")
Back to Journals » Lung Cancer: Targets and Therapy » Volume 14
Stage as the Sole “Biomarker” for Adjuvant Pembrolizumab in Resected Stage IB to IIIA NSCLC without Considerations for PD-L1 Expression Level, ALK/EGFR Mutational Status, and Prior Adjuvant Chemotherapy per FDA Approval Indications of PEARLS/Keynote-091?
Authors Nagasaka M , Ou SI
Received 31 July 2023
Accepted for publication 5 December 2023
Published 12 December 2023 Volume 2023:14 Pages 101—109
DOI https://doi.org/10.2147/LCTT.S433195
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Fengying Wu
Misako Nagasaka,1– 3 Saihong Ignatius Ou1,2
1University of California Irvine School of Medicine, Orange, CA, USA; 2Chao Family Comprehensive Cancer Center, Orange, CA, USA; 3Division of Neurology, Department of Internal Medicine, St. Marianna University School of Medicine, Kawasaki, Kanagawa, Japan
Correspondence: Saihong Ignatius Ou, Chao Family Comprehensive Cancer Center, Department of Medicine, Division of Hematology Oncology, University of California Irvine School of Medicine, 200 South Manchester Avenue, Suite 400, Orange, CA, 92868-3298, USA, Tel +1-714-456-5153, Fax +1-714-456-2242, Email [email protected]
Abstract: One of the most recent advancements in NSCLC was the approval of immunotherapy in the adjuvant setting. Both atezolizumab and pembrolizumab have been approved for the use in early stage NSCLC patients post resection. As it broadens the options for our patients, multiple approvals in the same setting are generally welcomed. However, there were important differences in the two studies that led to the approvals and the data could be confusing. Here we review IMpower010, the study that led to the first approval of atezolizumab in the adjuvant setting with comparison to the Keynote-091 study evaluating pembrolizumab in the adjuvant setting, gaining the most recent FDA approval for adjuvant use in early stage NSCLC.
Keywords: post operative therapy, checkpoint inhibitors, atezolizumab, IMpower010, biomarker
Introduction
The use of immune checkpoint inhibitors (ICI) is now well-entrenched in the treatment of NSCLC with neoadjuvant use in combination with platinum-based chemotherapy,1 adjuvant treatment of resected early-stage NSCLC,2,3 as maintenance therapy after definitive chemoradiation for unresectable stage III NSCLC,4,5 single agent,6–9 or in combination with platinum-based chemotherapy as first-line treatment of advanced NSCLC10–16 to second line monotherapy after disease progression on platinum-based chemotherapy,17,18 the earliest approved indication for ICI in NSCLC. Dual checkpoint blockade with nivolumab and ipilimumab could be another option in some cases.19
One of the most recent advancements in NSCLC was the approval of immunotherapy in the adjuvant setting.2,3 Both atezolizumab and pembrolizumab have been approved for the use in early stage NSCLC patients post-resection (Table 1). As it broadens the options for our patients, multiple approvals in the same setting are generally welcomed. However, there were important differences in the two studies that led to the approvals and the data could be confusing. Here we review IMpower010, the study that led to the first approval of atezolizumab in the adjuvant setting with comparison to the PEARLS/Keynote-091 study evaluating pembrolizumab in the adjuvant setting, gaining the most recent FDA approval in early stage NSCLC.
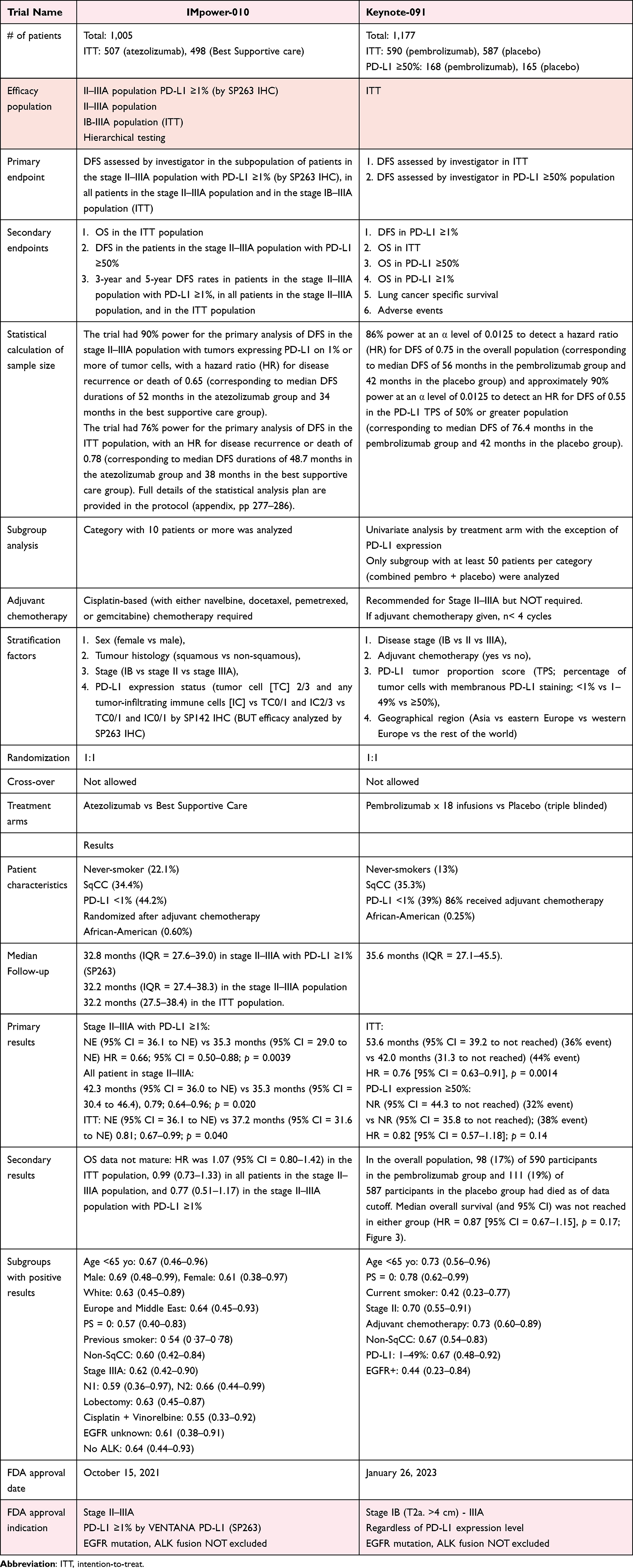 |
Table 1 Comparison of IMpower-010 and Keynote-091 Trial Characteristics and Approval Indication |
IMpower010 (NCT02486718) vs Keynote-091/PEARLS (NCT02504372)
In brief, atezolizumab’s adjuvant indication was approved based on the first hierarchical testing primary population (PD-L1 ≥1%, resected stage II–IIIA) although all resected stage II–IIIA still achieved their endpoint. The intention-to-treat (ITT) population (IB–IIIA) achieved a HR of 0.81 (0.67–0.99; p=0.040) but not statistically significant.2 On the other hand, the primary analysis population for Keynote-091 was the ITT population and there was statistically significant improvement in DFS with pembrolizumab over placebo, hence the FDA approved indication was from stage IB–IIIA regardless of PD-L1 expression level. From the subgroup analysis of Keynote-091, stage II and PD-L1 expression level 1–49% was positive for DFS benefit (HR = 0.67; 95% CI = 0·48–0·92).3 It is important to note that the prespecified analysis of DFS in subgroups of the overall population were performed on the basis of randomization stratification factors (disease stage, receipt of adjuvant chemo, PD-L1 TPS, and geographical region), histology, smoking status, sex, age, ECOG PS, race and EGFR mutation using a univariate Cox model with treatment as a single covariate, with the exception of PD-L1 TPS subgroup analyses for which a multivariate Cox proportional hazards model adjusted for the randomization stratification factors plus two additional factors of histology and smoking status were taken into account.
FDA Approval of PEARLS/Keynote-091 and IMpower010
Recently both atezolizumab and pembrolizumab have received FDA approval as monotherapy as additional treatment to adjuvant chemotherapy based on the IMpower-010 and PEARLS/Keynote-091 trials, respectively. Comparison of the trial characteristics are listed in Table 1.
The FDA drug approval process traditionally takes into account the whole study population (ITT) and if the ITT achieved the primary endpoint of survival (PFS, DFS, or OS) improvement, then the FDA will grant the indication to the whole ITT.20–22 The approval of IMpower010 came earlier than PEARLS/Keynote-091 and the indication was narrower for only resected II–IIIA resected NSCLC with PD-L1 ≥1% as that was the primary population in the first statistical hierarchical testing. Of note, in the IMpower010 study, randomization was stratified by sex, histology, stage, and PDL1 expression status and the prespecified exploratory subgroup analyses of DFS and OS included baseline demographics (age, sex, race, ethnicity) and prognostic characteristics (stage, PD-L1 expression, chemo regimen before randomization, histology, smoking history, and ECOG PS).2 Although one may argue that the benefit from IMpower010 was seen mostly in high PD-L1 TC ≥50% with a HR for DFS at 0.43 (0.27–0.68), since the primary population PD-L1 TC ≥1% was nonetheless positive with a HR for DFS at 0.66 (0.49–0.87), this lead to the FDA approval in this setting.2
Thus, while subgroup analysis of PEARLS/Keynote-091 demonstrated DFS benefit primarily among stage II patients, PD-L1 expression between 1–49%, receipt of adjuvant chemotherapy, non-squamous histology, and somewhat surprisingly patients who were EGFR+ (as EGFR mutations and ALK fusions were not excluded from both IMpower010 and Keynote-091) as the study still reached its primary endpoint, the FDA approval was granted in that setting. Overall, a “blanket” approval without regard to PD-L1 expression (analyzed by multivariate model just like the HR for the ITT) by the US FDA, while not surprising, abdicates its potential to set the treatment landscape based on available scientific evidence.
Design of PEARLS/Keynote-091 versus IMpower010
There were some differences in the design of PEARLS/Keynote-091 and IMpower010. PEARLS/Keynote-091 had a sample size calculation for an 86% statistical power planned for a HR of 0.75 for the ITT population3 compared to 0.78 for the ITT population of IMpower010.2 Furthermore, the robust sample size of Keynote-091 allowed for a 90% power to detect a HR of 0.55 in the PD-L1≥ 50%3 compared to the sample size powered for 90% power to detect HR of 0.65 improvement in DFS for II–IIIA patients with PD-L1 expression in the IMpower010 study.2
The control arm in PEARLS/Keynote-091 was placebo with triple-blinding, compared to the open label best supportive care arm as the control in IMpower010, which was another key difference in the two studies. The median number of treatments and median duration of treatment were similar among pembrolizumab- or placebo-arms.2,3
On-Going Trials
Two more “pure” adjuvant IO trials are on-going. First is adjuvant nivolumab (ANVIL) (NCT02595944) randomizing 903 patients to nivolumab 240 mg IV for 1 year versus observation with the co-primary endpoints of DFS and OS in the ITT population (stage IB greater than or equal to 4 cm, II and IIIA, NSCLC following surgical resection and standard adjuvant therapy). This design will allow for the approval of the ITT population if positive, but the co-primary endpoint of OS in the ITT is unlikely to be reached, given that in IMpower010, OS was only reached to date in II–IIIA stage patients whose tumor expressed PD-L1 ≥50%.23
Another important trial is BR-31 (NCT02273375), randomizing 1,350 patients to durvalumab versus placebo with co-primary endpoints of DFS in the PD-L1 ≥1% patients and then in the ITT population. While this trial will enroll the highest amount of patients out of the four trials, speculating from the PEARLS/Keynote-091 data, the PD-L1 ≥1% group is unlikely to be positive for DFS, making the presumed hierarchical testing of DFS in the ITT population not feasible.
Of note, both trials do not mandate the completion of four cycles of adjuvant chemotherapy and while the use of adjuvant chemotherapy was high in PEARLS/Keynote-091 and benefit was observed in patients with adjuvant chemotherapy, the role of adjuvant chemotherapy could still be potentially addressed by the remaining two trials.
Trial Design Lessons Learned from PERLS/Keynote-091 and IMpower010 (and Eventually ANVIL and BR31)
The “triumph” of pembrolizumab in the PEARSL/Keynote-091 study is the simplicity of this primary endpoint-DFS in the ITT and not the complicated multiple hierarchical testing by stage and PD-L1 expression or having OS as a co-primary endpoint. While embracing a dual-primary endpoint approach allows “multiple shots on the goal” for approval since it would be considered positive if at least one of the dual-primary endpoint was met, the nature of hierarchical testing does have inherent risks of not being able to carry out the next analysis if the first (or earlier) endpoints were not met.
Discussion
For the most part, multiple approvals in the same or similar setting are generally welcomed, as it broadens the options for our patients. However, when there are multiple options for adjuvant immunotherapy, how would you choose your treatment? Should we be offering adjuvant immunotherapy to everyone that fits the indication? Or, the more appropriate question may be who are the patients we should be offering adjuvant immunotherapy to? An approval does not necessarily mandate therapy. Just because the study met its primary endpoint, should we really be offering adjuvant immunotherapy to all comers?
The holy grail of immunotherapy in NSCLC is to identify both positive and negative predictive factors of responses. As such many of the FDA approval of (ICI) for the treatment of NSCLC includes selection of treatment broadly by the level of PD-L1 expression (<1%, 1–49%, ≥50%) (Table 2). Based on an FDA internal analysis, the use of single agent ICI resulted in statistically similar overall survival when compared to chemo + ICI. Thus, to avoid additional cost and toxicities, in patients with NSCLC tumors harboring PD-L1 expression ≥50%, most oncologists will use ICI monotherapy.24 Indeed with increasing levels of PD-L1 expression greater than 50%, the ORR and OS improved with single agent IO, as demonstrated in EMPOWER-Lung-01 and other studies.6–9
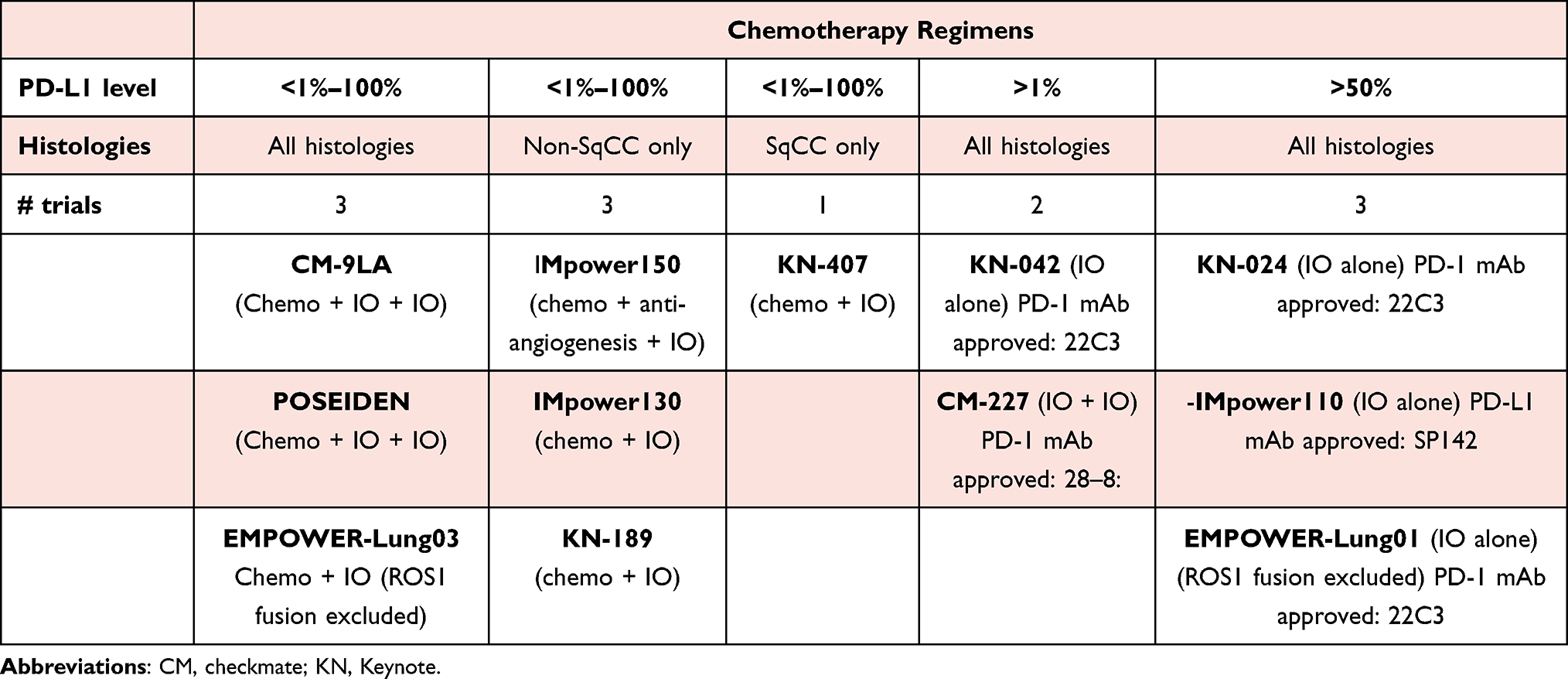 |
Table 2 Indications of the 12 Immunotherapy Regimens Approved by the FDA in US Circa February 2023 |
The current negative predictive factors for ICI use in advanced NSCLC are tumors that harbored the two well established actionable driver mutations (EGFR mutations and ALK ALK fusions). ROS1 fusions were a further exclusion biomarker if cemiplimab is used as a single agent (EMPOWER-1) or in combination (EMPOWER-3). Indeed all FDA indications for ICI use in advanced NSCLC excluded EGFR+ and ALK+ NSCLC even if these patients were included in IMpower15012 and IMpower130,13 two regimens approved by the US FDA, but EGFR+ and ALK+ NSCLC patients were excluded per prescribing package insert. This is a sound decision given there are now third-generation EGFR TKIs that confer median progression-free survival of ~20 months as first-line (1L) treatment of advanced EGFR+ NSCLC.25 Similarly, lorlatinib, a next-generation ALK TKI, is projected to confer >60 months PFS as 1L treatment of advanced ALK+ NSCLC.26
Furthermore, it is well established that ICI has minimum activity in EGFR+ NSCLC, even if the PD-L1 expression was ≥50%.27 In the adjuvant setting, osimertinib has conferred statistically significant improvement in disease-free survival in resected stage IB to IIIA EGFR+ NSCLC.28 Despite data being immature, it was still considered “positive” in the FDA risk-benefit analysis.29 One may argue that the benefit of adjuvant osimertinib derives mostly from its ability to prevent relapse in the central nervous system (CNS) during its 3 years of treatment, whereas the CNS activity of single agent immunotherapy remains uncertain.
Moreover, in those patients with EGFR and ALK (and potentially other targets), one must be cognizant of the increased toxicities the patient may face when given immunotherapy prior to the use of TKIs,27,30 whether it be in the adjuvant setting (ADAURA) or upon relapse.
Thus, in those patients with resected NSCLC cancer with the sensitizing EGFR mutations, the priority of adjuvant therapy should be given to adjuvant osimertinib, regardless of adjuvant chemotherapy or not,31 and clinicians should avoid adjuvant single agent immunotherapy, regardless of the PD-L1 score.
Issues to be Addressed
The Paradoxical Activity of IO in EGFR Mutations in PEARLS/Keynote-091
Some of the data from the subgroup analysis from Keynote-091 was somewhat puzzling and part of the issue we saw was how to interpret the paradoxical activity of immunotherapy in NSCLC with EGFR mutations. It is, however, important to note that the number of patients with EGFR mutations was only 39 (out of the 590 total patients in the pembrolizumab group; 7%) and having just a handful of patients with good outcomes may have skewed the data. Furthermore, it must also be noted that EGFR mutation status was not centrally confirmed and the type of EGFR mutations (del19, L858R, exon 20 insertions, sensitizing (or possibly unknown if sensitizing or not) “uncommon mutation”) were not reported, leaving some potential for false positives.
The Role of Adjuvant Chemotherapy
While the inclusion criteria for IMpower010 was in those who had completed resection and adjuvant chemotherapy,2 Keynote-091 did not mandate adjuvant chemotherapy.3 Based on the HR 1.25 (0.76–2.05) for DFS in the ITT population for those who did not receive adjuvant chemotherapy versus the HR being 0.73 (0.60–0.89) in those who received adjuvant chemotherapy, Keynote-091 appears to at least support the use of adjuvant chemotherapy and, at this time, there is no evidence to omit adjuvant chemotherapy to replace it with adjuvant immunotherapy, although this is a question that may be answered (perhaps partially) through the ongoing adjuvant immunotherapy studies.
Lack of African American Participations in IO Randomized Trials
In February 2022, the FDA’s Oncologic Drugs Advisory Committee convened to review the biologics license application of sintilimab, a checkpoint inhibitor that was developed and evaluated solely in China. The Oncologic Drugs Advisory Committee ultimately ruled 14–1 to require a clinical trial evaluating sintilimab in the US population, stating that the population studying sintilimab was not reflective of the US population.32 The oncology community as a whole must strive toward improving the enrollment of patients from minority groups, as IMpower010 and Keynote-091 only included 0.6% and 0.25% of African Americans, respectively, which certainly does not reflect the US population.
The Need to Identify Positive and Negative Biomarkers for IO Efficacy
As clinicians, we aspire to provide (survival) benefit while reducing toxicities and being able to tease out the patients both with positive and negative biomarkers for IO efficacy would be ideal. While PD-L1 and TMB have shown some value as predictive markers in the advanced/metastatic NSCLC setting,7,9 it is far from being perfect. Especially in the adjuvant setting where the bulk of the tumor is presumed resected, subjecting patients with further therapy that may cause toxicities must be justified by the benefit it would provide. We are not there yet to know the biomarkers for IO efficacy in adjuvant therapy, except for, perhaps, stage of disease; having stage IB–IIIA, regardless of PD-L1 expression or EGFR mutations. Stage was ultimately the one and only criteria for adjuvant pembrolizumab use per FDA approval of PEARLS/Keynote-091. In short, is stage now the new biomarker? We must do better and now is the time.
CRediT Authorship Contribution Statement
We confirm that both authors have made a significant contribution to the work reported. Both authors were involved in the conception, study design, execution, acquisition of data, analysis, and interpretation. Both authors drafted and revised the manuscript. Both have agreed on the journal to which the article will be submitted, and reviewed and agreed on all versions of the article before submission, during revision, and the final version accepted for publication. Both authors agree to take responsibility and be accountable for the content of the article.
Disclosure
There was no funding allocated for this research and there are no direct conflicts of interest. Potential COI from all authors are listed below.
MN is on the advisory board for AstraZeneca, Daiichi Sankyo, Takeda, Novartis, EMD Serono, Janssen, Pfizer, Eli Lilly and Company, Bayer, and Genentech; a consultant for Caris Life Sciences (virtual tumor board); a speaker for Blueprint Medicines, Janssen, Mirati and Takeda; and reports travel support from AnHeart Therapeutics.
SHIO has stock ownership and was on the scientific advisory board of Turning Point Therapeutics Inc (until February 28, 2019), is a member of the SAB of Elevation Oncology, and has received speaker honorarium from Merck, Roche/Genentech, Astra Zeneca, Takeda/ARIAD, and Pfizer; and has received advisory fees from Roche/Genentech, Astra Zeneca, Takeda/ARIAD, Pfizer, Foundation Medicine Inc, Spectrum, Daiichi Sankyo, Janssen/JNJ, and Xcovery.
References
1. Forde PM, Spicer J, Lu S, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N Engl J Med. 2022;386(21):1972–1985. doi:10.1056/NEJMoa2202170
2. Felip E, Altorki N, Zhou C, et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, Phase 3 trial. Lancet. 2021;398(10308):1344–1357. doi:10.1016/S0140-6736(21)02098-5
3. O’Brien M, Paz-Ares L, Marreaud S, et al. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB-IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): an interim analysis of a randomised, triple-blind, phase 3 trial. Lancet Oncol. 2022;23(10):1274–1286. doi:10.1016/S1470-2045(22)00518-6
4. Antonia SJ, Villegas A, Daniel D, et al. Durvalumab after chemoradiotherapy in stage iii non-small-cell lung cancer. N Engl J Med. 2017;377(20):1919–1929. doi:10.1056/NEJMoa1709937
5. Antonia SJ, Villegas A, Daniel D, et al. Overall survival with durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N Engl J Med. 2018;379(24):2342–2350. doi:10.1056/NEJMoa1809697
6. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
7. Mok TSK, Wu YL, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019;393(10183):1819–1830. doi:10.1016/S0140-6736(18)32409-7
8. Herbst RS, Giaccone G, de Marinis F, et al. Atezolizumab for First-Line Treatment of PD-L1-Selected Patients with NSCLC. N Engl J Med. 2020;383(14):1328–1339. doi:10.1056/NEJMoa1917346
9. Sezer A, Kilickap S, Gümüş M, et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: a multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet. 2021;397(10274):592–604. doi:10.1016/S0140-6736(21)00228-2
10. Gandhi L, Rodriguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22):2078–2092. doi:10.1056/NEJMoa1801005
11. Paz-Ares L, Luft A, Vicente D, et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med. 2018;379(21):2040–2051. doi:10.1056/NEJMoa1810865
12. Socinski MA, Jotte RM, Cappuzzo F, et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N Engl J Med. 2018;378(24):2288–2301. doi:10.1056/NEJMoa1716948
13. West H, McCleod M, Hussein M, et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019;20(7):924–937. doi:10.1016/S1470-2045(19)30167-6
14. Paz-Ares L, Ciuleanu TE, Cobo M, et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): an international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(2):198–211. doi:10.1016/S1470-2045(20)30641-0
15. Johnson ML, Cho BC, Luft A, et al. PL02.01 - Durvalumab ± Tremelimumab + Chemotherapy as First-line Treatment for mNSCLC: results from the Phase 3 POSEIDON Study. WCLC; 2021.
16. Gogishvili M, Melkadze T, Makharadze T, et al. LBA51 - EMPOWER-Lung 3: cemiplimab in combination with platinum doublet chemotherapy for first-line (1L) treatment of advanced non-small cell lung cancer (NSCLC). Anna Oncol. 2021;32(suppl_5):S1283–S1346. doi:10.1016/annonc/annonc741
17. Brahmer J, Reckamp KL, Baas P, et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med. 2015;373(2):123–135. doi:10.1056/NEJMoa1504627
18. Borghaei H, Paz-Ares L, Horn L, et al. Nivolumab versus docetaxel in advanced nonsquamous-cell non-small-cell lung cancer. N Engl J Med. 2015;373(17):1627–1639. doi:10.1056/NEJMoa1507643
19. Hellmann MD, Paz-Ares L, Bernabe Caro R, et al. Nivolumab plus ipilimumab in advanced non-small-cell lung cancer. N Engl J Med. 2019;381(21):2020–2031. doi:10.1056/NEJMoa1910231
20. Mushti SL, Mulkey F, Sridhara R. Evaluation of overall response rate and progression-free survival as potential surrogate endpoints for overall survival in immunotherapy trials. Clin Cancer Res. 2018;24(10):2268–2275. doi:10.1158/1078-0432.CCR-17-1902
21. Kok PS, Cho D, Yoon WH, et al. Validation of progression-free survival rate at 6 months and objective response for estimating overall survival in immune checkpoint inhibitor trials: a systematic review and meta-analysis. JAMA Netw Open. 2020;3(9):e2011809. doi:10.1001/jamanetworkopen.2020.11809
22. Tang PA, Pond GR, Chen EX. Influence of an independent review committee on assessment of response rate and progression-free survival in Phase III clinical trials. Ann Oncol. 2010;21(1):19–26. doi:10.1093/annonc/mdp478
23. Felip E, Altorki N, Vallieres E, et al. IMpower010: Overall Survival Interim Analysis of a Phase III Study of Atezolizumab Vs Best Supportive Care in Resected NSCLC. WCLC; 2022.
24. Akinboro O, Vallejo JJ, Nakajima EC, et al. Outcomes of anti-PD-(L)1 therapy with or without chemotherapy for first line treatment of advanced non-small cell lung cancer with PD-L1 score ≥ 50%: FDA pooled analysis. ASCO; 2022.
25. Ramalingam SS, Vansteenkiste J, Planchard D, et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N Engl J Med. 2020;382(1):41–50. doi:10.1056/NEJMoa1913662
26. Solomon BJ, Bauer TM, Mok TSK, et al. Efficacy and safety of first-line lorlatinib versus crizotinib in patients with advanced, ALK-positive non-small-cell lung cancer: updated analysis of data from the phase 3, randomized, open-label CROWN study. Lancet Respir Med. 2023;11(4):354–366. doi:10.1016/S2213-2600(22)00437-4
27. Lisberg A, Cummings A, Goldman JW, et al. A Phase II Study of Pembrolizumab in EGFR-Mutant, PD-L1+, Tyrosine Kinase Inhibitor Naïve Patients With Advanced NSCLC. J Thorac Oncol. 2018;13(8):1138–1145. doi:10.1016/j.jtho.2018.03.035
28. Wu YL, Tsuboi M, He J, et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer. N Engl J Med. 2020;383(18):1711–1723. doi:10.1056/NEJMoa2027071
29. Koch AL, Vellanki PJ, Drezner N, et al. FDA Approval Summary: osimertinib for Adjuvant Treatment of Surgically Resected Non-Small Cell Lung Cancer, a Collaborative Project Orbis Review. Clin Cancer Res. 2021;27(24):6638–6643. doi:10.1158/1078-0432.CCR-21-1034
30. Schoenfeld AJ, Arbour KC, Rizvi H, et al. Severe immune-related adverse events are common with sequential PD-(L)1 blockade and osimertinib. Ann Oncol. 2019;30(5):839–844. doi:10.1093/annonc/mdz077
31. Wu YL, John T, Grohe C, et al. Postoperative Chemotherapy Use and Outcomes From ADAURA: osimertinib as Adjuvant Therapy for Resected EGFR-Mutated NSCLC. J Thorac Oncol. 2022;17(3):423–433. doi:10.1016/j.jtho.2021.10.014
32. Benjamin DJ, Prasad V, Lythgoe MP. FDA decisions on new oncological drugs. Lancet Oncol. 2018;23:585–586. doi:10.1016/S1470-2045(22)00135-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.