")
Back to Journals » Patient Preference and Adherence » Volume 17
The attitude of the Public Toward Social History Taking in Southern Saudi Arabia
Authors Alkhaldy HY , Al Manya AS, Alshehri RM, Alamri RSM , Alqhtany NAA , Almusaad S , Al-Qahtani WHA , Sabah ZU , Algarni AM
Received 25 March 2023
Accepted for publication 12 July 2023
Published 21 July 2023 Volume 2023:17 Pages 1751—1758
DOI https://doi.org/10.2147/PPA.S414213
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Husain Y Alkhaldy,1 Asal S Al Manya,2 Renad M Alshehri,2 Raghad S M Alamri,2 Norah Ali A Alqhtany,2 Samar Almusaad,2 Wejdan HA Al-Qahtani,2 Zia Ul Sabah,1 Abdullah M Algarni3
1Department of Internal Medicine, College of Medicine, King Khalid University, Abha, Saudi Arabia; 2College of Medicine, King Khalid University, Abha, Saudi Arabia; 3Aseer Central Hospital, Abha, Saudi Arabia
Correspondence: Husain Y Alkhaldy, Department of Internal medicine, college of Medicine, King Khalid University, P.O. Box 641, Abha, Saudi Arabia, Tel +96672417578, Fax +96672418111, Email [email protected]
Background: Social history taking is an important element of a medical interview. No previous studies, however, addressed public attitudes regarding social history taking in Saudi Arabia.
Objective: This study explores public attitudes about the importance of social history taking by doctors in Southern Saudi Arabia.
Methods: A cross-sectional study was conducted to collect public opinion about social history taking using a self-administered questionnaire. Social history taking was defined as questions about general sociodemographics (job, income, marital status, housing conditions, and animal contact) and social habits (travel, smoking, alcohol drinking, illicit drug use, and sexual history). Descriptive statistics were conducted, along with a comparison between categorical variables.
Results: A total of 510 respondents completed the questionnaire, of which 381 (74.7%) had a medical history taken before. A complete social taking was not obtained from those with medical history previously taken. Marital status (73.2%), smoking (49.1%), and occupation (32.8%) were the commonest inquiries, while income (3.7%) and sexual history (6.6%) were the least. Most respondents had no reservations about answering questions about their social history. Among the general demographic questions, job and marital status were more likely to be answered, whereas income and housing inquiries were less likely to be answered. Among social habits, sexual history followed by illicit drug use and alcohol drinking inquiries were less likely to be answered.
Conclusion: Detailed social history taking is uncommon among doctors. The public is open to discussing their social status and habits. However, questions involving income, housing, and some social habits like illicit drugs, alcohol, and sexual history are less likely to be faithfully reported and thus need to be handled appropriately. It is crucial for healthcare providers to approach social history taking with sensitivity and respect and to create a private environment for patients where they can freely and accurately share their social histories.
Keywords: attitude, social history taking, social barriers, Saudi Arabia
Introduction
The medical interview is an essential and important part of the doctor-patient relationship. Social history is that part of a medical history that explores the sociodemographic determinants of illness, including living conditions, marriage, job, housing conditions, and income. Social habits like travel, smoking, alcohol drinking, illicit drug, and sexual behavior are also essential to effective social history gathering. Understanding a patient’s social history can shorten time to diagnosis and facilitate the intended care.
For a long time, patients have complained that doctors focus on disease-related inquiries with lesser consideration given to key social determinant factors for the patients themselves.1 Medical educators have long noticed that social history gathering has become rare to seek and obtain.2–4 This issue could be part of declining clinical skills.5 However, since social history involves eliciting sensitive and personal information, it is also difficult for physicians and patients. This perceived difficulty could be related to less training in gathering social history or prior judgments that personal and sensitive information is neither welcomed nor important for care.6 Moreover, dealing with patients from different cultures or religions can also add to the complexity of taking good social history.7–9
Not only will social history taking assist in reaching a diagnosis, but it will also help establish rapport with the patient and build a lasting healthy, relationship, especially for those diseases requiring extended follow-up and care. Improving cross-cultural communication and understanding cultural differences and sensitivities has become an integral competency skill for many health trainees in multicultural communities. It is particularly important in the Saudi context, as Saudi Arabia is a dynamically changing country aiming to expand its population by 2030 to 50 million, from the current 30 million, with 50% then being non-Saudi.
Patient-centeredness is a core dimension of high-quality care, starting from the first encounter, the medical interview, and continuing throughout the patient care journey.10 Building a successful patient-doctor relationship starts with listening to patient input about the provided care. Some studies have explored the barriers to good social history taking from the perspective of healthcare practitioners. For example, undergraduate medical students avoid sexual history and intimate body parts examination for various reasons, including fear of patient refusal.11 However, no previous local studies have addressed this issue from the patient’s perspective. This study explores public attitudes toward social inquiry and aims to identify the barriers that hinder doing a thorough and complete taking of social history.
Materials and Methods
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. We conducted a descriptive cross-sectional survey with a newly developed questionnaire that was distributed online between June and July of 2022. The Bioethical Committee of King Khalid University, Abha, Southern Saudi Arabia, approved the protocol for this study (ECM#2022-1908). Electronic informed consent was a mandatory prerequisite for completing the survey. We did not collect respondent-identifying data; thus, the respondents were free to complete the survey without restraint.
Questionnaire Design and Data Collection
We used Google Forms to design and deliver an Arabic language questionnaire (Supplement 1). The authors met with medical educators and senior physicians to develop the first version of the questionnaire. The form was then sent to selected physicians and the public for piloting, any suggested editing, and corrections. The final version was distributed to the general public through the King Khalid University email system and as a social media advertisement.
For this study, social history has two elements. First, general sociodemographic characteristics that include age, gender, job, income, marital status, housing, and animal contact (pets in homes or domestic animals). Second, social habits included smoking, alcohol drinking, travel, illicit drug use, and sexual history. Sexual history was reduced to asking only about any extramarital sexual relationship for simplicity and also to explore public opinion regarding the sensitivity of sexual history questions.
Those who had had their medical history taken before were asked if a social inquiry about each item was conducted then. They were also asked if any explanation was provided about why the question was being asked and whether they thought the question they were asked was important to their health encounter. All respondents were then asked their general opinions about the importance of social inquiry, whether they would answer faithfully, and if more explanation by the doctors would change their attitude. Finally, participants were asked about the factors that might affect the quality of their answers to any social inquiry, like the rank of the doctor, the gender of the doctor (being the opposite sex), the place where the history is taken (emergency room, multi-bedded room, or private room), if a family member or other person is present when the social inquiry is taken, if a fill-in form rather than a face-to-face interview would be easier, and if they would agree to document their answers in their medical records.
Statistical Analysis
Descriptive statistics on the obtained responses were conducted using the Stata 17 SE software. Numerical variables were reported in terms of means and standard deviations, while the categorical variables were described using frequencies and percentages. Comparisons between the categorical variables were conducted using Fisher’s exact test.
Results
A total of 510 respondents completed the questionnaire (Figure 1). Table 1 summarizes the demographic characteristics of the respondents. The mean age of the respondents was 36 (±11.4), with 379 (74%) females and 390 (76.5%) having at least a university degree. The majority were from the Aseer region, (382, 74.9%). Most of the respondents had had a previous encounter with a doctor once, (80, 15.7%), or more (410, 80.4%), and (381, 74.7%) had had their clinical history taken before.
 |
Table 1 Characteristics of the Study Respondents |
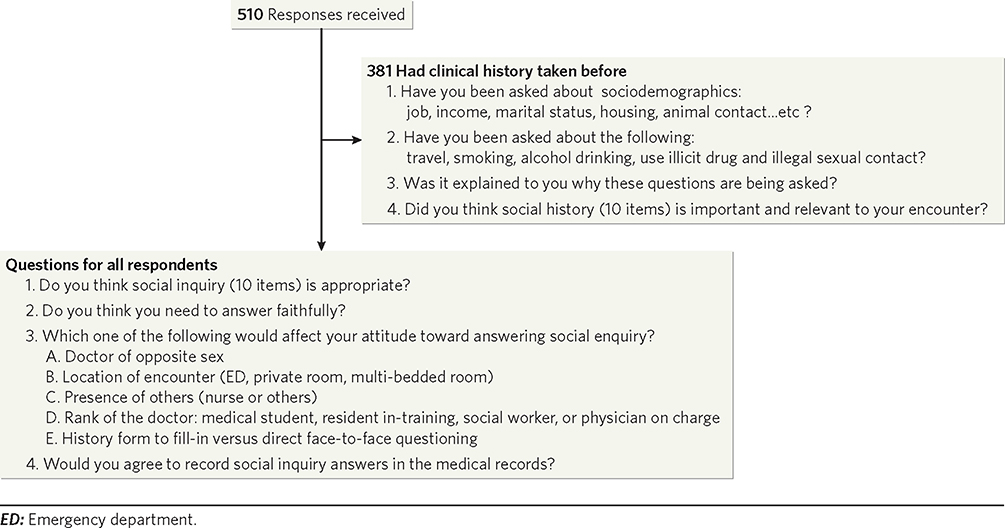 |
Figure 1 Flowchart representing the questions asked for all respondents. |
Overall, apart from asking participants about marital status (279, 73.2%), smoking (187, 49.1%), and job (125, 32.8%), a detailed social inquiry was not completed by doctors with income, (14, 3.7%), housing, (24, 6.3%) and sexual history (25, 6.6%) were the topics least asked about . Participants agreed that most social inquiry items are important to be asked with few exceptions (Table 2). Participants did not think asking about income (308, 85.6%) or housing (304, 79.8%) was as important or as relevant to their encounter. Most respondents do not consider it appropriate to be asked about income (342, 67.1%) and housing conditions (266, 52.2%). For the social habits inquiry, sexual history was considered inappropriate by (231, 45.3%), illicit drugs (144, 28.2%), and alcohol drinking (135, 26.5%). Fewer respondents would answer faithfully for income (231, 45.3%), housing (296, 58%), and sexual history (407, 79.8%) compared to other items. Providing more explanation about why a specific question is being asked resulted in an increase in those who would provide answers for all types of questions (Table 2 and 3).
 |
Table 2 Participants Answers for Questions Related to Sociodemographic Characteristics |
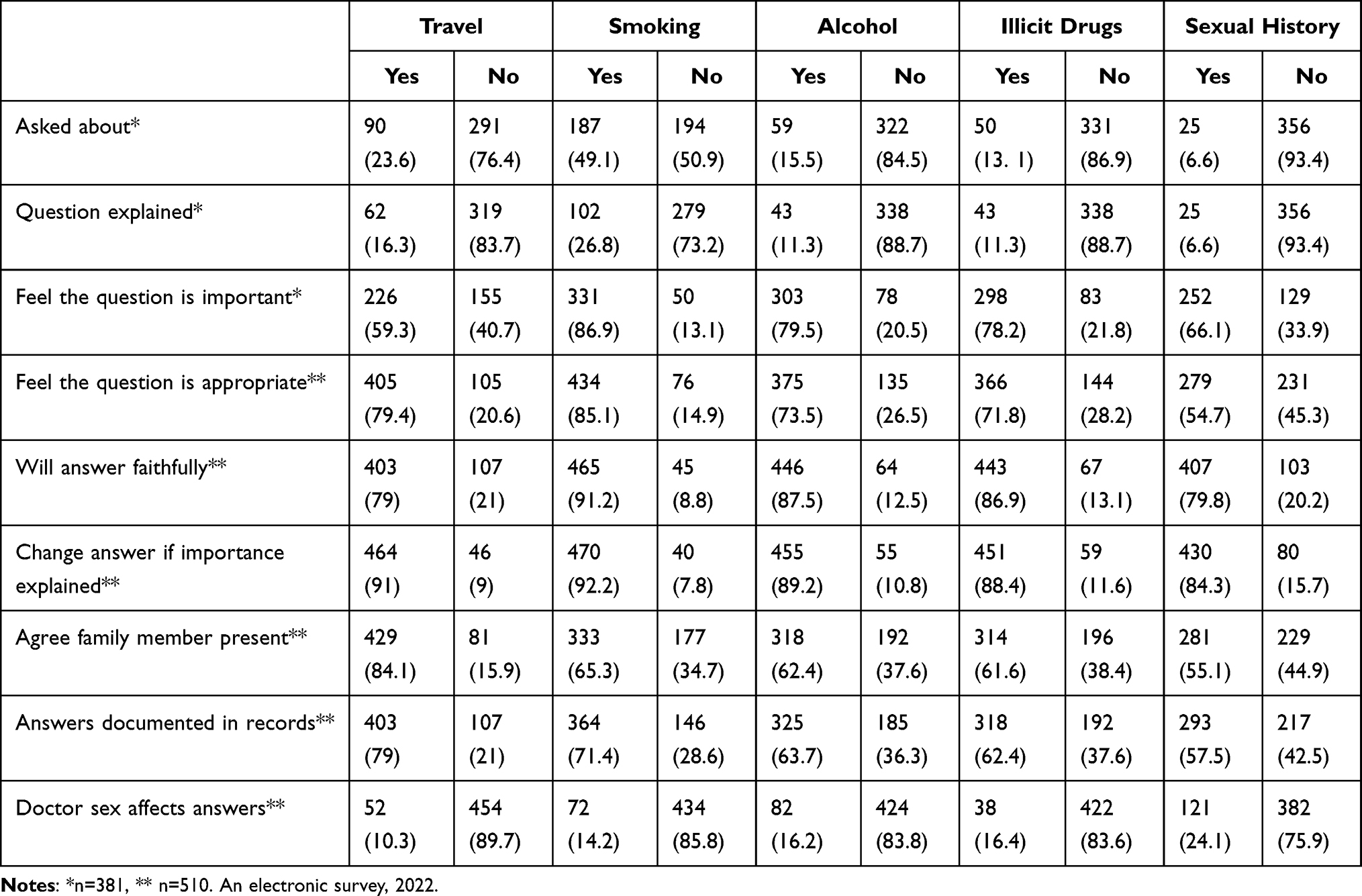 |
Table 3 Participants’ Answers to Questions Related to Social Habits |
When asked about the factors that may affect the quality of their answers, about 50% of respondents thought their responses would be affected if interviewed in an open area like an emergency room or a multi-bedded shared room or when another healthcare worker like a nurse is present (see Table 4). The presence of a family member would also affect the quality of answers, especially for social habits like sexual history (281, 55.1%). Most did not think that being asked by a doctor of the opposite sex would affect their answers. Doctor rank did not seem to affect the quality of the answers, although more would answer if the doctor is a consultant (495, 97.1%) compared to being a medical student (402, 79%). For sexual history, 217 respondents (42.5%) did not agree that their answer is documented in the medical record. A majority of (410, 80.4%) thought a fill-in form is easier to complete compared to face-to-face interviews.
 |
Table 4 Percentage of Those Who Think Their Answers Will Be Affected by the Clinical Area or Presence of Others. n=510 |
Analysis by gender, education level, and age above 40 compared to being younger was done (Supplement 2, Tables S1–S8). Those over 40 are less likely to change their answers if more explanation is given (P value <0.05). Respondents older than 40 also gave more consideration to privacy when history is taken and are also more likely not to answer income and housing condition questions (P value <0.05).
Discussion
Social Medicine–the practice of deliberate inquiry into the social context of patient care–is challenging to teach and not routinely emphasized in the clinical learning environment. As Virchow indicated, “Medicine is a social science in its very bone and marrow”.12 Teaching how to take appropriate social history is important in undergraduate medical education. When students are involved in these activities, they tend to develop a good understanding of the importance of this dimension and reflect on it properly.5,13,14 Our study showed that detailed social history taking is unusual among doctors, and medical educators should take it seriously during both undergraduate and postgraduate training. Our study found that patients generally are open to discussing their private and personal information if they feel that the information that they provide is vital to help guide their care. Although not overtly sensitive, a large portion of the respondents in this study considered questions about income and housing inappropriate. Some respondents were surprised about why a doctor would want to know about their income and housing condition. Thus, it is possible that the importance of income and housing to health is still unclear to the public compared to other topics.
Social determinants of health go beyond traditional questioning and involve exploring a broad range of individual, mental, and environmental factors.15 Patients’ attitudes toward thorough social history questioning vary widely. Some patients may be open and willing to discuss their social history, while others may be more reserved or hesitant to share personal information. Several factors can influence a patient’s attitude toward social history taking. Our study showed that confidentiality is an important consideration. Taking social history in a private environment was clearly appreciated. Person and family boundaries are vague in our culture. While family presence offers needed support and may be associated with a better outcome, this aspect should not be interpreted as acceptance or the willingness to discuss patients’ private matters in front of family members.16 Providers can help create a comfortable and welcoming environment by explaining the importance of gathering social history information, being non-judgmental and respectful when collecting it, and ensuring that the patient’s privacy is fully respected.
Research has shown that cultural and religious beliefs can influence clinical practice in many countries worldwide, including in Middle Eastern countries.17,18 Alcohol consumption and sex outside marriage are major sins in Islam and are less likely to be reported even when asked. Some patients may feel offended if asked about sex or alcohol, so some doctors will avoid asking about it. It is common for undergraduate Saudi medical students to avoid sexual history taking and intimate body parts examination for several reasons.11 These issues are some of the factors that make physicians reluctant to take appropriate social histories. Physician reluctance to take good social history has been extensively reported.19 Some cultures, including South American, Asian, and Middle Eastern, are known to have barriers to seeking sexual health care.18 For example, Iranian American physicians feel reluctant to take a full social history if the patient is female or married.20,21 In Saudi Arabia, some female patients prefer to be seen by female doctors, and this choice is likely to impair the disclosure of sensitive health information.22 Patients being of the opposite sex also reported as a reason for doctors not attempting to gather any sexual history at all.11
We can improve social history-taking skills by implementing certain strategies. A study has looked at how medical students conduct history-taking when observed. Deficient interviewing skills were noted, and social histories, particularly, were poorly taken.23 Students’ shyness from possible intrusion on patient privacy and improper teaching were among the causes of poor social history taking. The commonly utilized case presentation method of teaching history taking emphasizes a medical history’s content and diagnostic reasoning with little focus on how that history is taken. Bedside (observed) history-taking is better suited to offer needed feedback to students. The undergraduate curriculum design, however, should explicitly incorporate teaching blocks about advanced history-taking techniques that do address complex situations.24 Many methods could be used to teach students how to improve their history-taking skills.25 Dedicated sessions on teaching medical students how to better communicate during challenging scenarios like social history gathering and transcultural communication can produce better student performance and satisfaction with the clinical encounter.26 A “medical social ward round” attended by both a physician and a social worker can offer medical students and trainees a better understanding of all the different aspects of social determinants of illnesses and result in better social inquiries overall.1
Our descriptive study does have some limitations, including those inherently related to the study design. In addition, most respondents were young and well-educated. An older population might offer more conservative answers, especially concerning social habits forbidden by the local culture and religion. Although an important part of social history, detailed sexual history was not addressed in this study, and public attitudes might differ from what is reported here regarding general social inquiries. Our study intended to shed light on this crucial subject rather than generate new evidence. More studies are needed to explore this topic and whether poor social inquiry affects the patient-doctor relationship by examining different sequels like patient dissatisfaction, undesired health outcomes, and even litigation.
Despite these limitations, we believe that this study sets the ground rules for more discussion among educators and practitioners that will reinforce the delivery of positive and better social history-taking skills during both undergraduate and postgraduate training.
Conclusion
History taking is an essential skill for a successful patient-doctor relationship. Every effort should be made to explore, review, and improve the gathering of medical histories, including gathering a complete and relevant social history. Medical educators and residency training programs should thus design and revise their teaching /training curricula to adapt to current and anticipated changes in our community to ensure full competency in our health system.
In conclusion, the respondents in this study were mostly willing to discuss their general social status, such as job, marital status, and social habits like travel and smoking. However, many were hesitant to answer questions about income, housing conditions, and sexual activities. Anticipating patient refusal as a reason to avoid proper social history gathering may be unfounded. At the same time, it is important for healthcare providers to approach the topic of social history taking with sensitivity and respect and to create a comfortable environment for patients to share their social histories with clear and proper explanations. By gathering social history information, healthcare providers will better understand their patients’ health needs and challenges and thereby provide even more effective and successful care to those patients.
Acknowledgment
We want to thank Dr. Omar Elfaky for his guidance throughout the preparation of this article. English editing of this manuscript was provided through servicescape.com.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
All authors contributed to the research proposal writing, data collection, analysis, and manuscript writing. All authors reviewed and approved the final version of this manuscript.
Funding
The authors extend their appreciation to the Deanship of Scientific Research at King Khalid University for funding this work through General Research Project under grant number GRP/117/44.
Disclosure
The authors report no relevant disclosure.
References
1. Cohen E, Derow HA. Teaching medical students objectives for care of patients and social aspects of illness. Arch Intern Med. 1935;56(2):351–359. doi:10.1001/archinte.1935.03920020143009
2. Anderson R, Schiedermayer D. The social history matters! Acad Med. 2010;85(7):1103. doi:10.1097/ACM.0B013E3181E19330
3. Maguire GP, Rutter DR. History-Taking for Medical Students. Lancet. 1976;308(7985):556–558. doi:10.1016/s0140-6736(76)91804-3
4. Pfeiffer CA, Madray H, Ardolino AJ, Willms JL. The social history: a vanishing portion of the medical interview. Adv Med Educ. 1997;695–697. doi:10.1007/978-94-011-4886-3_209
5. Pfeiffer C, Madray H, Ardolino A, Willms J. The rise and fall of students’ skill in obtaining a medical history. Med Educ. 1998;32(3):283–288. doi:10.1046/J.1365-2923.1998.00222.X
6. Rahman A, Tasnim S. Twelve tips for better communication with patients during history-taking. Sci World J. 2007;7:519–524. doi:10.1100/tsw.2007.73
7. Qureshi B. Transcultural medicine: Dealing with patients from different cultures. Springer Science & Business Media; 2012.
8. Hs S, Rc G, Kashtan H, Stadler J, Bruce W. How to avoid pitfalls in ethnic medical history, examination and diagnosis. J R Soc Med. 1992;85:65. doi:10.1177/014107689208500202
9. Galanti GA. Caring for Patients from Different Cultures. University of Pennsylvania Press; 2015. doi:10.9783/9780812290271
10. Langberg EM, Dyhr L, Davidsen AS. Development of the concept of patient-centredness – a systematic review. Patient Educ Couns. 2019;102(7):1228–1236. doi:10.1016/j.pec.2019.02.023
11. Abdulghani HM, Haque S, Irshad M, et al. Students’ perception and experience of intimate area examination and sexual history taking during undergraduate clinical skills training: a study from two Saudi medical colleges. Medicine. 2016;95(30). doi:10.1097/MD.0000000000004400
12. Rather LJ. Rudolph Virchow and scientific medicine. AMA Arch Intern Med. 1957;11:1007–1014. doi:10.1001/archinte.1957.00260120151019
13. Kirkland JT, Berry A, Beck Dallaghan GL, Moore Z, Koonce TF. Social factors of health care: a thematic analysis of first and second year medical student reflections. Med Sci Educ. 2021;31(5):1685–1692. doi:10.1007/S40670-021-01360-5
14. Lypson M, Perlman R, Lash R, Silveria M, Johnson C. The social history…It’s about the patient - culture and all. MedEdPORTAL. 2009;3149. doi:10.15766/MEP_2374-8265.3149
15. Behforouz HL, Drain PK, Rhatigan JJ. Rethinking the social history. New England J Med. 2014;371(14):1277–1279. doi:10.1056/NEJMP1404846/SUPPL_FILE/NEJMP1404846_DISCLOSURES.PDF
16. Fakhry M, E WM-A. Impact of family presence on healthcare outcomes and patients’ wards design. Alex Eng J. 2022;61(12):10713–10726. doi:10.1016/j.aej.2022.04.027
17. Hammoud MM, White CB, Fetters MD. Opening cultural doors: providing culturally sensitive healthcare to Arab American and American Muslim patients. Am J Obstet Gynecol. 2005;193(4):1307–1311. doi:10.1016/J.AJOG.2005.06.065
18. Julliard K, Vivar J, Delgado C, Cruz E, Kabak J, Sabers H. What latina patients don’t tell their doctors: a qualitative study. Ann Fam Med. 2008;6(6):543–549. doi:10.1370/AFM.912
19. Dyer K, Das Nair R. Why don’t healthcare professionals talk about sex? A systematic review of recent qualitative studies conducted in the United Kingdom. J Sex Res. 2013;3(11):2658–2670. doi:10.1111/j.1743-6109.2012.02856.x
20. Rashidian M, Minichiello V, Knutsen SF, et al. Effect of attitudes towards patients on sexual history taking: a survey of Iranian–American physicians in California, USA. Sex Health. 2017;14(6):514–522. doi:10.1071/SH17016
21. Rashidian M, Minichiello V, Knutsen S, Ghamsary M. Western, Asian, and middle eastern societies’ cultural attitudes and barriers impacting the management of sexual health care. Trend Androl Sex Med. 2020;165–182. doi:10.1007/978-3-030-36222-5_10
22. Alqufly AE, Alharbi BM, Alhatlany KK, Alhajjaj FS. Muslim female gender preference in delaying the medical care at emergency department in Qassim Region, Saudi Arabia. J Family Med Prim Care. 2019;8(5):1658. doi:10.4103/JFMPC.JFMPC_141_19
23. Ahmed AM. Deficiencies of history taking among medical students. Saudi Med J. 2002;23(8):991–994.
24. Carrillo JE, Green AR, Betancourt JR. Cross-cultural primary care: a patient-based approach. Ann Intern Med. 1999;130(10):829. doi:10.7326/0003-4819-130-10-199905180-00017
25. Keifenheim KE, Teufel M, Ip J, et al. Teaching history taking to medical students: a systematic review. BMC Med Educ. 2015;15(1). doi:10.1186/s12909-015-0443-x
26. Rosen J, Spatz ES, Gaaserud AMJ, et al. A new approach to developing cross-cultural communication skills. Med Teach. 2004;26(2):126–132. doi:10.1080/01421590310001653946
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.