in the PubMed, Medline (OVID), and Web of Science databases. The following search terms were used:
(psoriasis) OR (psoriatic) OR (psoriatic disease) OR (plaque psoriasis) OR (nail psoriasis) OR (scalp psoriasis)
AND
(comorbid) OR (comorbid disease) OR (cardiometabolic) OR (type 2 diabetes) OR (TIID) OR (metabolic syndrome) OR (diabetic) OR (diabetes) OR (obesity) OR (overweight) OR (nonalcoholic fatty liver disease) OR (metabolic disease) OR (comorbidities)
AND
(biologics) OR (biologic treatment) OR (certolizumab pegol) OR (Cimzia) OR (Cosentyx) OR (secukinumab) OR (enbrel) OR (etanercept) OR (humira) OR (adalimumab) OR (Ilumya) OR (tildrakizumab) OR (remicade) OR (infliximab) OR (Siliq) OR (brodalumab) OR (Skyrizi) OR (risankizumab) OR (Stelara) OR (ustekinumab) OR (Taltz) OR (ixekizumab) OR (tremfya) OR (guselkumab)
Article screening was completed by two independent investigators (A.O and A.T). Duplicate studies were removed, and the rest of the articles were screened by title and abstract. Peer-reviewed publications were included that were published in English, isolated psoriasis patients with cardiometabolic comorbidities, reported a PASI score, and reported any associations between patients with cardiometabolic comorbidities and disease progression when treated with biologics. Articles that did not isolate data for biologic treatments reported a PASI score, and did not isolate data on patients with cardiometabolic comorbidities were excluded. Similarly, articles that only evaluated the effects of biologics on cardiometabolic factors and not vice versa were excluded.
Included studies had the following categories of data collected: study design, patient demographics, study quality, study length, biologic drug used (if reported), cardiometabolic factor, effect on PASI score, type of psoriasis (if reported), and follow-up intervals (if reported).
Non-randomized studies were evaluated for study quality using the Methodological Index for Non-Randomized Studies (MINORS) score.24 Categories were scored as 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate). Noncomparative studies featured 8 questions for the MINORS score with total scores ranging from 0 (poor study quality) to 16 (high study quality), while comparative studies featured 12 questions with total scores ranging from 0 to 24.
Due to heterogeneity of the data, only qualitative analysis was possible. Study demographics, biologic treatment, and PASI outcomes were reported separately for each study (Tables 1–3).
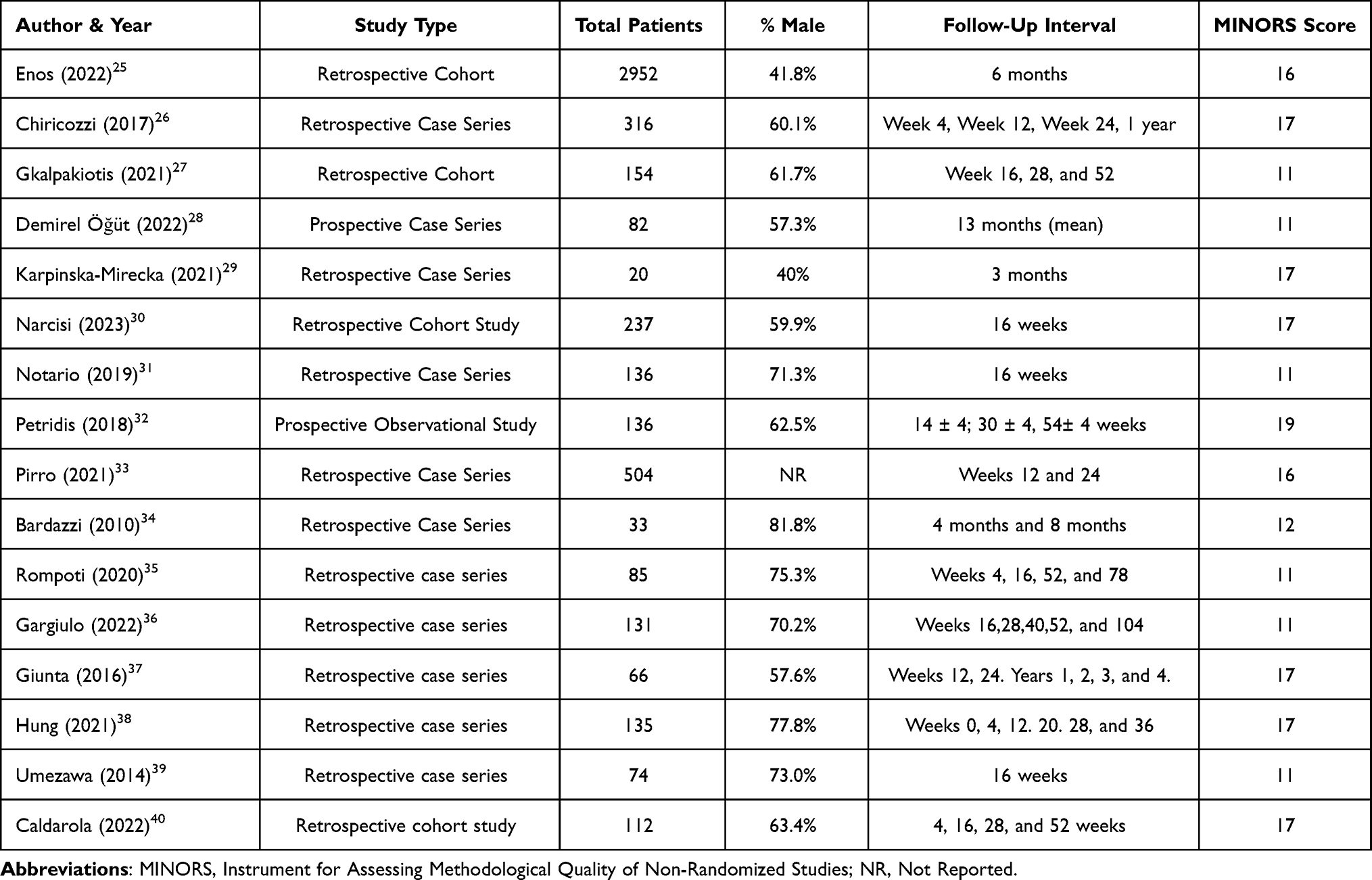 |
Table 1 Study Demographics and Study Quality of Included Studies |
 |
Table 2 Findings of Included Studies |
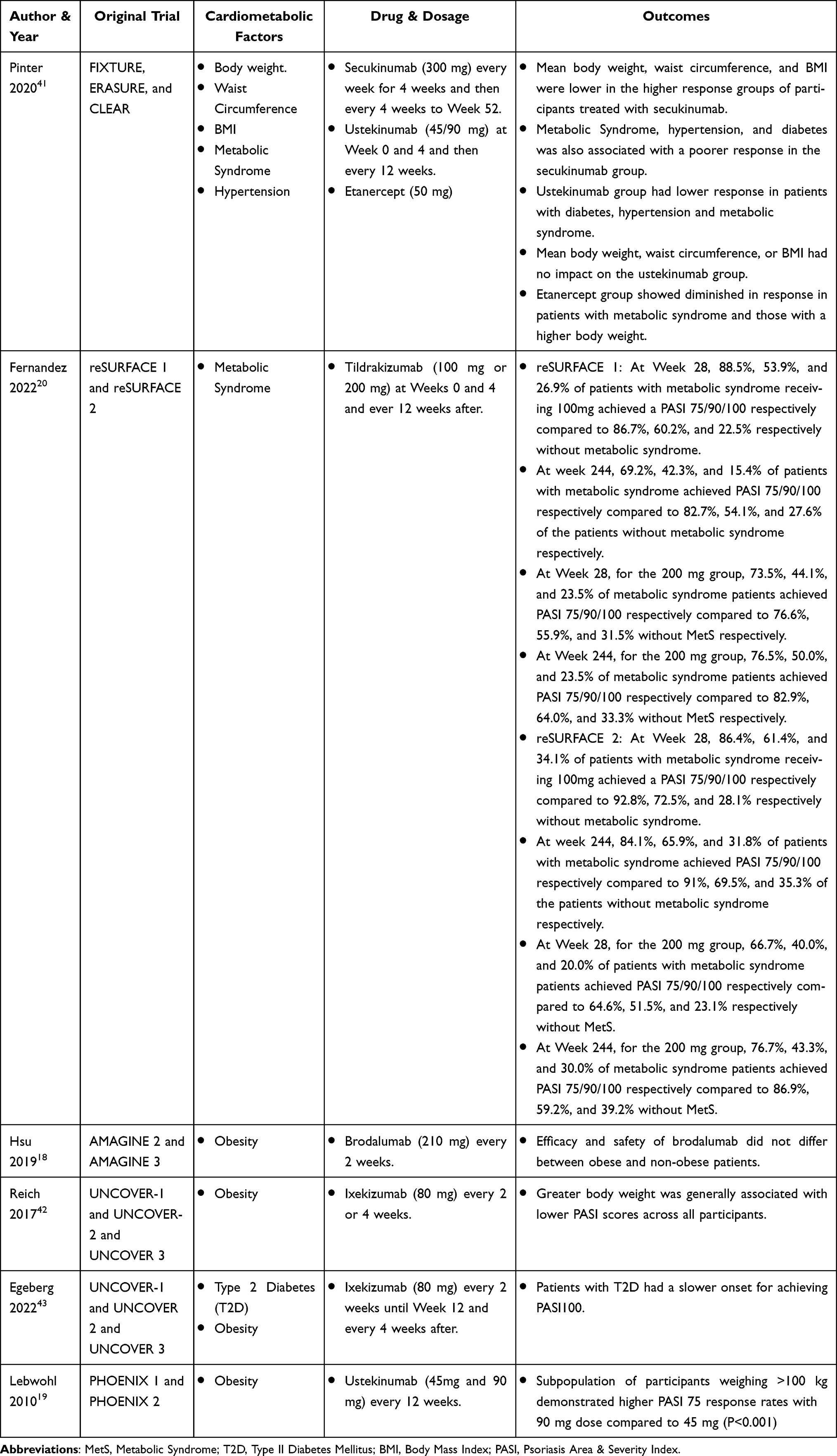 |
Table 3 Findings of Post-Hoc Analyses |
Results
Overall, 4756 articles were identified from databases. After removal of duplicates, 2305 articles were considered for inclusion. A total of 23 studies were included in the qualitative analysis (Figure 1). Eighteen of the 24 studies were not posthoc analyses for which the MINORS score was able to be calculated (Table 1). The average MINORS score for the included studies was 14.3 ± 3.1.
 |
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Diagram of Included Studies. Notes: PRISMA figure adapted from Liberati A, Altman DG, Tetzlaff J et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. Creative Commons.23 |
A total of 18 studies met inclusion criteria. Most studies (13/18) were published within the past five years (2018–2023). Plaque psoriasis was the primary analyzed form of psoriasis. Two studies included patients with psoriatic arthritis,26,39 and one study included patients with psoriasis vulgaris and generalized pustular psoriasis.39 A total of 7936 patients across all studies were evaluated for biologic efficacy and response. Follow-up time/intervals ranged from 3 months – 4 years to analyze long-term drug efficacy.
A total of 17 studies evaluated obesity/BMI as a cardiometabolic factor,25–30,32–40,44 4 studies evaluated diabetes,25,29,31,34 4 studies evaluated hypertension25,29,31,34 and 4 studies evaluated lipid disorders.25,29,31,34 Most of the studies tested drug efficacy for the IL-12/IL-23 inhibitors.25,33,36,38–40,45 Seven papers also analyzed TNF inhibitors,25,26,32–34,37,45 5 analyzed IL-17 inhibitors25,28,31,33,35 One study did not specify the class of the biologic and instead referred to treatment as biological agents.29 Outcomes of each study are summarized in Table 2.
Several post-hoc analyses of randomized control trials were identified in the literature review. Posthoc analyses of the following randomized control trials were included: FIXTURE, ERASURE, CLEAR, reSURFACE 1, reSURFACE 2, AMAGINE 2, AMAGINE 3, and UNCOVER 1–3. Findings of each post-hoc analyses are shown in Table 3.
A total of 5 post-hoc analyses analyzed obesity/bodyweight/BMI.18,19,41–43 Metabolic syndrome and T2D were the second most common cardiometabolic factor analyzed, with a total of 3 articles.20,41,43 Finally, one posthoc analysis looked at hypertension in addition to metabolic syndrome and BMI.41 Relevant outcomes of each posthoc analysis are summarized in Table 3.
Discussion
Here, in a qualitative systematic review of 23 manuscripts, we highlight response to biologics among patients with concurrent metabolic comorbidity. The average MINORS score of the non-randomized was a 14.2/24, indicating weaknesses in the methodology of some included studies.
Most of our included studies have assessed psoriasis treatment outcomes in patients with a high BMI/obesity,25–30,32–40,44 which overwhelmingly highlight lower rates of achieving both PASI75 and PASI90. The majority of studies reported proportions of participants achieving PASI75, PASI90, and/or PASI100 based on BMI. Multiple studies also reported the effect of confounders on the odds of achieving PASI, with a focus on factors such as smoking, previous biologic treatment, alcohol consumption, and presence of a family history of psoriasis. One study calculated odds ratios of achieving PASI 75 and 90 based on associated comorbidities.25 These results were found in almost all biologics used in the included studies, with some exceptions found during the use of Risankizumab,27 infliximab,32 brodalumab,18 and in some cases adalimumab.33 Pirro et al additionally found that patients with obesity had much higher rates of discontinuation of the drug, most likely due to the decreased levels of efficacy.33 A posthoc analysis done by Lebwohl et al19 demonstrated that patients weighing above 100kg benefited from the 90 mg dose of ustekinumab compared to the 45 mg dose. Aside from needing dosing adjustments, obese patients were also shown to have a slower response.38 Hung et al found that although obese patients demonstrated a diminished response initially, this was no longer the case after four weeks of treatment with Guselkumab.38 Further studies should be done that evaluate drug response in obese patients over a longer period, similarly to the reSURFACE clinical trial used to evaluate long-term impacts of metabolic syndrome.20
Type II Diabetes/Metabolic Syndrome were also commonly studied, with nearly every study finding lower frequencies of achieving PASI75 & PASI90 in patients with these comorbidities. In the post-hoc analysis conducted by Pinter et al, etanercept specifically showed a diminished response in patients with metabolic syndrome.41 The same result was found for tildrakizumab in the post-hoc analysis conducted by Fernandez et al.20 Enos et al found that patients with a history of diabetes showed decreased odds of PASI75 and PASI90 at 6 months following biologic initiation.25
Of the studies evaluating hypertension, two found an association between diminished drug responses and hypertension.25,41 Using real-world data, Enos et al found that, overall, patients with hypertension had lower odds ratios of achieving PASI75.25 Additionally, Pinter et al conducted a post-hoc analysis of multiple randomized control trials finding that patients in the lower response category to secukinumab had higher rates of ongoing hypertension.41 Due to hypertension often being one of the many symptoms of metabolic syndrome, it is difficult to say how much hypertension specifically is related to poorer drug response. Future studies should isolate hypertensive patients when looking at odds of achieving a proper biologic response.
Only two of the studies included in this review analyzed hyperlipidemia as a cardiometabolic factor. Neither study found an association between hyperlipidemia and a biologic response. Similar to hypertension, hyperlipidemia is often one of the many symptoms of metabolic syndrome, making it difficult to assess how much of a direct effect it had in the studies evaluating metabolic syndrome.
Overall, psoriasis patients with cardiometabolic factors less frequently achieved PASI75 and PASI90 response when treated with biologics. An overwhelming number of studies focus on obesity/increased BMI. Future studies should explore other cardiometabolic factors such as diabetes mellitus, hypertension, and hyperlipidemia to assess for associations with treatment response to biologics. Such studies could aid in a more tailored care plan for patients on an individual level.
Limitations
Due to heterogeneity of the data, only a qualitative analysis of the data was possible. Additionally, all systematic reviews have an element of selection bias based on the keywords and journals selected by the primary and co-investigators. Additionally, the included studies had a low average MINORS score, indicating limitations in the methodology of the studies. Few studies factored in lifestyle factors, treatment adherence, or other confounding variables in their analysis of the results. Other limitations of this review are that few studies assess multiple agents, the population size varies for each study, and there is a difference in follow-up for each study included in this review.
Conclusion
Multiple published studies have demonstrated a poorer response to biologic treatment of psoriasis in the presence of cardiometabolic factors such as obesity, hypertension, type II diabetes, and other cardiometabolic disorders. With multiple studies pointing to a diminished rate of achieving PASI scores in the presence of cardiometabolic comorbidities, and the observed benefit of weight-based dosing for ustekinumab and infliximab in the presence of obesity,19 future clinical investigations should focus on designing trials with biologic dose adjustments when comorbidities are present. Additional further research is also needed to understand the underlying mechanisms behind the associations of cardiometabolic risk factors and poorer response to biologic therapies. It is recommended that clinicians assess the comorbid disease status of psoriasis patients when developing a therapeutic care plan to optimize their care.
Funding
There is no funding to report.
Disclosure
CE has received grant funding from Arcutis Biotherapeutics; investigator for Amgen and Castle Biosciences. The authors report no other conflicts of interest in this work.
References
1. Elmets CA, Leonardi CL, Davis DMR, et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with awareness and attention to comorbidities. J Am Acad Dermatol. 2019;80(4):1073–1113. doi:10.1016/j.jaad.2018.11.058
2. Langan SM, Seminara NM, Shin DB, et al. Prevalence of metabolic syndrome in patients with psoriasis: a population-based study in the United Kingdom. J Invest Dermatol. 2012;132(3 Pt 1):556–562. doi:10.1038/jid.2011.365
3. Mehta NN, Yu Y, Saboury B, et al. Systemic and vascular inflammation in patients with moderate to severe psoriasis as measured by [18F]-fluorodeoxyglucose positron emission tomography-computed tomography (FDG-PET/CT): a pilot study. Arch Dermatol. 2011;147(9):1031–1039. doi:10.1001/archdermatol.2011.119
4. Kamiya K, Kishimoto M, Sugai J, Komine M, Ohtsuki M. Risk Factors for the Development of Psoriasis. Int J Mol Sci. 2019;20(18):4347. doi:10.3390/ijms20184347
5. Boehncke WH, Schön MP. Psoriasis. Lancet Lond Engl. 2015;386(9997):983–994. doi:10.1016/S0140-6736(14)61909-7
6. Menter A, Strober BE, Kaplan DH, et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics. J Am Acad Dermatol. 2019;80(4):1029–1072. doi:10.1016/j.jaad.2018.11.057
7. Gordon KB, Blauvelt A, Papp KA, et al. Phase 3 Trials of Ixekizumab in Moderate-to-Severe Plaque Psoriasis. N Engl J Med. 2016;375(4):345–356. doi:10.1056/NEJMoa1512711
8. Nakamura M, Lee K, Jeon C, et al. Guselkumab for the Treatment of Psoriasis: a Review of Phase III Trials. Dermatol Ther. 2017;7(3):281–292. doi:10.1007/s13555-017-0187-0
9. Enos CW, O’Connell KA, Harrison RW, McLean RR, Dube B, Van Voorhees AS. Psoriasis Severity, Comorbidities, and Treatment Response Differ among Geographic Regions in the United States. JID Innov Skin Sci Mol Popul Health. 2021;1(2):100025. doi:10.1016/j.xjidi.2021.100025
10. Amin M, No DJ, Egeberg A, Wu JJ. Choosing First-Line Biologic Treatment for Moderate-to-Severe Psoriasis: what Does the Evidence Say? Am J Clin Dermatol. 2018;19(1):1–13. doi:10.1007/s40257-017-0328-3
11. Kaushik SB, Lebwohl MG. Psoriasis: which therapy for which patient: focus on special populations and chronic infections. J Am Acad Dermatol. 2019;80(1):43–53. doi:10.1016/j.jaad.2018.06.056
12. Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases: epidemiology. J Am Acad Dermatol. 2017;76(3):377–390. doi:10.1016/j.jaad.2016.07.064
13. Kurnool S, Nguyen NH, Proudfoot J, et al. High Body Mass Index is Associated with Increased Risk of Treatment Failure and Surgery in Biologic-treated Patients with Ulcerative Colitis. Aliment Pharmacol Ther. 2018;47(11):1472–1479. doi:10.1111/apt.14665
14. Shan J, Zhang J. Impact of obesity on the efficacy of different biologic agents in inflammatory diseases: a systematic review and meta-analysis. Joint Bone Spine. 2019;86(2):173–183. doi:10.1016/j.jbspin.2018.03.007
15. Clark L, Lebwohl M. The effect of weight on the efficacy of biologic therapy in patients with psoriasis. J Am Acad Dermatol. 2008;58(3):443–446. doi:10.1016/j.jaad.2007.11.011
16. Puig L. Obesity and psoriasis: body weight and body mass index influence the response to biological treatment. J Eur Acad Dermatol Venereol JEADV. 2011;25(9):1007–1011. doi:10.1111/j.1468-3083.2011.04065.x
17. Prussick R, Unnebrink K, Valdecantos WC. Efficacy of Adalimumab Compared With Methotrexate or Placebo Stratified by Baseline BMI in a Randomized Placebo-Controlled Trial in Patients With Psoriasis. J Drugs Dermatol JDD. 2015;14(8):864–868.
18. Hsu S, Green LJ, Lebwohl MG, Wu JJ, Blauvelt A, Jacobson AA. Comparable efficacy and safety of brodalumab in obese and nonobese patients with psoriasis: analysis of two randomized controlled trials. Br J Dermatol. 2020;182(4):880–888. doi:10.1111/bjd.18327
19. Lebwohl M, Yeilding N, Szapary P, et al. Impact of weight on the efficacy and safety of ustekinumab in patients with moderate to severe psoriasis: rationale for dosing recommendations. J Am Acad Dermatol. 2010;63(4):571–579. doi:10.1016/j.jaad.2009.11.012
20. Fernandez AP, Dauden E, Gerdes S, et al. Tildrakizumab efficacy and safety in patients with psoriasis and concomitant metabolic syndrome: post hoc analysis of 5-year data from reSURFACE 1 and reSURFACE 2. J Eur Acad Dermatol Venereol JEADV. 2022;36(10):1774–1783. doi:10.1111/jdv.18167
21. Lee JL, Sinnathurai P, Buchbinder R, Hill C, Lassere M, March L. Biologics and cardiovascular events in inflammatory arthritis: a prospective national cohort study. Arthritis Res Ther. 2018;20:171. doi:10.1186/s13075-018-1669-x
22. Lin C, Ji H, Cai X, Yang W, Lv F, Ji L. The association between the biological disease-modifying anti-rheumatic drugs and the incidence of diabetes: a systematic review and meta-analysis. Pharmacol Res. 2020;161:105216. doi:10.1016/j.phrs.2020.105216
23. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. doi:10.1136/bmj.b2700
24. Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. 2003;73(9):712–716. doi:10.1046/j.1445-2197.2003.02748.x
25. Enos CW, Ramos VL, McLean RR, et al. Cardiometabolic multimorbidity is common among patients with psoriasis and is associated with poorer outcomes compared to those without comorbidity. J Dermatol Treat. 2022;33(7):2975–2982. doi:10.1080/09546634.2022.2089329
26. Chiricozzi A, Zangrilli A, Bavetta M, Bianchi L, Chimenti S, Saraceno R. Real-life 9-year experience with Adalimumab in psoriasis and psoriatic arthritis: results of a single-centre, retrospective study. J Eur Acad Dermatol Venereol JEADV. 2017;31(2):304–311. doi:10.1111/jdv.13771
27. Gkalpakiotis S, Cetkovska P, Arenberger P, et al. Risankizumab for the Treatment of Moderate-to-Severe Psoriasis: real-Life Multicenter Experience from the Czech Republic. Dermatol Ther. 2021;11(4):1345–1355. doi:10.1007/s13555-021-00556-2
28. Demirel N, Koç S, Erbağcı E, Hapa FA. Ixekizumab treatment in patients with moderate-to-severe plaque psoriasis in a real-world clinical setting. J Cosmet Dermatol. 2022;21(11):6215–6224. doi:10.1111/jocd.15217
29. Karpinska-Mirecka A, Bartosinska J, Krasowska D. The Impact of Hypertension, Diabetes, Lipid Disorders, Overweight/Obesity and Nicotine Dependence on Health-Related Quality of Life and Psoriasis Severity in Psoriatic Patients Receiving Systemic Conventional and Biological Treatment. Int J Environ Res Public Health. 2021;18(24). doi:10.3390/ijerph182413167
30. Narcisi A, Valenti M, Gargiulo L, et al. Real‐life effectiveness of tildrakizumab in chronic plaque psoriasis: a 52‐week multicentre retrospective study—IL PSO (Italian landscape psoriasis). J Eur Acad Dermatol Venereol. 2023;37(1):93–103. doi:10.1111/jdv.18594
31. Notario J, Deza G, Vilarrasa E, et al. Treatment of patients with plaque psoriasis with secukinumab in a real-life setting: a 52-week, multicenter, retrospective study in Spain. J Dermatol Treat. 2019;30(5):424–429. doi:10.1080/09546634.2018.1528000
32. Petridis A, Panagakis P, Moustou E, et al. A multicenter, prospective, observational study examining the impact of risk factors, such as BMI and waist circumference, on quality of life improvement and clinical response in moderate-to-severe plaque-type psoriasis patients treated with infliximab in routine care settings of Greece. J Eur Acad Dermatol Venereol JEADV. 2018;32(5):768–775. doi:10.1111/jdv.14802
33. Pirro F, Caldarola G, Chiricozzi A, et al. Impact of Body Mass Index on the Efficacy of Biological Therapies in Patients with Psoriasis: a Real-World Study. Clin Drug Investig. 2021;41(10):917–925. doi:10.1007/s40261-021-01080-z
34. Bardazzi F, Balestri R, Baldi E, Antonucci A, De Tommaso S, Patrizi A. Correlation between BMI and PASI in patients affected by moderate to severe psoriasis undergoing biological therapy. Dermatol Ther. 2010;23 Suppl 1:S14-19. doi:10.1111/j.1529-8019.2009.01281.x
35. Rompoti N, Sidiropoulou P, Panagakis P, et al. Real-world data from a single Greek centre on the use of secukinumab in plaque psoriasis: effectiveness, safety, drug survival, and identification of patients that sustain optimal response. J Eur Acad Dermatol Venereol JEADV. 2020;34(6):1240–1247. doi:10.1111/jdv.16202
36. Gargiulo L, Ibba L, Pavia G, et al. Real-Life Effectiveness and Safety of Risankizumab in 131 Patients Affected by Moderate-to-Severe Plaque Psoriasis: a 52-Week Retrospective Study. Dermatol Ther. 2022;12(10):2309–2324. doi:10.1007/s13555-022-00795-x
37. Giunta A, Babino G, Ruzzetti M, Manetta S, Chimenti S, Esposito M. Influence of body mass index and weight on etanercept efficacy in patients with psoriasis: a retrospective study. J Int Med Res. 2016;44(1 suppl):72–75. doi:10.1177/0300060515593254
38. Hung Y, Lin Y, Chiu H, Huang Y. Impact of previous biologic use and body weight on the effectiveness of guselkumab in moderate-to-severe plaque psoriasis: a real-world practice. Ther Adv CHRONIC Dis. 2021;12. doi:10.1177/20406223211046685
39. Umezawa Y, Saeki H, Nakagawa H. Some clinical factors affecting quality of the response to ustekinumab for psoriasis. J Dermatol. 2014;41(8):690–696. doi:10.1111/1346-8138.12538
40. Caldarola G, Zangrilli A, Bernardini N, et al. Risankizumab for the treatment of moderate-to-severe psoriasis: a multicenter, retrospective, 1 year real-life study. Dermatol Ther. 2022;35(6). doi:10.1111/dth.15489
41. Pinter A, Gerdes S, Papavassilis C, Reinhardt M. Characterization of responder groups to secukinumab treatment in moderate to severe plaque psoriasis. J Dermatol Treat. 2020;31(8):769–775. doi:10.1080/09546634.2019.1626973
42. Reich K, Puig L, Mallbris L, Zhang L, Osuntokun O, Leonardi C. The effect of bodyweight on the efficacy and safety of ixekizumab: results from an integrated database of three randomised, controlled Phase 3 studies of patients with moderate-to-severe plaque psoriasis. J Eur Acad Dermatol Venereol. 2017;31(7):1196–1207. doi:10.1111/jdv.14252
43. Egeberg A, Merola JF, Schäkel K, et al. Efficacy of ixekizumab in patients with moderate-to-severe plaque psoriasis and prediabetes or type 2 diabetes. Front Med. 2022;9:1092688. doi:10.3389/fmed.2022.1092688
44. Enos CW, Ramos VL, McLean RR, et al. Comorbid obesity and history of diabetes are independently associated with poorer treatment response to biologics at 6 months: a prospective analysis in Corrona Psoriasis Registry. J Am Acad Dermatol. 2022;86(1):68–76. doi:10.1016/j.jaad.2021.06.883
45. Baloghova J, Feketeova E, Kolarcik P. Homocysteine Is a Marker of Increased Cardio-Cerebrovascular Disease Risk in Psoriatic Patients, but It Does Not Reflect the Effect of Biological Therapy in the Longitudinal Observation. Int J Clin Pract. 2022;2022:3820094. doi:10.1155/2022/3820094
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.