")
Back to Journals » Clinical Optometry » Volume 15
Spotlight on Digital Eye Strain
Authors Mylona I , Glynatsis MN, Floros GD , Kandarakis S
Received 9 January 2023
Accepted for publication 22 February 2023
Published 27 February 2023 Volume 2023:15 Pages 29—36
DOI https://doi.org/10.2147/OPTO.S389114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Mr Simon Berry
Ioanna Mylona,1 Mikes N Glynatsis,2 Georgios D Floros,3 Stylianos Kandarakis4
1Department of Ophthalmology, General Hospital of Katerini, Katerini, Greece; 2Department of Ophthalmology, ‘Hippokration’, General Hospital of Thessaloniki, Thessaloniki, Greece; 3 2nd Department of Psychiatry, Aristotle University of Thessaloniki, Thessaloniki, Greece; 4 1st Department of Ophthalmology, General Hospital “G. Gennimatas”, National and Kapodistrian University of Athens, Athens, Greece
Correspondence: Ioanna Mylona, Ophthalmology Department, General Hospital of Serres, Serres, 62210, Greece, Tel +306941406978, Email [email protected]
Abstract: Digital Eye Strain (DES) is a clinical syndrome manifested with visual disturbances and/or ophthalmic dysfunction related to the usage of screen-enabled digital equipment. This term is gradually replacing the older term computer vision syndrome (CVS) that focused on the same symptoms found on personal computer users. DES is encountered more frequently during the past years due to the explosive increase in the usage of digital devices and subsequent increase in time in front of any screens. It presents with a series of atypical symptoms and signs stemming from asthenopia, dry eye syndrome, preexisting untreated vision issues and poor screen ergonomics. This review summarizes research data to date to determine whether the concept of DES has been conclusively defined and demarcated as a separate entity and if sufficient guidance is offered on professionals and the lay public. The maturity of the field, grouping of symptoms, examination techniques, treatment and prevention modalities are summarily presented.
Keywords: digital eye strain, computer vision syndrome, classification, management
Introduction
Vision problems attributable to prolonged viewing of screen-enabled digital devices have been reported since 19871 with an article detailing both ocular and orthopedic issues that were related to spending long hours in front of a computer terminal. Initially, the focus of research was the workplace, since screen-enabled devices were predominantly used for professional purposes due to their cost and size. However, the focus was expanded outside the workplace with the advent of home computing and the gradual reduction in size of screens with the shift from cathodic ray tubes to liquid crystal displays (LCDs) and light emitting displays (LEDs).2 “Terminology has changed as well, with the initial terms, which were limited to computer use” (computer vision syndrome – CVS) gradually expanding to “Digital eye strain – DES”,3 a term coined to include any type of digital screen. In either case, both terms, CVS and DES, have come to signify a clinical syndrome, which includes numerous eyesight symptoms related to lengthy engagement in front of a screen-enabled digital device.
DES symptoms are perceived as various degrees of irritation, which interferes with further screen viewing. Symptoms generally recede after some time away from the screen and receiving symptomatic treatment, while they may be prevented by correcting pre-existing errors in refraction or viewing habits. Although this syndrome has been widely reported and its existence even acknowledged by a number of professional bodies,4–7 its transient nature and wide variance of symptoms leads to challenges with classification of cases, assessing its prevalence and stipulating recommendations for both the professional and the lay public. Estimates of prevalence range from 33% of the general public, up to 50% for groups that are using digital screens for an extended period of time, as for example were children and college students following classes online due to restrictions imposed during the COVID-19 pandemic.8,9 These studies also demonstrate a clear increase of symptoms, which was proportional to the increase on time spent online. Symptoms overlap with, or are dependent on the existence of other nosological entities, such as dry eye disease or various causes of uncorrected refraction. The syndrome also includes symptoms of extraocular origin that are attributed to poor ergonomics of the environment where screen viewing takes place and are thus outside the immediate attention of the optometrist or ophthalmologist who would evaluate the patient. Despite these objective hurdles in assessment, a recent anonymous survey of 406 optometrists in the UK and Ireland10 found that the vast majority of respondents were in agreement that DES is an important concern for the profession (88.9%) with 91.4% responding that they felt confident in discussing symptoms and management options. It thus appears that adoption of DES is driven by necessity, despite those difficulties in its exact definition and classification. The purpose of this narrative review is to evaluate the significant body of research evidence that has accumulated over the years and determine whether the concept of DES has been conclusively defined and demarcated as a separate entity, and if sufficient guidance is offered on professionals and the lay public. We have opted for a narrative review, which focuses on recent developments, since the subject has been studied extensively for considerable time.
Materials and Methods
A search on PubMed with the most frequently employed terms (“digital eye strain”, “computer vision syndrome” and “video game vision”) returned more than 500 results. Interest has grown exponentially ever since the first related publication on 1987,1 with nearly 400 articles published during the past ten years and 280 within the past five. Thirty-five articles since 2002 have been reviews of previously published material11–43 and this article will present a synthesis of their findings and recommendations along with a limited number of guidelines and recommendations for the public from professional bodies. The latter include those of the American Optometric Association (AOA),5 American Academy of Ophthalmology,4 UK College of Optometrists7 and Canadian Association of Optometrists.6
Review
Maturity of the Field
Among this large number of reviews, the field appears to have matured enough to include suggestions for some very specific instances and special populations, such as children and adolescents.11,17,29,42 Video gamers,32,36 contact lens wearers,18 specific occupations and work environments.18,34,41 The conclusion is that there is sufficient body of evidence to draw conclusions regarding DES, provided there are no major changes in the way that screen-enabled devices are used in the near-future. This may change with future technological advances that will permit a near-field experience of digital visual content. The publication of the four sets of official guidelines and recommendations for the public4–7 appears timely.
Recommendations from Professional Bodies
Three professional associations have offered guidance for symptoms of DES to either the public or to professionals. The American Optometric Association has an online presentation of DES with useful information for professionals and patients alike, including tips on office ergonomics and suggestions for patients in order to alleviate the symptoms.5 Although the content is useful, the mixed nature of the presentation, which switches from a more professional note to suggestions for patients, is somewhat confusing.
The American Academy of Ophthalmology has an extensive online presentation, which includes information for the professional and the lay public.4 Although some effort was made to catalog this information in a logical manner, there are interspersed sections that include a list of potential issues with video display terminals outside the scope of DES (radiation, link to cataract formation, usage during pregnancy, sleep and neuro-psychiatric issues) and recommendations for children’s activity levels. Recommendations for management also venture outside the scope of DES. Overall, there is useful information available but in need of a reflow to separate sections.
The Canadian Association for Optometrists is addressing the lay public with a simple online presentation of possible symptoms and practical advice for self-help and prevention.6 There is a set of simple questions regarding the usage of screens for the patient when visiting a professional which should ideally be read beforehand; these include duration of use, distance to the screen, workstation setup and lighting. Tips on ergonomics and rest time between screen sessions are offered along with the possibility of using artificial tears for dry eye symptoms and appropriate lenses for refraction issues.
The UK’s Royal College of Optometrists does not formally employ the term DES on its website. However, it does offer guidance for professional practice when examining patients who work with display screen equipment or computers.7 There is no suggestion that patients may be affected by other types of screentime however and the overall focus is on symptoms of DES from the viewpoint of a professional hazard.
Despite the existence of those recommendations from official professional bodies, there is little in the way of commonly accepted attributes for DES. This is apparent in the employed terms, the clinical symptoms and signs, the diagnostic procedures and the suggestions regarding prevention and treatment.
Terminology of Choice
Along with DES, the term “CVS” still persists in the relevant literature up to 2022.2,5,16,20–24,28,37,44 There is no clear rationale for choosing one term over the other on offer in any publication or official set of recommendations, while some authors include both terms.4,6 The term “CVS” appears more in line with accepted medical terminology since it implies the existence of a specific syndrome in the domain of vision. However, the keyword “computer” is very limiting in the day and age where computational powers are embedded in a wide variety of handheld and household appliances whose principal use is other (eg, smartphones, TVs, etc.). DES as a term, on the one hand, is more suitable to the source of the problem (all things digital) and appears more friendly to the lay public, yet limits the description to the sense of eye strain. Clearly both terms are not sufficient to describe the clinical syndrome and its causes. However, establishing yet another term would be counter-productive. Hence, our suggestion would be to prefer the employment of the term DES since it will be more easily conveyed in a public initiative to attract attention to the issue, an important consideration since the syndrome is affecting children and adolescents to an alarming extent.
Attributes of DES as a Clinical Syndrome
A large number of symptoms and signs have been associated with DES and these overlap in nearly all publications. They can be divided into four major categories (Table 1).
- Symptoms and signs of asthenopia.
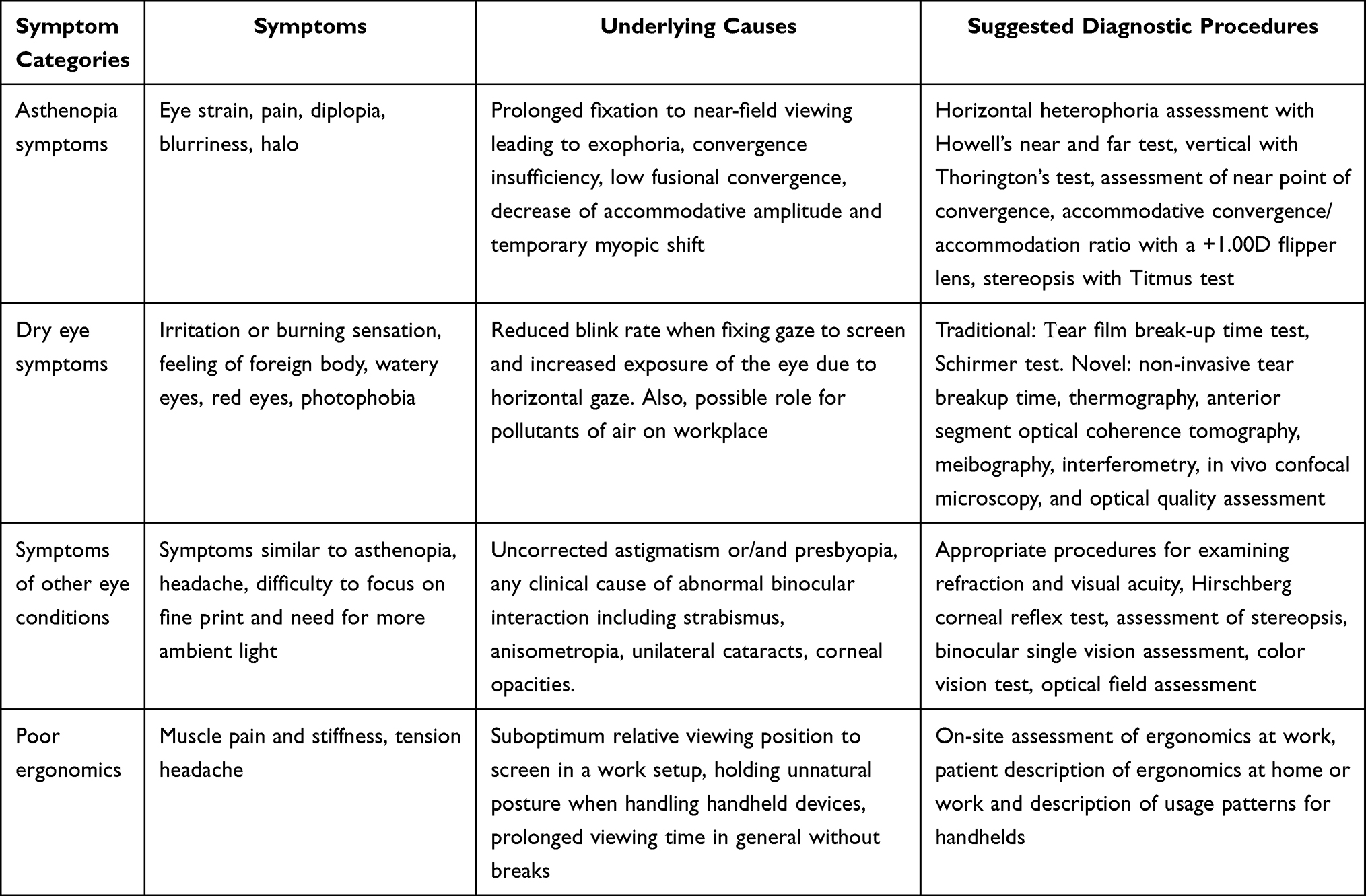 |
Table 1 DES Symptom Categories and Diagnostic Procedures |
Asthenopia, or eye strain, in DES relates to the process of fixing the glance while using a computer terminal or otherwise screen-enabled device for a long period of time. Asthenopia in the past has been used as an all-encompassing term for DES symptoms, however it is now limited to the subjective feeling of discomfort stemming from convergence insufficiency during prolonged screen time. The subjective feeling of eye strain is attributed to the presence of changes in accommodative and vergence functions including exophoria, convergence insufficiency, low fusional convergence, decrease of accommodative amplitude and temporary myopic shift. Changes are transient, with no lasting impact after the subjects reduced their involvement with screens.
Dry eye syndrome in DES is attributable to reduced blink rate and increased exposure of the eye due to horizontal gaze, which are both common during prolonged screen viewing.
Those will lead to subjective discomfort in shorter period of exposure compared to unaffected individuals, but they are expected to diminish once the underlying issue is resolved.
These are musculoskeletal problems (muscle stiffness and pain of the shoulders, neck and back, also tension headaches) that are attributed to assuming body positions that generate tension for a prolonged period of time, either in a work environment or outside work. The home environment is not regulated to professional standards and there is the added burden of using a handheld device, typically not at a desk.
There is also a significant number of technical factors that play a role on the development of symptoms including: display quality, display refresh rate, display size, display readability and legibility, and ambient environmental lighting during use.
However, there is an open question as to the relative degree of importance of these variables on the severity of DES, particularly regarding asthenopia. A recent study45 of DES patients for the prevalence of binocular and accommodative anomalies, to evaluate potential mechanisms for the benefit from +0.75D addition lens did not find an important role for binocular and accommodative anomalies, save for the rarer instances of patients who had an eso-fixation disparity on the near Mallett unit. A comparative study of smartphone users to users of virtual reality head-mounted displays (VR SHMD) following two hours of continuous use, found significant changes in near-point convergence and accommodation, exophoric deviation, stereopsis, and accommodative lag after the use of the VR SHMD but not after that of smartphones.46 Given that the proximity of the eye to the VR SHMD units was minimal (50 mm to 65 mm) it would appear that the effect of using digital screens at the typical viewing distances could be negligible per se; this however does not denote that their additive effect in conjunction with other sources of ocular discomfort would not be clinically meaningful. Indeed, a comparative study of viewing a documentary movie via smartphone or tablet47 showed a decrease in post-use near point accommodation and convergence, which was larger for smartphone use, yet the accommodative response induced by dynamic accommodative stimulus of auto refractometer/keratometer did not change significantly post-use. The subjects reported more subjective discomfort after smartphone use, even when use time was shorter. Apparently, the eye discomfort may be only appreciable immediately after using the display, at least in adults. Reports, however, from the study of children and pre-teens found some evidence for an increase in convergence disorders following lengthy periods of online study during the COVID-19 epidemic; these included an increase in cases of acute acquired comitant esotropia48 and an increase of mean near exophoria, negative fusional vergence and accommodation amplitude,49 following more than four hours of daily smartphone use. The examination of variables related to asthenopia could be more important in children.
Diagnostic Procedures for DES and Diagnostic Issues
Proposed diagnostic procedures relate to the four symptom categories (Table 1); clinicians should examine patients for the variables related to asthenopia and dry eye syndrome, they should ensure that no comorbid eye conditions are undetected or inadequately treated, while providing suggestions for better ergonomics during screen use. The examination of the accommodative and vergence functions would include standard procedures for the evaluation of ocular motility and squint,50 examination of vergence insufficiency,51 near point of accommodation, accommodative response and amplitude.47 A multitude of new methods for the non-invasive diagnosis of dry eye syndrome are becoming available,52 and are expected to help more than the less reliable or reproducible tear film break-up time test and Schirmer test. These include non-invasive tear breakup time, thermography, anterior segment optical coherence tomography, meibography, interferometry, in vivo confocal microscopy, and optical quality assessment. Refraction should be re-evaluated; small refractive errors may aggravate symptoms, while uncorrected presbyopia for adults over forty years of age could be first diagnosed during the examination for DES-related complaints. Posture-related symptoms are harder to assess outside a work environment and the advent of handheld screen-enabled devices has made this factor even harder to examine and control.53 The patient could be instructed to measure a number of variables related to office ergonomics like the distance-to-screen and relative height of the line-of-eyesight and screen. However, other related parameters including relative angle to screen, ambient lighting and glare are hard to assess.
The use of diagnostic questionnaires for DES has been suggested by the American Academy of Ophthalmology for evaluating the severity of the syndrome.4 A number of questionnaires are now available, including the Visual Fatigue Questionnaire,54 the CVS questionnaire (CVS-Q),55 the Computer Vision Symptom Scale (CVSS17)56 and the Digital Eye Strain Questionnaire (DESQ).57 All questionnaires attempt to cover the range of symptoms and may include either individual subfactors, which cluster groups of related symptoms57 or attempt to measure the severity of individual symptoms.55,56 All such questionnaires attempt to assess subjective discomfort and not objective eyesight parameters, thus any wide-arching conclusion on the objective burden of DES on the patient’s eyesight should be discouraged. Furthermore, the question that was raised above, of the relative importance of symptoms in the severity of DES, is not addressed in any questionnaire. Hence, a false outcome of more or less severe impediment for the patient may be formed on the basis of these self-report questionnaires, since the effect of a small number of more severe manifestations may be equalized with a larger number of less severe ones in a total unweighted score. Also, since the symptoms fall into any one of the four different domains that were described above, it is unclear whether they may affect one another and to which extent, or whether they may be ordered in a clear time sequence. Their use would be of help in large-scale screening for the syndrome symptoms and an individual follow-up on the response following treatment.
Prevention and Management of DES
There is consensus on all reviews that management of DES is dependent on the results from the diagnostic procedures and underlying disorders; the existence of asthenopia, dry eye syndrome, any uncorrected visual issues, or poor ergonomics should be addressed according to established professional guidelines. However, prevention is key, since on the one hand all symptoms are potentially avoidable to a significant extent and on the other hand treating the symptoms without resolving their root causes will lead to a relapse. All sets of existing guidelines on DES4–7 offer such guidance on DES prevention, although the framing is problematic and the average reader needs to skim through the entire publication and cherry-pick the relevant information. Separate sets of guidelines for the workplace, daily use of different handheld devices and for the parents of underage children would be ideal. Material in a printable hand-out form that the professional can have available in the consultation office would be helpful. Furthermore, there is little experimental evidence to confirm the effectiveness of a number of proposed treatments. Such an example is the proposed use of blue-light blocking glasses. LED screens and lighting have an intense emission in the blue wavelength, linked with retinal damage in experimental models58 and circadian rhythm disruption. The use of glasses that selectively block this wavelength has been suggested as a protective measure against DES symptoms,5 yet recent randomized studies have disputed this claim.59,60 Various manufacturers have claimed that their specially designed products reduce focusing efforts while looking at computer screens, and although using these products has been suggested as a potential optical aid,6 there are no experimental data in peer-reviewed publications to back it up. A list of suggestions regarding prevention and management of DES is presented in Table 2.
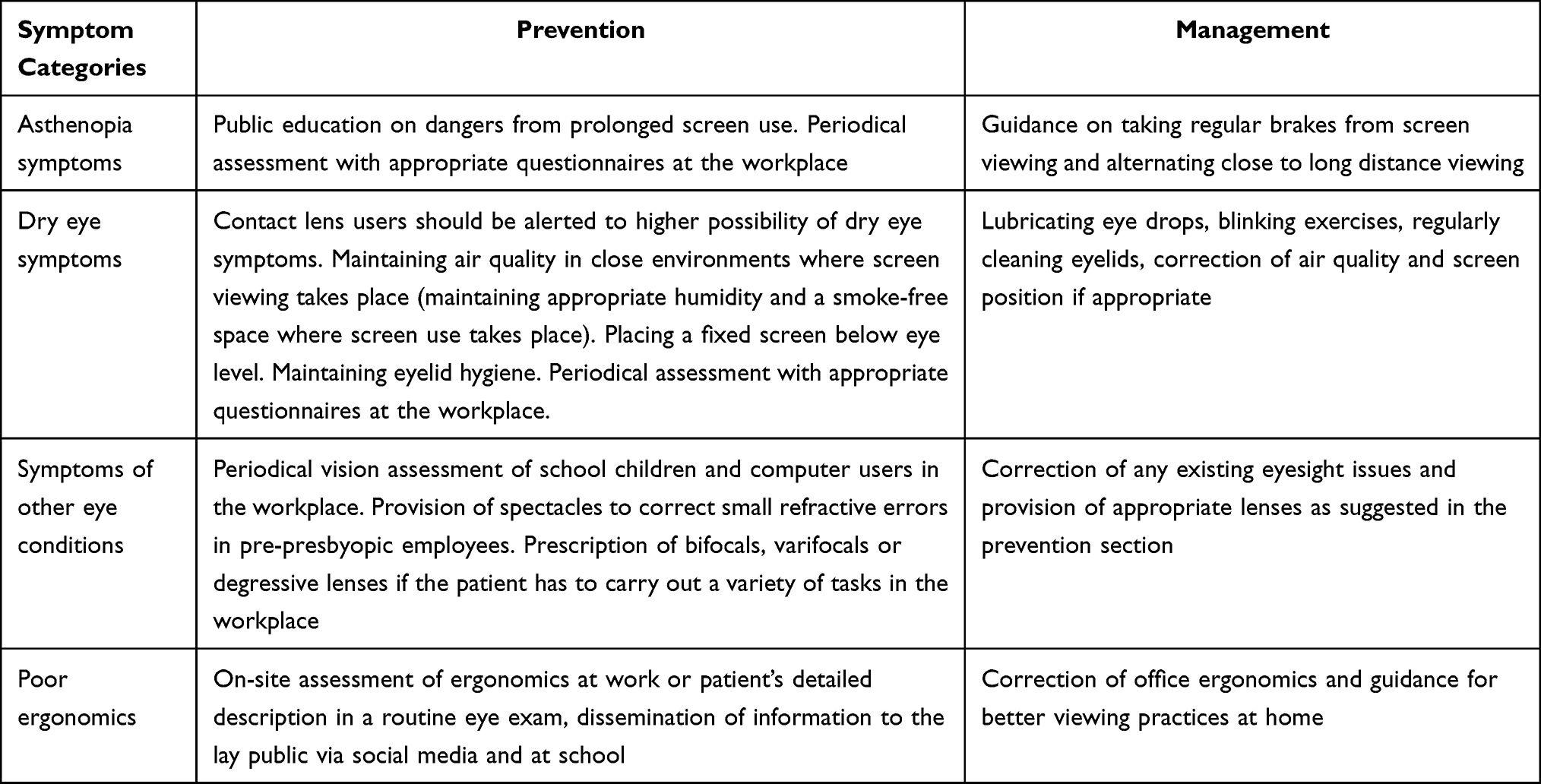 |
Table 2 Management and Prevention of DES |
Conclusion
Although there is a wealth of relevant studies, reviews and proposed guidelines available for DES, information for the lay public has not been filtered down to an easily accessible and clear format, while information for the professional may include suggestions, which remain unconfirmed, or even scientifically debunked. The need for standardization in proposed prevention and management strategies initially stemmed from the workplace; however, an additional challenge brought about by the introduction and dominance of screen-enabled handheld devices has emerged. Head mounted displays are slowly creeping into the living room and an increased uptake of technology related to virtual reality in the near future will mean that near-field vision will further increase the importance of addressing DES.
Disclosure
The authors have no competing interests to disclose.
References
1. Grant AH. The computer user syndrome. J Am Optom Assoc. 1987;58:892–901.
2. Blehm C, Vishnu S, Khattak A, Mitra S, Yee RW. Computer vision syndrome: a review. Surv Ophthalmol. 2005;50:253–262. doi:10.1016/j.survophthal.2005.02.008
3. Sheppard AL, Wolffsohn JS. Digital eye strain: prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018;3:e000146. doi:10.1136/bmjophth-2018-000146
4. American Academy of Ophthalmology. Computer vision syndrome (digital eye strain). EyeWiki. Available from: https://eyewiki.aao.org/Computer_Vision_Syndrome_(Digital_Eye_Strain).
5. American Optometric Association. Computer vision syndrome. Healthy eyes. Available from: https://www.aoa.org/healthy-eyes/eye-and-vision-conditions/computer-vision-syndrome?sso=y.
6. Canadian Association of Optometrists. Computer vision syndrome (digital eye strain). Eye Health Library. Available from: https://opto.ca/eye-health-library/computer-vision-syndrome-digital-eye-strain.
7. College of Optometrists UK. Examining patients who work with display screen equipment or computers. Clinical Guidance. Available from: https://www.college-optometrists.org/clinical-guidance/guidance/knowledge,-skills-and-performance/examining-patients-who-work-with-display-screen-eq.
8. Ganne P, Najeeb S, Chaitanya G, Sharma A, Krishnappa NC. Digital eye strain epidemic amid COVID-19 pandemic – a cross-sectional survey. Ophthalmic Epidemiol. 2021;28:285–292. doi:10.1080/09286586.2020.1862243
9. Mohan A, Sen P, Shah C, Jain E, Jain S. Prevalence and risk factor assessment of digital eye strain among children using online e-learning during the COVID-19 pandemic: digital eye strain among kids (DESK study-1). Indian J Ophthalmol. 2021;69:140–144. doi:10.4103/ijo.IJO_2535_20
10. Moore PA, Wolffsohn JS, Sheppard AL. Attitudes of optometrists in the UK and Ireland to digital eye strain and approaches to assessment and management. Ophthalmic Physiol Opt. 2021;41:1165–1175. doi:10.1111/opo.12887
11. Kerr CM, Tappin DM. Do poor nutrition and display screens affect visual acuity in children? Br J Community Nurs. 2002;7:80–89. doi:10.12968/bjcn.2002.7.2.9206
12. Gillespie RM. The physical impact of computers and electronic game use on children and adolescents, a review of current literature. Work. 2002;18:249–259.
13. Barar A, Apatachioaie ID, Apatachioaie C, Marceanu-Brasov L. [Ophthalmologist and “computer vision syndrome”]Oftalmolog și “computer vision syndrome”. Oftalmologia. 2007;51:104–109. Romanian.
14. Loh K, Redd S. Understanding and preventing computer vision syndrome. Malays Fam Physician. 2008;3:128–130.
15. Pimenidi MK, Polunin GS, Safonova TN. [Meibomian gland disfunction in computer vision syndrome]Мейбомиан гланд дисфунцтион ин цомпутер висион синдроме. Vestnik oftalmologii. 2010;126:49–52. Russian.
16. Rosenfield M. Computer vision syndrome: a review of ocular causes and potential treatments. Ophthalmic Physiol Opt. 2011;31:502–515. doi:10.1111/j.1475-1313.2011.00834.x
17. Straker L, Abbott R, Collins R, Campbell A. Evidence-based guidelines for wise use of electronic games by children. Ergonomics. 2014;57:471–489. doi:10.1080/00140139.2014.895856
18. Tauste Francés A, Ronda-Pérez E, Seguí Crespo Mdel M. [Ocular and visual alterations in computer workers contact lens wearers: scoping review]Alteraciones oculares y visuales en personas que trabajan con ordenador y son usuarias de lentes de contacto: una revisión bibliográfica. Rev Esp Salud Publica. 2014;88:203–215. Spanish. doi:10.4321/S1135-57272014000200004
19. Sue D, Ray P, Talaei-Khoei A, Jonnagaddala J, Vichitvanichphong S. Assessing video games to improve driving skills: a literature review and observational study. JMIR Serious Games. 2014;2:e5. doi:10.2196/games.3274
20. Klamm J, Tarnow KG. Computer vision syndrome: a review of literature. Med Surg Nurs. 2015;24:89–93.
21. Gowrisankaran S, Sheedy JE. Computer vision syndrome: a review. Work. 2015;52:303–314. doi:10.3233/WOR-152162
22. Parihar JK, Jain VK, Chaturvedi P, Kaushik J, Jain G, Parihar AK. Computer and visual display terminals (VDT) vision syndrome (CVDTS). Med J Armed Forces India. 2016;72:270–276. doi:10.1016/j.mjafi.2016.03.016
23. Munshi S, Varghese A, Dhar-Munshi S. Computer vision syndrome-a common cause of unexplained visual symptoms in the modern era. Int J Clin Pract. 2017;71:e12962.
24. Randolph SA. Computer vision syndrome. Workplace Health Saf. 2017;65:328. doi:10.1177/2165079917712727
25. Coles-Brennan C, Sulley A, Young G. Management of digital eye strain. Clin Exp Optom. 2019;102:18–29. doi:10.1111/cxo.12798
26. Ahmed SF, McDermott KC, Burge WK, et al. Visual function, digital behavior and the vision performance index. Clin Ophthalmol. 2018;12:2553–2561. doi:10.2147/OPTH.S187131
27. Jaiswal S, Asper L, Long J, Lee A, Harrison K, Golebiowski B. Ocular and visual discomfort associated with smartphones, tablets and computers: what we do and do not know. Clin Exp Optom. 2019;102:463–477. doi:10.1111/cxo.12851
28. Chawla A, Lim TC, Shikhare SN, Munk PL, Peh WCG. Computer vision syndrome: darkness under the shadow of light. Can Assoc Radiol J. 2019;70:5–9. doi:10.1016/j.carj.2018.10.005
29. Mylona I, Deres ES, Dere GS, Tsinopoulos I, Glynatsis M. The impact of internet and videogaming addiction on adolescent vision: a review of the literature. Front Public Health. 2020;8:63. doi:10.3389/fpubh.2020.00063
30. Talens-Estarelles C, García-Marqués JV, Cervino A, García-Lázaro S. Use of digital displays and ocular surface alterations: a review. Ocul Surf. 2021;19:252–265. doi:10.1016/j.jtos.2020.10.001
31. Jahn SW, Plass M, Moinfar F. Digital pathology: advantages, limitations and emerging perspectives. J Clin Med. 2020;9(11):3697. doi:10.3390/jcm9113697
32. Emara AK, Ng MK, Cruickshank JA, et al. Gamer’s health guide: optimizing performance, recognizing hazards, and promoting wellness in esports. Curr Sports Med Rep. 2020;19:537–545. doi:10.1249/JSR.0000000000000787
33. Donthineni PR, Shanbhag SS, Basu S. An evidence-based strategic approach to prevention and treatment of dry eye disease, a modern global epidemic. Healthcare. 2021;9:89. doi:10.3390/healthcare9010089
34. Londoño-Candonaza FE, Fiori-Chincaro GA, Agudelo-Botero AM, Llaguno-Rubio J, Arriola-Guillén LE. Occupational health in oral radiologists: a review. Dent Med Probl. 2021;58:405–410. doi:10.17219/dmp/134789
35. Kamøy B, Magno M, Nøland ST, et al. Video display terminal use and dry eye: preventive measures and future perspectives. Acta Ophthalmol. 2022;100:723–739. doi:10.1111/aos.15105
36. Szot M, Karpęcka-Gałka E, Dróżdż R, Frączek B. Can nutrients and dietary supplements potentially improve cognitive performance also in esports? Healthcare. 2022;10(2):186. doi:10.3390/healthcare10020186
37. Adane F, Alamneh YM, Desta M. Computer vision syndrome and predictors among computer users in Ethiopia: a systematic review and meta-analysis. Trop Med Health. 2022;50(1):26. doi:10.1186/s41182-022-00418-3
38. Priya DB, Subramaniyam M. Fatigue due to smartphone use? Investigating research trends and methods for analysing fatigue caused by extensive smartphone usage: a review. Work. 2022;72:637–650. doi:10.3233/WOR-205351
39. Singh S, McGuinness MB, Anderson AJ, Downie LE. Interventions for the management of computer vision syndrome: a systematic review and meta-analysis. Ophthalmology. 2022;129:1192–1215. doi:10.1016/j.ophtha.2022.05.009
40. Kaur K, Gurnani B, Nayak S, et al. Digital eye strain- a comprehensive review. Ophthalmol Ther. 2022;11:1655–1680. doi:10.1007/s40123-022-00540-9
41. Dahshan D, Rosdahl JA. Digital eye strain during the virtual interviews: evidence-based strategies for medical students. Digit J Ophthalmol. 2022;28:22–25. doi:10.5693/djo.01.2022.05.003
42. Bhattacharya S, Heidler P, Saleem SM, Marzo RR. Let there be light-Digital Eye Strain (DES) in children as a shadow pandemic in the era of COVID-19: a mini review. Front Public Health. 2022;10:945082. doi:10.3389/fpubh.2022.945082
43. Lem DW, Gierhart DL, Davey PG. Can nutrition play a role in ameliorating digital eye strain? Nutrients. 2022;14(19):4005. doi:10.3390/nu14194005
44. Mowatt L, Gordon C, Santosh ABR, Jones T. Computer vision syndrome and ergonomic practices among undergraduate university students. Int J Clin Pract. 2018;72(1):e13035. doi:10.1111/ijcp.13035
45. Yammouni R, Evans BJW. Is reading rate in digital eyestrain influenced by binocular and accommodative anomalies? J Optom. 2021;14:229–239. doi:10.1016/j.optom.2020.08.006
46. Yoon HJ, Moon HS, Sung MS, Park SW, Heo H. Effects of prolonged use of virtual reality smartphone-based head-mounted display on visual parameters: a randomised controlled trial. Sci Rep. 2021;11:15382. doi:10.1038/s41598-021-94680-w
47. Kang JW, Chun YS, Moon NJ. A comparison of accommodation and ocular discomfort change according to display size of smart devices. BMC Ophthalmol. 2021;21:1–9. doi:10.1186/s12886-020-01789-z
48. Mohan A, Sen P, Mujumdar D, Shah C, Jain E. Series of cases of acute acquired comitant esotropia in children associated with excessive online classes on smartphone during COVID-19 pandemic; digital eye strain among kids (DESK) study-3. Strabismus. 2021;29:163–167. doi:10.1080/09273972.2021.1948072
49. Mohan A, Sen P, Shah C, Datt K, Jain E. Binocular accommodation and vergence dysfunction in children attending online classes during the COVID-19 pandemic: digital Eye Strain in Kids (DESK) study-2. J Pediatr Ophthalmol Strabismus. 2021;58:224–231. doi:10.3928/01913913-20210217-02
50. Kuriakose T. Examination of ocular motility and squint. In: Clinical Insights and Examination Techniques in Ophthalmology. Springer; 2020:85–106.
51. Aletaha M, Daneshvar F, Mosallaei M, Bagheri A, Khalili MR. Comparison of three vision therapy approaches for convergence insufficiency. J Ophthalmic Vis Res. 2018;13:307. doi:10.4103/jovr.jovr_99_17
52. Di Cello L, Pellegrini M, Vagge A, et al. Advances in the noninvasive diagnosis of dry eye disease. Applied Sciences. 2021;11:10384. doi:10.3390/app112110384
53. Alabdulkader B. Effect of digital device use during COVID-19 on digital eye strain. Clin Exp Optom. 2021;104:698–704. doi:10.1080/08164622.2021.1878843
54. Rajabi-Vardanjani H, Habibi E, Pourabdian S, Dehghan H, Maracy MR. Designing and validation a visual fatigue questionnaire for video display terminals operators. Int J Prev Med. 2014;5:841–848.
55. Del Mar Seguí M, Cabrero-García J, Crespo A, Verdú J, Ronda E. A reliable and valid questionnaire was developed to measure computer vision syndrome at the workplace. J Clin Epidemiol. 2015;68:662–673. doi:10.1016/j.jclinepi.2015.01.015
56. González-Pérez M, Susi R, Antona B, Barrio A, González E. The Computer-Vision Symptom Scale (CVSS17): development and initial validation. Invest Ophthalmol Vis Sci. 2014;55:4504–4511. doi:10.1167/iovs.13-13818
57. Mylona I, Glynatsis MN, Dermenoudi M, Glynatsis NM, Floros GD. Validation of the digital eye strain questionnaire and pilot application to online gaming addicts. Eur J Ophthalmol. 2022;32:2695–2701. doi:10.1177/11206721211073262
58. Jaadane I, Boulenguez P, Chahory S, et al. Retinal damage induced by commercial light emitting diodes (LEDs). Free Radic Biol Med. 2015;84:373–384. doi:10.1016/j.freeradbiomed.2015.03.034
59. Palavets T, Rosenfield M. Blue-blocking filters and digital eyestrain. Optom Vis Sci. 2019;96:48–54. doi:10.1097/OPX.0000000000001318
60. Singh S, Downie LE, Anderson AJ. Do blue-blocking lenses reduce eye strain from extended screen time? A double-masked randomized controlled trial. Am J Ophthalmol. 2021;226:243–251. doi:10.1016/j.ajo.2021.02.010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.