")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 15
Spinal Dystonia Associated with Transverse Myelitis in an Adolescent Female: A Case Report
Authors Deginet E , Abebe AM, Abatkun M
Received 9 November 2023
Accepted for publication 15 January 2024
Published 20 January 2024 Volume 2024:15 Pages 1—4
DOI https://doi.org/10.2147/AHMT.S445606
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Endayen Deginet, Abeba Mengesha Abebe, Meskerem Abatkun
Department of Pediatrics and Child Health, School of Medicine, College of Health and Medical Sciences, Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Endayen Deginet, Email [email protected]
Background: Dystonia, one of the most common movement disorders, It was mostly a result of pathology in basal ganglia; there have been increasing numbers of dystonia cases reported in patients with spinal cord pathology.
Case Presentation: Here we report, a 14 year old female adolescent from Addis Ababa Ethiopia presented with dystonia of extremities within one month after she was diagnosed with transverse myelitis.
Conclusion: Although any spinal cord pathology can result in spinal dystonia, demyelinating diseases are among the leading causes. There are few case reports on dystonic spasm caused by acute transverse myelitis. This case report describes an instance of spinal dystonia associated with transverse myelitis in an adolescent female.
Keywords: spinal dystonia, transverse myelitis, adolescent
Introduction
Dystonia is a movement disorder characterized by sustained or intermittent muscle contractions causing abnormal, often repetitive movements, postures, or both. Dystonic movements are typically patterned and twisting, and may be tremulous.1
Dystonia can be inherited, acquired, or idiopathic. Inherited dystonia have proven genetic origins and acquired dystonias can be caused by structural disorders of the brain, drugs or toxins.
Dystonia occur mostly as a result of pathology in the basal ganglia but multiple brain areas including motor cortex, supplementary motor areas, cerebellum, and their connections can also be involved.
There are increasing numbers of dystonia cases reported in patients with spinal cord pathology. A recent study performed on mice to determine the role of the spinal cord in this movement disorder also supports the major role played by the spinal cord in dystonia.2
There are increasing numbers of dystonia cases reported in patients with spinal cord pathology. These movement disorders are called spinal-generated movement disorders (SGMDs) as they originate from the spinal cord, or the spinal cord plays an important role.2,3 A recent study on mice to determine the role of spinal cord in spinal-generated movement disorder also supports the major role played by the spinal cord in dystonia.4
Any spinal cord pathology can result in spinal dystonia. Demyelinating diseases, such as multiple sclerosis (MS) and neuromyelitis optica spectrum disorders (NMOSD) are among the leading causes of SGMDs. Novel presentation of severe dystonia in anti-MOG disease is also reported in pediatric patient.5
This case report will also be one of the very few cases reported on spinal dystonia and transverse myelitis in a pediatric patient.
Case Presentation
A 14 year old female adolescent presented with an acute onset of weakness involving all extremities of 10 days duration. Associated symptoms include numbness of the extremities, urinary incontinence, and constipation.
On neurologic examination at the time of presentation she was quadriplegic and the tone was hypotonic in all extremities due to spinal shock but progressively the tone was increased.
Brain MRI of the patient was normal and spinal magnetic resonance imaging (MRI) showed a long-segment cord lesion extending from the foramen magnum to the C7 level with mild cord expansion (Figures 1 and 2).
 |
Figure 1 Cervical spinal MRI shows T2 hyperintense lesions of the cervical cord from foramen magnum to C7 level. |
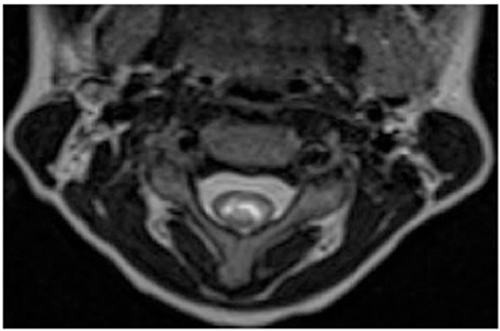 |
Figure 2 Cervical axial spinal MRI shows T2 hyper intense lesion at C2 level. |
She was treated with intravenous methylprednisolone IV for 5 days followed by IVIG for 2 days. She was discharged after 2 weeks of hospitalization with weekly tapered prednisolone and continuation of physiotherapy. She showed marked improvement and began to walk with support within one month.
During the recovery period, 5 weeks after the initial symptom, she developed dystonic posturing characterized by intermittent muscle contractions of the upper and lower extremities bilaterally with twisting (Figure 3). The attack gradually increased in frequency and recurred every 15 min, with each episode lasts for 30–40 seconds. It was then precipitated through exercise.
 |
Figure 3 Image of the patient with dystonic episodes. |
Brain MRI was normal. Genetic testing for selected primary dystonias that can manifest at this age (DYT-1 dystonia, DYT-5 and DYT11 dystonia) did not show genetic mutations.
She initially started treatment for dystonia with clonazepam, trihexyphenidyl, gabapentin, and baclofen, but showed no significant improvement and responded to carbamazepine 400 mg PO BID.
Discussion
There is an overlap of terms in the medical literature regarding spinal dystonia and tonic spasms. Spinal dystonia is defined as sustained contraction of antagonistic muscles resulting in complex abnormal posture (other than simple flexion, extension, or adduction) that can be paroxysmal or non-paroxysmal secondary to spinal cord pathology, whereas tonic spasms are sustained increases in muscle tone involving one set of muscle groups, leading to isometric contraction or simple posturing in flexion, extension, or adduction.2 Our patient had complex abnormal posturing involving the contraction of antagonistic muscles (Figure 2); therefore, we considered spinal dystonia rather than tonic spasm.
The case report of Chung and Kim presented a patient with tonic spasm as the first symptom of acute transverse myelitis6 and the recent case report by Khan et al also present a 3 year old child presented with dystonia during the acute phase of his illness.5 This is in contrast to our patient who presented with dystonia during the recovery phase and is similar to case report by Schmidt et al in 2011 on four female patients who were admitted with an acute attack of cervical or cervicodorsal myelitis and developed paroxysmal dystonia during the recovery phase. All patients were diagnosed with NMOSD, and the authors had difficulty explaining why these movements occurred at the time of recovery rather than during the acute phase. They speculated that severe damage to the spinal cord did not allow the clinical expression of paroxysmal dystonia in the acute phase of NMO. They concluded that a local biochemical imbalance during the recovery period could have prompted the disinhibition of spinal interneurons and the onset of paroxysmal dystonia.7
Our patient was treated with various medications, and showed significant improvement with carbamazepine. This is different from the patient reported by Khan et al, who responded to treatment with diazepam, baclofen, and botulinum toxin injections5 and is similar to the case report by Chung and Kim, who showed resolution of tonic spasm with carbamazepine.6 All four cases of paroxysmal dystonia reported by Schmidt et al also show improvement with carbamazepine.7 This can be explained by the hypothesis that ion dysfunction is the main pathophysiological mechanism underlying tonic spasm.8
Consent for Publication
Written informed consent was obtained from the patient and the patient’s mother for the publication of this case report. No institutional approval is required to publish the case details.
Disclosure
The authors report no competing interests in this work.
References
1. Albanese A, Bressman BK, Delong SB, et al. Phenomenology and classification of dystonia: a consensus update. Mov Disord. 2013;28:863–873.
2. Sarin S, Lawal T, Abboud H. Spinal dystonia and other spinal movement disorders. Dystonia. 2023;2:1.
3. Termsarasab P, Thammongkolchai T, Frucht SJ. Spinal-generated movement disorders: a clinical review. J Clin Mov Disord. 2015;2(1). doi:10.1186/s40734-015-0028-1
4. Pocratsky AM, Nascimento F, Özyurt MG, et al. Pathophysiology of Dyt1-Tor1a dystonia in mice is mediated by spinal neural circuit dysfunction. Sci Transl Med. 2023;15(694):eadg3904.
5. Khan TB, Waugh JL, Wang C. Anti-Myelin Oligodendrocyte Glycoprotein (MOG) antibody disease presenting with severe dystonia. Neuroimmunol Rep. 2021;1:1.
6. Chung EJ, Kim SJ. Tonic spasms in acute transverse myelitis. J Clin Neurosci. 2009;16. doi:10.1016/j.jocn.2008.05.007
7. Schmidt FR, Costa FH, Silva FM, et al. Paroxysmal dystonia and neuromyelitis optica. Arq Neuro-Psiquiatr. 2011;4(70):271.
8. Waubant E, Alizé P, Tourbah A, Agid Y. Paroxysmal dystonia (tonic spasm) in multiple sclerosis. Neurology. 2001;57(12):2320.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.