")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 16
The Assessment of Male Erectile Dysfunction Characteristics in Patients Undergoing Continuous Ambulatory Peritoneal Dialysis and Hemodialysis Using the International Index of Erectile Function (IIEF-5) Combined with Hospital Anxiety and Depression Scales
Authors Warli SM, Alamsyah MT, Nasution AT, Kadar DD, Siregar GP, Prapiska FF
Received 1 February 2023
Accepted for publication 27 April 2023
Published 5 May 2023 Volume 2023:16 Pages 155—161
DOI https://doi.org/10.2147/IJNRD.S402540
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Syah Mirsya Warli,1,2 Mohammad Taufiq Alamsyah,3 Alwi Thamrin Nasution,4 Dhirajaya Dharma Kadar,1 Ginanda Putra Siregar,1 Fauriski Febrian Prapiska1
1Division of Urology, Department of Surgery, Faculty of Medicine, Universitas Sumatera Utara – Haji Adam Malik General Hospital, Medan, Indonesia; 2Department of Urology, Universitas Sumatera Utara Hospital, Universitas Sumatera Utara, Medan, Indonesia; 3Department of Urology, Faculty of Medicine, Universitas Indonesia - Haji Adam Malik General Hospital, Medan, Indonesia; 4Division of Nephrology, Department of Internal Medicine, Faculty of Medicine, Universitas Sumatera Utara – Haji Adam Malik General Hospital, Medan, Indonesia
Correspondence: Syah Mirsya Warli, Division of Urology, Department of Surgery, Faculty of Medicine, Universitas Sumatera Utara – Haji Adam Malik General Hospital, Medan, Indonesia, Tel +6261-8218928, Email [email protected]
Purpose: To determine the differences in mean scores of erectile dysfunctions (EDs) assessed by the International Index of Erectile Function (IIEF-5) questionnaire between patients with chronic kidney disease (CKD) undergoing hemodialysis and patients undergoing continuous ambulatory peritoneal dialysis (CAPD).
Patients and Methods: This is an analytic observational study with a cross-sectional design that was conducted from June to December 2022 at the Urology Center of Haji Adam Malik General Hospital and Rasyida Kidney Specialized Hospital. The sample of this study were male CKD-patients who underwent regular hemodialysis (HD) and who underwent CAPD, and met the inclusion and exclusion criteria. Psychological disorders experienced during therapy session are considered as risk factors and assessed via the Hospital Anxiety and Depression Scale (HADS). These disorders assessment was used to evaluate the severity of the patients’ anxiety and depressive symptoms. Statistical data analysis was carried out.
Results: Both groups had HADS-A and HADS-D scores with an average < 7, classified as normal anxiety and depression. Most of the patients in the HD group had mild-to-moderate ED (28.6%), while in the CAPD group had mild severity of ED (38.1%). There were no significant differences in severity of ED between patients undergoing HD and CAPD (p > 0.05). However, there was a significant difference in ED scores (IIEF-5) between patients undergoing HD and those with CAPD (p < 0.05), in which patients in the CAPD group had a higher IIEF-5 score. In addition, there was a significant positive correlation with moderate strength (p< 0.001; r=0.494) between anxiety disorders and ED disorders in patients undergoing HD and CAPD, whereas there is no significant correlation between depressive disorders and ED conditions (p > 0.05).
Conclusion: There was a significant difference in IIEF-5 scores between patients undergoing HD and CAPD.
Keywords: erectile dysfunction, CAPD, HD, IIEF-5
Introduction
Chronic kidney disease (CKD) is a pathophysiological process that develops into a progressive deterioration of kidney function.1 The worldwide prevalence of CKD is estimated at 13.4% or 8–16% of the entire population, and in Indonesia, the incidence of CKD per a million population (data from 2002–2006) 10.2, 11.7, 13.8, 18.4 to 23.4.2 Based on a report of the 2018 Indonesian Baseline Health Research (Riskesdas), patients aged 15 years were diagnosed with chronic kidney failure accounted for 3.8%, an increase from 0.2% in 2013.3 Treatment for patients with end-stage CKD requires kidney replacement therapy, such as kidney transplantation and dialysis therapy. The options for dialysis-therapies are hemodialysis (HD) and continuous ambulatory peritoneal dialysis (CAPD) which aim to maintain the patient’s quality of life.4,5
CKD affects not only the kidneys but also all other vital organs in men, including sexual dysfunction.6,7 Erectile dysfunction (ED) is a sexual dysfunction that is often encountered as a complication for male patients with end-stage CKD.4,6,7 In several studies, the prevalence of ED in patients with end-stage CKD were between 50% and 80%.8 Compared to the general population of the same age, the prevalence of sexual dysfunction was significantly higher in patients with end-stage CKD.6 In patients with CKD, there was a decrease in total testosterone levels which will affect sexual function. In addition, there was an increase in urea levels in the blood which will trigger atherosclerosis contributing directly in pathophysiology of ED in CKD patients.4
To improve patient’s quality of life, several studies conducted research on the effect of dialysis modalities on ED patients. Gorsane et al have found that 33.3% of the patients with end-stage CKD had severe ED before hemodialysis, and the number reduced to 29.2% after hemodialysis therapy.9 Savadi et al reported that 6 months of hemodialysis can improve erectile function, orgasmic function, sexual desire, sexual satisfaction, and overall satisfaction in patients with CKD.10 Duarsa et al conducted a study by comparing ED improvement between patients on regular HD and patients with CAPD. Their finding showed that 11 patients (50.0%) had severe ED before CAPD and 13 patients (59.1%) had mild-to-moderate ED after CAPD. Moreover, there was also a significant difference in the improvement in ED severity and IIEF-5 scores in the CAPD group. In contrast, no significant differences in improving the severity of ED and the IIEF-5 score was found in the HD group.4
Psychological disorders which are considered as ED risk factors are related to the dialysis therapy. These psychological disorders could be assessed using the Hospital Anxiety and Depression Scale (HADS) questionnaire to evaluate the severity of the participants’ anxiety and depressive symptoms. The scale consists a total of 14 questions. The odd-numbered questions were designed to measure anxiety (ie, anxiety on the HADS-A subscale) and the even-numbered ones for depression (ie, depression on the HADS-D subscale).
As a high prevalence of ED in CKD patients has a significant impact on quality of life, this problem must take a full consideration to improve their quality of life. Furthermore, based on the results of previous studies which remains controversial regarding the effect of dialysis modalities on ED, this study was conducted to evaluate the effect of dialysis therapy on sexual function among male CKD patients. The determination of the differences in ED severity and IIEF scores among end-stage CKD patients undergoing hemodialysis with patients undergoing CAPD in order to improve patient’s quality of life is aimed.
Materials and Methods
This is an analytic observational study with a cross-sectional design that was conducted from June to December 2022 at the hemodialysis installation unit of Haji Adam Malik General Hospital (HAM-GH) and hemodialysis installation unit of Rasyida Kidney Specialized Hospital (RK-SH). This study complied with 1964 Helsinski Declaration and was approved by the Ethical Committee of Faculty of Medicine Universitas Sumatera Utara with registration number 656/KEPK/USU/2022. The sample of this study were male CKD patients who underwent regular hemodialysis (HD) times a week, 5 hours per session and the patients who underwent CAPD. The inclusion criteria were male patients with CKD, aged >18 years, had a partner, had the mental capacity to understand and answer the questionnaire, and patients undergoing dialysis treatment (HD and CAPD) in Nephrology Department at (HAM-GH) and (RK-SH). The exclusion criteria included not completing dialysis therapy for at least 3 months, smoking behavior, consuming alcohol, having co-morbid in neurological disorders (stroke), suffering cognitive impairment, experiencing major psychiatric illness (schizophrenia), taking drugs to improve sexual performance, and having a history of previous surgery in the urogenital. Risk factor of ED such as psychological disorders were assessed using the Hospital Anxiety and Depression Scale (HADS) questionnaire to evaluate the severity of anxiety and depressive symptoms. The cut-off score for HADS-A was determined as 10 of 11, and the cut-off score for HADS-D was determined as 7 of 8. The lowest and highest scores of the two subscales were, respectively, 0 and 21. The assessment of the HADS questionnaire was carried out along with IIEF-5 questionnaire at the same time. The IIEF-5 difference scores in CKD patients were analyzed using an unpaired t-test if normally distributed. Otherwise, the Mann–Whitney tests were used. A 95% confidence interval was considered statistically significant with p < 0.05. Characteristics of ED in CKD patients undergoing HD and CAPD were analyzed using the chi-square test if they met the requirements, otherwise the alternative was Fisher’s test or Kolmogorov–Smirnov test.
Results
Of total 42 samples, the mean age of HD group was 49.5 years and the CAPD group was 41.19 years. The average BMI of both HD and CAPD groups were respectively 24.3 and 24.17. Most of the samples in HD and CAPD groups (Table 1) were smokers (52.4% and 61.9%), never drink alcohol (57.1% and 71.4%), entrepreneur in CAPD group (53.4%), and employee (42.9%) in HD group; also, their educational status was high-school education (42.9% and 42.9%). Comorbid disease and the primary cause of CKD in the majority of patients in both groups were hypertension. Both groups had HADS-A and HADS-D scores with an average of <7, classified as normal condition of anxiety and depression. Based on the statistical analysis, it is known that there is no significant difference between the two groups (Table 1).
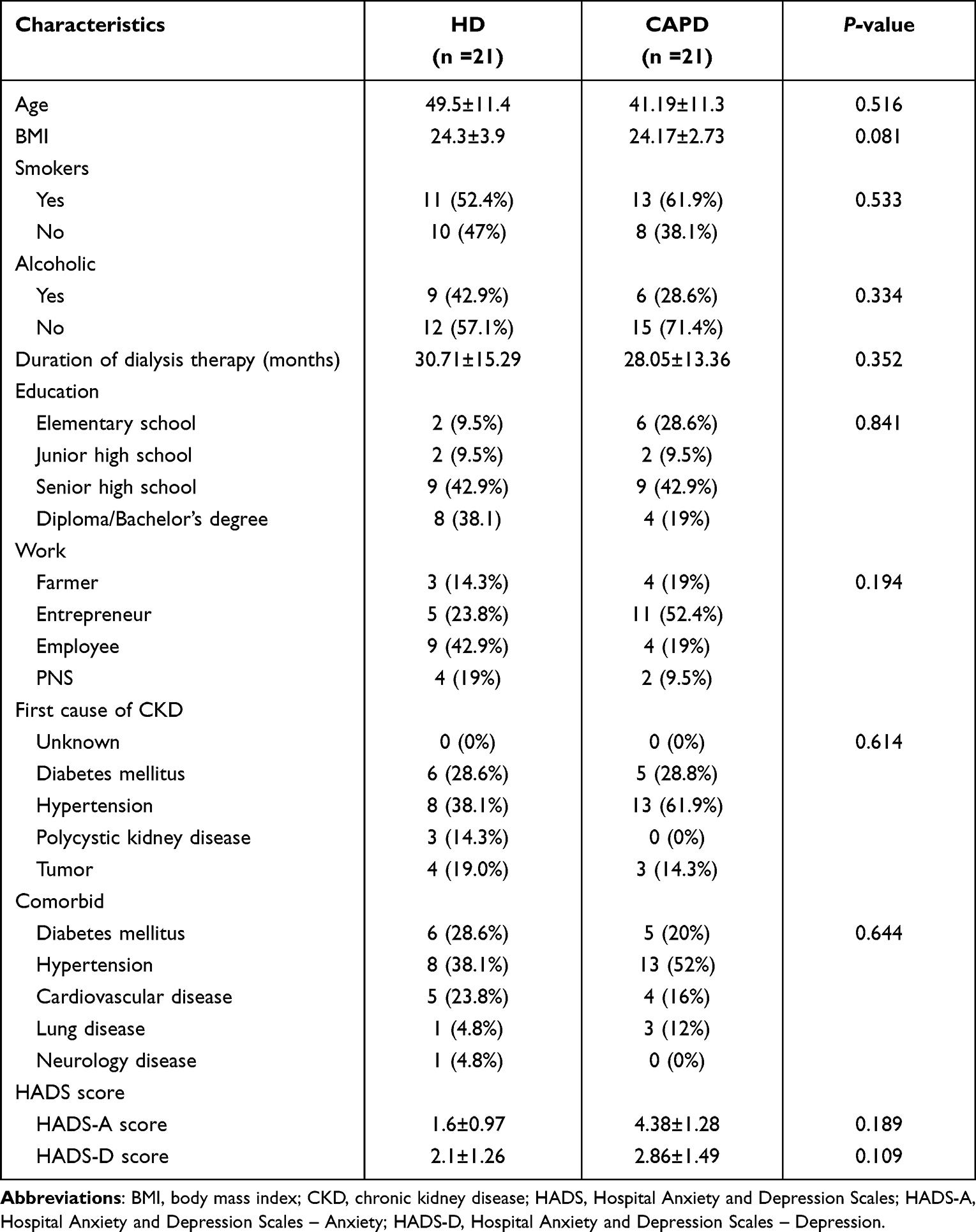 |
Table 1 Sample Characteristics |
Based on Table 2, most of the patients in the HD group experienced mild-to-moderate ED (28.6%), while in the CAPD group most of them experienced mild ED (38.1%). In addition, there was no significant difference in severity of ED between patients undergoing HD and CAPD (p-value >0.05), where the CAPD group experienced milder ED than the CAPD group.
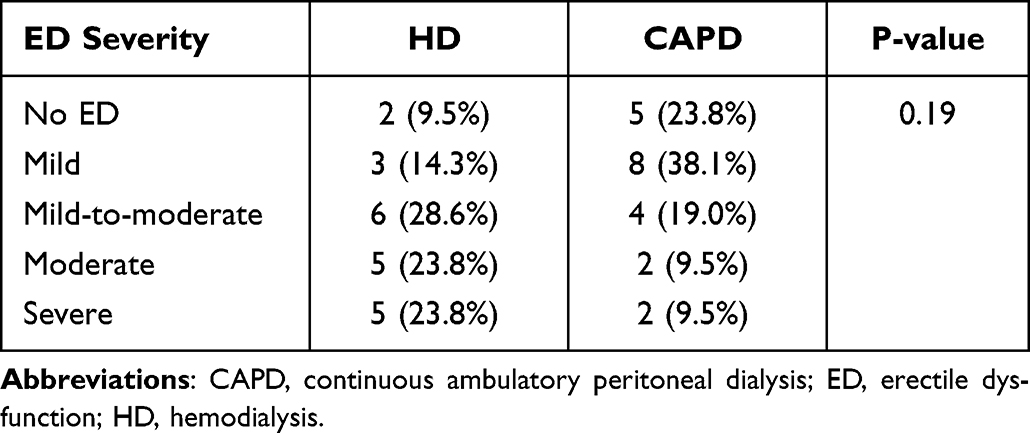 |
Table 2 Prevalence of ED in HD and CAPD Groups |
Based on the analysis shown in Table 3, there was a significant difference in ED score (IIEF-5) between patients with HD and CAPD (p-value <0.05), where patients in the CAPD group have a greater IIEF-5 score than those in the HD group.
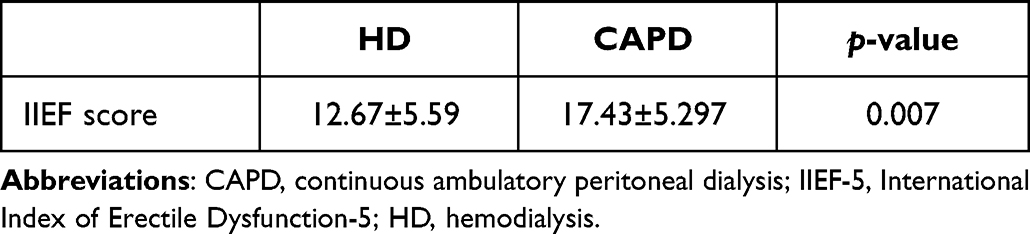 |
Table 3 Differences in IIEF-5 Scores Between HD and CAPD Patients |
Table 4 shows no significant difference in the IIEF-5 score in patients who are >50 years old and have DM comorbidities. There was a significant difference in IIEF-5 score (p-value <0.05) in patients with hypertension comorbid, where patients with comorbid hypertension have a lower IIEF-5 score (13.10 ± 5.366) than patients who do not have hypertension (17.00 ± 5.87). In addition, from Table 5, there was also a positive correlation with moderate strength and significant results between anxiety disorders (HADS-A) and ED disorders (IIEF-5) in patients undergoing HD and CAPD (p<0.001; r=0.494). Moreover, depressive disorder (HADS-D) and ED in patients undergoing HD and CAPD did not have a significant correlation (p-value >0.05).
 |
Table 4 Risk Factors for ED |
 |
Table 5 Correlation Between HADS-A and HADS-D with IIEF Score |
Discussion
In this study, the prevalence of ED in patients undergoing HD was 90.5% consisting of mild (14.3%), mild-to-moderate (28.6%), moderate (23.8%) and severe (23.8%). In line with Duarsa et al, the prevalence of ED in patients with HD was 60.3%.4 Lai et al also showed the prevalence of erectile dysfunction, identified by the IIEF erectile domain score, accounted for 51.9%.11 A high prevalence of ED was also found among patients in a study conducted by Mekki et al, that were 83% of ED cases among HD patients and 67.5% among kidney transplant recipients.12 In Gorsane et al’s study, ED appeared in 8.4% of the patients before being diagnosed with kidney failure and in 91.6% of the patients at the beginning treatment of dialysis.9
A study by Winarta et al showed that the severity of DE was assessed by IIEF5 questionnaire after being diagnosed with stage 5 CKD, by which mild-to-moderate ED in 13 people (59.1%) was found.13 Azevedo et al conducted a study on 30 patients undergoing HD in Porto, Portugal, in 2012, and found a high prevalence of severe ED before CAPD therapy (up to 93.3%). Even more, there was change in degree of severe erectile dysfunction to 44.8% after receiving dialysis using CAPD.14
In this study, there was a significant difference in the IIEF-5 score between patients undergoing HD and CAPD (p-value <0.05), where patients in the CAPD group had a greater IIEF-5 score than those in HD (17.43±5.297 vs 12.67±5.59). Duarsa and team recruited 44 male patients with stage 5 CKD, and found changes in ED degrees before and after dialysis were assessed using the IIEF-5; significant differences in the increase in ED degrees and IIEF-5 scores in the CAPD group were reported.4 In evaluating the effects of sexual-dysfunction to dialysis modalities in male patients with chronic renal failure, Tekkarismaz et al found patients treated with CAPD therapy showed sexual dysfunction which was more common than those treated with HD only (based on two questionnaires, HADS and IIEF-5).6
The risk factors for ED can be multi-system due to its pathological implications at the molecular level. Adequate endothelial function or blood vessel vasculature is needed to achieve optimal erection quality. The interaction between nitric oxide (NO), cyclic guanosine monophosphate (cGMP), and penile corporal smooth muscle greatly affects the function of constriction and relaxation of penile vasculature smooth muscle in general. Therefore, pathological disruption of these factors can increase the risk of developing ED as a manifestation of a metabolic or systemic disease.15–17
The relationship between hypertension and ED is directly related to the endothelial dysfunction. Smoking is thought to have a negative impact on the function and anatomy of an individual’s vasculature, apart from its relation to hypertension and other cardiovascular diseases which are also associated with the incidence of ED. The relationship between obesity and ED is also associated with chronic and systemic inflammation as a result of excessive caloric intake and physical inactivity. As a result, an over-production of cytokines, including C-reactive protein (CRP), tumor necrosis factor-alpha (TNF-α), and interleukin-6 (IL-6) could be occuring. In addition, there is a linear relationship between increased inflammatory markers and the severity of ED, in which the higher the severity of the associated risk factors, the more severe the ED will be.16,18,19
Both ED and depression can theoretically influence each other’s severity to some degree.20 Yang et al stated that there was a higher diagnosis of psychiatric disorders (anxiety and depression) in the population with ED, with onset before and after the diagnosis of ED. The more severe the psychiatric symptoms encountered, the higher the degree of ED reported, especially in the younger patient sub-population with a longer duration of ED.21 Mourikis et al stated that there was a higher level of anxiety in the ED group; conclusively speaking, there was a significant association between erectile dysfunction and psychiatric disorders, such as anxiety.22
Conclusion
There were no significant differences in severity of ED between patients undergoing HD and CAPD. However, there was a significant difference in ED scores (IIEF-5) between patients undergoing HD and those treated with CAPD. Regarding the risk factors associated with the occurrence of ED, there was no significant difference in IIEF-5 score in patients who were >50 years old and had DM comorbid, but there were significant differences in patients who had hypertension comorbid. HADS is an instrument used to measure levels of anxiety and depression. In this study, there was a positive correlation with moderate strength and significant results between anxiety disorders (HADS-A) and ED (IIEF-5) among patients undergoing HD and CAPD, while there was no significant correlation between depressive disorders (HADS-D) and ED (IIEF-5).
Acknowledgments
We thank Haji Adam Malik General Hospital Hemodialysis Installation unit and Rasyida Kidney Specialized Hospital Hemodialysis Installation unit for the support and permission to conduct this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pralisa K, Dewi DAK, Ilmiawan MI. Gambaran etiologi penyakit ginjal kronik stadium V pada pasien rawat inap di RSUD dokter soedarso pontianak tahun 2017–2018. J Cerebellum. 2021;6(3):59. doi:10.26418/jc.v6i3.45308
2. Fitri KF, Iskandar S, Achadiyani A. Mental Health stakeholders’ Perception Toward Mental Illness in West Java. Jurnal Kedokteran Dan Kesehatan Indonesia. 2017;8(3):146–153. doi:10.20885/JKKI.Vol8.Iss3.art2
3. Pakaya RE, Syam Y, Syahrul S. Analysis of self-efficacy and characteristics of patients with chronic kidney disease underwent hemodialysis. J Keperawatan. 2021;12(1):93–98. doi:10.22219/jk.v12i1.13248
4. Duarsa GWK, Kandarini Y, Winarta GK, et al. A comparison of erectile dysfunction improvement between patients with regular hemodialysis and patients with continuous ambulatory peritoneal dialysis. J Sex Med. 2021;18(5):920–925. doi:10.1016/j.jsxm.2021.02.007
5. Duarsa GWK, Kandarini Y, Luciana L, et al. Sexual dysfunction reduction in female patients with chronic kidney disease undergoing continuous ambulatory peritoneal dialysis. Acta Med Indones. 2020;52(4):360–365.
6. Tekkarismaz N, Tunel M, Ozer C. Dialysis modality and sexual dysfunction in male patients. Andrologia. 2020;52(10):1–7. doi:10.1111/and.13735
7. Nassir A. Erectile dysfunction risk factors for patients entering dialysis programme. Andrologia. 2010;42(1):41–47. doi:10.1111/j.1439-0272.2009.00954.x
8. Antonucci M, Palermo G, Recupero SM, et al. Male sexual dysfunction in patients with chronic end-stage renal insufficiency and in renal transplant recipients. Arch Ital Di Urol e Androl. 2015;87(4):299–305. doi:10.4081/aiua.2015.4.299
9. Gorsane I, Amri N, Younsi F, Helal I, Kheder A. Erectile Dysfunction in Hemodialysis Patients Imen. Saudi J Kidney Dis Transpl. 2016;27(1):23–28. doi:10.4103/1319-2442.174057
10. Savadi H, Khaki M, Javnbakht M, Pourrafiee H. The impact of hemodialysis on sexual function in male patients using the international index of erectile function questionnaire (IIEF). Electron Physician. 2016;8(5):2371–2377. doi:10.19082/2371
11. Lai CF, Wang YT, Hung KY, et al. Sexual dysfunction in peritoneal dialysis patients. Am J Nephrol. 2007;27(6):615–621. doi:10.1159/000108357
12. Mekki MO, El hassan KA, El Mahdi EM, et al. Prevalence and associated risk factors of male erectile dysfunction among patients on hemodialysis and kidney transplant recipients: a cross-sectional survey from Sudan. Saudi J Kidney Dis Transpl. 2013;24(3):500–506. doi:10.4103/1319-2442.111023
13. Winarta GK, Duarsa GWK, Kandarini Y. Perbedaan derajat disfungsi ereksi pada pasien penyakit ginjal kronik derajat 5 sebelum dan setelah menjalani continuous ambulatory peritoneal dialysis. Medicina. 2020;51:3.
14. Azevedo P, Santos R, Duraes J. Sexual dysfunction in men and women on peritoneal dialysis: differential link with metabolic factors and quality of life perception. Revista Nefrologia. 2014;34(6):703–709.
15. Makkar V, Kumar M, Mahajan R, et al. Comparison of outcomes and quality of life between hemodialysis and peritoneal dialysis patients in Indian ESRD population. J Clin Diagn Res. 2015;9(3):OC28–OC31. doi:10.7860/JCDR/2015/11472.5709
16. DeLay KJ, Haney N, Hellstrom WJ. Modifying risk factors in the management of erectile dysfunction: a review. World J Men Health. 2016;34(2):89–100. doi:10.5534/wjmh.2016.34.2.89
17. Pastuszak AW, Khera M. Erectile Dysfunction: Etiology and Risk Factors. InContemporary Treatment of Erectile Dysfunction. Cham: Humana Press; 2016:57–70.
18. Kaya E, Sikka SC, Gur S. A comprehensive review of metabolic syndrome affecting erectile dysfunction. J Sex Med. 2015;12(4):856–875. doi:10.1111/jsm.12828
19. Sanchez E, Pastuszak AW, Khera M. Erectile dysfunction, metabolic syndrome, and cardiovascular risks: facts and controversies. Transl Androl Urol. 2017;6(1):28. doi:10.21037/tau.2016.10.01
20. Mirone V, Fusco F, Cirillo L, Napolitano L. Erectile Dysfunction: From Pathophysiology to Clinical Assessment. In: Practical Clinical Andrology. Cham: Springer; 2023:25–33.
21. Yang Y, Song Y, Lu Y, Xu Y, Liu L, Liu X. Associations between erectile dysfunction and psychological disorders (depression and anxiety): a cross‐sectional study in a Chinese population. Andrologia. 2019;51(10):e13395. doi:10.1111/and.13395
22. Mourikis I, Antoniou M, Matsouka E, et al. Anxiety and depression among Greek men with primary erectile dysfunction and premature ejaculation. Ann Gen Psychiatry. 2015;14(1):1–8. doi:10.1186/s12991-015-0074-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.