")
Back to Journals » Clinical Optometry » Volume 15
Spectacle Coverage Rate After Cataract Surgery in an Urban Area in Indonesia
Authors Rahayu T , Lestari YD, Ayudianingrum A, Rif'ati L
Received 19 May 2023
Accepted for publication 20 July 2023
Published 16 August 2023 Volume 2023:15 Pages 167—173
DOI https://doi.org/10.2147/OPTO.S417876
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Tri Rahayu,1,* Yeni Dwi Lestari,1,* Asti Ayudianingrum,1,* Lutfah Rif’ati2
1Ophthalmology Department, Faculty of Medicine Universitas Indonesia - Dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia; 2National Research and Innovation Agency, Jakarta, Indonesia
*These authors contributed equally to this work
Correspondence: Yeni Dwi Lestari, Jl. Kimia No. 8, RT.10/RW.1, Pegangsaan, Kec. Menteng, Jakarta Pusat, Daerah Khusus Ibukota, Jakarta, 10320, Indonesia, Tel +62 2131902885, Email [email protected]; [email protected]
Purpose: Uncorrected refractive errors after cataract surgery contribute to visual impairments. The aim of this study was to investigate the spectacle coverage rate (SCR) following cataract surgery and its relationship with socioeconomic factors in an urban city in Indonesia.
Patients and Methods: This population-based cross-sectional study was conducted in 2015 in Jakarta. The former participants of the Rapid Assessment of Avoidable Blindness (RAAB) survey had a history of cataract surgery and met either of the following criteria: (1) wore spectacles with presenting visual acuity (PVA) 6/12 or (2) had PVA less than 6/12 regardless of spectacle use but achieved the best visual acuity (BVA) 6/12 with pinhole correction.
Results: Of the 2998 participants of the RAAB survey, 173 (5.6%) (252 eyes) had a history of cataract surgery, among whom 53 (86 eyes) met our inclusion criteria. The SCR was 69.8% and was associated with age group, household income level, education level, and physicians’ recommendation of spectacle wear. Participants who were of nonproductive age (80%), had the highest household income level (88.2%), the highest level of education (87.5%), and had been recommended for spectacle use by their physicians (80.9%) demonstrated higher SCR. Participants with the highest household income had the highest SCR. Patients who had received a physician’s recommendation showed a higher SCR and were 26 times more likely to wear spectacles (odds ratio [OR] 25.99, 95% CI 2.59– 260.10).
Conclusion: There is an unmet need for refractive errors after cataract surgery. Factors such as household income levels and physician recommendations were predictive of spectacle wear.
Keywords: cataract surgery, RAAB, socioeconomic factors, spectacle coverage rate
Introduction
Cataract is the leading cause of blindness and the second leading cause of moderate-severe visual impairment after refractive errors.1 Uncorrected refractive error following cataract surgery still contributes to the prevalence of visual impairment and blindness with varying prevalence reaching 55.3%.2 A study in Ghana reported 90.4% of uncorrected refractive error.3 This is considerably higher than that in other countries such as China (39.5%), Singapore (57.1%), and India (52.5%).4–6 Therefore, despite its treatable nature through surgery, correction of refractive errors remains an issue.
Spectacle coverage rate (SCR), one of the parameters of the correction status of refractive errors in a population, differs across socioeconomic status. A study in Pakistan reported an SCR of 4.4% in a lower socioeconomic population.7 The use of corrective spectacles is thought to be related to socioeconomic factors. As a socioeconomic factor, poverty is estimated to affect the use of corrective spectacles and health awareness of visual impairment in individuals with refractive errors.
This was an advanced study of the Rapid Assessment of Avoidable Blindness (RAAB) survey in 2015 which estimated the prevalence and causes of blindness and visual impairment in people aged 50 years and above.8 The aim was to investigate the prevalence of met need and unmet need for spectacles following cataract surgery in former participants of the RAAB survey.
Materials and Methods
This population-based cross-sectional study was part of RAAB survey and was conducted in Jakarta in 2015 on people aged 50 years and above. The study adhered to the Declaration of Helsinki and was approved by the Universitas Indonesia Ethical Review Board (955UN.2F1/ETIK/2015) on 2 November 2015. Written informed consent was obtained from all participants prior to their enrollment in the study.
The minimum sample size formula for a cross sectional study was used. The type I error was set at 5%, precision was 5%, and known proportions of patients who had undergone cataract surgery in Cambodia was 6.1%.9 The final minimum sample size was 87.
Presenting visual acuity (PVA) was examined using a tumbling “E” chart with Snellen optotype sizes 6/12, 6/18, and 6/60. The best visual acuity (BVA) was measured using pinhole correction. The inclusion criteria were RAAB participants with a history of cataract surgery and either of the following conditions: (1) “met need” was defined as subjects who wore distance spectacles and had a PVA of 6/12 and (2) “unmet need” was defined as subjects who wore or did not wear distance spectacles and had a PVA of less than 6/12 but could achieve a BVA of 6/12. Participants with communication barriers, such as mental disorders, speech disorders, or severe hearing loss, were excluded. SCR was defined as the proportion of “met need” “divided by the sum of met need” and “unmet need”.
Household income level, education level, and occupation were independent variables. Age, sex, insurance, place of surgery, and physician information were analyzed as confounding variables. Age was later categorized into productive (50–64 years) and nonproductive (≥65 years) based on the definition established by the Indonesian Central Bureau Statistics. Household income levels were assessed using the National Socioeconomic Survey or Survei Sosial Ekonomi Nasional Indonesia 2014 questionnaire by considering the household profile and ownership of valuable objects. The first quintile is defined as the lowest household income level.
The data were processed using STATA 9 software. Household income levels were determined using the principal component analysis. Bivariate analysis was conducted using chi-squared or Fisher’s exact tests to assess the association of SCR with age, sex, household income level, education level, age, sex, insurance, place of surgery, and physician’s recommendation. These factors were later analyzed using multiple logistic regression to assess the potential predictors of “met need”. Multivariate logistic regression analysis was performed to assess the correlation between these factors and SCR (potential predictors of SCR).
Results
The total number of participants examined in the RAAB survey was 2998, and 173 (5.8%) of whom (252 eyes) had a history of cataract surgery. Most eyes 241/252 (95.6%) had an intraocular lens (IOL). Post-operative distance refractive error was found in 53/252 eyes (21.0%). Following surgery, 167/241 (69%) eyes had a PVA of 6/18 or better and 187/252 (74%) eyes had a BVA of 6/18 or better. Of the 11 participants who had no IOL following surgery, 10 (91%) had a PVA worse than 6/60. However, this number decreased to 6/11 (55%) after the pinhole correction. Visual acuity outcomes after surgery are shown in Table 1.
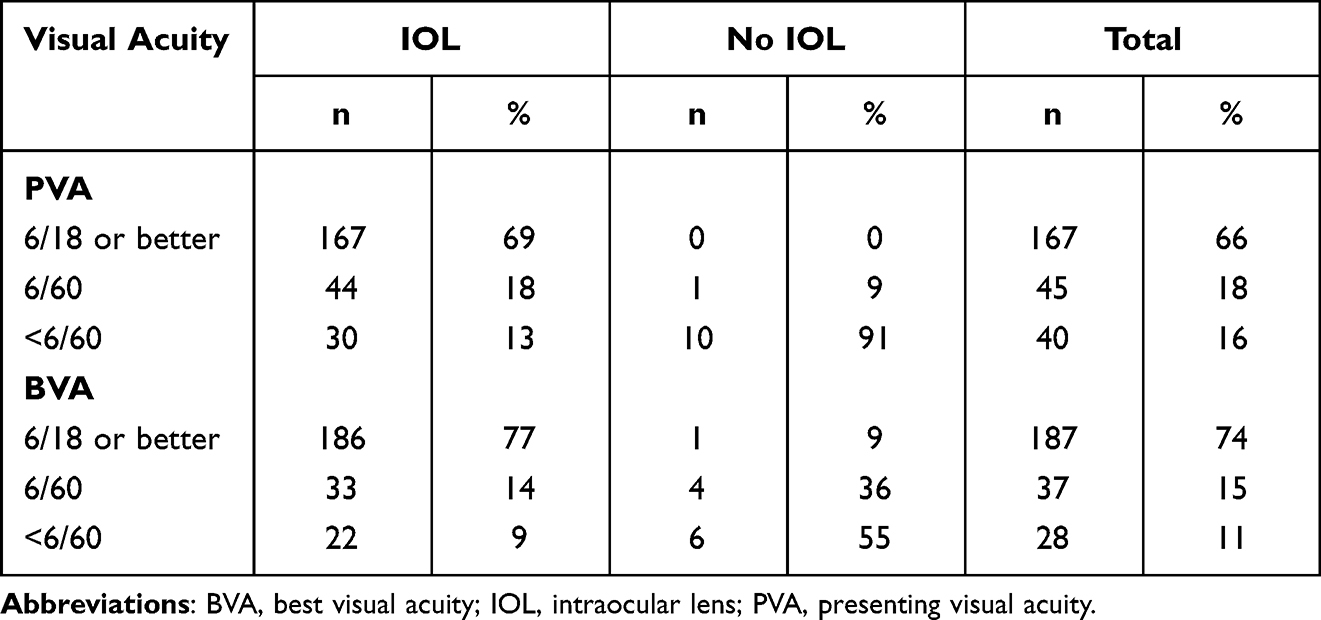 |
Table 1 Visual Acuity Outcomes After Cataract Surgery |
Fifty-three participants (86 eyes) met our inclusion criteria. Our subjects were mostly female (66%), aged 70 (50–86), employed (75.5%), and had IOL implants (97%). Table 2 shows demographic characteristics of the subjects. The majority of the subjects (92%) had a BVA better than 6/18, 2/86 (2%) could see better than 6/60, 1/86 (1%) could see better than 3/60, and 4/86 (5%) were blind.
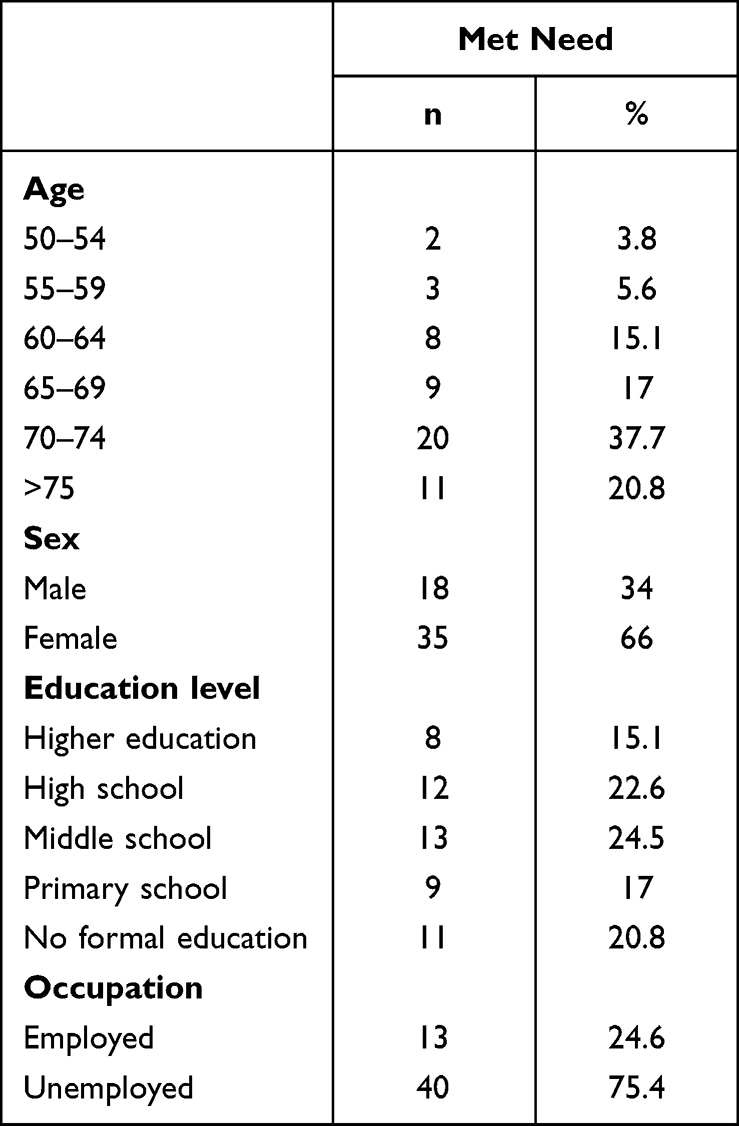 |
Table 2 Demographic Characteristics of Subjects |
Among 53 participants, 37 had “met need” criteria; thus, the SCR was 69.8%. Table 3 shows the bivariate analysis of the spectacle coverage group with socioeconomic and confounding variables. There was a significant difference between household income levels (p<0.05) with the third quintile showing the highest SCR. Statistically significant differences (p<0.05) were observed among education levels, and the highest SCR was found in subjects with at least postgraduate education background. The unemployed group had a higher SCR; however, there was no significant difference between the groups (p>0.05).
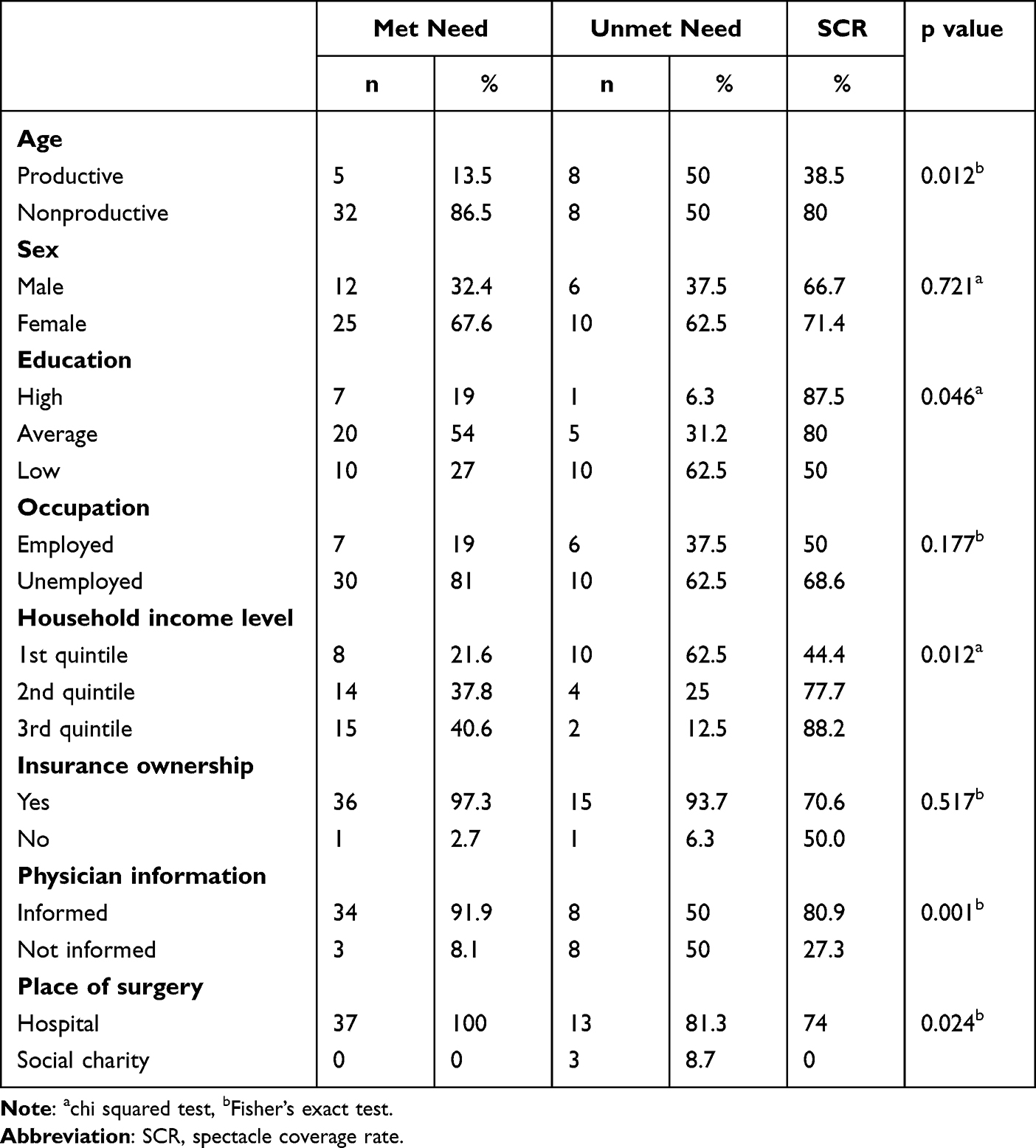 |
Table 3 Bivariate Analysis of Spectacle Coverage Group with Socioeconomic and Confounding Variables |
Age, place of surgery, and physician information were significantly different between the two groups (p<0.05). Subjects of nonproductive age, those who underwent surgery in the hospital, and those who were informed by physicians about spectacle use were reported to have a higher SCR.
There were no significant differences between the sexes and insurance groups. Most respondents (96%) had health insurance; however, 43% were unaware of the spectacle-related benefits. Table 4 presents the distribution of spectacle prescription status for PVA. Reasons for spectacle non-wear such as unawareness of problems (58.4%), need not felt (33.3%), and social stigma (8.3%) were observed.
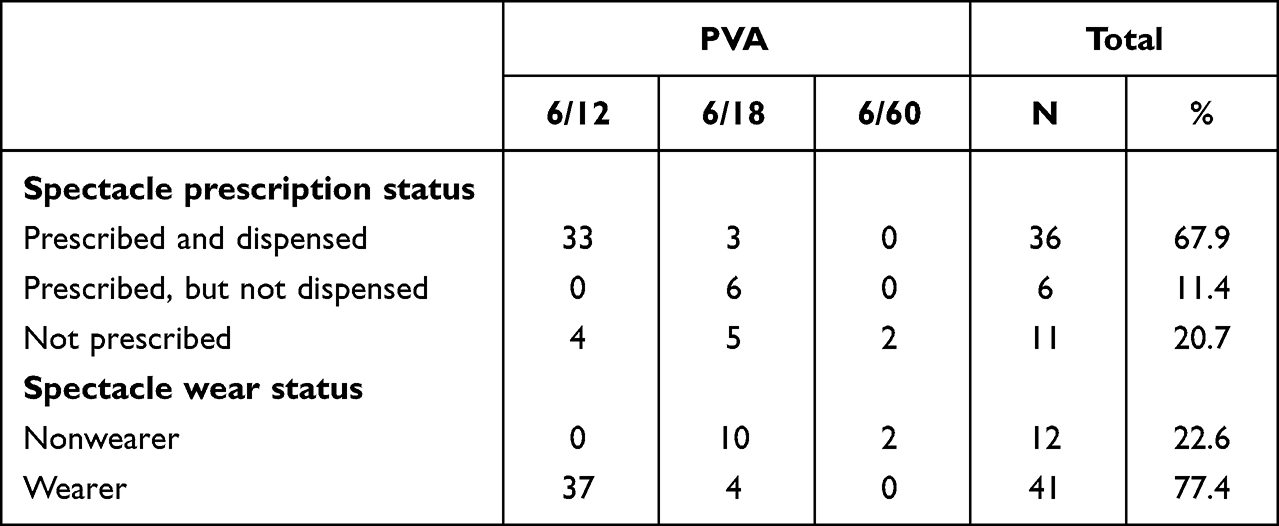 |
Table 4 Distribution of Spectacles Prescription Status and Presenting Visual Acuity |
Multiple logistic regression was conducted for all variables, with a p-value less than 0.25. Multivariate analysis determined the predictive factors that influenced SCR. The value of SCR was directly proportional with the proportion of “met need”. The higher the proportion of “met need”, the higher the SCR value.
As shown in Table 5, a significant association was found between “met need” and physician’s recommendation with odds ratio (OR) 25.99 (95% CI 2.59–260.10), age OR 7.78 (95% CI 1.01–59.93), and household income levels OR 4.39 (95% CI 1.10–17.47). Physician information, age group, and household economic level were predictive variables strongly related to SCR. Physician information and age were confounding variables, aside from socioeconomic factors that might influence SCR. The confidence interval of this analysis was found to be within a broad range; however, the power analysis of this study was 80%.
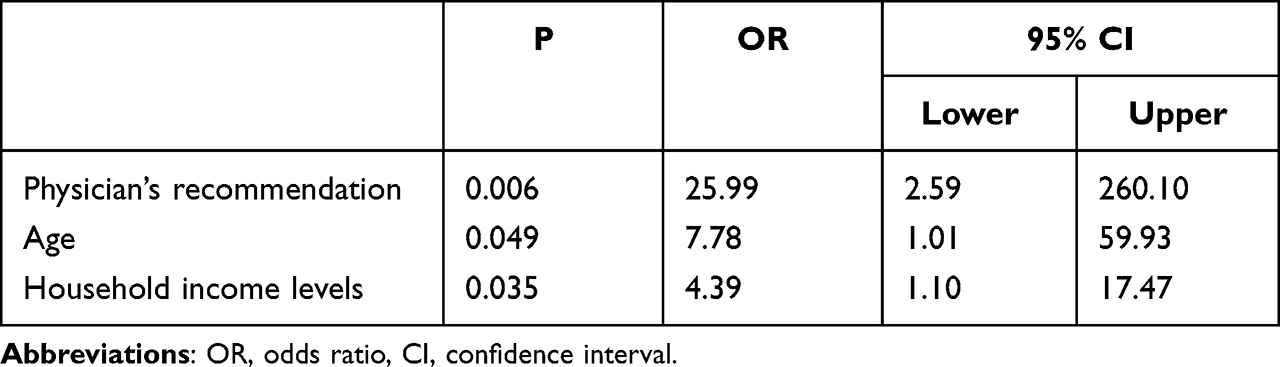 |
Table 5 Multivariate Analysis of Factors Predictive of “Met Need” |
Discussion
The SCR after cataract surgery in our population aged ≥50 years was 69.8%. To our knowledge, this is the first study to report on SCR after cataract surgery. The RAAB survey in Takeo Province, Cambodia reported that only 18/273 (6%) subjects wore spectacles after cataract surgery.9 According to the survey, cataract surgery resulted in good visual acuity in 252/345 eyes (73%).9 Refractive error after cataract surgery was found in 53/252 eyes (21.0%). Fifty-six out of 173 subjects in the RAAB survey in DKI Jakarta wore spectacles after cataract surgery. According to the RAAB survey in DKI Jakarta, cataract surgery resulted in good visual acuity in 187/252 eyes (74%). A more recent study in Sweden demonstrated a higher spectacle use postoperatively for distance glasses (48.7%).10 Tinner et al11 reported high postoperative spectacle use (97%), however, only 2 subjects (3%) wore distance glasses as they demonstrated minimum postoperative refractive errors.11
A higher proportion of “unmet need” caused low SCR and indicated unaddressed residual uncorrected refractive errors which contributed to visual impairment and blindness. Spectacles are the easiest, simplest, and lowest-cost tools for correcting refractive errors. A higher SCR would reduce the prevalence of refractive errors, visual impairment, and blindness.
The economic level of the household showed a significant difference. The higher the economic level of the household, the higher the number of “met need” and SCR. Higher household income levels are more likely to have higher SCR. This is in line with the study by Gilbert et al7 which reported varying SCR: 7.3% in low income households, 14.9% in middle income households, and 25.9% in high income households. Emamian et al12 also reported that a higher number of unmet need was found at a low socioeconomic level in Shahroud, Iran. This evidence shows that socioeconomic status is related to SCR.
The education group also had a significant difference, and groups with higher education had a higher number of met need than the other education groups. The higher the education level, the higher the number of met need and SCR. These results corresponded to SCR values in populations with refractive disorders in Baoshan district of China; Tehran, Iran; and Timor Leste.13–15
SCR in Baoshan, China increased according to the level of education, which was 15.79% in the no-education group and 63.22% in the junior/high school education or higher education group.13 The higher education group in Tehran Iran had the highest SCR (83.4%) compared to the lower education groups, with no significant difference between the study groups. SCR in the education group in the refractive error population in Timor Leste was 50.9%, while that in the no-education group was 2.8%.15
No difference in SCR was observed between employment status groups. This was in contrast to the reports of the refractive error population in Timor Leste, where the SCR was higher in the employed subject group.15 This could be explained by the type of occupation of our subjects which mostly required close-work activities, such as tailors, merchants, business owners, boarding house owners, and electronic repairs. Tailors and electronic repairs are typically associated with short-distance vision. This requires near or intermediate spectacles. The need for visual acuity tends to be affected by daily activity. However, this study did not aim to conduct further examinations of respondents’ daily activities.
The nonproductive age group had a higher SCR than the productive age group, and demonstrated a strong correlation with the number of met needs. These results were consistent with the studies conducted in Andhra Pradesh, India (with minimum age of 50) whereas age group of 70 years and above had a higher SCR (42.6%) compared to the age group of 50–69 years (23.9%).16 The results in this study were different from the studies on populations with refractive disorders in Baoshan district of China (minimum age of 60 years) and Timor Leste (minimum age of 40 years).13,15 SCR of the age group of 60–69 years in the refractive error population in Baoshan district of China was higher (56.9%) than age 70–79 (30.5%) and age 80 or older (15.69%).13 The SCR of younger age groups in the refractive error population in Timor Leste was higher than that of the older age. The SCR in the age group of 40–49 years, 50–59 years, 60–69 years and ≥ 70 years age groups in Timor Leste were 21.2%, 18.4%, 14.8%, and 11.5%, respectively. However, there was no significant difference in the refractive error population in each age group in Timor Leste (p=0.59).15
The need for spectacles as a result of age might be affected by work or daily life activities, especially among nonproductive age groups. However, this study did not aim to conduct a further analysis of the need for spectacles by age related to daily activities. The productive age group in this study did not represent the actual productive age of the population ie 15–64. The only limitation of this study was that the age of the participants was ≥ 50 years. Although there were significant differences in the productive age groups in this study, different results might have emerged if all productive ages were included in the study.
The SCR in the female group was higher than that in the male group. This was in contrast to the results of a study on other populations with refractive disorders, such as Andhra Pradesh, India, Tehran, Iran, Zoba Ma’ekel, Eritrea, Baoshan, China, and Timor Leste which revealed no difference between the two groups.13–17
Despite the high rate of insurance participation (96%), nearly half of the participants (43%) were unaware of the spectacle-related benefits. Indonesia’s National Health Insurance (NHI) provides the benefit of spectacle procurement, with the amount varying according to its class.18 Information about this benefit should be included in postoperative education. Another issue that may arise is that opticians affiliated with the NHI are still limited and not in the direct vicinity of the eye centers, thus creating barriers for spectacle procurement.
Our findings suggest that physicians’ recommendations for spectacle use were highly predictive of “met need”. Seventy-seven percent of patients who were advised to obtain distance spectacles obtained new spectacles postoperatively and 78.9% of patients who were not advised did not obtain spectacles.10 This implies the role of physicians in ensuring the continuity of care. Management of cataracts entails not only opacity removal, but also optimization of visual outcomes by integrating visual rehabilitation with cataract post-surgery care. Considering a 40% increase in the effective coverage of refractive error by 2030, our findings could serve as a basis for conceptualizing national action plans to achieve this target.
Limitations
Our study included a small number of participants and a limited age group (≥ 50 years) which might not be representative of the population. The correlation between reproductive age and SCR is yet to be determined because not all productive age categories were included in the study. Younger individuals are more likely to dispense their spectacle prescriptions compared to participants in our study. This could be a selection-bias that leads to underestimation of the spectacle coverage rate. Further studies with a larger number of respondents and wider range of demographic characteristics should be conducted.
Another limitation is the study period of this study ie 2015. Enhancements in cataract refractive surgery may have evolved ever since.
Conclusion
Unmet need for spectacles following cataract surgery causes visual impairments. Factors, such as higher household income levels and physicians’ recommendations for spectacle use, are predictive of higher spectacle use. Correction of refractive error following cataract removal and physician’s recommendation should be a part of continuity of care.
Abbreviations
BVA, best visual acuity; CI, confidence interval; IOL, intraocular lens; PVA, presenting visual acuity; SCR, spectacle coverage rate; RAAB, rapid assessment of avoidable blindness.
Acknowledgments
We thank Dr. Cicih Opitasari, MARS, and Dr. Aria Kekalih, M. T. I, for providing guidance in planning and conducting this research. This study was an extension of the Rapid Assessment of Avoidable Blindness Survey conducted in 2015 which received financial support from the Ministry of Health, Republic of Indonesia. The authors received no financial support for the authorship or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Steinmetz JD, Bourne RR, Briant PS, et al. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the right to sight: an analysis for the global burden of disease study. Lancet Glob Health. 2021;9(2):e144–e160. doi:10.1016/S2214-109X(20)30489-7
2. Antwi-Adjei EK, Owusu E, Kobia-Acquah E, Dadzie EE, Anarfi E, Wanye S. Evaluation of postoperative refractive error correction after cataract surgery. PLoS One. 2021;16(6):e0252787. doi:10.1371/journal.pone.0252787
3. Ilechie AA, Boadi-Kusi B, Ndudiri O, Ofori E. Evaluation of post-operative visual outcomes of cataract surgery in Ghana. Int J Health Res. 2012;5(1):35–42.
4. Shen W, Yang Y, Yu M, et al. Prevalence and outcomes of cataract surgery in adult rural Chinese populations of the Bai nationality in Dali: the Yunnan minority eye study. PLoS One. 2013;8(4):e60236. doi:10.1371/journal.pone.0060236
5. Gupta P, Zheng Y, Ting TW, Lamoureux EL, Cheng C-Y, Wong T-Y. Prevalence of cataract surgery and visual outcomes in Indian immigrants in Singapore: the Singapore Indian eye study. PLoS One. 2013;8(10):e75584. doi:10.1371/journal.pone.0075584
6. Vijaya L, George R, Rashima A, Raju P, Arvind H, Mani Baskaran RSV. Outcomes of cataract surgery in a rural and urban south Indian population. Indian J Ophthalmol. 2010;58(3):223. doi:10.4103/0301-4738.62648
7. Gilbert CE, Shah S, Jadoon M, et al. Poverty and blindness in Pakistan: results from the Pakistan national blindness and visual impairment survey. Br Med J. 2008;336(7634):29–32. doi:10.1136/bmj.39395.500046.AE
8. Rif’Ati L, Halim A, Lestari YD, Moeloek NF, Limburg H. Blindness and visual impairment situation in Indonesia based on rapid assessment of avoidable blindness surveys in 15 provinces. Ophthalmic Epidemiol. 2021;28(5):408–419. doi:10.1080/09286586.2020.1853178
9. Mörchen M, Langdon T, Serey Bonn T, et al. Rapid assessment of avoidable blindness in Takeo Province, Cambodia. Asia Pac J Ophthalmol. 2012;4(1):25–31. doi:10.1097/APO.0000000000000061
10. Farhoudi DB, Behndig A, Montan P, et al. Spectacle use after routine cataract surgery: a study from the Swedish National Cataract Register. Acta Ophthalmol. 2018;96(3):283–287. doi:10.1111/aos.13554
11. Tinner C, Eppenberger L, Golla K, et al. Use of spectacles after cataract surgery. Klin Monbl Augenheilkd. 2023;240(4):408–414. doi:10.1055/a-2034-6365
12. Emamian MH, Zeraati H, Majdzadeh R, Shariati M, Hashemi H, Fotouhi A. Unmet refractive need and its determinants in Shahroud, Iran. Int Ophthalmol. 2012;32(4):329–336. doi:10.1007/s10792-012-9567-8
13. Zhu M, Tong X, Zhao R, et al. Visual impairment and spectacle coverage rate in Baoshan district, China: population-based study. BMC Public Health. 2013;13(1):1–13. doi:10.1186/1471-2458-13-311
14. Fotouhi A, Hashemi H, Raissi B, Mohammad K. Uncorrected refractive errors and spectacle utilisation rate in Tehran: the unmet need. Br J Ophthalmol. 2006;90(5):534–537. doi:10.1136/bjo.2005.088344
15. Ramke J, Du Toit R, Palagyi A, Brian G, Naduvilath T. Correction of refractive error and presbyopia in Timor-Leste. Br J Ophthalmol. 2007;91(7):860–866. doi:10.1136/bjo.2006.110502
16. Marmamula S, Ravuri L, Boon MY, Khanna RC. Spectacle coverage and spectacles use among elderly population in residential care in the South Indian state of Andhra Pradesh. Biomed Res Int. 2013;2013:1–5. doi:10.1155/2013/183502
17. Chan VF, Mebrahtu G, Ramson P, Wepo M, Naidoo KS. Prevalence of refractive error and spectacle coverage in Zoba Ma’ekel Eritrea: a rapid assessment of refractive error. Ophthalmic Epidemiol. 2013;20(3):131–137. doi:10.3109/09286586.2013.783082
18. Putri AE, Paham JKN. Jaminan Kesehatan Nasional. Jakarta: Friedrich-Ebert-Stiftung; 2014.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.